Embed Size (px)
Citation preview

Immunology 1998 95 360-369
High-level production of alternatively spliced soluble interleukin-6 receptor in serumof patients with adult T-cell leukaemia/HTLV-I-associated myelopathy
S. HORIUCHI,* W. AMPOFO,* Y. KOYANAGI,* A. YAMASHITA,* M. WAKIt A. MATSUMOTO,t M. YAMAMOTOT& N. YAMAMOTO* *Departments of Microbiology & Molecular Virology, Faculty of Medicine, Tokyo Medical and Dental
University, Tokyo, Japan, tResearch Institute of Tokyo, Seikagaku Corporation, Tokyo, Japan, and IDepartment of Biochemistry,National Defense Medical College, Saitama, Japan
SUMMARY
We have previously shown, using human T-cell lymphocytotrophic virus-I (HTLV-I)-infected celllines, that soluble interleukin-6 receptor (sIL-6R) is generated through an alternative splicingmechanism. In this study, we examined human sera for the presence of alternatively splicedsoluble IL-6R (AS-sIL-6R). We produced a monoclonal antibody (mAb) recognizing the uniquesequence of AS-sIL-6R peptide, generated by an altered reading frame. We also made recombinantAS-sIL-6R protein in Spodoptera frugiperda-9 (Sf-9) cells carrying baculovirus, which encodedaltered sIL-6R or conventional IL-6R cDNA. mAbs specifically recognized AS-sIL-6R, but notconventional IL-6R, as demonstrated by Western blot analyses, fluorescence-activated cell sorter,immunofluorescence analyses and enzyme-linked immunosorbent assay (ELISA). We adapted an
ELISA system and used it for detection of altered sIL-6R in sera from 23 healthy persons, 12patients with adult T-cell leukaemia (ATL) and 13 patients with HTLV-I-associated myelopathy(HAM). Serum levels of AS-sIL-6R were 6 4 or 6 1 times greater in ATL (28 7+20 4ng/ml,P<0-0001) and in HAM patients (275+121 ng/ml, P<00001) than in healthy individuals(4-5 + 21 ng/ml). High levels of AS-sIL-6R were also observed in plasma from rheumatoidarthritis patients and in persons with elevated levels of alanine aminotransferase (ALT), antinuclearantibody (ANA), or oc-fetoprotein (AFP). However, in human immunodeficiency virus-I (HIV-1),hepatitis B virus (HBV) or hepatitis C virus (HCV)-infected individuals, AS-sIL-6R levels were
not elevated. In this study, we confirmed that AS-sIL-6R is indeed present in human sera. Theseobservations suggest that alternative splicing of IL-6R mRNA is of consequence in ATL, HAMand in some autoimmune diseases. The HTLV-I-infected T cells appeared to play an importantrole in AS-sIL-6R production.
INTRODUCTION
Interleukin-6 (IL-6) acts on its target cells via a surfacereceptor complex consisting of two subunits: a receptor(IL-6R) and a signal transducer (gpl30). 2 IL-6 promotes thefinal maturation of B cells into antibody-forming cells, andinduces proliferation and activation of a wide array of targetcells, such as hepatic, neuronal3 and haemopoietic cells.4 In
Received 26 March 1998; revised 20 July 1998; accepted 22July 1998.
Abbreviations: AS-sIL-6R, alternatively spliced solubleinterleukin-6 receptor; ATL, adult T-cell leukaemia; HAM, HTLV-I-associated myelopathy; mAb, monoclonal antibody; PC-sIL-6R, pro-teolytically cleaved sIL-6R; Sf-9, Spodoptera frugiperda-9 cells; TM;transmembrane.
Correspondence: Dr N. Yamamoto, Department of Microbiology,Faculty of Medicine, Tokyo Medical and Dental University, 1-5-45Yushima, Bunkyo-ku, Tokyo, 113, Japan.
addition to cell-expressed IL-6R, soluble forms (sIL-6R) arepresent in the plasma of normal, healthy individuals. However,increased levels of sIL-6R have been reported in patients withgammopathy,5 plasma cell dyscrasias,6 rheumatoid arthritis,7or viral diseases, such as human immunodeficiency virus-i(HIV-l )-induced diseases,8 and Paget's disease induced by themeasles virus.9 Several reports describe that, once bound withIL-6, the sIL-6R activates cell types that are normally unableto respond to IL-6.10-12 In vitro studies show that thesIL-6R/IL-6 complex promotes cellular proliferation,11"3osteoclast formation12 and myocardial hypertrophy.14 Thepresence of increased levels of sIL-6R in these pathologicalconditions strongly indicates that some biological or immuneresponse, elicited as part of disease progression, leads toincreased production of soluble IL-6R.
Two different mechanisms for the generation of solubleforms have been described in the case of sIL-6R.`-7 Byproteolytic cleavage (PC), sIL-6R was generated in culturemedium of COS-7 cells transiently infected with full-length
(30 1998 Blackwell Science Ltd360

High production of altered soluble IL-6R in patients with ATL or HAM
IL-6R cDNA.15 In contrast, other studies have shown thatcertain lymphocytic cell lines express two distinct mRNAtranscripts for the IL-6R.'6"7 The smaller mRNA was ident-ified as an alternatively spliced IL-6R, lacking 94 base pairscorresponding to the transmembrane (TM) region. Thisshorter transcript probably results in a soluble product owingto an altered reading frame because the TM region is deleted.This spliced IL-6R isoform, named AS-sIL-6R, was found topossess a unique 10-amino acid sequence (GSRRRGSCGL).Antiserum against this novel peptide was produced and usedto immunoprecipitate an AS-sIL-6R protein from supernatantsof various human T-cell lymphocytotrophic virus-I (HTLV-I )-infected T-cell lines. We detected the soluble IL-6R 45 x 103MW peptide, which was generated through an alternativesplicing mechanism.17
A number of investigators have reported that there areelevated levels of sIL-6R in the serum of patients with auto-immune diseases or certain virus infections. However, thepresence of sIL-6R generated through alternative splicingremains unclear. In this study, we investigated the presence ofAS-sIL-6R protein in human serum and determined the relativeconcentration of AS-sIL-6R relative to total soluble IL-6R inpatients with immune disorders. An enzyme-linked immuno-sorbent assay (ELISA) for AS-sIL-6R was adapted usingmonoclonal antibodies (mAbs). Standard proteins were syn-thesized via a transfer vector carrying cDNA coding forAS-sIL-6R. After transduction into Spodoptera frugiperda-9(Sf-9) cells by homologous recombination with baculovirus,AS-sIL-6R protein was expressed. The level of AS-sIL-6R inthe serum of patients with pathological conditions, includingadult T-cell leukaemia (ATL), HTLV-I-associated myelopathy(HAM), rheumatoid arthritis and hepatic disorders, was theninvestigated.
MATERIALS AND METHODS
Cell culturesThe T-cell line, MT-1, was maintained in RPMI-1640 mediumsupplemented with 10% fetal calf serum (FCS), 100 IU/mlpenicillin and 100 pg/ml streptomycin at 370 in a CO2 incu-bator. Sf-9 cells used for co-transfection and plaque assayswere grown in TC-100 insect medium (Gibco BRL, GrandIsland, NY) supplemented with 10% FCS, minus antibiotics,at 270 in a CO2 incubator.
Construction ofa transfer vector encoding human AS-sIL-6R orIL-6RcDNA coding for AS-sIL-6R was constructed using reversetranscription-polymerase chain reaction (RT-PCR) technol-ogy, described previously,17 with 0 5 gg MT-1 mRNA as tem-plate, for 1 hr at 37°. Oligonucleotide primers used andamplified regions are shown in Fig. 1 and Table 1. Primers6R5-1F and 6R3-4R were located upstream and downstream,respectively, of the extracellular region of IL-6R. The 6R5-2Fand 6R3-2R primers encompassed the TM domain followingthe intracellular region (Fig. 1). Two regions, IL-6REC andIL-6RIC, were amplified (Table 1), PCR products were separ-ated by agarose gel electrophoresis and then extracted. Thesetwo PCR products had 74-bp overlapping sequences locatedfrom positions 937 to 1010 of the reported IL-6R cDNA
numbering.18 A mixture of 1 ng each of IL-6REC and IL-6RICfragments were reamplified using 6R5-lF and 6R3-2R primers.The PCR product, coding for the AS-sIL-6R region, was
separated by agarose gel electrophoresis, extracted, and clonedinto a pGEM-T vector (Promega, Madison, WI). ThepGEM-T plasmid was digested with EcoRI and NotI restric-tion endonucleases and the AS-sIL-6R fragment was clonedinto the EcoRI/NotI-digested baculovirus transfer vectorpVL1393 (PharminGen, CA). As shown in Fig. 1, theAS-sIL-6R construct was cut at nucleotide 1192 with stopcodon TGA, although the coding region of the altered sIL-6Risoform was extended to nucleotide 1334. Conventional IL-6RcDNA was obtained by PCR using primers 6R5-l F and6R3-IR, with plasmid pBSF2R.236 carrying the IL-6R geneas template DNA.18 The PCR product was first cloned into a
pGEM-T vector and then into the EcoRI/NotI-digested bacu-lovirus transfer vector pVL 1393 (PharMingen).
Production ofrecombinant AS-sIL-6R or IL-6R in Sf-9 cellsRecombinant baculoviruses were produced by homologousrecombination, as indicated in the BaculoGold transfectionkit manual (PharMingen). A single recombinant baculoviruswas isolated by a plaque assay and amplified by infecting Sf-9cells at a multiplicity of infection (MOI) of less than one.
Exponentially growing Sf-9 cells were infected with the con-
structed recombinant baculovirus, encoding AS-sIL-6R or
IL-6R, at a MOI of 10-20. After incubation at 270 for 72 hr,cells were sedimented by centrifugation at 1000 g for 10 minand supernatants were stored in aliquots at - 70°. As alteredsIL-6R lacks a TM domain, this isoform was released into theculture medium. The origin of this receptor was confirmed byWestern blot analysis using anti-AS-sIL-6R mAb. ThisAS-sIL-6R recombinant protein was used as the proteinstandard for ELISA determination of altered sIL-6R isoformsin human sera.
Production ofmonoclonal antibodies (mAb) against AS-sIL-6RmAb were produced as described previously."9 Three microg-rams of synthetic peptide comprising amino acid residuesGSRRRGSCGL, was coupled to the carrier protein OVA(15 mg) in 1 5 ml of H20 containing 30mg 1-ethyl-3-dimethylaminopropyl-carbodiimido hydrochloride at room
temperature overnight. Conjugates (100 jl/animal) emulsifiedin complete Freund's adjuvant (CFA) were injected intofootpads of 7-week-old BALB/c mice. The mice were boostedafter 3 weeks with an identical dose and, 3 weeks later, were
finally given 30 gg synthetic peptide only. Three days after thelast immunization, their spleens were removed and the cellsdispersed. Hybridomas were produced by fusion of 5 x 107lymphocytes with 2 x 107 P3U1 myeloma cells in 50%PEG-1 500, according to the protocols provided by BoehringerMannheim (Mannheim, Germany). Hybridomas producingimmunoglobulin G (IgG) were screened by ELISA for reactionwith the immobilized synthetic peptide. Positive cultures were
expanded and cloned directly by limiting dilution using miceperitoneal macrophage as feeder cells. Clones were then scre-
ened for antibody production. Stable antibody-producinghybridoma cells (5 x 106) were transferred into the peritonealcavity of BALB/c mice treated 1 week previously with 1 ml of2,6,10,14-tetramethylpentadecane (Aldrich Chemical Co. Inc.,
© 1998 Blackwell Science Ltd. Immunology, 95, 360-369
361

S. Horiuchi et al.
WI). After 10 days, ascitic fluid was harvested and purifiedwith protein A-sepharose columns.
Immunofluorescence analysisSf-9 cells were sedimented by centrifugation, washed withphosphate-buffered saline (PBS), mounted on a glass slide,air-dried, then fixed by immersion in cold methanol for5 min. mAb (I gg/ml) was applied first for 45 min at 370,followed by washing three times with PBS for 10 min. Anti-IgG fluorescein isothiocyanate (FITC; 5 gg/ml; Cappel) was
(a)6R*-F6R5-IF
S
IL-6R
1
then applied, in an identical procedure, as the second antibodyand indirect immunofluorescence was observed by fluorescencemicroscopy (BX50F, Olympus Optical Co. Ltd, Tokyo,Japan).
Flow cytometric analysisThe binding of IL-6R antibody to Sf-9 cells was analysed byindirect flow cytometry with a fluorescence-activated cell sorter(FACS) Calibur system (Becton-Dickinson Co., MountainView, CA). Cells (5 x 106) were washed with PBS, treated
6R5-2F -*
6R5-3F *>JO
-o 6R3-4R
EC
-4m- -6R3-1R
44- 6R3-2R
44- 6R3-3R
TM IC
I I1075 115857 1407
AS-sIL-6R
3 1334
1066 1161 1189
(b)
226bp -*
132bp -*
- 1057bp
4- 335bp
4- 210bp
4- 79bp
(c)1067
GT TCGGly Ser356
AGA AGA CGT GGAArg Arg Arg Gly
AGC TGC GGGSer Cys Gly
1192I
CTC TGALeu Ehd365
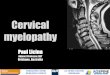
Figure 1. (a) Schematic representation of human soluble IL-6R cDNA. The coding regions are presented as boxes: striped boxes,signal sequence (S); cross-hatched box, transmembrane domain (TM); filled box, generated by a different reading frame.Extracellular domain, EC; intracellular domain, IC. The positions of the primers are shown at the top of the figure. Numbersbelow the boxes show the positions of the nucleotides of IL-6R cDNA according to Yamasaki et al."8 (b) RT-PCR of the alteredIL-6R. The baculovirus transfer vector, pVL1393. coding for the altered or conventional IL-6R gene, was subjected to PCR withthe primers 6R5-3F and 6R3-3R shown in (a). The PCR products were separated by SDS-PAGE. HincII-digested4X174 was usedas a DNA size marker. (c) Altered C-terminal region of AS-sIL-6R. Deletion of 94 base pairs corresponding to the transmembraneregion cause a reading frameshift and, as a result, the C-terminal domain of the AS-sIL-6R contains 10 unique amino acids.
© 1998 Blackwell Science Ltd, Immunology, 95, 360 369
362

High production of altered soluble IL-6R in patients with ATL or HAM 363
Table 1. Oligonucleotide primer sequences and amplified region of IL-6R
Gene segment Primer Sequences Amplified region*
IL-6R 6R5-IFt 5'-CGAATTCACCATGGAGTGGTAGCCGAG EcoRI 1-14076R3-1Rt 5'-TGCGGCCGCCTATCAGGGGAAGAAGTAGTCTGTATT Not!
IL-6RECt 6R5-1F 5'-CGAATTCACCATGGAGTGGTAGCCGAG EcoRI 1-10106R3-4R 5'-TTAGTAGTAAGTGCCTGCAT
IL-6RIC§ 6R5-2F 5'-ACGCCTTGGACAGAATCCAG 937-13346R3-2R 5'-GATGCGGCCGCTGGCTCGAGGTATTGTCAGACCCCA Not!
AS-sIL-6R 6R5-1 F 5'-CGAATTCACCATGGAGTGGTAGCCGAG EcoRI 1-13346R3-2R 5'-GATGCGGCCGCTGGCTCGAGGTATTGTCAGACCCCA Not!
*Numbers show the amplified region of the IL-6R gene reported by Yamasaki et al."9tF, forward; R, reverse.tEC, extracellular region.§IC, Intracellular region.Underlining indicates restriction endonuclease cutting sites.
with 70% methanol for 5 min and then rewashed with PBS.After incubation with 5 jg/ml antibody for 1 hr on ice, fol-lowed by washing with cold PBS, cells were incubated withanti IgG FITC-conjugated antibody (5 tg/ml; Cappel) for1 hr on ice. After a final wash, the fluorescence intensity wasmeasured.
Western blot analysis ofIL-6R proteinAt 72 hr postinfection, the Sf-9 cells were sedimented bycentrifugation at 1000 g for 5 min and culture supernatantswere collected. Aliquots of 300 jl volumes, precleared withprotein A-Sepharose, were mixed with monoclonal or poly-clonal antibody at 2 ptg/ml concentrations. The immune com-plexes were precipitated with 100 pl of protein A-Sepharose4B at 40 overnight using a rotator, and the precipitates weresubjected to sodium dodecyl sulphate-polyacrylamide gel elec-trophoresis (SDS-PAGE) using 10% polyacrylamide gels.Proteins were transferred to nitrocellulose membranes andsubjected to Western blot analysis. The membranes weretreated with antibodies (2 ,ug/ml) for 45 min at room tempera-ture, washed, then stained with a 1: 10 000 dilution of a secondantibody conjugated with horseradish peroxidase (Cappel).Antibody binding was detected by incubation with chemilumi-nescence reagents, as recommended by the manufacturer(NEN Life Science Products, Boston, MA).
Sera andpatientsSera of 12 patients with ATL or 13 patients with HAM, whowere out-patients or admitted to Kyushu University Hospitalfrom October 1991 to November 1994, were studied. Seraobtained from rheumatoid arthritis (RA) patients, hepatitis Bvirus (HBV) or hepatitis C virus (HCV)-infected individuals,persons with elevated levels of alanine aminotransferase(ALT), antinuclear antibody (ANA) or x-fetoprotein (AFP),were out-patients or admissions at the Tokyo Medical andDental University Hospital from February to June 1997. Thesera of HIV-1-infected carriers were obtained from TeikyoUniversity Hospital out-patients collected from February toJuly, 1994. Sera were stored at -80° until assayed. The seraof 27 healthy control individuals (15 males and 12 females;aged 35 to 60 years), were examined for HBV, HCV, HTLV-I
or HIV-1 infections and levels of rheumatoid arthritis factor(RAF), ALT, ANA and AFP were measured.
Detection ofAS-sIL-6R in human serumLevels of AS-sIL-6R in human sera were determined using amodified version of the human sIL-6R immunoassay ELISAkit (DR600; R&D systems, Minneapolis, MN). Briefly, microt-itre plates (Immuno Plate Maxi Sorp; Nunc, Roskilde,Denmark) were coated with mAb 2F3 (20 jg/ml in 0 1 Msodium carbonate buffer, pH 9-0) at 40 for 24 hr, then blockedwith 0 5% bovine serum albumin (BSA)-PBS (pH 7-4) for24 hr. After washing, test samples (200 gl) were added to eachwell and incubated at 370 for 3 hr. Bound AS-sIL-6R was thendetected by commercial horseradish peroxidase (HRP)-conju-gated polyclonal antibody after a further wash. Altered sIL-6Rconcentrations were determined using the baculovirus-expressed form of AS-sIL-6R as a control standard.
RESULTS
Generation of human AS-sIL-6R or IL-6R by usingrecombinant baculovirus
An sIL-6R cDNA variant of the full-length cDNA wasobtained, characterized by a deletion of 94 bp between nucleo-tide positions 1066 and 1161. This was confirmed by PCRwith the primer pair 6R5-3F (nucleotides 967-986:GCTGAGAACGAGGTGTCCAC) and 6R3-3R (nucleotides1170-1192: TCAGAGCCCGCAGCTTCCACGTC; seeFig. 1). As shown in Fig. 1(b) a 226-bp product was generatedfrom the IL-6R template, whereas a l 32-bp product wasdetected from AS-sIL-6R, indicating that recombinant baculo-virus encoding the altered sIL-6R isoform lacked some region.Nucleotide sequence analyses of these PCR products showedthat IL-6R did not display any deletion or insertion andconfirmed that AS-sIL-6R indeed lacked a 94-bp nucleotideregion. This in-frame deletion resulted in a cDNA with adifferent reading frame coding for an IL-6R protein lackingthe TM domain, and with a termination codon at nucleotidepositions 1190-1192. A mature protein with 365 amino acidresidues was thus produced, differing from IL-6R at the
©O 1998 Blackwell Science Ltd. Immunology, 95, 360-369

S. Horiuchi et al.
C-terminal end by 10 amino acid residues (GSRRRGSCGL)(Fig. Ic).
Monoclonal antibody reactivity and cytoplasmicimmunofluorescence analysis of Sf-9 cells
Four stable mAbs were produced and specific AS-sIL-6Rrecognition was investigated by cytoplasmic immunofluores-cence analysis. As expected, mAb 2F3 (IgG type) stained onlySf-9 cells carrying AS-sIL-6R cDNA (Fig. 2a), but not Sf-9cells transfected with conventional IL-6R cDNA (Fig. 2b). Incontrast, polyclonal antibody AB-277-NA (R&D Systems)reacted with Sf-9 cells transfected with the cDNA of AS-sIL-6R(Fig. 2c) or IL-6R (Fig. 2d). IgG-type mAbs ( IF 10 and 4C 12)and the IgM-type mAb (1D9) recognized Sf-9 cells carrying
the AS-slL-6R gene, similarly to mAb 2F3, but did not reactwith Sf-9 cells transfected with the IL-6R gene (data notshown).
Next, confirmation of mAb specificity was obtained byFACScan analysis. As shown in Fig. 3(a), mAb 1D9 reactedwith Sf-9 cells carrying AS-sIL-6R but not IL-6R (Fig. 3b).The polyclonal antibody AB-227-NA recognized Sf-9 cellscarrying either the altered isoform or conventional IL-6R(Fig. 3b, data not shown for AS-sIL-6R). In the case of alteredsIL-6R, virtually the same results were obtained with mAb
Figure 2. Staining of permeabilized Sf-9 cells transfected with cDNAencoding the AS-sIL-6R or the full-length IL-6R. Indirect immuno-fluorescence analysis of Sf-9 cells is shown. (a) and (c), Sf-9 cellstransfected with AS-sIL-6R cDNA. (b) and (d), Sf-9 cells transfectedwith IL-6R cDNA. (a) and (b), stained with mouse antihumanAS-sIL-6R mAb 1D9; (c) and (d), stained with goat antihuman IL-6Rpolyclonal antibody AB-277-NA. Second antibodies used were FITC-conjugated goat antimouse IgG (a, b) or rabbit antigoat IgG (c, d).
6
cJ(3)a)
coa1)er
(a) AS-slL-6R
PBS 1D9
101 102 103 104
(b) IL-6R
1 D9 AB-227-NA
10° 101 102 103 104
Fluorescence intensity
Figure 3. Flow cytometric analysis of Sf-9 cells transfected with thecDNA of AS-sIL-6R (a) or IL-6R (b). mAb ID9 or goat antihumanIL-6R polyclonal antibody AB227-NA were used as described in thelegend to Figure 2.
lFIO, 2F3 and 4C12 (data not shown). The data shows thatthese four mAbs specifically recognized AS-sIL-6R only.
Production of AS-sIL-6R and IL-6R proteins from Sf-9 cells
mAbs 1D9 and 1 F 10, with established specific reactivityagainst the AS-sIL-6R (GSRRRGSCGL) peptide, were
employed to detect altered sIL-6R and IL-6R proteins pro-duced in Sf-9 cells. The culture supernatant of Sf-9 cellscarrying AS-sIL-6R was treated first with mAb D9 and thenwith 1F10, resulting in the immunoprecipitation of a 45 x 103MW polypeptide (Fig. 4, lane 1). In contrast, mAbs 1D9 and1FlO did not react with Sf-9 cells carrying the conventionalpIL-6R (Fig. 4, lane 2). Commercial polyclonal antibody,AB-227-NA, reacted to a similar extent with polypeptides ofmolecular weights 45 x 103 and 48 x 103 from the culturesupernatant of Sf-9 cells either carrying either the alteredisoform or conventional IL-6R proteins (Fig. 4, lanes 4 and5). These three antibodies did not react with Sf-9 cell culturesupernatant from the uninfected cells (Fig. 4, lanes 3 and 6).Immunoprecipitation experiments with cell lysate of the Sf-9
1998 Blackwell Science Ltd. Immunology, 95, 360-369
364

High production of altered soluble IL-6R in patients with ATL or HAM
1 2 3 4 5 6
MWx1O3
58-0 -*.
48.5 -*
AS SIL-6R -
36-5 --P
.. ..
Antibody + ID9, l F10
4- PC-sIL-6R
4- AS-slL-6R
AB-227-NA
Figure 4. Detection of the altered sIL-6R in recombinant virus-infected Sf-9 cells. At 72 hr post-transfection, the supernatants weresubjected to immunoprecipitation/Western blot analysis (as described in the Materials and methods). The proteins electrotransferredto nitrocellulose membranes were probed with anti-IL-6R antibodies, and antibody binding was demonstrated by incubation withchemiluminescence reagents. Lanes 1-3, proteins were immunoprecipitated with 1 D9 antibody and nitrocellulose membrane stainedwith IFIO antibody; lanes 4-6, antibody AB-227-NA was used for immunoprecipitation and staining of the nitrocellulosemembrane.
cell-carrying recombinant baculovirus also gave similar results(data not shown). These experiments confirmed Sf-9 culturesas suitable production sources for AS-sIL-6R and IL-6Rproteins.
Differential quantification of AS-slL-6R and PC-sIL-6R inserum by ELISA
Initially, the sensitivity of mAb 2F3-coated ELISA plates wasestablished using supernatants from Sf-9 insect cells infectedwith baculovirus carrying AS-sIL-6R or IL-6R cDNA. Variousdilutions were assayed and optical density measurements at450 nm increased linearly from 0-2 ng/ml (lower detectionlimit) to 5 ng/ml (data not shown). mAb 2F3-coated platesreacted with AS-sIL-6R, but not with conventional IL-6R orcommercial sIL-6R standard peptides. On the other hand,with commercial anti IL-6R antibody-coated plates (DR600)both altered and conventional IL-6R were recognized (datanot shown). After establishing the sensitivity of the alteredIL-6R ELISA, we examined human plasma samples for thepresence of altered sIL-6R.
Control sera from healthy individuals of both genders,with a variety of ages, were assayed for AS-sIL-6R by2F3-coated ELISA plates. The serum level of AS-sIL-6R for21-30-year-old individuals was 13-1 + 10-3 ng/ml (mean + SD).This decreased with increasing age, reaching 74 ±4+7 ng/mland 45 + 2 1 ng/ml, respectively, for the 31-40 years and41-60 years age-groups. The control individuals were allnegative for HTLV-I antibody. No differences were found inthe serum level of AS-sIL-6R between females and males. Asthe patients with ATL and HAM were over 41 years old, thesera from healthy individuals in the 41-60 year age-group,
© 1998 Blackwell Science Ltd, Immunology, 95, 360-369
was used as the age-matched reference control. Resultsobtained are shown in Figs Sal and 5a2 according to AS-sIL-6R levels. The average level of AS-sIL-6R was 4-5 + 2 1 ng/ml(mean+SD) in healthy individuals (Fig 5a). By contrast, theserum levels of AS-sIL-6R were elevated significantly inpatients with ATL (Fig. 5b) averaging 28-7+204ng/ml(mean+SD, P<00001) and 27-5+121 ng/ml (P<0-0001) inthose with HAM (Fig. Sc). The serum levels of patients withATL or HAM were 64 or 6-1 times greater than that ofhealthy individuals, respectively. The ranges of serumAS-sIL-6R in patients with ATL (81-6-9-2 ng/ml) or HAM(48-3-10A4 ng/ml) were extremely diverse compared with thelow and narrow ranges found in healthy individuals(7-2-1-2 ng/ml). As serum levels of AS-sIL-6R were elevatedin patients with ATL or HAM, we also examined levels inHTLV-I-infected carriers. However, serum levels of AS-sIL-6Rwere not increased (2-3-8-6 ng/ml). On the other hand, theserum levels of PC-sIL-6R did not differ significantly inpatients with ATL (236 + 28 1 ng/ml, mean + SD) or HAM(341 + 30 8 ng/ml) compared with normal individuals(29-6+11-7 ng/ml).
We also measured the serum levels of AS-sIL-6R in somepatients with autoimmune disease and hepatic disordersbecause high serum levels of sIL-6R in these patients havebeen described previously.58'20 Sera with elevated levels ofALT (>100 U/ml), ANA (>40 times), RAF (>100 U/ml)and AFP (>400 ng/ml) were additionally tested. The sera ofhealthy control persons were measured for ALT, ANA, AFPand RAF, and sera which exhibited abnormal levels wereexcluded as healthy controls. The sera of 27 normal healthyindividuals (over 35 years of age) were used as age-matchedreference controls. The control individuals were all negative
365

S. Horiuchi et al.
(al)
I AS-slL-6R
U PC-slL-6R
I I I I I I II7
1 2 3 4 5 6 7 8 9
I.
I
(a2)
10 11 12 13 14 15 16 17 18
Sample no. healthy individuals
(b)
80 -
60 -
40 -
I1 2 3 4 5 6 7 8 9
Sample no. ATL patients
28-7
23.6 20
10 11 12
(C)
I I34-1
27.5
1 2 3 4 5 6 7 8 9 10 11 12 13
Sample no. HAM patients
Figure 5. (a) Serum levels of soluble IL-6R in healthy individuals. The squares with arrows represent the mean value of AS-sIL-6R(4 5 ng/ml) or PC-sIL-6R (29-6 ng/ml), respectively. The serum levels represent an average of two independent measurements foreach sample. The results obtained are arranged in respect to decreasing AS-sIL-6R concentrations. (b) Serum levels of sIL-6R inATL patients. The mean value of serum levels for AS-sIL-6R or PC-sIL-6R are 28-7 ng/ml and 23-6 ng/ml, respectively. (c) Serumlevels of sIL-6R in HAM patients. The mean value of serum levels for AS-sIL-6R or PC-sIL-6R are 34 1 ng/ml and 27-5 ng/ml,respectively.
C 1998 Blackwell Science Ltd, Immunology, 95, 360-369
80 -
60 -
E
0)
-J(a
40 -
20 -
29-6
4-5
80 -
E
-oGo
60 -
40 -
20 -
r
I77 P.
7
A
PI 77
7
7 7
"I11
I
r 7
-1I I II-
11
366

High production of altered soluble IL-6R in patients with ATL or HAM
for HIV-1, HBV and HCV. As shown in Fig. 6(a), the levelsof AS-sIL-6R were significantly higher in ALT(14-0+7-1 ng/ml, P<0-0001), ANA (9-8 + 5-6 ng/ml,P<0-0001), AFP (9-4+8-1 ng/ml, P<0-0001) and RAF sera(7 5 + 2-9 ng/ml, P= 0 06), as compared with control sera fromhealthy individuals (4 7 + 2-6 ng/ml). In particular, in patientswith elevated levels of ALT, the serum levels of AS-sIL-6Rwere higher than healthy controls in all patients except forone. Enhanced release of sIL-6R by HIV-1 infection haspreviously been reported.8 Therefore, we assessed serum levelsof AS-sIL-6R in nine HIV-1-infected carriers who were over35 years old. The ratio of CD4/CD8-positive cells in the HIV-1-infected asymptomatic carriers were 0-33-0-76. However,
(a)
40 -
30 -
20 -
15'
10-
5.-
P=0-06
P<0.0001P<0.0001
P<0.0001
00
80-4--
0 14.0
* c80
*Is
t4.7O
0
00
8 0o o°o 0
000°O0 0°°9-8 9.4
800 c00
0
0
00
075
0
Healthy ALT ANA AFP RAFn=27 n=19 n=18 n=16 n=23
(b)
NS
NS
NSI
0
* 0088 00
g}0 5-1
8°Healthy HIV-1 HBVn=27 n=9 n=15
Patient groups
000 .0--000 5.0
0
0
HCVn=8
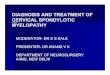
Figure 6. (a) AS-sIL-6R in the sera of normal healthy individuals or
patients. The serum levels of AS-sIL-6R were measured in patientswith elevated levels of alanine aminotransferase (ALT), antinuclearantibody (ANA), ca-fetoprotein (AFP) and rheumatoid arthritis factor(RAF). n, number of serum samples. (b) HIV-1, HBV or HCV-infected carriers.
serum levels of AS-sIL-6R in these asymptomatic carriers werenot raised (Fig. 6b), indicating that the AS-sIL-6R may notcontribute to elevation of sIL-6R in HIV-1 infection. Elevatedlevels of AS-sIL6R may be involved in hepatic disorders, asindicated by the observations in patients with higher levels ofALT or AFP. We also examined AS-sIL-6R levels in HBV orHCV-infected persons with unknown clinical status. The levelsof AS-sIL-6R were not increased (Fig. 6b).
DISCUSSION
The principal aim of this study was detection and differentialquantification of alternatively spliced sIL-6R protein fromhuman sera. Two different mechanisms have been describedfor the generation of sIL-6R: proteolytic cleavage of mem-brane-bound receptor or alternative splicing of IL-6RmRNA.5'-7 Soluble IL-6R binds to its ligand and inducescellular responses by associating with gpl 30, thus acting as anIL-6R agonist. Soluble IL-6R is thus of potential importancein T-cell abnormalities, such as ATL and acquired immunedeficiency syndrome (AIDS).8"' It also participates in thecytokine network associated with diseases, such as monoclonalgammopathies,5 systemic lupus erythematosus,20 osteoclastdifferentiation12 and rheumatoid arthritis.7 Therefore, we stud-ied the presence of AS-sIL-6R and sought to determine therelative contribution of the two IL-6R isoforms to the totalplasma fractions of sIL-6R under various pathophysiologicalconditions. Accordingly, we constructed an alternativelyspliced IL-6R cDNA, cloned into a baculovirus transfer vector,and examined its expression in Sf-9 insect cells. Specificity ofaltered IL-6R mAb were confirmed by immunofluorescenceand flow cytometry analyses. We subsequently produced anAS-sIL-6R isoform as a standard protein for ELISA andsuccessfully measured human AS-sIL-6R serum levels.
Our modified ELISA system demonstrated an efficientcapacity for quantification of alternatively spliced solubleIL-6R in the sera of patients with viral hepatitis, hepatoma orautoimmune disease. Although AS-sIL-6R was also found inthe plasma of healthy persons, levels were significantly elevatedin patients with ALT, AFP, ANA or RAF. In vivo and in vitrostudies imply that the sIL-6R/IL-6 complex system may chap-erone the cytokines and widen the spectrum of IL-6R-respon-sive cells to those that do not express endogenous IL-6RmRNA.1-14 Moreover, the role of sIL-6R has been recognizedin patients with rheumatoid arthritis. The elevated levels ofIL-6 and sIL-6R form a complex that causes bone destructionand induces osteoclast formation in synovial fluids of thesepatients.12 This suggests that the presence of high levels ofAS-sIL-6R in patients with rheumatoid arthritis, hepatoma orautoimmune disease may also be involved in diseaseprogression.
We have shown previously that production of alteredsIL-6R mRNA is associated with T-cell abnormalities such asHTLV-I-infected cells, MT-1, MT-2 and MT-4.'7 Consistentwith the production of altered sIL-6R mRNA in peripheralblood mononuclear cells (PBMC) of patients with ATL, theserum level of AS-sIL-6R in patients with ATL was 6-4 timesgreater than that of healthy individuals. The precise cells ororgans that predominantly produce AS-sIL-6R, remainunclear. However, it may be noteworthy that monoclonal oroligoclonal integration of HTLV-I is detected in patients with
C 1998 Blackwell Science Ltd, Immunology, 95, 360-369
367
40 -
30 -
20 -
15 -
10 -
5-
ECD
-j
CD)cn

368 S. Horiuchi et al.
ATL, as opposed to polyclonal integration in HAM. ATL isa consequence of malignant clone development. Perhaps, inpatients with ATL, HTLV-I-integrated monoclonal or oligo-clonal T cells, at least in part, play an important role forAS-sIL-6R production.
It has been reported that optional mRNA splicing eventsfrom a single mRNA precursor generates increased codingcapacity with overlapping reading frames.2' The alternativeRNA processing has been shown to be mediated by RNA-binding proteins that do not participate in the general splicingmachinery.21'22 HTLV-I Rex protein is known to splice relatedproteins during gag, pol and env gene RNA expression. It mayplay a role in cellular RNA expression as well as in the virallife cycle.2324 Indeed, alternative splicing for IL-2R a-chainor IL-6R are observed in HTLV-I-infected T-cell lines orPBMC of patients with ATL.17'25 Virtually nothing is knownas yet about the physiological roles of HTLV-I in the enhance-ment of differential processing site selection. The promotionof differential splicing is not restricted to HTLV-I-infectedT cells but is also observed in normal PBMC upon activationwith phytohaemagglutinin (PHA).17 Although perturbation inRNA processing may not be a general phenomenon in manycellular genes, we provide evidence that a limited number ofgenes, including the IL-2Rcx-chain or IL-6R, possess optionalRNA-processing mechanisms. These splicing alterationsappeared to be concentrated at the site adjacent to the TMregion. Genomic sequences around the TM region are themost likely targets of regulatory proteins that may be inducedor activated by HTLV-I infection. The mechanisms of alterna-tive splicing in IL-6R mRNA in HTLV-I-infected cells requiresfurther investigation.
In this study, we detected alternatively spliced solubleIL-6R protein in patients using an ELISA for AS-sIL-6Rprotein. AS-sIL-6R proteins were previously detected in thesupernatant of HTLV-I-infected cell lines.17 We have demon-strated that AS-sIL-6R is indeed present in the sera of patientswith ATL or HAM at significantly higher levels than in healthyindividuals. In vitro and in vivo evidence thus indicates thatHTLV-I plays an important role in the mechanism for alterna-tive splicing of mRNA of IL-6R.
ACKNOWLEDGMENTS
We thank T. Taga, Tokyo Medical and Dental University, for provid-ing plasmid pBSF2R.236, F. Matsumoto and C. Sato, Tokyo Medicaland Dental University, for providing patient sera and N. Kurosakifor technical advice on flow cytometric analysis. This work wassupported by grants from the Ministry of Public Health and Welfare,the Ministry of Biotechnology Science in Japan, the Japan HealthSciences Foundation, Priority Areas from the Ministry of Education,Sports and Culture, CREST (Core Research for Evolutional Scienceand Technology) of the Japan Science and Technology Corporation(JST) and the Program for Promotion of Fundamental Studies inHealth Sciences of the Organization for Drug ADR Relief, R&DPromotion and Product Review of Japan.
REFERENCES
1. TAGA T., HIBI M., HIRATA Y. et al. (1989) Interleukin-6 triggersthe association of its receptor with a possible signal transducer,gpl 30. Cell 58, 573.
2. PAONESSA G., GRAZIANI R., SERIo A.D. et al. (1995) Two distinctand independent sites on IL-6 trigger gp 130 dimer formation andsignaling. EMBO J 14, 1942.
3. GAULDIE J., RICHARDS C., HARNISH D., LANSDORP P. &BAUMANN H. (1987) Interferon 02/B-cell stimulatory factor type2 shares identity with monocyte-derived hepatocyte-stimulatingfactor and regulates the major acute phase protein response inliver cells. Proc Natl Acad Sci USA 84, 7251.
4. IKEBUCHI K., WONG G.C., CLARK S.C. et al. (1987) Interleukin-6enhancement of interleukin-3-dependent proliferation of multi-potential hemopoietic progenitors. Proc Natl Acad Sci USA84, 9035.
5. GAILLARD J.P., BATAILLE R., BRAILLY H. et al. (1993) Increasedand highly stable levels of functional soluble interleukin-6 receptorin sera of patients with monoclonal gammopathy. Eur J Immunol23, 820.
6. OHTANI K., NINOMIYA H., HASEGAWA Y. et al. (1995) Clinicalsignificance of elevated soluble interleukin-6 receptor levels in thesera of patients with plasma cell dyscrasias. Br J Haematol 91, 116.
7. BENEDETTI F.D., MASSA M., PIGNATTI P. et al. (1994) Serumsoluble interleukin 6 (IL-6) receptor and IL-6/soluble IL-6 recep-tor complex in systemic juvenile rheumatoid arthritis. J Clin Invest93, 2114.
8. HONDA M., YAMAMOTO S., CHENG M. et al. (1992) Human solubleIL-6 receptor: its detection and enhanced release by HIV infection.J Immunol 148, 2175.
9. HOYLAND J.A., FREEMONT A.J. & SHARPE P.T. (1994)Interleukin-6, IL-6 receptor, and IL-6 nuclear factor geneexpression in Paget's disease. J Bone Mineral Res 9, 75.
10. ROSE-JOHN S. & HEINRICH P.C. (1994) Soluble receptors forcytokines and growth factors: generation and biological function.Biochem J 300, 281.
11. MURAKAMI-MORI K., TAGA T., KISHIMOTo T. & NAKAMURA S.(1996) The soluble form of the IL-6 receptor (sL-6Roc) is a potentgrowth factor for AIDS-associated Kaposi's sarcoma (KS) cells;the soluble form of gpl3O is antagonistic for sIL-6Rct-inducedAIDS-KS cell growth. Int Immunol 8, 595.
12. UDAGAWA N., TAKAHASHI N., KATAGIRI T. et al. (1995) Interleukin(IL)-6 induction of osteoclast differentiation depends on IL-6receptors expressed on osteoblastic cells but not on osteoclastprogenitors. J Exp Med 182, 1461.
13. MIHARA M., MORIYA Y., KISHIMOTo T. & OHSUGI Y. (1995)Interleukin-6 (IL-6) induces the proliferation of synovial fibro-blastic cells in the presence of soluble IL-6 receptor. Br J Rheum34, 321.
14. HIROTA H., YOSHIDA K., KISHIMOTo T. & TAGA T. (1995)Continuous activation of gpl30, a signal-transducing receptorcomponent for interleukin 6-related cytokines, causes myocardialhypertrophy in mice. Proc Nati Acad Sci USA 92, 4862.
15. MULLBERG J., OBERTHUR W., LOTTSPEICH F. et al. (1994) Thesoluble human IL-6 receptor: mutational characterization of theproteolytic cleavage site. J Immunol 152, 4958.
16. LUST J.A., DONOVAN K.A., KLINE M.P. et al. (1992) Isolation ofa mRNA encoding a soluble form of the human interleukin-6receptor. Cytokine 4, 96.
17. HORIUCHI S., KOYANAGI Y., ZHOU Y. et al. (1994) Solubleinterleukin-6 receptors released from T cell or granulocyte/macro-phage cell lines and human peripheral blood mononuclear cellsare generated through an alternative splicing mechanism. EurJ Immunol 24, 1945.
18. YAMASAKI K., TAGA T., HIRATA Y. et al. (1988) Cloning andexpression of the human interleukin-6 (BSF-2/IFNt2) receptor.Science 241, 825.
19. HOLMDAHL R., MORAN T. & ANDERSSON M. (1985) A rapid andefficient immunization protocol for production of monoclonalantibodies reactive with autoantigens. J Immunol Methods 83, 379.
©) 1998 Blackwell Science Ltd, Immunology, 95, 360-369

High production of altered soluble IL-6R in patients with ATL or HAM 369
20. GABAY C., SILACCI P., GENIN B. et al. (1995) Soluble interleukin-6receptor strongly increases the production of acute-phase proteinby hepatoma cells but exerts minimal changes on human primaryhepatocytes. Eur J Immunol 25, 2378.
21. MANIATIs T. (1991) Mechanisms of alternative pre-mRNA splic-ing. Science 251, 33.
22. MArrOX W., RYNER L. & BAKER B.S. (1992) Autoregulation andmultifunctionality among trans-acting factors that regulatealternative pre-mRNA processing. J Biol Chem 267, 19023.
23. MARUYAMA M., SHIBUYA H., HARADA H. et al. (1987) Evidence
for aberrant activation of the interleukin-2 autocrine loop byHTLV-I-encoded p4Oc and T3/Ti complex triggering. Cell 48, 343.
24. INOUE J., SEIKI M., TANIGUCHI T., TsuRu S. & YOSHIDA M. (1986)Induction of interleukin 2 receptor gene expression by p40xencoded by human T-cell leukemia virus type 1. EMBO J 5, 2883.
25. HORIUCHI S., KOYANAGI Y., TANAKA Y. et al. (1997) Alteredinterleukin-2 receptor a-chain is expressed in human T-cell leu-kaemia virus type-I-infected T-cell lines and human peripheralblood mononuclear cells of adult T-cell leukaemia patients throughan alternative splicing mechanism. Immunology 91, 28.
© 1998 Blackwell Science Ltd, Immunology, 95, 360-369