Embed Size (px)
Citation preview
OBSERVATIONS ON PARTIAL ATRIO-VENTRICULAR HEART BLOCK INTHE HORSE
J. R. Holmes* and B. J. Alps*
INTRODUCIION
THE PROBLEM of assessing the clinical sig-nificance of partial heart block in horseshas been a controversial subject for manyyears because missed beats occur at restin a large number of apparently healthyhorses.
Atrioventricular heart block has beendefined as "an abnormal mechanism inwhich there is delay in, or absence of,ventricular responses to the auricular im-pulses" (17). It is reported to be one ofthe more common disorders of the heartbeat in man (9, 14).
Partial heart block (P.A.V.B.) in thehorse has been described (1, 2, 6, 7, 8,21, 22, 37). It has also been observed inassociation with other disorders in thehorse (18, 24, 28, 32, 33, 34, 38).
INCIDENCE OF P.A.V.B.
Second degree P.A.V.B. was observedin 16% of apparently normal horses whichwere examined and impaired ventricularconduction was present in 60 out of 100horses with cardiac arrhythmias (22).Moretti (19) considered that the Wencke-bach type of block was one of the mostcommon arrhythmias affecting horses. Ithas been reported that 16.9% of a totalof 306 racehorses demonstrated electro-cardiographic evidence of P.A.V.B. atsome stage of their racing careers (31).Second degree P.A.V.B. was observed in6.4% of a total of 332 apparently healthyhorses (13). Included in this total were38 horses which had completed the re-quirements of Three Day Event Trials;10.5% of these demonstrated second degreeP.A.V.B. at rest. It has been stated thatfrom 10 to 15% of horses with no othersigns of heart disease have P.A.V.B. andcontinue to work for years (5).
*Department of Veterinary Medicine, Uni-versity of Bristol, Bristol, England.
CLASSIFICATION OF ATRIOVENTRICULARHEART BLOCK
Atrioventricular block can occur in fourdegrees:
(1) First degree partial heart block.The atrioventricular transmission time isprolonged but every impulse reaches theventricles.
(2) Second degree partial heart block.Some of the atrial impulses fail to reachthe ventricles which therefore do not con-tract. One form of this condition is knownas the Wenckebach phenomenon (36).
(3) Third degree partial heart block.Only a few atrial impulses reach theventricles.
(4) Complete heart block. None of theatrial impulses reach the ventricles. Theventricles are then controlled by an idio-ventricular pacemaker which beats at aslower rate than the sinus node.On electrocardiographic examination,
the Wenckebach phenomenon can bedivided into two basic types: Type 1.The P-Q interval increases progressivelyuntil a beat is dropped. There are severalvariations of this type of block. Type 2.The missed beat occurs without any altera-tion in the P-Q interval.
There may be a regular block when onebeat is dropped out of a given repeatablenumber. Occasionally, paired missed beatsoccur.
The mechanism of the Wenckebachphenomenon in relation to A.V. conduc-tivity has been explained (14).The electrocardiograms (E.C.G.'s) of
some cases of P.A.V.B. in horses demon-strated that the P-Q intervals fluctuatedbetween certain maximum and minimumvalues without missed beats occurring (3).This condition has been termed "floatingP-Q interval".
MECHANISM AND ETIOLOGY
A.V. conduction disturbances havebeen presented and discussed (3, 35).The etiology of partial heart block in
,80
CAN. VET. JOUR., vol. 7, no. 12, December, 1966
HEART BLOCK IN HORSES
horses involving the refractory periodof the myocardium, which is affected bythe autonomic nervous system or injurydepressing conductivity, has been reported(29, 30).The mechanism of the irregular sinus
rhythm in A.V. block has been described(27). These workers considered that theslowing of sinus rhythm is caused by reflexinhibition of the sinus node through theaortic arch and carotid sinus reflexes(depressor reflexes). Brooijmans (3) re-ported that blood pressure graduallybuilds up in the large arteries during aconsecutive series of beats. This causes agradual increase in vagal tone whichresults in a progressive decrease in sinusfrequency, and is one of the contributingfactors in the gradual lengthening of theA.V. conduction time observed in theWenckebach block. During block, thearterial pressure falls, vagotonia decreases,sinus rhythm quickens, and A.V. conduc-tion time is shortened.
Second degree P.A.V.B. in horses hasbeen attributed to increased vagal tonebecause it could be eliminated by a smalldose of atropine (22). Norr (23) wasable to induce P.A.V.B. by twitching themuzzles of horses showing tendencies to-ward block. He considered that vagotoniawas increased by afferent impulses comingfrom the compressed upper lip. A similareffect has been produced by exerting pres-sure on the carotid sinus (20). Partialheart block has been induced using pos-terior pituitary extracts (25). It wasassumed that this was caused by anincreased vagotonia resulting from anelevated blood pressure, although Brooij-mans (3) suggested that the subsequentconstriction of coronary arteries resultingin myocardial ischemia was responsible.Heart block may be caused by the vagaleffect of excessive doses of digitalis (11).
Degenerative and inflammatory changesin the A.V. node and bundle of His mayaccompany certain infectious diseases ofthe respiratory tract which have been con-sidered to be among the most importantcausative factors of equine heart block(3, 28, 34).
MATERIALS AND METHODS
The cases reported herein were basedon observations of 646 horses from three
main sources: (a) Cases referred to theVeterinary School1 by veterinary surgeonsin general practice. One hundred and fiftyhorses were examined by auscultation,pulse palpation and electrocardiography.(b) Four hundred and twenty-nine Armyhorses, nine of which had also competedin Three Day Event Trials. (c) Fifty-fourhorses which were competing in ThreeDay Events. Thirteen other horses wereexamined at the Trials but were notentered in competition.The Army and Three Day Event horses
formed the basis of a routine, primarilyelectrocardiographic survey on apparentlyhealthy horses at rest. Approximately 25%of these horses were examined by ausculta-tion. Many of the horses were examinedon more than one occasion.
OBSERVATIONS
IncidenceNo cases of third degree or complete
heart block were observed. The incidenceof first and second degree P.A.V.B. isillustrated in Table I. Paired missed beatsas well as single missed beats occurred inthree cases. One of the 37 cases of firstdegree P.A.V.B. had a murmur and pre-mature atrial systoles, and one demon-strated premature ventricular systoles anda wandering atrial pacemaker. Four ofthe 94 cases of second degree P.A.V.B.had murmurs, three had murmurs andwandering atrial pacemakers, and 30 hadother electrocardiographic irregularitiesdue to wandering atrial pacemakers, sinusarrhythmia, sinoatrial block or prematureventricular systoles.
Nineteen horses were examined twiceby electrocardiography at an intervalof from three months to two years (TableII). Eleven other horses examined initiallyby electrocardiography were auscultatedone year later. Of this number, fivedemonstrating no previous evidence ofheart block and four demonstrating firstdegree block at the initial examination, hadmissed beats. Two of these horses also hadelectrocardiographic evidence of firstdegree block at the second examination.Two other horses which had first degreeblock initially had no missed beats onauscultation one year later. It is probable
1University of Bristol, Bristol, England.281
CANADIAN VETERINARY JOURNAL
TABLE IPARTIAL ATRIOVENTRICULAR BLOCK IN HORSES
Survey Horses
Othersexamined at Cases seen at
Army Three day three day veterinaryhorses event horses event trials school Total
Numbers of horses 420 63 13 150 646*First degree P.A.V.B. only 24 4 1 8 37Second degree P.A.V.B.t 40 12 4 28 84Second degree P.A.V.B.
diagnosed on auscultation only 10 10
*No E.C.G. abnormality detected in 377. Thus 147 horses showed other electrocardiographicirregularities.
tlncludes some horses which showed first degree block on previous examinations.
TABLE IIRESULTS OF REPEAT EXAMINATIONS IN EQUINE HEART BLOCK
First examination Second examination*
No. Normal lst degree 2nd degree
No heart block 11 111st degree block 5 4 12nd degree block 3 2 1
*Two years after first examination, except one case at 3 monthsand one at 1 year.
that they still had first degree block butthis could only be determined by electro-cardiography.
Clinical RecognitionFrequently, a long first heart sound
(luub) or a split first heart sound (lu lub)was observed on auscultation in horseshaving a slow heart rate at rest. An E.C.G.was necessary to confirm the presence offirst degree P.A.V.B.
Second degree P.A.V.B. was character-ized on auscultation by missed beats whichoccurred regularly or irregularly at restingheart rates. In approximately 80% of cases,the atrial contraction sound (lu) couldbe heard in the pause of a missed beat.This differentiated the condition from sino-atrial block in which this sound is absent.
ELECTROCARDIOGRAPHIC CHANGES
The P-Q IntervalThe P-Q interval is an important
measurement because it is an index ofA.V. conduction time. There is a closerelationship between the heart rate andthe P-Q interval and measurements ofinterval without reference to the relevantheart rate are of little value. A formula
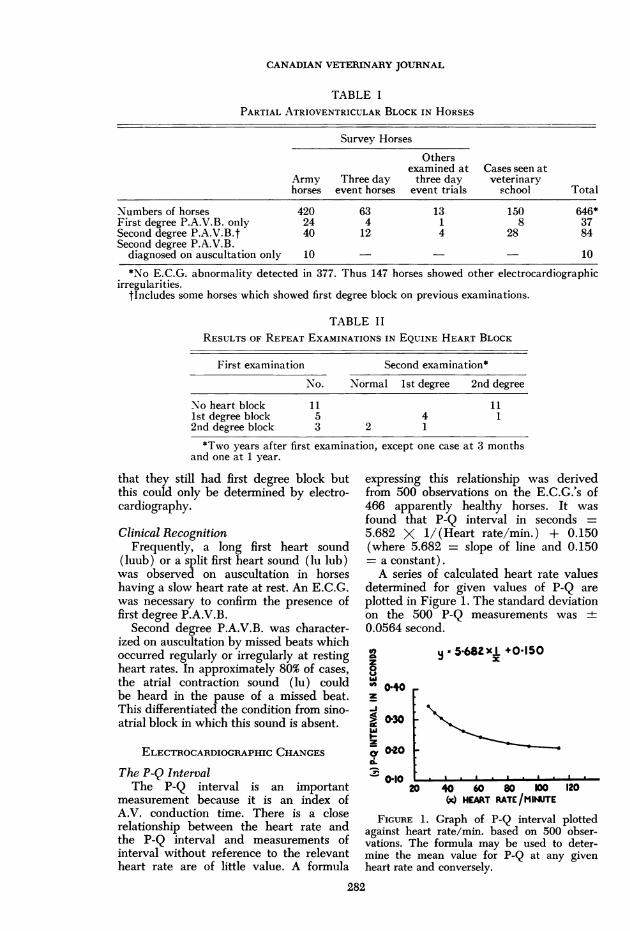
expressing this relationship was derivedfrom 500 observations on the E.C.G.'s of466 apparently healthy horses. It wasfound that P-Q interval in seconds =5.682 X 1/(Heart rate/min.) + 0.150(where 5.682 = slope of line and 0.150- a constant).A series of calculated heart rate values
determined for given values of P-Q areplotted in Figure 1. The standard deviationon the 500 P-Q measurements was ±0.0564 second.
z80 Ot"' 0.40z
-i> 0'30.--a 0-20
010
y5.682xl +0.150x
..
..I
.I ..
20 40 60 s0 100 120(x) HEART RATE/MINUTE
FIGURE 1. Graph of P-Q interval plottedagainst heart rate/min. based on 500 obser-vations. The formula may be used to deter-mine the mean value for P-Q at any givenheart rate and conversely.
282
HEART BLOCK IN HORSES
P-Q Interval in First Degree BlockA P-Q interval, when calculated on the
above formula in excess of 1.5 standarddeviations from the mean in the absenceof missed beats, was regarded as indica-tive of first degree block. On this basis,any horse with a P-Q in excess of 0.425second at a heart rate above 30 per minutecould be included.
In this series, 28 of the 37 cases ob-served had a P-Q interval above 0.40 sec.The remaining nine cases were deducedfrom the formula. Eight of these hadrelatively high heart rates at the time ofexamination. All the cases of first degreeblock demonstrated "floating P-Q inter-vals".P-Q Interval in Second Degree Block
Missed beats occurred at heart ratesbetween 26.5 and 45.5 per minute at rest.They occurred in 68 cases at heart ratesbetween 30 and 40 per minute, of which38 were between 35 and 40 per minute.The frequency of missed beats was ex-tremely variable and no cases demonstrateda constant rhythm maintained for a longperiod.The 84 cases of second degree P.A.V.B.
were mainly Wenckebach type I incharacter; no pure cases of type II blockwere recorded.Classification of Second Degree P.A.V.B.Wenckebach Type I
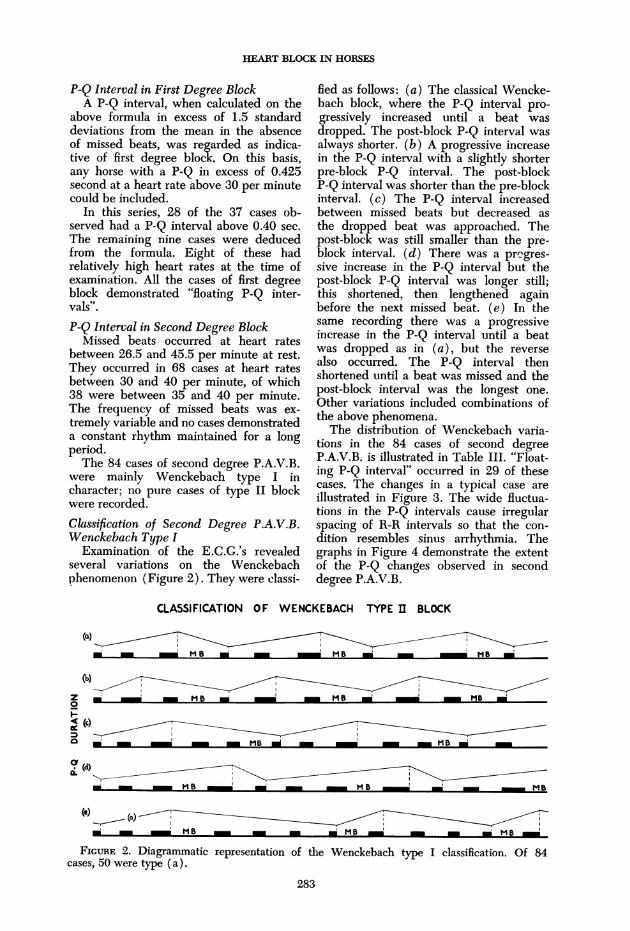
Examination of the E.C.G.'s revealedseveral variations on the Wenckebachphenomenon (Figure 2). They were classi-
fled as follows: (a) The classical Wencke-bach block, where the P-Q interval pro-gressively increased until a beat wasdropped. The post-block P-Q interval wasalways shorter. (b) A progressive increasein the P-Q interval with a slightly shorterpre-block P-Q interval. The post-blockP-Q interval was shorter than the pre-blockinterval. (c) The P-Q interval increasedbetween missed beats but decreased asthe dropped beat was approached. Thepost-block was still smaller than the pre-block interval. (d) There was a prmgres-sive increase in the P-Q interval but thepost-block P-Q interval was longer still;this shortened, then lengthened againbefore the next missed beat. (e) In thesame recording there was a progressiveincrease in the P-Q interval until a beatwas dropped as in (a), but the reversealso occurred. The P-Q interval thenshortened until a beat was missed and thepost-block interval was the longest one.Other variations included combinations ofthe above phenomena.The distribution of Wenckebach varia-
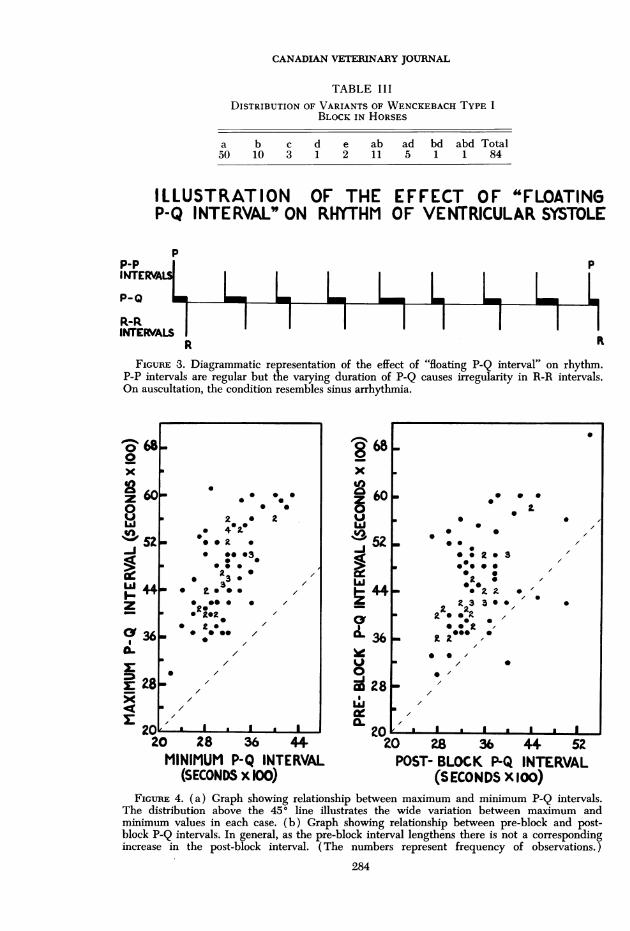
tions in the 84 cases of second degreeP.A.V.B. is illustrated in Table III. "Float-ing P-Q interval" occurred in 29 of thesecases. The changes in a typical case areillustrated in Figure 3. The wide fluctua-tions in the P-Q intervals cause irregularspacing of R-R intervals so that the con-dition resembles sinus arrhythmia. Thegraphs in Figure 4 demonstrate the extentof the P-Q changes observed in seconddegree P.A.V.B.
CLASSIFICATION OF WENCKEBACH TYPE I BLOCK
Z - - MB _- M ~ - M
0
(b)
-, _MB ___ MsB __ MB
FIGURE 2. Diagrammatic representation of the Wenckebach type I classification. Of 84cases, 50 were type (a).
283
CANADIAN VETERINARY JOURNAL
TABLE IIIDISTRIBUTION OF VARIANTS OF WENCKEBACH TYPE I
BLOCK IN HORSES
a b c d e ab ad bd abd Total50 10 3 1 2 11 5 1 1 84
ILLUSTRATION OF THE EFFECT OF "FLOATINGP-Q INTERVAL" ON RHYTHM OF VENTRICULAR SYSTOLE
pp pINTERVA
P _
R-RINTEFVALS I IH
L LLI I I
p
RFIGURE 3. Diagrammatic representation of the effect of "floating P-Q interval" on rhythm.
P-P intervals are regular but the varying duration of P-Q causes irregularity in R-R intervals.On auscultation, the condition resembles sinus arrhythmia.
0 680
z0xa 6
z
0aU 3-J
z
Cyr36
r 28
268x
Z 60z0UWa5Z-J
A4-4
VOr0co 28Lii
20 28 36 44.MINIMUM P-Q INTERVAL
(SECONDS x 100)
0 28 36 44 52POST- BLOCK P-Q INTERVAL
(SECONDS X 100)FIGURE 4. (a) Graph showing relationship between maximum and minimum P-Q intervals.
The distribution above the 450 line illustrates the wide variation between maximum andminimum values in each case. (b) Graph showing relationship between pre-block and post-block P-Q intervals. In general, as the pre-block interval lengthens there is not a correspondingincrease in the post-block interval. (The numbers represent frequency of observations.)
284
0- 0 0 0
00 0
2 * 2* 420. a
* 0*
0 00032 *
* 30- 0 2a3*
@00 0 0
2 0* 20*
* 0 s /
///* /
/
* I . I
HEART BLOCK IN HORSES
The P WaveThere was no apparent difference be-
tween the duration of the normal andblocked P waves. Thirty-nine recordsdemonstrated constant P wave durationsranging from 0.08-0.20 second. In theremaining cases the duration was variableto within about 0.02 second in the samerecord. It was merely chance that some ofthe longest P-Q intervals included a longP wave duration.
Sometimes an increased P-Q intervalwas partially influenced by a change inthe P wave form, especially where an
erect P wave changed abruptly to a dipha-sic form.
The Ta WaveThe Ta wave represents repolarization
of the atria. It is usually superimposed on
the final portion of the QRS complex andthe S-T segment. This wave is fully re-
vealed in cases of P.A.V.B. The Ta wavewas observed in 60 of the 84 cases ofsecond degree block. In the majority ofcases it was inscribed in an opposite direc-tion to the P wave.
The P-P IntervalIn 55 of the 84 cases of second degree
P.A.V.B. the blocked P-P intervals werepredominantly the longest, but in 10 ofthese the pre-block P-P intervals were
sometimes of the same length as the blockP-P interval. The duration of the P-Pinterval decreased in the immediate post-
block cycles before gradually increasingto reach a maximum either just before,or during, a blocked beat. There was,therefore, some sinus arrhythmia.
Variation also occurred, sometimes inthe same record between pre-block andblocked P-P intervals.
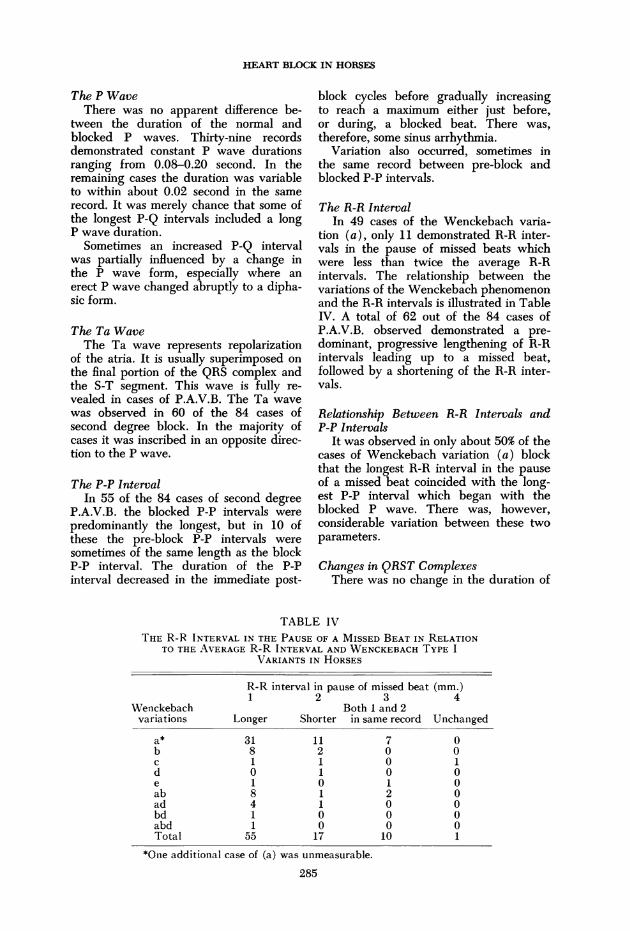
The R-R IntervalIn 49 cases of the Wenckebach varia-
tion (a), only 11 demonstrated R-R inter-vals in the pause of missed beats whichwere less than twice the average R-Rintervals. The relationship between thevariations of the Wenckebach phenomenonand the R-R intervals is illustrated in TableIV. A total of 62 out of the 84 cases ofP.A.V.B. observed demonstrated a pre-dominant, progressive lengthening of R-Rintervals leading up to a missed beat,followed by a shortening of the R-R inter-vals.
Relationship Between R-R Intervals andP-P Intervals
It was observed in only about 50% of thecases of Wenckebach variation (a) blockthat the longest R-R interval in the pauseof a missed beat coincided with the long-est P-P interval which began with theblocked P wave. There was, however,considerable variation between these twoparameters.
Changes in QRST ComplexesThere was no change in the duration of
TABLE IVTHE R-R INTERVAL IN THE PAUSE OF A MISSED BEAT IN RELATION
TO THE AVERAGE R-R INTERVAL AND WENCKEBACH TYPE IVARIANTS IN HORSES
R-R interval in pause of missed beat (mm.)1 2 3 4
Wenckebach Both I and 2variations Longer Shorter in same record Unchanged
a* 31 11 7 0b 8 2 0 0c 1 1 0 1d 0 1 0 0e 1 0 1 0ab 8 1 2 0ad 4 1 0 0bd 1 0 0 0abd 1 0 0 0Total 55 17 10 1
*One additional case of (a) was unmeasurable.
285
CANADIAN VETERINARY JOURNAL
the QRS complexes. Changes in the vol-tages of QRS and T deflections in cyclesassociated with missed beats were ob-served in the first post-block beat, thesecond post-block beat, and in a morecomplex form in cycles between missedbeats in 20 cases.
The Q-T IntervalIn nearly all the cases of second degree
P.A.V.B. the Q-T interval in the post-blockbeat was shorter than in the beats pre-ceding a missed beat. This shorter intervalcould sometimes be related to a change ofT wave configuration but was most fre-quently due to an earlier than usual timeof onset of the post-block T wave. Thepost-block T wave duration was usuallyunchanged when compared with pre-blockvalues.
Effect of Exercise in Horses withP.A.V.B. at Rest
Five of the 27 cases of first degreeP.A.V.B. were examined after exercise.Twenty-five cases of second degreeP.A.V.B. were examined after exercise(21 by electrocardiography). Only twohorses demonstrated missed beats on aus-cultation immediately after light exerciseat heart rates two to three times greaterthan their resting rates. These, however,disappeared after more strenuous exer-cise. Twelve horses did not have missedbeats after exercise and they did notoccur during the subsequent period ofobservation. The missed beats also dis-appeared in 10 other horses and did notreappear until the heart rate had slowedto within 10 beats of the resting rate.
In one case, at a heart rate of 91 perminute after exercise, apparent missedbeats were recorded. The condition wasdue to premature atrial systoles and aber-rant ventricular conduction.
Effect of Exercise on the P-Q IntervalTwenty-one horses were observed in
order to determine whether an accelera-tion of heart rate due to exercise wouldaffect the P-Q interval, and whether itwould cause the interval to reach acceptednormal values at a high heart rate eventhough the interval was unduly long atrest. It was considered that the responsemight also have prognostic significance.
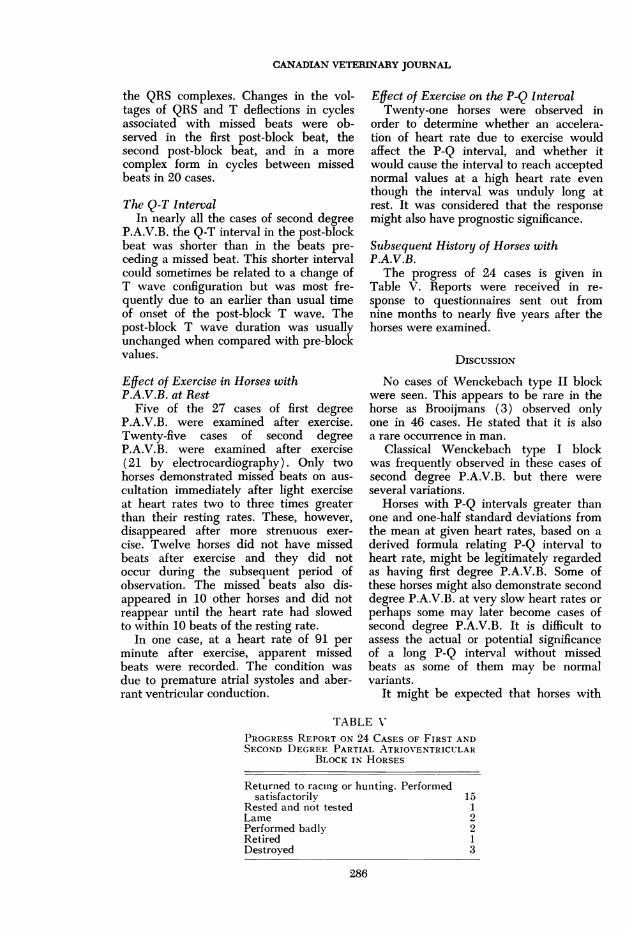
Subsequent History of Horses withP.A.V.B.The progress of 24 cases is given in
Table V. Reports were received in re-sponse to questionnaires sent out fromnine months to nearly five years after thehorses were examined.
DIsCUSSION
No cases of Wenckebach type II blockwere seen. This appears to be rare in thehorse as Brooijmans (3) observed onlyone in 46 cases. He stated that it is alsoa rare occurrence in man.
Classical Wenckebach type I blockwas frequently observed in these cases ofsecond degree P.A.V.B. but there wereseveral variations.
Horses with P-Q intervals greater thanone and one-half standard deviations fromthe mean at given heart rates, based on aderived formula relating P-Q interval toheart rate, might be legitimately regardedas having first degree P.A.V.B. Some ofthese horses might also demonstrate seconddegree P.A.V.B. at very slow heart rates orperhaps some may later become cases ofsecond degree P.A.V.B. It is difficult toassess the actual or potential significanceof a long P-Q interval without missedbeats as some of them may be normalvariants.
It might be expected that horses with
TABLE V
PROGRESS REPORT ON 24 CASES OF FIRST ANDSECOND DEGREE PARTIAL ATRIOVENTRICULAR
BLOCK IN HORSES
Returned to racing or hunting. Performedsatisfactorily
Rested and not testedLamePerformed badlyRetiredDestroyed
1512213
286

HEART BLOCK IN HORSES
second degree P.A.V.B. would demon-strate electrocardiographic evidence offirst degree P.A.V.B. during periods whenno missed beats occurred and heart ratewas slow. This has been observed inmany cases (22). It was not always seen,however, and seven of the 84 cases ofsecond degree P.A.V.B. had P-Q intervalsnot exceeding the normal limits for givenheart rates. This was calculated from theformula, either before a missed beat orduring long periods when there were nomissed beats. Therefore, although a stan-dard and range for P-Q intervals in relationto heart rate may be set, some cases ofheart block will occur occasionally with-out any deviation in P-Q interval from thenormal at any time. It has been observedthat in P.A.V.B. the P-Q interval variedfrom 0.25 to 0.55 sec. (21).Lannek and Rutqvist (16) have re-
ported that the upper normal limit of theP-Q interval in draught horses is 0.409second but the authors' observationsindicate that it is not essential for the atrio-ventricular conduction time to be pro-longed above 0.40 second before a missedbeat occurs. A P-Q interval of 0.425second is probably normal at a heart rateof 30 per minute but abnormal at 40 perminute. At this heart rate an interval of0.386 second is the maximum within thenormal range.
P.A.V.B. was observed in horses ofwidely differing ages (3 to 21 years) butunless their progress had been followedfor several years there would be no wayof determining how long the conditionhad been present. The resting heart rateappears to be an important factor indetermining the appearance of missedbeats. Missed beats occurred most fre-quently at heart rates below 40 per minuteat rest. Some horses giving no electro-cardiographic evidence of either first orsecond degree P.A.V.B. on first examina-tion did so when examined about twoyears later. An inspection of their recordsdemonstrated that in most cases the heartrate had been higher on first examinationthan at the second examination. It istherefore possible that the horses mighthave had block on first examination if theheart rate had been slower.
Following light exercise, missed beatswere detected on auscultation in only twocases. They were not confirmed electro-
cardiographically and disappeared aftermore strenuous work. Every missed beat isnot necessarily due to P.A.V.B. Non-con-ducted premature atrial systoles andpremature ventricular systoles with com-pensatory pauses may resemble the missedbeats of second degree P.A.V.B. on auscul-tation. It was observed that only a slightelevation in heart rate due to excitementwas generally necessary to abolish missedbeats. Occasionally horses which werevery relaxed and unresponsive to theirsurroundings were encountered and theseoften demonstrated regular intermittenciesof cardiac rhythm. In horses with irregu-lar missed beats it was apparent that whenthey were quiet and almost asleep, a regu-lar intermittence often became established.It is believed that no prognostic signifi-cance can be attached to the rhythmicityof missed beats in the horse.
"Floating P-Q interval" was observed inboth first and second degree P.A.V.B.(3). This phenomenon could possibly beassociated with the mechanism of sinusarrhythmia because Katz (14) consideredthat apart from variations in vagal toneaffecting the rhythmicity of the sinus pace-maker, sinus arrhythmia may also becaused by a wandering of the pacemakerwithin the sinus node.
In man, the direction of the Ta waveis normally opposite to that of the P wavein the extremity E.C.G.'s (10). This hasalso been observed in the horse.
It has been reported that the P-P inter-vals, beginning with block P waves, wereusually the longest (3, 29, 30). Theseobservations agree with those of Katz(14) regarding classical Wenckebach typeof P.A.V.B., in that after the pause of amissed beat the ventricles show an accele-ration for a few beats and then slow as thenext missed beat is approached. Katzstated that the fact that the P-Q intervalfollowing a pause is less than that beforethe pause makes the R-R interval of thepause less than twice the average R-Rinterval. In spite of post-block P-Qshortening, however, the R-R intervalin the pause of a missed beat was usuallylonger than twice the average R-R interval.The longest R-R and P-P intervals did notalways coincide with the pause of amissed beat. In nearly every case the R-Rintervals preceding a missed beat showeda progressive lengthening and then a
287
CANADIAN VETERINARY JOURNAL
shortening after the missed beat causing asinus arrhythmia (29, 30).A few cases demonstrated QRS and T
voltage changes associated with missedbeats. They usually occurred in post-blockcycles. These changes in the QRS complexmay result either from a changing relationbetween the QRS and Ta waves, or fromconduction disturbances in the ventricles(3).There was usually a shortening of the
Q-T interval and changes in the form ofT wave in the cycle immediately followinga blocked beat. Lanek (15) regarded thisshortening as due to a heightened sympa-thetic tone since he found that he couldevoke similar T wave changes by injectingadrenaline intravenously.
In most cases there was an earlier thanusual time of onset of the post-block Twave without change in T wave duration.This suggests that in post-block beatsthe length of the period of ventriculardepolarization was shortened but thatventricular repolarization was probably un-altered. Similar changes in the form of theT waves after exercise or adrenaline in-jections have been reported (26).
In the observations reported in thispaper, 17.9% of 496 apparently healthyhorses demonstrated varying degrees ofP.A.V.B. (4.2% first degree block and 12.9%second degree block). If the 150 horsesexamined at the Veterinary School (whichis probably a biased sample) are also in-cluded, a total of 18.9% cases of first andsecond degree block were observed in 646horses.
There is a wide diversity of opinion re-garding the clinical significance of P.A.V.B.in horses. It has been considered that thecondition is functional, resulting from theaction of the vagal nerves at rest (5,22, 30). Other workers considered thatP.A.V.B. signified disease of the specificconducting tissue or the myocardium (3,12, 31). Evidence to this effect in indi-vidual horses has been presented (2, 6)and Corticelli (4) observed second degreeP.A.V.B. in a horse which subsequentlydeveloped atrial fibrillation.
Workers have always agreed that the ap-pearance of missed beats after exercisejustifies a grave prognosis but very fewhorses with P.A.V.B. at rest had missedbeats at high heart rates. The question thenarises whether all cases of P.A.V.B. in the
horse are consistent with normality (physio-logical) and if this is not so whatmethod can be used to differentiate physio-logical from pathological cases in orderto arrive at a rational prognosis. In somehorses P-Q intervals may become normal athigh heart rates whereas in others theyremain abnormally long. The subsequenthistory of animals falling into these twocategories, however, does not suggest thatthose with long P-Q intervals at high heartrates are any less able to continue workingnormally. At least five out of eight horseswith prolonged P-Q intervals after exercisereturned to hunting or racing and workedwell. There is little evidence that any af-fected horses were discarded as a directresult of cardiac dysfunction caused byP.A.V.B., and reasons for disposal includ-ing lameness, unthriftiness or poor per-formance were no more significant thanfor any group of horses.
In the horse, the missing of an occasionalventricular systole might be a way ofconserving cardiac energy but if it becomesvery frequent over long periods theremight be effects on circulatory efficiencysuch as the development of compensatorydilatation and valvular changes.
In this study of 68 cases of P.A.V.B.,12% had murmurs and 38% demonstratedelectrocardiographic irregularities, of whichat least 50% had wandering pacemakerswith no arrhythmia on auscultation. Theremight not have been any association be-tween heart block and these other ab-normalities in these particular animals.Follow-up observations in cases of blockhave not shown any evidence of a ten-dency toward the development of murmursand all the cases have compensated both atrest and after exercise. Evidence thathorses with P.A.V.B. at rest are capableof completing Three Day Event Trials hasbeen presented previously (13).From the evidence presently available
it would appear that the majority of casesof first and second degree P.A.V.B. ob-served at rest are benign, provided thefollowing criteria are fulfilled. The missedbeats should disappear on exercise or pulseacceleration and not reappear until heartrate approaches former resting levels.Horses should not demonstrate any distresson exercise or visible evidence of circu-latory impairment (edema or jugular pulsa-tion). If there are no murmurs or other
288
HEART BLOCK IN HORSES
causes of arrhythmia (both of which wouldhave to be assessed separately), the pre-sence of missed beats would not warranta grave prognosis although their presencewould have to be reported when examin-ing a horse for soundness or insurance.
SUMMARY
Observations on partial A.V. block inthe horse have been described. The electro-cardiographic changes were analyzed andin second degree P.A.V.B., the Wencke-bach phenomenon type I, was furtherclassified. The effect of exercise on P.A.V.B.was described and the prognostic signifi-cance of the condition has been discussed.
REsuME
On decrit les observations obtenues parsuite du blocage auriculo-ventriculairepartiel chez le cheval. Les changementsobtenus a l'electrocardiogramme furentanalyses et l'effet Wenckebach de type Ifut mieux defini pendant le blocage ausecond degre. On decrit l'effet de l'exercisesur le blocage auriculo-ventriculaire partielet on discute le prognostic de cette con-dition.
ACKNOWLEDGMENTS
The authors would like to thank Lt. Col.P. W. Dean and Capt. C. A. McGilligan ofthe R.A.V.C. for providing facilities and valu-able co-operation and assistance in the ex-amination of army horses; the organizers ofThree Day Event Trials at Badminton, Tid-worth and Burghley for permission to examinethe horses, and to the owners for their co-operation in this investigation. Thanks are alsodue to the many veterinary surgeons in prac-tice in the South West who have referredhorses for examination, and to Mr. A. A. W.Addicott for assistance with the horses duringthis study. The work was made possible bya grant from the Horserace Betting LevyBoard.
REFERENCES
1. BARRY, D. T., and J. A. NICHOLSON. Anunusual case of Heart Block in aThoroughbred gelding. Vet. Rec. 52: 848.1940.
2. BOSNIC, L., and S. RAPIC. Two furthercases of Adams-Stokes syndrome inhorses. Vet. Arhiv. (Zagreb). 11: 166.1941. (Abst. in Vet. Bull. 18: 548. 1948.)
3. BROOIJMANS, A. W. M. Electrocardio-graphy in Horses and Cattle. Laboratoryof Veterinary Physiology, State Uni-versity, Utrecht. 1957.
4. CORTICELLI, B. Fibrillazione e flutteratriali nel cavallo. Arch. vet. ital. 1: 177.1950.
5. DETWEILER, D. K., and D. F. PATTERSON.Diseases of Blood and CardiovascularSystem. In Equine Medicine and Surgery.Chapter 16. Wheaton, Illinois: AmericanVeterinary Publications. 1963.
6. DUKES, H. H. A case of Heart Block ina horse. Cornell Vet. 30: 248. 1940.
7. DUKEs, H. H., and H. T. BATT. Studieson the electrocardiogram of the horse.Amer. J. Physiol. 133: 265. 1941.
8. FoDRoczY, E. ElektrokardiographischeUntersuchungen bei Rhymus - und Reiz-leitungsstorungen beim Pferde. Diss.Budapest. 1938.
9. FRIEDBERG, C. K. Diseases of the Heart.London: Saunders. 1949.
10. FRIEDMAN, H. H. Outline of Electro-cardiography. Toronto: McGraw-Hill.1963.
11. GADDUM, J. H. Pharmacology. 4th Ed.London: Oxford University Press. 1955.
12. GLAZIER, D. B. Electrocardiography inVeterinary Medicine. Irish Vet. J. 12:230. 1958.
13. HOLMES, J. R. Clinical Examination ofthe Equine Heart. Proc. 17th Wld. Vet.Congr., Hanover. 2: 1195. 1963.
14. KATZ, L. N. Electrocardiography. 2ndEd. Philadelphia: Lea and Febiger. 1949.
15. LANNEK, N. The terminal ventricularcomplex of the post-block beat in thehorse's E.C.G. Nord. Vet. Med. 3: 425.1951.
16. LANNEK, N., and L. RuTQVIST. Normalarea of variation for the E.C.G. ofhorses. A statistical examination of ex-tremity leads and unipolar leads. Nord.Vet. Med. 3: 1094. 1951.
17. LEWIS, T. Electrocardiography and Clini-cal Disorders of the Heart Beat. London:Shaw and Sons. 1949.
18. MORETTI, B. Sindrome di Morgagni-Adams-Stokes in un cavallo determintada blocco totale del cuore. Atti. Soc. ital.Sci. vet. 2: 1. 1948.
19. MORETTI, B. Patologia del ritmo cardiacodegli animali domestici. Atti. Soc. ital.Sci. vet. 5: 19. 1951.
20. NEFF, W. Die Beeinfluszung des Herz-rhythmus beim Pferde durch Brems-versuch und Karotis-Sinus Druck. Thesis,Miinchen. 1934.
21. NORR, J. Das sog. Reizleitungssystem imHerzen und seine Beziehungen zu kar-dialen Funktionsstorungen. Munch. tier-arztl. Wschr. 31: 404. 1924.
289
CANADIAN VETERINARY JOURNAL
22. NORR, J. 100 klinische Falle von Herz-und Pulsarrhythmien beim Pferde. Mh.prakt. Tierheilk. 34: 177. 1924.
23. NORR, J. Ueber eine besondere Wirkungdes "Bremsens" auf die Herztatigkeitdes Pferdes durch Vaguszerrung und ihreklinische Bedeuntung. Munch. tierarztl.Wschr. 46: 382. 1930.
24. NoRm, J. Paroxysmale Tachykardie undpartieller Vorhof-Kammerblock bei einemReitpferd mit Aorteninsuffizienz. Arch.Wiss. prakt. Tierheilk. 63: 103. 1931.
25. OBEL, N. Fysiologiska synpunter pa dethabituella Atrioventrikularblocket hoshast. Skand. VetTidskr. 32: 200. 1942.
26. OBEL, N. Studier av hiistens normalaelectrokardiogram med sarskild hansyntill forandringrar i ventrikelkomplexetefter arbete. Skand. VetTidskr. 32: 324.1942.
27. RoTH, I. R., and B. KISCH. The Mecha-nism of Irregular Sinus Rhythm inAuriculoventricular Heart Block. Amer.Heart J. 36: 257. 1948.
28. SCHUEIZLER, G. Beobachtungen am Be-lastungs-Elektrokardiogramm des Pferdes.Arch. wiss. prakt. Tierheilk. 78: 40. 1942.
29. SpORRi, H. Ueber den Atmungsgesteuertenreflektorischen Herzblock des Pferdes.Tierarztl. Umsch. 6: 419. 1951.
30. SP6RRI, H. Ueber die Genese und Kli-nische Bedeuntung des partiellen Herz-
blockes beim Pferd. Schweiz. Arch. Tier-heilk. 94: 337. 1952.
31. STEEL, J. D. Studies on the Electro-cardiogram of the Racehorse. Sydney:Australasian Medical Publishing Co.1963.
32. STEFFAN, H. Das Herz bei innerenErkrankungen des Pferdes. I. Elektro-und phonokardiographische Untersuchun-gen. Arch. wiss. prakt. Tierheilk. 68:159. 1934.
33. STEFFAN, H. Das Herz bei innerenErkrankungen des Pferdes. II. InfektioseAnemie. Elektro- und phonokardio-graphische Untersuchungen. Arch. wiss.prakt. Tierheilk. 68: 328. 1934.
34. STEFFAN, H. Das klinische Bild desansteckenden Katarrhs der Luftwege desPferdes. Z. Veterinark. 53: 71. 1941.
35. VAN ZIJL, W. J. Atrioventriculairegeleidingsstoornissen bij paard, rund enbond. T. Diergeneesk. 77: 536. 1952.
36. WENCKEBACH, K. F., and H. WINTER-BERG. Die unregelmaszige Herztatigkeit.Leipzig: Engelmann. 1927.
37. WESTER, J. Orgaanziekten bij de grooteHuisdieren. Utrecht: Van Boekhoven.1935.
38. WIRTH, D. Adams-Stokes'sche Krank-heit bei zwei Pferden, bedingt durchHerzblock. Wien. tierarztl. Mschr. 14: 1.1927.
ABSTRACTS
Rose, M. A. (1966) Equine influenzaviruses isolated at Cambridge in 1963 and1965.-Proc. R. Soc. Med. 59, 51-52 (Dep.Anim. Pathology, Univ. Cambridge, U.K.).
A/Equi 2/England 65 (serologicallysimilar to A/Equi 2/Miami 63) aggluti-nated r.b.c. of fowl, g. pig, human 0,pigeon, pig, horse, cow, turkey and sheep.H.I. tests of this virus and of A/Equi1/Cambridge 63 (serologically identical toA/Equi 1/Prague 56) revealed that thesub-types of V antigen of the two viruseswere distinct. Sera collected during the1963 outbreak and between 1948 and1962 were all negative for A/Equi 2/Miami 63, but some of the sera collectedduring the 1965 outbreak showed anincrease in titre for A/Equi I/Camb. 63.
Reprinted from "The Veterinary Bulletin",Vol. 36, No. 6, June, 1966.
Morter, R. L., Herschler, R. C., Fessler,J. F., and Lavignette, A. (1965). Experi-mental equine leptospirosis (Leptospirapomona). Proc. 68th Ann. Meet. U.S.Livestock Sanit. Ass., Memphis, Tennessee(1964) pp. 147-152 (School Vet. Sci.Med., Purdue Univ., Lafayette, Indiana).
Nine ponies injected s/c with bloodfrom infected g. pigs became infectedwith L. pomona. Leptospires were re-covered from the blood and urine but notfrom the aqueous humour. Agglutinationtitres were detected by the ninth day afterinfection and persisted for the 56-weekperiod of observation. Ocular lesions,typical of recurrent uveitis developed inall infected ponies. Controls remainedapparently normal.
Reprinted from "The Veterinary Bulletin",Vol. 36, No. 2, February, 1966.
290










![Clinics in Surgery Case Report · Atrio-ventricular rupture is usually witnessed following mitral . replacement in the presence of a heavily calcified annulus [1,2] although it may](https://img.pdfslide.net/doc/110x75/5f27ee2933003732b85069be/clinics-in-surgery-case-atrio-ventricular-rupture-is-usually-witnessed-following.jpg)


















