Embed Size (px)
Citation preview


Objectives
Discuss the anatomy of the spine in relation to fractures or degenerative disease.
Identify common nursing goals in care of the adult spine patient.
Describe typical nursing concerns for a post-op spine patient.

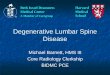
Anatomy
Bony = Vertebrae Soft tissue = Discs,
ligament Cord & Nerve Roots

Definitions
Cervical (7)
Thoracic (12)
Lumbar (5)
Sacral (5)-fused

Definitions con’t
Normal Curve-”S shaped” looking from lateral view
Scoliosis – abnormal lateral curve with rotation of vertebrae as well
Kyphosis- anterior curvature of thoracic spine
Radicular- referred pain from pressure on spinal nerve root

Spine Fracture
Etiology: Trauma vs non traumatic
•Elderly – Tumors, metabolic, renal, thyroid
Stable vs unstable Neurologic status

3 Column Theory
Anterior
Posterior third
Middle ThirdAnterior Third
Any 2 = unstable

Fractured C-Spine Examples
OdontoidHangman’s Tear drop Jefferson’s

Odontoid
Type I Type II
Most difficult to heal-shown
Type III

Hangman’s
Hyperextension and distraction
Injury occurs in anterior portion of C2 vertebrae
Piths spinal cord

Tear Drop
HyperflexionAnterior Ligament pulls off corner of anterior vertebraeUNSTABLE

Jefferson’s Fracture
Burst fracture of C1, disrupting the ring of the atlas
Spinal canal is widened
50% - NO neuro deficits
Occasionally requires fusion of occiput to C1

Complications
Atlanto-occipital dislocation Neurologic damage
Permanent or temporary below level of bony injury
Death

Diagnostic Studies Needed
X-ray 2 planes AP & x table lateral May need swimmer’s
view for ? Otontoid fx Flexion Extension C-spine Ligamentous
injury Spasm 10-14 days

Diagnostic Studies Needed con’t
CT scan MRI if nerve
injury suspected

Therapeutic Modalities
Log roll Specialty beds Braces Surgery

Surgical Spinal Fixation
Halo Posterior Spinal fusion
Rods, Hooks, Screws Anterior Spinal fusion
Plates, Cage

Nursing Interventions
Neurologic Status Documentation Sensation level Motor function Spasm Nursing / Body Mechanics Communication of findings key!!

Neurologic Status Documentation
Sensation levels Shoulder = C-5 Nipple T-4 Umbilicus T-10 Great toe L-4
Sensation Levels

Neurologic Status Documentation Motor Function EHL toe extension L4-5 Tighten Anus S 3-5 Thumb pointing up,
index finger straight ahead C-6-8
Motor Function

Nursing Considerations
Cast Syndrome Potentially life threatening syndrome caused by
hyperextension of lumbar spine that results in compression of the superior mesenteric artery-bowel ischemia
Brace use / skin care / pin care Activity / Bowels / Nutrition

Nursing Considerations
Home Care Instructions Neurovascular symptoms to report Brace use Surgical care

Question #1
Joshua, 19, was involved in a motor vehicle crash, unbelted. He reportedly has an L-2 burst fracture. As his nurse, you would:
A. Have him use the trapeze to lift himself in bed.
B. Log roll him side to side as a unit.C. Have him sit first then dangle his legs to
prevent dizziness.D. Boost him with help lifting under his armpits.

Answer #1
Joshua, 19, was involved in a motor vehicle crash, unbelted. He reportedly has an L-2 burst fracture. You will :
b. Log roll him side to side as a unit.Rationale: Log rolling a spine patient is
essential to prevent further neurological impairment

Question #2
Joshua is taken emergently to the OR for decompression and posterior spinal fusion. His post-op orders call for a TLSO. Which of the following instructions about TLSO care is correct?
a. Red and purple marks on skin under brace are normal.
b. It is acceptable to wear it loose.c. Take it off when ever you are standing upright.d. Report any vomiting or abdominal pain
immediately.

Answer #2
Joshua is taken emergently to the OR for decompression and Posterior spinal fusion. His post-op orders call for a TLSO. Which of the following statements are true?
D. Report any vomiting or abdominal pain immediately.
Rationale: Vomiting or abdominal pain might indicate compression against the abdominal cavity, causing vomiting and abdominal pain.

Spondylolysis / Spondylolisthesis
Define: Spondylo =
vertebrae Lysis = broken Listhesis = slipped
forward

Spondylolysis / Spondylolisthesis
M = F Teens or Elderly Genetics, stress, degenerative Gymnasts, football lineman, weight
lifters Elderly OA of facets > loose joints,
repetitive stress on vertebrae

Spondylolysis / Spondylolisthesis
Chronic or acute LBP Often radicular in nature Exam
Spasms + SLR Tight hamstrings

Spondylolysis / Spondylolisthesis
Treatment- Conservative Rest 3 days maximum!! /Back Brace Analgesics / Antispasmodics / ice or heat Physical therapy / Back School
(Education) Avoid painful activities

Spondylolysis / Spondylolisthesis
PSF with or without instrumentation
ASF for severe slips or failed PSF

Question #3
The surgeon has chosen to fix a spine with pedicle screws and posterior spinal fusion. During a post-op nursing assessment, which one of the following would be urgently reported to the surgeon?
a. Absent or sluggish bowel sounds.b. Pain and spasm in lower mid back.c. Inability to feel side of left thigh or move
left leg.d. Burning on urination.

Answer #3
The surgeon has chosen to fix a spine with pedicle screws and posterior spinal fusion. During pre-op nursing assessment you note this (these) urgently reportable changes related to fracture site.
C. Inability to feel side of left thigh or move left legRationale: This would be indicative of neurological
impairment and are essential to be reported immediately. The other problems are expected and/or not emergent.

Herniated Nucleus Pulposa
M > F 20-45yrs Etiology
Degeneration Abnormal body mechanics Deconditioned - Poor muscle tone Trauma

Herniated Nucleus Pulposa
History- Some Event Back and leg pain Numbness and/or dysesthesias Muscle weakness-nerve distribution ^ with sitting / sneezing, coughing Worse with valsalva

Herniated Nucleus Pulposa
Exam “Classic Sign” Painful SLR Won’t lean forward Change in sensation,
strength or reflexes Bowel or Bladder
changes

Herniated Nucleus Pulposa
Radiographs / MRI /EMG

Herniated Nucleus Pulposa
Treatment- Conservative (80%) Rest 3 days max Analgesics / Antispasmodics / ice or heat Physical therapy / Education Avoid painful activities
Epidural Steroids Surgical
Laminectomy no fusion

Question #4
Fred c/o pain, which is horrible if he sneezes. He can’t even sit in his car. He was dx with a herniated disc, hates hospitals & wants to know what else can be done besides surgery. Which of the following is the best response?
a. Rest, analgesics, antispasmodics, and back care education help 80% of the people.
b. He should continue all activity even if it is painful for 3 days.
c. There is no other treatment. He needs a fusion.d. Steroid injection it works 100% of the time.

Answer #4
Fred c/o pain, which is horrible if he sneezes. He can’t even sit in his car. He was dx with a herniated disc, hates hospitals & wants to know what else can be done besides surgery. You explain:
A. Rest, analgesics, antispasmodics, and back school help 80% of the people.
Rationale: For this type of problem, conservative treatment is the most beneficial.

Degenerative Disc Disease
M >F Not Always Elderly water content in disc Annular ligament fiber
failure Hx: back pain w/ activities
for a while May have radicular
symptoms

Spinal Cord Problems
SCI Spinal Stenosis

Spinal Cord Injury
Traumatic M>F Complete vs Incomplete
Meaning some sparing of neurological function, either sensory or motor
Level is everything!

Levels
Spinal Cord – C1-L1 Conus Medularis Dist spinal cord
Bowel Bladder Cauda Equina Lesions = Roots below
Conus L-2

Spinal Stenosis
Etiology: congenital vs acquired (degenerative)
Lumbar region most common Also called neurogenic claudication

Spinal Stenosis
Back pain, leg pain when upright Walking usually makes
symptoms worse-“neurogenic claudication”
Relieved by bending, sitting Nocturnal leg cramps

Spinal Stenosis
Exam normal Can be abnormal if severe hypertrophy of
bone in foramen, causing nerve root compression
Check pulses r/o PVD- may need ABIs Check for hip OA X-ray: normal for age but may demonstrate
hypertrophy of bone in foramen MRI to eval. nerves

Spinal Stenosis Treatment
Activity modification Altered expectations Therapy to improve endurance, strength Epidural steroids Surgery: Decompression
+/- fusion

Degenerative Scoliosis
Lateral curvature of the spine
40-50 ° may require surgery
Etiol: Degenerative disc

Kyphosis (45°)
Posterior “hump” thoracic region Etiology
Congenital Scheuermann’s disease Neuromuscular Ankylosing spondylitis Metabolic (Osteoporosis) Tumor

Ankylosing Spondylitis
M > F Inflammatory disease

Surgical Intervention
ABC’s, normal Post-op Often serious cardio- pulmonary
compromise Neurologic exams
DOCUMENT Pain control, positioning Bowel & bladder

Questions
Thank You!