Embed Size (px)
Citation preview

OH and Headache
Dr David PB Watson
GPwSI
Hamilton Medical Group
Aberdeen

Objectives
• Headache impact and epidemiology
• Headache diagnosis
• Headache management
• audit and useful information
• case study

Objective 1
Headache Impact and Epidemiology

Headache types
90%
10% Episodic
primary headaches
Chronic primary headaches
Primary headache
No underlying medical cause:
Tumour
Meningitis
Vascular disorders
Systemic infection
Head injury
Drug-induced
Secondary headache
Underlying medical cause:

Episodic primary headaches
Episodicprimary
headaches
Migraine +/- aura
Tension-type headache (TTH)
Cluster
Probablemigraine

Chronic cluster
Chronic migraine +/- medication overuseChronic tension
Chronic daily headache (CDH)
Hemicrania continuaNew daily persistent
Chronic primary headaches / chronic daily headaches

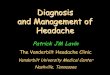
Rasmussen et al 1991Rasmussen et al 1991
Lifetime prevalence of primary headache
(n=740)
Episodic migraine
Episodic TTH
Chronic daily - all types
16%
78%
4%

Impact
• Episodic TTH –low (common)
• Episodic Migraine – high (1 in 10)
• Chronic Daily Headache - high ( 1 in 25)
• Cluster – very high (1-2 in 1000)

Migraine Impact
• Meets WHO definition of disability
• Epidemiology– 6 million people in UK– Women 3x men– most sufferers aged 20 to 50

Personal Impact
• 187000 migraine attacks experienced every day
• 3/4 report disability at least sometimes
• 1/3 feel migraine controls their lives
• 47% of migraineurs experience depression compared 17% on non migraineurs

Impact of Migraine
• UK migraine survey 1999 showed that– 30% were unable to look after their family– 63% were either totally or significantly
prevented from going to work– 39% had suffered an attack whilst driving

Economics of Migraine
• 50% of migraine sufferers miss up to 26 days work a year
• 18 million working days a year lost
• lost productivity valued at almost £2 billion a year
• sufferers function at 50% efficiency with migraine symptoms for up to 1 week

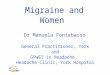
Indirect cost of migraineFor most sufferers, migraine results in lost
productivity rather than days lost from workWork loss
(%)
0 40 1000
20
40
80
100
60
20 60 80Migraine sufferers (%)
Adapted from von Korff et al 1998Adapted from von Korff et al 1998
30 9010 50 70
The most severely affected sufferers (40% of the sample) accounted for all days lost from work
Almost all sufferers reported reduced productivity equivalent to lost work days

Objective 2
Headache Diagnosis
This slide kit is for educational purposes only

“Red flags”• Single cohort (Level 3) or expert opinion (Level 4)
• new onset headache in patients who are aged over 50 29-31
• abrupt onset (thunderclap) 28-30, 32, 33
• focal symptoms including atypical aura greater than one hour 28, 32, 34, 35
• abnormal neurological examination 28, 29, 35, 36
• altered mental status 28, 30, 34
• altered characteristics or associated features of headache 28, 31
• headache that changes with posture 37
• headache worse in the morning and during physical activity, and the valsalva manoeuvre 28, 38
• patients with risk factors for thrombosis 34, 39, 40
• new onset headache in a patient with a history of HIV infection 41
• jaw claudication 16
• neck stiffness 30
• fever 42
• new onset headache in a patient with a history of cancer 9

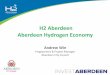
Abbreviated diagnostic checklist based on IHS 2004 criteria
Essential (3)
Essential (2)
Essential (1)
• Recurrent• No organic disease• Duration 4-72 h
• Moderate / severe + one other
• Recurrent• No organic disease• Duration 0.5 h-7 days
• Generalised• Pressure / tightness• Slight / moderate
• Photo / phonophobia
• Recurrent• No organic disease• Duration 4-72 h
• Unilateral• Pulsating• Moderate / severe• Aggravated by
movement
• Nausea / vomiting• Photo / phonophobia
Migraine Probable migraine Tension-type
Essential (3) = all items essential for diagnosis; Essential (2) = two items from list essential for diagnosis; Essential (1) = one item from list essential for diagnosis
IHS 2004

What features make migraine more likely?
• episodic severe headache that causes disability11, 23, 24
• nausea16, 23
• sensitivity to light during migraine headache16, 23
• sensitivity to light between migraine attacks 25
• aura16, 18
• sensitivity to noise16
• exacerbation by physical activity16
• positive family history of migraine16
• The features which give the greatest sensitivity and specificity are disability, nausea and sensitivity to light23
– ID Migraine validation study (Level 3)

Other primary headache
• Trigeminal autonomic cephalalgias (TACs)– Cluster headache– Paroxysmal Hemicrania– SUNCT
• Hemicrania continua
• New daily persistent headache

What features make TACs more likely?
• The following features differentiate trigeminal autonomic cephalalgias from migraine: 16, 26 (Level 4)
– Onset: rapid in TAC, gradual in migraine
– Duration: TACs < 3 hours, migraine 4 - 72 hours
– Frequency: multiple attacks may occur daily in TACs
– Restlessness during an attack: 100% in cluster headache, 50% in paroxysmal hemicrania
– Prominent ipsilateral autonomic features in TACs
• Features which differentiate trigeminal autonomic cephalalgias from each other and from trigeminal neuralgia are listed in Annex 2

Diagnosis Summary
• Key question is impact
• Default diagnosis for intermittent headache is migraine(Landmark study 90%)
• Migraine v Cluster imagine typical patient
• Chronic headache consider medication overuse

Objective 3
Headache Management

Non-pharmacological therapies• Behavioural treatments include:
– stress management / relaxation training
– regular diet and sleep
– trigger identification and avoidance
– avoidance of excessive over-the-counter medications
• Physical treatments include:– natural remedies /
complementary medicines
– acupuncture
– transcutaneous electrical nerve stimulation
– occlusal adjustment
– cervical manipulation
Adapted from US Headache Consortium Headache GuidelinesAdapted from US Headache Consortium Headache Guidelines

Acute pharmacological therapiesDrug class
Analgesics
5-HT1B/1D agonists
(Triptans)
antiemetics
Drug name
Aspirin 900 mg, ibuprofen 400mg
Almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan ,zolmitriptan
Domperidone, prochloroperazine
Avoid opioids

Management Summary
• Provide acute medication to all migraine patients and recommend it is taken early
• Provide rescue medication
• Tailor treatment to the individual
• Prophylactic Rx if high impact
• Lifestyle management important

Objective 4
Audit
Useful Information

Ideas for Audit
• Number of Migraineurs
• Assess migraine impact and lost time
• Migraine awareness campaign
• Medication Overuse awareness
• Reassess impact and lost time

Migraine Resources
• British Association for the Study of Headache www.bash.org/
• Migraine Action Association www.migraine.org.uk/
• www.sign.ac.uk

Objective 5
Case Study

Migraine and Sickness absence
• Triggers– Long hours
– Stress
– Sleep disturbance
– Missing meals
– Travel/jet lag
– Office lighting
– Hormones
• Disabling headache and ? DDA
• Reasonable adjustments eg dark room, lie down, flexi time,
• No medication 100% effective, acute treatment side effects

Case Study
• ITU nurse aged 28 with chronic migraine and medication overuse headache
• Issues include– Shift work affecting sleep, diet, exercise– Work pressures, short staffed, studying for
exam, often lack of senior staff, management attitude to sick leave, lack of understanding/empathy from colleagues

Any Questions?