Embed Size (px)
Citation preview
On the Road Again: Surgical Simulation is Rural Practice
D.R.Antonenko, MD.PhD.Professor of Surgery
Director of Surgical Simulation CenterUniversity of North Dakota School of Medicine and
Health Sciences
Simulation in Rural Surgery
Objectives• Describe the educational background for
simulation training in surgery• To describe the possible role of simulation in
rural/community surgical practice using a mobile simulation center
• To discuss how on site simulation training might help attract and retain surgeons in rural practice
Physician Learning
Patient focused learning
Resource accessibility
Clinical applicability
Familiarity with the resource
Return on investment in time
Physicians and Learning
Relevance to clinical practice needs
Scheduling conflict
Cost of attendance
Simulator Skills Training Curriculum
Sound educational principles
Goal oriented
Sensitive/objective performance metrics
Appropriate instruction/feedback
Simulator Skills Training Curriculum
Deliberate/distributed/variable practice
Allow overtraining
Provide maintenance training
Must have cognitive component
Simulator Skills Training Curriculum
Deliberate/distributed/variable practice
Allow overtraining
Provide maintenance training
Must have cognitive component
PROFICIENCY BASED
Simulation = Deliberate Practice
Move learning curve out of the OR
BUT performance still required
Reduce stress of learning
Focus is on learner, not the patient
Feedback improved

Simulators
Simulators
Procedural (task) trainers
Computer screen (micro-simulators)
VR trainers
Patient trainers
ACS/APDS Core skills Curriculum Phase I Curriculum Modules
Asepsis/instrumentsKnot tyingSuturingTissue handling wound
managementAdvanced tissue
handling/flaps/graftsCatheterizationAirway managementChest tubesCentral linesSurgical biopsy
Vascular anastomosisLaparotomyBone Fixation/castingInguinal AnatomyUpper endoscopyColonoscopyBasic laparoscopic skillsAdvanced laparoscopic skillsHand sewn anastomosisStapled anastomosis.
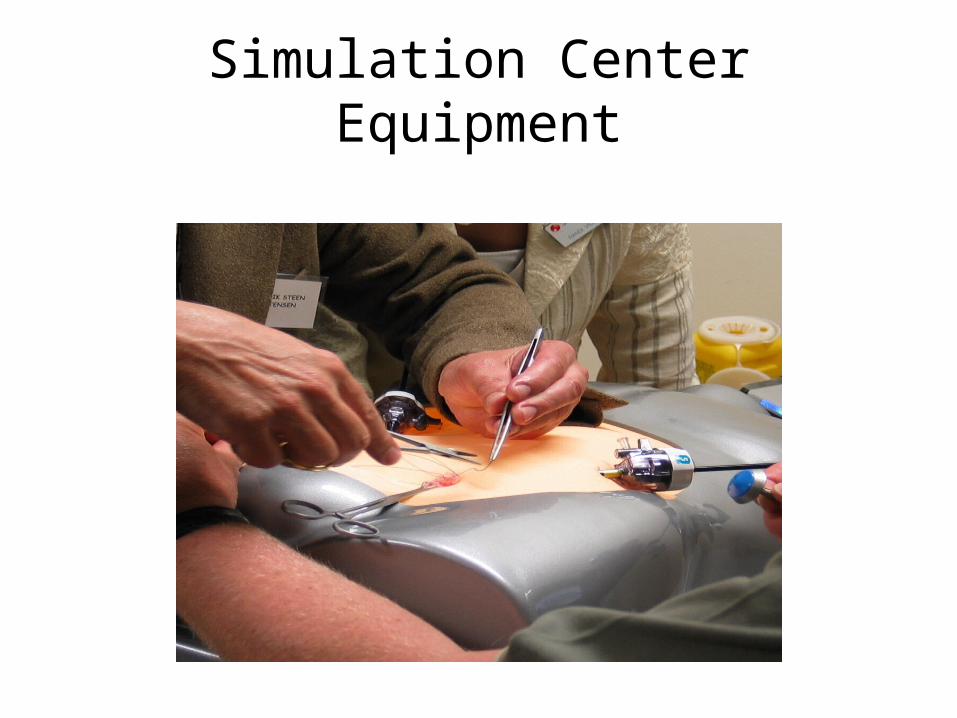
Simulation Center Equipment
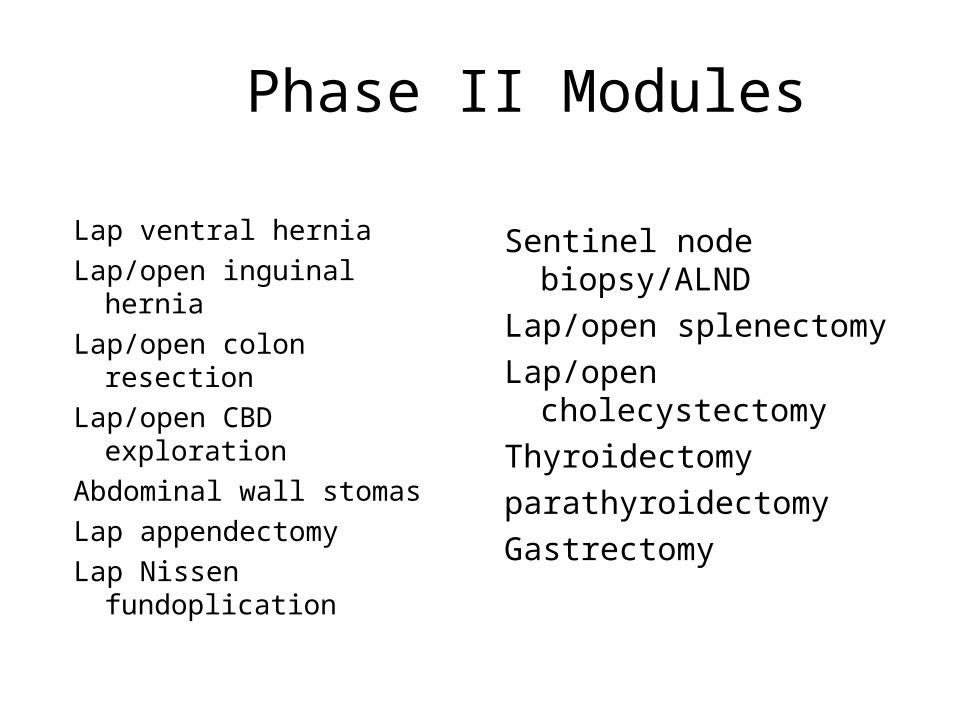
Phase II Modules
Lap ventral hernia
Lap/open inguinal hernia
Lap/open colon resection
Lap/open CBD exploration
Abdominal wall stomas
Lap appendectomy
Lap Nissen fundoplication
Sentinel node biopsy/ALND
Lap/open splenectomy
Lap/open cholecystectomy
Thyroidectomy
parathyroidectomy
Gastrectomy
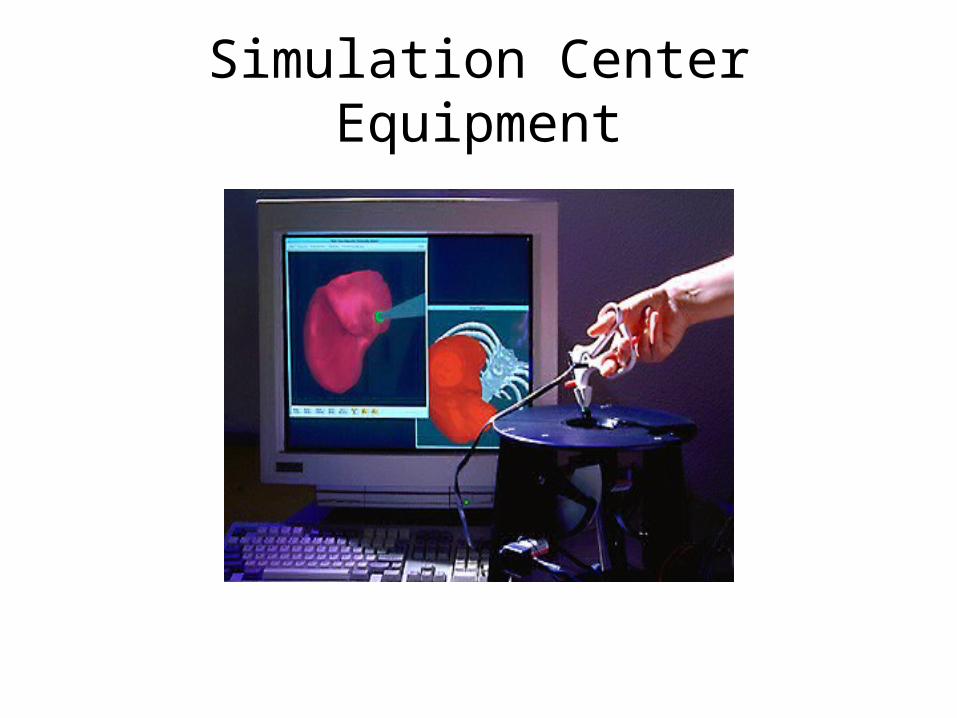
Simulation Center Equipment

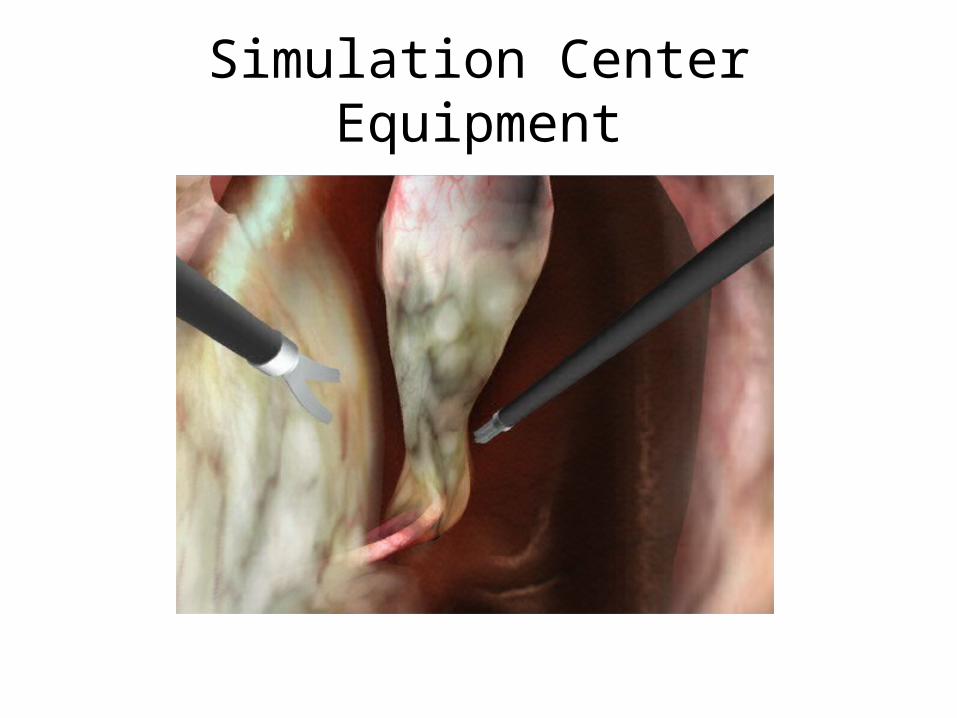
Simulation Center Equipment
Simulation Center Equipment
`ACS/APDS Core Skills Curriculum
Phase III: Team Based Training
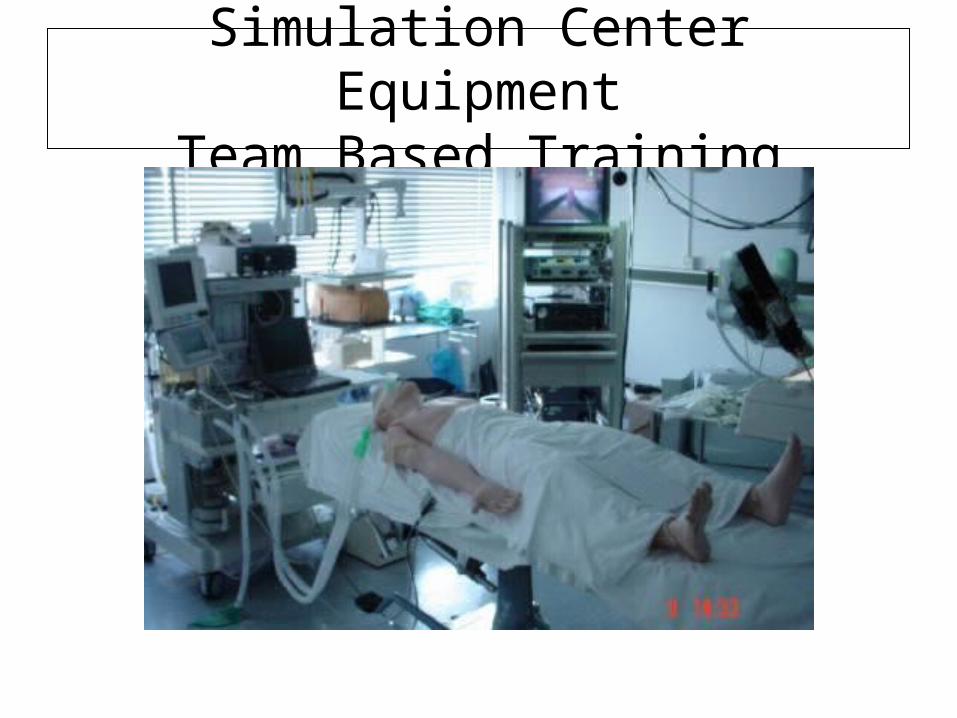
Simulation Center EquipmentTeam Based Training
Rationale For Simulator Training in Rural Surgery
Fiscal Restraints
Changing technology
Ethical Concerns
Patient Safety
Advantages of Simulation in Rural Surgery
Maintain skills
Enhance skills
Increase practice opportunities
Increase income
Reduce malpractice premiums (?)
Simulation for Rural Surgery
Surgeon specific
Site specific
High fidelity
Timely
Cost effective
Distributed vs. massed practice
Simulations for Rural Surgery
Minimally invasive
Ultrasound
ATLS procedures(?)
Airway management
Procedure specific
Endoscopy upgrades
The Future of Simulation for Rural Surgery
Tele-simulation
Tele-proctoring
Tele-mentoring 3 dimensional reconstruction
COST
Rural/Community Surgeons
Your Thoughts/comments