Embed Size (px)
Citation preview

Off‐patent of the radar?Scoping the needs for new pediatric formulations of old medicines
Dr. Catherine Litalien, Executive DirectorGoodman Pediatric Formulations CentrePediatrician, CHU Ste‐Justine, Canada

Why are we here ?
● 8-month-old liver transplant recipienthospitalized with acute rejection due to inappropriately low tacrolimuscompounded suspension
● 18-month old asthmatic infant refusing to take his prednisone suspension due to bad taste
● 3-year-old child fighting leukemiawith adult tablets that need to besplitted
● 9-year-old boy who died frombaclofen overdose following a compounding error
Availability of age-appropriate, innovative and
high-quality pediatric formulations can spell the
difference between successful treatment or
therapeutic failure

The GPFC mandate
● To facilitate the development and market authorization of pediatric drug formulations by:● Promoting a research-based approach ● Contributing to a favorable clinical and regulatory
environment● Contributing to uncovering incentives● Promoting cost effective treatment for children
● To promote safety of medicines administered to children
Improving Access to Child‐Friendly Medicines

The GPFC strategy
Identifypediatric needs in Canada
Identifypediatric needs in Canada
Advocacy &awareness
Pharmaceutical partner to bring ped form. to the Canadian market (and other countries)
Pharmaceutical partner to bring ped form. to the Canadian market (and other countries)
Pharmaceutical partner(s) to develop ped. formulations and bring to market (Canada, US, EU …)
Pharmaceutical partner(s) to develop ped. formulations and bring to market (Canada, US, EU …)
● Services offered by GPFC ● Clinical needs document to
support the NDS ● Guidance on using Third Party
review strategy including Systematic Reviews
● Accompany sponsors to Health Canada meetings to support the submission with clinical expertise
● Expertise in design and conduct of pediatric studies
Yes
Pediatricformulationavailability ?
No
LinkingStakeholders
Understandingeconomics
Regulatory requirements

Scoping the needs for new pediatric formulations of old medicines in Canada
● Which drugs are currently compounded for oral administration in Canadian children ?
● Are they available in US and/or EU as commercial pediatric formulations ?
● Which ones should we prioritize first ?

Drugs frequently compounded in a Canadian pediatric tertiary hospital
● 60 drugs identified● 3 most frequent categories of drugs using AHFS
Pharmacologic-Therapeutic classification:● Cardiovascular: 30 %● Central nervous system: 18 %● Anti-infectious: 10 %
● 98% are off-patent drugs ● On the Canadian market for a median of 35 years (14 –
65 years) ● Canadian pediatric indication for 23 drugs (38%)
* American Hospital Formulary Service Pharmacologic – Therapeutic Classification

Availability of commercial pediatricoral formulations in US and/or EU
Category Definition N=60,n(%)
1 Liquid form with known safe ingredients 15 (25)2 Liquid form containing one or more
ingredients with potential safety concerns in children
Non-liquid oral form requiringmanipulation by the parent before administration (e.g.,powder or granules for oral suspension)
Chewable tablets
18 (30)
14 (23)
3(5)
1(2)
3 No commercialized pediatric oral formulation in US or EU
27 (45)

Why do we have to compound medicines when suitable pediatric formulations exist ? Category 1

Still splitting tablets to treat leukemia...
● In Canada, 6-mercaptopurine:● Approved for the treatment of ALL● Available only as 50 mg tablet resulting in:
● Tablet splitting● Compounded liquid oral formulation
● Consequences of underdosing or overdosing canbe catastrophic
● Environmental toxicity related to compounding● Prolonged treatment
Approved and marketed in EU (2012) and US (2014)

Pan-Canadian survey: prioritization of needs
● Thirteen centers among 16 contacted completed the telephone survey between April and June 2017 (81.3%)
● When sites were asked to list their 10 compounded medicines most in need of commercialized pediatric formulations:
A total of 53 drugs were identified

Drugs most in need of commercialized oral pediatric formulations in Canada
1Proton pump inhibitors; 2contains propylene glycol and sorbitol; 3Angiotensinconverting enzyme inhibitors (captopril, enalapril); 4contains sorbitol

PPI unit dose packet US EU Canada
Esomeprazole 2.5 mg •Esomeprazole 5 mg •Esomeprazole 10 mg • • •Esomeprazole 20 mg •Esomeprazole 40 mg •Omeprazole 2.5 mg •Omeprazole 10 mg •Pantoprazole 40 mg •
PPIs: Why are Canada and EU lagging behind ?
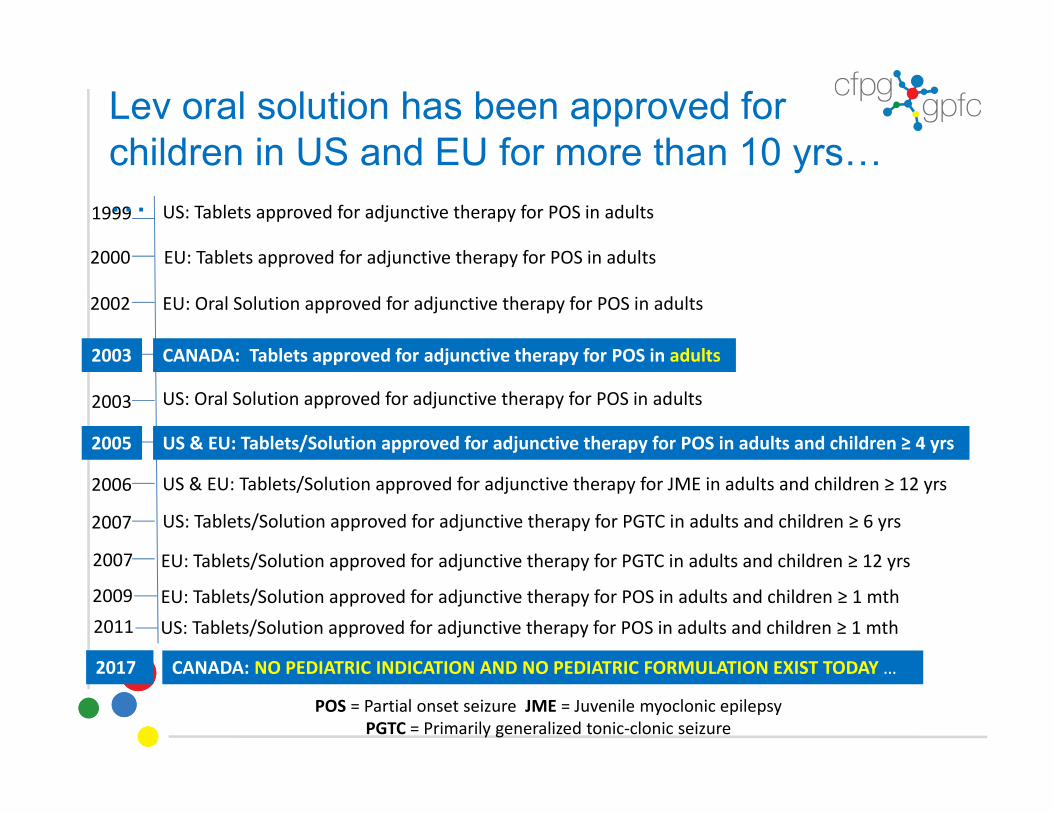
1999 US: Tablets approved for adjunctive therapy for POS in adults
2000 EU: Tablets approved for adjunctive therapy for POS in adults
2002 EU: Oral Solution approved for adjunctive therapy for POS in adults
2003 CANADA: Tablets approved for adjunctive therapy for POS in adults
2003
2007
2005 US & EU: Tablets/Solution approved for adjunctive therapy for POS in adults and children ≥ 4 yrs
2006
2007
POS = Partial onset seizure JME = Juvenile myoclonic epilepsy PGTC = Primarily generalized tonic‐clonic seizure
Lev oral solution has been approved for children in US and EU for more than 10 yrs……
US: Oral Solution approved for adjunctive therapy for POS in adults
US: Tablets/Solution approved for adjunctive therapy for PGTC in adults and children ≥ 6 yrs
EU: Tablets/Solution approved for adjunctive therapy for PGTC in adults and children ≥ 12 yrs
US & EU: Tablets/Solution approved for adjunctive therapy for JME in adults and children ≥ 12 yrs
2009
CANADA: NO PEDIATRIC INDICATION AND NO PEDIATRIC FORMULATION EXIST TODAY …
EU: Tablets/Solution approved for adjunctive therapy for POS in adults and children ≥ 1 mth2011 US: Tablets/Solution approved for adjunctive therapy for POS in adults and children ≥ 1 mth
2017

How can we move forward with these prioritized drugs ?
Ped formulation available
Amlodipine, enalapril, lisinopril, 6-mercaptopurine,
PPIs
Amlodipine, enalapril, lisinopril, 6-mercaptopurine,
PPIs
From a regulatory perspective
NO ped indication in Canada but ped indication
in US ± EU
NO ped indication in Canada but ped indication
in US ± EU Levetiracetam, sildenafil Levetiracetam, sildenafil
NO Ped indication in Canada
NO Ped indication in Canada
Dexamethasone, tacrolimus, topiramate
Dexamethasone, tacrolimus, topiramate
Spironolactone, clonidine, hydrochlorothiazide,
hydroxyurea
Spironolactone, clonidine, hydrochlorothiazide,
hydroxyurea
Ped indication in Canada and US ± EU
Ped indication in Canada and US ± EU
“Suboptimal” Ped formulation or NO Ped formulation available
Ped indication in Canada and US ± EU
Ped indication in Canada and US ± EU

Why aren’t pediatric formulations being made available in Canada?
● Market size is too small ● Regulatory pathway perceived
as unclear or complex● Seeking reimbursement is
viewed as challenging
Various incentives have proven to be an important
motivator in other jurisdictions
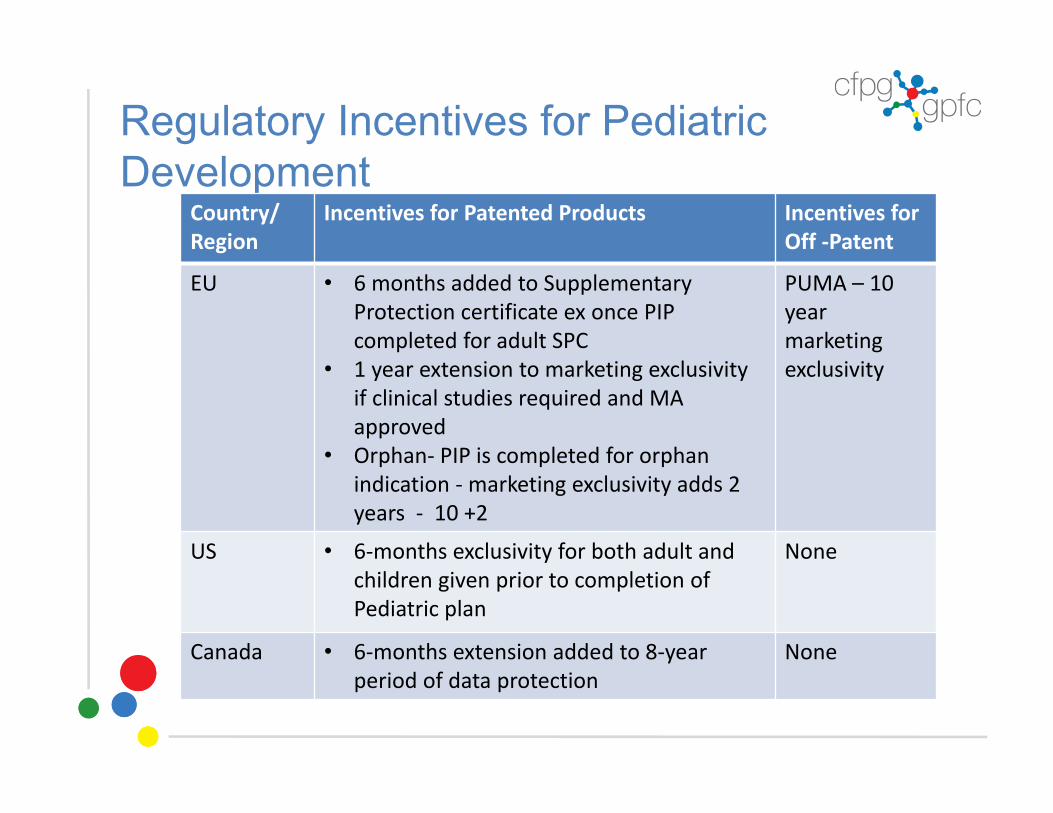
Regulatory Incentives for Pediatric Development
Country/Region
Incentives for Patented Products Incentives for Off ‐Patent
EU • 6 months added to Supplementary Protection certificate ex once PIP completed for adult SPC
• 1 year extension to marketing exclusivity if clinical studies required and MA approved
• Orphan‐ PIP is completed for orphan indication ‐ marketing exclusivity adds 2 years ‐ 10 +2
PUMA – 10 year marketing exclusivity
US • 6‐months exclusivity for both adult and children given prior to completion of Pediatric plan
None
Canada • 6‐months extension added to 8‐year period of data protection
None

Regulatory Incentives for Pediatric Formulation
Country/Region
Incentives for Pediatric Formulation
EU Orphan/Rare Diseases not approved or offering clinical benefit 10+2 years
Hybrid Applications –possible 1 year marketing exclusivity
US Orphan/Rare Diseases not approved or offering clinical benefit Pediatric Rare disease voucher possible to keep or to sell
505(b)(2)3‐5 years exclusivity possible
Canada No incentiveNDA No exclusivity

Off-patent drugs: a black hole that needs to be addressed finally…
● Most of the pediatric formulation needs are for off-patent drugs
● Depending on the region/country:● Unprecise or inexistent rules and regulations● Few or no incentives
● No sound reason why compounding shouldoccur when there is somewhere a commercially-available safe and effective pediatric formulation

How do we improve access to child-friendly medicines in 2017 ?
● Centralized agency dedicated to off-patent-drugs with regulatoryrepresentatives from interested countries (large, middle-sized, small…) + Pediatricresearch networks● Identifying needs● Data sharing● Harmonization of regulatory framework● ↑ market size● Incentives● Accelerated process “One stop shop”

Working together we can make a difference…..● We are currently supporting a
pharma company with two medicines, one of which is using a NDS relying on Third Party Review process
● We are looking for more partners● We are speaking to major
stakeholders● We are willing to collaborate with
international organizations● Pharmaceutical companies that
partner with us have a tremendous opportunity to be leaders
We leave you with a video:https://youtu.be/4kDxlhabb7I

Andrea GilpinJulie AutmizguineDenis LebelZoulfia AllakhverdiCatherine LitalienYves ThéorêtCarmen MovilaJean-Marie Leclerc
The GPFC Team
Acknowlegments:The Morris & Rosalind Goodman Family FoundationDavid GoodmanLen NeirinckYves RosconiPatricia AndersonSabrina MétayerFabrice Brunet

Dr. Catherine Litalien, Executive Director514‐773‐[email protected]
Andrea Gilpin, General Manager514‐465‐[email protected]





























