Embed Size (px)
Citation preview
MAKING A NEW LACRIMAL PUNCTUM 677
phora of both eyes which he had come to regard as incurable after frequent ineffectual treatment with lotions and syringing thru small puncta which only just failed to be in proper apposition with the globes; the procedure mentioned above, done in ten minutes, cured him permanently.
Sometimes in elderly people so affected, the lids are somewhat thickened. Even so, the new punctum, if properly made, usually lies in contact with the globe: I have rarely found it necessary to resort to some means to bring the new punctum into contact with the globe; in one case I did so by making with the cautery a fine line of surface scar tissue in the epi-
My interest in lethargic encephalitis was especially aroused by the symptoms and course of the following case:
M. W., aged 51, called at my office December 15, 1924, complaining of blurred near vision, sensation of eyes being crossed and slight dizziness. Duration of symptoms was four or five days, and they had followed what his physician thought was influenza. Examination of the eyes was negative, with the exception that the pupils were markedly contracted and very sluggish in their reaction to light and accommodation. His right vision was 0.8; + -25 C + -50 X 100 = 0.8 L.V. was 0.8; -f .75 = 0.8 + 1.75 added for near brought Snellen chart D.75 down to 13.5 inches. He could, however, read only for about one minute and then the "lines ran together again," as he stated. A +3.00 was finally added to his distance correction, and he could read Snellen D.75 at thirteen inches with comfort, and could bring the chart to within eleven inches from his eyes. The latter apparently was his near point, and his accommodation = 3.7D (100:27.5). Subtracting 3 D. from this amount leaves a balance of 0.70 D. The average accommodation was evi-
thelium of the fornix below the opening.
It may not be out of place to mention the following way of securing the patient's assistance in small procedures of this sort when an assistant is not procurable: The patient can hold a swab of sterilized cotton wool against his cheek to catch any blood if the swab is gripped in an anaethetist's flat tongue-forceps. The lump of cotton is gripped in the forceps, dipped in boiling water, the hot water then vigorously shaken out of it and the patient given the hot sterile pad in the forceps to hold. That is helpful when performing, unaided, minor operations such as that described above, or opening chalazia.
dently markedly reduced or partially paralyzed.
I tentatively attributed this paresis to influenza and instructed the patient to return for further study of his case. His condition, however, grew worse, and he was unable to keep his appointment. He developed twitching of the face, slight temperature and insomnia. After several consultations the case was diagnosed as one of lethargic en-cephelitis.
I saw him once more during the acute stage, and at that time the right pupil was larger than the left, both almost fixed to light and accommodation. One drop of homatropin dilated pupils to 5 mm. The fundus examination was negative.
June 17, 1925, or six months later, the patient called at my office again, asking for near glasses as he was still unable to use his eyes for near work. This time I found in addition a slight divergence of the left eye. Under homatropin he accepted R. - j - .75 e= 0.6 - 3 ; L. + 1.2:5 = 1 . 0 - 3 ; add + 3.00 for near. Evidently there had been no change in his accommodative power.
To determine what role ocular symp-
OCULAR DISORDERS IN ENCEPHALITIS LETHARGICA. M. L. FOLK, M.D.
CHICAGO, ILL.
A case marked by paresis of accommodation, inequality and rigidity of pupils is reported. The records of such cases at Cook County Hospital for the preceding six years were examined and the relative frequency of different ocular symptoms is given in tabular form. Literature bearing on the more frequent symptoms is cited. Entrance thesis read before the Chicago Ophthalmological Society, March IS, 1926.
678 M. L. FOLK
toms play in the clinical picture of lethargic encephalitis, I made a study of the records of the Cook County Hospital, (thanks to the courtesy of Dr. Hassin) for the years 1919 to part of 1925 inclusive.
There were about 200 cases diagnosed as lethargic encephalitis, but a considerable number had to be eliminated as the eye findings were vague and questionable; only 157 records in which the eye findings were confirmed by an attending man were studied. Out of these, eighty were acute, seven suspected and seventy postlethargic cases. In the acute series, sixty-four, or 80 percent, showed positive eye findings of one kind or another, and sixteen were negative. Of the postlethargic series, forty-four cases, or 63 percent, had positive eye findings. Most of the patients showed several ocular disturbances.
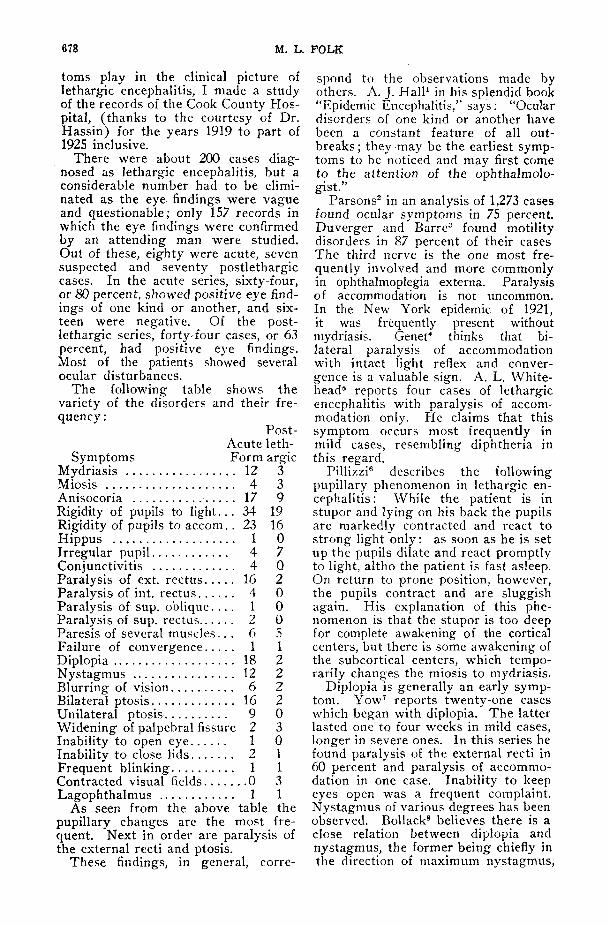
The following table shows the variety of the disorders and their frequency :
Post-Acute leth-
Symptoms Form argic Mydriasis 12 3 Miosis 4 3 Anisocoria 17 9 Rigidity of pupils to l ight. . . 34 19 Rigidity of pupils to accom.. 23 16 Hippus 1 0 Irregular pupil 4 7 Conjunctivitis 4 Q Paralysis of ext. rectus 16 2 Paralysis of int. rectus 4 0 Paralysis of sup. ob l ique . . . . 1 0 Paralysis of sup. rectus 2 0 Paresis of several muscles . . . 6 5 Failure of convergence 1 1 Diplopia 18 2 Nystagmus 12 2 Blurring of vision 6 2 Bilateral ptosis 16 2 Unilateral ptosis 9 0 Widening of palpebral fissure 2 3 Inability to open eye 1 0 Inability to close lids 2 1 Frequent blinking 1 1 Contracted visual fields 0 3 Lagophthalmus 1 1
As seen from the above table the pupillary changes are the most frequent. Next in order are paralysis of the external recti and ptosis.
These findings, in general, corre
spond to the observations made by others. A. J. Hall1 in his splendid book "Epidemic Encephalitis," says: "Ocular disorders of one kind or another have been a constant feature of all outbreaks; they may be the earliest symptoms to be noticed and may first come to the attention of the ophthalmolo-gist."
Parsons2 in an analysis of 1,273 cases found ocular symptoms in 75 percent. Duverger and Barre3 found motility disorders in 87 percent of their cases The third nerve is the one most frequently involved and more commonly in ophthalmoplegia externa. Paralysis of accommodation is not uncommon. In the New York epidemic of 1921, it was frequently present without mydriasis. Genet4 thinks that bilateral paralysis of accommodation with intact light reflex and convergence is a valuable sign. A. L. White-head5 reports four cases of lethargic encephalitis with paralysis of accommodation only. He claims that this symptom occurs most frequently in mild cases, resembling diphtheria in this regard.
Pillizzi6 describes the following pupillary phenomenon in lethargic encephalitis : While the patient is in stupor and lying on his back the pupils are markedly contracted and react to strong light only: as soon as he is set up the pupils dilate and react promptly to light, altho the patient is fast asleep. On return to prone position, however, the pupils contract and are sluggish again. His explanation of this phenomenon is that the stupor is too deep for complete awakening of the cortical centers, but there is some awakening of the subcortical centers, which temporarily changes the miosis to mydriasis.
Diplopia is generally an early symptom. Yow' reports twenty-one cases which began with diplopia. The latter lasted one to four weeks in mild cases, longer in severe ones. In this series he found paralysis of the external recti in 60 percent and paralysis of accommodation in one case. Inability to keep eyes open was a frequent complaint. Nystagmus of various degrees has been observed. Bollack8 believes there is a close relation between diplopia and nystagmus, the former being chiefly in the direction of maximum nystagmus,
OCULAR DISORDERS WITH LETHARGIC ENCEPHALITIS 679
and their frequency being about the same.
Conjunctivitis was frequently seen in the Russian epidemic of 1921, particularly in the initial stages of the disease. Paralysis of conjugate movements, especially upward, is common, according to Hall. Sainton and Cornat9 observed asynergia between upper lids and frontalis muscle. H. Butler10 saw three cases of retrobulbar neuritis and one of optic neuritis. Grinker11 records the case of a young woman in whom there was a gradually increasing optic neuritis, followed by optic atrophy. Hemianopsia have been described. Various groups of symptoms were found in different epidemics. In the French outbreaks of 1919-20, ptosis and paralysis of accommodation were common, while in those of 1921 nystagmus and anisocoria were more prevalent.
As to ocular manifestations in post-lethargic cases, while they are not so common as in the acute stage of the disease, yet their percentage is fairly large. They may vary from day to day and from year to year. There may be an interval of even three or four years between the acute and postlethargic or Parkinsonian stage, as it is called, thus resembling syphilis in this regard. Disorders of the oculopalpebral reflex (blinking) are common, either as in-frequency of blinking or inabality to open eyes after closure. In some cases there are fluttering movements of the lids on trying to open them. Rossi12 reports a case of temporary ptosis after closing the eyes several times. One youth would fall from his bicycle on account of inability to open his eyes after closure. The infrequency of blinking is probably due to hyper-tonicity of orbicularis, or respective antagonistic muscles.
Cords and Blank13 report residual symptoms six to thirty-six months
BIBLIOGRAPHY. 1. Hall, A. J. Epidem. Enceph., N. Y.. 1924. 2. Parsons. Report of Ministry of Health, 1922. 3. Duverger and Barre. Revue Neurol., 1920, vol. XXXVII, p. 439. 4. Genet. Lyon Med., 1920, vol. CXXIV, p. 721. 5. Whitehead, A. L. Brit. Med. Jour., 1924, vol. II, p. 665. 6. Pillizzi. Wilbrand and Saenger. Neurologie des Auges, 1922, p. 23. 7. Yow. Lancet, 1924, vol. I, p. 1260. 8. Bollack. Revue Neurol., 1921, vol. XXXVII, p. 294. 9. Sainton and Cornat. Paris Med., 1921. vol. I, p. 408.
10. Butler, H. Epidemic Enceph., N. Y., 1924. 11. Grinker. Jour, of Nervous and Mental Dis., 1920, vol. LII, p. 323. 12. Rossi. Revue di Ratol. neurol. e. ment., 1922, vol. XXVII, p. 135. 13. Cords and Blank. Klin. M. fur Augenh., V. 72, p. 394.
after lethargic encephalitis, in forty-four out of fifty cases. They found paralysis of accommodation in thirteen cases, paralysis of convergence in thirty-three, paralysis of external ocular muscles in twelve, pupillary disturbances in twelve, nystagmus in eleven and ptosis in four cases.
PATHOLOGY : The macroscopic changes are congestion of superficial vessels, hemorrhage, thickening and opacity of pia and arachnoid. The gray matter is more affected than the white, and the basal ganglia, parts around the aqueduct of Sylvius and the floor of the fourth ventricle seem to be places of predilection. The ventricle may contain an excess of cerebrospinal fluid. The vessels of the choroidal plexus are frequently distended. The cord may be involved in similar changes.
The microscopic changes are most striking in the reaction of the blood vessels. We get the socalled "perivas-cular cuffs" or an accumulation of round cells (mononuclear or plasma) around the wall. The intima, however, remains intact. Degenerative changes in the nerve cells, such as glial nodes, are also found. As most changes are found in the vicinity of the nuclei of the third, fourth and sixth cranial nerves, practically all the symptoms enumerated above can readily be explained on a pathologic basis.
CONCLUSIONS.
1. Ocular disturbances are very frequent and are found early in lethargic encephalitis.
2. Mild cases are easily overlooked and may first come to the attention of the ophthalmologist.
3. When associated with headache, dizziness, insomnia and increased temperature, ocular symptoms make the diagnosis of lethargic encephalitis almost certain. 2756 W. Division St.