Embed Size (px)
Citation preview


WEST NILE VIRUSreborn in the USA
26
OBESITYdefusing the health time bomb
36
SECOND-HAND SMOKEgetting serious about it
14 On the State of the Public Health
INTRATHECAL CHEMOTHERAPYkeeping up the pressure for safe administration
46POOR MEDICAL PERFORMANCEgetting to grips
54
CO
NT
EN
TS
2
CreditsDesign and production: Redhouse LanePhotography: Simon Jarratt, Phil Starling,Science Photo Library, Photodisc
Progress onrecommendations in the Chief Medical Officer‘s annual report for 2001
4E. Coli O157 6Epilepsy 8Alcohol and Liver Cirrhosis 9High blood pressure 10Health inequalities 12
Regional focus:spotlightinglocal healthproblems
65

Over the last 150 years, annual reportshave been published by the ChiefMedical Officer, not every year but mostyears.These reports provided animportant record of the nation’s healthand the major challenges faced bygovernment in tackling the mainproblems. In the last twenty years or so,the annual report has also provideddetailed accounts of a wide range ofinitiatives taken by the government on public health and in the NationalHealth Service.
I am the 15th Chief Medical Officer in aline of succession that dates back to 1858. Inthis role I wrote my first annual report in2001. I adopted a different approach to thereports of recent decades. I felt there wasless need to cover in detail policies andprogrammes which are contained in otherdocuments. I also recognised that the rangeof government publications on health topicshad greatly expanded in the second half ofthe twentieth century. I wanted to writeshorter more accessible reports highlightingeach year a number of important healthissues which would be clearly visible andupon which action was necessary. I believethis particularly preserves the spirit of earlyChief Medical Officer annual reports: high-lighting major problems, calling for actionand allowing subsequent progress to betracked.The report for 2002, follows the same format.
In 2001 I highlighted five topics: the long-standing issue of health inequalities; theproblem of unrecognised or inadequatelytreated high blood pressure putting peopleat unnecessary risk of heart attacks or strokes;the worrying upward trend in deaths fromliver cirrhosis at younger ages and bingedrinking amongst young people; the need forfurther action to combat illness and deathfrom E.coli O157 a particularly serious form offood poisoning; and, epilepsy a disease Idescribed as having been ‘in the shadows’yetit affects 380,000 people in this country.
In this 2002 report, the first section reviewsprogress in the five areas covered in the 2001report. In some, excellent progress is beingmade, in others progress has been slower,though there is every sign that there iscommitment across the board to the action Irecommended.
I have also spotlighted one issue from eachof the nine public health regions.The issuesare those in which one part of the regionappears to be an ‘outlier’ for an importanthealth statistic. For example, I have high-lighted one area in North East of England that
On the State of the Public Health

HEALTH CHECK CMO ANNUAL REPORT 2002 3
shows an increase in death rates from cancerwhilst most other parts of the country haveshown falls.This regional focus is new to thisyear's report. I intend to draw attention tothese issues and generate debate in theregions concerned.
My 2002 annual report identifies five morehealth issues. Many of the topics coverfamiliar areas but all demand our attentioneither because they herald potentially seriousproblems in the future or because action sofar has failed to make the inroads which arenecessary.
Last year, I produced the first compre-hensive strategy on infectious diseases for theNHS. Amongst the many themes in thisdocument `Getting Ahead of the Curve’(www.doh.gov.uk/cmo/idstrategy) I identifiedthe problem of new and emerging infections.These are infectious diseases that seem tocome from nowhere (as the HIV virus did inthe early 1980s to cause AIDS) or that changetheir geographical patterns. One of theexamples I gave of an emerging disease wasWest Nile fever. Caused by a mosquito-bornevirus which previously existed only in OldWorld countries, it broke through its tradi-tional geographical boundaries in 1999 andattacked New York City: 62 people became illand seven died. Since then the infection hasswept across the United States of America;by 2002 it had been found in 44 statesamongst mosquitos, birds and other animals.In 2002 alone, 4161 human cases of West Nilevirus infection were detected and 277 peopledied. In the report, I ask could West Nile viruscome to this country and what contingencyplans do we need to make?
Over the last few years, we have seen thestrongest programme of government actionever in this country to combat the healtheffects of tobacco.This has included: the publi-cation in 1998 of a White Paper `Smoking Kills'(www.archive.official-documents.co.uk/document/cm41/4177/contents.htm); theestablishment of a network of NHS smokingcessation clinics; nicotine replacementtherapy available on prescription; a £13 millionanti-smoking advertising and educationcampaign; and new legislation to deliver acomprehensive ban on tobacco advertising,promotion and sponsorship which startedwith the end of billboard, newspaper,magazine and radio advertising in February 2003.
Much weaker has been the approach topassive smoking.The health, social and
economic effects of passive smoking – orsecond-hand smoke, as I have called it in thisreport – are very substantial. Other countrieshave done more to combat its effects and inmy report I call for further action on this front.
Whilst smoking continues to be the majorcause of premature loss of life in this country,the risk factor which is causing the mostconcern for the future health of our country isobesity. Many developed countries –including our own – are heading for an‘epidemic’of overweight and obesity.This willcause many lives to be lost prematurely in thefuture to heart disease, diabetes mellitus andcancer. Action is needed to help and supportpeople – particularly children – to reshapetheir diet. Action is also needed to increasethe amount of regular physical activity thatpeople take. Curbing the obesity epidemic isone of the biggest public health challengesof the new century and will requirecommitment by individuals, health careprofessionals, by government departmentsand a wide range of agencies and sectors ofindustry.
The safety of patients is a vital componentof the NHS programme to put a commitmentto high quality of care at the heart of localservice delivery. In its approach to patientsafety and health care quality, the NHS is upwith the leading countries of the world in this field.
Patient safety is an issue that I havepersonally championed hard in the last fewyears as part of our programme of clinicalgovernance. I am convinced that our workon patient safety is on the brink of trans-forming attitudes and approaches toreducing the risks of health care for NHSpatients.The work of the newly establishedNational Patient Safety Agency is vital to thisendeavour. As part of the wide range ofaction which will tackle many differentsources of risk in health care, we havetargeted for elimination a rare but cata-strophic error which has claimed the lives ofa small number of children and youngpeople worldwide over the last thirty years.The injection of the wrong drug into apatient's spine during cancer chemotherapyoccurs rarely but with devastating effectswhen it happens.The last incident in thiscountry was in Nottingham in 2001, when ateenager died and worldwide the lastreported incident was in Spain in 2002.
Action has been taken to try to eliminatethe causes of this error within the NHS. I report
on the background to this problem and onprogress made so far in resolving it.
The standard of medical practice in thiscountry is very high but in a large workforceof doctors, there will always be some whosepractice gives rise to concern. In the past thisproblem was not well dealt with in the NHS.Sometimes patients were left at unnecessaryrisk because no-one knew how to deal with aproblem doctor effectively. Equally, somedoctors were suspended for months or yearsat a time without any clear plan as to howthey should be dealt with.
In the last few years, an entirely newapproach has been designed for dealingwith poor clinical practice within the NHSwhich is better for patients and fairer fordoctors. I report on how this is starting tomake an impact. Not surprisingly, given thatthe issue had not been satisfactorilyaddressed for about 50 years, makingprogress has not been easy.There is nowevidence that sustained focus and the devel-opment of new expertise will soon bear fruit.
In compiling this report I am grateful forthe contribution of a number of colleagues inthe Department of Health. I am also gratefulto a number of people outside theDepartment of Health who providedcomments and suggestions on earlier drafts,in particular: Professor Sarah Randolph;Professor Angus Nicoll; Dr Judith Hilton;Dr Alastair Scotland; Professor John Tooke andDr Peter Goldblatt.The conclusions andopinions expressed in the report are my own.
I hope you enjoy reading this report as wellas finding it of interest and value. Please try toplay your individual part in addressing theissues I have raised as well as trying to interestothers in them.
By working together on the themes in thisand last year's reports we can improve thehealth of our country and make the quality ofcare experienced by NHS patients evenbetter.
I would welcome your comments (email: [email protected]).
Sir Liam DonaldsonChief Medical Officer

HEALTH CHECK CMO ANNUAL REPORT 20024
PROGRESS ON RECOMMENDATIONS IN THE CHIEF MEDICAL OFFICER‘S

ANNUAL REPORT FOR 2001
E. Coli O157 six
Epilepsy eight
Alcohol and Liver Cirrhosis nine
High blood pressure ten
Health inequalities twelve

In the 2001 annual report I drewattention to the rise in cases of seriousfood poisoning from E coli O157.In 1996, this organism was responsible for amajor outbreak in Lanarkshire which killed 17people and made 496 others very ill. A reportinto the Lanarkshire outbreak by ProfessorHugh Pennington made a wide range ofrecommendations to reduce the risk of thisserious form of foodborne illness. In my 2001annual report I emphasised the need toensure Professor Pennington's recommenda-tions were implemented and that concertedaction was taken. My recommendationscame at a time when the number of generaloutbreaks of E.coli O157 in England had risenin the year 2000 to 10 whilst the total numberof cases in that same year was 850 (the thirdhighest on record).Three outbreaks occurredin nurseries and one in Suffolk caused 22people to become ill of whom two childrendeveloped kidney complications.
I am pleased to say that in England, theprovisional number of laboratory reports ofE. coli O157 fell to 559 for the year 2002.This is34% lower than the number of casesreported in 2000. A total of six outbreakswere reported, none involving more than 20people. Only one was thought to be food-borne.
The Food Standards Agency has continuedto implement its strategy to reduce food-borne disease in the United Kingdom by 20%by 2006.The national five year Food HygieneCampaign, which was launched in February2002, is a major component of this strategy,involving a range of media, including TVadvertising.The first phase of the campaignwas designed to show how easily bacteriaspread in the kitchen and the second phasefocussed on the importance of handwashing.The campaign is only one aspect of thestrategy, which includes a broad range ofinterventions in all food sectors, including on-farm, in the abattoir, throughout the
I am pleased to say that inEngland, the provisionalnumber of laboratory reportsof E. coli O157 fell to 559 forthe year 2002.This is 34%lower than the number ofcases reported in 2000.
E.CO
LI O1
57

HEALTH CHECK CMO ANNUAL REPORT 2002 7
processing and distribution chain, in retailand catering outlets, as well as in the home.
The Clean Livestock Policy aims to improvehygiene standards by minimising the risk offood poisoning caused by bacteria on dirtyand wet coats and fleeces of cattle andsheep. Only animals that are clean and dry areaccepted for slaughter without remedialaction being taken. Key messages about thelink between clean cattle and meat safetywere communicated at a series of on-farminformation days. Procedures based onHazard Analysis and Critical Control Point(HACCP) principles and the microbiologicaltesting of carcasses have been implementedin large fresh meat slaughterhouses and willbe implemented in the remaining slaughter-houses by June 2003.
Forthcoming changes in legislation toconsolidate existing food hygiene laws willrequire all food businesses (except thoseengaged in primary production) to have afood safety management system based onHACCP principles.This is expected to becomelaw by 2005.The Food Standards Agency hasdeveloped a strategy to improve awarenessof food safety and increase the uptake ofHACCP-based systems, focusing in the firstinstance on the catering industry.The Agencyis currently developing a range of simple,practical and proportionate approaches toHACCP aimed at minimising the burdenplaced on small businesses.The aim will be toprovide guidance and training materialbacked up by a support programme.TheAgency is also working with other
I would recommend that key actionsinclude:
+ The promotion of personal hygiene tonursery staff and to those working withyoung children
+ The education of young children in thecorrect use of hygiene facilities
+ The promotion of appropriate outbreakcontrol measures to those with responsi-bility for early education and childcare toprevent the spread of infection amongstchildren once a case has occurred.
I intend to collaborate with otherGovernment departments and Agenciesto take steps to increase the awarenessof both the public, schools and themedical profession of the risks of thisinfection and how to avoid them.
section titleProgress on last year ‘s recommendations
government agencies and bodies such as theSector Skills Councils to influence vocationaltraining provision.
In response to the Pennington Report, theFood Standards Agency further strengthenedexisting food safety controls in retail butchersselling raw meat and ready to eat food by theintroduction in 2000 of the Butchers’Licensing Regulations.These Regulationsrequire butchers to operate a HACCP systemwhich, in practice, will help prevent crosscontamination through the application ofappropriate control measures, such askeeping raw meat and cooked foodsseparate.
Food business operators are required by lawto ensure that all food handlers are instructedand/or trained in hygiene matters commen-surate with their work activities,and are super-vised effectively.As part of its Food HygieneCampaign, the Food Standards Agency hasissued a hygiene training video to around400,000 catering businesses. It has alsopublished advice to help food businessesidentify training appropriate to the needs oftheir staff.
I am delighted to see the excellent progressmade in addressing the problem of E.coli O157in the past year.Much of this good work hasbeen led by the Food Standards Agency but itis important that all other individual agenciesand organisations continue to play their part.
I believe it is particularly important that thefocus of prevention should be kept on nurs-eries where there have been such seriousproblems in the past.

HEALTH CHECK CMO ANNUAL REPORT 20028
I am very encouraged by theaction that has been taken onepilepsy since it was highlightedin my 2001 report though thereis much more still to do.
The 2001 report drew attention to thesize of the problem of epilepsy inEngland – 380,000 people suffer fromthe disease (one in 130 people) whilstalmost 800 people a year die during orshortly after an epileptic seizure or fit.Young adults with epilepsy may diesuddenly, often in their sleep and no othercause of death is established. In my 2001report, I drew attention to the stigmasuffered by many people with epilepsythrough Society’s attitudes. I pointed out thatit remained an unfashionable area of clinicalpractice. I pointed out that five governmentreports over a forty year period have drawnmuch the same conclusion about epilepsy:that services are generally poorly co-ordi-nated and fragmented. I summed up myconcern by using as the title for this chapterof the 2001 report:‘Epilepsy – death in theshadows’. I called for a range of measures tobe taken to improve the quality of care forpeople with epilepsy. I recommended specifi-cally that an action plan should be publishedto respond to the (then) forthcoming reportof a National Sentinel Audit of Sudden Deathin Epilepsy.
The Audit report was published(www.sudep.org/) in May of 2002 and foundshortfalls in:
● the overall quality of epilepsy care in generalpractice and hospitals (54% of adults and 77%of children received inadequate care,and 42%of epilepsy deaths were potentially orprobably avoidable);
● guidelines for the investigation of epilepsyspecific death,poor quality death certification,and no mechanism for pathologists to informrelatives about post-mortem results;
● communicating information about epilepsymanagement and risks to epilepsy patients,and their families and carers.
On 19th February 2003 the Department ofHealth published an action plan to improveservices for people with epilepsy(www.doh.gov.uk/cmo/epilepsy/index.htm).
Although the delays in publication of thePlan led to criticism by some stakeholders, itsappearance represents a major step forward inraising standards of care for people withepilepsy and also towards reducing thenumber of unexpected sudden deaths from
epilepsy (which are so tragic for the familiesconcerned).
The Department of Health action plan gavea commitment,early in 2003, to engage withNHS Trusts and Primary Care Trusts andStrategic Health Authorities to review localepilepsy services in the light of the Auditedfindings and address any shortfalls as a resultof their local delivery plans.Also a £1.2 millionModernisation Agency project will start inApril 2003 aimed at improving the quality of,and access to,neurology services.Specificinitiatives will be taken in primary care.Twonew National Service Frameworks (NSFs) arebeing developed:the Children's NationalService Framework (www.doh.gov.uk/nsf/children.htm) will set standards aimed atimproving care for disabled children includingthose with epilepsy and the maternity moduleof this National Service Framework will addressstandards of management of epilepsy in preg-nancy.The National Service Framework forlong-term conditions (www.doh.gov.uk/nsf/longterm.htm) will have a particular focus onneurological conditions, including epilepsy.Separate action has been set in hand toimprove the quality of prescribing andmedicine management in epilepsy treatment(www.medicines-partnership.org/) whilst theNational Institute for Clinical Excellence(www.nice.org.uk/) has been commissionedby the Department of Health to look at a rangeof new anti-epileptic drugs for children andadults and clinical guidelines will be producedin June 2004.
Action has also been taken to improve thequality of information on epilepsy for serviceusers and their families including a £400,000grant to support work by the NationalSociety of Epilepsy, together with otherepilepsy charities.
I am very encouraged by the action that hasbeen taken on epilepsy since it was high-lighted in my 2001 report.There is much moreto do but I am delighted that the commitmentwhich has been missing in the past,appearsnow to be in place.
Epilepsy

In my 2001 annual report I discussed thelarge rises in deaths from liver cirrhosiswhich have occurred over recent years,particularly amongst younger people.The rising trends in deaths from cirrhosis inEngland are unusual compared with ourEuropean Union neighbours.There are manypossible causes of liver cirrhosis.The mostimportant in explaining the trends that Ihighlighted of deaths in younger people isexcess alcohol consumption. I particularlydrew attention to binge drinking patterns.The problem of unhealthy drinking patternsand particularly binge drinking amongstyoung people was the aspect of my 2001annual report that attracted most mediacoverage. Indeed, the issue has continued tobe covered in many media features over thelast year.
I called for concerted and co-ordinatedaction to address this problem. I am pleasedto report that the Prime Minister has askedthe Cabinet Office Strategy Unit to carry outa project on tackling the problems asso-ciated with alcohol misuse.The project isworking closely with stakeholders toproduce a National Alcohol Harm ReductionStrategy.The strategy will be published inSummer 2003 and will be implemented by2004.The Strategy Unit team has considereda wealth of evidence on the causes andconsequences for a wide variety of alcohol-related harm, including the harm to healththat is caused by both heavy drinking andbinge drinking.The Cabinet Office StrategyUnit will also examine ways in which theGovernment and other stakeholders canwork together to ensure that the strategy isdeveloped and implemented in a coherentand effective way.
In line with another of my recommenda-tions the Health Development Agencypublished a report in Summer 2002 -"Prevention and reduction of alcohol misuse"(http://194.83.94.67/niche_docs/EB_DATABASE_CONTENT/HTML_database_content/EBBD-Alcohol.html ) – which reviews theeffectiveness of a range of prevention andtreatment interventions.
I also made three recommendations toaddress the risk of cirrhosis caused by hepa-titis B and C.
Alcohol and Liver Cirrhosis
offenders have been especially targeted sothat some may become immune prior tocommencing injecting.The programmeenables injecting drug users to access hepa-titis B immunisation.
I am pleased to report that thePrime Minister has asked theCabinet Office Strategy Unit tocarry out a project on tacklingthe problems associated withalcohol misuse.
Progress on last year ‘s recommendations
In response to this, in August 2002, theDepartment of Health issued for consultation‘Hepatitis C Strategy for England’(www.doh.gov.uk/cmo/hcvstrategy/)
The strategy proposed:
● communicating developing professionaland public awareness of hepatitis C;
● strengthening measures to prevent trans-mission of the virus;
● increased testing among groups at risk ofacquiring infection, so that more individualswith chronic hepatitis C infection can beidentified and referred for specialistassessment and treatment, where appro-priate, in order to reduce their risks of devel-oping cirrhosis and liver cancer.
The proposals in the strategy, together withthe outcomes of the consultation exercisesand of two stakeholder meetings, will formthe basis of an action plan to be issuedduring 2003.This will set out the main objec-tives and actions necessary to strengthenprevention diagnosis and treatment services.Nationally agreed standards for antenataltesting of hepatitis B and other infections(Screening for Infectious Diseases in Pregnancy:Standards to support the UK AntenatalScreening Programme) are currently in prepa-ration.
In order to help increase the uptake ofhepatitis B vaccine among groups atincreased risk of acquiring infection:● the Department of Health is providingcentrally purchased extra vaccine to genito-urinary medicine clinics for immunising gayand bisexual men, in support of the proposedaction in the national strategy for sexualhealth and HIV;
● the Prison Service has made funds availablefor the development and implementation of athree year hepatitis B immunisation strategyfor prisoners.This immunisation programmebegan in 37 establishments in 2001/2extended to 41 in 2002/3.The programmeoffers hepatitis B immunisation to everyprisoner on reception.Existing prisoners areoffered immunisation at a specific regularprison clinic.The programme will be extendedfurther in 2003/4. Juvenile and young
HEALTH CHECK CMO ANNUAL REPORT 2002 9

HEALTH CHECK CMO ANNUAL REPORT 200210
management of blood pressure and lipidlevels of people with Type 2 diabetes mellitushave also been introduced.
In the new General Medical Servicescontract document published in February2003, practices will be expected to provideappropriate health promotion advice andreferral for patients with chronic disease.Subject to agreement on the contract, addi-tional funding will be made available to prac-tices to support a range of quality standards.These standards will be underpinned byquality indicators around setting up registersand the management of patients with highblood pressure.
The year 2002 saw a significant scaling-upof the Blood Pressure Association’s NationalBlood Pressure Testing Week with 100,000people tested at 1350 blood pressure testingstations nationwide – a five-fold increase onthe previous year. Funded by the Departmentof Health, this is the climax of a campaign toraise public awareness of high blood pressureand to encourage everyone to know theirown blood pressure numbers.
Since my last report, the Food StandardsAgency has published a consumer leafletdesigned to raise awareness of salt intake,how to cut down on salt and the health
High blood pressure – hypertension – isa major risk factor for stroke, coronaryheart disease and other illnesses such askidney disease and aortic aneurysm.In my 2001 annual report, I drew attention tosurvey data of the population of Englandshowing that half the people with highblood pressure were not being treated, and afurther fifth are being treated ineffectively.These people are at risk of serious illness andpremature death both of which could beprevented if high blood pressure wasproperly identified and controlled throughmodern treatment regimes. I made a numberof recommendations to NHS bodies andprofessional organisations to remedy thissituation. I also called for a major initiativewith the food industry to reduce the saltcontent of processed and catered foods.
Hypertension is included in one of the keytargets within the NHS Planning andPriorities Framework, with advice on diet,physical activity and smoking to be system-atically provided to people at risk of coronaryheart disease. A National Institute for ClinicalExcellence (NICE) guideline for themanagement of hypertension in primarycare is being developed for issue in February2004. NICE guidelines covering the
High blood pressure
A National Institute for ClinicalExcellence (NICE) guideline forthe management ofhypertension in primary care isbeing developed for issue inFebruary 2004.

HEALTH CHECK CMO ANNUAL REPORT 2002 11
benefits of reducing salt in the diet.The FoodStandards Agency regularly publishes a rangeof surveys, and a survey showing the saltlevels in certain food products will bepublished later this year.
The Scientific Advisory Committee onNutrition (SACN), which advises both theDepartment of Health and Food StandardsAgency published its report on ‘Salt andHealth’ in May 2003.The Scientific AdvisoryCommittee on Nutrition supports thereduction in salt intake to 6g per day, withevidence that this would help to loweraverage blood pressure and provide a signif-icant public health benefit by helping toreduce the burden of cardiovascular disease.I endorsed this target in my last report.TheScientific Advisory Committee on Nutritionreport also makes recommendations on saltintake in children, the first time that suchrecommendations have been made in theUnited Kingdom.With the Foods StandardsAgency, I welcome and endorse these newrecommendations for children.
The Secretary of State for Health has calledon industry to take a meaningful lead inreducing salt in processed foods. I and Sir JohnKrebs, Chairman of the Foods StandardsAgency have held meetings with key industrygroups where attendees acknowledged theconclusions of the Scientific AdvisoryCommittee on Nutrition.The Foods StandardsAgency and the Department of Health havealso held meetings with various food sectorsrepresenting the main contributors to salt inthe diet, to discuss the scope for saltreduction.The Foods Standards Agency is alsolooking at options for labelling of salt on foodproducts.A high profile stakeholder event isbeing planned by the Department of Healthto highlight the role of all stakeholders inaddressing dietary salt and its significance intackling high blood pressure.Wider initiativesled by the Department of Health may alsohelp reduce blood pressure – such as the 5 ADAY initiative to increase fruit and vegetableconsumption (increasing fruit and vegetableintakes by just 1.5 portions has been shown toreduce systolic pressure by 4 mm Hg).
In my 2001 annual report, I pointed out thatthe health benefits of physical activity,including links with hypertension and latercoronary heart disease and stroke, need to bemore widely communicated, and genuinecommitment is needed across governmentand local agencies to increase physical activitylevels and reduce obesity.Nine Primary Care
Trusts in neighbourhood renewal areas havebeen selected to run pilot schemes toencourage people to take up physical activityfor the good of their health. Local ExerciseAction Pilots (LEAP) – will identify and test thebest ways of getting people more active byincreasing opportunities amongst high riskand disadvantaged groups.The pilots will berigorously evaluated to find out what workswell and why, and the results will be sharednationally.
Establishing an active lifestyle in early lifecan help to avoid high blood pressure.TheDepartment of Health is working closelywith the Department for Culture, Media andSport on its £459 million programme toenhance school sport and club links.TheNew Opportunities Fund programme isproviding £581 million to enhance schoolsports facilities and encourage their widercommunity use.
A cross-government Sport and PhysicalActivity Board is now exploring new ways toencourage mass participation in sport andphysical activity.
In my 2001 annual report I also recom-mended that wherever possible, peoplewho have suffered a stroke should bemanaged in a dedicated specialiststroke unit. Outcomes for strokepatients are better when they arecared for by specialist stroke teamswithin designated stroke units.Lengths of stay are also, on average,shorter. Since the publication of theNational Service Framework for OlderPeople, many more specialist strokeservices have been set up and more areplanned. Around 75% of hospitals that carefor people who have had a stroke now have aspecialist stroke unit.There have been signif-icant increases in the number of stroke physi-cians, the proportion of patients beingtreated in specialist stroke units and thenumber of patients returning home followinghospital treatment.There have beenimportant improvements in care, for examplea record 83% of patients are now receivingbrain scans to improve diagnosis.
Good progress is being made on therecommendations I made in my 2001 annualreport to reduce the number of people whohave uncontrolled high blood pressure.
The momentum needs to bekept up. I would particularlyurge the food industry –including manufacturers,retailers and caterers – and theFood Standards Agency to drivedown the salt content of food – apotentially life saving measure.I would also urge primary careservices to move more quicklyto put in place good systems toidentify people with high bloodpressure and to ensure they arereceiving effective treatment.
section titleProgress on last year ‘s recommendations
WE MUST CUT DOWN ON SALT

HEALTH CHECK CMO ANNUAL REPORT 200212
● The strategy is made up of commitmentsfrom Departments across Government – witheach identifying the contribution it can maketo tackling this complex, cross-cuttingproblem. Commitments explicitly meetrecommendations of Acheson’s independentinquiry into health inequalities; and arefocused on delivering change throughmainstream services, rather than short-terminitiatives.
● It clearly sets out responsibilities at local,regional and national level.
● It identifies an important role for theDeputy Prime Minister and his Cabinet sub-committee on social exclusion andregeneration.
● It underlines the importance of preventiveinterventions.
● It locks into other key Governmentprogrammes to tackle poverty and socialexclusion, and to deliver social justice.
The Report sets out the Government’sambitious strategy for achieving the 2010 lifeexpectancy and infant mortality targets, andfor tackling the wider determinants ofinequalities in health over the long-term.
Health inequalitiesTARGETING THE PROBLEM
In my 2001 annual report I focussed onhealth inequalities. Although thiscountry has seen increased prosperityand overall reductions in mortality overthe last 20 years, the gap in healthbetween those at the top and bottom ofthe social scale has widened.
Death rates of the most deprived sectionsof the population declined little in the 1990s,whereas death rates amongst the better offdeclined substantially. In a fresh look at healthinequalities, one of my analyses in the 2001Report showed that some communities inEngland had death rates equivalent to thenational average in the 1950s.
In my 2001 annual report I called for arange of action at governmental, regional andlocal level to tackle the root causes of healthinequalities.
I am pleased that so much has happenedon health inequalities since my 2001 report.
The Government has published its strategyfor tackling inequalities in health – the reportof the Cross-Cutting Review of HealthInequalities. In the strategy’s approach – andthe implementation of it – there are some keypoints:

HEALTH CHECK CMO ANNUAL REPORT 2002 13
Progress on last year ‘s recommendations
in disadvantaged areas;attainment rates insecondary schools have risen faster in manydeprived areas than other places.
● Full time education for every permanentlyexcluded pupil.
● Long-term youth unemployment has beennearly eradicated;overall unemployment levelsare at their lowest rates for 25 years.
● Minimum Income Guarantee (MIG) ensures adecent minimum weekly income for singlepensioners and pensioner couples.
There has also been considerable progresswithin the NHS in particular to embed healthinequalities into mainstream performance andplanning systems and make it for the first time a`must do'.The Priorities and Planning Framework(PPF) 2003-2006,published last year,describedhow the national commitments translate intopriority areas and targets for the NHS and socialservices to achieve the ambitious programmeset out within The NHS Plan.
Policies across Government to tackle theroot causes of health inequalities arealready being put into action:
● Tax and welfare reforms to reduce poverty;
● National Service Frameworks intended to‘level up’health service access and quality;
● Health Action Zones directing resources topartnership working in disadvantagedcommunities;
● Neighbourhood renewal strategy -addressing the complex causes and effects ofdisadvantage at neighbourhood level;
● Fuel poverty strategy directed at vulnerableindividuals and families;
● Investment in early years development(Sure Start) and educational attainment.
Specific examples of cross-Governmentpolicy outcomes that will have the effect ofnarrowing the health gap in the medium tolong term include:
● 439 Sure Start local programmes are up andrunning and have reached around 335,000children.
● Attainment standards in schools have risen
THERE HAS ALSO BEENCONSIDERABLEPROGRESS WITHIN THENHS IN PARTICULAR TOEMBED HEALTHINEQUALITIES INTOMAINSTREAMPERFORMANCE ANDPLANNING SYSTEMSAND MAKE IT FOR THEFIRST TIME A ‘MUST DO’.


HEALTH CHECK CMO ANNUAL REPORT 2002 15
Since the publication in 1998 of the Government’s White Paper ̀ SmokingKills’, a wide range of action has been taken to control tobacco in thiscountry.This has covered three broad strands: prevention, cessation andprotection. Major initiatives have included: a comprehensive ban ontobacco promotion and advertising which came into effect on 14February 2003;the development of new NHS smoking cessation services;a free helpline for smokers; bigger, starker health warnings on packets;price increases and a major anti-smoking advertising campaign. A keypart of tackling the health risks of smoking is protecting people (bothsmokers and non-smokers) from tobacco smoke. Inhaling second-handsmoke (passive smoking) is unpleasant and is a direct hazard to health.Measures to control people’s exposure to second-hand smoke have hada limited impact so far. Action to reduce second-hand smoke exposurewill increase the impact of the overall tobacco control programme.
Second-hand smoke
about second-hand smoke
GETTINGSERIOUS

16 HEALTH CHECK CMO ANNUAL REPORT 2002
Key points
● Exposure to other people’s ciga-rette smoke (second-hand smoke,passive smoking, environmentaltobacco smoke) can: increase therisk of contracting smoking relateddiseases such as cancer and heartdisease; place extra stress on theheart and affect the body’s ability totake in and use oxygen; triggerasthma attacks; increase thechances of sudden infant deathsyndrome (SIDS); and harm childrenand babies even more than adults.
Smoking kills120,000people each year in
the United Kingdom.In England27% of adults now
smoke.Although this is down from 40% in 1978 it is
only a few percentage points lower than the rate in
1990.This overall rate hides major societal differences;
32% of manual workers smoke compared with
21% of those in non-manual occupations;28%
of men smoke while the figure for women is 25%;
smoking during pregnancy now stands at19%;
10% of 11 to 15 year olds are regular smokers.
● Standing in the path of a smoker ortheir cigarette or being in a room inwhich there are smokers meansbeing exposed to at least 50 agentsknown to cause cancer and otherchemicals that increase bloodpressure, damage the lungs andcause abnormal kidney function.
● Seriously reducing second-handsmoke in the environment would:save lives, improve air quality, reducechildhood and adult illness, providemore smokers with the chance to giveup, and enhance millions of people’squality of life at work and in leisuretime.
● Many public places are alreadysmoke-free but many others are not:the health risks and discomfort ofsecond-hand cigarette smoking are adaily occurrence for millions ofpeople in workplaces; in restaurants,bars and pubs; in sporting and enter-tainment venues; and, in enclosedpublic areas.
● Comprehensive workplace smokingbans could reduce the estimatedprevalence of smoking to 23% fromits present level of 27% (achievingthis effect by tax rises would meandoubling the price of cigarettes).
● Public opinion surveys have shownrepeatedly that the majority ofsmokers as well as non-smokers want to see a wider smoke-freeenvironment.

HEALTH CHECK CMO ANNUAL REPORT 2002 17
Second-hand smoke
A major health hazardTobacco smoke contains over four thousandchemicals in gaseous and particulate form.Second-hand smoke (also known as environ-mental tobacco smoke (ETS) or passive smoke)is a mixture of side stream smoke, from theburning tip of the cigarette, and mainstreamsmoke exhaled by the smoker.
Second-hand smoke contains five regulatedhazardous air pollutants, 47 regulated hazardouswastes, more than 50 known or suspectedcancer-causing agents and more than 100chemical poisons.The cancer-causing agents intobacco smoke include benzo(a)pyrene,benzene, chromium, vinyl chloride, dimethylni-trosamine and 2-naphthylamine.Toxic gasessuch as ammonia, carbon monoxide, nitrogendioxide, acrolein and hydrogen cyanide arepresent in higher concentrations in side streamsmoke which makes up about 85% of thetobacco smoke pollution in a room where thereare smokers.The World Health Organisation´sInternational Agency for Research on Cancerhas recently declared that environmentaltobacco smoke causes cancer in people andthat it includes more than 50 knowncarcinogens.
Second-hand smoke causes lung cancer,increasing the risk by 20-30% in people wholive with smokers, equivalent to severalhundred deaths a year. Second-hand smokecauses heart disease, increasing the risk byaround 25% in people who live with smokers.Second-hand smoke from parents is causallylinked to: sudden infant death syndrome (adoubling of risk); lower respiratory illness (a 50%increase in risk); asthma (a 50% increase in risk);and middle ear disease (a 40% increase in risk).Overall estimates of the impact of second-handsmoke in California have been made for a rangeof conditions set out in Table 2.
EXAMPLEAcetone
Acetic AcidAluminumAmmonia
ArsenicBenzene
Benzo(a)pyreneButane
CadmiumCopper
Carbon MonoxideDDT
DieldrinFormaldehyde
HexamineHydrogen Cyanide
LeadMagnesium
MethaneMethanol
NaphthaleneNicotine
NitrobenzeneNitrous Oxide Phenols
Polonium 210Silicon
SilverStearic Acid
TitaniumToluene
Vinyl ChlorideZinc
COMMON USENail polish removerVinegarMetalFloor and toilet cleanerRat poisonIndustrial solvent Diesel exhaust Cigarette lighter fluid Rechargeable batteries Electric wiring Car exhaust Insecticide InsecticidePreservative for dead bodies,wood, and fabrics Barbecue lighter Gas chamber poison Fishing sinkers Flares Swamp gas Rocket and car fuel Moth balls Insecticide and the addictivedrug in tobacco Petrol additive Disinfectant Radioactive compound Computer chips Jewellery Candle wax Aeroplane and missiles Industrial solvent Raw material to make plastic Metal, in coins
Table 1 Examples of chemicals to which people are exposedthrough second-hand smoke and their everyday use
Children's special vulnerability to second-hand cigarette smoke
● Children's lungs are smaller and their immune systems less developedrendering them more susceptible to respiratory and ear infections triggeredby passive smoking.
● Children are smaller and breathe faster than adults and so take in moreharmful chemicals per kg of weight than adults.
● Small children often have less choice than adults to leave a smoke-filled room.
Source:World Health Organisation
Source: 2002 Regents of the University ofCalifornia www.tobaccoscam.ucsf.edu/Secondhand/Secondhand_ti.cfm

18 HEALTH CHECK CMO ANNUAL REPORT 2002
Table 2 Estimated United States rates of death and ill health experienced by non-smokers as a result of exposure to second-hand cigarette smoke
CONDITION ESTIMATED NUMBER OF PEOPLE OR CASES PER 10 MILLION POPULATION
DEVELOPMENTAL EFFECTS
Low birthweight 360 to 690 casesSudden Infant Death Syndrome (SIDS) 70 to 100 deaths
RESPIRATORY EFFECTS IN CHILDREN
Middle Ear Infection 26,000 to 59,000 physician office visitsAsthma Induction 300 to 960 casesAsthma Aggravation 15,000 to 37,000 childrenBronchitis or Pneumonia in infants 5,500 to 11,000 cases and toddlers (< 18 months) 280 to 550 hospitalisations
5 to 8 deaths
CANCER
Lung 100 deaths
CARDIOVASCULAR
Ischaemic Heart Disease 1,300 to 2,300
Source: Health Effects of Exposure to Environmental Tobacco Smoke by California Environmental Protection Agency’s Officeof Environmental Health Hazard Assessment (September 1997)
THE BRITISH MEDICAL ASSOCIATION’S BOARD OFSCIENCE AND EDUCATION RECENTLY ESTIMATEDTHAT,IN THE UK,‘AT LEAST ONE THOUSAND PEOPLEARE ESTIMATED TO DIE EACH YEAR AS A RESULT OFEXPOSURE TO OTHER PEOPLE’S TOBACCO SMOKE.’
What the public wantsIn England 27% of adults smoke, making non-smoking, or, more accurately, smoke-free thenorm. The majority of adults who do notsmoke prefer breathing clean air to inhalingtobacco smoke.There is considerable supportamongst the general public in this countryfor much greater smoking restrictions inpublic places.
Table 3 Public views on smoking in public places
All people Current smokers
Percentage of people agreeing that smoking should be restricted:
at work 86% 72%in restaurants 87% 71%in pubs 50% 25%in other public places 85% 82%
Source: Smoking related behaviour and attitudes, 2001,Office for National Statistics.
Even amongst smokers there is a strongdesire to see sweeping measures to bringsmoke-free environments into public places.It is only in relation to pubs that the enthu-siasm among smokers for restrictions falls off.
A 2003 MORI survey about smoking inrestaurants in England revealed that over halfof adults said they would prefer to eat in anentirely smoke-free restaurant.The public’sknowledge of the health risks from second-hand smoke is variable. Generally those mostlikely to know about its health effects on bothadults and children are younger people(under 35 years) and those who have neversmoked.Woman and people living with achild under 11 years are most likely to beaware of the risk of cot death and ear infec-tions in children. Figures for people who areheavy smokers (over 20 a day) show a farlower understanding of the risks their smokepresents to others.
Table 4 Percentage of all adults who believe passive smoking increases a non-smokingadult’s risk of certain medical conditions
LUNG CANCER BRONCHITIS ASTHMA HEART DISEASE
Increases risk 86% 85% 80% 69%Does not increase risk 10% 11% 15% 24%Can’t say 4% 4% 5% 7%
Source: Smoking related behaviour and attitudes, 2001, Office for National Statistics


20 HEALTH CHECK CMO ANNUAL REPORT 2002
vulnerable are bar workers, waiters and wait-resses: the number of smoke-free pubs inEngland is fewer than 20.
Research among non-smoking bar staff inLondon pubs in 2001 measured cotinine, anaccurate indicator of exposure to second-hand smoke. Cotinine levels for these workerswere some three to four times greater thanthe average in non-smokers with smokingpartners. And they were 12 to 16 times morelikely to have a high cotinine level than non-smokers in the general population.
In the hospitality sector in this country theintroduction of smoke-free policies has beenpainfully slow. Objections usually centre onthe perception that becoming smoke-freewill result in a reduction in business for thehospitality industry. However a recent study,which reviewed nearly 100 published studieson the economic effect of smoke-free policieson the hospitality industry, concluded that "allthe best designed studies report no impactor a positive impact of smoke-free restaurantand bar laws on sales or employment".Thiscomplements previous work by the USOccupational Safety and HealthAdministration (OSHA) which estimated thatintroducing clean air policies increasesproductivity by 3%. Smoke-free workplacesalso eliminate the risk of legal action againstemployers who fail to protect theiremployees from second-hand smoke. As theWorld Bank puts it "fears in the hospitalityindustry that smoking bans may damagebusiness are largely unfounded".
.
Smoke-free workplacesIn the workplace, which covers practically allenclosed places the public might enter, UKemployers already have a requirement toprotect their employees under the Healthand Safety at Work Act 1974.This sets outhigh standards of health and welfareprotection for employees. Employers have aduty "to provide and maintain a safe workingenvironment which is, so far as is reasonablypracticable, safe, without risks to health andadequate as regards facilities and arrange-ments for their welfare at work." This includesconsidering exposure to second-hand smokeand failure to adhere to the Act will leaveemployers at risk of prosecution.
A draft Approved Code of Practice, whichtranslates the broad requirements of the 1974Act into specific guidance on tacklingexposure to second-hand smoke wasbrought forward by the Health and SafetyCommission in autumn 2000.This is still beingconsidered by Government.
Some worker protection from tobaccosmoke exposure has been achieved in thiscountry by voluntary action. In 2001 nearlyhalf of people said their workplace wassmoke-free, compared with 40% in 1996.
Although this is a rise of ten percent over afive year period, it still leaves half of the work-force in this country unprotected. It has beenestimated that some three million UK workersbecome passive smokers when they go towork whilst a further one million workers areexposed 75% of the time. Particularly
Advantages of smoke-free workplaces● Employee health, productivity, morale is higher.
● Employers can avoid the expected future increase in smoking-relatedworker compensation claims.
● Lower cleaning costs, reduced wear and tear on furniture and equipment,less chance of fire.
● Reduces nicotine-dependence, helping more workers who are smokers togive-up.
● Eliminate the chance of cigarette smoke chemicals combining with otherchemicals in the workplace to increase risks to health.

HEALTH CHECK CMO ANNUAL REPORT 2002 21
Second-hand smoke
Table 5 Estimated intake of chemicals from second-hand smoke by a restaurant worker in an eight hour shift
All chemicals shown in the table cause adverse health effects and those in bold type are carcinogens (they cause cancer).
CHEMICAL AMOUNT CHEMICAL AMOUNT CHEMICAL AMOUNT
(µg) (µg) (ng)
Carbon monoxide 5606 1,3-butadiene 25 Resorcinol 123
Tar 3128 Hydroquinone 24 Benzo[a]pyrene 18
Nicotine 678 Methyl ethyl ketone 23 Cadmium 9.7
Acetaldehyde 207 Catechol 22 1-aminonaphthalene 8.5
Nitric oxide 190 Propionaldehyde 17 Chromium 7.1
Isoprene 151 Cresols 15 Lead 6.0
Acetone 121 Hydrogen cyanide 14 2-aminonaphthalene 5.2
Toluene 66 Styrene 13 Nickel 4.2
Formaldehyde 54 Butyraldehyde 12 3-aminobiphenyl 2.4
Phenol 44 Acrylonitrile 11 4-aminobiphenyl 1.4
Acrolein 40 Crotonaldehyde 10
Benzene 36 Quinoline 1.3
Pyridine 33
Source: www.smoke-free.ca/factsheets/Chemicals.htm
As the majority of people in this countryare non-smokers, and object to otherssmoking near them, going smoke-free shouldrepresent an economic opportunity ratherthan a threat for the hospitality industry.
Smoking restrictions in the workplace havebeen established in Australia, Canada, HongKong and the United States of America. Othercountries have legislation to restrict smoking:the Netherlands, Kashmir, Sweden,Thailand,Romania and Italy.The 1995 California healthand safety legislation banning "the smokingof tobacco in all (100%) enclosed places ofemployment", saw a subsequentimprovement in the respiratory health ofbartenders who had previously beenexposed to considerable second-hand
smoke.The 1995 Finnish legislation to bansmoking in the workplace was associatedwith a reduction in workplace exposure aswell as in smoking prevalence.
Many other countries are in the process ofintroducing legislation. In Ireland the Healthand Safety Authority and the Office ofTobacco Control commissioned an inde-pendent investigation of the health risks ofsecond-hand smoke in the workplace. As aresult of the findings of this scientific workinggroup Ireland announced in January 2003that smoking will be banned in allworkplaces, including restaurants and pubs,from 1 January 2004. Attitudinal surveys inIreland since this announcement have shownstrong public support for this action.

ACTION ON SECOND-HAND SMOKE IS WHATTHE TOBACCO INDUSTRYHAS LONG FEARED MOST
‘THE ANTI-SMOKING FORCES'
LATEST TACK, HOWEVER – ON THE
PASSIVE SMOKING ISSUE – IS
ANOTHER MATTER.WHAT THE
SMOKER DOES TO HIMSELF MAY BE
HIS BUSINESS, BUT WHAT THE
SMOKER DOES TO THE NON-
SMOKER IS QUITE A DIFFERENT
MATTER. …THIS WE SEE AS THE
MOST DANGEROUS
DEVELOPMENT TO THE VIABILITY
OF THE TOBACCO INDUSTRY THAT
HAS YET OCCURRED’.
Source: Report commissioned by theTobacco Institute, cited in: RoperOrganization. A study of public attitudestoward cigarette smoking and the tobaccoindustry in 1978: Roper Organization; 1978.Vol. I. www.library.ucsf.edu/tobacco/mangini/html/l/104/

HEALTH CHECK CMO ANNUAL REPORT 2002 23
Second-hand smoke
In other countries, bans across individualcities, like that being introduced in New Yorkand led by Mayor Bloomberg, have served asa catalyst for wider change. An equivalent cityor town in England can act as a champion forsmoke-free public places across the countryand make a real impact on the health of theirpopulation. Regional Directors of PublicHealth have a key role in increasing smoke-free provision in their areas.
As part of moving towards a smoke-freesociety public awareness of the health risksassociated with passive smoking needs to beraised in all sections of the population.Smokers in particular need to be more awareof the risks to everyone, not just to childrenand to people with underlying illness, theirsecond-hand smoke presents.This willrequire a major new public educationcampaign.
In March 2003 New York City legislationbanning smoking in almost all public work-places, including bars and restaurants cameinto force.
Workplace smoking bans are a highlyeffective smoking cessation strategy.Estimated reductions in prevalence ofsmoking suggest a reduction from thepresent 27% to 23% if a comprehensive work-place ban were introduced in this country.Such a big gain could only be achievedthrough tax increases if the cost of cigaretteswere doubled.
Action to tackle passive smokingInternational experience has shown the onlyway to rapidly and successfully tackle thehealth risks from second-hand smoke is tointroduce a ban on smoking in public places.The recent lead taken by Ireland in providingthe evidence base and introducing legislationshows what it is possible to achieve.
The introduction of an Approved Code ofPractice, which will give guidance to allemployers on how they might meet theirexisting obligations under the Health andSafety at Work Act, will help to reduceexposure to tobacco smoke. But employerscan best meet their obligations, and minimisetheir costs, by becoming smoke-free.
The public sector should take a lead inbecoming smoke-free, and, as the biggestemployer in Europe, the NHS has a particu-larly important leadership role in providingsmoke-free environments. Smoking bansshould be the norm in all health care facilities,be rigorously enforced and be accompaniedby advice and support for staff and patientswho smoke. Directors of Public Health shouldact to ensure protection for staff and patientsin health care facilities in their areas.
The Department of Health has onlyrecently put its own house in order andbecame smoke-free on 1 April 2003. Similarlyall Government Departments should becomesmoke-free, and other public sectoremployers should set timetables forbecoming smoke-free and should insist onlocal services being smoke-free.
Introducing a smoke-free policy providesthe perfect opportunity for smokers to giveup. Support for smokers when introducingsmoke-free policies should be providedthrough local smoking cessation services.TheNHS stop smoking service is available to helpemployers who want to end smoking in theirworkplace.
New cigarette packwarnings take up morespace and are more explicit.
Conclusion
Second-hand smoke is harmful to humanhealth.Restrictions on smoking in publicplaces and overall smoking prevalencereduction are the key strategies to reducesecond-hand smoke exposure.Moves tomake public places smoke-free will both elim-inate the health risks and lead to more peoplegiving up smoking.More and more majoremployers are appreciating the benefits ofsmoke-free policies:cuts in sickness absen-teeism, fire insurance costs, maintenance costfor redecoration of premises and unscheduledwork breaks by smokers.Going smoke-freealso represents an opportunity for pubs, barsand restaurants to attract new customers; aswell as fully protecting the health of theiremployees.
As more and more countries and citiesaround the world make the change fromsmoke-filled to smoke-free rooms our countryhas the opportunity now to be in the forefrontof this improvement in public health.
Action recommended +
24 HEALTH CHECK CMO ANNUAL REPORT 2002
Very serious consideration should be given to introducing a banon smoking in public places soon.
All employers should plan to introduce smoke-free workplaces.
Public awareness of the health risks from second-hand smokeshould be increased through comprehensive educationcampaigns.These should be undertaken at national, regionaland local levels and by a wide range of organisations includinghealth professional bodies.
Health professionals’knowledge of the health risks fromsecond-hand smoke should be improved. Health professionalrepresentative bodies and academic/training organisationshave a key role.
Local tobacco alliances should raise awareness of second-handsmoke and, through broad coalitions of local decision makers,campaign for more smoke-free public and work places in theirregions.
The public sector, particularly Central GovernmentDepartments and the health service, should take a lead and thisyear set dates by which their premises will be become entirelysmoke-free.
Parliamentary buildings should become smoke-free and datesshould also be set to achieve this.
Regional Directors of Public Health should develop plans totackle second-hand smoke as part of their regional tobaccocontrol strategies and should take the lead as local championsof change.
Drawing on the experience of the United States, a measure ofthe population’s exposure to second-hand smoke at work andat home should be introduced to set a baseline and monitorprogress on smoke-free environments.

HEALTH CHECK CMO ANNUAL REPORT 2002 25
Givingupsmoking.co.uk. Implementing aworkplace smoking policy.http://www.givingupsmoking.co.uk/employers/workplace/implementing.htm
Tobacco control policies within the NHS: casestudies of effective practice. 2000;[23].http://www.hda-online.org.uk/documents/tobac_controlpol.pdf
Smoking policy for the workplace: an update.1999;[19].http://www.hda-online.org.uk/documents/smokingpolicy_update.pdf
Been there, done that: revisiting tobaccocontrol policies in the NHS. 1999;[63].http://www.hda-online.org.uk/documents/beentheredonethat.pdf
British Medical Association.Towards smoke-free public places. 2002.http://www.bma.org.uk/ap.nsf/Content/Smokefree
Centres for Disease Control and Prevention.Tobacco information prevention sources(TIPS) environmental tobacco smoke (ETS) –second-hand smoke. 2003.http://www.cdc.gov/tobacco/ets.htm
World Health Organisation and the TobaccoFree Initiative. Secondhand smoke.http://www5.who.int/tobacco/page.cfm?pid=43
Second-hand smoke
KEY WEB RESOURCES AND REFERENCES
SmokeFree London. Do you want that with, orwithout, someone else's cigarette smoke,madam. 2003.http://www.smokefreelondon.com/media
Lader D, Meltzer H. Smoking-relatedbehaviour and attitudes 2001: a report onresearch using the ONS Omnibus Surveyproduced by the Social Survey Division of theOffice for National Statistics on behalf of theDepartment of Health.The Stationery Office; 2002.http://www.statistics.gov.uk/downloads/theme_health/Smoking_Related_2001.pdf
Action on Smoking and Health (ASH),National Asthma Campaign,Trades UnionCongress. Smoking in the workplace. 2001.http://www.ash.org.uk/html/workplace/html/workplace.html
World Bank Health, Nutrition and Population.Smoke-free workplaces at a glance. 2002.http://www1.worldbank.org/tobacco/AAG%20SmokeFree%20Workplaces.pdf
Eisner et al. Bartenders respiratory health afterestablishment of smoke-free bars andtaverns. JAMA, 1998; 280: 1909-1914.
Health and Safety Authority and the Office ofTobacco Control, Ireland. Report on the healtheffects of environmental tobacco smoke (ETS)in the workplace. 2002.http://www.otc.ie/images/Reportfinal2.pdf. orhttp://www.ie.osha.eu.int/publications/tobacco_report.pdf
New York City Department of Health andMental Hygiene. Health Commissioner kicksoff start of 2002 Smoke-free Air Act withbartenders and waitresses. 2003.http://home.nyc.gov/html/doh/html/public/press03/pr027-0325.html
West R. Banning smoking in the workplace.BMJ 2002 Jul 27; 325(7357):174-175.
Poswillo David (Chairman) Great BritainScientific Committee on Tobacco and Health.Report of the Scientific Committee onTobacco and Health.The StationeryOffice;1998.http://www.archive.official-documents.co.uk/document/doh/tobacco/part-2.htm

26 HEALTH CHECK CMO ANNUAL REPORT 2002

West Nile virus
HEALTH CHECK CMO ANNUAL REPORT 2002 27
West Nile virus (WNV) is one of a family ofviruses that can cause encephalitis (braininflammation) in people. Other infectionscaused by this group of viruses include StLouis encephalitis and Japanese encephalitis.
Before recent events involving West Nilevirus in the United States of America, suchdiseases were far removed from beinghousehold names.The public’s awareness ofinfectious diseases more generally is largelyconfined to the common childhood diseases,some now largely prevented by vaccination(such as measles, mumps, diphtheria, rubellaand poliomyelitis); the more serious andpotentially life-threatening infections such asHIV/AIDS, meningitis and tuberculosis; and,those infectious diseases experienced bymost people during their lifetime such ascolds, influenza and food poisoning.
West Nile fever is an example of a type of disease termed
a ‘new or emerging’ infection. Until 1999 it had largely
been confined to the Old World. In that year it broke free of
its traditional geographical boundaries and was discovered
in New York City where 62 people became infected and
seven died of West Nile virus (WNV) infection. By the end of
2002, the virus has been found in 44 States and the District
of Columbia in the United States of America. Although the
risks of West Nile virus coming to the United Kingdom have
been assessed as ‘low’, the possibility cannot be ruled out
and contingency plans need to be put in place.
WEST NILE VIRUSREBORN IN THE USA

HEALTH CHECK CMO ANNUAL REPORT 200228
1West Nile virus (WNV) is anarbovirus or ‘arthropod-borne’virus; the natural host is birdsand the virus is usually trans-mitted by mosquitoes and cancause illness in people and somemammals (e.g. horses).
2West Nile virus has been trans-mitted through blood trans-fusion, organ transplantationand breast milk in a number of cases in the United States of America.
3When West Nile virus infectspeople it usually does not causesymptoms but when illness doesoccur it is most often a mild ‘flu-like condition. Some peopledevelop serious illness includingencephalitis; of those withserious symptoms an average of12% will die.There is currentlyno specific treatment or vaccinefor this infection.
4West Nile virus (WNV) wasdiscovered in Uganda, Africa in1937 and its occurrence over theyears has been mostly confinedto certain endemic areas in theso-called Old World (e.g. Israel,Africa, India, and Egypt).
Key points
5In 1999, the virus made its firstsurprising appearance in theNew World where in New YorkCity, deaths amongst blackcrows heralded the first humancases: 62 people were infectedand seven died in that year.
6Since then West Nile virus hasspread across the United Statesof America with infection beingdetected in birds, other animalsand mosquitoes. In 2002, 4161people were reported asinfected with the virus and 277died. In 2002 the largestoutbreak occurred in Illinois(835 cases).
7Three main factors willdetermine whether West Nilevirus establishes itself in thiscountry: climate change,whether the bird population isinfected and the nature and thedistribution of the mosquitopopulation.The risk of theinfection coming to the UnitedKingdom has been assessed as‘low’ for climatic reasons andbecause mosquito populationshere are relatively small.
8The possibility cannot be ruledout, however, and it is importantto have in place national contin-gency plans.
Above: Culex pipiens

West Nile virus
HEALTH CHECK CMO ANNUAL REPORT 2002 29
A new and emerging infectionWhen I produced the first ever comprehensiveinfectious diseases strategy for the NHS inJanuary of 2002 (‘Getting Ahead of the Curve’,www.doh.gov.uk/cmo/idstrategy), I drewattention to the problem of so-called ‘newand emerging infections’and gave West Nilefever as an example. Factors such as greatlyincreased international travel and trade,urbanisation, change in land use and climatechange can affect the delicate balancebetween micro-organisms (such as bacteriaand viruses), their environment and people.Infectious diseases can appear that werepreviously unrecognised.Those that havehitherto caused only mild illness can becomemore virulent or serious. Diseases that were aproblem in only a small part of the world canbecome a global threat.
West Nile virus was first discovered in theWest Nile area of Uganda, Africa in 1937.Themost common symptom after being infectedwith West Nile virus is a mild ‘flu-like illness.
West Nile virus in North AmericaIt was the sudden and completely unex-pected emergence of West Nile virus in NorthAmerica that has so greatly raised the profileof the infection as a public health problem(Figure 1 next page).
The first sinister sign was an unexpectednumber of dead crows in the City of New Yorkin the summer of 1999. In August 1999people began to fall ill with viral encephalitiswhich eventually affected 62 people ofwhom seven died.West Nile virus wasresponsible.
Mosquito spraying and the onset of colderweather brought the 1999 outbreak in NewYork City to an end.This was not the end ofWest Nile virus in North America. Since 1999,when West Nile virus was present in fourstates, it has spread extensively to reach 44states and the District of Columbia and fiveCanadian provinces by the end of 2002.Thevirus was found in more than 140 species ofbirds, in 36 species of mosquito, in horses, and
However, a proportion of those infected bythe virus will develop serious symptoms.Characteristically these will include acuteencephalitis (inflammation of the brain).Other serious symptoms can include menin-gitis and muscle paralysis or weakness,abdominal pain and rash. Around 12% ofthose with serious symptoms will die fromthe disease.
Until recently, the virus has tended to beconfined to tropical and subtropical areas ofthe world where it has caused occasionaloutbreaks of West Nile fever: for example, inIsrael in the 1950s and in South Africa in theearly 1970s.
During the mid-1990s, there were signsthat West Nile virus was beginning to breakout of its traditional geographical boundaries.Outbreaks of infection with the virusoccurred in the mid-1990s in Romania,Morocco and Tunisia. In the late 1990s, inRussia, some 800 human cases were reported (Table 1).
0 50 100 150 200 250 300
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
Figure 2 Papers in peer reviewed journals on West Nile FeverTable 1 West Nile virus occurrence worldwide
OLD WORLD
First discovery Western Nile, Uganda, Africa, 1937
Countries where Uganda Romania
epidemics have Central African Republic Israel
been reported Madagascar Italy
South Africa Russia
Egypt India
France
NEW WORLD
Human cases
First discovery New York, USA, 1999
Countries where USA 1999, 62 cases in 4 states
epidemics have (Declared endemic in 2002) 2000, 21 cases in 5 states
been reported 2001, 66 cases in 11 states
2002, 4161cases in 39 states
and District of Columbia
Canada (2002) Human cases in three provinces
Virus isolation in Cayman Islands (2001) Suspected human case
other countries

30 HEALTH CHECK CMO ANNUAL REPORT 2002
1999 (Figure 3).There is evidence to indicatethat within Lineage 1 the strains of virus circu-lating in North America are different fromthose circulating in Europe, though they areinfecting the same species of mosquitoes.
It has been suggested that the strain ofvirus responsible for the outbreak in New Yorkoriginated in Israel or elsewhere in the MiddleEast as the virus is most closely related, geneti-cally, to a West Nile virus strain that has circu-lated in Israel since 1997 and caused birddeaths. It has also been suggested that WestNile virus was introduced to the United Statesof America through the importation of aninfected bird (it first appeared near the BronxZoo), or possibly the arrival of an infectedperson, probably by air. Increased internationaltraffic may have increased the chance of thevirus’s arrival in the United States of America.Once there, the virus evidently foundgenerally permissive environmental condi-tions.Establishment may have been facilitatedby warmer than average weather in 1999.
were confirmed and 20 were fatal, as well asevidence that the virus was present in birdsand mosquitoes.Surveillance in France in2001 and 2002, concentrated on the areaswhere horses had been infected in the 2000outbreak, failed to find any evidence of WestNile virus in people, birds or mosquitoes.
Genetic analyses of West Nile virus providemore information on the structure of theviruses and aid in identifying the origin of theviruses in future outbreaks.Detailed studies ofthe virus have shown that there are twogenetic ‘lineages’, usually referred to as‘Lineage 1’and ‘Lineage 2’. Lineage 1 viruseshave been isolated in North,West and CentralAfrica, Southern and Eastern Europe, India, theMiddle East and Australia (Kunjin virus).Lineage 2 viruses have been isolated fromWest Africa, Central Africa, East Africa andMadagascar.All West Nile virus strains isolatedduring outbreaks in the last decade havebelonged to Lineage 1 including the virusresponsible for the outbreak in New York in
other mammals (bats, cats, rabbits andskunks). A particularly unusual feature in 2002was the rapid spread of infection to horsesacross the country. In 2002, 4161 people wereinfected with West Nile virus and 277 died.
Since its unexpected emergence as apublic health threat in North America,WestNile fever has been the subject of intensiveepidemiological and scientific study.Thegrowth of articles in the medical and scien-tific literature has been explosive over the lastfour years (Figure 2).
There has been a great deal of speculationabout the reason for the emergence of WestNile virus in North America.The effects ofWest Nile virus in America are in stark contrastto those associated with outbreaks elsewherein Europe. In the year 2000 there was anoutbreak of West Nile virus in the Camargueregion of France, the first such outbreak in thearea for 35 years.There, no human cases ofWest Nile fever occurred despite 141suspected clinical cases in horses of which 58
Figure 1 West Nile Virus in the United States 1999-2002

HEALTH CHECK CMO ANNUAL REPORT 2002 31
In North America, the action taken hasincluded: intensified surveillance of birds,certain other mammals, and mosquitoes; themonitoring of human encephalitis-type infec-tions; the implementation of mosquitocontrol measures; and, a comprehensivepublic health education campaign.
Health education messages to the public inaffected areas of the United States of Americainclude advice on the use of insect repellentwhen outdoors, wearing long sleevedclothing and long trousers, staying indoors at
dawn and dusk and eliminating standingwater sources around the home.
Transmission of West Nile virus (WNV)People are exposed to the West Nile virusthrough the bite of a mosquito. In the UnitedStates of America,West Nile virus has beenassociated with over thirty mosquito species,primarily members of the Culex species,including Culex pipiens, and Aedes vexans.
West Nile virus circulates in the blood ofinfected people. During 2002, 61 cases of
infection with West Nile virus in the UnitedStates of America were investigated after itwas suspected they had been acquiredthrough blood transfusion. Actual evidence oftransmission of West Nile virus through bloodtransfusion has been found in 23 of thesecases.There have also been a small number ofcases of West Nile fever in the United States ofAmerica following organ transplantation.Transmission of West Nile virus from breastmilk and intra-uterine transmission have alsobeen reported.The breast milk transmission
West Nile virus
The virus was found in morethan 140 species of birds, in 36species of mosquito, in horses,and other mammals (bats, cats,rabbits and skunks). In the USA,a particularly unusual featurein 2002 was the rapid spread ofinfection to horses across thecountry. In 2002, 4161 peoplewere infected with West Nilevirus in the USA and 277 died.
Kunjin
India
LIN-1
LIN-2
Phylogenetic Tree of West Nile Virus Strains(Envelope gene)
Modified from: Lanciotti et al.Science 1999
Source: The Centers for Disease Control and Prevention
Egypt 1951France 1965
South AfricaIsrael 1952
Romania 1996 MKenya 1998Senegal 1993Morocco 1996Italy 1998Volgograd 1999New York 1999Israel 1998-ANY2000 3282NY2000 3356NY 1999 equineNY 1999 humConn 1999MD 2000NJ 2000Israel 1999 HC.Afr.Rep 1989Senegal 1979Algeria 1968C.Afr.Rep 1967Iv.Coast 1981Kunjin 1960Kunjin 1973Kunjin 1984bKunjin 1991Kunjin 1984aKunjin 1966Kunjin 1994India 1955aIndia 1980India 1958India 1955bKenyaUgandaSenegal 1990Uganda 1937C.Afr.Rep 1972aC.Afr.Rep 1983Uganda 1959C.Afr.Rep 1972bMadagascar 1988Madagascar 1986Madagascar 1978JE SA 14
USA / ISRAEL
Figure 3 West Nile virus strain found in different outbreaks (country and year

HEALTH CHECK CMO ANNUAL REPORT 200232
followed infection of the mother by bloodtransfusion.The authorities in the UnitedStates of America are continuing their investi-gation into these incidents. In the UnitedKingdom, viral inactivation of blood plasmaimported from the United States of Americais carried out as a safety measure to removethe risk to patients from transfusion transmis-sible viruses, including West Nile virus.
Implications for health protection inthe United KingdomGiven the recent increases in West Nile virusactivity elsewhere in the world, it is importantto assess the implications for the health of thepopulation here.Three main factors woulddetermine whether West Nile virus becameestablished in this country.
The mosquito populationFirst, the distribution and abundance ofdifferent species of mosquito are key factors.Of the thirty-two species of mosquitorecorded in Britain, at least seven speciescould potentially transmit West Nile virus(Table 2).These include members of theCulex pipiens complex to which the commonhouse mosquito belongs, as well as the wide-spread Aedes cantans, found in woodlands.Not all of these species bite people to thesame extent.Their relative importance to thepotential of an epidemic of West Nile fever inthe United Kingdom therefore remainsunknown. Should West Nile virus be intro-duced to the United Kingdom, the most likelyvectors would be mosquitoes belonging tothe most widely distributed Culex pipienscomplex.These species are part of both the'bird-mosquito' and the 'bird-mosquito -human' cycles of West Nile virus circulation.They are known to have transmitted WestNile virus in the Middle East and in the formerSoviet Union.They were also implicated asthe principal vector in Romania in the 1990’s.The actual, rather than potential, role of thesemosquito species depends on their abun-dance.
The chances of the domestic birdpopulation becoming infectedSecondly, the emergence of West Nile fever inthis country will depend on whether the birdpopulation in the United Kingdom becomesinfected. Migratory birds have been instru-mental in the periodic reintroduction of WestNile virus to Europe (Figure 4). A recent studylooking for evidence of infection with West
Nile virus amongst both migratory and non-migratory birds has suggested that West Nilevirus is already present in native birds in theUnited Kingdom. However, these results needto be confirmed and further studies are beingundertaken in collaboration withGovernment Agencies.These include a surveyof bird carcasses submitted to laboratories forantibody detection and virus isolation.
Climate ChangeBoth the first two necessary conditions mightbe facilitated by climate change (Figure 5).Insect vectors are very sensitive to meteoro-logical conditions.Temperature and humidity,as well as food, predators and parasites areknown to influence significantly the trans-mission of West Nile virus. If the scenario ofglobal warming is correct (e.g. warm wintersfollowed by hot, dry summers), thenincreased temperatures could enhance thepopulation density of vector mosquitoes,although drier summers could ameliorate thiseffect.Warmer weather would also influence
people's behaviour leading to themspending more time outdoors in situationswhere they would be more prone tomosquito bites.The decreased seasonalclimatic variability accompanying globalwarming is an important factor and may haveencouraged the surprise emergence of theWest Nile virus in New York City in 1999.
Progress in assessing the risk to theUnited KingdomIn July 2002 I met with experts to discuss therisks for this country and the need to beprepared in the light of events in the UnitedStates of America.
The Department of Health is fundingstudies to determine whether West Nile virusis present in mosquitoes in England and alsoto assess the distribution of differentmosquito species in central and southernEngland.This work is vital. It will help us toassess the risk of human West Nile virusinfection occurring in the United Kingdom.
The Communicable Disease Surveillance
Table 2 Possible vectors of West Nile virus for the United Kingdom (UK):Mosquito species native to, or with the potential for introduction to, the UK
MOSQUITO CURRENTLY RECORDED IN UK FEEDS ON HUMANS
Aedes albopictus No – native to Asia. Imported to US, Belgium and France Yes
Aedes cantans Yes – widespread Yes – not prolifically (mainly cattle)
Aedes caspius Yes - scattered locations in England and Wales Yes
Aedes cinereus Yes – widespread but patchy distribution Yes
Aedes punctor Yes - widespread Yes
Aedes vexans Yes - limited scattered locations in England and Wales Yes
Anopheles atroparvus Yes - Limited scattered locations particularly in southern England Yes
Coquillettidia richiardii Yes – widespread in England and Wales Yes
Culex modestus Unlikely. Recorded in UK in 1944-45 but not since. Native to Mediterranean areas Yes
Culex pipiens ‘typical’ form Yes – ubiquitous Rarely (mainly birds)
Culex pipiens ‘molestus’ form Yes – mainly in urban areas Yes
Culex territans Yes - limited scattered locations in Yes – not prolifically England and Scotland (mainly birds & cattle)
Aedes atropalpus No - common in eastern North America.Imported to Italy Yes
Aedes japonicus No - native to Korea, Japan,Taiwan and southern China. Also been found in northern France and imported to the US Yes

West Nile virus
HEALTH CHECK CMO ANNUAL REPORT 2002 33
Mosquito vector
Bird reservoir hosts Incidental infections
Incidental infections
WEST NILE VIRUS
Figure 5 Predicted spread of West Nile virus in the United Kingdom based on modelling
Global model for West Nile virus (WNV) usingglobal Old World WNV data.The probability ofhabitat similarity to regions from which WNV isreported in Europe (shown as the blue dots)was established using discriminant analyticaltechniques applied to 30-year climate norms,and is coloured from red (low probability) togreen (high probability).Very few regions in
Figure 4 Transmission cycle of West Nile VirusCentre of the new Health Protection Agencyhas increased surveillance to identify peoplewho fall ill with aseptic meningitis andencephalitis. In this way any new or unex-plained increase will be detected quickly andthe possibility of West Nile virus infectioncould then be assessed.This surveillanceincludes a look-back survey of laboratorysamples from patients with nervous systemdisease compatible with West Nile fever. Astudy into the causes of viral encephalitis andviral meningitis is also planned for 2003.
Conclusion
Although there has been no recorded case ofinfection with West Nile virus in the UnitedKingdom so far, it is important to remainvigilant to the threat of such vector-bornediseases. Future environmental changes, suchas global warming, may affect the ecology ofthe United Kingdom and may lead to theintroduction of new pathogens such asarboviruses.
the UK are predicted to be similar to any WNVregion (see inset), but those parts of the USAcoloured green here have been invaded byWNV since 1999. Grey regions = habitats sodifferent from any of the WNV sites that nopredictions are possible for them (the defaultassumption is that they are WNV negative).Source:TALA Research Group, University of Oxford
= 0.00 – 0.349
= 0.35 – 0.449
= 0.45 – 0.499
= 0.50 – 0.549
= 0.55 – 0.649
=0.65 – 1.00
KeyProbability of habitatsuitability for WestNile virus

ENHANCED AND STRENGTHENEDSURVEILLANCE OF THE BIRDPOPULATION IN THIS COUNTRYSHOULD BE CARRIED OUT TO SEEKEVIDENCE OF WEST NILE VIRUSEXPOSURE AND INFECTION.

West Nile virus
HEALTH CHECK CMO ANNUAL REPORT 2002
Action recommended +
35
Enhanced and strengthened surveillance of the bird populationin this country should be carried out to seek evidence of WestNile virus exposure and infection.
Surveillance and regular testing for West Nile virus of themosquito population should be initiated in different parts of thecountry and in a way that enables different species of mosquitoto be monitored.
Enhanced and strengthened surveillance of relevant animalpopulations (e.g. horses) should be carried out to seek evidenceof West Nile virus exposure or infection.
Guidance on laboratory testing and safety procedures for WestNile virus should be prepared and provided for those laboratoriesthat might undertake testing.
Scientific research should be commissioned to develop valid andreliable tests to distinguish between active and inactive or postWest Nile virus infection.
Enhanced clinical surveillance should be carried out to provideearly warning of West Nile virus amongst people who are ill withmeningitis, encephalitis or related conditions.
Travellers should be given practical advice on how to reduce therisk of being infected with West Nile virus when visiting endemicareas (e.g. parts of the United States of America).
Health education advice for the public should be prepared incase West Nile virus should become established in this country.
Scientific advice should be obtained on the effectiveness andsafety of various insecticides in case their more widespread use iswarranted.
Scientific advice should be obtained on the most effective way ofreducing mosquito larval sources and breeding ponds.
A full contingency plan against the possibility of West Nile virusemerging and becoming established in this country should bepublished within the next two months.
KEY WEB RESOURCES AND REFERENCES
Department of Health:http://www.doh.gov.uk
Health Protection Agency http://www.hpa.org.uk/
Getting ahead of the curve - the Chief Medical Officer’sstrategy for combating infectious diseases,pp.41,43.http://www.doh.gov.uk/cmo/idstrategy/index.htm
CMO Update 29 (Feb 01): 'Unusual disease diagnosis' http://www.doh.gov.uk/cmo/cmo_29.htm
Public Health Laboratory Servicehttp://www.phls.org.ukhttp://www.phls.org.uk/topics_az/west_nile/menu.htm
Communicable Disease Reports weekly and monthly:http://www.phls.co.uk/publications/index.htmhttp://www.phls.org.uk/publications/pdf/cdph_wnv.pdf
Morbidity and Mortality Weekly Reporthttp://www.cdc.gov/mmwr/index.html
Association of Medical Microbiologyhttp://www.phls.org.uk/publications/pdf/cdph_wnv.pdf
CDC West Nile Virus Home Pagehttp://www.cdc.gov/ncidod/dvbid/westnile/index.htm
UK Zoonoses Grouphttp://www.defra.gov.uk/animalh/diseases/zoonoses/ukzg/index.htm
Advisory Committee on Dangerous Pathogenshttp://www.doh.gov.uk/acdp/index.htm
Crook PD et al. (2002) West Nile virus and the threat to theUK.Communicable Disease and Public Health 5(2):138-143.http://www.phls.co.uk/publications/cdph/issues/CDPHVol5/no2/CDPHv5n2.html
Davsion,K.L.et al. (2003) Viral Encephalitis in England 1989-1998:What Did We Miss? Emerging Infectious Diseases 9(2):234-240.http://www.cdc.gov/ncidod/EID/vol9no2/pdfs/02-0218.pdf
Giladi et al.(2001) West Nile Encephalitis in Israel,1999:TheNew York Connection EID 7(4):659-661.http://www.cdc.gov/ncidod/eid/vol7no4/giladi.htm
Scherret at al. (2001) The relationship between West Nileand Kunjin viruses.EID 7(4):697-705.http://www.cdc.gov/ncidod/eid/vol7no4/scherret.htm
Petersen et al. (2002) West Nile virus:a primer for theclinician.Annals Internal Medicine 137:173-179.

HEALTH CHECK CMO ANNUAL REPORT 200236

HEALTH CHECK CMO ANNUAL REPORT 2002 37
It is well recognised that overweight and obesity increase the risk of this country'sbiggest killer diseases – coronary heart disease and cancer – as well as diabetes, highblood pressure and osteoarthritis.The National Audit Office (NAO) found that obesityis responsible for more than 9,000 premature deaths each year in England and reduceslife expectancy on average by nine years. Obesity also has significant financial costs,both to the NHS and the wider economy. In common with other countries aroundthe world, levels of obesity in England are rising.The consequences are serious.
BESITYdefusing the health time bomb

38 HEALTH CHECK CMO ANNUAL REPORT 2002
Key points
OBESITY LEVELS IN ENGLAND HAVE TRIPLED IN THE PAST TWO DECADES; AROUND A
FIFTH (21%) OF MEN AND A QUARTER (24%) OF WOMEN ARE NOW OBESE
WHILST ALMOST 24 MILLION ADULTS ARE NOW OVERWEIGHT OR OBESE.
OBESITY IS ALSO RISING AMONG CHILDREN – IN THE FIVE YEARS BETWEEN 1996 AND
2001,THE PROPORTION OF OBESE CHILDREN AGED 6-15 YEARS ROSE BY SOME 3.5%.
CASES OF MATURITY-ONSET DIABETES ARE STARTING TO EMERGE IN CHILDHOOD.
WORLDWIDE,AROUND 58% OF TYPE 2 DIABETES,21% OF HEART DISEASE
AND BETWEEN 8% AND 42% OF CERTAIN CANCERS ARE ATTRIBUTABLE TO
EXCESS BODY FAT.
OBESITY IS RESPONSIBLE FOR 9,000 PREMATURE DEATHS EACH YEAR IN
ENGLAND,AND REDUCES LIFE EXPECTANCY BY,ON AVERAGE,9 YEARS.
OBESITY COSTS THE ECONOMY AT LEAST £2.5 BILLION A YEAR – INCLUDING
COSTS TO THE NHS AND COST TO INDUSTRY THROUGH SICKNESS ABSENCE.
STEMMING THE INCREASE IN OBESITY RATES WILL NEED EFFECTIVE MEASURES TO
IMPROVE DIET AND INCREASE EXERCISE LEVELS IN THE POPULATION.
ACTION BY THE FOOD AND FITNESS INDUSTRIES,AS WELL AS BY GOVERNMENT AND
LOCAL AGENCIES,IS NEEDED.

HEALTH CHECK CMO ANNUAL REPORT 2002 39
The scale of the problemThe growth in the number of people in thepopulation who are overweight and obese isof increasing concern in most developedcountries of the World. So much so that it hasbeen termed a ‘global epidemic’.
Overweight and obesity are mostcommonly assessed through the Body MassIndex (BMI) – calculated by dividing a person’sweight in kilograms by their height in metressquared (kg/m2). In England, an individual isconsidered to be ‘overweight’ if their BMI isbetween 25 and 30, and obese if over 30.Based on these definitions, around 21% ofadult men and 24% of adult women are nowobese. A further 47% of men and 33% ofwomen are overweight. So, two-thirds of allmen, and half of all women are now over-weight or obese.This is almost 24 million
adults. Rates have been rising in England, incommon with other countries, and havetrebled in the last 20 years.
Over the last few years in particular, publicattention has been drawn by a number ofinfluential bodies to the problem of obesity.This concern is not misplaced. Obesity rateshave increased dramatically in mostdeveloped countries. Although levels ofobesity in England have not yet reachedthose seen in the United States – where atthe start of the 21st century almost a third(31%) of all adults are obese (an increase froma quarter just a decade earlier) – a continu-ation of the recent trend of rising numbers ofoverweight and obese people would bedisastrous for the future health of our country.Globally now, more than one billion adults areoverweight and at least 300 million are obese.
Obesity:defusing the health time bomb
Prevalence of obesity (BMI >30 kg/m2)in adults aged over 16 years in England
1980*
86/87*
1993
1994
1995
1996
1997
1998
1999
2000
2001
0
Men Women
5 10 15 20 25%
* Data for 1980 and 1986/87 are for adults aged 16-64 years inGreat Britain. Source: ONS The Heights and Weights of Adultsin Great Britain, 1980; ONS The Dietary and Nutritional Survey
of British Adults, 1986/87; ONS, Health Survey for England1993; National Centre for Social Research, Health Survey forEngland, 1994-2001

40 HEALTH CHECK CMO ANNUAL REPORT 2002
globally we will see a one third increase in theloss of healthy life as a result of overweightand obesity over the next 20 years, with thenumber of global deaths rising from threemillion to five million each year.The WorldHealth Organisation estimates that around58% of type 2 diabetes, 21% of heart diseaseand between 8% and 42% of certain cancersare attributable to excess body fat.
For the NHS, it has been estimated that,based on current trends of increase, a generalpractice with 10,000 patients and five doctorswould have to cope with 80 new obesepatients each year. Already there is a signif-icant increase in NHS costs. Since the NationalInstitute of Clinical Excellence (NICE) issuedguidance on the prescribing of the anti-obesity drugs Orlistat and Sibutramine in2001, the number of these drugs dispensedhas trebled.
For those who are already obese, even amodest weight loss can have substantialbenefits. A 10kg loss is associated with a 20%fall in total mortality and a 10% reduction intotal cholesterol. Based on the National AuditOffice figures, it is estimated that one millionfewer obese people in this country could leadto around 15,000 fewer people with coronaryheart disease, 34,000 fewer people devel-oping type 2 diabetes, and 99,000 fewerpeople with high blood pressure.
Health risks of obesity As well as increasing mortality, it is well estab-lished that obesity is also associated withincreasing the risk of many serious diseases.
Obesity is associated with increasedrisk of:● Premature death● Heart disease and stroke● Type 2 diabetes● Hypertension● Angina● Gall bladder diseases● Osteoarthritis● Sleep apnea● Breathing problems● Some cancers, including
postmenopausal breast cancer andcolon cancer
● Lower back pain● Complications in pregnancy● Complications in surgery● Psychological and social problems● Reproductive disorders
The rapid increase in obesity in the UnitedStates has also been mirrored by an increase inthe prevalence of diabetes – by a thirdbetween 1990 and 1998.Such a scenario isalso being seen here,where 75% of adults withnewly diagnosed type 2 diabetes are over-weight or obese. In 2002,cases of ‘adult onset’diabetes in obese children were reported forthe first time in the United Kingdom.
ImplicationsThe World Health Organisation has recentlyhighlighted that in 2002 alone, around half amillion people across North America andEurope will die from obesity related diseases.It is estimated that if no action is taken,
Children: a particular concernObesity is more common in older age groupsbut the growth in the proportion of over-weight and obese children is a majorconcern. Analyses of the Health Survey forEngland suggest that a considerable numberof children are either overweight or obese –for example, in 2001 8.5% of 6 year olds and15% of 15 year olds were obese1. Despitedifferences of view on the definition of over-weight and obesity in childhood, all recentstudies, no matter which method is used,have shown that overweight and obesity arebecoming more common amongst childrenin England. Between 1996 and 2001 theproportion of overweight children (aged 6-15years) increased by 7% and obese children by3.5%. Particularly worrying are the first signsof children presenting with maturity-onset(or Type 2) diabetes which in the past hasoccurred in middle and older age.Researchers in the United Kingdom haverecently warned that the increase in obesitythreatens to reverse gains in longevity madeduring the last hundred years and in somecases could result in parents outliving theirchildren.
A health inequalities issueObesity is also a health inequalities issue –and there are large social class differences,particularly in women.The Health Survey forEngland has shown that in 2001 amongstprofessional groups 14% of men and womenare obese, compared to 28% of women and19% of men in unskilled manual occupations.Amongst women, there are also importantdifferences between ethnic groups: in 1999obesity was 50% higher than the nationalaverage amongst Black Caribbean womenand 25% higher amongst Pakistani women.
footnote 1: Calculations based on BMI above the 95thpercentile to represent obese and BMI above the 85thpercentile to represent overweight
0
20
40
60
80
100
Thousands
Coronaryheart disease
15,000FEWER CASES
34,000FEWER CASES
99,000FEWER CASES
Type 2Diabetes
High bloodpressure
Source: Reilly JJ, Dorosty AR. Epidemic of obesity in UK children. Lancet 1999; 354:1874.(using data from Health Survey for England 1995/97)
One million fewer obese people in the population could lead to…
BETWEEN 1996 AND 2001 THE PROPORTION OFOVERWEIGHT CHILDREN (AGED 6-15 YEARS)INCREASED BY 7% AND OBESE CHILDREN BY 3.5%.PARTICULARLY WORRYING ARE THE FIRST SIGNSOF CHILDREN PRESENTING WITH MATURITY-ONSET (OR TYPE 2) DIABETES WHICH IN THE PASTHAS OCCURRED IN MIDDLE AND OLDER AGE.

5 A DAY

42 HEALTH CHECK CMO ANNUAL REPORT 2002
each day) could prevent around 30% of newcases of obesity. Limiting TV viewing inchildren has also been associated with areduction in obesity – possibly by reducingthe snacking associated with TV viewing aswell as increasing activity.
Other changes in lifestyle may also beimportant – for example, alcohol intakesamong women and young men haveincreased in England during the past decade;alcohol provides almost as many calories asfat and high intakes have been shown tocontribute to weight gain and obesity.
What is being done to tackle obesity?The World Health Organisation has recentlyhighlighted prevention as the key to loweringthe global burden of heart disease and stroke.More than half of deaths and disability fromheart disease could be prevented by nationaland individual action to reduce major riskfactors, including obesity.
The Department of Health cannot tackleobesity alone. Considerable action is beingtaken across government to tackle obesity,especially through improving diet andincreasing physical activity levels. More needsto be done.The Department of Health isleading on the development of a new Foodand Health Action Plan, which will be of directrelevance to the prevention andmanagement of obesity. Focusing onnutrition policy in the broadest terms, it will
increasingly popular trend in this country andmay make it easier for people to overeat inad-vertently. A king size version of a chocolatebar can provide around 100 extra caloriesover the standard bar.To put this inperspective, just 50-100 calories each dayabove energy needs could lead to a weightgain of 5-10lb in one year. Some kingsize barsavailable in the UK provide around a fifth ofthe daily calorie needs of a ten year old child.
Equally important is the fact that peopleare also becoming less active in daily life.Themost recent surveys show that six in 10women and seven in 10 men do not do therecommended 30 minutes moderateintensity physical activity on five days a week.Similarly, four in 10 boys and six in 10 girls arenot meeting the recommended hour a day ofphysical activity for children.
Lower levels of activity in daily life are likelyto be key to the rise in obesity and due to arange of reasons - including greater use ofthe car for short journeys (walking andcycling have decreased since 1975), anincrease in sedentary occupations, lowersports participation and parental reluctanceto allow children to play outdoors. Conversely,sedentary activities, such as watching TV, areincreasingly popular. Indeed, the findings of aprospective study of nurses in the US suggestthat following a relatively active lifestyle(watching less than 10 hours of TV a weekand walking "briskly" for at least 30 minutes
Why has obesity increased? Without periods of increased energy (calorie)intake and/or reduced physical activity, indi-viduals will not gain weight, no matter whattheir genetic make up.The increase in over-weight and obesity across the world hasbeen too fast to be explained by geneticfactors alone and is most likely to be due tochanges in diet and in physical activity habits.
While dietary surveys in the UnitedKingdom seem to show a reduction in energyintake – an important and often unrecog-nised consideration is that our National FoodSurvey does not fully account for food eatenoutside the home – including for example,work lunches, snacks and fast food meals.Thenumber of meals and snacks eaten out hasincreased in recent years – as a nation, we ate675 million restaurant meals in 2000 (upalmost 13% since 1995) and, in 2001, we atearound 2 billion meals at "quick service"restaurants.
Meals and snacks eaten out tend to behigher in fat – with at least 40% of caloriescoming from fat in meals eaten outside thehome, compared with less than 37% in foodeaten at home. Calories from fat are particu-larly important. A high fat diet maypredispose to weight gain - by underminingthe normal mechanisms regulating energybalance and/or leading to passive overconsumption. Although the National FoodSurvey shows that average total fatconsumption has fallen in recent years,average total fat intakes remain above the35% recommended by the Committee onMedical Aspects of Food and Nutrition Policy(COMA) in 1994.
People are also snacking more.While theNational Diet and Nutrition Survey indicatesthat we are eating less cakes and biscuits,industry surveys show that sales of snacksand confectionery continue to increase,outstripping those in all other Europeancountries. People are also drinking moresugared drinks, which may contribute toexcess calorie intake. For example,consumption of carbonated drinks hasalmost doubled in the past decade.Youngadults now drink an average six cans eachweek, around half of which are non-`diet'types containing sugar.
Evidence from the United States alsosuggests that portion sizes are significantlylarger now than they were in the 1970s, espe-cially for high calorie snacks and fast foods.The supersizing of fast foods and snacks is an
Equally important is the fact thatpeople are also becoming lessactive in daily life.The mostrecent surveys show that six in10 women and seven in 10 mendo not do the recommended 30minutes moderate intensityphysical activity on five days aweek. Similarly, four in 10 boysand six in 10 girls are notmeeting the recommended houra day of physical activity forchildren.

HEALTH CHECK CMO ANNUAL REPORT 2002 43
set out a plan of action to address the rangeof factors that influence what we eat. It willlook at food supply, production and, prepa-ration, access to healthier choices andproviding information for consumers abouthealthier eating.
On-going initiatives have a role in obesityprevention, including the reform of theWelfare Food Scheme, action to promotebreastfeeding, various initiatives in schools toimprove the diets of children, and the 5 A DAYprogramme to increase intakes of fruit andvegetables. In addition, the NHS Plan makes acommitment to improve the overall balanceof the diet, including the amount of fat andsugar in food. I urge the food industry toconsider what it can do to ensure that thelevels of fat and sugar in products contributeto a healthier diet.
To ensure that there is a co-ordinated andstrategic approach to the planning anddelivery of sport and physical activity across adiverse range of sectors – such as transport,countryside management and townplanning – a Sport and Physical Activity Board(SPAB) has been established.The Board is tobe jointly led by the Department of Healthand Department of Culture, Media and Sport.It will oversee the co-ordination of action toincrease activity levels, physical education,school sport and club links programme -which will help fulfil the Prime Minister’scommitment to entitle all children to a
minimum of two hours a week of high qualityphysical education and school sport. Anotherkey project in the current Department ofHealth's programme of work is the LocalExercise Action Pilots (LEAP) which are jointlyfunded with Sport England and theCountryside Agency, and which will test theeffectiveness of Primary Care Trust led inter-ventions to increase access and levels ofphysical activity in communities based inNeighbourhood Renewal Areas. Activitiesrange from walking, cycling and swimminginitiatives to clinical based programmes thatare focusing on diabetes and weightmanagement.
The Government has recently set a chal-lenging target for 70% of the population tobe active by 2020.The target – at least 30
Obesity:defusing the health time bomb
minutes a day of a moderate activity, such asbrisk walking – will only be achieved byhelping people to build activity into theirdaily lives, in addition to encouraging partici-pation in sports.Therefore, addressingtransport to ensure that walking and cyclingcan be built in to daily life will be key.
Later this year I will be publishing a reportthat brings together the latest researchevidence on physical activity and health.Thisreport will inform local policy makers andhealth professionals to increase awareness ofthe strength of the evidence.
The NHS Priorities and Planning Frameworkfor 2003-2006 requires practice-basedcoronary heart disease registers andsystematic treatment regimes.This willinclude appropriate advice on diet, physical

44 HEALTH CHECK CMO ANNUAL REPORT 2002
Obesity is a growing challenge for Government as a whole – action acrossGovernment Departments must increase if we are to effectively tackle obesity.
The food industry – including manufacturers, retailers and caterers – is stronglyencouraged to address the added sugar, fat and salt content of foods, to ensure thatconsumers are able to make informed choices (for example,by providing clear infor-mation on product content – including those eaten at food outlets).
There is a case for adopting the precautionary principle for the marketing of foods tochildren. Industry should be asked to take a more responsible approach to thepromotion (especially to children) of foods high in fat,salt and added sugars andbalance this with the promotion of healthier options, including fruit and vegetables.
The leisure and sports industries – particularly those with high brand acceptance –should continue to market participation in exercise and sports as ‘cool’.
Local government should review the facilities for exercise provided in their areasaddressing the needs of all – e.g.sports,cycling to work,dancing,swimming.Policiesthat encourage active transport should be a priority.
Primary Care Trusts should work with partner organisations on exercise referral forhigh risk groups, including children (the new programme of Local Exercise ActionPilots will help with this).
Drug companies – such as those producing drug treatments for obesity - shouldhelp provide training for primary care professionals on effective ways of tacklingobesity and implementing the NICE guidance.
General Practitioners and Primary Care Trusts should take action to prevent andtackle obesity in their practice populations using effective interventions based onevidence.
Health professionals – including general practitioners,school nurses,practice nursesand health visitors - should identify early signs of obesity in children and offer inter-ventions at an early stage.
The Foods Standards Agency should examine options for reducing overweight andobesity through action to improve transparency in food labelling, improvedconsumer information on issues such as portion size and snacks,and alertconsumers to the risks of regular consumption of foods high in calories, fat andsugars.
Regional Government Offices should put together a `target obesity' programme fortheir regions, taking stock of the baseline prevalence of obesity.
To supplement data at a national level,Public Health Observatories should makeregular public reports tracking the prevalence of overweight and obesity in theirregions and identifying areas where progress is being made.
Action recommended +activity and smoking for patients withcoronary heart disease and those at high riskof coronary heart disease, including thosewho are obese. Extending the availability ofexercise referral schemes will be an importantcomponent of meeting this target. NationalInstitute for Clinical Excellence guidance ondrugs to tackle obesity, Orlistat andSibutramine, has added another valuableapproach to the options available to practi-tioners in tackling obesity.The National AuditOffice's report highlighted that the majorityof general practitioners and practice nursesbelieved that guidance on effective interven-tions in primary care to tackle obesityprevention and management would behelpful, and the intention of the NationalInstitute of Clinical Effectiveness to developsuch guidance is welcomed, as is evaluationby the Health Development Agency of theevidence base for the prevention andmanagement of obesity.
In the United States a range of fiscal andeconomic measures are being considered, aswell as health "warnings" on foods. I am notopposed to such an approach here.Regulating the promotion of foods throughschools and other approaches to discouragethe consumption of products high in fat andadded sugars are both worthy of consider-ation, including more radical fiscal options.The Food Standards Agency is currentlycarrying out research into the impact of foodadvertising on children’s diets.These findingswill be important in planning future measures.
Conclusions ■The growth of overweight and obesity in thepopulation of our country – particularlyamongst children – is a major concern. It is ahealth time bomb with the potential toexplode over the next three decades intothousands of extra cases of heart disease,certain cancers,arthritis,diabetes and manyother problems.Unless this time bomb isdefused the consequences for the popu-lation's health, the costs to the NHS and lossesto the economy will be disastrous.
No country has successfully tackled theproblem of obesity.With a co-ordinated andcomprehensive response from health andlocal authority services and acrossgovernment and with the co-operation of thefood,sports and leisure industries it is stillpossible to mitigate its impact on futuregenerations.

HEALTH CHECK CMO ANNUAL REPORT 2002 45
KEY WEB RESOURCES AND REFERENCES
National Audit Office.Tackling obesity inEngland. London:The Stationery Office, 2001.http://www.nao.gov.uk/pn/0001/0001220.htm
World Health Organisation. Obesity:preventing and managing the globalepidemic. Geneva:WHO, 2000.http://www.who.int/nut/publications.htm
Bajekal M, Primatesta P, Prior G, eds. HealthSurvey for England 2001: a survey carried outon behalf of the Department of Health.London:The Stationery Office, 2003.http://www.official-documents.co.uk/document/deps/doh/survey01/hse01.htm
Flegal et al. Prevalence and trend in obesityamong US adults, 1999-2000. JAMA 2002; 288:1723-1727.http://jama.ama-assn.org/cgi/content/abstract/288/14/1723
Erens B, Primatesta P, Prior G, eds. Healthsurvey for England: the health of minorityethnic groups ’99: a survey carried out onbehalf of the Department of Health. London:The Stationery Office, 2001.http://www.archive.official-documents.co.uk/document/doh/survey99/hse99.htm
US Surgeon General (2001). Call to action toprevent and decrease overweight andobesity.http://www.surgeongeneral.gov/topics/obesity/
Mokdad et al. Diabetes trends in the US: 1990-1998. Diabetes Care 2000; 23(9): 1278-83.http://care.diabetesjournals.org/cgi/content/abstract/23/9/1278
Drake A J et al.Type 2 diabetes in obese whitechildren. Arch Dis Child 2002; 86: 207-208.http://adc.bmjjournals.com/cgi/content/abstract/archdischild%3b86/3/207
World Health Organisation.The world healthreport: reducing risks, promoting health life.Geneva:World Health Organisation, 2002.http://www.who.int/whr/2002/en/
World Health Organisation. Diet, nutrition andthe prevention of chronic disease. Geneva:World Health Organisation, 2003.http://www.who.int/hpr/nutrition/ExpertConsultationGE.htm
International Obesity Taskforce and EuropeanAssociation for the Study of Obesity. Obesityin Europe: the case for action. InternationalObesity Taskforce, 2002.http://www.iotf.org/media/euobesity.pdf
National Institute for Clinical ExcellenceTechnology Appraisal Guidance No 22 –Guidance on the use of orlistat for thetreatment of obesity in adults (March 2001).http://www.nice.org.uk/article.asp?a=15724
National Institute for Clinical ExcellenceTechnology Appraisal Guidance No 31 –Guidance on the use of sibutramine for thetreatment of obesity in adults (October 2001).http://www.nice.org.uk/article.asp?a=23017
Department for Environment, Food and RuralAffairs. National food survey 2000: annualreport on food expenditure, consumptionand nutrient intakes. London:The StationeryOffice, 2001.http://www.defra.gov.uk/esg/Work_htm/publications/cf/nfs/current/nfs.htm
Prentice A,Jebb S.Obesity in Britain:Gluttony orSloth? BMJ 1995;311:437-439.http://bmj.com/cgi/content/full/311/7002/437
Committee on Medical Aspects of Food andNutrition Policy Nutritional Aspects ofCardiovascular Disease. London: HMSO, 1994.http://www.doh.gov.uk/coma/reports.htm
Henderson L et al. National diet and nutritionsurvey: adults aged 19 to 64 years (vol 1).London:The Stationery Office, 2002.http://www.foodstandards.gov.uk/news/pressreleases/nationaldiet
Nielson and Popkin. Patterns and trends infood portion sizes 1977-1998. JAMA 2003;289: 450-453.http://jama.ama-assn.org/cgi/content/abstract/289/4/450
Gregory, J. National diet and nutrition survey:young people aged 4 to 18 years. London:TheStationery Office, 2000.http://www.foodstandards.gov.uk/news/pressreleases/nationaldiet
Hu et al.Television watching and othersedentary behaviours in relation to risk ofobesity and type 2 diabetes mellitus inwomen. JAMA 2003; 289: 1785-1791.http://jama.ama-assn.org/cgi/content/abstract/289/14/1785
Wannamethee SG, Shaper AG. Alcohol, weightand weight gain in middle aged men. Am JClin Nutr 2003; 77: 1312-1317.http://www.ajcn.org/cgi/content/abstract/77/5/1312
WHO. Diet, Nutrition and the Prevention ofChronic Disease.Technical Report Series 916.Geneva:WHO, 2003.http://www.who.int/mediacentre/releases/2003/pr20/en/
Department of Health.The NHS Plan: A Planfor Investment, A Plan for Reform. London:TheStationery Office, 2000.http://www.doh.gov.uk/nhsplan/
Obesity:defusing the health time bomb

NTRATHECAL
A total of 23 incidents are known to have occurred around the worldin which the drug vincristine has been injected intrathecally(spinally) during the treatment of a patient.This drug is intended forintravenous (injected into a vein) use only. If injected intrathecallyby mistake it causes paralysis usually followed by death.This type ofmedical error was identified in my report ‘An organisation with amemory’ (www.doh.gov.uk/orgmemreport/) and was targeted forelimination as part of a drive to improve patient safety in the NHS.Progress has been made in putting in place action to reduce therisk of this specific class of error, but more still needs to be done.

Intrathecal chemotherapy
47
123 people worldwide (usually children or youngpeople) have been reported as paralysed or havingdied as a result of the maladministration ofvincristine intrathecally (spinally).The most recentBritish case was in Nottingham in 2001, andworldwide was in Spain in 1992.
2The true incidence of this medical error is unknownand the 23 cases only represent those which havebeen reported in medical journals or have becomepublic in other ways.
3Although rare, these incidents have catastrophiceffects for the patient, their family and the clinicalteam concerned.
4The circumstances of many incidents have beenvery similar and typically involve multiple failures ofprocedure, checking or decision-making.Thesefailures then create the conditions for a seriouserror to occur.
5So-called `systems failure’ as the cause of manyunsafe situations is well recognised in other sectors(eg. the airline industry) but until recently was notwell recognised in health care.
6Elimination of intrathecal error is one of a number oftargets set as part of a major NHS programme toimprove patient safety by learning from medicalerrors and strengthening systems to reduce futurerisks of health care.
7Action has been taken to achieve this target and moreis planned. Some local NHS organisations have beenslow in complying with national guidance.They needto be rigorous in implementing safer administrationof intrathecal chemotherapy.
CHEMOTHERAPYkeeping up the pressure for safe administration
Key points
HEALTH CHECK CMO ANNUAL REPORT 2002

HEALTH CHECK CMO ANNUAL REPORT 2002
Fatal event in Oviedo, SpainINTRATHECAL VINCRISTINE was inadvertently injected into a 12 year old girl with acute leukaemia. Her condition progressively deterio-rated with initial paralysis of both upper limbs and cranial nerves, proceeding to difficulty in swallowing and breathing, then paralysis of all four limbs, coma and death.
Source: Alcaraz A, Rey C, Concha A & Medina A. Intra-thecal vincristine: fatal myeloencephalopathy despite cerebrospinal fluid perfusion. Clinical Toxicology 2002; 40(5):557-561.
48
The NHS Patient Safety AgendaIn June 2000, I produced a report that estab-lished the way forward to ensure that theNHS learns from what goes wrong. Not onlydid ‘An organisation with a memory’drawattention to the scale of the problem ofpotentially avoidable events that result inunintended harm to patients, but it also set-out a number of proposals for developing aculture of openness, reporting and safetyconsciousness within NHS organisations.
Ensuring the safety of everyone whocomes into contact with health services isone of the most important challenges facinghealth care today, not just here butworldwide. In the United States of America,for example, medical error in hospitals is nowbelieved to be potentially the thirdcommonest cause of death. Perhaps as muchas a half of these adverse events are judgedto be avoidable. I promoted a resolution(WHA55.18) through the World HealthAssembly – adopted in May 2002(www.who.int/gb/EB_WHA/PDF/WHA55/ewha5518.pdf ) recognising theneed to promote patient safety as a funda-mental principle of all health systems.
These international developments areimportant for two reasons:● Firstly, they demonstrate that the problemswe face in this country are not unique to theNHS. Similar problems, of equal magnitude,and probably of similar causes with similarsolutions, are found in fee-for-service andinsurance based systems, every bit as muchas they are in the state funded NHS.
● Secondly, these data demonstrate thatthere is a huge potential to reduce sufferingand avoidable death if we pay greaterattention to safety and quality, if we learnfrom and act on our mistakes, and if we learnfrom other industries - such as the airlines -where safety is ‘mission critical’.
improvement became part of the routines ofevery clinical team and the centralcomponent of the culture of the hospital orprimary care service.The development ofclinical governance throughout the NHS isfacilitated by a National Clinical GovernanceSupport Team (www.cgsupport.org ), part ofthe NHS Modernisation Agency.
This NHS framework of quality (nationalstandards, local clinical governance) iscompleted by the process of inspection.Since 2000, this has been carried out by theCommission for Health Improvement (CHI).From 2004, subject to legislation, theinspection remit will broaden to includeprivate health care and will be undertaken bya Commission for Health Care Audit andInspection (CHAI).
Action specifically to prevent spinal injectionerrors needs to be seen within the broadercontext of the agenda to improve the safetyand quality of care for NHS patients.
In 1997, the government published itsWhite Paper,‘The New NHS, ModernDependable’, which set out to define andprovide the focus on quality.At a nationallevel, the National Service Frameworks (NSFs)and the National Institute for ClinicalExcellence (NICE) have helped to ensure thathealth care delivery is based on a clear set ofstandards.
At local level, all NHS organisations arerequired to fulfil a statutory duty of qualitywhich was set out in the Health Act 1999.This duty of quality is delivered by the estab-lishment in each local NHS organisation of asystem of clinical governance. In this wayquality assurance, patient safety and quality
Intrathecal vincristine errors haveoccurred in other countries:

49
An increasing body of evidence is alreadypointing to the fact that in the majority ofinstances, it is not bad or poorly performinghealth care professionals who are directlyresponsible for adverse events. Rather, thefault lies in the systems in place to supportthe delivery of safe, high quality health care.Health care professionals clearly need to betrained to be competent in the care ofpatients.They also need to practise veryconscientiously and be supported in doingso. However, if the risks to patients are to belessened and if the quality of care given topatients is to improve, within health careorganisations there need to be the skills torecognise, analyse and learn from errors.
In an organisation as complex as the NHS,things will sometimes go wrong and somepatients will suffer unintended harm.‘Anorganisation with a memory’concluded thatif the NHS was to successfully modernise itsapproach to learning from failure, four keyareas must be addressed:
● unified mechanisms for reporting andanalysis when things go wrong;
● a more open culture, in which errors orservice failures can be reported anddiscussed;
● mechanisms for ensuring that, wherelessons are identified, the necessary changesare put into practice;
● a much wider appreciation of the value ofthe system approach in preventing, analysingand learning from errors.
A National Patient Safety Agency (NPSA) hasbeen established (www.npsa.org.uk ). It hasalready begun collecting and analysing keyinformation from local organisations andfrom other sources - with the aim ofproviding relevant and timely feedback toorganisations and clinicians to help themimprove patient safety.The National PatientSafety Agency’s national reporting andlearning system for adverse events is under-going testing and development prior tobeing implemented across the NHS fromsummer 2003.
By collecting and analysing data onadverse events, the Agency will be able toidentify trends and patterns of avoidableadverse events, provide feedback to organisa-tions to enable them to change their workingpractices, help develop models of goodpractice and systems solutions at national
level, and also support ongoing educationand learning to promote patient safety.
The information received from the NationalPatient Safety Agency’s reporting system andfrom other information sources – such aslitigation and research – will inform the devel-opment of safety solutions to reduce boththe numbers of incidents that occur and theseriousness of the outcomes for patients.
Over time, the National Patient SafetyAgency will begin to give us a real under-standing of the scale of the problem – abaseline allowing us to understand the realextent and nature of adverse events, and ameans to act on that knowledge.
Improving patient safety requires changein many different areas, not least in theculture of organisations. Evidence shows thatif the culture is open and fair and people areencouraged to speak up about mistakes andnear misses, patient safety is improved aspeople are able to learn about what has gonewrong and are able to put things right.
SAFE ADMINISTRATION OF INTRATHECAL CHEMOTHERAPY –
NATIONAL GUIDANCE
‘AN ORGANISATION WITH A MEMORY’ PROPOSED A NUMBER OF
SPECIFIC TARGETS FOR ACTION (AGREED WITHIN ‘THE NHS PLAN’),
INCLUDING THE TARGET TO REDUCE TO ZERO THE NUMBER OF
DEATHS FROM MALADMINISTERED SPINAL INJECTIONS BY
THE END OF 2001.
Intrathecal chemotherapy
Subsequent reports in April 2001 – byProfessor Kent Woods on the prevention ofintrathecal medication errors(www.doh.gov.uk/ imeprevent/index.htm),and by Professor Brian Toft (www.doh.gov.uk/qmcinquiry/index.htm) who led the externalenquiry into the adverse event at Queen’sMedical Centre Nottingham which causedthe death of Wayne Jowett – highlighted thelarge number of separate factors which, incombination, can lead to this type of tragicmedical error.
These broadly fell into the areas of trainingand education, ward procedures andprotocols, and pharmacy procedures andprotocols. However, in preventing unsafepractices that lead to serious error, includingthe maladministration of chemotherapydrugs, there is a need to address broaderissues such as management accountability for
the systems and culture within organisations.Drawing on the learning from these
reports, the Department of Health issuednational guidance on the safe adminis-tration of intrathecal chemotherapy [HSC2001/022] on 6 November 2001.Thisrequired all NHS Trusts where intrathecalchemotherapy is administered to takeappropriate action to ensure the intro-duction of safe practice.The guidance issuedby the Department of Health was developedby an expert panel which drew on thelearning from the Toft and Woods reports.The recommendations by Brian Toft wereincorporated into the guidance exceptwhere the Panel was satisfied that an alter-native recommendation would furtherenhance safety.The Department of Healthconsulted on the draft guidance before itwas issued.
HEALTH CHECK CMO ANNUAL REPORT 2002

50 HEALTH CHECK CMO ANNUAL REPORT 2002

HEALTH CHECK CMO ANNUAL REPORT 2002 51
NHS organisations completed a self-assessment exercise in early 2003.Thisdemonstrated that a number of NHS Trustswere not completely compliant with thenational guidance and that further action wasrequired to ensure that services are beingdelivered safely.
Follow-up independent peer review visitsto all relevant NHS Trusts have now beencompleted.The aim of these visits was tovalidate NHS Trusts' original self-assessments,identify areas that fell below the acceptedlevel and make recommendations to addressthese, so that NHS Trusts can be certain theyare providing safe intrathecal chemotherapyservices to patients.
The visits have covered a range of issuesincluding: the clinical environment; formaland informal staff interviews; checks ofmedical notes and charts. A report of thenational position in May 2003 showed lessthan full compliance with the guidance andurgent action is being taken with thehospitals concerned.
I have been disturbed by the time taken toimplement this clear national guidance.Following this exercise, we aim to engagewith front line staff and managers to learnlessons and find out what more can be doneto support the NHS in ensuring that this andfuture safety guidance can be quickly andsuccessfully implemented.
A training pack and video will be availablein 2003 to support local training programmesand locally tailored protocols and processes.
Further work to help preventintrathecal chemotherapy errorsThere are a number of further steps that arebeing taken to prevent these and other errorsoccurring across the NHS.
A design solution could make it physicallyimpossible to accidentally inject vincristineand other drugs using the wrong route.Advocated by many people in the past, thisseemingly obvious solution is not as straight-forward as it might at first seem. Currently,standard medical connectors (Luerconnectors) are used in a wide variety ofsystems including the administration of intra-venous, spinal and other injections as well asdelivering fluids and gases in other settings.Their wide use in health care allows crossconnection between these different medicalsystems and this has been a contributingfactor in intrathecal chemotherapy errors.Weneed to be certain that any potential new
design solution is rigorously tested and,crucially, that by introducing new equipmentto prevent one specific type of error, we donot, in turn, introduce new unforeseen risks topatients.
The Department of Health is working withmanufacturers to identify a design solution.To identify options, an announcement wasplaced in the Official Journal of EuropeanCommunities (OJEC) seeking devices forspinal procedures which must be fitted withconnectors which are not compatible withstandard medical connectors.The announce-ment (OJEC Reference (02/S 66-51750/EN)sought expressions of interest for devicesincluding syringes, drawing up needles, spinalneedles, microbiological filters and epiduralcatheters.This is the first step in a programmeto identify and, if possible, introduce alter-native equipment as a further measure to
reduce risk of harm to patients through mis-connection errors.
Current connector systems are well estab-lished and in regular daily use across the NHS– consequently, identifying and introducingpossible new equipment and changingpractice will inevitably take time.
My report ‘An organisation with a memory’also highlighted the risks of medication errorsmore generally, in addition to the veryspecific risk with intrathecal chemotherapy.A prescribed medicine is the most frequenttreatment provided for patients in the NHS.General practitioners in England issue almost600 million prescriptions every year, and thereare an estimated 200 million prescriptions inhospitals. Standards of prescribing in thiscountry are high and the vast majority ofdrug treatment is provided safely. However,mistakes do occur - they can arise in the
Intrathecal chemotherapy

HEALTH CHECK CMO ANNUAL REPORT 200252
and took steps to ensure that companiescomplied with labelling changes.
Since then, the Medicines Control Agencyhas been working with the National PatientSafety Agency, the pharmaceutical industry,health care professionals and lay interests todevelop best practice guidance on medicineslabelling and packaging to improve patientsafety.
The Best Practice Guidance (www.mca.gov.uk/), published on 3 March 2003 andtaking effect immediately, set out the factorsto be considered when designing medicineslabelling.These include layout, size of text andcolours used. In addition, although 15 differentpieces of information are legally required toappear on a label, users need rapid access toonly five key pieces of critical information:● the name of the medicine● strength● route of administration● dose ● any warnings.
The guidance advises that these should bebrought together on the pack for ease of access.
prescribing, dispensing or administration ofmedicines, and the consequences can beserious.
The NHS is committed to making drugtreatment as safe as possible. I have thereforeasked the Chief Pharmaceutical Officer, todraw up a report providing guidance forhealth professionals and NHS organisations,drawing on experience and good practicewithin the NHS and worldwide.
Improving the labelling and packaging ofdrugs can be a further means to reducing therisks of these and other medication errors.Weknow that problems with labelling have alsobeen associated with a high percentage oferrors and that there is the potential forimproving the layout of medicines labellingto aid clarity.This would assist health profes-sionals and patients/carers to select thecorrect medicine and use it safely, therebyhelping to minimise medication errors.
Following the publication of ‘An organi-sation with a memory’,The Medicines ControlAgency (MCA, now called the Medicines andHealthcare products Regulatory Agency)reviewed the labelling of all vinca alkaloids
Conclusions ■Improving patient safety is now a majorgovernment priority. Indeed, ensuring thesafety of patients is becoming one of themost important challenges facing health caretoday, not just here but worldwide.
It is an issue that, properly addressed, willreap tremendous benefits both in reductionin unintended harm to patients and areduction in unnecessary financial costs asso-ciated with such harm. Improvements inpatient safety will contribute significantly toimproving the quality of care for NHSpatients. Reduction in errors will also free upresources at present used to cope with theconsequences of those errors.
Those specific errors involvingchemotherapy drugs, thankfully, appear to beuncommon, both here and internationally.However, when they do happen, the conse-quences can be devastating for everyoneinvolved: for patients and their loved ones, aswell as for staff.
Moreover, this is an area where we alreadyhave much of the learning we need to ensuresimilar cases are not repeated in the future –we have been able to set clear guidance tothe NHS to help achieve this goal.
However, we need to continue to work on anumber of fronts. In particular, NHS organisa-tions need to assure themselves that they aredoing all they can to deliver safe care forthose receiving spinal chemotherapy drugs.
The clear national guidance must be fullyimplemented, and the time being taken toachieve full compliance is a source ofconcern.
15 DIFFERENT PIECES OFINFORMATION ARE LEGALLYREQUIRED TO APPEAR ON ALABEL,USERS NEED RAPID ACCESSTO ONLY FIVE KEY PIECES OFCRITICAL INFORMATION:1.THE NAME OF THE MEDICINE2.STRENGTH3.ROUTE OF ADMINISTRATION4.DOSE 5.ANY WARNINGS

Intrathecal chemotherapy
HEALTH CHECK CMO ANNUAL REPORT 2002 53
KEY WEB RESOURCES AND REFERENCES
Health Service Circular (HSC 2001/022) on theSafe Administration of IntrathecalChemotherapyhttp://www.doh.gov.uk/intrathecalchemotherapy/index.htm
The Prevention of Intrathecal Medication Errors http://www.doh.gov.uk/imeprevent/index.htm
External Inquiry into the adverse incident atQueen's Medical Centre, Nottingham, 4thJanuary 2001http://www.doh.gov.uk/qmcinquiry/index.htm
National Patient Safety Agencyhttp://www.npsa.org.uk
An organisation with a memory: report of anexpert group on learning from adverse eventsin the NHShttp://www.doh.gov.uk/orgmemreport
Building a safer NHS for patientshttp://www.doh.gov.uk/buildsafenhs
The NHS Planhttp://www.nhs.uk/nationalplan
The Best Practice Guidance on the labellingand packaging of medicineshttp://www.mca.gov.uk
Action recommended +NHS organisations must ensure that they are complying in fullwith Health Service Circular 2001/022 on the Safe Administrationof Intrathecal Chemotherapy.
NHS Trust Chief Executives need to ensure that intrathecalchemotherapy and other patient safety issues are recognised asclear clinical governance issues and are addressed in quarterlyrisk management reports.
NHS Chief Executives must provide leadership in promoting asafety culture within their organisations, where all staff areactively encouraged to report and learn from mistakes and nearmisses, to avoid errors being repeated.
NHS organisations need to ensure that they provide adequateand appropriate induction and formal training for all staffentering a department where intrathecal chemotherapy isadministered.
Building on the work to develop a design solution to preventcross-connection errors and on safer labelling and packaging ofmedicines, the Department of Health and the NHS must continueto work with the pharmaceutical and medical devices industriesto jointly promote better and safer products.
The NHS should review the criteria it uses to inform itspurchasing decisions - as purchasing based on consistent, well-founded criteria could, in turn, help focus manufacturers andsuppliers on delivering improved patient safety.

55
GETTING TO GRIPSO
ver a hundred thousand doctors practise in the NationalHealth Service (NHS). Standards of education and trainingof doctors in this country are very high and much of thecare provided by them to patients is of superb quality. As
with any large workforce it is inevitable that problems will occur with aminority. When problems occur with a doctor's practice they can haveserious consequences for the individual patient, their family and forother members of the clinical team in the service concerned. Overmost of its history, the NHS has found great difficulty in addressingsuch problems – albeit involving a small minority of the medical work-force – in a way which gives priority to protecting patients whilst at thesame time recognising that disciplinary solutions are not always thefairest and most appropriate way of dealing with a doctor who hasgenuine problems in their practice. In the last few years, an entirelynew approach has been established.Given that this problem has proved intractable over a period of 50years, it is not surprising that making progress in recent years has notbeen easy. It is now clear that significant inroads are being made,creating a new climate in which poor clinical performance can be recog-nised earlier and dealt with in a more modern and acceptable way.
WITH POOR MEDICAL PERFORMANCE
HEALTH CHECK CMO ANNUAL REPORT 2002

HEALTH CHECK CMO ANNUAL REPORT 200256
1 The vast majority of NHS doctors practise to a highstandard, the poor performance of a minority hasgiven rise to serious public concern.
2 The NHS has in the past had great difficulty ineffectively addressing such problems, partlybecause of inflexible, legalistic and dauntingstatutory procedures.
3 A new approach was agreed in the year 2000 basedon early identification of problems and rapidobjective assessment of the doctor concerned by a National Clinical Assessment Authority.
4 During its first 21 months the National ClinicalAssessment Authority has taken 446 referrals,predominantly from the older age groups, four infive being male doctors and with the highestnumber in the surgical specialties.
5 The National Clinical Assessment Authority hasbeen consulted in 36 cases where NHS Trusts wereproposing suspension and in 30 cases the Authoritywas able to offer alternative approaches.
6 The performance problems amongst these referralswere mainly multifactorial: four in five were acapability issue combined with ill-health ordysfunctional conduct, behavioural problemsfeatured in half the cases; one in three concernedclinical capability alone.
7 The proposal to rescind the old NHS procedureswas intended to give full force to the new approach(including the National Clinical AssessmentAuthority role) but this has not yet happenedbecause of the consultant contract rejection.
8 A further national initiative is in train to try toreduce the number of long suspensions (whichincludes a hidden element of doctors absent fromwork on special leave) but there are early signs of areduction in numbers as a result of the work of theNational Clinical Assessment Authority and theDepartment of Health.
9 More NHS Trusts and Primary Care Trusts need touse the National Clinical Assessment Authorityroute to resolving problems of poor clinicalperformance.
10 Further attention also needs to be given to howbest to help sick doctors, given that ill-health is stilla major contributor to impaired performance.
Key points

HEALTH CHECK CMO ANNUAL REPORT 2002 57
The issue of the poorly performing doctor –someone whose competence, conduct orbehaviour poses a potential risk to patientsafety or to the effective running of a clinicalteam – was a subject seldom openlydiscussed during the first four decades or soof the National Health Service’s existence.
Cases of serious professional misconductwere dealt with by the General MedicalCouncil, but these were examples of cases atthe extreme end of the spectrum ofmisconduct.The National Health Service’sown procedures for dealing with poorperformance remained more or lessunchanged for thirty years from the early1960s.They were revamped in the early 1990sbut the core principles and even much of thedetail remained intact.The procedures thenin place were firmly disciplinary in emphasis,were strongly underpinned legally andoffered very little flexibility for addressing thevaried circumstances in which poor practi-tioner performance could manifest itself in amodern medical context. Local managersfound the legal environment daunting, andthe adversarial, court-like procedures inwhich serious cases were dealt with wasextremely intimidating for witnesses – bothmanagerial and medical. As a result, there islittle doubt that poor practice in the past wastolerated to a much greater extent than itshould have been.
There are other more complex reasons whythe question of the poorly performing practi-tioner has not been well dealt with tradi-tionally. In the relatively small social worldwhich comprises a hospital or a generalpractice there are few situations thatgenerate greater anxiety, tension or uneasethan that of a doctor whose conduct orcompetence is giving rise to concern.The issue poses fundamental dilemmas forthose involved – other doctors, managers,nurses, junior staff: how to balance the safetyof patients against the support for acolleague; how to maintain the cohesion of aclinical team when one member has lost theconfidence of the others; how to take thematter further when to do so might be seenas disloyal or vindictive towards someone indifficulties.
Public concern about poorlyperforming doctorsIt was against this backdrop that the wholequestion of poorly performing doctorsbecame the subject of major public contro-versy during the 1990s. A number of highprofile cases hit the headlines, such as that ofthe gynaecologist Dr Rodney Ledward whosepoor standards of clinical care led to himbeing struck off the Medical Register by theGeneral Medical Council.Whilst the Ledwardcase became national news there wereothers which did not have such a high profilebut nevertheless gave rise to similarconcerns.
Such service failures caused a great deal ofpublic unease.There is little doubt that theywere not common in relation to the generallyhigh standard of NHS provision. Nevertheless,they began to give the impression that theNHS could not stop history from repeatingitself. And what added to this unease was the
recognition that, while the precise circum-stances of these ‘problem doctor’casesdiffered, common features were emerging.Investigations or inquiries would often showthat concerns about such a doctor hadexisted over a long period of time but hadnot been acted upon, and the organisationalculture of the health care organisationswhere such problems arose was oftendysfunctional with cliques and tensionsbetween particular groups of staff, andbetween managers and clinicians.What wasof particular concern to the public was theidea, rightly or wrongly, that the safety ofpatients may have had a lower priority andthat risks were allowed to prevail because ofan unwillingness or inability to tackle aproblem, however complex.
The watershed in public and professionalattitudes towards serious failures in the stan-dards of health care was undoubtedlyreached with the events which took place in
Poor medical performance

58 HEALTH CHECK CMO ANNUAL REPORT 2002
The dawn of clinical governance: newframework for quality and safetyBy the late 1990s, the climate had begun tochange as a result of the Government, themedical profession and the NHS workingtogether to put a philosophy of qualityassurance, quality improvement and patientsafety at the heart of all local health services.Coupled with this was a determination thatmajor attention should be given toprotecting patients against poor standards ofcare whether arising from: dysfunctionalservices; weak, unsafe systems; or, poor practi-tioner performance.
As a result of this, a statutory duty of qualitywas placed on local NHS organisations.Theywere required to implement programmes ofclinical governance: to ensure that in everylocal NHS service there is established theleadership, the systems and the infrastructureto ensure that quality assurance, qualityimprovement and patient safety are part ofthe everyday routines of every clinical team. Anational clinical governance developmentteam (www.cgsupport.org/) has undertakena major programme of change to achieve thisaim.Clearer national quality standards are now
them with opiates, and suspected of killingvery many more – fuelled yet further thegrowing climate of public concern.There wasa general acceptance that individuals withsuch criminal intent arise very rarely in anyprofession, but there was alarm at how somany killings could have gone undetectedover such a long period of time.
Public attitudes and media climatechangingThis small group of tragic cases fuelled aperception of a NHS in the last two decadesof the 20th century which was dogged by‘medical scandals’ and an inability to identifyproblems and act quickly where there wereserious risks to patient safety.
During this time, incidents and eventswithin local health services became public ina way that would not have been conceivablein the early years of the NHS.Traditionaldeferential attitudes towards doctors andothers in positions of authority werechanging as British society became moreconsumer-orientated.This found its voicemost obviously in the way that the mediachallenged health care providers which hadbeen responsible for incidents involvingpoor standards of care, especially wherepatients had been harmed or died. Manysuch events in the past would not have seenthe light of day at all or, if they did, wouldhave been explained away in general termsand as quickly forgotten.
In the media hothouse of the late 20thcentury, and in the culture of investigativejournalism, patients’deaths were no longermishaps or unfortunate accidents.They werescandals in which, though the plight of thevictim was highlighted, as much emphasiswas placed on identifying those perceived asresponsible and pinning blame and account-ability firmly on them. One centrallyimportant consequence of this shift was tocreate a climate which made it much moredifficult to draw a distinction between indi-vidual failures, system failures and genuineuntoward outcomes which were not theresult of failure on anyone’s part.
In essence therefore, a welcome shift awayfrom the traditional clinical cultures wasbringing with it a media driven approach toclinical accountability which could quicklylead to a highly defensive approach topractice and could stifle the open and fairculture which good clinical governanceshould be founded on.
the Bristol children’s heart surgery serviceduring the late 1980s and early 1990s. Bristolappeared to be a statistical outlier formortality after surgery, particularly in relationto one type of operative procedure. Despiteconcerns within the hospital, attempts toaddress and resolve the problems of clinicalperformance were inadequate. It was left to a‘whistleblower’, a medical colleague, to bringthe matter to external attention. At one pointthe surgeons were asked not to proceed witha heart operation on a particular child, butjudged the risks acceptable and proceeded,only for the child to die post-operatively.
What led to particular outrage, when theseevents became public through disciplinaryhearings and media reports, was the extent towhich clinical decisions were being made onbehalf of parents rather than with them. Amajor public enquiry into the Bristol affairdrew attention to a ‘club culture’within thehospital, whereby some ‘belonged’and otherswere excluded, which was detrimental tohigh quality care.
A much more sinister case – that of HaroldShipman, the general practitioner in Hyde,Greater Manchester, convicted of murdering15 elderly patients by deliberately killing
THIS SMALL GROUP OFTRAGIC CASES FUELLEDA PERCEPTION OF ANHS IN THE LAST TWODECADES OF THE 20THCENTURY WHICH WASDOGGED BY ‘MEDICALSCANDALS’AND ANINABILITY TO IDENTIFYPROBLEMS AND ACTQUICKLY WHERE THEREWERE SERIOUS RISKSTO PATIENT SAFETY.

HEALTH CHECK CMO ANNUAL REPORT 2002 59
established set by the Medical Royal Colleges,the General Medical Council and the NationalHealth Service (through National ServiceFrameworks and the work of the NationalInstitute for Clinical Excellence).
A Commission for Health Improvementestablished in April 2000 undertakes a regularseries of independent inspections of theadequacy of clinical governance arrangementsin every NHS provider of service and makespublic its reports on the extent to which localquality standards are being met.From 2004,subject to legislation,the inspection remit willbroaden to include private health care and willbe undertaken by a Commission for HealthCare Audit and Inspection (CHAI).
A major initiative on patient safety waslaunched following a report which I producedin 2000 called ‘An Organisation with a Memory’(www.doh.gov.uk/orgmemreport/).This specif-ically sought to address the growing uncer-tainty,described earlier,between individualfailures,system failures and genuine untowardoutcomes without concomitant failure,and topromote an approach based on careful analysisof the root causes of medical errors leading tomedical accidents.
New policies to improve handling ofpoor doctor performanceThe strand of patient safety which deals withpoor practitioner performance was specificallyaddressed in policy proposals which I made ina consultation document ‘Supporting Doctors,Protecting Patients’(www.doh.gov.uk/cmoconsult.htm) and subse-quently accepted by the Government forimplementation as part of the NHS Plan.Thesepolicies entirely recast the approach to dealingwith poor clinical performance in the NHS.Theyplace an emphasis on prevention and earlyrecognition of problems.This has two advan-tages compared to the old way of doing things.Firstly,patients are not placed at unnecessary orprolonged risk of harm from the poorlyperforming practitioner.Secondly, they createthe opportunity for the doctor to be helpedand rehabilitated where possible.Under the oldNational Health Service procedures everyproblem had to be dealt with as a disciplinaryproblem.Under the new arrangements this willbe transformed so that problems in a doctor’spractice are picked up much earlier,objectivelyassessed and in the majority of cases a rehabili-tative approach can be taken.
Information on the size of the problem ofpoor medical performance is limited.The onlypublished study – based on my own expe-rience in the North East of England showed afigure of 6% of doctors with serious problemsin a hospital workforce.The true ‘epidemi-ology’of poor clinical performance across awhole health care system is still unclear, butanecdotal evidence based on discussionswith other colleagues around the worldsuggest that a figure of 5-6% is fairlyconsistent.
It is not surprising that any workforce ofwhatever kind should contain a smallproportion of individuals whose performanceis poor enough to give rise to concern.Whatis surprising and lies at the heart of the diffi-culty we have faced in the last decade isperhaps that medicine was somehowbelieved to be unique.The existence of realproblems was in effect denied.The strategiesto tackle poor performance effectively werenever developed.The new approachacknowledges that in every large workforcesome serious problems are inevitable. It isessential therefore to put in place systems torecognise them early and deal with them so
Poor medical performance
NEW POLICIES TO IMPROVEHANDLING OF POOR DOCTORPERFORMANCE

60 HEALTH CHECK CMO ANNUAL REPORT 2002
advice; in 30 of these, the National ClinicalAssessment Authority was able to advisealternative approaches.
The National Clinical Assessment Authorityprovides a wide-ranging service to help NHSbodies and doctors themselves addressperformance problems. It can offer generaladvice or more intensive support in resolvinga perceived problem, and where necessarywill undertake full performance assessments.
Advice from the National ClinicalAssessment Authority is provided by a teamof casework managers, advisers and seniorofficers of the Authority.The team of 16advisers forms the core of the advice service.This group comprises senior clinicians andmanagers experienced in managing doctors’performance issues.They are located aroundthe country and cover a set number ofStrategic Health Authority areas.They liaisedirectly with the advice-seeking body, byphone or on-site and advise on the localmanagement of a case of possible poorperformance.The National ClinicalAssessment Authority also assists in identi-fying, and where necessary building, appro-priate local performance procedures with theaim of achieving resolution of concernsraised at an even earlier stage of the genesisof a problem.
If local resolution of concerns cannot beachieved, the National Clinical AssessmentAuthority can undertake a thoroughassessment of the doctor’s performance to:● clarify areas of concern● identify the cause of the poorperformance● make recommendations about how toresolve the problems identified.
maintain their registration with the GeneralMedical Council.
The National Clinical AssessmentAuthority is establishedThe Department of Health has worked closelywith the new National Clinical AssessmentAuthority since it was established with itsprincipal remit to promote excellent clinicalperformance and to support NHS personnelin dealing with under-performing doctors.When serious concerns arise about theperformance of a doctor, their employer orcontracting organisation (in the case of mostgeneral practitioners) is expected to seekadvice from the National Clinical AssessmentAuthority on how to address the problem.
There is no general requirement that theNational Clinical Assessment Authority isconsulted on all cases where there areconcerns. However, where suspension of adoctor is being considered, I have formallyrecommended to all NHS Trusts and PrimaryCare Trusts that the National ClinicalAssessment Authority should be consultedfirst, where possible.This addresses directlyone of the major problems identified with themanagement of perceived under-performance – that this frequently led toinappropriate use of suspension – eitherusing it when other action could have beentaken or allowing a suspension to persistlonger than warranted.
Early evidence from the National ClinicalAssessment Authority’s work indicatessuccess in this area.The Authority reviewed aseries of 36 cases where NHS Trusts wereproposing suspension and approached theNational Clinical Assessment Authority for
that risks to patients are minimised, and sothat doctors in difficulty can he helped andsupported.
Problems in a doctor’s practice can manifestthemselves in many different ways. Ill-health isimportant to consider as a cause even whenthe problem presents with unsatisfactoryconduct or doubts about competence.Asidefrom ill-health, there are many other types andcauses of poor performance.Unreasonablebehaviour can become apparent in rudenessor aggression towards colleagues, other staffor patients or in the failure to fulfil clinicalduties such as on-call commitments, clinics orteaching sessions.A doctor’s clinicaljudgement may be poor and this can lead tobad clinical decisions in relation to the investi-gation, diagnosis or treatment of patients.Sometimes a doctor’s technical skills may bebelow the standard required to deliver safe,effective care.And finally, the doctor may findthat his or her working environment does notprovide him or her either with the resourcesor the support which enables him or her towork effectively.Central to all of this is the factthat these causes of poor performance areclosely interwoven and can affect each other.For example, where a doctor feels that his orher clinical skills have dropped below par, hisor her health may suffer because of the stressthis brings with it.
Two of the key proposals in the report‘Supporting Doctors, Protecting Patients’werethat every NHS doctor should undergo anannual appraisal and that a specialist body, theNational Clinical Assessment Authority, shouldbe established to support NHS employerswhen serious concerns arose about an NHSdoctor’s performance.
Appraisal is one of the cornerstones ofprofessional development for all staff at locallevel.All staff, whether doctors or any othergroup, now have a responsibility to take partin appraisal throughout their working lives inthe NHS. Its core principles are built on form-ative approaches to professional devel-opment as the most powerful methods ofmaintaining excellence in practice and inpreventing performance problems occurring.It will provide one of the most powerful toolsfor identifying any potential problem andenabling resolution before the problembecomes established. In addition to its role ina doctor’s day to day work in the NHS,appraisal will also form one of the centralelements of the new arrangements for revali-dation which all doctors will undertake to
THE NATIONAL CLINICAL ASSESSMENTAUTHORITY CAN UNDERTAKE A THOROUGHASSESSMENT OF THE DOCTOR’SPERFORMANCE TO CLARIFY AREAS OFCONCERN IDENTIFY THE CAUSE OF THEPOOR PERFORMANCE MAKERECOMMENDATIONS ABOUT HOW TORESOLVE THE PROBLEMS IDENTIFIED
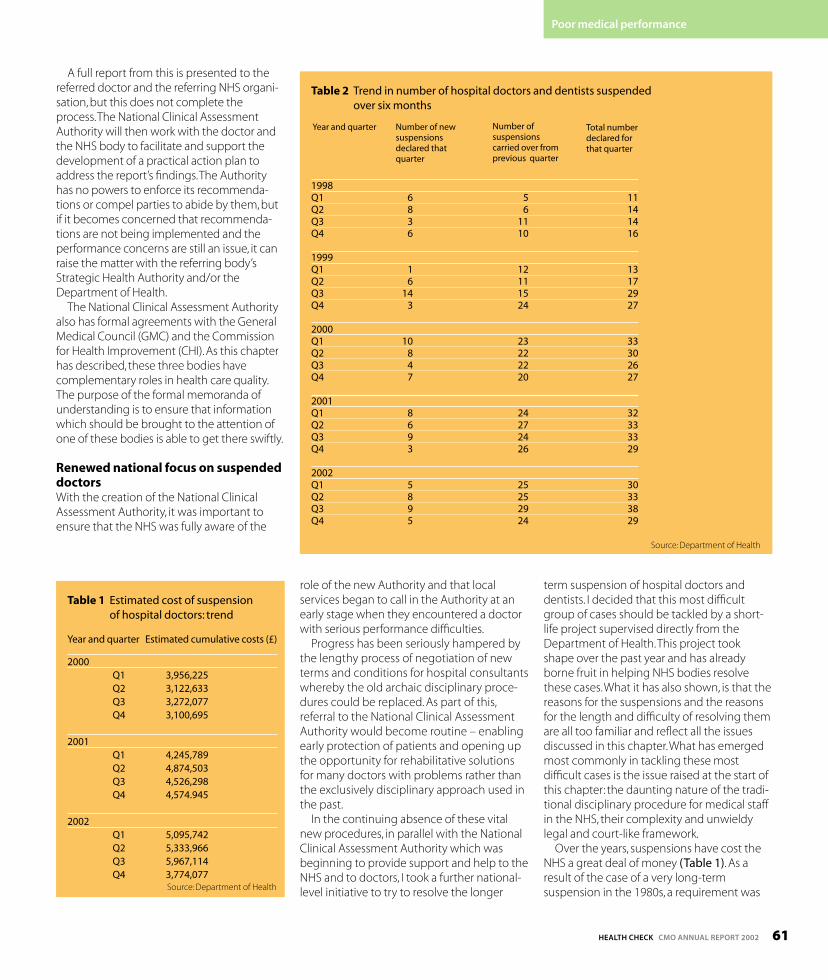
HEALTH CHECK CMO ANNUAL REPORT 2002 61
A full report from this is presented to thereferred doctor and the referring NHS organi-sation, but this does not complete theprocess.The National Clinical AssessmentAuthority will then work with the doctor andthe NHS body to facilitate and support thedevelopment of a practical action plan toaddress the report’s findings.The Authorityhas no powers to enforce its recommenda-tions or compel parties to abide by them, butif it becomes concerned that recommenda-tions are not being implemented and theperformance concerns are still an issue, it canraise the matter with the referring body’sStrategic Health Authority and/or theDepartment of Health.
The National Clinical Assessment Authorityalso has formal agreements with the GeneralMedical Council (GMC) and the Commissionfor Health Improvement (CHI).As this chapterhas described, these three bodies havecomplementary roles in health care quality.The purpose of the formal memoranda ofunderstanding is to ensure that informationwhich should be brought to the attention ofone of these bodies is able to get there swiftly.
Renewed national focus on suspendeddoctorsWith the creation of the National ClinicalAssessment Authority, it was important toensure that the NHS was fully aware of the
role of the new Authority and that localservices began to call in the Authority at anearly stage when they encountered a doctorwith serious performance difficulties.
Progress has been seriously hampered bythe lengthy process of negotiation of newterms and conditions for hospital consultantswhereby the old archaic disciplinary proce-dures could be replaced. As part of this,referral to the National Clinical AssessmentAuthority would become routine – enablingearly protection of patients and opening upthe opportunity for rehabilitative solutionsfor many doctors with problems rather thanthe exclusively disciplinary approach used inthe past.
In the continuing absence of these vitalnew procedures, in parallel with the NationalClinical Assessment Authority which wasbeginning to provide support and help to theNHS and to doctors, I took a further national-level initiative to try to resolve the longer
term suspension of hospital doctors anddentists. I decided that this most difficultgroup of cases should be tackled by a short-life project supervised directly from theDepartment of Health.This project tookshape over the past year and has alreadyborne fruit in helping NHS bodies resolvethese cases.What it has also shown, is that thereasons for the suspensions and the reasonsfor the length and difficulty of resolving themare all too familiar and reflect all the issuesdiscussed in this chapter.What has emergedmost commonly in tackling these mostdifficult cases is the issue raised at the start ofthis chapter: the daunting nature of the tradi-tional disciplinary procedure for medical staffin the NHS, their complexity and unwieldylegal and court-like framework.
Over the years, suspensions have cost theNHS a great deal of money (Table 1). As aresult of the case of a very long-termsuspension in the 1980s, a requirement was
Poor medical performance
Table 1 Estimated cost of suspension of hospital doctors: trend
Year and quarter Estimated cumulative costs (£)
2000Q1 3,956,225Q2 3,122,633Q3 3,272,077Q4 3,100,695
2001Q1 4,245,789Q2 4,874,503Q3 4,526,298Q4 4,574.945
2002Q1 5,095,742Q2 5,333,966Q3 5,967,114Q4 3,774,077
Source: Department of Health
Table 2 Trend in number of hospital doctors and dentists suspended over six months
1998Q1 6 5 11Q2 8 6 14Q3 3 11 14Q4 6 10 16
1999Q1 1 12 13Q2 6 11 17Q3 14 15 29Q4 3 24 27
2000Q1 10 23 33Q2 8 22 30Q3 4 22 26Q4 7 20 27
2001Q1 8 24 32Q2 6 27 33Q3 9 24 33Q4 3 26 29
2002Q1 5 25 30Q2 8 25 33Q3 9 29 38Q4 5 24 29
Source: Department of Health
Total numberdeclared forthat quarter
Number ofsuspensionscarried over fromprevious quarter
Number of newsuspensionsdeclared thatquarter
Year and quarter

62 HEALTH CHECK CMO ANNUAL REPORT 2002
Clinical Assessment Authority was set up.Figure 2 looks at age and shows that
referred doctors are generally established intheir careers, though hospital and communityreferrals tend to be younger than generalpractitioners. One overall aim is to see moreproblems being identified earlier, so thatinvestment in further training to rebuild thedoctor’s career is at its most effective.
Four in every five referrals are men, whoaccount for only about two thirds of theworkforce. But before concluding thatwomen outperform men, we should
of a case where suspension has beenconsidered, working closely with the NHSbody on the handling of a complex case, orproviding a thorough assessment of thedoctor’s performance and enabling a prac-tical approach to resolution.
As NHS organisations become more awareof the National Clinical AssessmentAuthority’s work, its caseload is graduallyrising.To some extent, of course, this mayreflect the varying abilities of local NHSorganisations to recognise problems as wellas the real size of the under-performanceproblem. But the National ClinicalAssessment Authority is still in a uniqueposition to pass on the lessons learnt from itscasework activity.
The Authority is now getting about onenew case a day, a third from general practiceand two thirds from hospital and communitycare, closely reflecting the NHS workforce’scomposition. Primary Care Trusts are stilldeveloping their new performancemanagement role so the number of casescoming to the National Clinical AssessmentAuthority from general practice may increasewith time. But the broad message is clear:performance problems occur right across themedical profession, regardless of gender, age,country of training, ethnicity.
Figure 1 shows how referrals to theNational Clinical Assessment Authority havebuilt up over its first 21 months.These aresingle doctor cases, and exclude referralsabout dysfunctional teams and practices orinquiries about performance systems.Thebalance between primary and secondarycare has changed little since the National
placed on NHS bodies to notify theDepartment of Health of any suspensionlasting longer than six months. Recent expe-rience has shown that there has been a rela-tively constant number of cases - about 30 –with a similarly constant turnover of cases –about one third each quarter (Table 2). Sincethe National Clinical Assessment Authoritystarted work, the trend does appear to bedownwards as judged by the last quarter of2002.The commonest specialties in whichsuspensions were made were surgical andmental health (Table 3).
The number of declared suspensionspotentially masks a much less clear numberof cases of doctors on ad hoc or unstructuredleave which has the same purpose assuspension but which lies outside normalemployer protocols – often colloquially called‘gardening leave’.This group of poorlyperforming doctors is largely hidden fromview. So I made a request of NHS bodies fordeclarations.This revealed a similar figure tothose cases on formal suspension (Table 4).
The further national initiative to reduce thenumber of suspensions of doctors has beentaken forward in parallel with the creationand development of the National ClinicalAssessment Authority.What has been veryencouraging is the close collaboration whichhas developed with the National ClinicalAssessment Authority and local NHS bodies.
The National Clinical AssessmentAuthority making an impactThe National Clinical Assessment Authority’swork has had an early and sustained impact,whether advising on the early management
Table 4 Number and clinical specialty ofhospital doctors on ‘special leave’but notformally suspended: Spring, 2002.
Specialty group Number of doctors
Surgical 15
Anaesthetics 4
Medical 4
Mental Health 6
Other 4
Paediatrics 2
Total 35
Source: Survey of NHS Trusts carried out by the ChiefMedical Officer
Table 3 Clinical specialty of hospitaldoctors and dentists suspended for over sixmonths at any time during the period 1998-2002
Specialty Total
Surgical specialties* 207
Anaesthetics 28
Medical specialties 35
Mental health 81
Paediatrics 42
Other 41
Not known 80
Total 514* this includes obstetrics and gynaecologySource: Department of Health
0
10
20
30
40
50
60
70
80
90
100
01/0
2 Q
1
01/0
2 Q
2
01/0
2 Q
3
01/0
2 Q
4
02/0
3 Q
1
02/0
3 Q
2
02/0
3 Q
3
General practitionersHospital and community doctors
YEAR AND QUARTER OF THAT YEAR
NU
MB
ER O
F D
OC
TOR
S R
EFER
RED
0
5
10
15
20
25
30
35
<35 35-39 40-44 45-49 50-54 55-59 60+ <35 35-39 40-44 45-49 50-54 55-59 60+
General practitionersHospital and community doctors
PER
CEN
TAG
E O
F R
EFER
RA
LS
AGE GROUP (YEARS)
Figure 1 Doctors referred to the NationalClinical Assessment Authority (NCAA)April 2001 to end December 2002
Figure 2 Ages of doctors referred to theNational Clinical Assessment Authority

HEALTH CHECK CMO ANNUAL REPORT 2002 63
remember that there are fewer women in theolder cohorts from which most of theAuthority’s referrals come. Also, there arefewer women in those specialties with themost referrals (Figure 3).
There is probably a backlog effect, withmore easily-identified surgical problemscoming to the National Clinical AssessmentAuthority first.
The National Clinical Assessment Authorityis aiming only to release data where interpre-tation can be aided by some sort ofcomparison.The National Clinical Assessment
Authority is monitoring the ethnicity of itsreferrals. For the nine months for which theNational Clinical Assessment Authority hasethnicity data, there was a slight excess ofAsian or Asian British referrals but with indica-tions that the difference is reducing as datacompleteness improves (Figure 4).There iscurrently no ethnicity profile for general prac-titioners as a whole so the National ClinicalAssessment Authority will not releaseethnicity data about general practitionerreferrals at this stage.
The National Clinical Assessment Authority
Poor medical performance
0 5 10 15 20 25 30
Surgical group
Psychiatry group
General medicine
Obstetrics
Paediatric group
Radiology group
Pathology group
Accident and emergency
Anaesthetics
Other specialties
PERCENTAGE
SPEC
IALT
Y G
RO
UP
% of hospital doctors
% of hospital referrals
and gynaecology
0 10 20 30 40 50 60 70
White
Black orBlack British
Asian orAsian British
Mixed
Chinese
Any otherethnic group
Not stated
ETH
NIC
ITY
OF
REF
ERR
ED D
OC
TOR
S
PERCENTAGE
% of hospital workforce
% of hospital doctors referred
OVER THE LAST 18 MONTHS,MUCH WORK HASBEEN DONE TO SET IN PLACE A RANGE OFPRACTICAL APPROACHES TO HELPING NHSBODIES AND DOCTORS THEMSELVES PREVENTPROBLEMS ARISING,IDENTIFY THEM EARLYWHERE THEY DO OCCUR AND TAKE ACTION TORESOLVE THEM.
Figure 3 Clinical specialties of hospital doctorsreferred to the National Clinical AssessmentAuthority relative to the size of those samespecialties in the medical workforce
Figure 4 Ethnicity of hospital doctors referredto the National Clinical Assessment Authorityrelative to the size of different ethnic groups in the hospital workforce.
Fig 1 source: National Clinical Assessment AuthorityFig 2 source: National Clinical Assessment Authority; data
cover the time period 1st April 2001 to endDecember 2002.
Fig 3 source: National Clinical Assessment Authority; datacover the time period 1st April 2001 to endDecember 2002.
Fig 4 source: National Clinical Assessment Authority; datacover the time period 1st April 2002 to endDecember 2002.

HEALTH CHECK CMO ANNUAL REPORT 200264
Action recommended +All NHS Trusts and Primary Care Trusts should be reminded of the needto consult with the National Clinical Assessment Authority beforeconsidering the suspension of a doctor and in cases where there areserious concerns about a doctor's performance.
The Department of Health’s project to review all doctors who havebeen suspended for longer than six months should be integrated into the work of the National Clinical Assessment Authority and led by the Authority.
New advice for local NHS bodies on suspension of doctors should beissued. It should emphasise the need for prior consultation with theNational Clinical Assessment Authority (unless there is an immediatethreat to patient safety). In future, suspensions should be one monthperiods at a time renewable after review within the local NHS organi-sation (rather than in perpetuity as at present).
The practise of unstructured, informal leave (so-called ‘gardeningleave’) should be brought to an end except in the most exceptionalcircumstances.
A further national initiative should be taken to address effectively theneeds of sick doctors or those with drug and alcohol problems.Previous initiatives have not resolved concerns about this source ofpoor performance and how it is dealt with at local level.
case files start to give a picture of the typesof performance problems that the NHS isencountering. Problems are multifactorial:
● about one case in three concerned clinicalcapability, pure and simple;
● about four in five were about a capabilityissue compounded with a health or dysfunctional conduct;
● behavioural problems featured in just overhalf the cases;
● in about one case in six the problem waspurely behavioural;
● in about one case in five there was anunderlying health problem;
● in about one case in five all three problemswere seen in the same case.
An important aim of the new approach isto remove the need for suspension ofdoctors save in the most exceptional circum-stances. It will only be necessary if there is animmediate danger to patients or if thedoctor refuses to co-operate with theiremployer and the National ClinicalAssessment Authority in the assessmentprocess. But, as noted above, in the shortseries reviewed by the National ClinicalAssessment Authority, alternatives tosuspension were possible in all but a fewcases. In many situations, the doctor willvoluntarily restrict clinical work during theprocess of referral to the National ClinicalAssessment Authority, relinquishing thoseareas of work where there is a concern, butleaving the doctor able to continue prac-tising in those areas where no concern hasbeen noted.
Conclusions ■The overwhelming majority of doctors in theNHS work hard to deliver an excellent service.A small group find themselves in difficulty, fora broad range of reasons, and the NHS hastraditionally found great difficulty in dealingwith these problems.Over the last 18 months,much work has been done to set in place arange of practical approaches to helping NHSbodies and doctors themselves preventproblems arising, identify them early wherethey do occur and take action to resolvethem.There is still much to do to address allthe causes of difficulty, but there are a numberof areas where further action is needed.
KEY WEB RESOURCES AND REFERENCES
Donaldson LJ. Doctors with problems in an NHS workforce. BMJ 1994; 308: 1277-1282.
Learning from Bristol: the Report of the Public Inquiry into Children's Heart Surgery at theBristol Royal Infirmary 1984-1995http://www.bristol-inquiry.org.uk/final_report/
National Clinical Assessment Authorityhttp://www.ncaa.nhs.uk/
Department of Health. Supporting doctors, protecting patients. London: Department ofHealth, 1999.http://www.doh.gov.uk/cmoconsult/htm

HEALTH CHECK CMO ANNUAL REPORT 2002 65
Regional focus
Below the Department of Health (at national level), themanagement structure of the NHS is organised into 28Strategic Health Authorities that cover England.Withineach Strategic Health Authority's boundaries are between5 and 19 Primary Care Trusts (PCTs).These new organisa-tions receive the funds allocated by the government for theNHS. Primary Care Trusts plan and provide primary careservices as well as commissioning hospital care (in accor-dance with the needs of their populations) from NHSHospital Trusts and other providers of care.
The local NHS is also responsible for public healthservices. Public health teams are located in Primary CareTrusts as well as in Strategic Health Authorities. Linked tothe public health services within the NHS are the publichealth teams (led by a Regional Director of Public Health)outposted by the Department of Health to RegionalGovernment Offices where they work alongside senior
officials from seven Government Departments: theDepartment for the Environment, Food & Rural Affairs; theDepartment for Transport, Local Government and theRegions; the Department of Trade and Industry; theDepartment for Education and Skills; the Department forWork and Pensions; the Home Office; and the Departmentfor Culture, Media and Sport.
In this section of the report one local health issue is high-lighted in each of the geographical areas covered by thenine public health regions in England.The purpose of thissection of the report is to shine a spotlight on a particularhealth or health service problem which warrants localinvestigation or action.
This is not intended to be a comprehensive review of thehealth of each region but simply a way of drawingattention to a striking finding on analysis of the manyhealth statistics that are collated.
SPOTLIGHTING LOCAL HEALTH PROBLEMS

66 HEALTH CHECK CMO ANNUAL REPORT 2002
East Midlands
Rutland Unitary Local Authority in the EastMidlands has the highest rate of deathsfrom motor vehicle accidents in the wholeof England. In addition, of the top ten localauthorities in England with the worstrecords on deaths from motor vehicleaccidents, six (Rutland, West Lindsey, NorthKesteven, East Lindsey, South
Northamptonshire, Daventry) are local authorities in the EastMidlands. In Rutland the death toll from motor vehicle accidents inthe three year period 1998 to 2000 was 19.6 per 100,000 populationcompared with an average for England of 5.7 deaths per 100,000.Action is needed by all agencies in this part of England to addressthe root causes of the problem and to find a way of removingRutland (and other parts of East Midlands) from their unenviableposition as the motor vehicle death capital of England. Fullcomparison tables of deaths from motor vehicle accident deaths canbe found at: www.doh.gov.uk/ cmo/annualreport2002/regional.
West Midlands
Abortion statistics for England and Wales in2001 showed that just under 88% of legalterminations of pregnancy were performedbefore 13 weeks of gestation. However, thestatistics also showed that eight of the 13health authorities in West Midlands had ahigher than average percentage of NHSabortions performed on their residents at13 or more weeks gestation. The England
and Wales average was 13.4% but Dudley Health Authority andWalsall Health Authority were the highest in the country for lateabortions with percentages of 23.9% and 23.7% respectively. Theearlier in pregnancy an abortion is performed, the lower the risk ofcomplications. The Sexual Health and HIV Strategy ImplementationAction Plan (June 2002) sets a recommended standard that, from2003, Primary Care Trusts should work towards the national standardthat women who meet the legal requirements should have access toan abortion within three weeks of the first appointment with thereferring doctor. This issue needs further investigation in the WestMidlands. Full comparison tables for all health authorities can befound at: www.doh.gov.uk/cmo/annualreport2002/regional.
North East
Between the mid 1990s (1995-1997) andthe late 1990s (1998-2000) death rates fromcancer amongst people under the age of75 years fell by 6.4% in England. Fallsoccurred in 91 of the 95 local healthauthorities. Sunderland was one of onlyfour to show an increase and it showed thelargest percentage increase (3.5%) over
that time period. There is no obvious explanation for this adversetrend for Sunderland but it warrants further investigation. Fulltabulations of these trends in cancer mortality can be found at:www.doh.gov.uk/ cmo/annualreport2002/regional.
London
London has a poor record compared to the rest of the country forsome of the most important disease prevention services. Forwomen's cancer screening services and most of the commonchildhood vaccines, uptake levels for Londoners are well below therest of England. These preventive services are potentially life-savingso poor coverage means that sections of the population whosehealth could be protected are at risk. Nor is the problem restricted toone issue such as a particular vaccine. Across-the-board preventiveservices in London are not delivering the public health protectionthey should be. The poor uptake of breast cancer screening isparticularly worrying. Undoubtedly, public health services in Londonface challenges which are different to some other part of the country- for example of the high mobility of the population. However, thisshould not be an insoluble problem. Concerted action, a specialfocus and sustained commitment should be brought to bear onimproving access to preventive services in London.
Percentage coverage for: London Rest ofEngland
1Breast cancer screening 57.2% 71.6%1Cervical cancer screening 75.9% 82.7%2Meningitis C vaccine 84.2% 93.3%2Whooping cough (pertussis) vaccine 86.9% 93.9%2Diphtheria and tetanus vaccine 87.4% 94.5%2Mumps, measles and rubella vaccine 72.9% 84.5%2Haemophilus influenzae type b vaccine 86.9% 94.1%3Number (per 100,000) quitting smoking after smoking cessation programme 66 137
Source: COVER programme, Department of Health1 data for 2001-20022 Coverage at 24 months of age (July to September 2002)3 Covers period April to September 2002

HEALTH CHECK CMO ANNUAL REPORT 2002 67
North West
Between January 1999 and the end of February 2003, 435 cases ofsyphilis were detected in Greater Manchester. This is a major outbreakby modern standards of a serious sexually transmitted disease. Around80% of the cases were gay men and half had had previous sexuallytransmitted diseases. A quarter of these men who had syphilis werealso HIV positive.
Oral sex was identified as a key transmission route. A more detailedstudy showed that over 90% of the gay men affected never used acondom for oral sex compared to the 88% who regularly used acondom for anal sex.This is very high risk behaviour for acquiring syphilis.Genitourinary medicine services in Greater Manchester are under a greatdeal of pressure with this outbreak. In the North West of England almosthalf of genitourinary medicine clinics have waiting times over 14 days fornon-urgent patients. A lot of work is going on to control this outbreakbut the keys to success will remain rapid identification of infection andprompt action by genitourinary services, and changes to sexualbehaviour particularly amongst gay and bisexual men.
Eastern
It has been recognised that England has a lower level of doctors perhead of population than many other developed countries. This is whycommitments were made in the NHS Plan (published July 2000) togreatly expand the number of NHS consultants. Building up thenumbers of consultants is an essential step in developing theinfrastructure of the NHS so that it can meet the needs andexpectations of a modern health service. It is important that thisoccurs in all parts of the country, since the NHS aims to provide anequitable service.
The latest statistics for numbers of consultants per head ofpopulation in March 2002 show that in the area covered by the EssexStrategic Health Authority, the number of consultants per 100,000population is 41.5. This compares to the national average of 53.3 per100,000 and the area with the highest number of consultants is NorthCentral London (73.7 per 100,000 population). The figures areweighted to take account of need and population flows. There may besome reason why Essex can run services with fewer doctors thanelsewhere but the explanation is not obvious.
Data for each Strategic Health Authority in the country are shown at:www.doh.gov.uk/cmo/annualreport2002/regional.
Regional focus

68 HEALTH CHECK CMO ANNUAL REPORT 2002
Yorkshire and Humber
Bronchitis and emphysema areserious chest diseases in whichthere is destruction of the lungsand obstruction to airflow. They arestrongly associated with cigarettesmoking but certain occupations(such as mining) and atmosphericpollution can also play a part intheir causation. The rate of deathfrom bronchitis and emphysema inDoncaster is the highest in the
country. The standardised mortality ratio (SMR) for deaths from theselung diseases in the time period 1998 to 2000 was 591 for Doncastermen and 465 for both sexes combined. The national average for theSMR is by definition 100. The next highest figure was Wansbeck inNorthumberland which had a SMR of 377 for both sexes combined.The situation for Doncaster represents a major challenge for publichealth and the provision of services for respiratory illness. The fullnational figures for deaths from bronchitis and emphysema can befound at: www.doh.gov.uk/cmo/ annualreport2002/regional.
South East
The area around Brighton andHove has the second highest drugrelated mortality in the country asreported by the Office for NationalStatistics in 2001. In this year therewere 34 deaths in the areacovered by the Brighton and HoveCoroner, representing an annualdeath rate of 13.7 per 100,000population, compared with anational average rate of 3.1 in thesame year. However, the local
public health and substance misuse teams are doing ground-breaking work, putting in to effect the recommendations of the localconfidential inquiry, which may become the model for other areas tofollow. They are working closely with the Chief Executive of the CityCouncil and his staff to tackle the problems raised by drug misuse.
South West
For malignant melanoma the South West Region has the higheststandardised registration ratio (SRR) at 137 (i.e. over a third higherthan the national average of this form of cancer were diagnosed lastyear), and the highest standardised mortality ratio (SMR) at 126 (i.e.26% more people die from it than the national average), out of thenine English Regions. When Local Authorities are ranked by SRR, ofthose that are significantly higher than the average for England andWales, Penwith (231) and Carrick (225) are in first and secondposition. Five other South West Local Authorities are in the top ten(Christchurch, West Devon, South Hams, Teignbridge and Restormel).
A similar pattern is seen for deaths where four out of the top tenLocal Authorities in the country are within the South West. Mendiphas the highest death rate in the country with the SMR at 211. Thereasons for the high incidence and mortality rates, and some genderdifferences, are currently under investigation. New ways of promotingmelanoma awareness are being looked at.
The incidence rate for malignant melanoma in England has beenincreasing over the past three decades. In contrast, survival hasimproved over the past two decades. This pattern is mirrored in theSouth West. It has been suggested that the improved survival may beattributable to better public awareness of the signs and symptoms ofmelanoma, leading to earlier presentation to medical services. It isnot clear whether the continued increase in incidence is due to alag-time in melanoma prevention messages taking effect or whetherunlike the early recognition messages, those on prevention havebeen less effective. There is evidence that a sun-tanned appearanceis still popular and that many people do not take adequateprecautions to reduce ultraviolet exposure. In Australia, after decadesof active pubic health education about the risks of UV exposure, theincidence of melanoma is now decreasing. More needs to be done inthe South West of England to combat this cancer.
Full tabulations of National SRRs and SMRs are available at:www.nchod.nhs.uk.