Embed Size (px)
Citation preview

Advances in Anesthesia 24 (2006) 177–192
ADVANCES IN ANESTHESIA
Off-Label Uses of Dexmedetomidine
Keyuri Popat, MD*, Ronaldo Purugganan, MD,Imrana Malik, MDM.D. Anderson Cancer Center, 1400 Holcombe Boulevard, 409, Houston, TX 77030, USA
Dexmedetomidine (Precedex) is a highly selective, potent alpha-2 adren-ergic receptor agonist. It has sedative, analgesic, and anxiolyticproperties with, amazingly, no effect on the respiratory rate. Dexmede-
tomidine binds alpha-2 receptors eight times more avidly than does clonidineand is shorter acting. Its mechanism of action includes stimulation of receptorsin the locus ceruleus to provide sedation and in the spinal cord to enhanceanalgesia.
Among the drugs used for anesthesia, alpha-2 agonists are unique in thatthey provide hemodynamic and sympathoadrenal stability and possess seda-tive, hypnotic, and analgesic properties [1]. Of the alpha-2 agonists, clonidinehas been studied most extensively. Aside from its common use as an antihyper-tensive, it is widely known that clonidine, with its ability to cause a decrease incirculating catecholamines, is also highly effective in minimizing the periopera-tive stress response. Its use as such is limited by a common side effect, how-ever: sedation. Anesthesia for surgical procedures may exploit these benefitsand the side effects. Dexmedetomidine, a newer alpha-2 agonist, shares the ad-vantages of clonidine but with greater selectivity for the alpha-2 receptor [2].With this increased selectivity, dexmedetomidine is capable of reducing circu-lating catecholamines by 90%, is much more effective than clonidine in blunt-ing the sympathetic response during laryngoscopy and intubation, and isa much more potent analgesic [3–7].
The use of dexmedetomidine as an anesthesia adjunct in balanced anesthesiaand total intravenous (IV) anesthesia for surgical procedures has been increas-ing. Aside from the benefits of alpha-2 agonism discussed previously, dexmede-tomidine is advantageous in the balanced anesthesia setting because it reducesthe minimum alveolar concentration requirements for volatile anesthetics andhas an additive effect when combined with benzodiazepines and narcotics [8–10]. With dexmedetomidine, satisfactory balanced anesthesia, hemodynamicstability, and rapid emergence can be achieved with lower doses of coadminis-tered drugs.
*Corresponding author. E-mail address: [email protected] (K. Popat).
0737-6146/06/$ – see front matterª 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.aan.2006.06.007
178 POPAT, PURUGGANAN, & MALIK
Analgesia is defined as insensibility to pain without loss of consciousness.This state can be achieved various methods, including pharmacologic interven-tions, acupuncture, psychotherapy, and invasive methods. Dexmedetomidineis one the pharmacologic methods to achieve analgesia.
Sedation is described as reduction of anxiety, stress, irritability, or excite-ment usually caused by administration of drugs. Dexmedetomidine is a safesedative agent because of the properties described in the following sections.
PHARMACOLOGYDexmedetomidine exhibits an affinity for alpha-2 adrenoceptors over alpha-1adrenoceptors 1620:1, as demonstrated in vitro [11]. Dexmedetomidine hasa half-life of approximately 6 minutes. Dexmedetomidine infusion also showslinear kinetics in the dose range of 0.2 to 0.7 lg/kg/h for up to 24 hours. Inhealthy volunteers, dexmedetomidine is 94% protein bound. It is not signifi-cantly displaced by some commonly used drugs, nor does it displace drugssuch as phenytoin, warfarin, theophylline, and digoxin [11].
MetabolismDexmedetomidine undergoes glucuronidation and cytochrome P450–mediatedmetabolism in the liver. It is excreted mainly via the urine (95%). Dose reduc-tion should be considered in patients with significant hepatic impairment(Child-Pugh class A, B, or C) [11].
EliminationThe elimination half-life for dexmedetomidine is 2 hours. There is no change inthe pharmacokinetics with respect to gender or renal impairment [11].
MECHANISM OF ACTIONAlpha-2 receptors are mainly located in the presynaptic nerve terminals. Acti-vation of alpha-2 receptors presynaptically decreases the release of norepineph-rine. Stimulation of the postsynaptic alpha-2 receptor causes hyperpolarizationof the membrane, which produces a negative feedback loop and decreases re-lease of norepinephrine even more. In the central nervous system, stimulationof the alpha-2 receptor reduces sympathetic outflow, which causes vasodilata-tion, sedation, reduction in brain noradrenergic activity, decreased heart rate,and analgesia. The adrenoreceptors in the locus ceruleus control wakefulness;stimulation of alpha-2 receptors causes sedation. The reduction in sympathetictone also leads to decreased myocardial oxygen consumption [12].
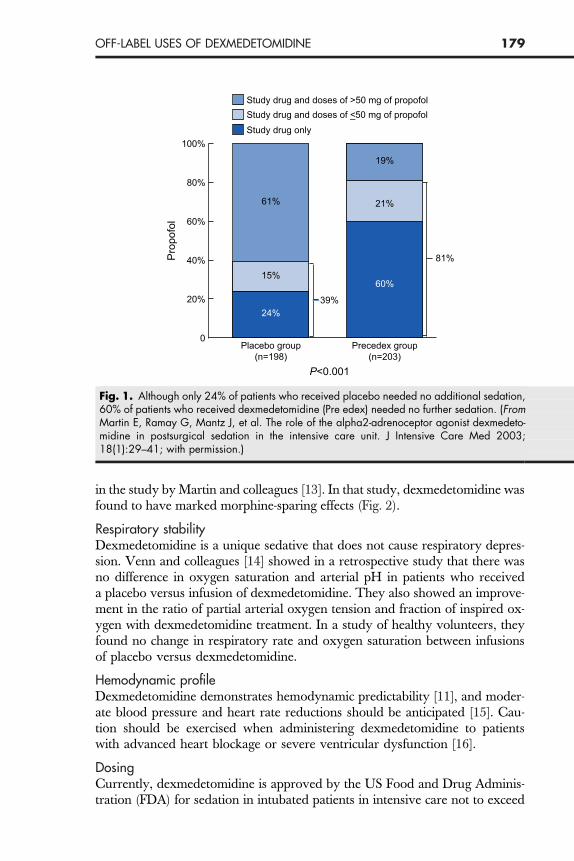
CLINICAL EFFECTSSedationAs demonstrated by Martin and colleagues [13] in a double-blinded, random-ized, multicenter trial, 60% of patients on dexmedetomidine for postoperativeintensive care unit (ICU) sedation needed no additional sedative (Fig. 1). Dexme-detomidine has significant analgesic properties, which were also demonstrated
179OFF-LABEL USES OF DEXMEDETOMIDINE
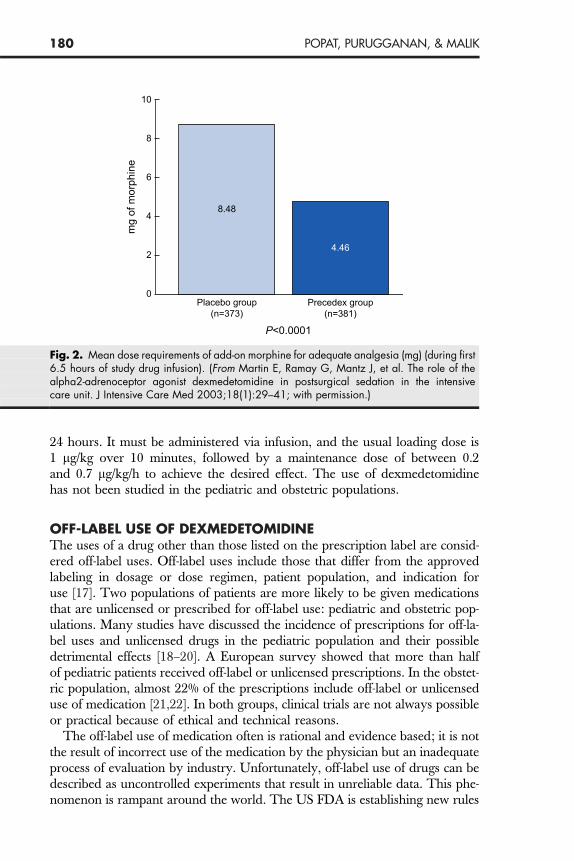
in the study by Martin and colleagues [13]. In that study, dexmedetomidine wasfound to have marked morphine-sparing effects (Fig. 2).
Respiratory stabilityDexmedetomidine is a unique sedative that does not cause respiratory depres-sion. Venn and colleagues [14] showed in a retrospective study that there wasno difference in oxygen saturation and arterial pH in patients who receiveda placebo versus infusion of dexmedetomidine. They also showed an improve-ment in the ratio of partial arterial oxygen tension and fraction of inspired ox-ygen with dexmedetomidine treatment. In a study of healthy volunteers, theyfound no change in respiratory rate and oxygen saturation between infusionsof placebo versus dexmedetomidine.
Hemodynamic profileDexmedetomidine demonstrates hemodynamic predictability [11], and moder-ate blood pressure and heart rate reductions should be anticipated [15]. Cau-tion should be exercised when administering dexmedetomidine to patientswith advanced heart blockage or severe ventricular dysfunction [16].
DosingCurrently, dexmedetomidine is approved by the US Food and Drug Adminis-tration (FDA) for sedation in intubated patients in intensive care not to exceed
Study drug and doses of >50 mg of propofol Study drug and doses of <_50 mg of propofol Study drug only
100%
80%
60%
Prop
ofol
Placebo group(n=198)
Precedex group(n=203)
P<0.001
39%
61%
15%
21%
19%
24%
60%
81%40%
20%
0
Fig. 1. Although only 24% of patients who received placebo needed no additional sedation,60% of patients who received dexmedetomidine (Pre edex) needed no further sedation. (FromMartin E, Ramay G, Mantz J, et al. The role of the alpha2-adrenoceptor agonist dexmedeto-midine in postsurgical sedation in the intensive care unit. J Intensive Care Med 2003;18(1):29–41; with permission.)
180 POPAT, PURUGGANAN, & MALIK
24 hours. It must be administered via infusion, and the usual loading dose is1 lg/kg over 10 minutes, followed by a maintenance dose of between 0.2and 0.7 lg/kg/h to achieve the desired effect. The use of dexmedetomidinehas not been studied in the pediatric and obstetric populations.
OFF-LABEL USE OF DEXMEDETOMIDINEThe uses of a drug other than those listed on the prescription label are consid-ered off-label uses. Off-label uses include those that differ from the approvedlabeling in dosage or dose regimen, patient population, and indication foruse [17]. Two populations of patients are more likely to be given medicationsthat are unlicensed or prescribed for off-label use: pediatric and obstetric pop-ulations. Many studies have discussed the incidence of prescriptions for off-la-bel uses and unlicensed drugs in the pediatric population and their possibledetrimental effects [18–20]. A European survey showed that more than halfof pediatric patients received off-label or unlicensed prescriptions. In the obstet-ric population, almost 22% of the prescriptions include off-label or unlicenseduse of medication [21,22]. In both groups, clinical trials are not always possibleor practical because of ethical and technical reasons.
The off-label use of medication often is rational and evidence based; it is notthe result of incorrect use of the medication by the physician but an inadequateprocess of evaluation by industry. Unfortunately, off-label use of drugs can bedescribed as uncontrolled experiments that result in unreliable data. This phe-nomenon is rampant around the world. The US FDA is establishing new rules
10
8
6
Placebo group(n=373)
Precedex group(n=381)
P<0.0001
mg
of m
orph
ine
4
2
0
4.46
8.48
Fig. 2. Mean dose requirements of add-on morphine for adequate analgesia (mg) (during first6.5 hours of study drug infusion). (From Martin E, Ramay G, Mantz J, et al. The role of thealpha2-adrenoceptor agonist dexmedetomidine in postsurgical sedation in the intensivecare unit. J Intensive Care Med 2003;18(1):29–41; with permission.)
181OFF-LABEL USES OF DEXMEDETOMIDINE
to allow the spread of information about off-label uses of certain medications ifthese uses have been documented in reputable, peer-reviewed scientific publica-tions [22]. The reporting of experiences with off-label uses of medications helpsphysicians decide what role the off-label use of the medication will play. Thisprocess does not, however, substitute for controlled trials that evaluate thesafety, effectiveness, and dosing for a particular off-label scenario.
The off-label use of a medication is acceptable if there is no suitable alterna-tive and if a physician feels confident that he or she is using the medication inaccordance with current medical opinion [23]. Physicians who prescribe the off-label use of a medication should document the rationale for that use and anydiscussions they may have with the patient regarding that use [24].
The US FDA recognizes that although off-label uses may represent a devia-tion from their specific recommendations, these uses play an important role inthe progression and evolution of modern medicine [17]. The US FDA states,‘‘once a product has been approved for marketing, a physician may prescribeit for uses or in treatment regimens or patient populations that are not includedin approved labeling. Valid new uses for drugs already on the market are oftenfirst discovered through serendipitous observations and therapeutic innova-tions’’ [17].
Off-label use of dexmedetomidine in the operating roomThe US FDA approved dexmedetomidine in 1999 for short-term use (definedas less than 24 hours) in adult intensive care patients who are initially intubatedand mechanically ventilated [17,25]. In our practice, which is based in a univer-sity-affiliated tertiary care cancer hospital with a patient population that encom-passes all cancer diagnoses and stages, the authors have used dexmedetomidineadvantageously off-label in various anesthetic scenarios in the operating room,including (1) regional anesthesia, (2) awake fiberoptic intubation/airway sur-gery, including monitored anesthesia care sedation cases with field (airway)avoidance, (3) cardiothoracic surgery, and (4) neurosurgery (spinal surgery/awake craniotomies).
Regional anesthesiaDexmedetomidine is a useful anesthetic adjunct for sedation during either theplacement of regional anesthetic blocks or the conduction of regional anesthe-sia. At MD Anderson, the use of dexmedetomidine in patients undergoing re-gional anesthesia allows us to maintain a relatively deep level of anesthesia withreduced administration of narcotics and benzodiazepines, while at the sametime allowing spontaneous respirations and easy arousal, which are importantfor communicating with patients to gauge the effectiveness of the block. In thesedation regimen, the benzodiazepine midazolam is limited to 0.5 to 2 mg IV,remifentanil is titrated starting at 0.02 lg/kg/min, and dexmedetomidine is ti-trated (no bolus) at a rate of 0.2 lg/kg/h. Propofol also may be introduced ata low infusion rate (5–10 lg/kg/min) and titrated to effect. Once the desiredlevel of sedation is achieved (ie, the patient is relaxed, spontaneously breathing,and easily arousable), infiltration of local anesthesia in the desired field and

182 POPAT, PURUGGANAN, & MALIK
regional anesthesia are performed. This technique provides a good level of an-esthesia with preserved respiration, stable hemodynamics, and decreased ben-zodiazepine/narcotic administration. For patients continuing on with surgeryunder regional anesthesia and monitored anesthesia care sedation, dexmedeto-midine and remifentanil are continued, and the infusions are adjusted toachieve an adequate level of comfort. For patients continuing on with surgeryunder general anesthesia, the dexmedetomidine and remifentanil infusions maybe continued into the general anesthesia phase, which reduces the amount ofcoadministered anesthetic drugs needed to maintain an adequate level of gen-eral anesthesia. Dexmedetomidine also has been reported to possibly improvethe quality of analgesia and decrease the analgesic requirement in IV regionalanesthetic techniques when administered as part of the local anesthetic solution[26].
Awake fiberoptic intubation/airway surgeryA patient who presents with a challenging airway that requires fiberoptic endo-tracheal intubation also may benefit from dexmedetomidine as a sedative agent[27]. The maintenance of spontaneous ventilation and cooperation during fiber-optic-guided intubation is of prime importance. Dexmedetomidine results inless respiratory depression than other comparable anesthetic agents and hasbeen shown to blunt the sympathoadrenal response to endotracheal intubation[7,10]. Another benefit of the alpha-2 agonist characteristics of dexmedetomi-dine is decreased salivation and secretions, although glycopyrrolate still maybe coadministered for a further reduction in oral secretions.
A sedation regimen using low-dose dexmedetomidine combined with care-fully titrated reduced doses of benzodiazepines and ultra–short-acting narcoticsis used for awake airway manipulation. The level of anesthesia desired canbe obtained easily during the administration of local airway anesthesia. Themain advantages of dexmedetomidine over a comparable anesthetic agent,such as propofol, are the maintenance of spontaneous ventilation, arousability/cooperation, and hemodynamic stability during this critical and stressful periodof time for the patient and anesthetist. Once the intubation is completed, end-tidalCO2 can be confirmed and fiberoptic broncoscopy may be performed for tubepositioning before induction of general anesthesia.
For airway surgery, IV anesthesia (either total or as a supplement to inhala-tion anesthesia) may be the only means of providing adequate anesthesia to thepatient, because there is frequently a breech in the continuity of the trachea orin one of the conducting portions of the airway. In the setting of total IV anes-thesia, other sedative hypnotic agents, such as propofol, may be included in theinfusion regimen (at reduced doses) to supplement the sedative action of dex-medetomidine. Using dexmedetomidine as a main total IV anesthesia agent al-lows the maintenance of spontaneous ventilation in some types of airwaysurgery in which it is essential to maintain spontaneous ventilation while pro-viding adequate anesthesia. A main advantage of dexmedetomidine in patientswith difficult/challenging airways (especially in the total IV anesthesia setting) is
183OFF-LABEL USES OF DEXMEDETOMIDINE
rapid emergence from anesthesia, with a return of spontaneous ventilation andairway reflexes, at the end of the operation.
Finally, dexmedetomidine in combination with low-dose benzodiazepinesand narcotics also has been used with success in monitored anesthesia care se-dation cases in which rapid access to a patient’s airway may not be possible (ie,cases in which field avoidance is necessary). Because it does not cause respira-tory depression and spares the use of opiates, dexmedetomidine is an idealchoice in this anesthetic scenario, in which airway maintenance maneuversand assisted ventilation may not be performed readily.
Cardiothoracic surgeryBecause of its stable hemodynamic profile, dexmedetomidine may be the sed-ative hypnotic of choice for patients undergoing cardiac, vascular, or thoracicsurgery. The ability of dexmedetomidine to decrease circulating catechol-amines and decrease hemodynamic instability in the perioperative settingmay decrease the likelihood of ischemic events in this high-risk population. Ithas been shown to reduce the occurrence of ischemic events in vascular sur-gery [28,29]. In thoracic surgery, volume restriction with preserved hemody-namics is essential but may be difficult to achieve. One-lung ventilation,lateral thoracotomy position, open pneumothorax, surgical manipulation ofthe heart and lungs, and patient comorbidities all contribute to intraoperativeinstability in patients undergoing thoracic surgery.
At the MD Anderson Cancer Center, a combination of IV volatile andregional anesthetic agents (with dexmedetomidine being the main sedative-hypnotic) are used to provide anesthesia to this potentially hemodynamicallyunstable population of patients. The regimen includes premedication with0.5 to 2 mg IV midazolam, dexmedetomidine infusion with an initial dose of0.2 lg/kg/h (started before the placement of the thoracic epidural) with no bo-lus loading, and remifentanil infusion at reduced doses (0.025–0.05 lg/kg/minstarted before thoracic epidural placement). The incidence of adverse effects as-sociated with dexmedetomidine, namely hypotension, hypertension, bradycar-dia, and atrial fibrillation, may be reduced by avoiding bolus loading doses.Infusions are continued through induction, and reduced doses of propofol(10–30 mg prn) are administered (guided by hemodynamics, bispectral indexmonitoring, and subjective assessment of patient anesthetic depth) to achievean adequate plane of anesthesia for intubation. Once the airway is secured, in-vasive monitors are in place, the patient is hemodynamically stable, and the bis-pectral index value is appropriate, a short-acting volatile anesthetic agent (eg,desflurane) is titrated to a monitored anesthesia care ‘‘amnesia’’ level (0.4–0.5 end-tidal concentration) and maintained. Epidural narcotics are adminis-tered before skin incision, and dexmedetomidine and remifentanil/narcoticinfusions are adjusted to reflect changes in bispectral index or hemodynamics.If necessary, low-dose propofol IV infusion or low-concentration local anesthe-sia via an epidural may be used to ensure adequate anesthesia. Intraoperativebispectral index monitoring is used with other standard parameters to assist in
184 POPAT, PURUGGANAN, & MALIK
assessing a patient’s anesthetic depth. In preparation for emergence, the volatileanesthesia is discontinued upon muscle closure, the remifentanil is discontin-ued upon skin closure, and a bolus of local anesthesia is administered viathe thoracic epidural. The patient is maintained on dexmedetomidine untilextubation.
This method of carefully titrated and mainly IV anesthesia offers the cardi-oprotective effects of alpha-2 agonism: stable hemodynamics and rapid awak-ening/extubation. Dexmedetomidine has been shown to be a potentiallyeffective analgesic alternative to thoracic epidural anesthesia and may be usefulin patients in whom an epidural is contraindicated [30].
NeurosurgeryDexmedetomidine has been used successfully in awake craniotomies, in whichalternating light and deep levels of sedation are required intraoperatively [31].The advantages of using dexmedetomidine in these procedures include rapidawakening, hemodynamic stability, and decreased dosage of coadministeredanesthetics. Because of its ability to cause a decrease in cerebral blood flow,some authors caution against the use of dexmedetomidine in patients with in-tracranial pathology [32]. Dexmedetomidine is also suitable for neurosurgicaloperations that involve the spinal cord and using somatosensory evoked poten-tials to monitor for possible spinal cord compromise. At MD Anderson CancerCenter, dexmedetomidine is used as an anesthesia adjunct to volatile anes-thetics, which can interfere with somatosensory evoked potentials waveforms[33].
Non–intensive care unit out-of-operating-room use of dexmedetomidineUse of dexmedetomidine in the pediatric population and for adults outside theICU and operating room is still novel. A review of the literature suggests that ithas been used for sedation in various ICU scenarios and as an adjuvant duringgeneral anesthesia but was found to be inadequate for sedation during outpa-tient procedures when used alone [24,34]. Dexmedetomidine is an excellentagent for sedation in patients with respiratory compromise caused by a medias-tinal mass or obesity, however.
Mediastinal massSometimes, mediastinal tumors can cause life-threatening complications, suchas upper airway obstruction, superior vena cava obstruction, cardiac or pulmo-nary artery compression, and acute pulmonary edema. These complicationscan be exacerbated when the sedation given to patients decreases muscletone or patients become apneic and cannot breathe spontaneously to maintainpatency of the airway (all the way from the oropharynx to the carina). Thesecases are challenging for anesthesiologists, and they become even more com-plex when the anesthesia/sedation must be administered outside of the operat-ing room. The key to sedation of a patient with a large mediastinal mass iskeeping the patient breathing spontaneously. In a review by Ferrari and

185OFF-LABEL USES OF DEXMEDETOMIDINE
Bedford [35], 20% of pediatric patients with an anterior mediastinal mass hadrespiratory complications during general anesthesia.
ObesityPatients with morbid obesity or obstructive sleep apnea are tricky to sedate forout-of-operating-room procedures, mainly because increasing the propofol dosecan result in dose-dependant collapse of the airway [36].
Several different methods can be used to provide sedation/anesthesia in thesepatients: (1) Using ketamine as an analgesic and sedating agent. It does havea risk of unpleasant neuropsychiatric side effects, however, which may notbe acceptable in an outpatient setting. (2) Using propofol for procedural seda-tion. There is a risk of apnea and collapse of the airway, however, which couldbe fatal in this subset of patients. (3) Using dexmedetomidine alone or in com-bination with ketamine. At a tertiary cancer referral center, procedural sedationfor large mediastinal mass biopsies, radiation therapy is often performed. Theusual loading dose of dexmedetomidine that we use is 1 lg/kg/h for 10 minutesand then 0.2 to 0.7 lg/kg/h maintenance infusions. This regimen has been usedon patients from 11 months to 85 years of age without any complications.There are some suggestions that dexmedetomidine might attenuate the neuro-psychiatric symptoms of ketamine [37].
Although dexmedetomidine has not been studied formally in the pediatricpopulation, there are increasing reports regarding its safety and efficacy. Ithas not proved to be a great solo agent for sedation, but in combinationwith ketamine or propofol it has been useful [38,39].
The quality of sedation is similar to propofol, but patients may be arousedwith stimuli. There also may be a more profound drop in blood pressureand heart rate with dexmedetomidine compared to propofol. Compared withpropofol, dexmedetomidine takes longer to achieve peak effect (up to 20 min-utes) and wear off after infusion is stopped (up to 20 minutes) after short-termuse for sedation.
Off-label uses of dexmedetomidine in the intensive care unitAmong the current off-label uses of dexmedetomidine in the ICU are (1) pro-longed administration of a continuous infusion (ie, more than 24 hours), (2)continuous infusion without a prior loading dose, (3) higher-than-recommen-ded dosage levels, (4) use in pediatric ICU patients, and (5) use in sedative-hyp-notic withdrawal.
Prolonged duration of administrationAccording to the current recommendations, more than 24 hours of continuousdexmedetomidine infusion is considered long-term infusion. Since its initial ap-proval of dexmedetomidine, the US FDA has requested phase IV studies oflong-term continuous infusion of dexmedetomidine to evaluate further its phar-macokinetics, safety, and effectiveness in ICU patients and patients with renalfailure [17]. In the initial new drug application submitted for dexmedetomidine,only 78 patients (of 3038 subjects, with 1473 ICU patients) received

186 POPAT, PURUGGANAN, & MALIK
dexmedetomidine for more than 24 hours, with none receiving the medicationfor longer than 40 hours [17]. Dexmedetomidine is increasingly being used inthe ICU for durations exceeding 24 hours, however. In 2004, Dasta and col-leagues [40] retrospectively reviewed data from ten institutions regarding theadministration of dexmedetomidine as part of routine adult patient care.They found that the average duration of treatment was 54 hours, there wereno rebound effects regardless of the duration, and no statistically significantadverse drug reactions were noted.
No loading doseIncreasing evidence in the literature seems to suggest a trend toward foregoingthe administration of a bolus or a loading dose when the dexmedetomidine in-fusion is initiated. Studies have shown that there is an initial fall in cardiac out-put shortly after the loading dose, although dexmedetomidine exerts no directeffects on the heart [41,42]. It is presumed that this effect is caused by an initialtransient increase in afterload [43]. A retrospective review of 136 patients byDasta and colleagues [40] showed that only 33% of the patients who receiveddexmedetomidine received a loading dose. Others have suggested that the rea-sons for limited use of the loading dose included omission of the loading dosein the institution’s protocol and never having used the loading dose at thatinstitution.
Greater-than-recommended dosageThe US FDA-approved and -recommended dexmedetomidine infusion dosingis 0.2 to 0.7 lg/kg/h. Although the recommended dose is generally followedand reviews reveal that only 27% of patients receive dexmedetomidine abovethe maximum dose, doses ranging from 0.7 to 1.4 lg/kg/h have been reportedin the literature [40]. One study reported the use of rates as high as 2.5 lg/kg/h,with only modest decreases in blood pressure, heart rate, and cardiac output[43]. From their experience, Venn and colleagues [43] noted that an infusionrate more than 1.5 lg/kg/h did not seem to improve or augment the sedationeffects. There is, however, literature in the form of case reports, in which dex-medetomidine was administered at dosages as high as 5 and 10 lg/kg/h, asa component of total IV anesthesia [44]. These authors maintained that dexme-detomidine’s properties of sedation, analgesia, and no respiratory depressionpersisted even at the anesthetic doses. No significant bradycardia or hypoten-sion was noted in these case reports. The dosage ceiling for sedation with dex-medetomidine infusion is still unclear, and additional studies are necessary toclarify this.
Pediatric intensive care unit patientsIn the initial new drug application for dexmedetomidine, no data were submit-ted regarding safety in pediatric patients [17]. Since the approval of dexmede-tomidine in 1999, there have been multiple articles regarding the use of thismedication in the pediatric population, ranging from anecdotal to prospective,randomized trials and including intubated and nonintubated ICU and

187OFF-LABEL USES OF DEXMEDETOMIDINE
non-ICU patients. Tobias and Berkenbosch [45] prospectively compared dexme-detomidine (0.25 or 0.5 lg/kg/h) and midazolam (starting at 0.1 mg/kg/h) for se-dation of infants and children during mechanical ventilation. The lower dose ofdexmedetomidine (0.25 lg/kg/h) provided sedation equivalent to 0.22 mg/kg/hof midazolam; however, the higher dose (0.5 lg/kg/h) provided sedation andanalgesia superior to midazolam, as evidenced by the more appropriate Ramsaysedation scores and the lower requirement for supplemental morphine doses overa 24-hour period in the dexmedetomidine group [45]. Systolic or diastolic bloodpressures did not differ significantly between the three groups; however, heartrates were significantly lower in the two dexmedetomidine groups as comparedto the midazolam group [45].
Sedative-hypnotic withdrawalDexmedetomidine also has been used for sedative-hypnotic withdrawal inthe ICU. A case report from 2003 presented the use of dexmedetomidine ina multiple-substance abuser with acute respiratory distress syndrome and ven-tilator-associated pneumonia who was successfully weaned from the ventilator,lorazepam, and IV fentanyl after 7 days of continuous dexmedetomidine infu-sion [46]. This patient had no adverse cardiovascular sequelae from the pro-longed dexmedetomidine use.
Use of dexmedetomidine in noninvasive proceduresDexmedetomidine has been evaluated anecdotally and prospectively for seda-tion during noninvasive procedures in children. In one study, dexmede-tomidine was used successfully to sedate 48 children undergoingelectroencephalography, MRI (head or other), and nuclear medicine imagingwithout significant changes in heart rate, blood pressure, or respiratory rate[47]. Dexmedetomidine use also was reported in a retrospective case seriesthat described its use as a rescue sedation agent (loading and maintenance in-fusions) in five children undergoing MRI who had failed conventional sedationwith chloral hydrate or midazolam [48]. The mean loading doses were 0.78 �0.42 lg/kg/h, the mean maintenance infusion rates were 0.57 � 0.06 lg/kg/h,and no clinically significant cardiorespiratory changes were reported [38].
USE OF DEXMEDETOMIDINE BY NONANESTHESIOLOGISTSNonanesthesiologists (eg, adult and pediatric intensivists, surgeons, and phar-macists) are using dexmedetomidine more and more frequently [25,40]. Dastaand colleagues [40] reported that anesthesiologists were the most common pre-scribers of dexmedetomidine (38%). Other specialists who prescribed dexmede-tomidine included surgical specialists (13%), critical care specialists (11%),pulmonologists (9%), and pharmacists (8%).
SAFETY CONSIDERATIONSThe major safety concerns regarding dexmedetomidine include the following:(1) A 24-hour limitation on the use of dexmedetomidine as a continuous infu-sion was instituted secondary to concerns regarding possible tolerance,

188 POPAT, PURUGGANAN, & MALIK
rebound withdrawal, and accumulation of active metabolites. (2) Dexmedeto-midine has not been approved in the pediatric population. (3) Patients olderthan 65 years are prone to conduction defects, and this drug should be usedwith caution in this subset of patients. (4) Dose reduction should be consideredin patients with renal impairment. (5) No data are available on the safety ofdexmedetomidine in the obstetric population.
The sedative and sympatholytic effects of dexmedetomidine are dose depen-dently antagonized by IV atipamezole. Both drugs have similar half-lives [48].
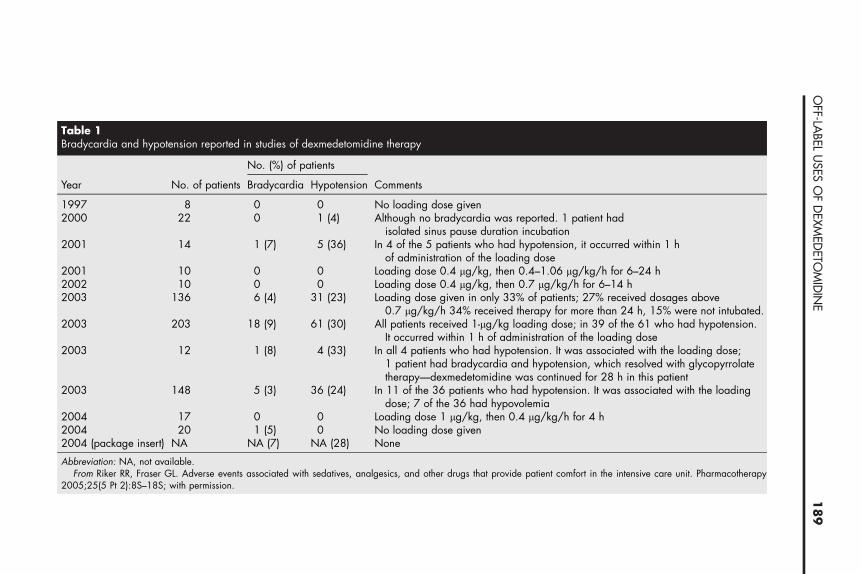
Adverse reactionsAccording to Dasta and colleagies [40], the most common adverse reaction todexmedetomidine was hypotension, which occurred in 23% of patients, fol-lowed by bradycardia, which occurred in 4.4% of patients. Table 1 showsthe incidence of bradycardia and hypotension from various studies datingfrom 1997 to 2004 [25]. Of significance is the finding that most of the bradycar-dia and hypotension occurred shortly after administration of the loading dose.In the studies in which no loading dose was given, the incidences of bradycar-dia and hypotension were 0% to 5% and 0%, respectively (Table 1).
Other adverse reactions include nausea (11%), atrial fibrillation (7%), anemia(3%), pain (3%), pleural effusion (3%), leukocytosis (2%), oliguria (2%), pulmo-nary edema (2%), infection (2%), and thirst (2%).
Drug interactionsDexmedetomidine administration may be affected by various drug interac-tions. CYP2A6 inhibitors, such as isoniazid, methoxsalen, and miconazole,may increase the level and effects of dexmedetomidine. Conversely, dexmede-tomidine may increase the levels and effects of CYP2D6 substrates, which in-clude amphetamines, selected beta blockers, and lidocaine. Dexmedetomidinemay decrease the levels and effects of CYP2D6 prodrug substrates, such ascodeine, oxycodone, and tramadol. Adverse reactions associated withdexmedetomidine, such as hypotension and bradycardia, may be augmentedor potentiated by vasodilators and heart rate–lowering medications, such asdigoxin and esmolol [49].
Tolerance and withdrawalAlthough tolerance with the potential for rebound or withdrawal effects isa common complication of sedation, it has not been reported to date with dex-medetomidine [40]. Even long-term administration of dexmedetomidine infu-sion (averaging 33 hours) did not result in clinically significant rebound afterdrug discontinuation [43].
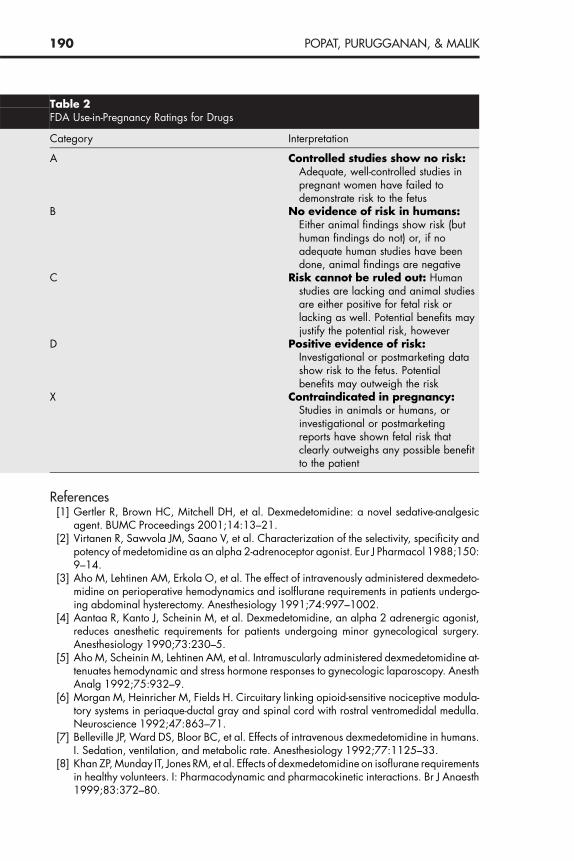
PregnancyExperience and safety data regarding dexmedetomidine in the obstetric popu-lation are lacking. Currently, dexmedetomidine is considered a category C bythe US FDA for use in pregnancy, which indicates that ‘‘risk cannot be ruledout’’ (Table 2).
TableBradyc
Year
19972000 ported. 1 patient had
incubation2001 ypotension, it occurred within 1 h
g dose2001 .4–1.06 lg/kg/h for 6–24 h2002 .7 lg/kg/h for 6–14 h2003 of patients; 27% received dosages above
erapy for more than 24 h, 15% were not intubated.2003 ading dose; in 39 of the 61 who had hypotension.
nistration of the loading dose2003 nsion. It was associated with the loading dose;
d hypotension, which resolved with glycopyrrolateas continued for 28 h in this patient
2003 d hypotension. It was associated with the loadinglemia
2004 lg/kg/h for 4 h20042004 (
AbbreviFrom patient comfort in the intensive care unit. Pharmacotherapy
2005;2
18
9O
FF-LABEL
USES
OF
DEX
MED
ETOM
IDIN
E
1ardia and hypotension reported in studies of dexmedetomidine therapy
No. (%) of patients
No. of patients Bradycardia Hypotension Comments
8 0 0 No loading dose given22 0 1 (4) Although no bradycardia was re
isolated sinus pause duration14 1 (7) 5 (36) In 4 of the 5 patients who had h
of administration of the loadin10 0 0 Loading dose 0.4 lg/kg, then 010 0 0 Loading dose 0.4 lg/kg, then 0
136 6 (4) 31 (23) Loading dose given in only 33%0.7 lg/kg/h 34% received th
203 18 (9) 61 (30) All patients received 1-lg/kg loIt occurred within 1 h of admi
12 1 (8) 4 (33) In all 4 patients who had hypote1 patient had bradycardia antherapy—dexmedetomidine w
148 5 (3) 36 (24) In 11 of the 36 patients who hadose; 7 of the 36 had hypovo
17 0 0 Loading dose 1 lg/kg, then 0.420 1 (5) 0 No loading dose given
package insert) NA NA (7) NA (28) None
ation: NA, not available.Riker RR, Fraser GL. Adverse events associated with sedatives, analgesics, and other drugs that provide
5(5 Pt 2):8S–18S; with permission.
190 POPAT, PURUGGANAN, & MALIK
References[1] Gertler R, Brown HC, Mitchell DH, et al. Dexmedetomidine: a novel sedative-analgesic
agent. BUMC Proceedings 2001;14:13–21.[2] Virtanen R, Sawvola JM, Saano V, et al. Characterization of the selectivity, specificity and
potency of medetomidine as an alpha 2-adrenoceptor agonist. Eur J Pharmacol 1988;150:9–14.
[3] Aho M, Lehtinen AM, Erkola O, et al. The effect of intravenously administered dexmedeto-midine on perioperative hemodynamics and isolflurane requirements in patients undergo-ing abdominal hysterectomy. Anesthesiology 1991;74:997–1002.
[4] Aantaa R, Kanto J, Scheinin M, et al. Dexmedetomidine, an alpha 2 adrenergic agonist,reduces anesthetic requirements for patients undergoing minor gynecological surgery.Anesthesiology 1990;73:230–5.
[5] Aho M, Scheinin M, Lehtinen AM, et al. Intramuscularly administered dexmedetomidine at-tenuates hemodynamic and stress hormone responses to gynecologic laparoscopy. AnesthAnalg 1992;75:932–9.
[6] Morgan M, Heinricher M, Fields H. Circuitary linking opioid-sensitive nociceptive modula-tory systems in periaque-ductal gray and spinal cord with rostral ventromedidal medulla.Neuroscience 1992;47:863–71.
[7] Belleville JP, Ward DS, Bloor BC, et al. Effects of intravenous dexmedetomidine in humans.I. Sedation, ventilation, and metabolic rate. Anesthesiology 1992;77:1125–33.
[8] Khan ZP, Munday IT, Jones RM, et al. Effects of dexmedetomidine on isoflurane requirementsin healthy volunteers. I: Pharmacodynamic and pharmacokinetic interactions. Br J Anaesth1999;83:372–80.
Table 2FDA Use-in-Pregnancy Ratings for Drugs
Category Interpretation
A Controlled studies show no risk:Adequate, well-controlled studies inpregnant women have failed todemonstrate risk to the fetus
B No evidence of risk in humans:Either animal findings show risk (buthuman findings do not) or, if noadequate human studies have beendone, animal findings are negative
C Risk cannot be ruled out: Humanstudies are lacking and animal studiesare either positive for fetal risk orlacking as well. Potential benefits mayjustify the potential risk, however
D Positive evidence of risk:Investigational or postmarketing datashow risk to the fetus. Potentialbenefits may outweigh the risk
X Contraindicated in pregnancy:Studies in animals or humans, orinvestigational or postmarketingreports have shown fetal risk thatclearly outweighs any possible benefitto the patient
191OFF-LABEL USES OF DEXMEDETOMIDINE
[9] Fragen R, Fitzgerald P. Effect of dexmedetomidine on the minimum alveolar concentration(MAC) of sevoflurane in adults age 55 to 70 years. J Clin Anesth 1999;11:466–70.
[10] Scheinin B, Lundgren L, Randell T, et al. Dexmedetomidine attenuates sympathoadrenalresponses to tracheal intubation and reduces the need for thiopentone and perioperativefentanyl. Br J Anaesth 1992;68:126–31.
[11] Dyck J, Shafer S. Dexmedetomidine pharmacokinetics and pharmacodynamics. AnaesthPharm Review 1993;1:238–45.
[12] Khan ZP, Ferguson CN, Jones RM. Alpha-2 and imidazoline receptor agonists: their phar-macology and therapeutic role. Anaesthesia 1999;54(2):146–65.
[13] Martin E, Ramay G, Mantz J, et al. The role of the alpha2-adrenoceptor agonist dexmede-tomidine in postsurgical sedation in the intensive care unit. J Intensive Care Med2003;18(1):29–41.
[14] Venn RM, Karol MD, Grounds RM. Pharmacokinetics of dexmedetomidine infusions for se-dation of postoperative patients requiring intensive care. Br J Anaesth 2002;88(5):669–75.
[15] Ickeringill M, Shehabi Y, Adamson H, et al. Dexmedetomidine infusion without loading dosein surgical patients requiring mechanical ventilation: haemodynamic effects and efficacy.Anaesth Intensive Care 2004;32(6):741–5.
[16] Videira RL, Ferreira RM. Dexmedetomidine and asystole. Anesthesiology 2004;101(6):1479 [author reply: 1479–80].
[17] Chang NS, Simone AF, Schultheis LW. From the FDA: what’s in a Label? A guide for theanesthesia practitioner. Anesthesiology 2005;103(1):179–85.
[18] Neubert A, Dormann H, Weiss J, et al. The impact of unlicensed and off-label drug use onadverse drug reactions in paediatric patients. Drug Saf 2004;27(13):1059–67.
[19] Conroy S, Choonara I, Impicciatore P, et al. Survey of unlicensed and off label drug use inpaediatric wards in European countries: European Network for Drug Investigation in Chil-dren. BMJ 2000;320(7227):79–82.
[20] Choonara I. Unlicensed and off-label drug use in children: implications for safety. ExpertOpin Drug Saf 2004;3(2):81–3.
[21] Wong I, Sweis D, Cope J, et al. Paediatric medicines research in the UK: how to move for-ward? Drug Saf 2003;26(8):529–37.
[22] Baker R. FDA proposes new rules for off-label use of prescription drugs. Food and DrugAdministration. BETA 1998;July:8–9.
[23] Hill P. Off license and off label prescribing in children: litigation fears for physicians. ArchDis Child 2005;90(Suppl 1):i17–8.
[24] Tobias JD, Berkenbosch JW. Initial experience with dexmedetomidine in paediatric-agedpatients. Paediatr Anaesth 2002;12(2):171–5.
[25] Riker RR, Fraser GL. Adverse events associated with sedatives, analgesics, and other drugsthat provide patient comfort in the intensive care unit. Pharmacotherapy 2005;25(5 Pt 2):8S–18S.
[26] Esmaoglu A, Mizrak A, Akin A, et al. Addition of dexmedetomidine to lidocaine for intrave-nous regional anaesthesia. Eur J Anaesthesiol 2005;22(6):447–51.
[27] Avitsian R, Li J, Jain U, et al. Dexmedetomidine and awake fiberoptic intubation for possiblecervical spine myelopathy: a clinical series. J Neurosurg Anesthesiol 2005;17(2):97–9.
[28] Talke P, Chen R, Thomas B, et al. Effects of perioperative dexmedetomidine infusion inpatients undergoing vascular surgery: the Study of Perioperative Ischemia Research Group.Anesthesiology 1995;82:620–33.
[29] Talke P, Chen R, Thomas B, et al. The hemodynamic and adrenergic effects of perioperativedexmedetomidine infusion after vascular surgery. Anesth Analg 2000;90:834–9.
[30] Wahlander S, Frumento RJ, Wagener G, et al. A prospective, double-blind, randomized,placebo-controlled study of dexmedetomidine as an adjunct to epidural analgesia after tho-racic surgery. J Cardiothorac Vasc Anesth 2005;19(5):630–5.
[31] Mack PF, Perrine K, Kobylanz E, et al. Dexmedetomidine and neurocognitive testing inawake craniotomy. J Neurosurg Anesthesiol 2004;16(1):20–5.
192 POPAT, PURUGGANAN, & MALIK
[32] Zornow MH, Maze M, Dyek JB, et al. Dexmedetomidine decreases cerebral blood flowvelocity in humans. J Cereb Blood Flow Metab 1993;13:350–3.
[33] Thornton C, Lucas MA, Newton DE, et al. Effects of dexmedetomidine on isoflurane require-ments in healthy volunteers. II: Auditory and somatosensory evoked responses. Br J Anaesth1999;83(3):381–6.
[34] Tobias JD, Berkenbosch JW, Russo P. Additional experience with dexmedetomidine in pedi-atric patients. South Med J 2003;96(9):871–5.
[35] Ferrari LR, Bedford RF. General anesthesia prior to treatment of anterior mediastinal massesin pediatric cancer patients. Anesthesiology 1990;72(6):991–5.
[36] Eastwood PR, Platt PR, Shepherd K, et al. Collapsibility of the upper airway at different con-centrations of propofol anesthesia. Anesthesiology 2005;103(3):470–7.
[37] Levanen J, Makela ML, Scheinin H. Dexmedetomidine premedication attenuates ketamine-induced cardiostimulatory effects and postanesthetic delirium. Anesthesiology 1995;82(5):1117–25.
[38] Nichols DP, Berkenbosch JW, Tobias JD. Rescue sedation with dexmedetomidine for diag-nostic imaging: a preliminary report. Paediatr Anaesth 2005;15(3):199–203.
[39] Koroglu A, Demirbileks S, Teksan H, et al. Sedative, haemodynamic and respiratory effectsof dexmedetomidine in children undergoing magnetic resonance imaging examination:preliminary results. Br J Anaesth 2005;94(6):821–4.
[40] Dasta JF, Kane-Gill SL, Durtschi AJ. Comparing dexmedetomidine prescribing patterns andsafety in the naturalistic setting versus published data. Ann Pharmacother 2004;38(7–8):1130–5.
[41] Bloor BC, Ward DS, Belleville JP, et al. Effects of intravenous dexmedetomidine in humans. II.Hemodynamic changes. Anesthesiology 1992;77(6):1134–42.
[42] Dutta S, Lal R, Karol MD, et al. Influence of cardiac output on dexmedetomidine pharmaco-kinetics. J Pharm Sci 2000;89(4):519–27.
[43] Venn M, Newman J, Grounds M. A phase II study to evaluate the efficacy of dexmedetomi-dine for sedation in the medical intensive care unit. Intensive Care Med 2003;29(2):201–7.
[44] Ramsay MA, Luterman DL. Dexmedetomidine as a total intravenous anesthetic agent. Anes-thesiology 2004;101(3):787–90.
[45] Tobias JD, Berkenbosch JW. Sedation during mechanical ventilation in infants and children:dexmedetomidine versus midazolam. South Med J 2004;97(5):451–5.
[46] Multz AS. Prolonged dexmedetomidine infusion as an adjunct in treating sedation-inducedwithdrawal. Anesth Analg 2003;96(4):1054–5.
[47] Berkenbosch JW, Tobias JD, Wankum PC. Prospective evaluation of dexmedetomidine fornoninvasive procedural sedation in children. Pediatric Critical Care Medicine 2005;6(4):435–9.
[48] Scheinin H, Aantaa R, Anttila M, et al. Reversal of the sedative and sympatholytic effects ofdexmedetomidine with a specific alpha2-adrenoceptor antagonist atipamezole: a pharma-codynamic and kinetic study in healthy volunteers. Anesthesiology 1998;89(3):574–84.
[49] Berkenbosch JW, Tobias JD. Development of bradycardia during sedation with dexmedeto-midine in an infant concurrently receiving digoxin. Pediatr Crit Care Med 2003;4(2):203–5.





























