Embed Size (px)
Citation preview
Patient
quotes
introduc
ing each
chapter
are tak
en from
Occupa
tional T
herapy O
utcomes
: perspe
ctives of
patient
s with
advanced
cancer.
MSc diss
ertation
by Gail
Eva, Sc
hool of
Health C
are, Oxf
ord Broo
kes Univ
ersity, D
ecember
2001
For mor
e inform
ation ab
out HOP
E, go to
www.co
t.co.uk/
specialis
t/hope/i
ntro.htm
lRef
erencing
College
of Occup
ational
Therapi
sts, HOP
E The Sp
ecialist S
ection of
Occupa
tional T
herapists
in HIV/A
IDS,
Oncolog
y, Palliati
ve Care
and Edu
cation (2
004).
Occupa
tional th
erapy in
terventi
on in ca
ncer. Gu
idance f
or profe
ssionals
, manag
ers and
decision
-makers
. Londo
n. COT.
Members
of the B
ritish Ass
ociation
of Occup
ational
Therapi
sts: £15
.00Non
-Membe
rs of th
e British
Associa
tion of O
ccupatio
nal The
rapists:
£18.75
Publishe
d by the
College
of Occup
ational
Therapi
sts Ltd
106-114
Boroug
h High
Street
Southw
ark, Lon
don SE
11LB
Publishe
d April
2004
©Colleg
e of Occ
upation
al Thera
pists Ltd
ISBN 0-9
546491
-1-7Enq
uiries ab
out this
docume
nt shou
ld be ad
dressed
to:Coll
ege of O
ccupatio
nal The
rapists
Educatio
n and Pr
actice De
velopme
nt020
7357 64
80
Author
sEdit
or/writer
: Simon C
rompton
Working
party m
embers:
contribu
tors sho
wn abo
veFina
l editing
group:
Jo Bray,
Chair H
OPEJill C
ooper, T
reasurer
HOPE
Gail Eva
, Resear
ch Office
HOPE
Ann Ma
son, CO
T Libraria
nAck
nowledg
ements
This doc
ument w
as produ
ced by a
workin
g party
of HOPE
membe
rs and r
epresent
atives of
the
College
of Occup
ational
Therapi
sts, with
the inp
ut of a
number
of OT ex
perts in
the field
of cance
r and
palliativ
e care.
Ros Arth
ur, Maccl
esfield D
istrict Ge
neral Ho
spital
Ali Barcla
y, Weste
rn Gene
ral Hospi
tal, Edin
burgh
Sheila B
arnett, S
t James H
ospital,
Leeds
Ann Bos
tock, Qu
een Eliz
abeth T
he Quee
n Mothe
r Hos
pital , M
argate
Helen Bo
usie, Nig
htingale
Macmil
lan Unit
, Derby
Jo Bray,
TheRoy
al Marsd
en NHS F
oundati
on Trust
, Londo
nHea
ther Bro
wn, Ma
cmillan
Palliative
Care O
T,Manch
ester
Susie Ch
amberla
in, Velind
re Cance
r Centre
, Cardiff
Melanie
Chudle
y, Royal H
ull Hospi
tal Trust
Jill Coop
er, TheR
oyal Ma
rsden NH
S Found
ation Tr
ust, Lon
donPat
Davidso
n, Birmi
ngham
Heartlan
ds Hospi
talMar
y Deall, Q
ueen A
lexandra
Hospita
l, Herts
Julie Do
novan,
Whipps
Cross Ho
spital, Le
ytonston
eGail
Eva,Joh
n Radclif
fe Hospi
tal,Oxo
nCaro
line Evan
s, Penrith
and Com
munity H
ospital,
Cumbria
Charlie
Ewer-Sm
ith, The
Royal M
arsden N
HS Foun
dation
Trust, Lo
ndon
Debbie
Fletcher,
Bristol H
aematol
ogy & O
ncology
Centre
Jill Fulto
n, St Ge
mma's H
ospice,
Leeds
Kate Ge
m, Christ
ie Hospi
tal NHS T
rust, Ma
ncheste
rCaro
line Gilb
ert, Hea
ther Go
ld, The A
lexande
r Hos
pital, Ch
eshire
Mark Ha
ll, Denb
igh Clin
ic, Wales
Vicky He
ather, St
Catheri
ne's Ho
spice, C
rawley,
W Susse
xHele
ne Hibbe
rt
Emma Hi
cks, Roy
al Shrew
sbury Ho
spital, Sh
ropshire
Gail Ho
lloway, M
arie Cur
ie Centr
e, Edinb
urghRose
mary Hu
ghes, W
est Wales
General
Hospita
l, Carma
rthen
Janice J
ones, Su
e Ryder
Care Cen
tre, Leed
sAliso
n King,
Wakefie
ld Hospi
ce, W. Y
orksAnn
a Kittel,
Marie C
urie Cen
tre, Cate
rham, Su
rreyHaz
el Lake,
St Franc
is Hospi
ce, Rom
fordJack
ie Lunn,
Stafford
shireCaro
line Mat
hias, An
dover W
ar Memo
rial Hos
pital, Ha
ntsLind
a Middl
eton, Ed
ith Cavel
l Hospita
l, Cambr
idgeshire
Helen M
ussell, St
Michae
l's Hospi
ce, Here
fordAnn
Norris,
St Ann's
Hospic
e, Lanca
shireJenn
ie Pepp
er, Velind
re Cance
r Centre
, Cardiff
Margare
t Power
, Marie C
urie Cen
tre, New
castle
Linda Ro
gers, Ne
vill Hall H
ospital,
Abergav
enyJulie
Saarik,
St John's
Hospic
e, Donc
aster
Fiona Sh
eldon, S
alisbury
District
General
Hospita
lJane
t Stoneh
am, The
Rowans
Hospice
, Portsm
outhKare
n Taylor,
St Luke
's Hospi
ce, Plym
outhKath
y Thomp
son, Coo
kridge H
ospital,
Leeds
Carole T
hompson
, Hartlep
ool Gen
eral Ho
spital, Cl
eveland
Linda Th
ompson,
Marie C
urie Cen
tre, Birm
ingham
Helen Vo
ckins, Th
eRoyal M
arsden N
HS Foun
dation T
rust,
Surrey
Graham
Wilson,
St Barna
bas Hos
pice, Lin
coln
Workin
g Party
of HOPE
Membe
rsAll
the fol
lowing
are Stat
e Regist
ered Oc
cupatio
nal The
rapists
Occupa
tional t
herapy
interve
ntion in
cancer
Guidan
ce for p
rofessio
nals, ma
nagers
and dec
ision-m
akers
HOPE (th
e College
of Occup
ational
Therapi
sts’ Spe
cialist S
ection fo
rHIV/
AIDS, O
ncology
, Palliati
veCare
and Edu
cation)
Introduction 2Aims of the guidance 2Background 2The relevance of this guidance today 3Chapter 1About occupational therapy in oncology 4What is occupational therapy? 4How do occupational therapists work in oncology? 4Where do occupational therapists work in oncology? 5Chapter 2Using this guidance 6How the guidance is arranged 6What groups of patients and settings are covered? 6Expert testimony 7Other important information 7Chapter 3The guidelines 1 – General points for all interventions 8Chapter 4The guidelines 2 – Interventions for specific symptoms 11PAIN 11FATIGUE 12NAUSEA/VOMITING/SORE MOUTH/DYSPHAGIA 13CONSTIPATION/DIARRHOEA/URINARY PROBLEMS 14BREATHLESSNESS AND COUGH 14INSOMNIA 15TISSUE VIABILITY/SKIN INTEGRITY 16WEIGHT LOSS (ANOREXIA) 17NEUROLOGICAL PROBLEMS 18COGNITIVE DEFICITS 19ANXIETY AND DEPRESSION 20FLUID RETENTION (LYMPHOEDEMA, OEDEMA, ASCITES) 21BODY IMAGE (INCLUDING HAIR LOSS, SURGERY, LYMPHOEDEMA etc) 21BONE METASTASES 22Appendices 23References 23
1
ContentsContents
Introduction
2
Aims of the guidance What is the contribution of occupational therapyin the care of people with cancer? That is thesimple question this document aims to answer.It is guidance in its loosest sense – not a set ofstrict guidelines that occupational therapists orthose who commission their services mustfollow. The document is a general description ofwhat occupational therapists can and doaccomplish for people with cancer, designed toguide and support those who are involved withcommissioning or providing cancer services.The publication aims to demonstrate thepotential of occupational therapy, using as itsbasis the expert consensus of the professionsupported by references to literaturedocumenting the occupational therapycontribution. It is targeted at cancer networkmanagers and tumour groups, with the aim ofimproving appropriate referral and encouragingbest practice, and at occupational therapistsand their teams.
BackgroundThe publication has been produced by HOPE –the occupational therapy specialist section forHIV/AIDS, Oncology, Palliative Care andEducation. HOPE is affiliated to the College ofOccupational Therapists.Occupational therapists and other rehabilitationprofessionals have long been aware of the
contribution they can make to helping peoplewith cancer live fulfilled lives, but until recentlytheir role has not been widely appreciated.However, since the publication of the CalmanHine report in 19951 and the ensuingimplementation of a national Cancer Plan2,there has been a growing awareness amongother professions of the importance ofrehabilitation in the care of people with cancer. The change has not been solely due tocentralised moves to improve cancer services inthe UK. Over the past two decades, theimplementation of the Disability DiscriminationAct (1995), the increasing currency of socialmodels as opposed to medical models ofdisability, and the increasing strength andinfluence of the hospice movement have madeall the more apparent the importance of healthprofessionals whose first priority is improvingquality of life. Current moves towardscommunity-based care, and reducing hospitaladmission times, has further reinforced thevalue of occupational therapy.In the field of palliative care, there has been agradual and vital realisation that rehabilitation does not simply mean getting peoplefunctioning independently again. It meansaffirming peoples’ lives – no matter what stageof illness they are at – by providing them withphysical, social and emotional opportunities,and a sense of control. This found expression inthe National Council for Hospice and SpecialistPalliative Care Services document “Fulfillinglives”3. Cancer services, however, have beenslower in understanding the full potential ofrehabilitation services. In 2002, the NHS Modernisation Agencytestified to the role of occupational therapy inthe critical care setting4. In its report on the roleof allied health professions in critical care it saidthat critical care was all too often seen only as
Introduction“I need to be independent. That’s themain thing. I haven’t got to have someonecome in and wash me and things like that.I can still do that for myself.”
1 Calman K, Hine D (1995) A policy framework for commissioning cancer services. London: Department of Health2 Department of Health (2001) The NHS Cancer Plan: a plan for investment, a plan for reform. London: Department of Health3 National Council for Hospice and Specialist Palliative Care Services (2000) Fulfilling lives: rehabilitation in palliative care. London: NCHSPCS4 NHS Modernisation Agency AHP and HCS Advisory Group (2002) The role of healthcare professions within critical care services. London: Department of Health
the act of saving life, and therefore the role ofoccupational therapists could be overlooked.“The lack of recognition of the role in criticalcare makes it difficult to access resourcesappropriate to meet the needs of the patient,”it said. It was against this background thatHOPE began to plan this document – tocapitalise on the momentum and pin downand publicise the exact contribution ofoccupational therapy in the field of cancer andpalliative care. The organisation originallyenvisaged publishing a series of documents,each looking at particular types of cancer,beginning with breast cancer and lung cancer.It compiled information from specialistpractitioners and literature to form an expertconsensus. The practitioners contributed theirthoughts at three workshops, and the Collegeof Occupational Therapists contributed areview of relevant literature. Forty sevenspecialist occupational therapy practitionershave helped develop this document.So many common elements emerged for bothbreast and lung cancer, that it was decided thatthere should be this one core document for allcancers, and then additional accompanyingsheets that could spell out some of thespecialist issues for occupational therapy andparticular cancers.
The relevance of this guidance todayThis HOPE and College of OccupationalTherapists guidance comes at a particularlyimportant time. The contribution ofoccupational therapy (OT) is not alwaysunderstood by managers and policy makers,and there is evidence that current standards ofprovision are variable. A HOPE questionnaire ofpalliative care providers in 2001 showed thatonly 14% of services employed more than one
3
Occupational therapy intervention in cancer
5 Bray J (2001) HOPE survey of occupational therapy services among palliative care providers. Conference paper for the Help the Hospices conference, London6 Guidance on Cancer Services: Improving Supportive and Palliative Care for Adults with Cancer: NICE 20047 Due to be published during 2004
Occupational therapy intervention in cancer
full-time occupational therapist5. The averagenumber of OT hours per palliative care serviceranged between 0 and 98, with the averagesize of a palliative care unit being 12 beds, plushome care services for patients in thecommunity.This cannot continue. The provision of qualityrehabilitation for people with cancer hasbecome a matter of national priority. TheNational Institute for Clinical Excellence (NICE)has issued new service guidance, “Supportiveand Palliative Care Services”6, intended mainlyfor those who commission cancer services. Thisspells out the requirement for consistent andquality rehabilitation services in oncology andpalliative care across cancer networks. It meansthat occupational therapists will have to co-ordinate and communicate across serviceboundaries to improve patient care.Underpinning this is the Department ofHealth’s first Allied Health Professions CancerStrategy for England and Wales (2004)7. Thisvital document sets out what will be needed todeliver the standards defined in the NICEguidance. For the first time, the role ofoccupational therapy is being set in cancerstandards, and services will have to bedeveloped to fulfil the requirements of policy. At the same time, many commissioners,particularly Primary Care Trusts need good,concise information to guide them in decision-making. They need to know, more than ever,the value they are getting for their money.And, with the advent of Patient Choice, theyneed to be able to demonstrate to patients thequality of treatment options that are availableto them. This guidance aims to provide them with thatinformation.
What is occupational therapy?An occupational therapist uses specific activities to limit the effects of disability and promoteindependence in all aspects of daily life8.Occupational therapy has recently been definedby the College of Occupational Therapists asfollows:“Occupational therapy focuses on the nature,balance, pattern and context of occupationsand activities in the lives of individuals, familygroups and communities. It is concerned withthe meaning and purpose that people place onoccupations and activities and with the impactof illness, disability or social or economicdeprivation on their ability to carry them out.“The main aim of occupational therapy is tomaintain, restore, or create a match, beneficialto the individual, between the abilities of the
person, the demands of her/ his occupationsand the demands of the environment, in orderto maintain or improve the client’s functionalstatus and access to opportunities forparticipation.“Occupational therapy personnel work with people of all ages, with physical, mental andsocial impairments and learning disabilities.They work with people who have multiple andcomplex problems, people with minor copingdifficulties and those who are functioning welland wish to maintain and promote their well-being.”9
How do occupationaltherapists work in oncology?Some occupational therapists are part ofspecialist teams working in cancer centres,cancer units, on general medical units and inthe community. Others work in the field ofpalliative care – that is, the active total care ofpeople whose cancer does not respond tocurative treatment. Like other rehabilitation professionals,occupational therapists aim to improve qualityof life, so that peoples’ lives will be ascomfortable and productive as possible andthey can live as independently as possible. Thisapplies even if life expectancy is short. Becausepeople with cancer can experience very rapidchanges in their illness and care setting,occupational therapists working with thesepeople need to be particularly responsive tochanging need. They respond quickly and plan
4
Chapter 1Chapter 1About occupational therapy in oncology“The occupational therapist encouragedme to do things I wouldn’t have done on my own. So you don’t just sit there andthink ‘I can’t do anything’. It’s making youfeel more the whole person instead ofthinking about your…the tumour. Do youknow what I mean? It enriches your life.”
8 Health Professions Council www.hpc-uk.org/professions/ot.htm9 Creek J (2003) Occupational therapy defined as a complex intervention. London: College of Occupational Therapists
5
Occupational therapy intervention in cancer
10 Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP (1982) Toxicity And Response Criteria Of The EasternCooperative Oncology Group. American Journal of Clinical Oncology 5: 649-655 11 From Interface to Integration: a strategy for modernising occupational therapy services in local health and social care communities.London, College of Occupational Therapists, 2002
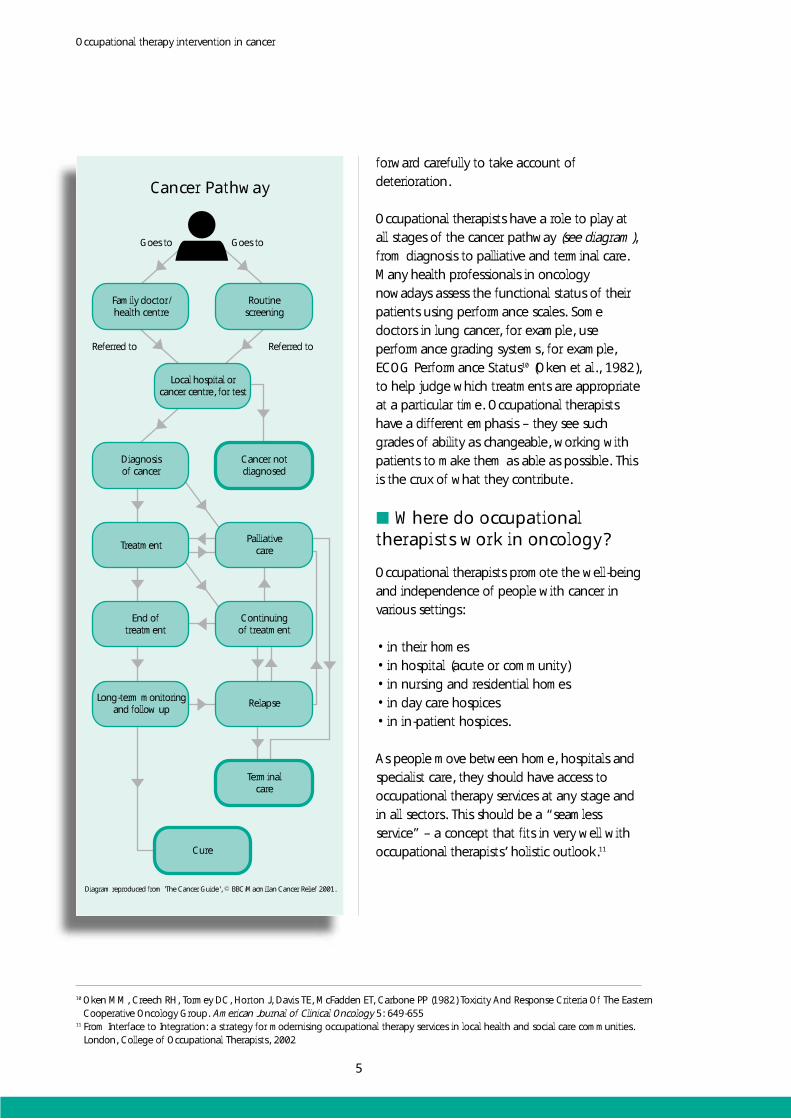
Cancer Pathway
Long-term monitoringand follow up
End oftreatment
Treatment
Diagnosisof cancer
Family doctor/health centre
Cure
Terminalcare
Relapse
Continuingof treatment
Palliativecare
Cancer notdiagnosed
Local hospital orcancer centre, for test
Routinescreening
Goes to
Referred to Referred to
Goes to
Diagram reproduced from 'The Cancer Guide', © BBC/Macmillan Cancer Relief 2001.
forward carefully to take account ofdeterioration.Occupational therapists have a role to play at all stages of the cancer pathway (see diagram),from diagnosis to palliative and terminal care.Many health professionals in oncologynowadays assess the functional status of theirpatients using performance scales. Somedoctors in lung cancer, for example, useperformance grading systems, for example,ECOG Performance Status10 (Oken et al., 1982),to help judge which treatments are appropriateat a particular time. Occupational therapistshave a different emphasis – they see suchgrades of ability as changeable, working withpatients to make them as able as possible. Thisis the crux of what they contribute.
Where do occupationaltherapists work in oncology?Occupational therapists promote the well-being and independence of people with cancer in various settings:• in their homes• in hospital (acute or community)• in nursing and residential homes• in day care hospices• in in-patient hospices.As people move between home, hospitals andspecialist care, they should have access tooccupational therapy services at any stage andin all sectors. This should be a “seamlessservice” – a concept that fits in very well withoccupational therapists’ holistic outlook.11
How the guidance is arrangedThe following chapter (chapter 3) presents anoverview of occupational therapy interventionsfor people with cancer – looking at the keyprinciples of occupational therapy that areapplied whatever the symptom, whatever thesetting.Then the bulk of this publication (chapter 4) isguidance on what occupational therapy can do for specific symptoms associated with cancer. There are many possible ways of documentingthe occupational therapy contribution in thisfield. An alternative arrangement would havebeen to explain occupational therapy coreskills, and then provide a list of how they canbe applied in caring for people with cancer.However, this would take occupational therapyas the starting point, not the person withcancer. This document aims to demonstratehow occupational therapists respond to real patient needs – symptoms in theirloosest but most real sense.
This inevitably means there will be someoverlap and repetition in the lists of whatoccupational therapists can contribute. Manyof the occupational therapy interventions for,say breathlessness, will be very similar to thosefor fatigue. Indeed, it is in some ways artificialto itemise all the symptoms separately anyway,because people with cancer don’t just haveone symptom – they have many. The way anoccupational therapist responds will depend onthe complex interplay of symptoms and howthey affect a person’s quality of life. However, the guidance is arranged like this foreasy reference – to demonstrate at a glancethe difference occupational therapists canmake to a wide range of conditions andpeople.HOPE is also publishing a series of informationsheets dealing with particular cancers – looking at the policy context, any specific clinical issues that arise for that type of cancer, and therelative importance and interplay of symptomsthat may be particularly important. Fact sheetson breast and lung cancer are inserted into theflap at the back of this publication andadditional sheets can be found at the HOPEwebsite.
What groups of patients and settings are covered?This main document covers people with alltypes of cancer, and on all parts of the cancerpathway from diagnosis onwards – treatment,end of treatment, long-term monitoring and
6
Chapter 2Chapter 2Using this guidance“It makes me feel good that I actually feelI’ve achieved something. You know, justbecause you’ve got an illness doesn’tmean to say we’re confined to, say, sittingand reading a book. I like to be able touse my hands as much as I can.”

follow up, relapse, continuing treatment, cure,palliative care and terminal care. It also coversall settings in which occupational therapistswork – in hospitals, hospices, nursing andresidential homes, and people’s own homes.The additional HOPE information sheets dealingwith occupational therapy and specific cancersare obviously more focussed.
Expert testimonyThroughout the following sections, smallextracts from the literature accompany theaccounts of the OT contribution to differentsymptoms. These are included to providefurther expert backing to the points beingmade. They are usually not exact quotationsfrom the articles, but provide a summary of thepertinent points made in the article. The fullreferences for the articles quoted are providedin the appendix at the back of this document.
Other important informationOne thing has to be made explicit about thisguidance. An occupational therapist will not doanything unless it is with the person withcancer’s full agreement. It is easy to create theimpression in guidance such as this thatoccupational therapy has a set agenda – a listof things they expect to do, and to which theperson with cancer somehow is expected toconform. Nothing could be further from thetruth. An occupational therapist’s starting pointis always the experiences of the people theyare working with – the person with cancer andtheir family/carers – and their choices andpriorities drive any interventions that takeplace. Occupational therapists work inpartnership with people with cancer, and helpthem find new options to improve the qualityof their lives.
7
Occupational therapy intervention in cancer
At its simplest, the key outcome ofoccupational therapy intervention is quality oflife. For many people with cancer helped byoccupational therapists, one of the mostimportant means to achieving this will beindependence. However, for people who arereceiving palliative care, this may not always bethe first priority. Quality of life may have far moreto do with affirming life – providing peoplewith physical, social and emotional opportunity,and a sense of control in their own lives. To achieve these objectives, occupationaltherapists apply their core skills to allinterventions. This applies as much to cancer asany other condition. They use these skills toempower people to make choices, achieve apersonally acceptable lifestyle, and maximisehealth.These skills are:• Enabling people to maximise their physical,emotional, cognitive, social and functionalpotential
• Anticipating the effects of disability througheducation and therapeutic intervention• Enabling people to achieve a quality of life by preparing them for a return to work, or developing opportunities in leisure, education, training and voluntary work• Advocating for people on access matters• Providing practical advice and support for families and carers• Changing their input as the needs of people change• Forming partnerships with others to developservices for people.12
Occupational therapists’ starting point willalways be the choices and priorities of theperson with cancer. This will guide allinterventions and decisions.Occupational therapists are quite systematicabout the way they apply these core skills. Thenext chapter illustrates the way they can applythem to help specific symptoms, but it is worthnoting here the process they invariably use inaddressing all these problems. They will workthrough the following sequence13:1. Information gathering2. Initial assessment3. Identifying abilities and needs4. Goal setting5. Action planning6. Action 7. Ongoing assessment 8. Revision of action9. Outcome measurement10.Discharge/end of intervention11.Review
8
Chapter 3Chapter 3The guidelines 1 – General points for all interventions“It’s their encouragement to try things.Otherwise I’d have been so depressed,because I can’t use this hand. Even thoughI can’t do all of it in the way I used to, it’sstill very satisfying. It’s started me offagain, doing things at home. I wasfeeling so frustrated before.”
12 Adapted from Core Skills and a Conceptual Framework for Practice, a College of Occupational Therapists position statement, 199413 Adapted from Occupational Therapy Defined as a Complex Intervention, College of Occupational Therapists, April 2003
In all interventions with people with cancer,occupational therapists will need to planahead, and anticipate the possibility of changesin the person’s condition or circumstances.Sometimes change or deterioration can happenquickly or unexpectedly, and occupationaltherapists will need to be able to react to that.Continuous review is essential to ensure thatthe occupational therapist is still workingtowards the priorities of the individual, andthat priorities are still realistic and achievable. There are other common threads that arewoven throughout occupational therapists’work with people with cancer. Here are threethemes of special relevance, which will befound throughout the succeeding chapterabout how occupational therapists approachspecific symptoms.Lifestyle managementThe occupational therapist can: • work with people with cancer and family/carers to achieve balance in life • help them assess what priorities are mostimportant to them – including social and spiritual priorities• help them find occupation which is meaningful to them• take into account the influences of culture • provide a crucial link between care inhospital and living at home.Fatigue managementThe occupational therapist can: • recognise that fatigue affects people’s ability to function and be independent• provide information and advice to peoplewith cancer and family/carers aboutstrategies to manage their fatigue andconserve energy • help them understand the need to adjust tochange, and accept some dependency andfluctuation
• help them establish realistic expectations and goals• use reduced energy levels as an opportunity for the person to establish what is important to them, and what their priorities should be• help them adapt their lifestyle to meet theirchanged energy levels, providing equipmentand adapting the environment wherenecessary.Self-esteemThe occupational therapist can: • recognise that a person’s inner feeling of self-worth influences their motivation• recognise that involvement in purposeful activity affects feelings of self-worth• help people explore their feelings, recognise who they are and what is important to them• help people acknowledge their values, andtheir role within their family and thecommunity• help them adapt to these roles changing • help them reflect on their current and pastachievements to underpin self-worth.One further point is worth noting. On a totallypragmatic level, all occupational therapyinterventions, by virtue of aspiring to makepeople more independent, have the potentialto bring cost benefits to the NHS and voluntarysector. • By providing preventative advice andtreatment they can head off complicationswhich are likely to require further referralsand admissions• By helping make people more physicallycompetent, they can reduce use of Accidentand Emergency services – for example, byhelping someone with lymphoedema takemeasures to protect their limbs from injury,or by teaching someone with breathingdifficulties how to cope with panic attacks.
9
Occupational therapy intervention in cancer
Occupational therapists improve thequality of survival of people with cancer,so that during the period of survival theywill be able to lead as independent andproductive lives as possible at a minimumlevel of dependency, regardless of lifeexpectancy. (Dietz, 1981) Researchers and clinicians should give asmuch attention to the development andmaintenance of psychological well-being inthe face of serious illness as they do to theaetiology and treatment of psychiatricsymptoms. (Folkman and Greer, 2000)Client-centred practice is an approach toproviding occupational therapy whichembraces a philosophy of respect for, andpartnership with, people receiving services.(Law et al., 1995)In working with people who are terminallyill, occupational therapists value anindividual’s remaining life, help a client livein the present, recognise an individual’sright to self-determination, andacknowledge and prepare for theapproaching death. (Bye, 1998)Occupational therapy intervention at thesupportive and palliative care stagescentres around improving quality of lifethrough the remediation of occupationalrole dysfunction. Engagement inmeaningful activities, be they craft,recreation or work-related, assist inimproving self-concept and attain taskmastery. The occupational therapist is ableto use the developing therapeuticrelationship to assist the person withcancer and his or her family to adjust torole changes. (Strong, 1987)
In terminal illness, the person’s physicaland social environment must be adaptedaccording to changing abilities, needs andchoices. One of the dominant roles of theoccupational therapist is to help theperson maintain independence andintegrity and some control of theenvironment.(American Occupational Therapy Association, 1986)Occupational therapists have a unique role in maintaining and increasingindependence. Occupational therapistsalso help people gain greater autonomyand control of their environment throughthe provision of aids and therapeuticgroups. (Dawson, 1982)Occupational therapists have skills incontinuous assessment and evaluation.They can be flexible in changing treatmentand goals to ensure meaningful life.(Flanigan, 1982)An individual can benefit fromoccupational therapy intervention at anystage of an illness, from primary diagnosis,through attempts at curative treatment, topalliation and finally terminal illness.(Penfold, 1996)People with fears about functional decline can be helped with therapeutic goals andrehabilitation throughout the trajectory ofmalignant disease. Occupational therapyallows people to execute the fine motortasks required for self-care, and restoresautonomy at home. (Cheville, 2001)
10
Occupational therapy intervention in cancer
11
This chapter, the heart of these guidelines,itemises the contribution of occupationaltherapy (OT) in helping people with specificsymptoms. The division between differentsymptoms is designed to provide easyreference, but it is also to some extent artificial.People with cancer experience a range ofsymptoms, often simultaneously. While usingthis chapter, it is worth bearing in mind that asurvey of hospital and hospices found that onaverage, people were suffering from sevensymptoms at the same time14. The 12 mostcommon symptoms, in descending order offrequency, were weakness, dry mouth,anorexia, depression, insomnia, pain, swollenlegs, nausea, constipation, vomiting, confusionand dyspnoea.The symptoms itemised in this chapter arethose most commonly encountered byoccupational therapists in their work withpeople with cancer. They are (listed inapproximate order of how commonlyencountered):• Pain• Fatigue• Nausea / vomiting / sore mouth / dysphagia• Constipation / diarrhoea / urinary problems• Breathlessness and cough• Insomnia• Tissue viability / skin integrity (pressureproblems)• Weight loss (anorexia)• Neurological problems• Cognitive deficits• Anxiety and depression
• Fluid retention (lymphoedema, oedema,ascites)• Body image (including hair loss, surgery,lymphoedema).Pain
Pain may affect a person’s ability to care forthemselves, to work or to participate infulfilling activities. This may cause emotionaldistress to both the person with cancer andtheir family/carers, affecting their wellbeing andrelationships. The main treatments for pain arepharmacological, but OTs have an importantrole in helping people cope with the impact ofpain, and addressing some of its emotionalaspects.The occupational therapist can:• Assess the impact of pain on self-care, work,leisure activities and social roles• Analyse problems and solutions
Chapter 4Chapter 4The guidelines 2 – Interventions for specific symptoms
“When you’ve got cancer, there’s anawful side to it that’s like a downhillslope. You know, people are very ill, andit can be very depressing. The physio andoccupational therapy side of it is a bitmore go for it – you know, get out thereand do it.”
14 Dunlop GM (1989) A study of the relative frequency and importance of gastrointestinal symptoms and weakness in patients with faradvanced cancer. Palliative Medicine 4: 37-43. Cited in Kaye P (1994) A to Z of Hospice and Palliative Medicine. London: EPL Publications
12
FATIGUEFatigue can have a devastating effect onpeople’s ability to maintain normality in theirlives. It can:• Affect a person’s ability to carry out normalactivities of daily living, self-care and leisure• Cause emotional and physical distress to theperson and family/carers• Reduce cognitive ability• Affect psychological wellbeing• Affect relationships.The occupational therapist can:• Identify with the person the factors affectingfatigue• Assess self-care, work, leisure activities androles• Work with the person and family/carers toadapt and practise self-care, work andleisure activities within the person’sfunctional abilities• Work with the person to identify their goalsand priorities• Educate the person and family/carersregarding pacing, planning, balancing andprioritising activities, and energyconservation techniques• Liaise with community and support services • Teach relaxation techniques • Teach assertiveness techniques to avoidovertiredness• Assess whether equipment andenvironmental adaptation are required tosuit the person’s needs (for example,wheelchairs and bath aids).This aims to:• Promote psychological wellbeing andadjustment
• Work with the person and family/carers toadapt and practise self-care, work, leisureactivities and social roles within the person’sfunctional abilities and pain parameters• Work with the person to identify goals and priorities• Collaborate with the person about lifestylemanagement, including pacing, planningand prioritising, anxiety management,relaxation skills, ergonomics, fatiguemanagement and working within paintolerance• Assess whether equipment andenvironmental adaptation are needed tomeet the person’s needs • Liaise with the multiprofessional team toensure optimum pain management• Provide regular review to assess changes incondition and function.This aims to:• Increase the individual’s control over theirpain• Maximise independence• Promote psychological wellbeing andadjustment• Maintain the individual’s activities and roles• Support family and carers • Facilitate close liaison within the multiprofessional team• Improve quality of life.
Successful pain management can beachieved through coordinated efforts ofteam members of the cancer care team.Occupational therapy is vital to the painmanagement service and can help modifyperceptions of pain and individuals’lifestyles. (Lloyd and Coggles, 1988)
13
Occupational therapy intervention in cancer
• Improve quality of life • Maximise independence• Increase the person’s control over theirfatigue• Maintain the person’s activities and roles• Facilitate close liaison with themultiprofessional team• Allow the person and their family/carers tounderstand the effects of fatigue• Support family and carers • Enhance understanding of symptoms andreduce friction in relationships. Occupational therapy has a role ineducating both patient and carers aboutenergy conservation, lifestyle changes,leisure activities, and alternative means ofcarrying out activities of daily living.(Lloyd and Coggles, 1988)The patient with a deteriorating conditionneeds to exercise control and findmeaning in life. He or she should beencouraged to conserve energy foractivities that are important to him/her inthe areas of self-care and leisure.(Holland, 1984)Pre-existing mobility problems place cancerpatients at high risk from fatigue andweakness. Weakness is a serious safetyconcern and may have impact on ability toperform at work and home. Patients needinformation, and to plan day to dayactivities and set priorities for energy use.Occupational therapists can also help withmobility and safety aids, environmentalmodifications and finding appropriateways to perform tasks. (Nail and Winningham, 1995)
NAUSEA/VOMITING/SOREMOUTH/DYSPHAGIAThese symptoms have many social, emotionaland physical effects. They will:• Cause eating, drinking and digestivedisturbances• Affect meal and drink preparation• Reduce the social aspect of eating meals andinvolvement in family life• Disturb daily routine and sleep patterns• Alter roles in the home.The occupational therapist can: • Address the difficulties of meal/drinkpreparation and explore alternatives (forexample, using ready meals to avoid longcooking times and cooking smells)• Advise on seating and positioning fordysphagia• Advise on the practical implications of thesymptoms (for example, on laundry andhygiene)• Teach relaxation techniques to help reducenausea and vomiting• Liaise with the multiprofessional team aboutmouth care • Provide education and support to help withthe psychological aspects of these symptoms• Increase the understanding of family/carers,who may find it hard to have normalfeeding routines disturbed.This aims to:• Reduce nausea and vomiting • Reduce anxiety levels associated with foodand meal times• Facilitate improved relationships and reducestress regarding meal preparation and lack ofconsumption/reduced dietary intake.
Interviews with working women with breastcancer reveal the importance of establishinga daily occupational routine includinghousehold chores such as preparing meals.Resuming their daily occupational routineserves as a source of satisfaction and asource of motivation that distracts themfrom the anxiety associated with their lives.In a clinical situation, occupationaltherapists and their clients work together todevelop goals and plan interventionstrategies to facilitate the clientsparticipation in meaningful occupation.(Vrkljan and Miller-Polgar, 2001)
CONSTIPATION/DIARRHOEA/URINARY PROBLEMSThese symptoms will cause social isolation,distress, dressing problems, hygiene difficulties,fatigue, psychological problems. Treatmentssuch as radiotherapy can cause severediarrhoea.The occupational therapist can: • Assess the person’s ability to access toiletfacilities, looking at appropriate equipment,transfer, practice etc • Assess and adapt the environment asappropriate, addressing issues of hygieneand the problems of fatigue that mayaccompany frequent toilet visits • Advise about appropriate clothing • Investigate domestic facilities and ensurethey are adequate to manage laundry andhygiene, and refer for financial assistance toobtain bathroom adaptation or washingequipment if appropriate • Liaise with the multiprofessional team,including a continence advisor, about causes,contributing factors, possible treatment andmanagement
• Give advice about community facilities, suchas the RADAR toilet scheme, Shopmobilityetc, to promote engagement and increaseconfidence in the person’s normal socialactivities.This aims to:• Increase independence in going to the toilet• Increase the confidence of the person andtheir family/carers about managing toiletingproblems• Decrease anxiety and stress• Increase confidence in resuming socialactivities.
The community occupational therapist hasan important role in relation to theprovision of equipment, adaptations andadvice regarding home care, and the needfor skilled assessment.(Pushpangadan and Burns, 1996)
BREATHLESSNESS AND COUGHLike fatigue, breathlessness (dyspnoea) andcontinued coughing can affect a person’sproductivity and ability to participate in self-care and leisure. It can cause emotional andphysical distress to the person and family/carersand affect relationships.An occupational therapist can:• Assess how shortness of breath is affecting aperson’s activity • Assess and analyse activities, daily living, theenvironment, mobility needs, positioning inbed and seating• Examine solutions• Provide advice on communicating effectively,for example by writing• Advise on lifestyle management, and pacingactivity
14
• Advise on anxiety management and energyconservation• Teach coping mechanisms and relaxationexercises for episodes of breathlessness• Provide new equipment, and adaptequipment, such as wheelchairs • Advise family and carers on handling theperson and equipment.This aims to:• Improve the person’s quality of life• Improve independence and ability• Improve confidence and control• Reduce the need for medication anddependence on bottled oxygen• Reduce fear and anxiety• Reduce psychological dependency onfamily/carers and others.
Patients with respiratory distress tend toexperience high levels of anxiety. The teamapproach helps patients maintain as muchcontrol over their environment as possible.Occupational therapy has a role in thisteam helping the patient maintain a senseof control, encouraging coping, increasingengagement in meaningful leisure pursuitsand providing with exercise programmes.(Centers, 2001)Patients’ and carers’ understanding aboutbreathlessness, anxiety and depressionneeds to be addressed. Patients needpersonal goals and can be taughtbreathing control techniques, copingstrategies and energy conservationtechniques. (Corner, 1997)
A multiprofessional breathlessness clinicoffers sessions run by a physiotherapist,occupational therapist and nursepractitioner. The occupational therapistfocuses on energy conservation and givesa clear description of the aims oftreatment and the techniques taught.(Stent, 2001)Multi-dimensional assessment is necessary.Some symptoms respond topharmacological interventions, others arebetter managed by expressive/supportivecounselling, occupational therapy andphysiotherapy. The intensity of dyspnoeasignificantly correlates with anxiety.Education of patients and families isrequired so that they can anticipateepisodes of increased dyspnoea.(Roberts, 1999)INSOMNIA
Poor sleep quality can cause great distress andfatigue to the person with cancer, worseningtheir symptoms and exhausting family andcarers. Some people with cancer choose tosleep upright in a chair, because breathing isharder when they lie down. Others may havedisturbed sleep patterns because they napduring the day. A good night’s sleep can bringcomfort to the person with cancer and theirfamily/carers.An occupational therapist can:• Examine daily routines and assist withlifestyle management• Ensure the person is active throughout the day• Assist with posture and positioning• Assist with mobility and transfers• Provide advice and equipment enabling bedmobility and transfers• Teach relaxation techniques
15
Occupational therapy intervention in cancer
16
• Provide family and carers with advice aboutencouraging good sleep, and getting sleepthemselves• Address environmental problems that maybe preventing sleep.This aims to:• Improve quality of life• Lower anxiety• Increase productivity• Reduce the risk of falling, which can becaused by night wandering or sleepdeprivation• Reduce feelings of depression and low self-esteem (which is linked to sleep deprivation).
Because hypnotic medications can haverisks such as dependence, psychologicinterventions such as stimulus control andcognitive therapy are the treatment ofchoice for sleep disturbances in thetreatment of cancer.(Sarvard and Morin, 2001)Occupational therapy as a holisticdiscipline confronts the debility of clientswith the belief that doing must bepurposeful and have meaning, therebyengaging the mind and spirit.(Brindle, 1999)TISSUE VIABILITY/SKIN INTEGRITY
People with cancer can remain immobile forlong periods. This can cause the skin to breakdown, which in turn causes discomfort in lyingand sitting. Some cancer treatments can alsomake the skin more vulnerable to breakdown.
Occupational therapists have a role in bothpreventing the problems associated withpressure to the skin, and helping the personengage in activities when they have pressureproblems. An occupational therapist can:• Assess the risk of pressure problems, orassess current pressure problems• Assess the person’s pressure care needs inrelation to their activity • Liaise with other members of the team onhow to manage pressure problems,examining issues such as wound care,medicines and nutrition• Provide advice on posture, pressure relief,and appropriate seating• Assist with bed mobility and transfers• Advise on lifestyle management, for example pacing activities, posture, sittingposition• Advise on finding appropriate clothing andwhere to find it.This aims to:• Prevent pressure ulcers• Maintain independence• Improve quality of life, and lessen emotionaldistress, for the person and their family/carers• Relieve pain and improve comfort• Lessen the burden on family and carers, byreducing laundry, the need for manualhandling, and the need for homeintervention by outside agencies • Allow the person to take part in desiredactivities• Reduce the professional cost associated withtreating pressure ulcers.
17
Occupational therapy intervention in cancer
• Assess and address issues surrounding bodyimage and self-esteem• Assess and address associated problems offatigue, weakness and pressure (see earliersections)• Provide equipment and feeding aids whererequired• Liaise with doctors and dieticians about thebest ways to help the person and theirfamily/carers.This aims to:• Support the person and family/carers byproviding practical strategies• Improve quality of life and independence • Raise self-esteem• Help reduce anxiety to the person andfamily/carers who prepare food.
Occupational therapy has a role ineducating patient and family/carers,energy conservation, lifestyle change, self-image, leisure activities, self-maintenance,home and community management.(Lloyd and Coggles, 1988)Three working women with breast cancerwere interviewed about the importance ofestablishing everyday routines during andafter treatment. Establishing a dailyoccupational routine, including visitingfriends and performing household choressuch as preparing meals, became vitallyimportant. (Vrkljan and Miller-Polgar, 2001)
Occupational therapists can and do makea positive contribution to patient care, inproviding carer support and equipment,symptomatic treatment for physicalmanifestations such as oedema and pain,and contributions to day careprogrammes. Prevention of pressure ulcersand hospital falls are examples of adverseoutcomes relevant to occupationaltherapists. (Brandis, 2000)Occupational therapy goals includeachieving independence in self-care,functional transfers, independent livingskills, maintaining skin integrity, andincreasing independence as progress ismade. Meal preparation, cleaning, laundry,energy conservation and worksimplification may also be necessary.(Tuel et al., 1992)
WEIGHT LOSS (ANOREXIA)Weight loss occurs in about 70% of peoplewith advanced cancer, most commonly withlung, gut and ovary tumours. It sometimesoccurs despite a reasonable food intake.People’s previous eating routine may not fit inwith their illness, or their illness may makeindependent eating difficult. Weight loss leadsto associated problems of fatigue, weaknessand reduced mobility, and reduces people’sability to perform daily living activities.An occupational therapist can:• Assess and address issues surroundingmeals, their timing and preparation
18
NEUROLOGICAL PROBLEMSCerebral metastases can cause difficultymanaging daily living activities andoccupations. There will be deterioration and/orfluctuations in people’s ability to performactivities such as washing, dressing, feedingand going to the toilet, and this causes aparticular burden for family and carers.Tumours affecting the spinal cord cause a widerange of symptoms. The person may experience weakness orparalysis, changes in function, vertigo, sensorydeficits, frustration, shock, anger, anxiety, pain,fatigue, depression, balance problems. Nervedamage (neuropathy) can cause similarproblems. (See also cognitive deficits below)An occupational therapist can:• Assess and analyse risks to the person’ssafety• Assess and analyse how well the personperforms Activities of Daily Living (ADL) andleisure activities• Help the person find ways to perform ADL,leisure activities and maximise independence• Assess the person’s environment and adapt itto suit their needs safely• Provide rehabilitation• Provide wheelchairs and seating• Provide positioning advice and pressure care• Provide advice on manual handling, transfersand mobility• Provide assistive aids and equipment• Provide lifestyle advice and teach adaptivetechniques• Provide advice, education and support tofamily and carers
• Provide regular review to take into accountfluctuations in the person’s condition, and tohelp the person cope with deterioration• Help communication between the person,family, carers and professionals through jointsessions• Help people and their family/carers adjustand set realistic goals• Provide splinting for hands withneuropathies.This aims to:• Maintain the person’s safety• Maximise the person’s independence andquality of life• Maintain the person’s previous lifestyle• Maintain the person at home for longerperiods• Facilitate discharge, reduce the likelihood ofhospital re-admission • Reduce the risk of complications such aspressure ulcers, poor posture, falls etc • Reduce care costs associated withcomplications• Help the person and family/carers cope toadapt, and cope with possible deterioration.
Occupational therapy is an integral part ofcare plan for patients with metastaticdisease. Interventions include daily livingskills, adjustment to disability, energyconservation, adapting environment. Thefunctional perspective of the OT can beeasily distinguished from the framework ofother professions. In a chronic disease likemetastatic cancer, the OT perspectivebroadens the focus of care.(Romsaas and Rosa, 1985)
19
Occupational therapy intervention in cancer
Cancer diagnosis and treatment can haveprofound effect upon hand function,presenting a challenge to occupationaltherapists who specialise in oncology or handtherapy. Return or improvement of handfunction is common after cancer treatment,meaning that restorative treatment goals inhand therapy are often appropriate. Handtherapy intervention includes gentle activerange of motion, positioning and splintingfor comfort and instruction in one-handedactivities of daily living.(Cook and Burkhardt, 1994)In a study, activities of daily living were usedto assess quality of life in brain tumourpatients. Patients made significant gains infunctional status during rehabilitation.(Huang et al., 2001) Occupational therapy has a role to play inimproving vertigo and balance throughgraded exercise and adapting theenvironment and activity. Patients haveimproved greatly in functional areas afterreceiving occupational therapy.Occupational therapists have a role inproviding adaptive equipment and worksimplification techniques to solve thevestibular symptoms seen in thesepatients. (Cohen, 1994)COGNITIVE DEFICITS
Patients with cognitive deficits due to cerebraltumours or metastases have difficulty managingdaily living activities and occupations. Theremay be problems with memory andsequencing, and a deterioration or fluctuation
in abilities. This can cause a particular burdenfor family/carers. (See also neurologicalproblems, above)An occupational therapist can:• Assess risks to the person’s safety• Assess how well the person performsActivities of Daily Living (ADL) and leisureactivities• Help the person find ways to perform ADL,leisure activities and maximise independence• Assess the person’s environment and adapt itto suit their needs • Assess the person’s cognition• Help the person and their family/carers usememory aids• Provide advice, education and support tofamily and carers• Provide regular review to take into accountfluctuations in the person’s condition, and tohelp the person cope with deterioration• Help the person and their family/carersunderstand and have confidence in the aimsof treatment. This aims to:• Maintain the person’s safety• Maximise the person’s independence • Maintain the person at home for longerperiods• Prevent or reduce hospital re-admission• Help family/carers cope with a person whosecognitive ability is deteriorating.
Brain tumour patients make functional gainsand significant changes in their functionalstatus during the course of theirrehabilitation. (Huang et al., 2001)
20
People with advanced disease have fearsrelating to functional decline. Therapeuticgoals and rehabilitation have valuethroughout the trajectory of malignantdisease, giving specific attention to motorand sensory deficits, cerebellar andcognitive dysfunction. Appropriate physicaland occupational therapy techniques shouldbe considered for all advanced cancerpatients experiencing functional decline.(Cheville,2001)Occupational therapists have skills incontinuous assessment and evaluation, andcan be flexible in treatments and goals toensure meaningful life to the end. Helpinga person prepare for the death, and thusadapt to loss of function, is part of theoccupational therapist’s role in health careof the terminally ill. (Flanigan, 1982)Occupational therapists are an integral partof care planning for patients withmetastatic disease. Their functionalperspective broadens the focus of care.Evaluation and treatment related toindependent living, sensorimotorcomponents, therapeutic adaptations, caneffectively address many of the problemsdocumented in metastatic cancer.(Romsaas and Rosa, 1985)
ANXIETY AND DEPRESSIONCancer and its treatments may induce feelingsof hopelessness, worthlessness and panic. Aquarter of people with cancer experiencedepression at some stage during their disease.Having cancer can lower people’s self-esteemand cause them to question their belief system.
In turn, anxiety and depression can diminishpeople’s concentration, ability to assimilateinformation and motivation to carry outactivities.An occupational therapist can:• Explore the anxiety, and assess its impact ondaily living activities and leisure• Identify goals which increase a person’ssense of control• Implement an anxiety managementprogramme• Implement a fatigue managementprogramme• Implement a lifestyle managementprogramme• Involve the person in purposeful activity• Refer on to other professionals wherenecessary• Help the person and their family/carersunderstand and have confidence in the aimsof treatment.This aims to:• Reduce anxiety• Give the person control and choices • Help the person to resume their normal roles• Improve a sense of wellbeing and quality oflife• Improve relationships.
A group of cancer patients felt re-humanised when dealt with as wholepeople – body, mind and spirit. Many ofthem feared hospitalisation and taking onthe role of patient. The emphasis was ontaking back responsibility for one’s ownlife and finding ways of coping that aresuitable to the individual, recognising thatthese may differ widely. (Oldham, 1989)
21
Patients with a deteriorating conditionneed to continue to exercise control andfind meaning in life. They may feel isolatedand need socialisation and verbal and non-verbal communication. (Holland, 1984)
FLUID RETENTION(LYMPHOEDEMA, OEDEMA,ASCITES)The swelling and pain associated with fluidretention causes difficulties with mobility andactivities, dressing, flexibility, balance, exercisetolerance and body image. Finding clothes thatare large enough or fasten properly may be aproblem. Some types of fluid retention can alsocause sensory deficits.An occupational therapist can:• Assess mobility, transfers, self-care, dressing,meal preparation, body image, leisure andwork roles, pressure problems, fatigue,relationships, sexuality• Address issues arising from assessment• Teach techniques to help the person adapttheir lifestyle – work, leisure, social roles,relationships, activities of daily living• Provide advice on safety issues• Provide advice on energy conservation• Help the person take account of fluctuationsin their condition • Help communication between the person,family, carers and professionals through jointsessions.This aims to:• Maintain or improve quality of life• Help the person to be independent, or makesense of their functional limitations• Increase the person’s feelings of self-worth
• Help the person resume normal roles• Help the person minimise limb damage, forexample when preparing meals• Facilitate a return to work.General health, attitude and lifestyle allaffect lymphoedema and its response totreatment. (Dennis, 1993)
BODY IMAGE (INCLUDINGHAIR LOSS, SURGERY,LYMPHOEDEMA etc)Cancer and its treatments can cause a physicalchange to body shape because of surgery, butalso hair loss, lymphoedema, weight loss andother changes. These can affect a person’s body image, andreduce their sense of self-esteem andwellbeing. This in turn can lead to socialisolation and a loss of roles in society.An occupational therapist can:• Increase self-confidence • Address self-care issues• Provide equipment where necessary• Advise on, and adapt, clothing wherenecessary• Help the person access assertiveness trainingand cognitive behavioural therapy • Teach relaxation and anxiety managementtechniques• Set realistic goals and use graded socialactivities to maximise independence• Refer on to other agencies, professionals orsupport groups• Help communication between the person,family, carers and professionals through jointsessions.
Occupational therapy intervention in cancer
22
This aims to:• Improve quality of life• Increase confidence• Increase engagement in desired roles• Reduce stress• Help the person resume normal roles.Occupational therapy has a role ineducation (both patient and family/carers),energy conservation (eg. alternative meansof carrying out ADL), counselling, self-image, leisure activities, self-maintenance,home and community management. (Lloyd and Coggles, 1988)
BONE METASTASESBone metastases (secondary tumours in thebones) cause pain and reduce mobility andrange of movement. They can also increase thelikelihood of postural problems andneurological problems. They can make a personmore fearful of activity, so affect alloccupational performance areas. An occupational therapist can:• Provide precautionary and preventativeinformation about protecting vulnerablebones• Assess risk and provide home safety advice• Help plan lifestyle changes to protect bonesand improve mobility• Provide wheelchairs and equipment (forexample for bathing as a preventativemeasure against fractures)• Provide advice to the person, family/carers,and caring staff on manual handling issues• Provide psychological support• Advise on posture, seating, positioning andpressure care
• Advise on energy conservation issues• Help communication between the person,family, carers and professionals through jointsessions.This aims to:• Help people adapt and return to normalroutines• Improve quality of life• Improve relationships• Give people greater control over their lives• Reduce anxiety and depression.
Occupational therapy is an integral part ofcare plan for patients with metastaticdisease. Interventions include daily livingskills, adjustment to disability, energyconservation, adapting environment. Thefunctional perspective of occupationaltherapy can be easily distinguished fromthe framework of other professions. In achronic disease like metastatic cancer, itsperspective broadens the focus of care.(Romsaas and Rosa,1985).Occupational therapists working in apalliative care unit can observe, listen andwork with people with lung cancer andmetastatic breast cancer to achieve theirparticular aims, to ensure that they havethe optimum quality of life.(Armitage and Crowther, 1999)
23
ReferencesAmerican Occupational Therapy Association(1986) Occupational therapy and hospice(position paper). American Journal ofOccupational Therapy 40(12): 839-840Armitage K, Crowther L (1999) The role of theoccupational therapist in palliative care.European Journal of Palliative Care 6(5): 154-157Brandis S (2000) The Australian Health CareAgreement 1998-2003: implications andstrategic directions for occupational therapists.Australian Occupational Therapy Journal 47(2):62Brindle MJ (1999) Are doing and beingdimensions of holism? American Journal ofOccupational Therapy 53(6): 636-639Bye R A (1998) When clients are dying:occupational therapists’ perspectives.Occupational Therapy Journal of Research18(1): 3-24Centers L (2001) Beyond denial and despair:ALS and our heroic potential for hope. Journalof Palliative Care 17(4): 259-264Cheville A (2001) Rehabilitation of patientswith advanced cancer. Cancer 92(4 Suppl):1039-1048Cohen H (1994) Vestibular rehabilitationimproves daily life function. American Journal ofOccupational Therapy 48(10): 919-925Cook A, Burkhardt A (1994) The effect of
cancer diagnosis and treatment on handfunction. American Journal of OccupationalTherapy 48(9): 836-839Corner J (1997) The palliation of breathlessnessin patients with cancer. Conclusions from aconsensus workshop. European Congress forPalliative Care, LondonDawson SS (1982) The role of occupationaltherapy in palliative care. AustralianOccupational Therapy Journal 29(3): 119-124Dennis B (1993) Acquired lymphoedema: achart review of nine women’s responses tointervention. American Journal of OccupationalTherapy 47(10): 891-899Dietz J H (1981) Rehabilitation Oncology. NewYork, John Wiley & SonsFlanigan K (1982) The art of the possible…occupational therapy in terminal care. BritishJournal of Occupational Therapy August: 274-276Folkman S, Greer S (2000) Promotingpsychological well-being in the face of seriousillness: when theory, research and practiceinform each other. Psycho-Oncology 9:11-19Holland AE (1984) Occupational therapy andday care for the terminally ill. British Journal ofOccupational Therapy November: 345-348Huang ME, Wartella JE, Kreutzer JS (2001)Functional outcomes and quality of life inpatients with brain tumors: a preliminaryreport. Archives of Physical Medicine andRehabilitation 82(11): 1540-1546
AppendicesAppendices
24
Law M, Baptiste S, Mills J (1995) Client-centredpractice: what does it mean and does it makea difference? Canadian Journal of OccupationalTherapy 62(5): 250-257Lloyd C, Coggles L (1988) Contribution ofoccupational therapy to pain management incancer patients with metastatic breast disease.American Journal of Hospice Care 5(6): 36-38Nail LM, Winningham ML (1995) Fatigue andweakness in cancer patients – the symptomexperience. Seminars in Oncology Nursing 1(4):272-278Oldham J (1989) Psychological support forcancer patients. British Journal of OccupationalTherapy 52(12): 463-465Penfold S (1996) The role of occupationaltherapy in oncology. Cancer Treatment Reviews22: 75-81Pushpangadan M, Burns E (1996) Caring forolder people: community services: health.British Medical Journal 313: 805-808Roberts C (1999) Management of dyspnoea inadvanced cancer patients. Support Cancer Care7: 233-243Romsaas EP, Rosa SA (1985) Occupationaltherapy intervention for cancer patients withmetastatic disease. American Journal ofOccupational Therapy 39(2): 79-83
Sarvard J, Morin CM (2001) Insomnia in thecontext of cancer: a review of a neglectedproblem. Journal of Clinical Oncology 19(3):895-908Stent G (2001) A non-pharmacologicalapproach to managing breathlessness. NursingTimes 97(34): 57-58Strong J (1987) Occupational therapy andcancer rehabilitation. British Journal ofOccupational Therapy 50(1): 4-6Tuel SM, Cross LL, Meythaler JM, Faisant TE,Krajnik SR, Hogan P, Sewell L, Wilson B,Rodwell DW, Smith J (1992) Interdisciplinarymanagement of hemicorporectomy after spinalcord injury. Archives of Physical Medicine andRehabilitation 73(7): 669-673Vrkljan B, Miller-Polgar J (2001) Meaning ofoccupational engagement in life-threateningillness: a qualitative pilot project. CanadianJournal of Occupational Therapy 68(4): 237-246.Zislis JM (1970) Rehabilitation of the cancerpatient. Geriatrics 25(3): 150-8