Embed Size (px)
Citation preview

E
Oa
J
Tssameitltcktoswemfts
tsrsfinpt
FCoTU
J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 3 , N O . 1 0 , 2 0 1 0
© 2 0 1 0 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 0 . 0 8 . 0 0 7
D I T O R ’ S P A G E
n Fishing Expeditions, Laws of Fishing,nd Good Fishermen. . .
agat Narula, MD, PHD,* William A. Zoghbi, MD,† Y. Chandrashekhar, MD, DM‡
mTtlpweioist
occmvgaroTtpfimcetogacten
he genesis of good research is based oncritical observations, but the way these ob-servations come about seems to generate asocial-status hierarchy in the medical re-
earch community. Traditionally, successful re-earch is viewed as a well deserved fruit of a neat
priori hypothesis, great toil, meticulous experi-ents, and a juggernaut of logical reasoning. Ser-
ndipitous discovery, a previously unknown find-ng that an investigator chances upon whileesting a primary hypothesis, occupies a slightlyesser standing in this hierarchy. However, sincehere have been numerous examples of such suc-ess and since the investigator deserves credit foreeping his eyes open to the unexpected finding,his kind of research is also often lauded. On thether hand, a fishing expedition, which exploresome possible relation between several variableshile often hoping wildly that something inter-
sting would show up, is considered to be of a di-inished pedigree. Scientists in general, and grant
unding agencies as well as journal editors in par-icular, have viewed it with disdain, even thoughuch findings may help move the field forward.
While we, as editors, are also commonly preyo this line of thinking, we often encourage our-elves to be open to such studies if the data areeally intriguing. One could also argue that re-earch in general is quite unpredictable, and ashing expedition, like many things in life, mayot necessarily be a bad thing; such efforts mayay off if something interesting is captured andhe ability to handle enormous amounts of data
rom the *Division of Cardiology, University of California Irvine, Irvine,alifornia; †Cardiovascular Imaging Institute, Department of Cardiol-gy, The Methodist DeBakey Heart and Vascular Center, Houston,
oexas; and the ‡Division of Cardiology, VA Medical Center andniversity of Minnesota, Minneapolis, Minnesota.
ight make such explorations even more useful.his has already happened in genomics and pro-
eomics and is being increasingly seen in metabo-omics. Indeed, the ever expanding computingower provides insights that could not be possibleith traditional methods of fishing—a la the re-
nactment of the differences between gill-net fish-ng versus traditional hook, line, and sinker meth-ds. We will be seeing more fishing expeditionsn future medical research, and journals, despiteome damage to their perceived prestige, will even-ually be more open to publishing such studies.
Of course, such forays need an extreme amountf caution. Fishing expeditions exponentially in-rease the likelihood of false-positive and nonrepli-able results and introduce bias. This should justake us increase the scientific protection to ensure
alidity of data rather than discourage its use alto-ether. There are many ways to be conservativebout outcomes in fishing expeditions includingobust statistical methodology to limit the numberf catches that can be considered “keepers” (1).he greater the number of relationships tested,
he more conservative we have to be in order toreserve the validity of observations. As goodshermen know, too much technology or tooany lines can often snag a lot of junk. The
ause and effect relationships of such findings,ven though optimistically espoused by their au-hors, are nearly always unclear. A large numberf associations will be red herrings and will en-ender unfruitful investigations with loss of timend wasted resources. Finally, such data will beonsidered nondefinitive, and will have to passhe scrutiny of more rigorous hypothesis-basedxperimentation. The natural ferment of science iseeded to finally determine if the results were real
r random.
iectegtaasImbTgmtmitcbdwgsdfi[utudbspatsadeoatfieo
psi1mdii1detpgmf
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 1 0 , 2 0 1 0
O C T O B E R 2 0 1 0 : 1 0 8 6 – 8
Narula et al.
Editor’s Page
1087
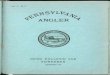
The report by Eleid et al. (2) in this issue ofJACC might be an example of such a preliminaryxploration. This study characterizes the serialhanges in left ventricular (LV) function forransplanted hearts, wherein the transplant recipi-nts demonstrated an improvement in global lon-itudinal strain within the first 3 months afterransplantation. This functional improvement wasssociated with reduced combined risk of deathnd hospitalization compared with those whohowed persistent strain abnormalities (Fig. 1).nterestingly, patients with abnormalities in LVechanics exceeded the number of patients with
iopsy-proven findings of acute cellular rejection.his is consistent with previous data where thelobal estimate of myocardial damage detected byyocardial uptake of radiolabeled monoclonal an-
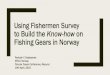
imyosin antibodies exceeded that seen in endo-yocardial biopsy specimens (3,4) (Fig. 2). Dur-
ng the first few months after heartransplantation, patients invariably showed myo-ardial uptake of monoclonal antimyosin anti-ody, revealing the presence of active myocardialamage. A gradual decrease in myocardial uptakeas later observed that was paralleled by a pro-ressive reduction in the number of rejection epi-odes in biopsy; this was considered to representevelopment of tolerance to the graft. Within therst 3 months (as also reported by Eleid et al.2]), a substantial decrease in antimyosin antibodyptake was observed in most patients; this resolu-ion of radiotracer uptake was associated with anneventful course, and less need for maintenance-ose steroids and the number of endomyocardialiopsies. On the other hand, a handful of patientshowing persistence of uptake or an increasingattern of antimyosin antibody uptake predictedn increased number of cellular and vascular rejec-ion episodes, likelihood of complications, neces-ity for retransplantation, and increased need fordditional immunosuppressive agents and depen-ence on steroids (3) (Fig. 2). This novel conflu-nce of observations highlights the phenomenonf retrodiction where older data are paralleled bynother imaging modality achievable more easily;he advantage indeed being that retrodiction con-rms that the current expedition should be free ofxperimental bias. Although a logical result was
bserved in the study by Eleid et al. (2) and therimary hypothesis was vindicated in this retro-pective evaluation, they further explored the clin-cal determinants of persistent LV dysfunction at-year after cardiac transplantation by correlatingultiple clinical and genetic variables with LV
eformation. This exploration revealed an intrigu-ng relationship of genetic expression profile as anndependent predictor of global LV strain at-year after transplantation. On examining the in-ividual components of the standard genetic testmployed for the prediction of allograft rejection,he correlation of LV deformation with gene ex-ression score was seen to be primarily driven byene coding for semanophorin (SEMA 7A), aembrane-tethered cell signaling molecule which
unctions in neural development and macrophage
Figure 1. Serial Changes in Longitudinal Strain After CardiacTransplantation
Color coded display shows the distribution of regional segments onand amplitude of longitudinal strain on y-axis. The time scale repreon the z-axis has been flattened in the 3-dimensional volumetric difocusing on spatial variations in longitudinal strains. A and B illustrapatient with improvement in longitudinal strains due to reduction i(red) and improvement (blue) in longitudinal shortening strains atmonths, whereas C and D illustrate a patient with lack of improvemlongitudinal strains. Note the reduction in shortening strains and instretch in the septum. The allograft recipients, such as in panels Ashowed an uneventful course. Figure courtesy of Partho P. SenguptMayo Clinic Arizona, Scottsdale, Arizona.
x-axissentedsplay forte an stretch3ent increase inand B,a, MD,

apb(ritaospcfjopsbn
R
1
2
Coll Cardiol Img 2010;3:989–1000. myocardial damage b
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 3 , N O . 1 0 , 2 0 1 0
O C T O B E R 2 0 1 0 : 1 0 8 6 – 8
Narula et al.
Editor’s Page
1088
nd T-cell activation pathways. This relationshiparallels recent reports where semanophorins haveeen suggested to modulate transmural mechanics5). Semanophorin has also been implicated ineinervation of the allograft, which is known tonfluence myocardial performance after transplan-ation. The uncharted exploration in the Eleid etl. (2) study thus seems to fit nicely with somebservations from other studies; indeed more ofuch collateral evidence may close the loop ofossibilities. One could argue that there is suffi-ient biological plausibility about the data andurther research into this line of thinking seemsustified. In addition to demonstrating the validityf this unexpected finding, this study (2) also sup-orts the important and often forgotten notion thatuccess in science is not only to discover new things,ut also to better understand old observations inew ways.
Ballester-Rodes, MD, and Ignasi Carrio, MD, Barcelona, Spain.
5
E F E R E N C E S
. Benjamini Y, Hochberg Y. Controllingthe false discovery rate: a practical andpowerful approach to multiple testing. JRoy Stat Soc B 1995;57:289–300.
. Eleid MF, Caracciolo G, Cho EJ, et al.Natural history of left ventricular me-chanics in transplanted hearts. J Am
3. Ballester M, Bordes R, Tazelaar H, etal. Evaluation of biopsy classificationfor rejection: relation to detection ofmyocardial damage by monoclonal an-timyosin antibody imaging. J Am CollCardiol 1998;31:1357–61.
4. Ballester M, Carrio I, Narula J. Algo-rithms for management of heart trans-plant rejection based on surveillance of
y antimyosin anti-
body imaging. In: Dec GW, Narula J,Ballester M, Carrio I, editors. CardiacAllograft Rejection. Boston, MA:Kluwer Academic Publishers, 2001:381–97.
. Carter BD, Feng N, Paolocci N. Thep75 neurotrophin receptor, semaphor-ins, and sympathetic traffic in the heart.Am J Physiol Heart Circ Physiol 2010;
Figure 2. Serial Changes in the Indium-111-Labeled Antimyosin AntibodyUptake After Transplantation
Antimyosin antibody uptake represents the presence of myocardial necrosis,and a semi-quantitative extent of myocardial damage is assessed by calcula-tion of heart-to-lung (H/L) ratio of the radiotracer uptake. The tracer uptakeis invariably seen after the transplantation which resolves gradually thereaf-ter and parallels the rate of development of tolerance. The antimyosin stud-ies from 2 allograft recipients (top and bottom) are presented at 1 (left)and 3 (right) months after the transplantation. Panels A and B representresolving antimyosin antibody uptake that predicted an uneventful course.C and D represent persistent antibody uptake; the post-transplantationcourse was riddled with numerous complications. Figure courtesy of Manuel
298:H1633–6.