Embed Size (px)
Citation preview

POSTGRAD. MED. J. (1964), 40, 549
TREATMENT OF TUBERCULOSIS OF THE KNEEF. HARWOOD STEVENSON, M.D., M.R.C.P.
Consultant Physician, Royal National Orthopadic Hospital, and the Institute of Orthopadics, London.
A FEW general observations are pertinentbefore considering the treatment of tubercu-losis of the knee in its different clinicalmanifestations.
1. Tuberculosis of a joint implies thatblood-stream dissemination following primaryinfection has occurred. Full investigation of thepatient with regard to the lungs, the urineand other bones and joints is thereforeessential.
2. Monarticular rheumatoid arthritis inadults or children is by no means uncommonand may exist in a child who already has apositive Mantoux, so that the diagnosis ofan early case without bone destruction mayrequire considerable investigation.
3. The range of clinical material and theincidence vary much in different parts of theworld. In England today tuberculosis of theknee is rarely seen, is frequently seen earlyand has become relatively much less commonin children. In many countries where thereare still numbers of sputum-positive patientsand a lower standard of living and medicalcare, and where communications are difficult,many patients and more with advanceddisease are seen.
4. The results of some of our diagnostictests vary with the race of the patient. Thisis particularly true of the sedimentation rate.Natives of Britain with active skeletaltuberculosis commonly have a sedimentationrate which is, if raised at all, between 15 and35 mm. in the first hour. Much higher figuresthan this in a spinal lesion raise a strongsuspicion that the disease is staphylococcaland not tuberculous; similar high figures in apatient with a single joint affected wouldsuggest rheumatoid disease. However whenwe meet patients in this country from Asia,Africa or the West Indies with a closedsingle tuberculous lesion, they commonly havea sedimentation rate in the higher range whenfirst seen, e.g., 50-70 mm. in the first hour.
5. Radiographically it is most important totake strictly comparable views of the soundknee, if possible on the same film, so as toaid the detection of minor degrees of
osteoporosis and changes in texture of thecancellous bone.
Before the era of antibiotics it was taughtthat spontaneous or deliberate arthrodesis wasthe only safe end-result in tuberculosis of theknee. Usually despite prolonged rest varyingdegrees of bone destruction occurred, withfibrous adhesions and restriction of move-ment. Such joints were always at risk ofre-activation by minor degrees of trauma. Thenatural resistance of the human body nowaided by antibiotics may ultimately producequiescence of the lesion. We have thencreated a desert for the mycobacteria inhabit-ing the lesion, but he would be bold whoasserted that nowhere in the areas of"healed" and probably fibrotic tissue werethere no lurking bacteria or their coccalforms. Blood and effusion provide the idealwatering of the desert, and it is for thisreason that the tearing of an adhesion in ajoint with limited movement can so easilyre-activate tuberculosis.
But with the new drugs, with or withoutoperation, we can commonly hold the situationif a diagnosis is made early enough, and thisgloomy outlook is no longer with us.
Clinical TypesClinically cases of tuberculosis of the knee
can be divided into a number of groupsdepending upon the stage the disease hasreached before diagnosis:
1. Effusion into the joint, with perhapssome thickening of the synovial membrane,with radiologically a good joint space and noevidence of a bone focus or any bone erosionor destruction; these joints commonly have avery good or even normal range of flexion,restricted if at all by the size of the effusion.
2. Little or no effusion, in a joint with along history, with varying degrees of thicken-ing and fibrosis of the synovial membrane,possibly with adhesions preventing full flexion,but still with a reasonably wide joint spaceand no radiological evidence of bonedisease.
Protected by copyright.
on January 30, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.467.549 on 1 Septem
ber 1964. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
3. Those with synovial disease and a bonefocus within the tibia, femur or patella. Sucha focus presumably must have at leastmicroscopic communication with the jointspace but this type still has a reasonable jointspace and radiologically intact joint surfaces.
4. Finally, with a diminished joint space,considerable destruction of the bone surfacesand very considerable loss of range of move-ment.
Clearly there are various gradationsbetween one group and the next.
InvestigationsProof of tuberculosis of the knee may be
obtained by inguinal gland biopsy, but thereis so little damage from a limited anteriorsynovial biopsy that this is preferable, andbesides it is more certain. It is importanthowever not to rely upon any one methodof investigation of the biopsy material. Thehistology may be non-specific and doubtful andmust be aided by Lowenstein culture andinserting some of the material into a musclepouch in the leg of a guinea pig. Examinationof unstained sections of the histological materialwith ultra-violet light may show fluorescingmycobacteria. Naturally a patient will not beconsidered possibly tuberculous unless knownto have a positive Mantoux or Heaf test; withan active lesion it is likely that they will bepositive 1 in 5000 or 2 to 4+, according to thetest used, rather than only weakly positive.
Principles of ChemotherapyExperience has shown that six to twelve
months chemotherapy is adequate in mostorthopaedic lesions, even though two yearschemotherapy is known to be the minimumnecessity in chest and renal lesions. Theobtaining of material for culture and sensitivitychecks against the three main drugs, strepto-mycin, PAS and INAH is obviously of greatimportance, particularly when there is thepossibility or likelihood of a patient havingreceived the primary infection from a personwith resistant organisms. In the first instancetriple drug chemotherapy is advisable, becausethe chance of a mutant developing whichis resistant to all three drugs is very slight.
Various antibiotic combinations have beenused. Our own preference has been for strepto-mycin 1 g. once a day for three months, andthereafter 1 g. three times a week; smallerdoses in proportion of course are given forchildren, for whom we have used 0.75 g.
between the ages of 5 and 10 years, below5 years 0.5 g. and below 2 years 0.25 g. PAS5 g. three times a day for an adult seemsadequate from the many trials which havebeen done, and in any case this is as much asmost patients can tolerate. There is someevidence from the M.R.C. trials in Madras(1960) that INAH is best given in one singledose daily in order to give a peak blood leveland that 300 mg. is an adequate dose evenfor patients who metabolise INAH rapidly.The dosages of PAS and INAH are not changedthroughout the course. Most of our patientsreceive a total of six months to nine monthsof treatment. If for any reason such as oto-toxicity or other difficulty the streptomycin hasto be stopped, PAS and INAH are continued.At that dose of INAH it is wise to givepyridoxine (vitamin B6) 20 mg. once daily toguard against the excess pyridoxine excretionduring INAH therapy which can result in apolyneuritis.
Antibiotics for use when any of the standardthree cannot for some reason be used or ifthe organism is known to be resistant to adrug are:-
(a) Viomycin: Adult dose 1 g. b.d. i.m.on two days a week, i.e., 4 g. a week. It ispotentially toxic to the 8th nerve so should notreplace streptomycin if that drug has beenstopped because of ototoxicity.
(b) Pyrazinamide: Is a potentially hepato-toxic drug but forms a very good combinationwith INAH. Adult dosage 0.5 g. t.d.s but aserum G.P. transaminase level should bechecked weekly or at least fortnightly. Any riseto over 40 Karmen units/ml. gives warning ofimpending liver damage before the developmentof jaundice and the drug of course should beimmediately and permanently stopped.
(c) Ethionamide in oral dosage 0.25 g. b.d.to q.d.s. varying with body weight. Some gastro-intestinal intolerance can occur.All these three drugs, like all anti-tuberculousdrugs, should of course not be used alone.
Intra-articular Chemotherapy. Whether thereis an effusion it is easy to use intra-articularchemotherapy. The presence of an effusion isstressed, because if there is only a thickenedcedematous or fibrotic synovium the insertionof a needle and the injection of fluid willproduce bleeding and trauma and possible re-activation. A needle into the joint space doesno harm. The effusion can be removed andthen another syringe with 1 g. of streptomycinattached to the same needle for the injection.
550 September, 1964P
rotected by copyright. on January 30, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.467.549 on 1 S
eptember 1964. D
ownloaded from

STEVENSON: Treatment of Tuberculosis of the knee
When this is done twice a week-instead of theintramuscular injection on these days- theeffusion tends to persist, but in our experienceat the end of three months when one ceases theintra-articular injections and simply continuesthe intramuscular injections three times aweek the effusion rapidly clears.
In patients with minimal and purely synovialinvolvement with effusion, good joint space,and good movement, the disease may havebeen present for a number of years, with ahistory of repeated effusions following minortrauma but clearly the degree of infectionis still minimal. These joints stiffen rapidly ifsplinted in plaster casts. They require chemo-therapy and do well with intra-articularstreptomycin. The presence of the effusionfacilitates this. These patients should alwaysbe allowed free movement in bed unless tooyoung to obey orders not to stand up, when aThomas's splint for two or three months mayhave to be used.Some case histories with comments will
illustrate the principles of treatment in theseveral groups:Type 1. Synovial involvement with effusion:
W.L., aged 43, male. T.B. glands treated 1953 with50 injections of streptomycin and six months PASand INAH. June 1963: one year history of ache inright knee, six months swelling, three months increas-ing pain and stiffness. Acid fast bacilli in the synovialfluid and culture positive: sensitive PAS and INAHbut slightly resistant to streptomycin at 4 mg./ml.A plaster cast was applied in another hospitalwhen flexion was possible to 90 degree. When theplaster was removed after one month, he couldhardly flex the knee at all. There was an effusionbut radiologically the knee was normal apart fromslight osteoporosis.He then lay free in bed without plaster. 1 g.
streptomycin intra-articularly twice weekly and onother days 1 g. intramuscularly. Oral PAS 5 t.d.s.and INAH 300 mg. once daily.
After two weeks flexion to 40 degrees, and at twomonths, 70 degrees. After three months, sterptomycinPAS and INAH continued but with streptomycinintramuscularly only and reduced to three times aweek. At the end of four months, streptomycinstopped because of slight deafness and PAS andINAH continued for a further six months.At five months flexion to 90 degrees, and at seven
months flexion 100 degrees with full extension. Theeffusion cleared after the end of the intra-articularcourse. At fourteen months: no effusion, no symptoms,flexion 120 degrees, extension full with full activity.
Stevenson, Cholmeley and Jory (1958)reported that of 24 patients with purely syno-vial disease 14 ended with full mobility, sevenwith 95 to 135 degree of flexion and anothertwo with 70 to 90 degree. The majority ofthese did not receive intra-articular chemo-therapy, but with an effusion intra-articular
streptomycin is simple, safe and helpful. Inthe above case particularly, one felt that thehigher local concentration of streptomycin wasvaluable in combating an organism moderatelyresistant to it.We have seen several patients in this group
recently who have lost much of their flexionmovement as a result of unnecessary fixationby plaster of Paris; not all recovered as well asthis man.
Type 2. Thickened fibrotic synovium with little orno effusion but a reasonable joint space:These joints commonly have a very limited range
of flexion and are consequently in danger fromminor trauma when walking on irregular surfacesor on stairs, etc. If the range of movement does notimprove in the first two months of chemotherapywith bed rest without splinting, then even if thereis no evidence of involvement of the bone, anarthrotomy with anterior synovectomy may give theonly chance of increasing joint function.Case History. Synovial disease, thickened synoviumwithout effusion:
B.M., aged 14, male. In September, 1962 he waskicked on the knee, which became swollen and tender.In April, 1963 the knee was still swollen andbeginning to stiffen in the morning and he waslimping. In June, 1963 the knee was aspirated and abiopsy in September was histologically positive.He was put into a plaster cylinder and on admissionto hospital in October, 1963 had only 20 degrees ofmovement, no effusion and a thick boggy synovialmembrane but a mobile patella. Intra-articularstreptomycin was not attempted but he was givendaily 1 g. i.m. with oral INAH 300 mg. once dailyand PAS 5 g. t.d.s. He was allowed freedom inbed. The range of flexion rapidly improved to 80degrees and by December, 1963 to 135 degrees. Inthe second three months triple drug chemotherapywas continued with the streptomycin reduced tothree times weekly.
Open operation:At this point it is pertinent to discuss the
place of open operation, synovectomy, curet-tage of juxta-articular bone lesions and ingeneral what has been also called debridementof the diseased joint. One of the best paperson this subject is that of M. C. Wilkinson(1962). He described 73 cases of tuberculosis ofthe knee treated by chemotherapy and in 39cases synovectomy with debridement wasjudged necessary and performed. Wilkinsonstates that with loss of joint space and marginalerosions or bone destruction within the jointopen operation is necessary. He first gives sixto ten weeks treatment without intra-articularstreptomycin and before and after operationuses a Thomas's splint until the joint is cooland the swelling almost gone. His operativeprocedure is to remove the diseased synoviumfrom the anterior and posterior parts of thejoint and from the supra-patellar pouch; he
September, 1964 551P
rotected by copyright. on January 30, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.467.549 on 1 S
eptember 1964. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
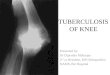
L.:._._..~.i 'FIG. 1.-G.M. Extra-articular lesion with sequestrum.
Synovial disease also.
removes pannus and also the semilunarcartilages if they are fragmented. He alsoremoves the infra-patellar fat pads because bysubsequent fibrosis they contribute to loss ofmobility of the joint. He makes a point ofremoving the tourniquet before closing thejoint so as to observe bleeding points andsecure perfect hamostasis. He gives antibioticsfor six months. 12 out of 14 patients of thistype so treated ended up with 90 degrees ormore of flexion, but in 25 adults his resultswere not so good as regards the amount offlexion, though they were otherwise successful.He points out that with at least 35 degrees offlexion walking is usually possible without toogreat a risk of catching the toe and tearingadhesions.Nagano and others (1962) have also
advocated joint clearance and six monthschemotherapy with three drugs. Out of 39cases they obtained "good mobility" in 82 percent. They start exercising the joint two weeksafter operation but do not allow weight bear-ing for at least two months. They state thatin children with radiologically normal jointsthere were good results in such cases withoutoperation. It will be agreed by many now thatin the type of case in which there is radiologicalevidence of intra-articular bone or cartilagedisease operative clearance is probably wise,
FIG. 2.-G.M. Immediately after sequestrectomy.Joint not opened and epiphyseal plate nottouched.
L
.,!-.ns,l:
FIG. 3.-G.M. Thirty months after sequestrectomy.Fully active.
552 September, 19644P
rotected by copyright. on January 30, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.467.549 on 1 S
eptember 1964. D
ownloaded from

September, 1964 STEVENSON: Treatment of Tuberculosis of the knee 553
FIG. 4.-H. O'N. Synovial tuberculosis and destruc-tion of part of lateral femoral condyle.
even though as in one of the cases to bequoted one may obtain 'a good result at timeswithout operation.Type 3 (1): Synovial tuberculosis with extra-articularand juxta-articular bone lesion:G.M. born 1951, male. At 18 months left knee
swollen and child was limping. Large gland in leftgroin. Radiologically a cavity in metaphysis of tibiawith a sequestrum and disease in the epiphysis.(Fig. 1). Inguinal gland biopsy histologically positiveNovember, 1952 commenced 0.25 g. streptomycinb.d. and PAS 0.75 g. t.d.s. January, 1953, sequestrumremoved from tibial metaphysis, cavity curetted, andstreptomycin powder 1 g. into the cavity. (Fig. 2).Epiphyseal plate seen at top of cavity but notpierced. Pus was guinea-pig and Lowenstein culturepositive; organism fully streptomycin sensitive.Following curettage of the cavity INAH (then a newdrug) 20 mg. t.d.s., i.e., 4 mg./kilo. body weight perday was added to treatment and streptomycinchanged to 0.5 g. once daily. February, 1953, PASstopped but other two drugs continued until May,1953. October, 1953 discharged home with full rangeof movement. 1958: Best runner in his class atschool, with full painless movement.Fig. 3 shows the knee in 1962, nine years afteroperation.Type 3 (2): Intra-articular epiphyseal destructivedisease and synovial involvement.H.O'N, female, born 1945. Trauma at the age of
three was followed by symptoms of tuberculosis ofthe knee in December, 1948. Pus from abscesspointing behind the knee was guinea-pig positive.Streptomycin 0.5 g. daily alone was given for fivemonths, and conservative treatment continued for a
FIG. S-H. O'N. Fourteen months after Fig. 6 wastaken. Recovery of bone lesions with chemo-therapy alone.
FIG6.NA Usls on.Atrdsspromd
Protected by copyright.
on January 30, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.467.549 on 1 Septem
ber 1964. Dow
nloaded from

554 POSTGRADUATE MEDICAL JOURNAL September, 1964
year. At the beginning of the course there wasconsiderable destruction of the lateral condyle of thefemur (Fig. 4), but with chemotherapy healingand reformation of the diseased condyle occurredwithout operation (Fig. 5).
It remains true that really gross joint destruc-tion is best treated by arthrodesis under anti-biotic cover. The production of a mobile jointin these circumstances will not occur, or atbest adhesions will only allow very slightmovement and their tearing will be liableto encourage reactivation.Type 4: Gross synovial and bone disease.N.A. born 1948, male. At the age of seven had
already a three-year history of tuberculosis of theleft knee. He received chemotherapy of doubtfulamount in 1954 and in November, 1955 a syno-vectomy was done. In June, 1956 he was seen(Fig. 6) with a fixed flexion deformity, loss of jointspace, and deformity of the femoral condyle. Itwas agreed that a safe useful mobile joint wasnot obtainable. A Charnley arthrodesis wasperformed.
In patients of this type and in those witheven grosser destruction of the bone surface,arthrodesis after removal of as much diseasedtissue as possible is the proper procedure.Chemotherapy should be given with threedrugs for at least six months.
Summary1. The principles of chemotherapy in ortho-
padic tuberculosis and the management ofof the tuberculous knee in particular aredescribed.
2. Four broad types of tuberculosis of theknee and the therapeutic approach to eachare described.
3. The place of synovectomy with debride-ment of the joint under chemotherapycover is described for those patients withdisease more advanced than that of thesynovium only but for whom a mobilejoint is still a reasonable hope.
REFERENCESNAGANO, M., UDAGAWA, E., HARA, T., HONDA, S., OHTA, M. (1962): Synovectomy as a Treatment of Tuberculosisof the Knee: Follow-up Studies and a Review of Literature, J. Jap. Orthop. Assn., 35, 1245.STEVENSON, F. H., CHOLMELEY, J. A. and JORY, H. I. (1958): Tuberculosis of the Knee: Results and Chemo-therapy between 1948 and 1956, Tubercle, 39, 1.TUBERCULOSIS CHEMOTHERAPY UNIT, Madras (1960): A Concurrent Comparison of Isoniazid plus PAS, with3 Regimens of Isoniazid alone, in the Domiciary Treatment of Pulmonary Tuberculosis in S. India, BullWld. Hlth. Org., 23, 535.WILKINSON, M. C. (1962): Partial Synovectomy in the Treatment of Tuberculosis of the Knee, J. Bone Jt. Surg.,44B, 34.
Protected by copyright.
on January 30, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.467.549 on 1 Septem
ber 1964. Dow
nloaded from