Embed Size (px)
Citation preview
OCCUPATIONAL RISK IN HEALTHCARE
Prof. Dr. Rusli Bin NordinMBBS; MPH; PhD; FFOMI; FAOEMM; AMProfessor of Public Health & HeadClinical School Johor BahruJeffrey Cheah School of Medicine and Health SciencesMonash University Sunway CampusE-mail: [email protected]: 012-7211994 (Mobile) /07-2264868 (Office) /07-2211628 (Direct) Fax: 07-2262413
Joint ICOH / ISSA Recommendations for protecting Health Care Workers’ Health (Kitakyushu, 2004)
• Occupational risk prevention for health care workers varies from country to country. In some countries, preventive measures are fairly well developed, in others they are practically non-existent.
• Regarding infectious risks, prevention is mostly insufficient in countries where these diseases are highly prevalent.
• Health care workers often have little knowledge of their occupational risks as well as preventive means.
Hazards in healthcare• PhysicalNoise, Heat, Vibration, Lighting
• BiologicalHIV, HBV, H1N1, DF/DHF, TB, Leptospirosis
• ChemicalChemical disinfectants (e.g. EO, Glutaraldehyde)
• ErgonomicsProlonged standing, awkward postures, repetitive work
• PsychosocialShift work, stress, anxiety, depression, burnout, work
disengagement, work-related quality of life, harassment, violence
Special issue: reproductive health (men and women)
Content1. Occupational Risk in Healthcare: Introduction
• OSHA 1994 & Regulations/ Guidelines / Codes of Practices2. Occupational Risk in Health Care: Health Care Workers (HCW)3. Occupational Risk in Healthcare: Patients4. Occupational Risk in Healthcare: Employers5. Health Risk Management
• OSH-MS• Safety & Health Committee• Safety Officer• HIRARC Guidelines• Medical Surveillance• Ergonomic Redesign of Workplaces• Universal Precautions• Healthy Hospital Register• Health Promotion Activities & CME• Employee Assistance Program
• Workplace counseling• Workplace compensation
6. Conclusion
OCCUPATIONAL RISK IN HEALTHCARE
Introduction
Occupational Risk in Healthcare: Introduction
Occupational Safety and Health Act (OSHA 1994) (Act 514)
Part IV GENERAL DUTIES OF EMPLOYERS AND SELF-EMPLOYED PERSONS15. General duties of employers and self-employed persons
to their employees 1816. Duty to formulate safety and health policy 2217. General duties of employers and self-employed persons to
persons other than their employees 2318. Duties of an occupier of a place of work to persons other
than his employees 2519. Penalty for an offence under section 15, 16, 17 or 18 26
Section 15 is one of the most important sections in the Act.
It states the general duties of employers and self-employed persons to their employees.
(1) It shall be the duty of every employer and every self-employed person to ensure, so far as is practicable, the safety, health and welfare at work of all his employees.
(OSHA, 1994)
17. General duties of employers and self-employed persons to persons other than their employees
(1) It shall be the duty of every employer and every self-employed person to conduct his undertaking in such a manner as to ensure, so far as is practicable, that he and other persons, not being his employees, who may be affected thereby are not thereby exposedto risks to their safety or health.
(OSHA, 1994)
19. Penalty for an offence under section 15, 16, 17 or 18
A person who contravenes the provisions of section 15, 16, 17 or 18 shall be guilty of an offence and shall, on conviction, be liable to a fine not exceeding fifty thousand ringgit or to imprisonment for a term not exceeding two years or to both.
(OSHA,1994)
Occupational Risk in Healthcare: Introduction
OSHA 1994 & Regulations/ Guidelines / Codes of Practices
Part VI GENERAL DUTIES OF EMPLOYEES
24. General duties of employees at work 3325. Duty not to interfere with or misuse things 34
provided pursuant to certain provisions26. Duty not to charge employees for things done 35
or provided 27. Discrimination against employee, etc 35
24. General duties of employees at work(1) It shall be the duty of every employee while at work:
(a) to take reasonable care for the safety and health of himself and of other persons who may be affected by his acts or omissions at work;
(b) to co-operate with his employer or any other person in the discharge of any duty or requirement imposed on the employer or that other person by this Act or any regulation made thereunder;
(OSHA 1994)

24. General duties of employees at work…(1) It shall be the duty of every employee while at work:..
(c) to wear or use at all times any protectiveequipment or clothing provided by the employer forthe purpose of preventing risks to his safety and health;and(d) to comply with any instruction or measure onoccupational safety and health instituted by hisemployer or any other person by or under this Act or anyregulation made thereunder.
(OSHA 1994)
24. General duties of employees at work…
(2) A person who contravenes the provisions of this section shall be guilty of an offence and shall, on conviction, be liable to a fine not exceeding one thousand ringgit or to imprisonment for a term not exceeding three months or to both.
25. Duty not to interfere with or misuse things provided pursuant to certainprovisions
A person who intentionally, recklessly or negligently interferes with or misuses anything provided or done in the interests of safety, health and welfare in pursuance of this Act shall be guilty of an offence and shall, on conviction, be liable to a fine not exceeding twenty thousand ringgit or to imprisonment for a term not exceeding two years or to both.
(OSHA 1994)
26. Duty not to charge employees for things done or provided
No employer shall levy or permit to be levied on any employee of his any charge in respect of anything done or provided in pursuance of this Act or any regulation made thereunder.
(OSHA 1994)
27. Discrimination against employee, etc.(1) No employer shall dismiss an employee, injure him in his employment, or alter his position to his detriment by reason only that the employee:
(a) makes a complaint about a matter which he considers is not safe or is a risk to health;(b) is a member of a safety and health committee established pursuant to this Act; or(c) exercises any of his functions as a member of the safety and health committee.
(OSHA 1994)
(2) No trade union shall take any action on any of its members who, being an employee at a place of work:
(a) makes a complaint about a matter which he considers is not safe or is a risk to health;(b) is a member of a safety and health committee established pursuant to this Act; or(c) exercises any of his functions as a member of a safety and health committee.
(OSHA 1994)

(3) An employer who, or a trade union which, contravenes the provisions of this section shall be guilty of an offence and shall, on conviction, be liable to a fine not exceeding ten thousand ringgit or to a term of imprisonment not exceeding one year or to both.
(OSHA 1994)
(4) Notwithstanding any written law to the contrary, where a person is convicted of an offence under this section the Court may, in addition to imposing a penalty on the offender, make one or both of the following orders:
(a) an order that the offender pays within a specific period to the person against whom the offender has discriminated such damages as it thinks fit to compensate that person;(b) an order that the employee be reinstated or re-employed in his former position or, where that position is not available, in a similar position.
(OSHA 1994)
29. Safety and health officerOccupational Safety and Health (Safety and Health Officer) Regulations 1997 have been madeand provide details of registration of SHO, notification of SHO, duties of SHO and employer.
(3) The safety and health officer shall be employed exclusively for the purpose of ensuring the due observance at the place of work of the provisions of this Act and any regulation made thereunder and the promotion of a safe conduct of work at the place of work.
(OSHA 1994)
30. Establishment of safety and health committee at place of work
(1) Every employer shall establish a safety and health committee at the place of work in accordance with this section if:
(a) there are forty or more persons employed at the place of work; or
(b) the Director General directs the establishment ofsuch a committee at the place of work.
(OSHA 1994)
Occupational Risk in Healthcare: Introduction
OSH Act (1994) & Regulations• Use and Standard of Exposure of Chemicals Hazardous to
Health (USECHH) Regulations 2000• Classification, Packaging and Labeling of Hazardous
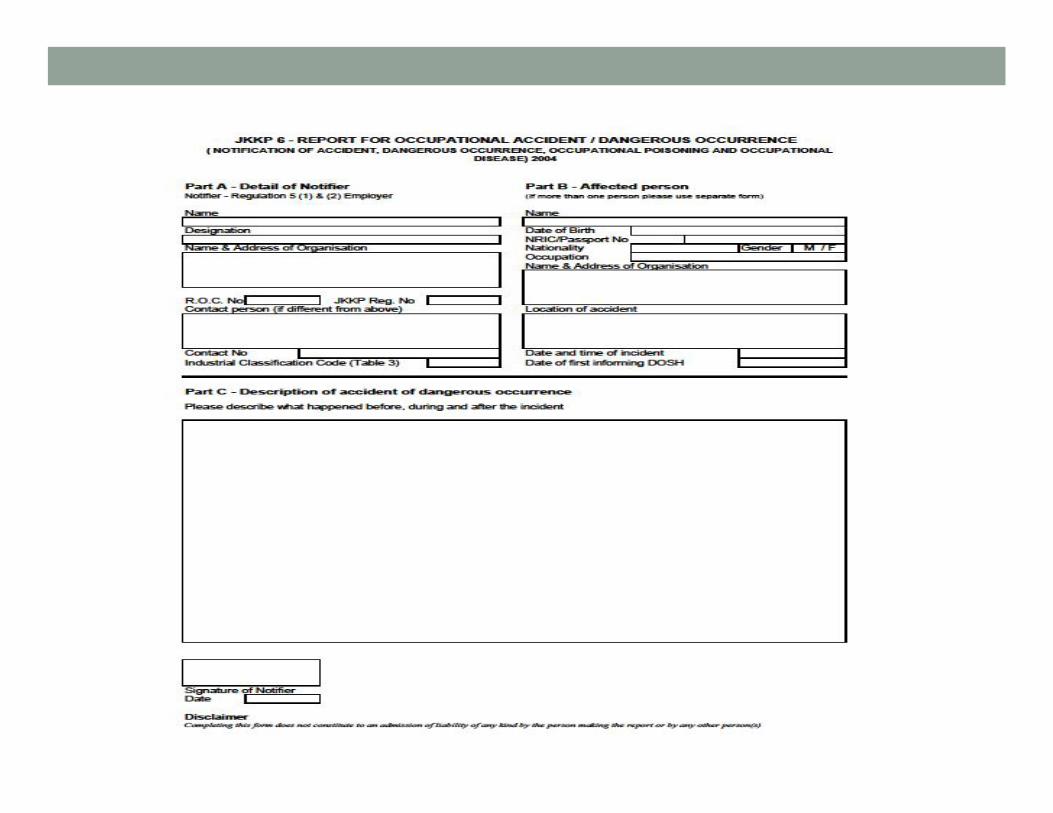
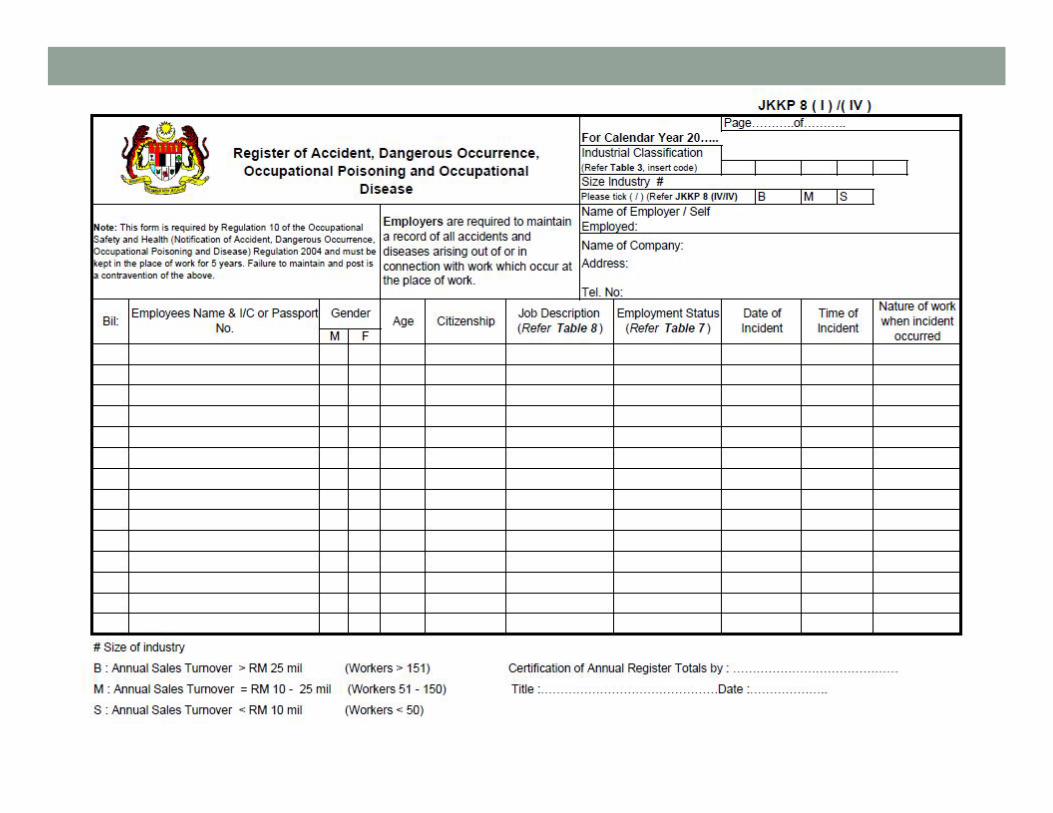
Chemicals (CPL) Regulations 1997• Notification of Accident, Dangerous Occurrence, Occupational
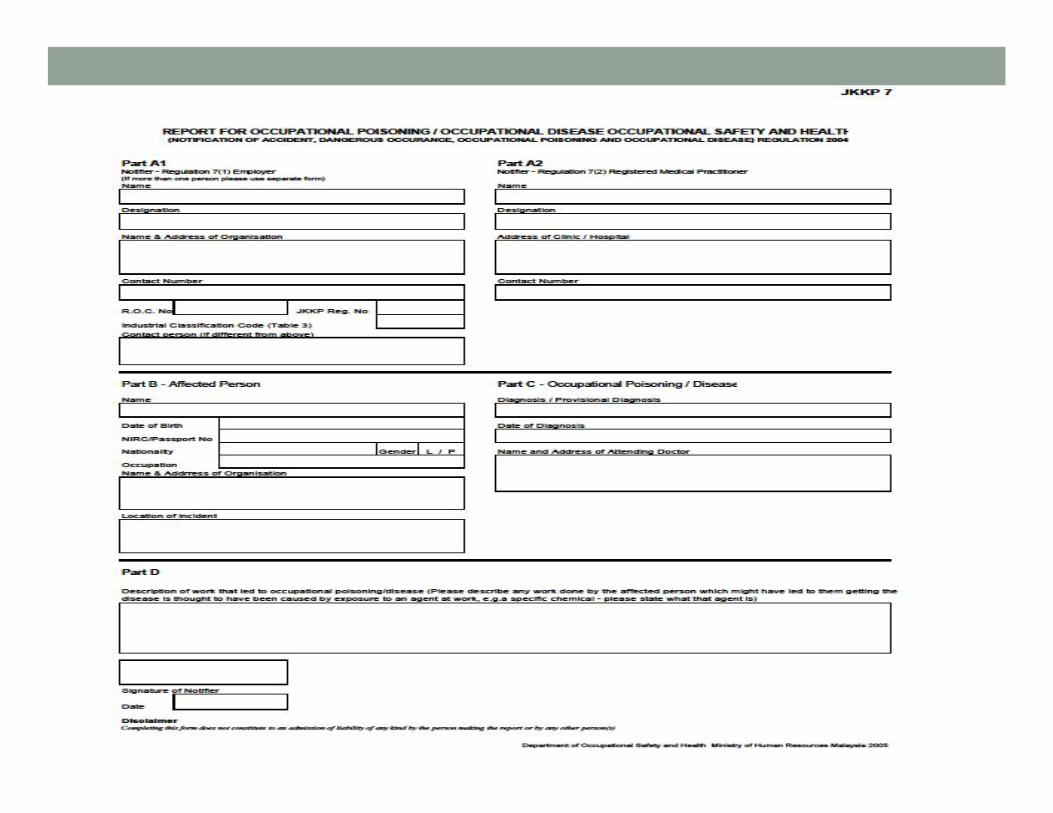
Poisoning, and Occupational Disease (NADOPOD) Regulations 2004
P.U.(A) 128/2004 OCCUPATIONAL SAFETY AND HEALTH (NOTIFICATION OF ACCIDENT, DANGEROUS OCCURRENCE, OCCUPATIONAL POISONING AND
OCCUPATIONAL DISEASE) REGULATIONS 2004
FIRST SCHEDULE
[sub-regulation 5(1)] SERIOUS BODILY INJURY
1. Emasculation 2. Permanent privation of the sight of either eye 3. Permanent privation of the hearing of either ear 4. Privation of any member or joint 5. Destruction or permanent impairing of the powers of any member or joint 6. Permanent disfiguration of the head or face 7. Fracture or dislocation of the bone 8. Loss of consciousness from lack of oxygen 9. Loss of consciousness or acute illness from absorption, inhalation or ingestion of any
substance, which requires treatment by a registered medical practitioner 10.Any case of acute ill health where there is a reason to believe that this resulted from
occupational exposure to isolated pathogen or infected material 11.Any other work related injury or burns which results in the person injured being
admitted immediately into hospital for more than 24 hours
P.U.(A) 128/2004 OCCUPATIONAL SAFETY AND HEALTH (NOTIFICATION OF ACCIDENT, DANGEROUS OCCURRENCE, OCCUPATIONAL
POISONING AND OCCUPATIONAL DISEASE) REGULATIONS 2004
SECOND SCHEDULE
[sub-regulation 5(1)]
DANGEROUS OCCURRENCE PART I
DANGEROUS OCCURRENCES WHICH ARE NOTIFIABLE WHEREVER THEY OCCUR
• COLLAPSE OF SCAFFOLDING• COLLAPSE OF A BUILDING OR STRUCTURE • ELECTRICAL SHORT CIRCUIT • ESCAPE OF A SUBSTANCE• EXPLOSION, FIRE OR FAILURE OF STRUCTURE• LIFTING MACHINERY, ETC.
5. Tuberculosis or leprosy Any occupation involving close or frequent contact with a source or sources of tuberculosis or leprosy infection by reason of employment: (a) in the medical treatment or nursing of a person or persons suffering from tuberculosis or leprosy or in a service ancillary to such treatment or nursing; (b) in attendance upon a person or persons suffering from tuberculosis or leprosy where the need for such attendance arises by reason of physical or mental infirmity; (c) as a research worker engaged in research in connection with tuberculosis or leprosy; or (d) as a laboratory worker, pathologist or post-mortem worker, where the occupation involves working with material which is a source of tuberculosis or leprosy infection or in any occupation ancillary to such employment.
6. Viral hepatitis Any occupation involving: (a) close and frequent contact with human blood or human blood products; or (b) close and frequent contact with a source of viral hepatitis infection by reason of employment in the medical treatment or nursing of a person or persons suffering from viral hepatitis, or in a service ancillary to such treatment or nursing.
7. Any illness caused by a pathogen Work involving a pathogen which presents a hazard to human health.
8. Acquired Immunodeficiency Syndrome (AIDS) Any occupation involving:(a)close and frequent contact with human blood or
human blood products; or(b) close and frequent contact with a source of AIDS infection by reason of employment in the medical treatment or nursing of a person suffering from AIDS, or persons infected with a Human Immunodeficiency Virus (HIV), or in a service ancilliary to such treatment or nursing.

Occupational Risk in Healthcare: Introduction
OSHA 1994 & Regulations/ Guidelines / Codes of Practices
OCCUPATIONAL RISK IN HEALTHCARE
HCW
HCW at risk• Underlying medical conditions
• Hypertension, IHD, DM• Allergy, Asthma, Eczema, Rhinitis• Obesity• Musculoskeletal disorders• Neurobehavioral disorders• Mental disorders• Sensory impairment
• Young, healthy, less experience• Older, not so healthy, more experience• Pregnant women• Breast feeding
HazardsHealth
• Biological• Virus: HIV, HBV, HCV, Nipah V, H5N1 V, SARS Corona V• Bacteria: Mycobacterium TB, Lepto Icterohemorrhagica
• Chemical• Glutaraldehyde, halothane, nitrous oxide, formaldehyde• Cytotoxics, pharmaceuticals, disinfectants, cleansing agents• Pyrethrins, pyrethroids, organophosphates
• Physical• Electric current, heat, light, laser, microwave, radiation, vibration, noise
• Ergonomic• Work design, posture, repetitive strain injury
• Psychosocial• Work stress, burnout, anxiety, depression, job dissatisfaction, shift work, night work, violence, harassment,
quality of working lifeSafety
• Needle stick injury• Slipping/tripping• Fire• Moving parts of machinery• Working at height• Prolonged standing• Lifting / manual handling
Environmental• Indoor Air Quality (IAQ), air pollution• Water pollution
(Guidelines for HIRARC, 2008)
Occupational Risk in Health Care: Health Care Workers (HCW)Occupational deaths among healthcare workers.Kent A. Sepkowitz* and Leon Eisenberg†Emerging Infectious Diseases • Vol. 11, No. 7, July 2005• Accessed on 23.03.2011: www.cdc.gov/eid
• *Memorial-Sloan-Kettering Cancer Center, New York, New York,USA; and †Harvard Medical School, Boston, Massachusetts, USA
Occupational Risk in Health Care: Health Care Workers (HCW)• Med J Malaysia. 2008 Aug;63(3):222-3.• Risk of blood-borne infection among health care workers in two Kuala Lumpur
hospitals.• Hesham R, Tajunisah ME, Ilina I.• Department of Pharmacy, Faculty of Allied Health Sciences, Universiti Kebangsaan Malaysia,
Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysia. [email protected]
• Health care workers (HCW) are at high risk of acquiring blood-borne diseases. • This study compared the risk of infection among HCW in different hospital units and also
between HCW and students in medical fields. • This cross-sectional study involved pre-tested questionnaires that were completed by 625
HCW and undergraduate students undergoing clinical attachments from February to August 2001.
• The respondents were separated into two groups: i) HCW from Hospital Kuala Lumpur, HKL (n=241) and Hospital Universiti Kebangsaan Malaysia, HUKM (n=153) ii) Medical students from Universiti Kebangsaan Malaysia, UKM (n=171) and HUKM student nurses (n=60).
• The results obtained showed that the risk of transmission of blood-borne infections varied significantly according to professional ranks (p<0.05) and to hospital units (p<0.05).
• The medical intensive care (ICU), haemodialysis, and nephrology and urology units had the highest scores for the risk of infection while the diagnostic laboratory had the lowest risk of infection (p<0.05).
• Preventive measures taken by the subjects in this study were not satisfactory especially with reference to the use of personal protective equipment and the practice of universal precautions.
Occupational Risk in Health Care: Health Care Workers (HCW)• Med J Malaysia. 2005 Oct;60(4):407-10.• Hepatitis B immunisation status among health care workers in two Kuala Lumpur
hospitals.• Hesham R, Zamberi S, Tajunisah ME, Ariza A, Ilina I.• Department of Pharmacy, Faculty of Allied Health Sciences, Universiti Kebangsaan Malaysia,
Kuala Lumpur.
• Health care workers (HCW) are at higher risk of acquiring blood borne infections such as hepatitis B virus, hepatitis C virus and human immunodeficiency virus from patients.
• To minimise exposure, Universal Precautions Policy guidelines were introduced. • This study looked into one of the aspects of hepatitis B prevention among HCW in the
Malaysian context. • The objective of this study was to assess hepatitis B vaccine coverage among HCW. A cross
sectional study involving pre-tested questionnaires was undertaken from February 2001 to August 2001. Hospital staff in Hospital Kuala Lumpur and Hospital Universiti KebangsaanMalaysia as well as undergraduate students undergoing clinical attachments were randomly chosen. A total of 625 subjects were enrolled. Only 58.4% had taken a complete hepatitis B vaccination. However, 82.2% have taken at least one dose of the hepatitis B vaccine and were supposed to complete the schedule in due course. Not all HCW were protected against hepatitis B.
• Preventing hepatitis B in HCW should be one of the priorities of the hospital management as it is definitely cheaper than managing chronic hepatitis B cases.
Southeast Asian J Trop Med Public Health. 2010 Sep;41(5):1192-9.Knowledge of blood-borne infectious diseases and the practice of universal precautions amongst health-care workers in a tertiary hospital in Malaysia.Hamid MZ, Aziz NA, Anita AR, Norlijah O.Department of Pediatrics, Faculty of Medicine and Health Sciences, University Putra Malaysia, Serdang, Selangor, Malaysia. [email protected]• To assess the knowledge of blood-borne diseases transmitted through
needle stick injuries and practices of universal precautions amongst health-care workers in a tertiary teaching hospital.
Materials & Method• Cross-sectional study of 215 HCW (63.3% staff nurses) in Serdang Hospital
(January to July 2008).• Self-administered questionnaire assessing knowledge of blood-borne
diseases and universal precautions and actual practice of universal precautions. Results• The mean knowledge score was 31.84 (SD 4.30) and the mean universal
practice score was 9.0 (SD 2.1). • There was a small, positive correlation between knowledge and actual
practice of universal precautions (r = 0.300, n = 206, p < 0.001) amongst the cohort studied.
• Age and years of experience did not contribute towards acquisition of knowledge about blood-borne illnesses or the practice of universal precautions.
European Journal of Social Sciences – Volume 13, Number 3 (2010) 354Needle Stick and Sharps Injuries and Factors Associated Among Health Care Workers in a Malaysian HospitalLekhraj Rampal, Rosidah Zakaria, Leong Whye Sook, Azhar Md ZainAbstractThe objective of this study was to determine the prevalence and factors associated with needle stick and sharps injuries.Methods: This cross sectional study was conducted in Serdang Hospital Malaysia using aself-administered validated questionnaire. The respondents consisted of 345 HCWs namelymedical assistant officer, staff nurses, medical laboratory technician and community nurse.Results: • The overall prevalence of needle stick or sharps injuries was 23.5%. • Staff nurses had the highest prevalence (27.9%). • The causes of NSSI in 58% of cases were hypodermic needle and 27.2% cases were recapping. • Medical ward reported the highest NSSIs (51.9%).• Knowledge on body fluid transmitted by HIV/AIDS and blood products was high (99.1%).• Majority stated that they throw needles or sharps immediately after use in sharp bins• (92.7%), do not separate needles from syringes prior to disposal (98.0%) and do not• dissemble needles or sharps with hand (98.5%) and do not recap needles after use (94.3%).• Majority also stated that they were aware about universal precaution guidelines (96.5%) and needle stick and sharps
injury needs to be reported (99.1%). However, out of those health• care workers (23.5%) who had NSSI, only 30.9% had reported the incident of needle stick and sharps injuries indicating
that there were gaps between knowledge and practice among the HCWs. • There was a statistically significant association between NSSIs and age (p=0.01) of respondent, working experience
(p=0.001) and job categories (p=0.03).Conclusions: The prevalence of NSSI was 23.5%. Although the knowledge on UniversalPrecautions is good, the prevalence of NSSIs is still high and there are gaps betweenknowledge and practice related to HIV prevention. NSSIs continue to pose a seriousoccupational problem.
Heart Lung. 1994 Jul-Aug;23(4):352-8.Universal precautions: an update.Gershon RR, Karkashian C, Felknor S.School of Hygiene and Public Health, Johns Hopkins University, Baltimore, MD 21205.
• Universal precautions, the set of work practice recommendations designed to help minimize occupational exposure to blood-borne pathogens, have been shown to be effective.
• However, lack of compliance with these recommendations has been well documented, both before and after the enactment of the OSHA Blood-borne Pathogens Standard.
Tuberculosis (Edinb). 2004;84(1-2):19-23.Risk factors of tuberculosis among health care workers in Sabah, Malaysia.Jelip J, Mathew GG, Yusin T, Dony JF, Singh N, Ashaari M, Lajanin N, Shanmuga Ratnam C, Yusof Ibrahim M, Gopinath D.Sabah Health Office, Tuaran, Sabah, Malaysia. [email protected]
• Age, gender, history of TB contact outside the workplace (other than family contact), duration of service and failure to use respiratory protection when performing high-risk procedures, were the main risk factors of TB among health care workers.
• Based on the study findings, we recommend that health care workers in the first 10 years of service should take extra precautions, such as using respiratory protection when performing procedures that are considered to be of high risk with respect to TB infection.
• They should also undergo TB screening at least once every 2 years and, if symptomatic, offered prophylactic treatment.
• The Respiratory Protection Program should be fully implemented to help reduce the risk of TB among health care workers in Sabah.
Risk of TB is elevated in following occupational groups:1. Hospital employees in wards with tuberculosis patients2. Nurses in hospitals3. Nurses of HIV-positive or drug-addicted patients4. Pathology and laboratory workers5. Respiratory therapists and physiotherapists6. Physicians in internal medicine, anaesthesia, surgery and psychiatry7. Non-medical hospital personnel in house keeping and transport work8. Funeral home employees and prison employeesRespiration 2005;72:431-446
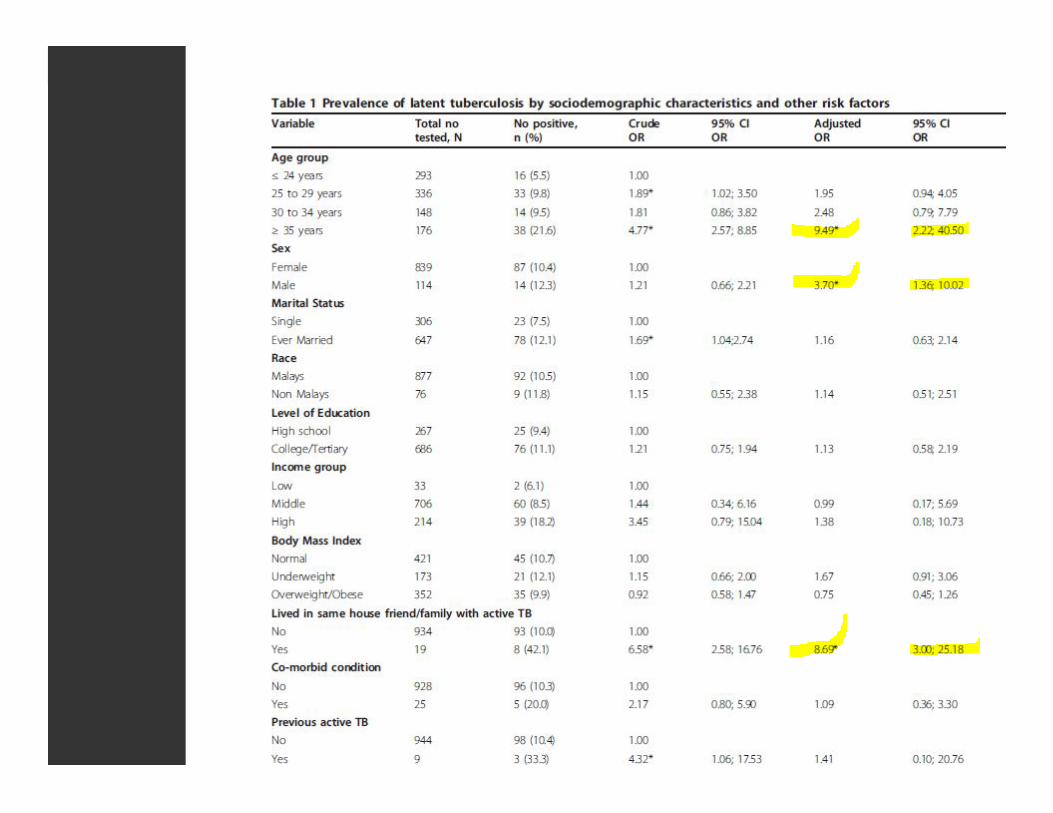
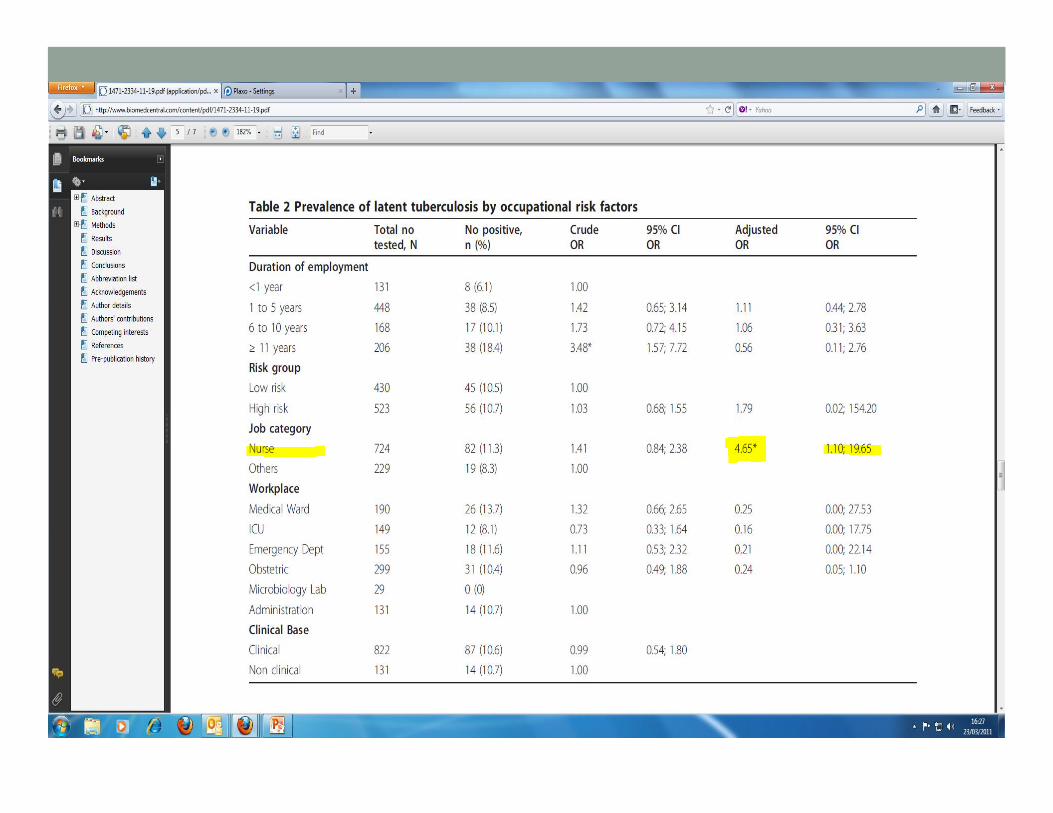
Occupational Risk in Health Care: Health Care Workers (HCW)• Prevalence and risk factors of latent tuberculosis infection
among health care workers in Malaysia• Shaharudin Rafiza1 , Krishna Gopal Rampal2 and Aris
Tahir3
• 1 Institute for Medical Research, Environmental Health Research Centre, Occupational Health Unit, Jalan Pahang, 50588 Kuala Lumpur, Malaysia
• 2 Universiti Kebangsaan Malaysia Medical Centre, Department of Community Health, Jalan Yaacob Latif, 56000 Kuala Lumpur, Malaysia
• 3 Institute for Public Health, Jalan Bangsar, 50590 Kuala Lumpur, Malaysia
• BMC Infectious Diseases 2011, 11:19 doi:10.1186/1471-2334-11-19
OCCUPATIONAL RISK IN HEALTHCARE
Patients
Occupational Risk in Health Care: Patients
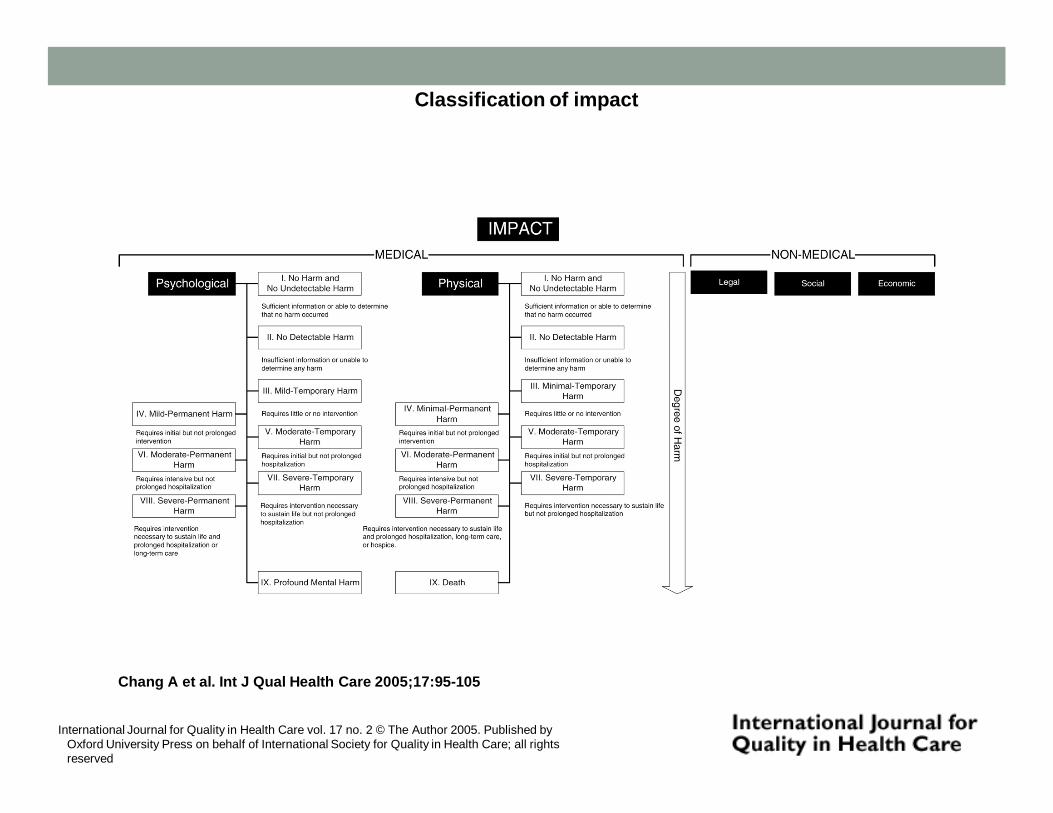
Classification of impact
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
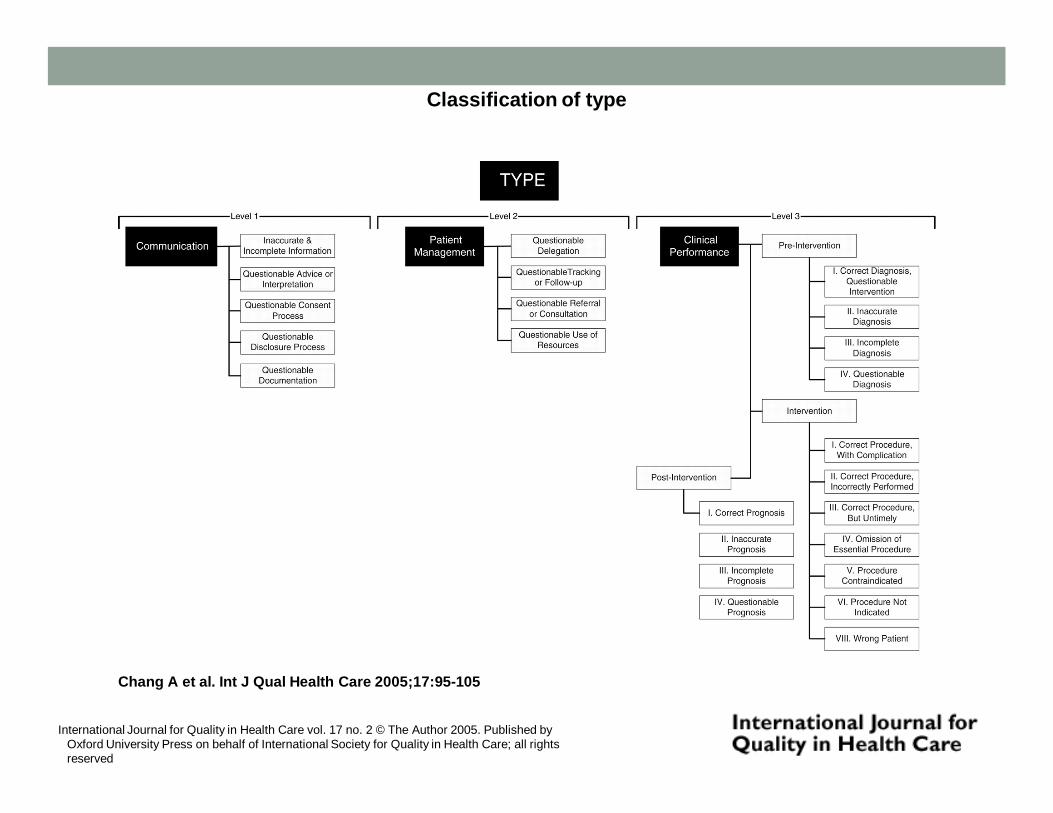
Classification of type
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
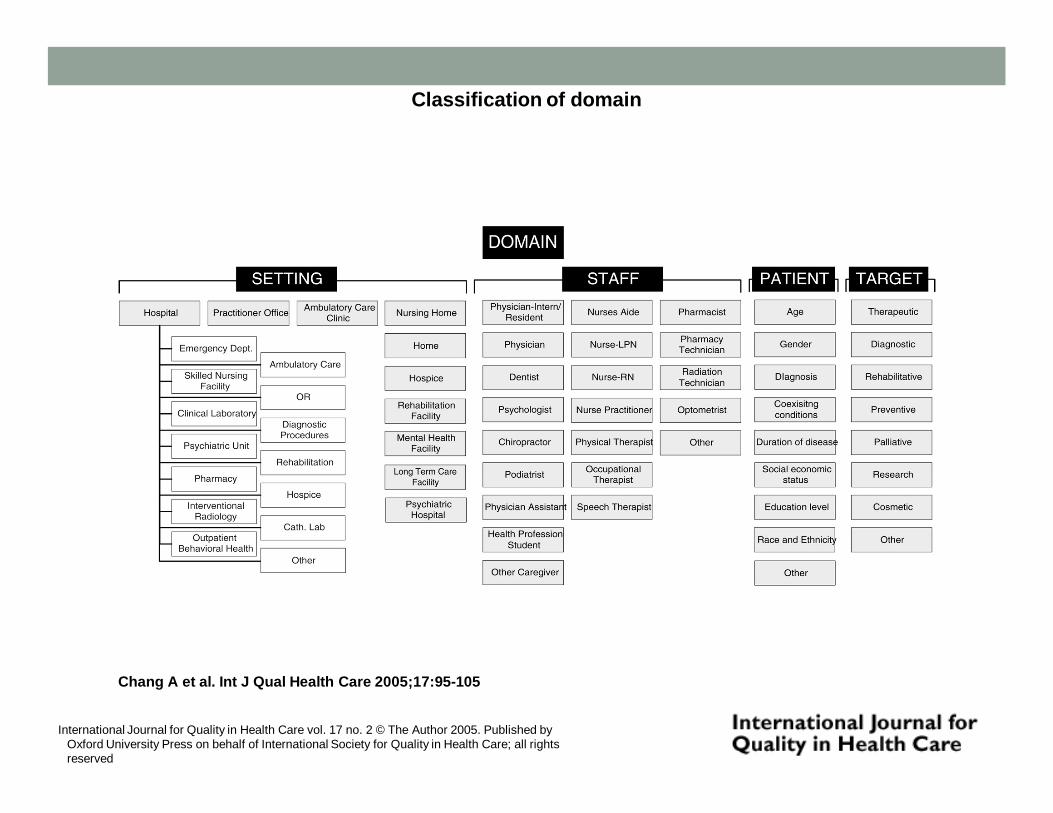
Classification of domain
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
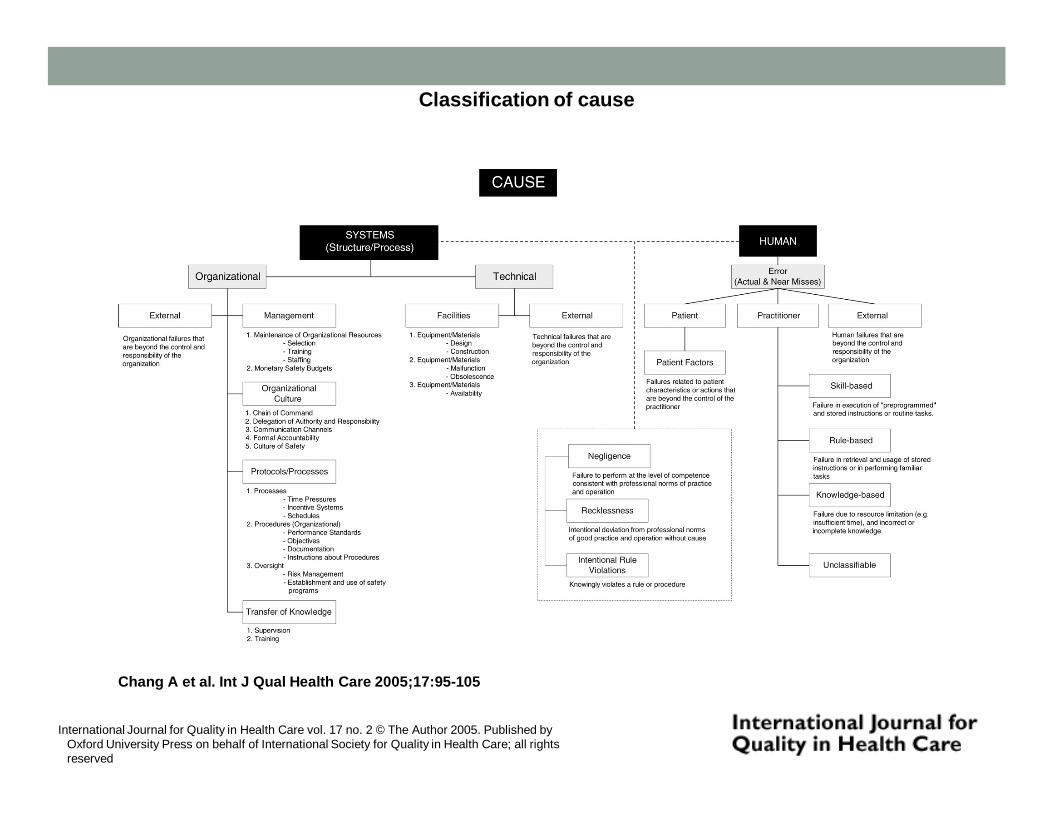
Classification of cause
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
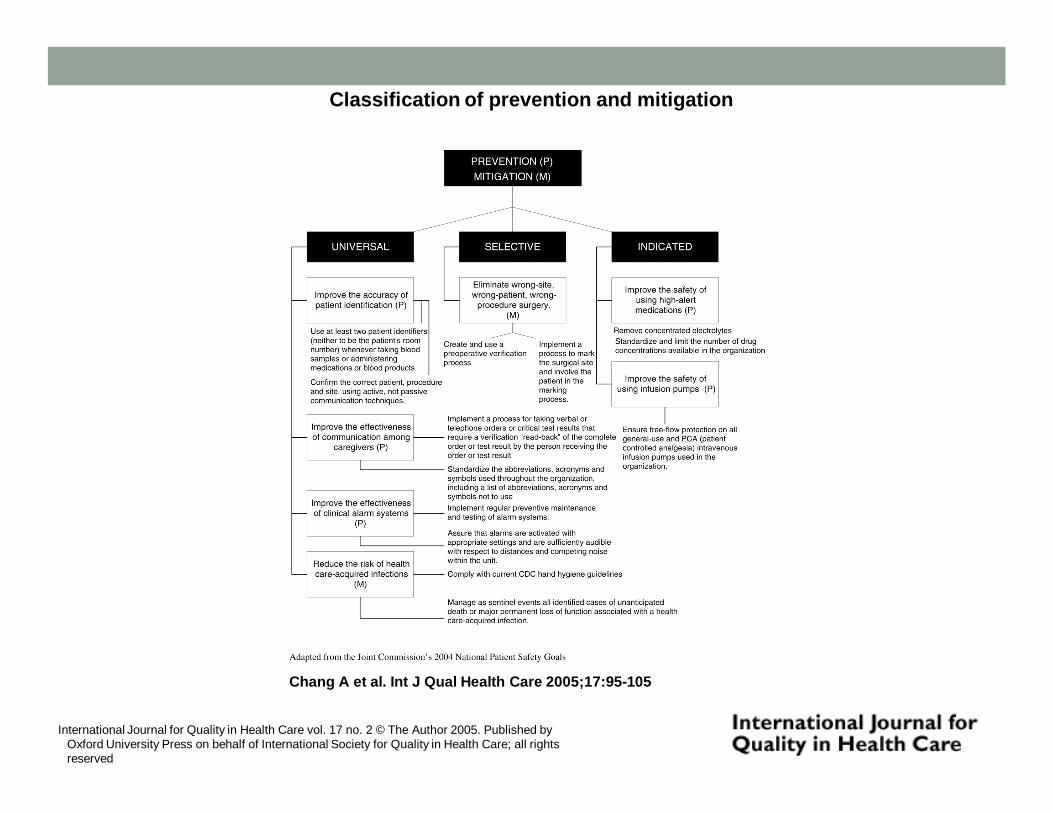
Classification of prevention and mitigation
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
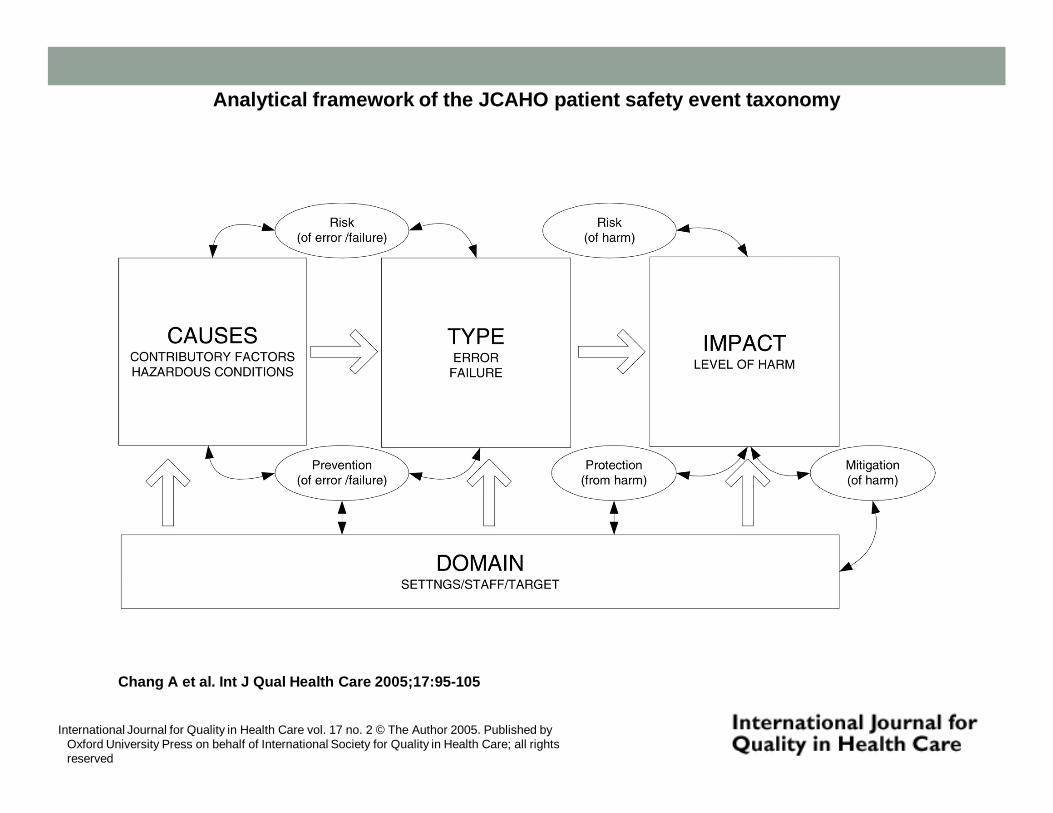
Analytical framework of the JCAHO patient safety event taxonomy
Chang A et al. Int J Qual Health Care 2005;17:95-105
International Journal for Quality in Health Care vol. 17 no. 2 © The Author 2005. Published by Oxford University Press on behalf of International Society for Quality in Health Care; all rights reserved
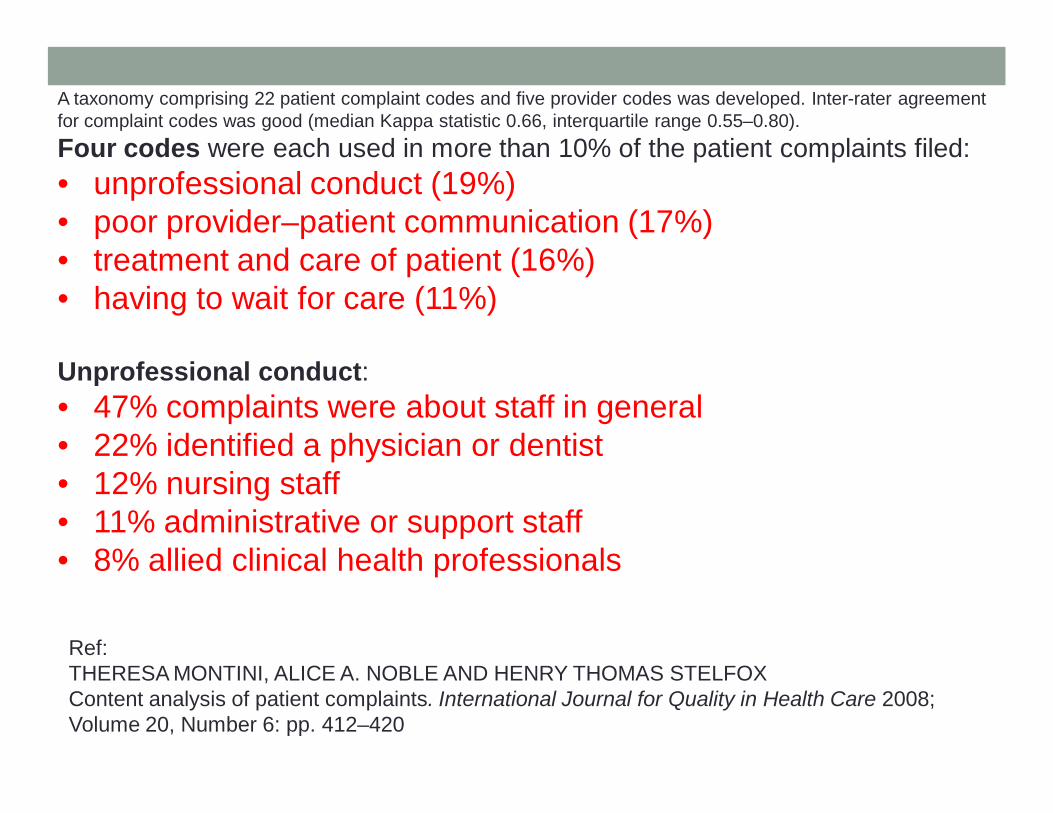
A taxonomy comprising 22 patient complaint codes and five provider codes was developed. Inter-rater agreement for complaint codes was good (median Kappa statistic 0.66, interquartile range 0.55–0.80). Four codes were each used in more than 10% of the patient complaints filed: • unprofessional conduct (19%)• poor provider–patient communication (17%)• treatment and care of patient (16%) • having to wait for care (11%)
Unprofessional conduct:• 47% complaints were about staff in general • 22% identified a physician or dentist • 12% nursing staff • 11% administrative or support staff • 8% allied clinical health professionals
Ref:THERESA MONTINI, ALICE A. NOBLE AND HENRY THOMAS STELFOXContent analysis of patient complaints. International Journal for Quality in Health Care 2008; Volume 20, Number 6: pp. 412–420

OCCUPATIONAL RISK IN HEALTHCARE
Employers
Health Risk Management• OSH-MS• Safety & Health Committee• Safety Officer• HIRARC Guidelines• Medical Surveillance• Ergonomic Redesign of Workplaces• Universal Precautions• Healthy Hospital Register• Health Promotion Activities & CME• Employee Assistance Program
• Workplace counseling• Workplace compensation

OCCUPATIONAL RISK IN HEALTHCARE
Conclusion
Conclusion• Managing occupational risk in healthcare depends on the
collective responsibility of management (employer) and healthcare workers (employees).
• Safety and Health Committee has the responsibility to ensure that OSH activities are diligently observed and in compliance with the prevailing OSH laws, regulations, guidelines and approved codes of practices.
• Health risk assessment activities must be carried out when there are changes to the work processes or when new technologies and procedures are adopted.
• Health risk management is aimed at ensuring that the workplace is safe and that each worker is fit for work.
• Employee assistance program is an important component of the OSH program.
THANK YOU