Embed Size (px)
Citation preview

Observations on the Mechanisms of
Glucosuria during Glucose Loads
in Nonnal and Nondiabetic Subjects
JOHNJ. MCPHAUL,JR. and JoHN J. SIMONAITIS
From the Department of Medicine, Wilford Hall United States Air Force Hospital,Aerospace Medical Division, Air Force Systems Command,Lackland Air Force Base, Texas 78236
A B S T R A C T The study of 14 normal youngmen by glucose titration procedures has definedthe magnitude of splay in this population, differ-ing from previously reported data in its unex-pected deviation from the line of theoretic unityhigh on the titration curve. Compared to thesenormal subjects, a group of glucosuric men couldbe divided into two subclasses, those with normalmaximal rate of glucose reabsorption (TmG) andthose with subnormal TmG, both with comparablyabnormal splay. Most consistent glucosurics fallinto the latter group. Nephritic patients studiedwere not such a homogeneous group in terms ofage and sex, but did manifest an abnormal splayduring their titration curves in most cases. Theyalso demonstrated a greater than normal reab-sorptive rate of glucose per unit measured glo-merular filtration rate. It is concluded that renalglucosuria must be defined not only in terms ofthe concept of TmGbut also by deviation of theglucose titration curve expressing an unusual de-gree of splay. The latter is presumed, as has beensuggested by others, to be a characteristic ofnonhomogeneity of glucose handling units in thekidney. This seems subject to exaggeration in
Major McPhaul's present address is the Department ofExperimental Pathology, Scripps Clinic and ResearchFoundation, La Jolla, Calif. 90237.
Major Simonaitis' present address is the MalcolmGrow United States Air Force Hospital, Andrews AirForce Base, Md. 21605.
Received for publication 20 April 1967 and in revisedform 4 October 1967.
the adaptations which accompanydisease.
chronic renal
INTRODUCTIONMarble (1) has proposed stringent criteria forthe definition and identification of classic or truerenal glucosuria, and has estimated its incidenceat approximately 0.1-0.4 % of the general popu-lation. Nevertheless, reports from surveys ofmilitary recruits at induction centers, factoryworkers, and a variety of pathophysiologicalstates associated with disordered metabolism,such as pregnancy and nephritis, have suggestedthat nondiabetic glucosuria may be encounteredrelatively frequently (2-5).
The mechanisms by which either occasional orconsistent glucosuria is initiated have not beeninvestigated systematically in man. Studies ofsaturation kinetics of renal tubular transport,first by Shannon and Fisher (6) in dogs andlater by Smith (7) in humans, have suggestedthat glucose is actively reabsorbed in the mam-malian nephron and that a limiting rate of trans-port, TmG, can be defined (8). Analysis of thesestudies and subsequent investigations by others(9, 10) have led to the hypothesis that the de-viation from a linear relationship between the fil-tered and reabsorbed glucose (splay) encounteredduring glucose titrations is representative of anonhomogeneity of nephron populations com-prising the kidney.
Review of published material indicated a dearth
702 The Journal of Clinical Investigation Volume 47 1968
of information which compares glucose titrationsin normal young men against men with glucos-uria (7, 11). In an effort to define similaritiesand differences in the renal handling of glucoseloads by normal young men, men with glucosuria,and patients with chronic nephritis, a series ofglucose titrations was performed on representa-tive groups of subjects.
In addition to confirming the magnitude of themaximum reabsorptive rate of glucose in nor-mal men, these studies indicated a lesser titrationsplay than has been described before. On the otherhand, glucosuric men, either with true renal glu-cosuria or a sporadic variety of inconsistent non-diabetic glucosuria, seem to posses the commoncharacteristic of an abnormal splay of their titra-tion curves. This latter characteristic is also man-ifest in many patients with nephritis, with andwithout renal insufficiency.
METHODSGlucose titrations were performed in 14 normal youngmale volunteers between the ages of 17 and 28 yr; allwere screened by history, physical examination, andurinalysis, and found free of obvious disease; none hadglucosuria. Two other subjects underwent determina-tions of Tm. without titration. These 16 subjects com-
1.2
I.0
0.8 A
0E
NI.-0P
0.6
0.4
0.2
0
prise the control group. The glucosuric group of pa-tients were 14 servicemen referred to us for evaluationof demonstrated glucosuria, after screening examina-tions had found them otherwise free of disease. Allhad at least two normal glucose tolerance tests with100 g glucose loads by mouth. Certain characteristicsof these subjects are tabulated in Table II. Consistentglucosuria is defined as glucosuria occurring on mostoccasions; rare urinalyses were glucose free. Occa-sional glucosuria represented -uncommon and inconsistentdetection of glucosuria discovered on more than oneoccasion. The third group studied were 10 biopsy-provennephritic patients who underwent investigation in thecourse of general evaluation, either in the outpatientclinic or on the renal ward at Wilford Hall UnitedStates Air Force Hospital. All had proteinuria, ab-normal urinary sediments, and history of renal disease.All but case 10 were normotensive; all were studiedoff medication and had normal glucose tolerance tests.Relevant clinical data from this group of patients aredisplayed in Table III.
Glucose titrations were performed in the forenoonwhile the subjects were fasting, and during water hy-dration by mouth after all subjects were duly informedand gave their consent. Urine was collected through anindwelling rubber catheter directly into graduated cyl-inders. After a suitable priming dose of inulin was ad-ministered intravenously, maintenance inulin in normalsaline was given by infusion pump at a rate of 3.15 ml/min to maintain a plasma level between 20 and 30 mg/100 ml. After collection of control period specimens,
0.2 0.4 0.6 0.8 1.0 1.2 1.4 i.6 i.8 2.0
LOAD/TmG
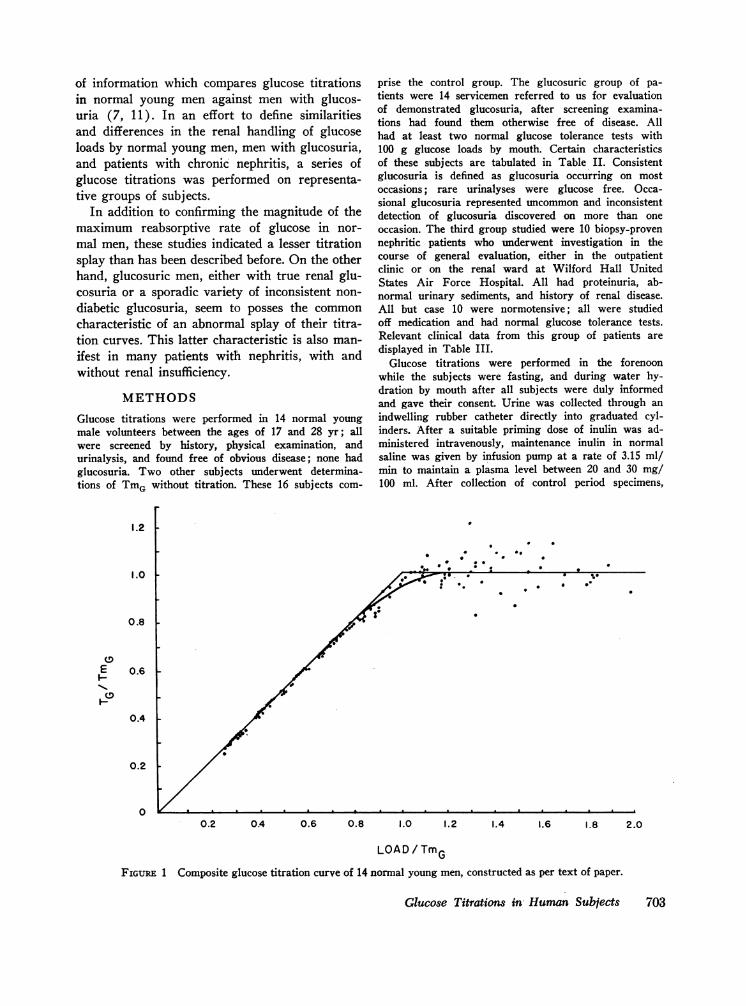
FIGURE 1 Composite glucose titration curve of 14 normal young men, constructed as per text of paper.
Glucose Titrations in Human Subjects 703
* * *-
we administered glucose loads as a 30% solution ofglucose in water at increasing pump speeds, using aseparate Bowman infusion pump. Arterial samples weredrawn via an indwelling arterial needle into heparinizedsyringes at appropriate intervals during each collectionperiod; 12-16 periods of 12-15 min duration were mea-sured in all subjects. Inulin was yeasted twice with freshbaker's yeast and then measured by the method ofSchreiner (12). Glucose was measured, with glucoseoxidase, by the technique of Washko and Rice (13).To ascertain the presence of isolated or multiple tubularexcretory abnormalities, phosphorus was measured by themethod described by Fiske and Subbarow (14) and uricacid by the uricase method of Feichtmeir and Wrenn(15).
We constructed smoothed titration curves as describedby Smith (7), plotted the rate of reabsorbed glucose(TG)/TmG against the load of glucose filtered (load)/Tm0 for each individual period, and drafted the individualcurves by visual approximation. Splay for each individualpatient was determined from the deviation of the curveof approximation drawn for each subject from the theo-retical reabsorption line. The average titration curve forall normal, nonglucosuric subjects was constructed in thesame manner and is reproduced in Fig. 1: the compara-tive groups are graphed in Figs. 2-5.
Statistical analysis, using approximate t tests, was per-formed according to Steel and Torrie (16) to comparenormal and glucosuric groups.
RESULTS
Normal subjects. Data from the different groupsof subjects are tabulated separately in Tables I, II,
and III. The normal control group (Table I) ofnonglucosuric young men had corrected, meanglomerular filtration rates (GFR) of 127 ml/min,not significantly different from our larger controlgroup of 31 men whose average GFRwas 124 ±12 ml/min. The mean TmGmeasured as the av-erage of three or more consecutive periods afterachievement of a stable value at satisfactory load/TmGlevel is 325 ± 36 mg/min (corrected to 1.73m2 body surface area). The latter figure is in rea-sonable accord with Smith's published values of375 ± 79.7 mg/min in a larger group of men. Themean point of splay from the theoretical reabsorp-tive line, as estimated from the individual curves,is 0.83 ± 0.04. This defines a much smaller splaythan previously published data on normal subjectshas indicated (7, 11). Although load to TmGra-tios in subjects 3, 8, 9, and 10 of Table I are inthe range of 1.17-1.27, collection and analysis ofadditional periods as part of another study, be-yond the periods used for calculation of TmG, in-dicated a stable reabsorptive rate at much higherload to Tmg ratios; this gave assurance that themaximal reabsorptive rate was indeed reached.TmGcorrected for body surface area and 100 mlof GFR yield a mean value of 234 ± 21 mg (1SD)/min.
TABLE I
Tabulation of Functional Data in Normal Subjects
Tmo/1.73 m2CInulin corrected TmGcorrected per 100 ml
Patient Age to 1.73 m2 to 1.73 m2 GFR Splay point Load/TmG
1 20 133 331 258 1.842 26 94 290 249 1.763 20 132 326 222 0.83 1.194 18 138 353 257 0.80 1.845 24 115 325 264 0.81 1.366 18 118 306 235 0.81 1.407 19 140 314 225 0.81 1.618 18 120 331 249 0.80 1.279 18 130 276 182 0.91 1.18
10 19 106 290 222 0.82 1.1711 17 105 270 223 0.80 1.6612 20 117 297 237 0.88 1.7613 22 149 375 239 0.80 1.9314 23 147 356 213 0.92 1.3215 24 140 390 250 0.86 2.4916 28 149 370 225 0.79 1.65
Mean 127 325 234 0.831 SD =117 ±t36 ±21 40.04
704 J. J. McPhaul, Jr. and J. J. Simonaitis
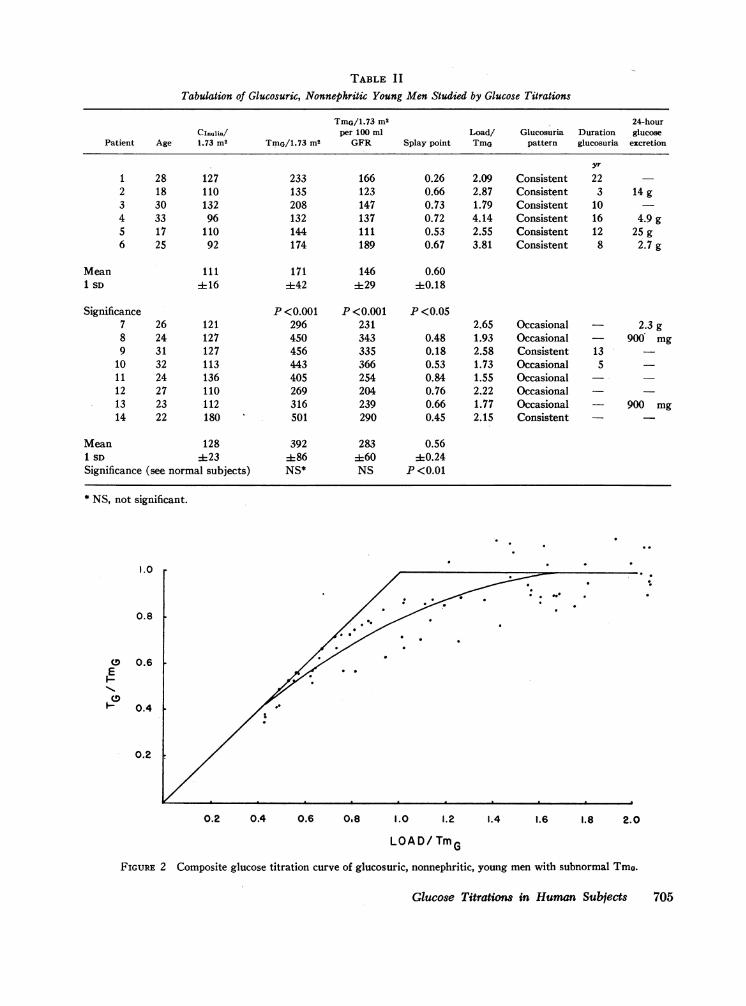
TABLE I ITabulation of Glucosuric, Nonnephritic Young Men Studied by Glucose Titrations
Tma/1.73 m2 24-hourCInulin/ per 100 ml Load/ Glucosuria Duration glucose
Patient Age 1.73 m2 TmG/1.73 m2 GFR Splay point TmG pattern glucosuria excretion
yr
1 28 127 233 166 0.26 2.09 Consistent 222 18 110 135 123 0.66 2.87 Consistent 3 14 g3 30 132 208 147 0.73 1.79 Consistent 104 33 96 132 137 0.72 4.14 Consistent 16 4.9 g5 17 110 144 111 0.53 2.55 Consistent 12 25 g6 25 92 174 189 0.67 3.81 Consistent 8 2.7 g
Mean 111 171 146 0.601 SD ±16 ±42 ±29 40.18
Significance P <0.001 P <0.001 P <0.057 26 121 296 231 2.65 Occasional 2.3 g8 24 127 450 343 0.48 1.93 Occasional - 900 mg9 31 127 456 335 0.18 2.58 Consistent 13
10 32 113 443 366 0.53 1.73 Occasional 511 24 136 405 254 0.84 1.55 Occasional --12 27 110 269 204 0.76 2.22 Occasional13 23 112 316 239 0.66 1.77 Occasional - 900 mg14 22 180 501 290 0.45 2.15 Consistent
Mean 128 392 283 0.561 SD ±23 ±86 ±60 ±0.24Significance (see normal subjects) NS* NS P<0.01
* NS, not significant.
1.0
0.8
CD 0.6E
0.4
0.2
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
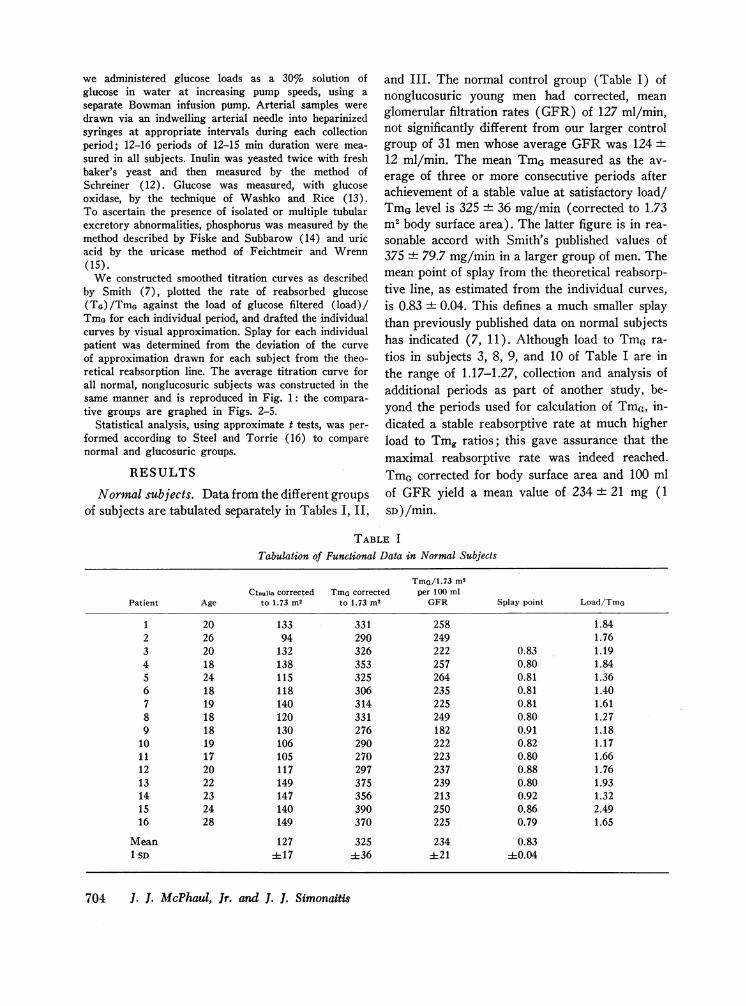
LOAD/ TmGFIGURE 2 Composite glucose titration curve of glucosuric, nonnephritic, young men with subnormal TmG.
Glucose Titrations in Human Subjects 705
1.0
0.8
0.6
0.4
0.2
0.2 0.4 0.6 0.8 1.0 1. 1.4 1.6 1.8 2.0
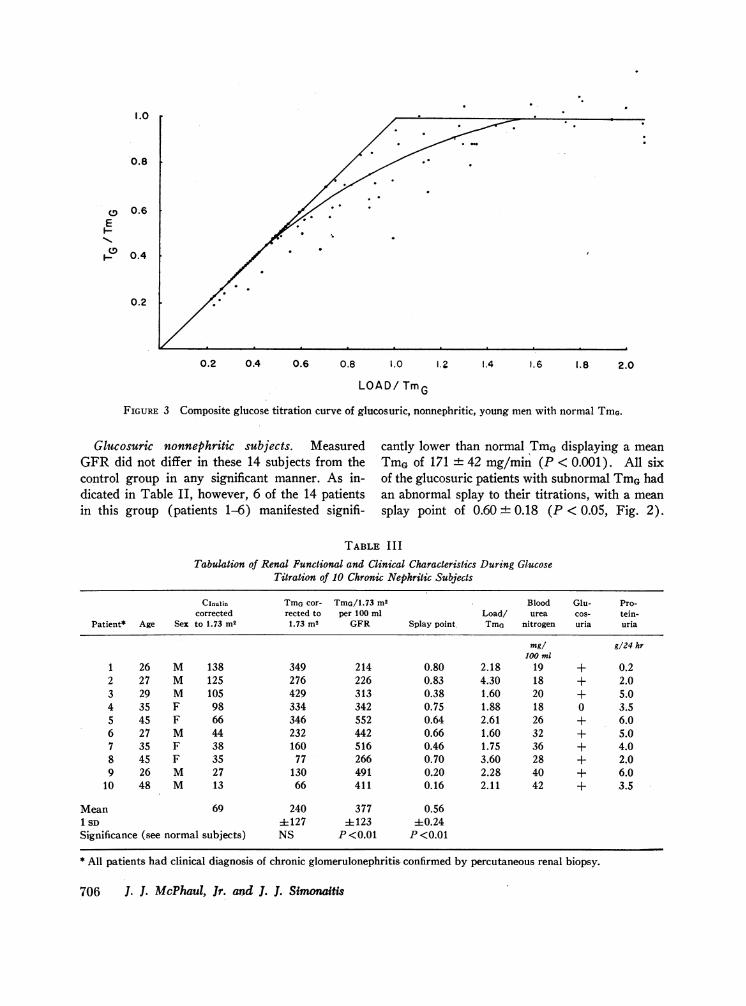
LOAD/ TmGFIGURE 3 Composite glucose titration curve of glucosuric, nonnephritic, young men with normal TmG.
Glucosuric nonnephritic subjects. MeasuredGFRdid not differ in these 14 subjects from thecontrol group in any significant manner. As in-dicated in Table II, however, 6 of the 14 patientsin this group (patients 1-6) manifested signifi-
cantly lower than normal TmGdisplaying a mean
TmGof 171 42 mg/min (P < 0.001). All sixof the glucosuric patients with subnormal TmGhadan abnormal splay to their titrations, with a mean
splay point of 0.60 + 0.18 (P < 0.05, Fig. 2).
TABLE I II
Tabulation of Renal Functional and Clinical Characteristics During GlucoseTitration of 10 Chronic Nephritic Subjects
CInulin TmGcor- TmG/1.73 m2 Blood Glu- Pro-corrected rected to per 100 ml Load/ urea cos- tein-
Patient* Age Sex to 1.73 m2 1.73 m2 GFR Splay point Tma nitrogen uria uria
mg/ g/24 hr100 ml
1 26 M 138 349 214 0.80 2.18 19 + 0.22 27 M 125 276 226 0.83 4.30 18 + 2.03 29 M 105 429 313 0.38 1.60 20 + 5.04 35 F 98 334 342 0.75 1.88 18 0 3.55 45 F 66 346 552 0.64 2.61 26 + 6.06 27 M 44 232 442 0.66 1.60 32 + 5.07 35 F 38 160 516 0.46 1.75 36 + 4.08 45 F 35 77 266 0.70 3.60 28 + 2.09 26 M 27 130 491 0.20 2.28 40 + 6.0
10 48 M 13 66 411 0.16 2.11 42 + 3.5
Mean 69 240 377 0.561 SD 4127 4123 40.24Significance (see normal subjects) NS P <0.01 P <0.01
* All patients had clinical diagnosis of chronic glomerulonephritis confirmed by percutaneous renal biopsy.
706 J. J. McPhaul, Jr. and J. J. Simonaitis
0E
"I-0
1.0
0.8
0.6E
0.4
0.2
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
LOAD/TmG
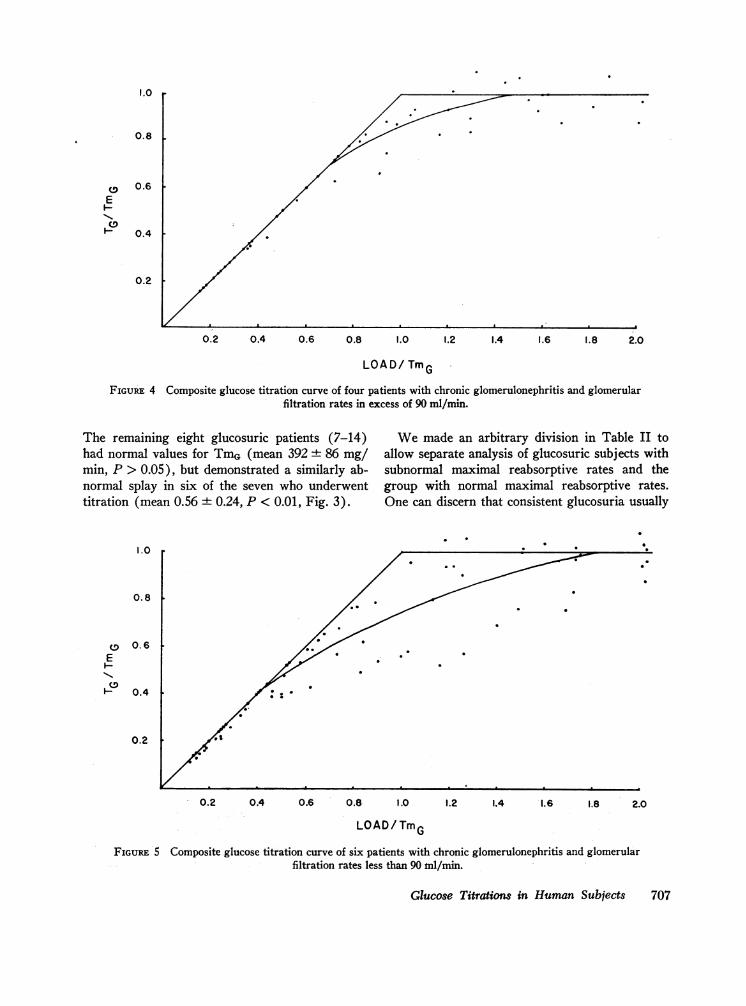
FIGURE 4 Composite glucose titration curve of four patients with chronic glomerulonephritis and glomerularfiltration rates in excess of 90 ml/min.
The remaining eight glucosuric patients (7-14)had normal values for TmG(mean 392 86 mg/min, P > 0.05), but demonstrated a similarly ab-normal splay in six of the seven who underwenttitration (mean 0.56 + 0.24, P < 0.01, Fig. 3).
I.0
0.8
0
E
Hp
0.6
0.4
0.2
Wemade an arbitrary division in Table II toallow separate analysis of glucosuric subjects withsubnormal maximal reabsorptive rates and thegroup with normal maximal reabsorptive rates.One can discern that consistent glucosuria usually
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
LOAD/TmG
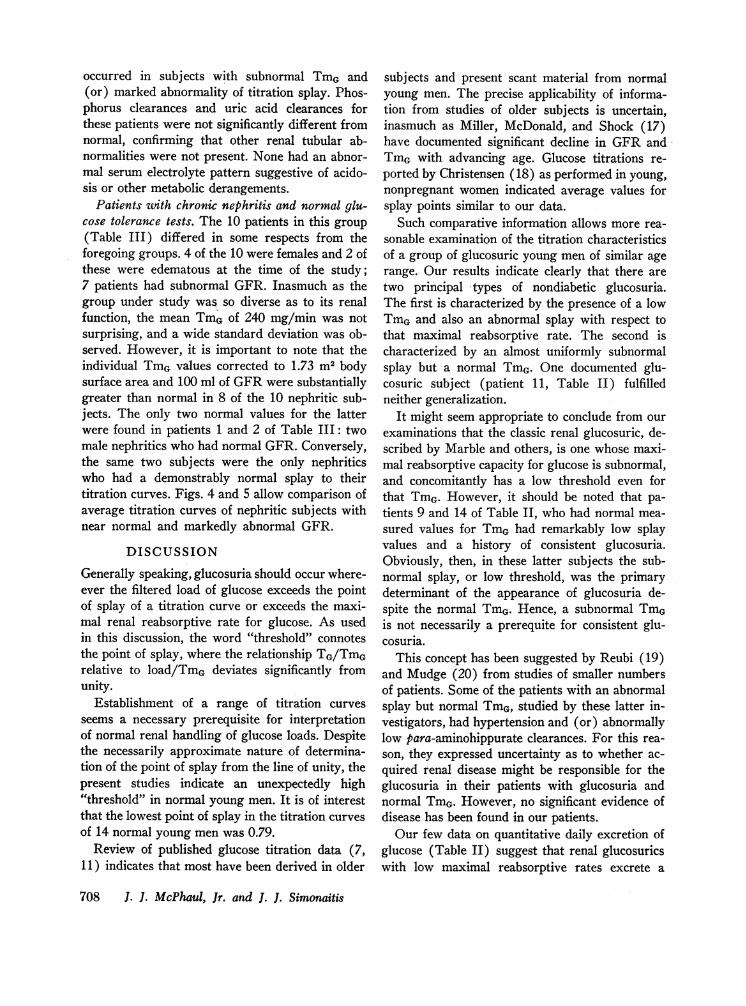
FIGURE 5 Composite glucose titration curve of six patients with chronic glomerulonephritis and glomerularfiltration rates less than 90 ml/min.
Glucose Titrations in Human Subjects 707
I
I.
occurred in subjects with subnormal TmG and(or) marked abnormality of titration splay. Phos-phorus clearances and uric acid clearances forthese patients were not significantly different fromnormal, confirming that other renal tubular ab-normalities were not present. None had an abnor-mal serum electrolyte pattern suggestive of acido-sis or other metabolic derangements.
Patients wvith chronic nephritis and normal glu-cose tolerance tests. The 10 patients in this group(Table III) differed in some respects from theforegoing groups. 4 of the 10 were females and 2 ofthese were edematous at the time of the study;7 patients had subnormal GFR. Inasmuch as thegroup under study was so diverse as to its renalfunction, the mean TmGof 240 mg/min was notsurprising, and a wide standard deviation was ob-served. However, it is important to note that theindividual TmGvalues corrected to 1.73 m2 bodysurface area and 100 ml of GFRwere substantiallygreater than normal in 8 of the 10 nephritic sub-jects. The only two normal values for the latterwere found in patients 1 and 2 of Table III: twomale nephritics who had normal GFR. Conversely,the same two subjects were the only nephriticswho had a demonstrably normal splay to theirtitration curves. Figs. 4 and 5 allow comparison ofaverage titration curves of nephritic subjects withnear normal and markedly abnormal GFR.
DISCUSSION
Generally speaking, glucosuria should occur where-ever the filtered load of glucose exceeds the pointof splay of a titration curve or exceeds the maxi-mal renal reabsorptive rate for glucose. As usedin this discussion, the word "threshold" connotesthe point of splay, where the relationship TG/TmGrelative to load/TmG deviates significantly fromunity.
Establishment of a range of titration curvesseems a necessary prerequisite for interpretationof normal renal handling of glucose loads. Despitethe necessarily approximate nature of determina-tion of the point of splay from the line of unity, thepresent studies indicate an unexpectedly high"threshold" in normal young men. It is of interestthat the lowest point of splay in the titration curvesof 14 normal young men was 0.79.
Review of published glucose titration data (7,11 ) indicates that most have been derived in older
subjects and present scant material from normalyoung men. The precise applicability of informa-tion from studies of older subjects is uncertain,inasmuch as Miller, McDonald, and Shock (17)have documented significant decline in GFRandTmGwith advancing age. Glucose titrations re-ported by Christensen (18) as performed in young,nonpregnant women indicated average values forsplay points similar to our data.
Such comparative information allows more rea-sonable examination of the titration characteristicsof a group of glucosuric young men of similar agerange. Our results indicate clearly that there aretwo principal types of nondiabetic glucosuria.The first is characterized by the presence of a lowTmGand also an abnormal splay with respect tothat maximal reabsorptive rate. The second ischaracterized by an almost uniformly subnormalsplay but a normal TmG. One documented glu-cosuric subject (patient 11, Table II) fulfilledneither generalization.
It might seem appropriate to conclude from ourexaminations that the classic renal glucosuric, de-scribed by Marble and others, is one whose maxi-mal reabsorptive capacity for glucose is subnormal,and concomitantly has a low threshold even forthat TmG. However, it should be noted that pa-tients 9 and 14 of Table II, who had normal mea-sured values for TmGhad remarkably low splayvalues and a history of consistent glucosuria.Obviously, then, in these latter subjects the sub-normal splay, or low threshold, was the primarydeterminant of the appearance of glucosuria de-spite the normal TmG. Hence, a subnormal TmGis not necessarily a prerequite for consistent glu-cosuria.
This concept has been suggested by Reubi (19)and Mudge (20) from studies of smaller numbersof patients. Some of the patients with an abnormalsplay but normal TmG, studied by these latter in-vestigators, had hypertension and (or) abnormallylow para-aminohippurate clearances. For this rea-son, they expressed uncertainty as to whether ac-quired renal disease might be responsible for theglucosuria in their patients with glucosuria andnormal TmG. However, no significant evidence ofdisease has been found in our patients.
Our few data on quantitative daily excretion ofglucose (Table II) suggest that renal glucosuricswith low maximal reabsorptive rates excrete a
708 J. J. McPhaul, Jr. and J. J. Simonaitis
greater amount of glucose than the glucosuricswhose titration curves are characterized by thesplay deviation but whose TmGis normal. Thisemphasizes the suggestion that splay determinesthe threshold for appearance of recognizable glu-cosuria whereas the maximum reabsorptive rateis the usual determinant of the magnitude of mea-sured glucosuria.
Examination of the nephritic patients, all ofwhom had normal glucose tolerance tests and allbut one of whom (patient 4, Table III) was glu-cosuric, is also of interest in the present context.Only two of these patients had normal splay; theselatter were subjects with normal GFR. Althoughthe measured TmGnecessarily displayed a widerange, it tended to be preserved disproportionatelyin the face of declining renal function. The net re-sult is that correction of the measured individualglucose Tm of the nephritic patient to body sur-face area and GFR proportionate to the nonne-phritic subjects indicates a supranormal reabsorp-tive rate per nephron unit in all the nephritic pa-tients with compromised renal function.
The frequency of the observed glucosuria in thechronic nephritic patients probably is conditionedby the same factor noted in the nonnephritic pa-tients; namely, the high incidence of abnormalsplay. The latter probably indicates a greater thannormal nonhomogeneity of nephron units amongthe residual functioning nephrons.
Several alterations of normal pathophysiologicalrelationships may be implicated in the latter.These include changes in perfusion to corticalnephrons and alterations of structure of proximaltubular epithelial cells due to hypertrophy, dilata-tion, and lipid infiltration. Other factors to beconsidered are general depression of proximaltubular reabsorptive activity and passive back dif-fusion of glucose into tubules through an anatomi-cally disrupted architecture at higher blood sugarlevels.
Although our data do not allow us to choosecritically between such diverse possibilities, thereis experimental support for some of them. Ab-normalities of para-aminohippurate extractionhave been documented in advanced nephritis byBradley, Bradley, Tyson, Curry, and Blake (21),and in shock associated with marked decrease inGFR by Lauson, Bradley, and Cournand (22),indicating that alteration of tubular perfusion pat-
terns may occur. Microdissection of whole neph-rons from kidneys from patients with chronicnephritis indicated frequent occurrence of atrophicnephrons in association with dilated and hyper-plastic nephrons, some of which were lipid-ladenand grossly distorted (23, 24). Similarly, a dis-crete, spotty, anatomic lesion of proximal tubuleshas been invoked by Monasterio, Oliver, Muiesan,Pardelli, Marinozzi, and MacDowell as an ex-planation for the observed splay in their subjectswith true renal diabetes (25).
Our results stand in contrast to the observationsof Rieselbach, Shankel, Slatopolsky, Lubowitz, andBricker (26) in man and Shankel, Robson, andBricker in the rat (27) in two respects. In theformer study, no abnormality of splay was detecteduntil advanced renal insufficiency supervened.This can be reconciled with our data inasmuch asthe splay of our nephritic patients with more andless advanced renal insufficiency was quite compar-able to theirs and clearly different from the groupof normal men (P < 0.01) reported herein. Sec-ondly, TmGcorrected to proportionate body sur-face area and GFR in nephritic patients of thisseries was significantly greater than normal (P <0.01). Although Rieselbach et al. implied that thenephritic patients they studied showed no suchrelative increase in glucose reabsorption per neph-ron, the mean inulin clearance/TmG ratio of theirpatients was 0.305, comparable to the value of thisratio for nephritic patients in this series (0.285,P > 0.05) and significantly different from normalsubjects (0.391, P < 0.01). That no such adap-tation was observed in experimentally diseased kid-neys of rats (27), may be due to the abrupt onsetof the lesion and the relatively short duration al-lowed for adaptation. Oliver (24) has suggestedthat an intermittency of disease is most advantage-ous for optimal development of maximal architec-tural adaptation. There can be no doubt, however,that as GFRdeclines, a greater osmolar clearanceper unit GFRdoes occur and conceivably mightexaggerate splay characteristics of the diseasedkidney (27, 28).
Despite the indication from our data that anabnormal splay is the most frequent abnormalityand likeliest explanation for either consistent oroccasional glucosuria in nondiabetic subjects, withand without nephritis, one nonnephritic subject(patient 11, Table II) and two nephritic subjects
Glucose Titrations in Human Subjects 709
(patients 1 and 2, Table III) had both normalsplay patterns and TmG. An explanation for theirglucosuria cannot be made to our complete satis-faction.
It is suspected that the glucosuria in these sub-jects may have been noted because of factors whichare not often mentioned but which should be con-sidered: the sensitivity of screening tests, the rela-tive differences of arterial and venous glucose con-centrations, and the contribution of a high GFR.Commercially prepared strips of paper impreg-nated with glucose oxidase are widely used formass screening tests of urine. Although clearlydemonstrated by O'Sullivan, Kantor, and Wilker-son (29), it is not recognized widely that thesestrips are exquisitely sensitive to relatively lowconcentrations of urinary glucose. Such eoncen-trations may be detected in many otherwise nor-mal people after a usual meal, as indicated byFine (3).
A relatively modest and transient rise of ar-terial glucose concentration in association with ahigh GFRand normal splay can result in a glucoseload which exceeds a "normal" threshold and causeglucosuria, despite normal glucose tolerance tests.
It is concluded that there are two general typesof glucosuric nondiabetic subjects: (a) peoplewith a low Tmg and abnormal splay, and (b)people with normal Tmg and abnormal splay. Glu-cosuria occurring during the course of chronicrenal disease usually is a manifestation of the lattertype of mechanism.
ACKNOWLEDGMENTThe assistance of Mr. Alton Rahe, Biomedical Statisti-cian, School of Aviation Medicine, Brooks Air ForceBase, is gratefully acknowledged.
REFERENCES
1. Marble, A. 1959. Non-diabetic mellituria. In Treat-ment of Diabetes Mellitus. E. P. Joslin, H. F. Root,P. White, and A. Marble, editors. Lea & Febiger,Philadelphia. 717.
2. Peel, A. A. F., and M. W. Peel. 1941. Glycosuria incruits. Glasgow Med. J. 135: 141.
3. Fine, J. 1965. Glucose content of normal urine. Brit.Med. J. 1: 1209.
4. Hawkins, J. A., E. MacKay, and D. D. Van Slyke.1929. Glucose excretion in Bright's disease. J. Clin.Invest. 8: 107.
5. Donato, L., and G. Turchetti. 1955. Renal glycosuriain pregnancy. Acta Med. Scand. 152: 223.
6. Shannon, J. A., and S. Fisher. 1938. The renal tubularreabsorption of glucose in the normal dog. Am. J.Physiol. 122: 765.
7. Smith, H. W. 1943. Application of saturation methodsto the study of glomerular and tubular function in thehuman kidney. In Lectures on the Kidney. UniversityExtension Division, University of Kansas, Lawrence.83.
8. Burgen, A. S. V. 1956. A theoretical treatment ofglucose reabsorption in the kidney. Can. J. Biochem.Physiol. 34: 466.
9. Oliver, J., and M. MacDowell. 1961. The structuraland functional aspects of the handling of glucose bythe nephrons and the kidney and their correction bymeans of structural-functional equivalents. J. Clin.Invest. 40: 1093.
10. Bradley, S. E., J. H. Laragh, H. 0. Wheeler, M.MacDowell, and J. Oliver. 1961. Correlation of struc-ture and function in the handling of glucose by thenephronis of the canine kidney. J. Clin. Invest. 40: 113.
11. Letteri, J. M., and L. G. Wesson, Jr. 1965. Glucosetitration curves as an estimate of intrarenal distribu-tion of glomerular filtrate in patients with congestiveheart failure. J. Lab. Clin. Med. 65: 387.
12. Schreiner, G. E. 1950. Determination of inulin bymeans of resorcinol. Proc. Soc. Exptl. Biol. 74: 117.
13. Washko, M. E., and E. W. Rice. 1961. Determinationof glucose by an improved enzymatic procedure. Clin.Chem. 7: 542.
14. Fiske, C. H., and Y. Subbarow. 1925. The colori-metric determination of phosphorus. J. Biol. Chem.66: 375.
15. Feichtmeir, T. V., and H. T. Wrenn. 1955. Directdetermination of uric acid using uricase. Am. J. Clin.Pathol. 25: 833.
16. Steel, R. G. D., and J. H. Torrie. 1960. Principles andprocedures of statistics. McGraw-Hill Book Company,New York. 67.
17. Miller, J. H., R. K. McDonald, and N. W. Shock.1952. Age changes in the maximal rate of renaltubular reabsorption of glucose. J. Gerontol. 7: 196.
18. Christensen, P. J. 1958. Tubular reabsorption of glu-cose during pregnancy. Scand. J. Clin. Lab. Invest.10: 364.
19. Reubi, F. C. 1954. Glucose titration in renal glycosuria.In Ciba Foundation symposium on the Kidney. A. A.G. Lewis and G. E. W. Wolstenholme, editors. Little,Brown and Company, Boston. 96.
20. Mudge, G. H. 1956. Disorders of renal tubular func-tion. Am. J. Med. 20: 448.
21. Bradley, S. E., G. P. Bradley, C. J. Tyson, J. J.Curry, and W. D. Blake. 1950. Renal function inrenal diseases. Am. J. Med. 9: 766.
22. Lauson, H. D., S. E. Bradley, and A. Cournand. 1944.The renal circulation in shock. J. Clin. Invest. 23: 381.
23. Oliver, J. 1939. Architecture of the Kidney in ChronicBright's Disease. Hoeber-Harper Bros., New York.102.
710 J. J. McPhaul, Jr. and J. J. Simonaitis

24. Oliver, J. 1944. New directions in renal morphology.A method, its results and its future. In The HarveyLectures. Academic Press, Inc., New York. 102.
25. Monasterio, G., J. Oliver, G. Muiesan, G. Pardelli, V.Marinozzi, and M. MacDowell. 1964. Renal diabetesas a congenital tubular dysplasia. Am. J. Med. 37: 44.
26. Rieselbach, R. E., S. W. Shankel, E. Slatopolsky, H.Lubowitz, and N. S. Bricker. 1967. Glucose titrationstudies in patients with chronic progressive renal dis-ease. J. Clin. Invest. 46: 157.
27. Shankel, S. W., A. M. Robson, and N. S. Bricker.1967. On the mechanism of splay in the glucose titra-tion curve in advanced renal disease in the rat. J.Clin. Invest. 46: 164.
28. Callaway, C. P. 1950. Unilateral renal glycosuria inassociation with diabetes mellitus and chronic pyelo-nephritis. Ann. Internal. Med. 33: 243.
29. O'Sullivan, J. B., N. Kantor, and H. L. C. Wilker-son. 1962. Comparative value of tests for urinaryglucose. Diabetes. 11: 53.
Glucose Titrations in Human Subjects 711