Embed Size (px)
Citation preview

Daniel Catenacci, MDAssociate Professor of MedicineDirector GI Oncology Program
October 10, 2019ISGIO
Novel Targets and Immunotherapy Advances in Esophagogastric Adenocarcinoma How do we Sequence New Immunotherapy Agents?

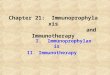
Comparing Efficacy: DFS, OS
FLOT CROSS
2Daniel Catenacci
mOS = 43.2 monthsmOS = 50 months
5yrOS = 45%5yrOS = 43%
(mDFS = 29.9 months)(mDFS = 30 months)
LN+ disease: 78%T4 disease: 8%
SR/Diffuse GC: 27%
LN+ disease: 65%T4 disease: 0%
SR/Diffuse GC: 0%
MAGICOnly Surgery
Al-Batran et al. Phase III FLOT4. Lancet 2019 van Hagen et al. Phase III CROSS. NEJM 2012Shapiro et al. Phase III CROSS. Lancet Oncol 2015
EGJ ACCROSS > just surg
HR 0.75
EGJ ACFLOT > MAGIC > Surgery
HR 0.76 HR 0.74

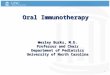
First Line Management of Advanced Gastroesophageal Adenocarcinoma
1. Murad, et al. Cancer 1993 2. Vanhoefer, et al. JCO 20003. Ajani, et al. ASCO 2009 4. Van Cutsem, et al. JCO 20065. Dank, et al. Ann Oncol 2008
6. Cunningham, et al. NEJM 2008 7. Kang, et al. Ann Oncol 20098. Guimbaud, et al. JCO 2014 9. Shah, et al. JAMA ONC 2016
BSC = best supportive care; MTX = methotrexate; S = S-1; A = doxorubicinF = 5-FU; C/P = cisplatin; I = irinotecan; E = epirubicin; O = oxaliplatin; D = docetaxel
mOS Months
BSC 1
60 2 4 128 10
FAMTX 2
SP 3
EOX 6
XP 7
FP 4
IF 5
EOF 6
DCF 4
ECF 6
ECX 6
FOLFIRI 8
FOLFOX 9
mOS = ~10-11m1yr OS = ~40%2yr OS = ~15-20%5yr OS < ~2%

GEA Standard Therapy
• Cytotoxics: 5FU, platinum, irinotecan, taxane, TAS-102
• Few targeted therapies incorporated into routine care:
Marker Incidence Treatment Therapy Line Approval Benefit
HER2++ ~15% Chemo+Trastuzumab 1L 2010 HR 0.65
none 100% Chemo+Ramucirumab 2L 2014/15 HR 0.8
MSI-High ~2-3% Pembrolizumab 2L+ 2017* HR? (great)
PDL1+ >1% ~50-60% Pembrolizumab 3L+ 2017 * HR? (marginal)
* Conditional approvals
MANY NEGATIVE ‘TARGETED/IO’ STUDIES!!

mOS Months
BSC 1
60 2 4 128 10
FAMTX 2
SP 3
EOX 6
XP 7
FP 4
IF 5
EOF 6
DCF 4
ECF 6
ECX 6
FOLFIRI 8
1. Murad, et al. Cancer 1993 2. Vanhoefer, et al. JCO 2000 3. Ajani, et al. ASCO 2009 4. Van Cutsem, et al. JCO 20065. Dank, et al. Ann Oncol 2008 6. Cunningham, et al. NEJM 2008 7. Kang, et al. Ann Oncol 2009 8. Guimbaud, et al. JCO 2014 9. Shah et al. JAMA Oncol 2016. 10. Bang et al. Lancet 2010.
X/FP+/-T10
X/FP+/-T10
HER2 IHC3+ or IHC2+/FISH+
HER2 (+) (IHC0-3+/FISH+)
X/FP+/-T10 HER2 IHC3+/FISH+
+T+T
14 16 18
FOLFOX 9
+T
All-comersmOS = ~10-11m1yr OS = ~40%2yr OS = ~15-20%5yr OS < ~2%
HER2+mOS = ~14-16m1yr OS = ~55-65%2yr OS = ~25-30%5yr OS < ~10-15%

Line Trial N Treatment 10 Endpt mOS HR Δ mPFS HR Δ RR Δ
2L Fuchs et alLancet 2013
REGARD
335 PlaceboRamucirumab
OS 3.55.2 0.78
p=0.047+1.7
1.32.1 0.48 +0.8
3%3% 0
2L Wilke et alLancet Oncol 2014
RAINBOW
665 Paclitaxel-PlboPaclitaxel-Ram
OS 7.49.6 0.8
p=0.017+2.2
2.94.4 0.64 +1.5
16%27% +11
3L Li et alJ Clin Oncol 2016
267 PlaceboApatinib
OS/PFS 4.76.5 0.71
p=0.015+1.8
1.82.6 0.44 +0.8
03% +3
Antiangiogenesis for EGA: 2L

Antiangiogenesis for EGA: 1LLine Trial N Treatment 10 Endpt mOS HR Δ mPFS HR Δ RR Δ
1L 1. Ohtsu et alJ Clin Oncol 2011
AVAGAST
774 Cis/F- placeboCis/F - Bev
OS 10.112.1
0.87N.S. +2
5.36.7
0.8p=0.004 +1.4
37.446
+8.6p=0.03
1L 2. Shen et alGastric Cancer 2015
AVATAR
202 Cis/Cape-placeboCis/Cape-Bev
OS 11.410.5
1.11N.S. -0.9
66.3
0.89N.S. +0.3
3441
+8N.S.
1L 3. Yoon et alAnnals Oncol 2016
JVBT
168 FOLFOX-placeboFOLFOX-Ramucirumab
PFS 11.711.5 1.08
N.S.-0.2
6.76.4 0.98
N.S.-0.3
4645 -1
N.S.
1L 4. Enzinger et alCancer 2019
ZAMEGA
641:2
FOLFOX-placeboFOLFOX-Aflibercept
6m PFS57.1%/60.5%
18.814.5
1.24N.S.
-4.3 7.49.9
1.11N.S. +2.5
7561
-14N.S.
1L 5. Fuchs et alLancet Oncol 2019
RAINFALL
645 Cis/F – placeboCis/F - Ram
PFS/OS 10.711.2
0.962N.S.
+0.5 5.45.7
0.75p=0.011
+0.3 3641
+5N.S.
1L 6. Yoshikawa et alJAMA Netw Open 2019
RAINSTORM
189 SOX - placebo Pac/RamSOX - Ram Pac/Ram
PFS1 14.2614.65
1.11N.S.
+0.4 6.746.34
1.07N.S.
-0.4 5058
+8N.S.

Le et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017
N= 86 MSI-H pts12 different tumor types
GEA:TCGA 23%Stage IV <3%
FDA Approves Pembrolizumab for Microsatellite Instability-High and Mismatch Repair Deficient Cancers. May 23, 2017
• ORR 3/5 = 60%
• KN059 3L+ORR 4/7 = 57%
• KN061 2LORR 7/15 = 47%
• KN062 1LESMO 2019 14 vs 14 vs 19 placebo
mOS NR NR 8.5
FDA approval 2L+ Pan-tumorN=149, historical control
Immune Checkpoint Blocakade for EGA
MSI-High

IO Trials: Gastroesophageal Cancer3L+
KN-059ATTRACTION-2
JAVELIN-300
2L
KN-061KN-181 (SCC 64%)
ATTRACTION-3 (SCC 100%)
1L Maintenance
KN-062
(CM-649)(KN590 AC/SCC)
(KN859)(ATTRACTION-4)
(JAVELIN-100)
Com
plet
edO
ngoi
ng

KN 059 Cohort 1 3L+: Response in All Patients
All patients (N = 259)Response* % 95% CI
ORR (CR+PR) 11.6 8.0–16.1DCR‡ 27.0 21.7–32.9
CR 2.3 0.9–5.0PR 9.3 6.0–13.5
SD 16.2 11.9–21.3PD 56.0 49.7–62.1
Data cutoff: Jan16, 2017*Only confirmed responses were included
‡CR+PR+SD≥2 months
• Median (range) follow-up: 5.8 months (0.5-21.6)

KN 059 Cohort 1:Response by PD-L1 Expression
Response* PD-L1 positive ( n= 148) PD-L1 negative (n = 109)
% 95% CI % 95% CIORR 15.5 10.1-22.4 6.4 2.6-12.8DCR‡ 33.1 25.6-41.3 19.3 12.3-27.9
CR 2.0 0.4-5.8 2.8 0.6-7.8PR 13.5 8.5-20.1 3.7 1.0-9.1
* Includes MSI-High tumors (13.3% MSS/PDL1+; 2-3 patients out of 20)FDA grants accelerated approval to pembrolizumab for advanced 3L+ PDL1+ gastric cancerhttps://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm577093.htmSeptember 22, 2017
Fuchs et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients With Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol 2018

• PD-L1 expression in gastric cancer is determined by Combined Positive Score (CPS)
• A specimen is considered to have positive PD-L1 expression if CPS ≥ 1
Tumor CellsImmune Cells
PD-L1 Expression IHC*
*22C3 pharmDx™IHC DAKO, Carpinteria, CA
Tumor Cells
Immune Cells
# PD-L1 staining cells (tumor cells, lymphocytes, macrophages) CPS = ----------------------------------------------------------------------------------- X 100
Total # viable tumor cells
PD-L1-positive PD-L1-negative
PD-L1 22C3 pharmDX assay

Progression-Free Survival
Presented By Yoon-Koo Kang at 2017 Gastrointestinal Cancers Symposium
Nivolumab (ONO-4538/BMS-936558) as salvage treatment after second or later-line chemotherapy for advanced gastric or gastro-esophageal junction cancer (AGC): A double-blinded, randomized, phase III trial.
TPS, PD-L1 28-8 pharmDX assay

Overall Survival
Nivolumab (ONO-4538/BMS-936558) as salvage treatment after second or later-line chemotherapy for advanced gastric or gastro-esophageal junction cancer (AGC): A double-blinded, randomized, phase III trial.
Kang et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017
TPS, PD-L1 28-8 pharmDX assay
ORR DCRKang et al. ASCO GI 201922C3 pharmDX assay

Bang et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: primary analysis of JAVELIN Gastric 300. Ann Oncol 2018
Avelumab vs SOC 3L Phase III JAVELIN-300
Avelumab vs chemoIrinotecan/taxane
Worse OSWorse PFS
PFS
PFS by PDL1

Immunotherapy in 3L+ Summary• KN059 COHORT1 – single arm
– pembrolizumab– PDL1+ CPS >1 only (conditional approval US only)
• ATTRACTION-02 – randomized to placebo – Nivolumab, all patients (Asia only)– PDL1 TPS (vs CPS?)
• JAVELIN300 – randomized to standard irinotecan/taxane– avelumab
Catenacci DVT, Hochster H, Klempner S. Keeping Checkpoint Inhibitors in Check. JAMA Netw Open 2019
TAS-102

Overall Survival, CPS ≥1
RAINBOWmPFS 4.4 mmOS 9.6 m
KEYNOTE 061 vs paclitaxel 2L
Shitara et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer(KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet 2018
PFS1.5 m4.1 m
(<0.0135)

Overall Survival by PD-L1 CPS
Presented By Kohei Shitara at 2018 ASCO Annual Meeting
ITT: N1=592 (296 vs 296)PDL1+ >1%: N2=395 (66%) (199 vs 196)
N2= NAN1= 195/592 = 33% 287/592 = 48% 108/592 = 18%
108/395 = 27%287/395 = 73%CPS >1 to <10% CPS >10%CPS <1%

OS, ORR, and DOR for MSI-H Tumorsa
Presented By Kohei Shitara at 2018 ASCO Annual Meeting
KEYNOTE 061 vs paclitaxel 2L

Pembrolizumab Versus Chemotherapy as Second-line Therapy for Advanced Esophageal Cancer: The Phase 3 KEYNOTE-181 Study
Presented By Takashi Kojima at 2019 Gastrointestinal Cancer Symposium

Overall Survival (ITT)
Presented By Takashi Kojima at 2019 Gastrointestinal Cancer Symposium

Overall Survival (SCC)
Presented By Takashi Kojima at 2019 Gastrointestinal Cancer Symposium

Overall Survival (PD-L1 CPS ≥10)
Presented By Takashi Kojima at 2019 Gastrointestinal Cancer Symposium

OS in Key Subgroups
KEYNOTE 181 vs paclitaxel 2L
~24% adeno CPS >10
FDA approves pembrolizumab for advanced esophageal squamous cell cancerhttps://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-advanced-esophageal-squamous-cell-cancerJuly 30, 2019

ATTRACTION-03 nivolumab vs taxane 2/3L+
Kato et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy ATTRACTION-3 a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 2019
(bad biomarker)
31% docetaxel69% paclitaxel
TPS, PD-L1 28-8 pharmDX assay
SCC

Immunotherapy in 2L Summary• KN061 – randomized to paclitaxel
– Pembrolizumab (MSI-H, >CPS 10?)
• KN181 SCC – randomized to paclitaxel – pembrolizumab, – SCC with PDL1+ CPS >10 only 2L+
• KN181 AC – randomized to paclitaxel– pembrolizumab (>CPS 10?)
• KNs MSI-High – single arm studies, KN061– pembrolizumab, (conditional approval US only) 2L+
Catenacci DVT, Hochster H, Klempner S. Keeping Checkpoint Inhibitors in Check. JAMA Netw Open 2019
ATTRACTION-3 SCC – randomized to taxane
nivolumab, SCCYin Yang!(PDL1 CPS >10, >1?)

Pembrolizumab With or Without Chemotherapy Versus Chemotherapy in Advanced G/GEJ Adenocarcinoma: The Phase 3, KEYNOTE-062 Study
Presented By Josep Tabernero at 2019 ASCO Annual Meeting

Statistical Considerations
Presented By Josep Tabernero at 2019 ASCO Annual Meeting
KN-062: A Story of Multiplicity Testing!!!1L HER2 neg: Chemo +/- Pembo or Pembro alone

Overall Survival: P+C vs C (CPS ≥1)
Presented By Josep Tabernero at 2019 ASCO Annual Meeting
(<0.0125)
KN-062 Primary Endpoint: Overall Survival –(HER2negative patients)

Overall Survival: P+C vs C (CPS ≥10)
Presented By Josep Tabernero at 2019 ASCO Annual Meeting
(<0.0075)
KN-062 Primary Endpoint: Overall Survival –(HER2negative patients)

Overall Survival: P vs C (CPS ≥1)
Presented By Josep Tabernero at 2019 ASCO Annual Meeting
Keynote 061 2L phase IIIpaclitaxel vs Pembro CPS>1
KN-062 Primary Endpoint: Overall Survival –(HER2negative patients)

Overall Survival: P vs C (CPS ≥10)
Presented By Josep Tabernero at 2019 ASCO Annual Meeting
KN-062 Primary Endpoint: Overall Survival –(HER2negative patients)
MSI-HighEBV+?PDL1 >30,40,50?TMB-high?PS 0 ?Low Disease Burden?
~10-15%

MSI-High KN-062
Shitara et al. ESMO 2019

MSS in KN-062
Shitara et al. ESMO 2019
ITT in KN-062

Immunotherapy in 1L Summary• KN062 monotherapy – randomized to Cis/5FU/placebo
– pembrolizumab – (some bad, some good: MSI-High, ??)
• KN062 chemotherapy – randomized to Cis/5FU/placebo– Pembrolizumab (some good: MSI-High, ??)
• Checkmate 649 1L pending• KEYNOTE 590 1L (AC/SCC) pending• KEYNOTE 859 1L pending• ATTRACTION-4 1L pending• JAVELIN 100 1L maintenance pending
Catenacci DVT, Hochster H, Klempner S. Keeping Checkpoint Inhibitors in Check. JAMA Netw Open 2019

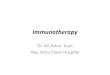
Anti-HER2 + IO Combination?
Anti-HER2 Ab

Anti-HER2 + IO Combination
Janjigian et al. GI ASCO 2019 Catenacci et al. GI ASCO, 2017/18/19, ESMO 2019
Second Line: Margetuximab/PembrolizumabFirstLine: Chemo/Trastuzumab/Pembrolizumab
KN-811 1L Phase IIIChemo/Tras +/- pembro
MAHOGANY 1L Phase II/III
24 24 22 22 22 21 21 18 18 16 13 12 11 10 9 8 8 8 8 8 5 4 3 3 3 1 1 1 1 1 032 32 31 29 28 28 25 25 22 20 17 13 13 12 10 9 8 6 6 5 4 2 1 1 08 7 6 6 6 6 6 6 5 3 3 3 3 3 2 1 06 6 5 4 3 1 1 0
IHC3+/PDL1+IHC3+/PDL1-IHC2+/PDL1+IHC2+/PDL1-
01
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
30
OS: Months from treatment initiation
0.0
0.2
0.4
0.6
0.8
1.0
Surv
ival P
roba
bility
01
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
30
OS: Months from treatment initiation
0.0
0.2
0.4
0.6
0.8
1.0
Surv
ival P
roba
bility
+ Censored
IHC3+/PDL1+
IHC3+/PDL1-
IHC2+/PDL1+IHC2+/PDL1-

GEA Standard Therapy1L 2L 3L+
HER2-/MSS/PDL1- FOLFOX Pac/Ram IrinotecanHER2 + FOLFOX-T FOLFIRI-Ram Taxane
TAS102PDL1 CPS >1 pembroMSI-High pembro
Few targeted therapies incorporated into routine care:
Marker Incidence Treatment Therapy Line Approval Benefit
HER2++ ~15% Chemo+Trastuzumab 1L 2010 HR 0.65
none 100% Chemo+Ramucirumab 2L 2014/15 HR 0.8
MSI-High ~2-3% Pembrolizumab 2L+ 2017* HR? (great)
PDL1+ >1% ~50-60% Pembrolizumab 3L+ 2017 * HR? (marginal)
* Conditional approvals
Molecular:

Thank You!