Embed Size (px)
Citation preview

Postgraduate Medical Journal (January 1970) 46, 32-39.
Obstetric radiology
J. H. HIGHMANM.R.C.P., F.F.R.
Consultant Radiologist, St Mary's Hospital, London, W.2
SummaryThe uses of radiology in obstetrics are described.The dangers to the foetus are described. It is con-cluded that with care these can be reduced and thebenefits from its use may often outweigh the dangers.The indications for pelvimetry, the technique and
its interpretation are discussed.Placentography and the use of ra iology in deter-
mining maturity are also described.
IntroductionRadiology contributes to obstetrics in resolving
problems related to pelvimetry and disproportion, tothe site of the placenta and to foetal age and foetalabnormality including the diagnosis of foetal death.Over the whole subject looms the problem ofradiation hazard.
Radiation hazardThe problem of radiation hazard may involve both
mother and foetus and theoretically could encompasssomatic and genetic effects to each. For practicalpurposes it is the potential hazard to the unbornfoetus of radiation-induced malignancy that hasover the last few years caused such considerableheart searching and disputation. It is necessary todiscuss this problem since one's whole approach toobstetric radiology will be determined by thestrength of the 'case against radiology'.
Discussion resolves itself into three main prob-lems:
(1) Does a hazard exist?(2) What is the degree of the hazard?(3) Is the hazard excessive?
(1) Does a hazard exist?The first real statement regarding the hazard to
the foetus from diagnostic radiology was in the paperby Alice Stewart and her colleagues published in theLancet (Stewart et al., 1956) in which she traced 547cases of malignant disease (roughly equal numbersof leukaemia and other neoplastic conditionsincluding those of CNS, kidneys and adrenals)occurring in children under the age of 10 years duringthe years 1953-55. On comparing these with the
controls it was found that there had been radiationto the maternal abdomen in eighty-five cases com-pared with forty-five in the control group. A further,more detailed report in 1958 (Stewart, Webb &Hewitt, 1958) confirmed an excess of child malig-nant disease apparently in relation to antenatalradiation, but also pointed out that other factorswere also present in excess in the malignant groupcompared with the controls-notably, maternal virusinfection, threatened abortion and excessive maternalage, while post-natally, pulmonary infections andsevere injuries were in excess.
Thus, a prima facie case has been made outalthough another report by Court Brown, Doll &Hill (1960) failed to confirm these figures and furtherit may be argued that the other factors associatedwith childhood malignancy had not been properlytaken into account.
(2) What is the degree ofhazard?The figures for this may best be taken from
Stewart & Kneale (1968) and Stewart et al. (1958)since they present the case against radiology.The total incidence of malignancy up to the tenth
birthday is one in 1200 live births.Abdominal radiation roughly doubles the hazard
to the foetus.Less than one in a thousand antenatal X-ray
examinations may be said to lead to death frommalignant disease before 10 years of age.Abdominal X-rays may account for about 6% of
all malignant deaths occurring before the age of10 years.
(3) Is the hazard excessive?The maximum estimated degree of risk has been
presented. Against this must be considered thehazards of prematurity, postmaturity, unsuspectedmalpresentation, placenta praevia, etc., in whichantenatal radiography may play a useful part in casemanagement. Whereas it is possible, though asindicated very difficult, to estimate the hazard it isfar more difficult to quantitate the beneficial effectsof radiology since it is so intricately a part of thewhole process of management. When one considersthat perinatal mortality is twenty-five per 1000, and
r
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
Obstetric radiology
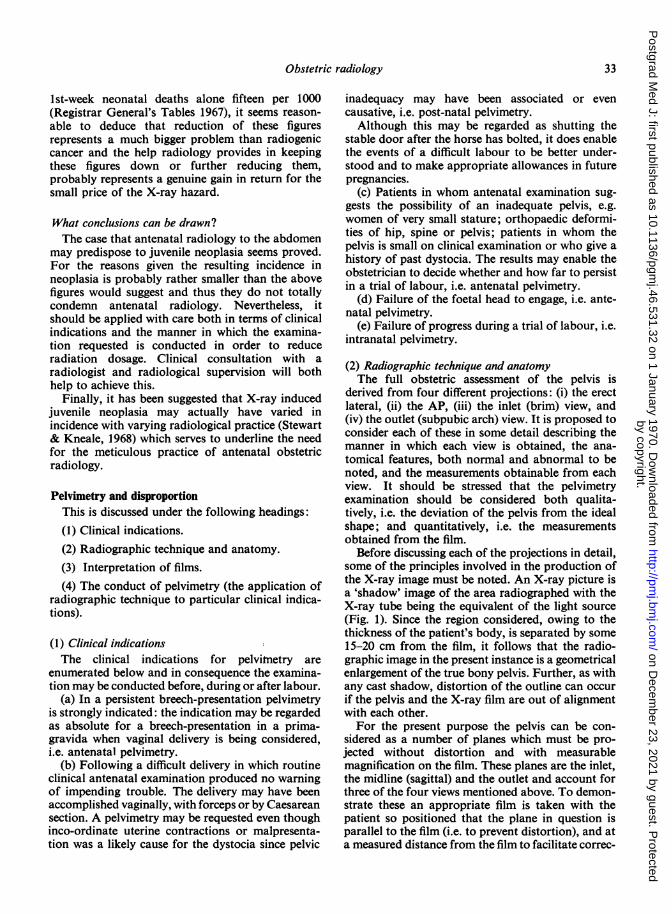
Ist-week neonatal deaths alone fifteen per 1000(Registrar General's Tables 1967), it seems reason-able to deduce that reduction of these figuresrepresents a much bigger problem than radiogeniccancer and the help radiology provides in keepingthese figures down or further reducing them,probably represents a genuine gain in return for thesmall price of the X-ray hazard.
What conclusions can be drawn?The case that antenatal radiology to the abdomen
may predispose to juvenile neoplasia seems proved.For the reasons given the resulting incidence inneoplasia is probably rather smaller than the abovefigures would suggest and thus they do not totallycondemn antenatal radiology. Nevertheless, itshould be applied with care both in terms of clinicalindications and the manner in which the examina-tion requested is conducted in order to reduceradiation dosage. Clinical consultation with aradiologist and radiological supervision will bothhelp to achieve this.
Finally, it has been suggested that X-ray inducedjuvenile neoplasia may actually have varied inincidence with varying radiological practice (Stewart& Kneale, 1968) which serves to underline the needfor the meticulous practice of antenatal obstetricradiology.
Pelvimetry and disproportionThis is discussed under the following headings:(1) Clinical indications.
(2) Radiographic technique and anatomy.(3) Interpretation of films.
(4) The conduct of pelvimetry (the application ofradiographic technique to particular clinical indica-tions).
(1) Clinical indicationsThe clinical indications for pelvimetry are
enumerated below and in consequence the examina-tion may be conducted before, during or after labour.
(a) In a persistent breech-presentation pelvimetryis strongly indicated: the indication may be regardedas absolute for a breech-presentation in a prima-gravida when vaginal delivery is being considered,i.e. antenatal pelvimetry.
(b) Following a difficult delivery in which routineclinical antenatal examination produced no warningof impending trouble. The delivery may have beenaccomplished vaginally, with forceps or by Caesareansection. A pelvimetry may be requested even thoughinco-ordinate uterine contractions or malpresenta-tion was a likely cause for the dystocia since pelvic
inadequacy may have been associated or evencausative, i.e. post-natal pelvimetry.
Although this may be regarded as shutting thestable door after the horse has bolted, it does enablethe events of a difficult labour to be better under-stood and to make appropriate allowances in futurepregnancies.
(c) Patients in whom antenatal examination sug-gests the possibility of an inadequate pelvis, e.g.women of very small stature; orthopaedic deformi-ties of hip, spine or pelvis; patients in whom thepelvis is small on clinical examination or who give ahistory of past dystocia. The results may enable theobstetrician to decide whether and how far to persistin a trial of labour, i.e. antenatal pelvimetry.
(d) Failure of the foetal head to engage, i.e. ante-natal pelvimetry.
(e) Failure of progress during a trial of labour, i.e.intranatal pelvimetry.
(2) Radiographic technique and anatomyThe full obstetric assessment of the pelvis is
derived from four different projections: (i) the erectlateral, (ii) the AP, (iii) the inlet (brim) view, and(iv) the outlet (subpubic arch) view. It is proposed toconsider each of these in some detail describing themanner in which each view is obtained, the ana-tomical features, both normal and abnormal to benoted, and the measurements obtainable from eachview. It should be stressed that the pelvimetryexamination should be considered both qualita-tively, i.e. the deviation of the pelvis from the idealshape; and quantitatively, i.e. the measurementsobtained from the film.
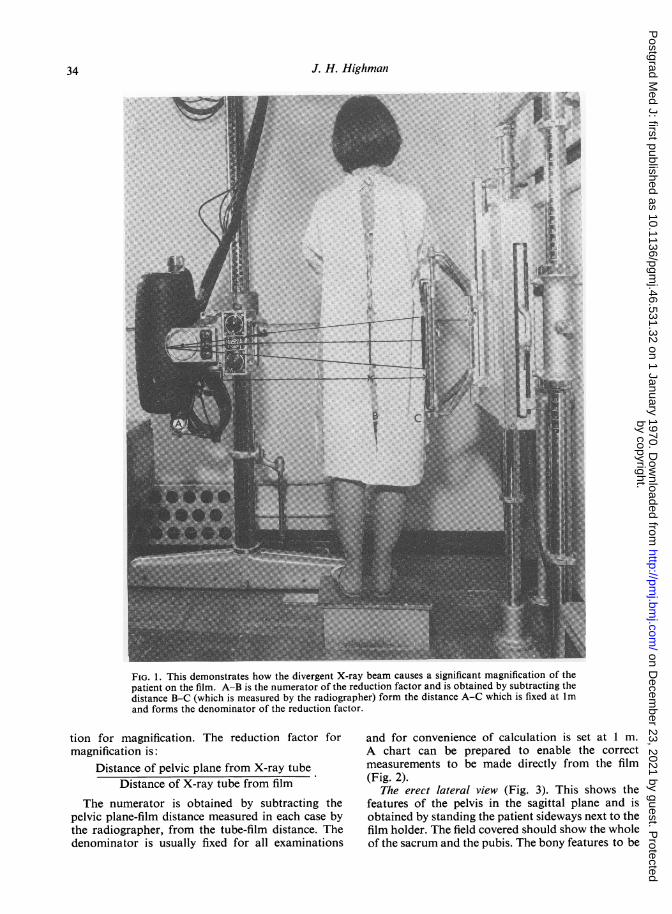
Before discussing each of the projections in detail,some of the principles involved in the production ofthe X-ray image must be noted. An X-ray picture isa 'shadow' image of the area radiographed with theX-ray tube being the equivalent of the light source(Fig. 1). Since the region considered, owing to thethickness of the patient's body, is separated by some15-20 cm from the film, it follows that the radio-graphic image in the present instance is a geometricalenlargement of the true bony pelvis. Further, as withany cast shadow, distortion of the outline can occurif the pelvis and the X-ray film are out of alignmentwith each other.For the present purpose the pelvis can be con-
sidered as a number of planes which must be pro-jected without distortion and with measurablemagnification on the film. These planes are the inlet,the midline (sagittal) and the outlet and account forthree of the four views mentioned above. To demon-strate these an appropriate film is taken with thepatient so positioned that the plane in question isparallel to the film (i.e. to prevent distortion), and ata measured distance from the film to facilitate correc-
33
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
J. H. Highman
FIG. 1. This demonstrates how the divergent X-ray beam causes a significant magnification of thepatient on the film. A-B is the numerator of the reduction factor and is obtained by subtracting thedistance B-C (which is measured by the radiographer) form the distance A-C which is fixed at Imand forms the denominator of the reduction factor.
tion for magnification. The reduction factor formagnification is:
Distance of pelvic plane from X-ray tubeDistance of X-ray tube from film
The numerator is obtained by subtracting thepelvic plane-film distance measured in each case bythe radiographer, from the tube-film distance. Thedenominator is usually fixed for all examinations
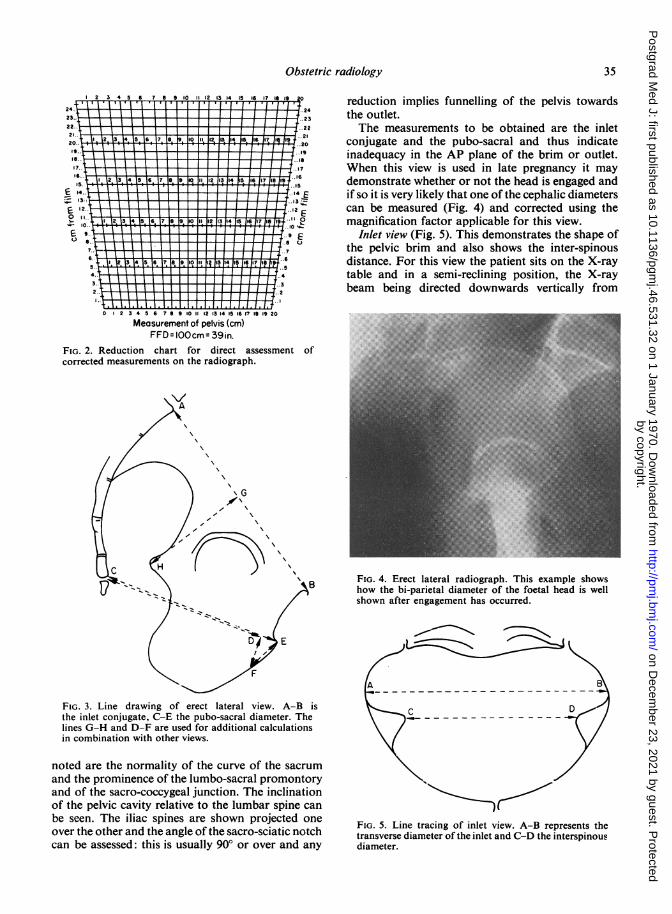
and for convenience of calculation is set at 1 m.A chart can be prepared to enable the correctmeasurements to be made directly from the film(Fig. 2).
The erect lateral view (Fig. 3). This shows thefeatures of the pelvis in the sagittal plane and isobtained by standing the patient sideways next to thefilm holder. The field covered should show the wholeof the sacrum and the pubis. The bony features to be
34
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
Obstetric radiology 35
22 3 4 5 6 7 9 10 11 12 13 14 15 16 17 16 19 0
"23.. .: :: ::: :24:'1'1
.2.. t \ I I I _ I I .2242 1 4I 1 I I I I 1 17 ..20.. 1 14 1 1 pevs20.. F - _ ..21
17.. I I I III",.
.. _..146
" . 12. 13. 14, 15. 16 17_ B e o _ 2 13 14 15 116 117 118 119
1- .. ..14T
12.. ..1
..0...Ei.. ..
+ 10.5 6.r9l 10_ __7.. ... 7~"½~I 3456 76910111 415 I 11665..
,"4 4III ! I I I I i / I~",
2.. -.2
.1 ... l.. ... . l.l.t0 2 3 4 5 6 7 8 9 10 1 12 13 14 15 16 171I 19 20
Measurement of pelvis (cm)FFD = IOOcm:-9qin
FIG. 2. Reduction chart for direct assessment ofcorrected measurements on the radiograph.
/\\
\ \
\F\D\
(^'^E, ,
FIG. 3. Line drawing of erect lateral view. A-B isthe inlet conjugate, C-E the pubo-sacral diameter. Thelines G-H and D-F are used for additional calculationsin combination with other views.
noted are the normality of the curve of the sacrumand the prominence of the lumbo-sacral promontoryand of the sacro-coccygeal junction. The inclinationof the pelvic cavity relative to the lumbar spine canbe seen. The iliac spines are shown projected oneover the other and the angle of the sacro-sciatic notchcan be assessed: this is usually 90° or over and any
reduction implies funnelling of the pelvis towardsthe outlet.The measurements to be obtained are the inlet
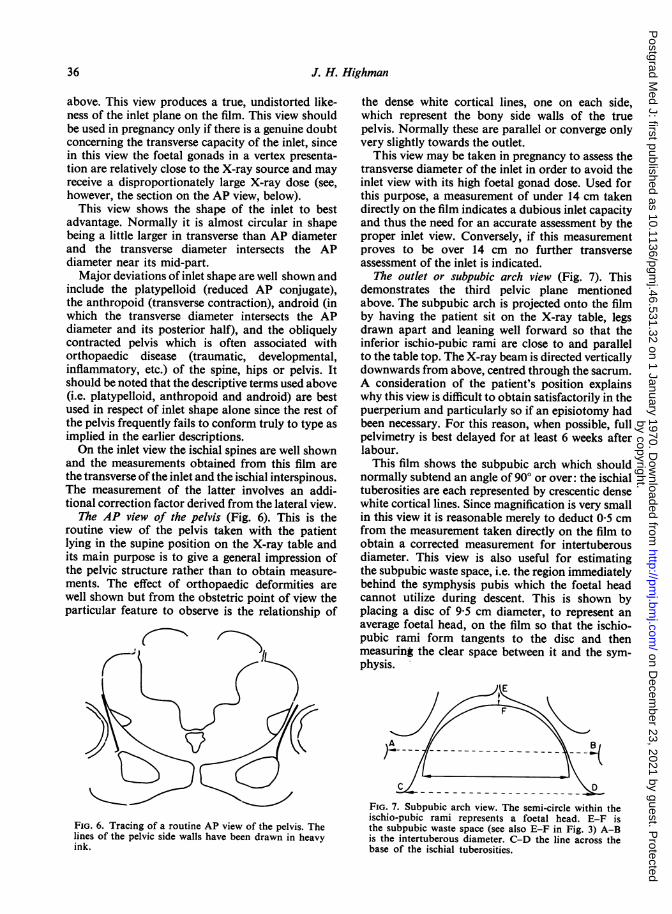
conjugate and the pubo-sacral and thus indicateinadequacy in the AP plane of the brim or outlet.When this view is used in late pregnancy it maydemonstrate whether or not the head is engaged andif so it is very likely that one of the cephalic diameterscan be measured (Fig. 4) and corrected using themagnification factor applicable for this view.
Inlet view (Fig. 5). This demonstrates the shape ofthe pelvic brim and also shows the inter-spinousdistance. For this view the patient sits on the X-raytable and in a semi-reclining position, the X-raybeam being directed downwards vertically from
'.:'::::::··liil···: .*.·.· i:ii': :·:·i ··::·:i:·:·::ldi:;*isI:8iiiiii2i%iilfil
···.::;g.i:iiiiii.ila!i.E.i.;.r mi.:ir;ri: ·'·····i.:.i.:...iCI8i":aiiPIiliii.ii:'gi'n'::'i'51.Z. .i.ss
·:·'li:r::···":lit;iF.!iliitiiSiELiiHiii:l:: .·.:x:l:i·i:I·.. ;j;:j:':i .d'liiiiiji::lii:'l.I :.. .ii. ··:i··iisii"'i.i8!2113.i.lssi i.ii;liillCliidi;:i; zl:i .·. : ·:'-'::':'"'":'::ii··: ··'·l:·PBi:ii:ldl pi:.··;··· ··.::·.:i:i$ii..iZiiiiii8iiSibiii: ::·.·i·.:·: .·:;·.i·liiL;:i::: ::' ::ICili8iZilBli::i:·· ::·::·;:..·:·i:·l'·IB.i .f..II.Z!liZifiiiZ
'i·"'-iWiei:K·l..:i:: i.i.iiljl.ljii:: :i:·::: ::. .:: ··;:·PFiiHiiiiiii!lijiiiijji"i'ii'i'ii'..i' ·:··::i·i··i·:·:· :· ··:·iiii.il%lIi)i:ls··':::':in::.iiiiiiii ·:::j·i· li'ii:.:i:::i'':: .·. :::.:. ·:· .·iillillillii.;.lliii4aisii-;:..;..; .i;:i: i:i·:::;i:·;·:··:·· :.:.::-:...I.II.I ··: ··· ·······:l·lii/::i.:ipi:i:isl:l:::::i:i.:i.i:.:::::::ii .:.·:·.::·:::·swsll.:lsl·i.::.::i:i:iiiiaiiiii:;i.!.i
""":":"i.;..ii%iEit:i:liC:n::1IJiliLfaiiaii#ii"l;i::l;·····:-:;·::-::·::.i:l:d5iiiiii::E::4ib:IL%6Riiiii:'i:iiiillisiiiiiiliiaiiii?iiisiiriifii:ia
·:b'iii'r"fl'·ii:a::·;ii.i.ii.!i.l.....i···;::l::i:::4i#iIHli"::i;·ir:·i ·:··ii;ii.:i8
;:;:::
.·..::n::a::?:I· .·i:l:i8
.,..;..
-::.I.::li6
ii:.ii;ii
I-.
a:r*:s:
Hiii
FIG. 4. Erect lateral radiograph. This example showshow the bi-parietal diameter of the foetal head is wellshown after engagement has occurred.
A 7c D
FIG. 5. Line tracing of inlet view. A-B represents thetransverse diameter of the inlet and C-D the interspinousdiameter.
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
J. H. Highman
above. This view produces a true, undistorted like-ness of the inlet plane on the film. This view shouldbe used in pregnancy only if there is a genuine doubtconcerning the transverse capacity of the inlet, sincein this view the foetal gonads in a vertex presenta-tion are relatively close to the X-ray source and mayreceive a disproportionately large X-ray dose (see,however, the section on the AP view, below).
This view shows the shape of the inlet to bestadvantage. Normally it is almost circular in shapebeing a little larger in transverse than AP diameterand the transverse diameter intersects the APdiameter near its mid-part.Major deviations of inlet shape are well shown and
include the platypelloid (reduced AP conjugate),the anthropoid (transverse contraction), android (inwhich the transverse diameter intersects the APdiameter and its posterior half), and the obliquelycontracted pelvis which is often associated withorthopaedic disease (traumatic, developmental,inflammatory, etc.) of the spine, hips or pelvis. Itshould be noted that the descriptive terms used above(i.e. platypelloid, anthropoid and android) are bestused in respect of inlet shape alone since the rest ofthe pelvis frequently fails to conform truly to type asimplied in the earlier descriptions.On the inlet view the ischial spines are well shown
and the measurements obtained from this film arethe transverse ofthe inlet and the ischial interspinous.The measurement of the latter involves an addi-tional correction factor derived from the lateral view.
The AP view of the pelvis (Fig. 6). This is theroutine view of the pelvis taken with the patientlying in the supine position on the X-ray table andits main purpose is to give a general impression ofthe pelvic structure rather than to obtain measure-ments. The effect of orthopaedic deformities arewell shown but from the obstetric point of view theparticular feature to observe is the relationship of
FIG. 6. Tracing of a routine AP view of the pelvis. Thelines of the pelvic side walls have been drawn in heavyink.
the dense white cortical lines, one on each side,which represent the bony side walls of the truepelvis. Normally these are parallel or converge onlyvery slightly towards the outlet.
This view may be taken in pregnancy to assess thetransverse diameter of the inlet in order to avoid theinlet view with its high foetal gonad dose. Used forthis purpose, a measurement of under 14 cm takendirectly on the film indicates a dubious inlet capacityand thus the need for an accurate assessment by theproper inlet view. Conversely, if this measurementproves to be over 14 cm no further transverseassessment of the inlet is indicated.
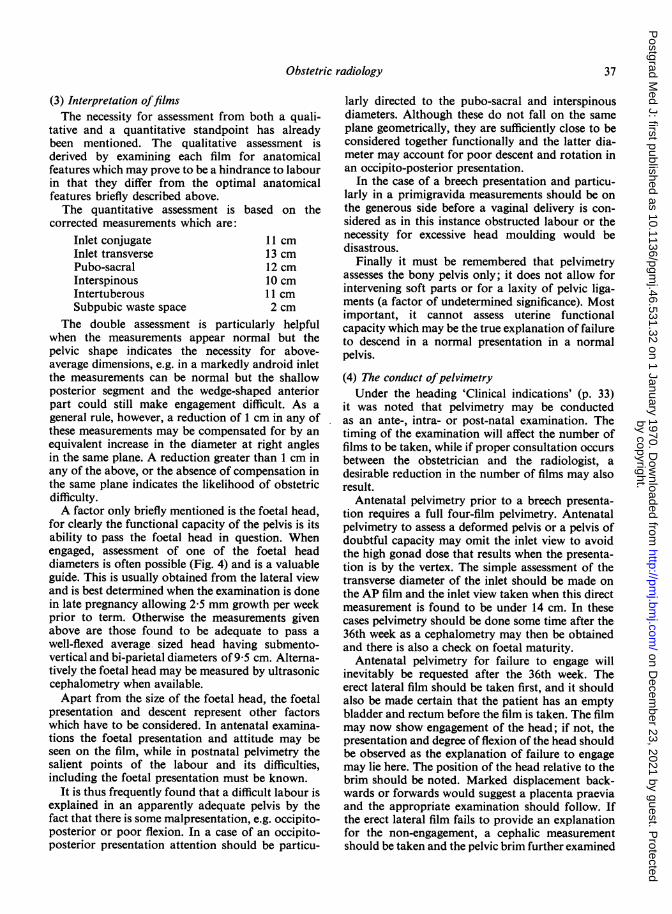
The outlet or subpubic arch view (Fig. 7). Thisdemonstrates the third pelvic plane mentionedabove. The subpubic arch is projected onto the filmby having the patient sit on the X-ray table, legsdrawn apart and leaning well forward so that theinferior ischio-pubic rami are close to and parallelto the table top. The X-ray beam is directed verticallydownwards from above, centred through the sacrum.A consideration of the patient's position explainswhy this view is difficult to obtain satisfactorily in thepuerperium and particularly so if an episiotomy hadbeen necessary. For this reason, when possible, fullpelvimetry is best delayed for at least 6 weeks afterlabour.This film shows the subpubic arch which should
normally subtend an angle of 90° or over: the ischialtuberosities are each represented by crescentic densewhite cortical lines. Since magnification is very smallin this view it is reasonable merely to deduct 0-5 cmfrom the measurement taken directly on the film toobtain a corrected measurement for intertuberousdiameter. This view is also useful for estimatingthe subpubic waste space, i.e. the region immediatelybehind the symphysis pubis which the foetal headcannot utilize during descent. This is shown byplacing a disc of 9-5 cm diameter, to represent anaverage foetal head, on the film so that the ischio-pubic rami form tangents to the disc and thenmeasuring the clear space between it and the sym-physis.
FIG. 7. Subpubic arch view. The semi-circle within theischio-pubic rami represents a foetal head. E-F isthe subpubic waste space (see also E-F in Fig. 3) A-Bis the intertuberous diameter. C-D the line across thebase of the ischial tuberosities.
36
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
Obstetric radiology
(3) Interpretation offilmsThe necessity for assessment from both a quali-
tative and a quantitative standpoint has alreadybeen mentioned. The qualitative assessment isderived by examining each film for anatomicalfeatures which may prove to be a hindrance to labourin that they differ from the optimal anatomicalfeatures briefly described above.The quantitative assessment is based on the
corrected measurements which are:Inlet conjugate 11 cmInlet transverse 13 cmPubo-sacral 12 cmInterspinous 10 cmIntertuberous 11 cmSubpubic waste space 2 cm
The double assessment is particularly helpfulwhen the measurements appear normal but thepelvic shape indicates the necessity for above-average dimensions, e.g. in a markedly android inletthe measurements can be normal but the shallowposterior segment and the wedge-shaped anteriorpart could still make engagement difficult. As ageneral rule, however, a reduction of 1 cm in any ofthese measurements may be compensated for by anequivalent increase in the diameter at right anglesin the same plane. A reduction greater than 1 cm inany of the above, or the absence of compensation inthe same plane indicates the likelihood of obstetricdifficulty.A factor only briefly mentioned is the foetal head,
for clearly the functional capacity of the pelvis is itsability to pass the foetal head in question. Whenengaged, assessment of one of the foetal headdiameters is often possible (Fig. 4) and is a valuableguide. This is usually obtained from the lateral viewand is best determined when the examination is donein late pregnancy allowing 2-5 mm growth per weekprior to term. Otherwise the measurements givenabove are those found to be adequate to pass awell-flexed average sized head having submento-vertical and bi-parietal diameters of 9-5 cm. Alterna-tively the foetal head may be measured by ultrasoniccephalometry when available.Apart from the size of the foetal head, the foetal
presentation and descent represent other factorswhich have to be considered. In antenatal examina-tions the foetal presentation and attitude may beseen on the film, while in postnatal pelvimetry thesalient points of the labour and its difficulties,including the foetal presentation must be known.
It is thus frequently found that a difficult labour isexplained in an apparently adequate pelvis by thefact that there is some malpresentation, e.g. occipito-posterior or poor flexion. In a case of an occipito-posterior presentation attention should be particu-
larly directed to the pubo-sacral and interspinousdiameters. Although these do not fall on the sameplane geometrically, they are sufficiently close to beconsidered together functionally and the latter dia-meter may account for poor descent and rotation inan occipito-posterior presentation.
In the case of a breech presentation and particu-larly in a primigravida measurements should be onthe generous side before a vaginal delivery is con-sidered as in this instance obstructed labour or thenecessity for excessive head moulding would bedisastrous.
Finally it must be remembered that pelvimetryassesses the bony pelvis only; it does not allow forintervening soft parts or for a laxity of pelvic liga-ments (a factor of undetermined significance). Mostimportant, it cannot assess uterine functionalcapacity which may be the true explanation of failureto descend in a normal presentation in a normalpelvis.(4) The conduct ofpelvimetryUnder the heading 'Clinical indications' (p. 33)
it was noted that pelvimetry may be conductedas an ante-, intra- or post-natal examination. Thetiming of the examination will affect the number offilms to be taken, while if proper consultation occursbetween the obstetrician and the radiologist, adesirable reduction in the number of films may alsoresult.
Antenatal pelvimetry prior to a breech presenta-tion requires a full four-film pelvimetry. Antenatalpelvimetry to assess a deformed pelvis or a pelvis ofdoubtful capacity may omit the inlet view to avoidthe high gonad dose that results when the presenta-tion is by the vertex. The simple assessment of thetransverse diameter of the inlet should be made onthe AP film and the inlet view taken when this directmeasurement is found to be under 14 cm. In thesecases pelvimetry should be done some time after the36th week as a cephalometry may then be obtainedand there is also a check on foetal maturity.
Antenatal pelvimetry for failure to engage willinevitably be requested after the 36th week. Theerect lateral film should be taken first, and it shouldalso be made certain that the patient has an emptybladder and rectum before the film is taken. The filmmay now show engagement of the head; if not, thepresentation and degree of flexion of the head shouldbe observed as the explanation of failure to engagemay lie here. The position of the head relative to thebrim should be noted. Marked displacement back-wards or forwards would suggest a placenta praeviaand the appropriate examination should follow. Ifthe erect lateral film fails to provide an explanationfor the non-engagement, a cephalic measurementshould be taken and the pelvic brim further examined
37
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
J. H. Highman
in its transverse diameter by means of the AP orpossibly the inlet view.
Pelvimetry performed in labour to assess progressis restricted to the erect lateral as it is the only filmthat can reasonably be obtained and gives most ofthe necessary information, i.e. degree of descent ofthe head, its presentation, degree of flexion and theAP dimensions of the pelvis.
Post-natalpelvimetry. A full four-film examinationshould be obtained.A note on the erect lateral view. This view is
sometimes requested as a single check on theobstetric features of the pelvis. Whereas it must beadmitted that this view is probably the most informa-tive of the four films that have been discussed, it mustalso be realized that it can only assess the pelvis in itssagittal plane, and it is unwise to assume that pelvicdeformities or inadequacies are confined only to thisplane. It is the purpose of this note, therefore, tostress that pelvic inadequacy can occur in thetransverse plane and that false reliance should not beplaced on a single film in a mistaken attempt toreduce radiation dosage to the patient or the foetus(Williams, 1958).
PlacentographyUsing conventional X-rays two techniques are in
regular use, namely arterial placentography andplain X-rays. Both can achieve high and similardegrees of accuracy in the demonstration of placentalsite.The arterial technique should only be practiced by
those skilled in arteriography, when it becomes onlya very minor surgical procedure. The placental sitecan often be determined using one well-timedradiographic exposure but one source of error lies inthe possibility of asynchronous sinusoidal filling sothat the full extent of a marginal placenta praeviamay not be shown on the one film. Another problemis the estimation of what in fact constitutes the lowersegment of the uterus, a structure defined in theobstetric textbooks without reference to bonylandmarks. For different approaches to the solutionof this problem see Basson & De Villiers (1963) andHerlinger (1968). In spite of these possible draw-backs the procedure is, in capable hands, an excel-lent one.
Alternatively where skilled arteriographic help isnot available, plain film techniques, well applied, canprovide an invaluable service. Two approaches arepossible; firstly, one may attempt to demonstratethe soft tissue shadow of the placenta using AP andlateral films. For the lateral view some form ofdifferential filtration is necessary to reduce the highsubject contrast between the posterior and anteriorparts of the maternal abdomen (Highman, 1969).Alternatively, a careful appraisal of any anterior or
posterior displacement of the foetal head as itpresents at the pelvic brim may be helpful (Highman,1969). Other techniques at present in more restricteduse are ultrasonic and radio-iostope scanning. Theirmain weakness is in the demonstration of theposterior placenta praevia but this problem is beingovercome and in the appropriate centres thesetechniques may yet come to rival the more conven-tional ones.
The foetusRadiology is now only rarely called upon to
demonstrate the presence of a foetus but determina-tion of maturity near term, the demonstration ofmultiple pregnancies, presentations difficult todetermine clinically, foetal abnormalities and foetaldeath may all be valid indications for radiography.
In spite of doubts cast upon it, Russell (1969) hascarefully analysed and proved the accuracy of ante-natal maturation estimates.An interesting advance in this field is the finding
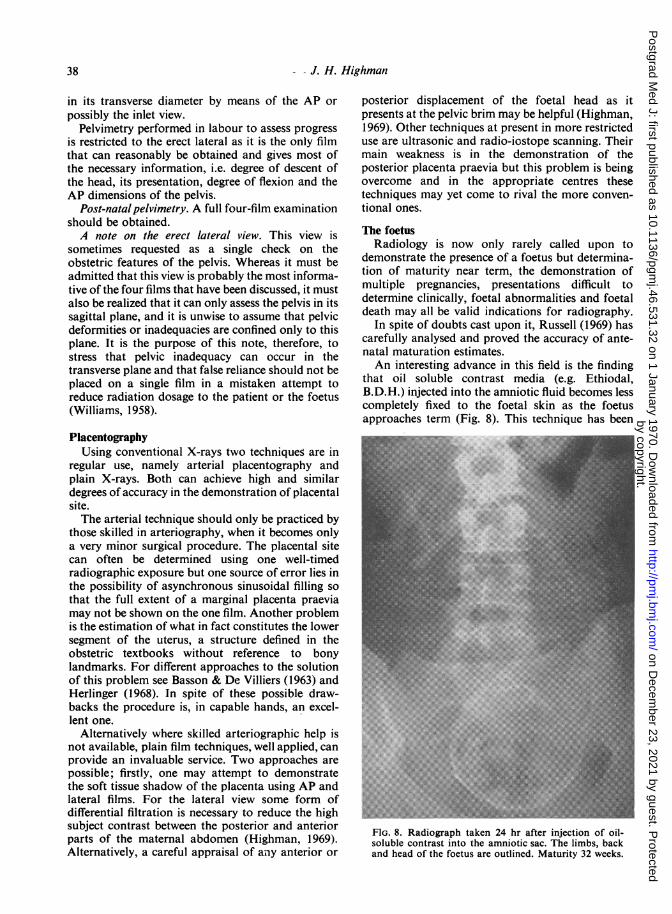
that oil soluble contrast media (e.g. Ethiodal,B.D.H.) injected into the amniotic fluid becomes lesscompletely fixed to the foetal skin as the foetusapproaches term (Fig. 8). This technique has been
FlG. 8. Radiograph taken 24 hr after injection of oil-soluble contrast into the amniotic sac. The limbs, backand head of the foetus are outlined. Maturity 32 weeks.
38
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from
Obstetric radiology 39
combined with a cytological method of foetalmaturity estimation (Brosens, Gordon & Baert,1969). Another advance worth recording is the useof ultrasonics either as a scan or by Doppler effectin the diagnosis of twins, confirmation of earlypregnancy and in foetal cephalometry.
ReferencesBASSON, J.M.M. & DE VILLIERS, J.N. (1963) Retrograde
aortic placentography. Clinical Radiolog,, 14, 230.BROSENS, I., GORDON, H. & BAERT, A. (1969) Prediction of
fetal maturity with combined cytological and radiologicalmethods. Journal of Obstetrics and Gynaecologv of theBritish Commonwealth, 76, 20.
COURT BROWN, W.M., DOLL, R. & HILL, A.B. (1960)Incidence of leukaemia after exposure to diagnosticradiation in utero. British Medical Journal, 2, 1539.
HERLINGER, H. (1968) Single film inclined angioplacento-graphy in the diagnosis of placenta praevia. ClinicalRadiology, 19, 59.
HIGHMAN, J.H. (1969) Textbook of Radiology (Ed. by D.Sutton and R. Grainger). Livingstone, Edinburgh.
RUSSELL, J.G.B. (1969) Radiological assessment of fetalmaturity. Journal of Obstetrics and Gynaecology of theBritish Commonwealth, 76, 208.
STEWART, A.M., WEBB, J.W., GILES, D. & HEWITT, D. (1956)Malignant disease in childhood and diagnostic radiation inutero. Lancet, ii, 447.
STEWART, A.M., WEBB, J.W. & HEWITT, D. (1958) A surveyofchildhood malignancies. British Medical Journal, 1, 1495.
STEWART, A.M. & KNEALE, G.W. (1968) Changes in cancerrisk associated with obstetric radiology. Lancet, i, 104.
WILLIAMS, R. (1958) For erect lateral only please. Lancet,ii, 1008.
by copyright. on D
ecember 23, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.46.531.32 on 1 January 1970. Dow
nloaded from