Embed Size (px)
DESCRIPTION
Realizing the Financial Benefits of Electronic Health Records: What do the Data Show? The VA Experience. October 25, 2005 Robert M. Kolodner, MD Chief Health Informatics Officer, VHA Department of Veterans Affairs. Cost Savings and EHRs in VA. - PowerPoint PPT Presentation
Citation preview

October 25, 2005
Robert M. Kolodner, MDChief Health Informatics Officer, VHA
Department of Veterans Affairs
Realizing the Financial Benefits of Electronic
Health Records: What do the Data Show?
The VA Experience

AMIA - S49 (Kolodner) October 25, 2005 2
Cost Savings and EHRs in VA
•20+ year history of computer use to support care in the Veterans Health Administration (VHA)
•Sometimes challenging to tease out effects of the Electronic Health Record from other major changes in VHA, especially since 1995
– Shift from Inpatient to Outpatient care– Reorganization to 22 (now 21) regional networks– Implementation of performance measures– Shift from facility-centric to veteran-centric

AMIA - S49 (Kolodner) October 25, 2005 3
Transformational Strategies for VA Health Care
“In summary, electronic health records, performance management, and a patient-centric focus have been critical transformational strategies for the VA. They have been utilized to support achievement and are associated with measurable progress in each of the VA’s value domains.”
The American Journal of Managed Care, November 2004

AMIA - S49 (Kolodner) October 25, 2005 4
2005: Who is “VHA” . . . Veterans Health Administration• 5.2 million patients, ~ 7.6 million enrollees
~ $30 Billion budget ~ 1,300 Sites-of-Care
– Including 171 medical centers or hospitals~ 870 clinics– 207 counseling centers & – long-term care programs
~ 197,500 Employees (~14,000 MD , 56,000 Nurses, 33,000 AHP)~ 150,000 volunteers• Affiliations with 107 Academic Health Systems
– 1,500 Health Professions Training Affiliations– Additional 25,000 affiliated MD’s; +35,000 residents & fellows in 14,000 slots~ 89,000 trainees in all disciplines– Nearly half US health professionals (>65% MDs) have some training in VA
~ $1.7B Research: Rehabilitation, Health Services, Clinical, Basic

AMIA - S49 (Kolodner) October 25, 2005 5
VA’s Health Information System is VistA
•“CPRS” is the integrated EHR application•VA runs 128 VistA systems these sites
– Down from 172 VistA systems 10 years ago– ~180,000 PCs and thin clients
•Delivers a complete hospital information system, electronic health record, imaging, Bar Code Medication Administration
– Hardware, software, maintenance, upgrades, staffing
•For FY2004:– Cost per enrollee
$78 / enrollee– Average cost per hospital (n=158)
$3.6 million

AMIA - S49 (Kolodner) October 25, 2005 6
And VistA Is Actively Used... Some National VistA Statistics (Total…Daily)
•Documents (Progress Notes, Discharge Summaries, Reports)
– 742,000,000…….. +576,000 each workday
•Orders– 1.48 Billion…….... +922,000 each workday
• Images– 385,000,000……… +587,000 each workday
•Vital Sign Measurements– 915,000,000……… +676,000 each workday
•Medications Administeredwith the Bar Code Medication Administration (BCMA) system
– 716,000,000……… +607,000 each workdayStatistics as of September 2005

AMIA - S49 (Kolodner) October 25, 2005 7
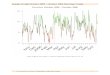
Rate of Increase of VistA Data
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
1,000,000
Nov-04 Dec-04 Jan-05 Feb-05 Mar-05 Apr-05 May-05 Jun-05 Jul-05 Aug-05 Sep-05
Date
Av
era
ge
Dai
ly I
nc
rea
se (
Wo
rkd
ays
)
Orders
Images
Documents
Medication Administration
Vital Sign Measurements
VistA Data Trend – Rate of Increase

AMIA - S49 (Kolodner) October 25, 2005 8
Financial Benefits of EHR in VA
•Unable to provide overall benefits for the system since DHCP/VistA implemented and matured over 20 years and baselines were not taken
HOWEVER
•Many local examples with costs•Some local examples with implications without exact costs
•Some speculations•…not counting savings by not repeating tests / or avoiding hospital admissions

AMIA - S49 (Kolodner) October 25, 2005 9
Myths: VA’s Different . . .
•“VA’s Command & Control”– Truth: Yes, 17,000 staff physicians, but 25,000 affiliated
faculty & 35,000 housestaff through affiliations with 107 academic health systems
•“VA has an appropriated budget”– True, but VA $1.5 of $25 B (FY03) was revenue from
billing, increased from $300 M, 3 years prior
•“VA’s patients are former military, thus overall healthier & follow instructions”
– VA patients define adverse selection
•Think of VA as “Living Laboratory”

AMIA - S49 (Kolodner) October 25, 2005 10
Examples
•Medications – Inpatient– Bar Code Medication Administration
•Medications – Outpatient (local initiatives)– Drug Cost feedback
•Disease Management - Diabetes– HgB A1c– Outcomes
• Impact of Vaccinations– Pneumovax
•Not having to pull charts or maintain a chart room

Bar Code Med Administration (BCMA)
INFORMATION TECHNOLOGY – SAFETY
Inpatient Medication Error Rate per 10,000 doses
1.571.49
0.97 0.96 0.93
0.73
1.3
0.82
0.41
1.09
0.921.01
0.48
1.03
0.87
0.61
0.13
0.33
0.53
0.73
0.93
1.13
1.33
1.53
1.73
1st Qtr01
2ndQtr 01
3rd Qtr01
4th Qtr01
1st Qtr02
2ndQtr 02
3rd Qtr02
4th Qtr02
1st Qtr03
2ndQtr 03
3rd Qtr03
4th Qtr03
1st Qtr04
2ndQtr 04
3rd Qtr04
4th Qtr04

AMIA - S49 (Kolodner) October 25, 2005 12
What is the AssociatedCost Avoidance or Cost Savings?

INFORMATION TECHNOLOGY – EFFICIENCY
Drug Costs
are listed in the order menu
Using Technology to Manage Drug Costs

INFORMATION TECHNOLOGY – EFFICIENCY
Using Technology to Manage Drug Costs
Here Fluoxetine is listed as
the preferred
drug, costs are also listed

INFORMATION TECHNOLOGY – EFFICIENCY
SSRI Total Costs for 30 Day Equvalent Rx's
$173,938
$90,955
$174,989
$91,101
$0
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
$140,000
$160,000
$180,000
$200,000
12/1
5/20
04
12/2
2/20
04
12/2
9/20
04
1/5/
2005
1/12
/200
5
1/19
/200
5
1/26
/200
5
2/2/
2005
2/9/
2005
2/16
/200
5
2/23
/200
5
3/2/
2005
Date
Co
st
Using Technology to Manage Drug Costs
Conversion from
Citalopram to Fluoxetine

AMIA - S49 (Kolodner) October 25, 2005 16
Diabetes Mellitus (DM)
•Prevalence of DM among VA patients is 20% – Substantially higher than in the general population– More than 1 million patients per year– Nearly all are male (2.4% women)– Largest group is >65 years old

AMIA - S49 (Kolodner) October 25, 2005 17
Performance MeasurementSetting the U.S. Benchmark for 18 Comparable Indicators
Clinical Indicator VA 2003 Medicare 03 Best Not VA or Medicare
Advised Tobacco Cessation (VA x3, others x1) 75 62 68 (NCQA 2002)
Beta Blocker after MI 98 93 94 (NCQA 2002)
Breast Cancer Screening 84 75 75 (NCQA 2002)
Cervical Cancer Screening 90 62 81 (NCQA 2002)
Cholesterol Screening (all pts) 91 NA 73 (BRFSS 2001)
Cholesterol Screening (post MI) 94 78 79 (NCQA 2002)
LDL Cholesterol <130 post MI 78 62 61 (NCQA 2002)
Colorectal Cancer Screening 67 NA 49 (BRFSS 2002)
Diabetes Hgb A1c checked past year 94 85 83 (NCQA 2002)
Diabetes Hgb A1c > 9.5 (lower is better) 15 NA 34 (NCQA 2002)
Diabetes LDL Measured 95 88 85 (NCQA 2002)
Diabetes LDL < 130 77 63 55 (NCQA 2002)
Diabetes Eye Exam 75 68 52 (NCQA 2002)
Diabetes Kidney Function 70 57 52 (NCQA 2002)
Hypertension: BP < 140/90 68 57 58 (NCQA 2002)
Influenza Immunization 76 P 68 (BRFSS 2002)
Pneumocooccal Immunization 90 P 63 (BRFSS 2002)
Mental Health F/U 30 D post D/C 77 61 74 (NCQA 2002)

INFORMATION TECHNOLOGY – QUALITY
CLINICAL REMINDERS

INFORMATION TECHNOLOGY – QUALITY
Effect of Clinical Reminders at 1 VAMC
HEMOGLOBIN A1cLower is Better
16
19 20
13
00
5
10
15
20
25
FY01 FY02 FY03 FY04 1st Qrt FY05
Perc
en
t
Implementation

INFORMATION TECHNOLOGY – QUALITY
HEMOGLOBIN A1cLower is Better
16
19 20
13
00
5
10
15
20
25
FY01 FY02 FY03 FY04 1st Qrt FY05
Perc
en
t
Implementation Education and Focus
Effect of Clinical Reminders at 1 VAMC

AMIA - S49 (Kolodner) October 25, 2005 21
Highest Quality of Care For Patients with Diabetes in VA
“Diabetes processes of care and 2 of 3 intermediate outcomes were better for patients in the VA system than for patients in commercial managed care.”
Annals of Internal Medicine, August 17, 2004

AMIA - S49 (Kolodner) October 25, 2005 22
VA-TRIAD Adjusted Intermediate Outcomes
VA, % CMC, %
A1C level (proportion <8.5%)* 83 65
A1C level (proportion <9.5%)* 92 80
LDL level (proportion <100)* 52 36
LDL level (proportion <130) * 86 72
BP level (proportion <130/80) 28 29
BP level (proportion <140/90) 53 52
*P<0.001
Kerr et al – Annals of Internal Medicine 2004

October 25, 2005 AMIA - S49 (Kolodner) 23
FY99-04 Changes in Total, Major and Minor Age-Adjusted Amputation Rates Among
Patients With Diabetes
0
1
2
3
4
5
6
7
8
9
Overall 7.94 6.24 5.42 4.53 4.4 4.04
Major 3.61 2.78 2.4 1.95 1.84 1.72
Minor 4.33 3.46 3.03 2.59 2.55 2.32
1999 2000 2001 2002 2003 2004
Am
puta
tions
per
100
0 pa
tien
ts

AMIA - S49 (Kolodner) October 25, 2005 24
What is the AssociatedCost Avoidance or Cost Savings?

AMIA - S49 (Kolodner) October 25, 2005 25
Pneumococcal Vaccination Rates in VHA
0
20
40
60
80
100
FY 95 4th Qtr97
4th Qtr98
FY 99 FY 00 CHG FY01* FY02 FY03
Perc
ent
Vaccin
ate
d
VHA Healthy People 2000 Iowa 99* NHIS
`
•Iowa: Petersen, Med Care 1999;37:502-9. >65/ch dz•HHS: National Health Interview Survey, >64
--BRFSS--
--BRFSS 90th--

AMIA - S49 (Kolodner) October 25, 2005 26
Pneumonia: Acute InpatientImproving Efficiency by Reducing Excess Health Care Utilization
104.0
100.5
94.5
16.0
15.5
15.2
14.614.8
1515.215.415.615.8
1616.2
FY1999 FY2000 FY2001
Th
ou
sa
nd
s
To
tal D
isch
arg
es
(be
dse
ctio
n)
889092949698100102104106
Th
ou
sa
nd
s
To
tal D
ays
(b
ed
sect
ion
)
Acute Days Discharges
9,500 fewer bed days
8,000 fewer discharges
• DRG89-90; Unadjusted for Pt. Population (up 20%, FY99-01)

AMIA - S49 (Kolodner) October 25, 2005 27
Vaccine Cuts Pneumonia Risk in High-Risk Patients*
• 50% of elderly Americans / high-risk individuals have not received the pneumococcal vaccine.
– VA Medical Center study of 1,900 elderly patients with chronic lung disease; 2/3 vaccinated against pneumonia.
• Pneumococcal vaccination:– 43% reduction in hospitalizations for pneumonia and
influenza, and a 29% reduction in the risk of death. • Pneumonia and Influenza vaccination:
– 72% reduction in hospitalizations for these two diseases and an 82% reduction in deaths from all causes.
• Pneumococcal vaccination saved an average of $294 per vaccine recipient over the 2-year period.
*Archives of Internal Medicine 1999;159:2437-2442Dr. Kristin Nichol, VAMC / Minneapolis

AMIA - S49 (Kolodner) October 25, 2005 28
Extrapolating from Dr. Nichol’s Study:
Between 1996 and 1998, Increased Rates ofPneumococcal Vaccination Averted 3914Excess Deaths Nationally in VHA Patientswith Chronic Lung Disease…Today, over 6,000 lives have been saved.

AMIA - S49 (Kolodner) October 25, 2005 29
What is the AssociatedCost Avoidance or Cost Savings?

AMIA - S49 (Kolodner) October 25, 2005 30
Priceless

AMIA - S49 (Kolodner) October 25, 2005 31

AMIA - S49 (Kolodner) October 25, 2005 32

AMIA - S49 (Kolodner) October 25, 2005 33
Paper versus Electronic – Elimination of Processes
•Without an EHR– Paper charts were pulled & delivered to clinic locations for
scheduled appointments– Also involved re-filing – Resulted in a 60% average chart availability rate
•One VA Medical Center– Budget of 1% of the entire VHA– Closed file room - cost avoidance estimated at $600,000
•VERY Conservative estimate – $1 per pull, delivery and re-file
Some estimates in private sector as high as $10/pull– Eliminating this for VA’s 50 million outpatient encounters
estimated $50 million cost avoidance in staff resources

AMIA - S49 (Kolodner) October 25, 2005 34
Home Telehealth
And what savings might we see from Home Telehealth?

October 25, 2005October 25, 2005 AMIA - S49 (Kolodner)AMIA - S49 (Kolodner) 3535
Home-Telehealth Technologies
Flexible Sensor Connectivity
Blood sugarBlood sugar
Blood pressureBlood pressure
ThermometerThermometer
StethoscopeStethoscope
ECGECG
Pulse O2Pulse O2
CameraCamera
Digital ScaleDigital Scale

October 25, 2005October 25, 2005 AMIA - S49 (Kolodner)AMIA - S49 (Kolodner) 3636

AMIA - S49 (Kolodner) October 25, 2005 37
What is the AssociatedCost Avoidance or Cost Savings?

AMIA - S49 (Kolodner) October 25, 2005 38
This presentation is available on the VHA internet at:
www.va.gov/vha_oi
Select “Office of Information Document Library” on the left hand bar
Presentation is Titled
“AMIA 2005 - Presentation by Robert M. Kolodner M.D.”
http://www1.va.gov/vha_oi/docs/AMIA_2005_Panel.pps