Embed Size (px)
Citation preview

Oncology 3
Locally advanced
renal cancer
Amar Mohee, Karyee Chow
North West Urology
September 2013

agenda
• Questions
• T3 Tumour
• T4 Tumour
• Targeted Therapy• Immunotherapy• Debulking Nephrectomy
• Paraneoplastic Syndrome
• Indications for adrenalectomy and lymphadenectomy
• Retroperitoneal fibrosis (RPF)

MCQ
• What is the most sensitive imaging for the detection of a tumour thrombus?
• CT-Urogram• CT abdo/pelvis with contrast• CT-KUB• USS with doppler• Contrast MR

MCQ
• What is the most sensitive imaging for the detection of a tumour thrombus?
• CT-Urogram F• CT abdo/pelvis with contrast F• CT-KUB F• USS with doppler F• Contrast MR T

MCQ
• Neoadjuvant systemic therapy for locally advanced renal tumour is associated with
• Increased overall survival• Increased recurrence free survival• Decreased time to recurrence in responders• Increased superficial wound dehiscence• Increased fascial dehiscence

MCQ
• Neoadjuvant systemic therapy for locally advanced renal tumour is associated with
• Increased overall survival F• Increased recurrence free survival
F• Decreased time to recurrence in responders F• Increased superficial wound dehiscence
T• Increased fascial dehiscence F

MCQ
• Which one is true in lymph node positive renal cancer patients?
• The overall survival in N+ve M0 patients is the better than N0 M+ve patients
• Between 7-22% of LN negative patients on imaging will be LN positive
• Chylous ascites >10% after lymphadenectomy• In left sided tumour, the most common site for
LN is para-caval

MCQ
• Which one is true in lymph node positive renal cancer patients?
• The overall survival of N+ve M0 patients is better than N0 M+ve patients F
• Between 7-22% of LN negative patients on imaging will be LN positive T
• Chylous ascites >10% after lymphadenectomyF
• In left sided tumour, the most common site for LN is para-caval F

MCQ
• Which one is NOT a feature of paraneoplastic syndrome?
• Hypercalcaemia• Polycythemia• Anaemia• Hypotension• Cushing’s Syndrome

MCQ
• Which one is NOT a feature of paraneoplastic syndrome?
• Hypercalcaemia F• Polycythemia F• Anaemia F• Hypotension T• Cushing’s Syndrome F

EMQAnswers
T3
T4
Sunitinib
Temsirolismus
Chemotherapy
3%
40%
90%
Level 2 thrombus
Level 3 thrombus
Level 4 thrombus
None
What percentage patient with RCC (all stages) will die of their disease?
Cardiopulmonary bypass is required during thrombectomy
The EAU guidelines recommend lymphadenectomy for which stage of locally advanced RCC?
In patients with metastatic clear cell RCC, with poor prognostic factors, what is the first line of treatment?

EMQAnswers
T3
T4
Sunitinib
Temsirolismus
Chemotherapy
3%
40%
90%
Level 2 thrombus
Level 3 thrombus
Level 4 thrombus
None
What percentage percent with RCC (all stages) will die of their disease?40%
Cardiopulmonary bypass is required during thrombectomyLevel 4
The EAU guidelines recommend lymphadenectomy for which stage of locally advanced RCC?None
In patients with metastatic clear cell RCC, with poor prognostic factors, what is the first line of treatment?
Temsirolismus

T3n0 Tumour
• 57 year female
• PC: Cough + Lower extremity Edema
• No urological complaints
• Performance status: 1
• Bloods: Hypercalcaemia and anaemia
• Imaging – which?

Imaging

imaging

Findings
• Locally advanced tumour involving right kidney
• Renal vein and vena cava thrombus
• CT Chest Negative
• Bone Scan Negative
• What would you recommend?

Management
• Tumour thrombectomy (Level 2)• Therapeutic anticoagulation, No IVC filter• Recent imaging as rapid progression of tumour
(within 1-2 weeks)• Experienced anaesthesia, hepatobiliary,
vascular, cardiac• Incision: midline, chevron, thoracoabdominal• Ligate renal artery first, isolate venous
structures, remove thrombus, repair/patch, then proceed to Radical Nephrectomy + RPLND

tumour thrombus
• Most often ccRCC, can also occur with non renal retroperitoneal tumours (urothelial, adrenal, Wilms)• 20% incidental finding (Gettman et al, Jurol 2003)
• In RCC• Venous invasion: 4-36% (Skinner 1972, Pouliot 2010)• IVC extension: 3-5% (Kearney 1981, Libertino 1987)• Atrial Extension: <1% (Zincke 1987)
• Symptoms• Suprahepatic: Arrhythmia, PE, Syncope• Suprarenal: Budd-Chiari, Ascited, Niliary symptoms• Infrarenal: Pain, Neuropathy, Dilated abdo wall veins

Tumour thrombus

Tumour thrombus
• Not surgical candidate• Poor cardiopulmonary function, poor performance
status, bulky mets, fulminant Budd-Chiari (triad of abdo pain, ascites, hepatomegaly secondary to occlusion of hepatic veins)
• Poorer outcome than operative management (Haferkamp Jurol 07)
• Evaluation of tumour thrombus• Contrast MRI: 100% sensitivity (Lawrenstschuck BJUI
2005)• CT : 84% sensitivity (Guzzo Jurol 2009)
• Invasion of IVC wall (Umbreit et al. AUA 2010)• Thrombus in renal vein >27mm or in IVC >42mm
100% invasion

Contrast enhanced MRI

Outcome
• Prognostic factors• Performance status, positive lymph nodes,
distant mets, sarcamatoid features, fat invasion
• Outcomes (without systemic treatment) – Pouliot et al JUrol 2010• Without mets: 5 year survival – 40-65% • With mets: 5 year survival – 4-30%

Histology
• Pathology• T3bN0Mx ccRCC with>95%
sarcomatoid/rhabdoid de-differentiation• Tumour invading renal vein and artery wall at
margin of resection
• What would you recommend for this patient?• Poor prognostic features• Likely to relapse locally and systemically• Survival < 2-5 years

Debulking nephrectomy and immunotherapy
Treatment n Median survival
Radical nephrectomy and immunotherapy
120 11.1 months
Immunotherapy alone
121 8.1 months
• EORTC 30947
Lancet 358, 966-69, 2001
SWOG 8949
NEJM 345, 1655-9, 2001
Treatment n Median survival
Radical nephrectomy and immunotherapy
42 17 months
Immunotherapy alone
43 7 months
Combined analysis of SWOG and EORTC trialsIFN-α alone – median survival of 7.8 monthsIFN- α +Nephrectomy – median survival of 13.6 months
Flanigan RC, (2004) J Urol 171:1071-1076
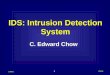
Interleukin-2 No randomised trial comparing IL2 VS IFN
Neph+IL-2 Neph +IF-α
1 Number of pts. 89 120
2 Median survival 16.7m 11.7m
3 5yr survival 19.6% 10%
Comparison of 89 pts. on UCLA database who underwent Nephrectomy +IL-2 Treatment with 120 pts. from SWOG Nephrectomy + IF-α
Pantuck AJ, NEJM,345:1711-1712
Debulking nephrectomy and immunotherapy

Mechanism of action of VHL protein

Lessons learnt from vHL studies
• Abnormalities to vHL gene (3p) are usually seen in clear cell RCC
• An abnormal or mutated vHL gene leads to non-functioning or reduced vHL protein
• vHL protein (amongst other duties) normally degrades HIFα, the latter being a substance released in hypoxic cell conditions
• Therefore, with less vHL protein, we have more cellular HIFα: i.e. the cell thinks it is hypoxic and sets out to fix this via angiogenesis
• This is achieved by increasing VEGF & PDGF which sets off a cascade of reactions mediated by tyrosine kinase promoting angiogenesis and cellular proliferation and probably reduced cell-cell binding

Variables Sunitinib IF-α
Patients 375 375
PF survival 11m 5m
Objective response
31% 6%
Fatigue 7% 12%
GI symptoms 7% 1%
Neutropenia 12% 7%
QOL Better for Sunitinib
Sunitinib malate
Previously untreated metastatic RCC (90% had nephrectomy). Multi centre (101 )RCT.Oral agent 50mg/OD, given for in 6 weeks cycle of 4 weeks and 2 weeks off medication.
Motzer et al NEJM 2007: 356; 115-24
Multikinase inhibitor esp. on VEGF/ PDGF Receptors.

Sorafenib
Variables Sorafenib Placebo
Patients 451 452
Response
Complete 1patient 0
Partial 10% 2%
Stable 74% 53%
Progression 12% 37%
Overall 57% 34%
PF survival 5.5m 2.8m
CVS/HTN 4% 0%
Fatigue 5% 4%
GI symptoms 35 1%
Multi centre (117) RCT. In metastatic RCC following failed immunotherapy.Either Sorafenib 400mg/po/bd Vs placebo (94% had Nephrectomy)
Escudier et al NEJM 2007: 356; 125-34
Mutikinase inhibitor especially RAF kinase

Systemic therapy

Neoadjuvant systemic therapy
PROS
• Primary tumour downstaging/sizing (around 30%) Van der Veldt et al. CCR 2008• Decrease surgical morbidity
• Nephron sparing, unresectable becomes resectable
• Identifies responders – will benefit most from surgery
• Guides choice of therapy in the adjuvant setting
• Improves prognosis
CONS
• ?increase surgical morbidity (systemic effect of treatment?)
• Therapy may alter biology of metastatic disease
• Long term toxicity not known

cytoreduction
12 weeks of Axitinib

Overall Survival after surgery
75 patients treated with Sunitinib neoadjuvant Abel et al. Eur Urol 2011

safety
Chapin et al. Eur Urol 2011

Adjuvant systemic therapy
• No evidence based for therapies below• Local therapy (radiation, embolisation, energy
ablation)• Hormonal therapy• Immunotherapy (IFN, IL-2)• Vaccines• Thalidomide
• Targeted therapy• Data awaited. Trials ongoing

Trials

Adjuvant systemic therapy
• Indication• In the context of a clinical trial
• Treatment duration• Not well defined
• Long term toxicity?

EAU Guidelines for metastatic RCC

T3ni tumour
• 62 female
• PC: Visible haematuria
• Imaging• CT Chest Negative• Bone Scan Negative• CT-U
• Locally advanced right renal tumour• Lymphadenopathy (retrocaval, pericaval, precaval
and interaortic space)

imaging

management
• Any role for• Biopsy?
• Primary vs Node? – ?Lymphoma• Clear cell (vs rest) more amenable to neoadjuvant
systemic therapy
• Neoadjuvant systemic therapy?• Will it improve ease of surgery?• If there is progression, is surgery futile?
• RN + RPLND?

Lymphadenectomy• Presence of LN – decrease OS (0-20%)
• LN dissection in patients with no evidence of lymphadenopathy: 7.5-22.5% detection
• OS• N+M0 = N0M1
• EORTC 30881 (<T3) • RPLND did not improve
• OS• Progression• Secondaries
Waters et al. JUrol 1979Robson et al. Jurol 1963Pantuck et al. Jurol 2003Blom et al Eur Urol 2008

lymphadenectomy
• Morbidity of LN is minimal (EORTC)
• When to do it?• Locally advanced
• (>cT2a)
• High grade• Non clear cell
• Leave a drain• chylous ascites <5%
Capitanio et al. Eur Urol 2011

lymphadenectomy
In metastatic disease• Series from Houston (377 patients with TanyNanyM1 with clear cell
histology)• Most local recurrence within 1 year• Poor prognostic factors for recurrence
• Clear cell histology• Sarcamatoid features• Performance status• >1 LN• Size of tumour
Delacroix et al. JUrol 2011
Aggressive resection may improve outcome in patients with positive nodes
EAU GuidelinesAn extended or radical lymph node dissection does not appear to improve long-term survival following tumournephrectomy

RPLND

T4 tumour
• 48 year male
• PC: Cough
• CXR: pleural effusion
• CT Chest• Effusion + left renal mass• No pulmonary nodules/lymphadenopathy
• How will you manage this patient?

imaging

Chest imaging
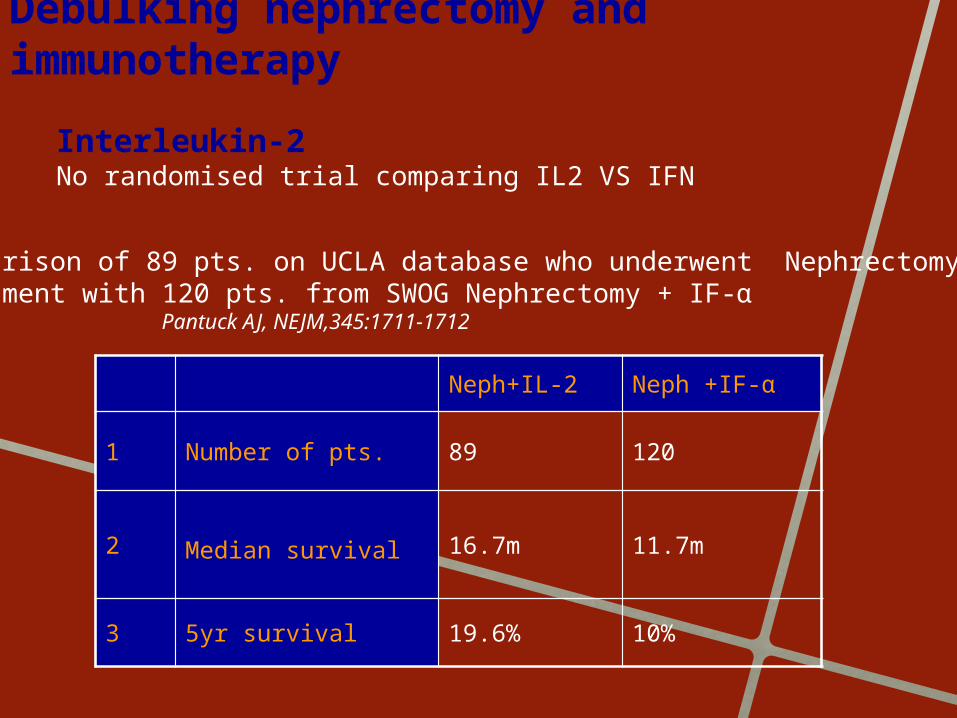
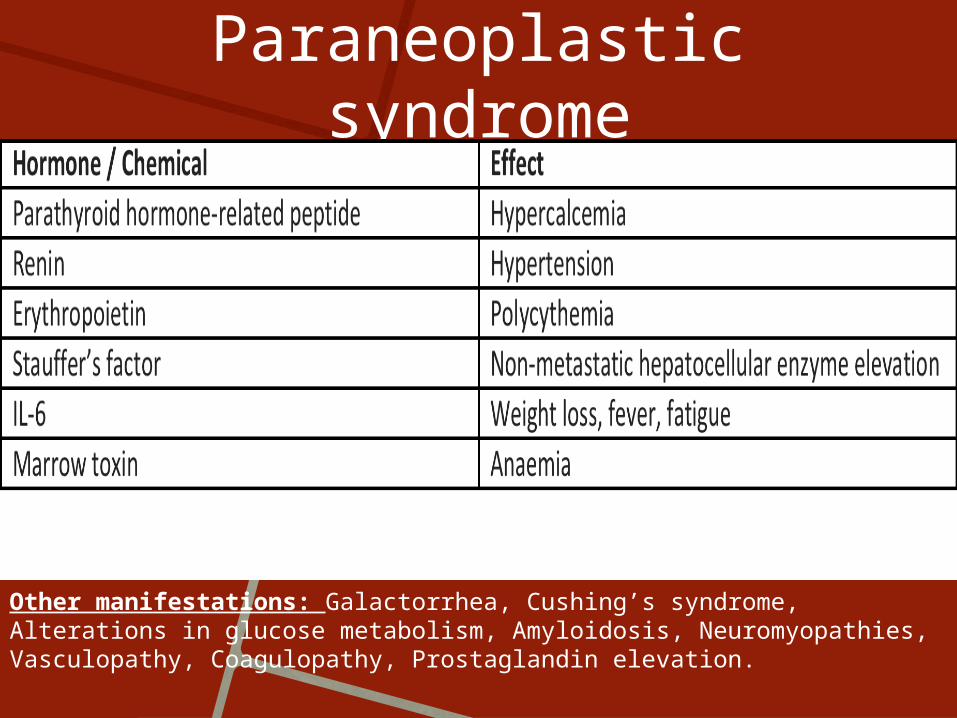
management
• Chest effusion drainage• Malignant vs inflammatory effusion
• If malignant effusion• For systemic therapy only• Cytoreductive surgery (<6 month survival for metastatic
T4)
• If effusion not malignant• Neoadjuvant systemic therapy (non trial basis)• Left RN with en bloc resection of diaphragm and
retroperitoneal musculature
• Pathology• T4N0M0 Furham Grade 4 ccRCC with 30% sarcomatoid de-
differentiation

Paraneoplastic syndrome
• Definition• Clinical syndromes involving non-metastatic
systemic effects that accompany malignant disease. • They are triggered either by an altered immune
system response to a neoplasm, or tumour production of hormonal substances.
• The tumour-related antibodies determine an immune reaction in certain body districts, leading to tissue damage and, hence, the clinical manifestation.
• These syndromes may occur in up to 10-40%.
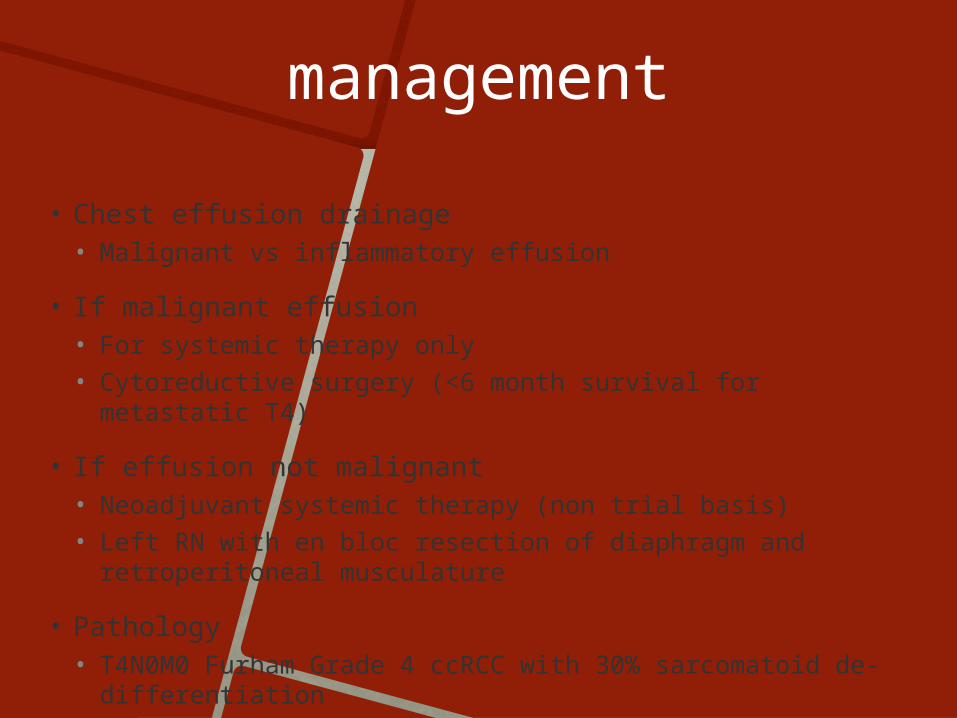
Paraneoplastic syndrome
Other manifestations: Galactorrhea, Cushing’s syndrome, Alterations in glucose metabolism, Amyloidosis, Neuromyopathies, Vasculopathy, Coagulopathy, Prostaglandin elevation.

Paraneoplastic syndrome
• Hypercalcaemia• The most common of the paraneoplastic syndromes in patients with RCC• Approximately 75% have high-stage lesions.• Approximately 50% of all patients with hypercalcemia and RCC have bone
metastases.
• Hypertension• 40% of those with RCC experience hypertension. • Typically associated with low-grade tumours of clear-cell histology.• Potential mechanisms of hypertension in these patients include increased renin
secretion, ureteral or parenchymal compression, presence of an arteriovenous fistula, and poly-cythemia.
• Neoplastic proximal tubular cells themselves may secrete rennin.
• Polycythemia• 1%–8% of cases of RCC.• Elevated serum red blood cell concentrations are believed to be mediated by
erythropoietin . • Although two thirds of RCC patients have elevated EPO levels, only 8% experience
erythrocytosis. • There is evidence to suggest that tumour cells may produce an inactive form of EPO.
Paraneoplastic syndrome
• Non metastatic hepatic dysfunction• Hepatic abnormalities in a patient with RCC with no evidence of
hepatic metastases. • Resolved with nephrectomy but returned with disease recurrence. • 3%–20% of RCC patients, the constellation of signs and symptoms
associated with these hepatic abnormalities is referred to as Stauffer’s syndrome.
• Constitutional symptoms• Up to one third of cases, symptoms such as fever, weight loss, and
fatigue are the first symptoms of RCC• Fever is found in 20%–30% of those with RCC and is the sole
presenting complaint in approximately 2% of patients.
• Most paraneoplastic syndromes associated with localized RCC are definitively treated with nephrectomy only; the recurrence of a previous paraneoplastic syndrome should alert the physician to possible disease progression.

Adrenalectomy
• Incidence• Adrenal metastasis noted in 3.1% post RN+Adrenalectomy
• Tumour size>8cm and M status were independent predictors
Paul R,J Urol. 2001 Jul;166(1):59-62
• Imaging• 511 RN from UCLA reviewed. Pre-op CT had a specificity of 99%
and sensitivity of 90%
• 0.6% incidence in T1-2, 8.1% for >T3.
Tsui K, J Urol. 2000 Feb;163(2):437-41
• Survival Benefit• 1010 pts with RN+A VS 625 pts with RN
• No survival advantage (75% vs73%).

Adrenalectomy• EAU Guidelines
• Adrenalectomy is not indicated in the following situations:• Pre-operative tumour staging (CT, MRI) shows a normal
adrenal gland• Intra-operative findings do not give any indication of a
nodule within the adrenal gland suspicious of metastatic disease
• There is no evidence of direct invasion of the adrenal gland by a large upper pole tumour.
• Indications for Adrenalectomy • Upper pole tumours• Tumours >7cm• M1 disease

RPF
• Epidemiology• 1 per 200,000-500,000• Age 40-60
• Extensive fibrosis typically centred over the anterior surface of the L4 and L5 vertebrae.
• Aetiology :• Autoimmune disease • Malignancy - 8% - associated with metastatic
malignancy • Retroperitoneal trauma• Inflammatory periaortitis (severe atherosclerosis) • Chronic retroperitoneal inflammation• Certain drugs (beta-blockers, methysergide, methyldopa)• Irradiation
RPF
• Symptoms• Dull, poorly localised pain in the flank, back,
scrotum or lower abdomen (92%)• 50% have hypertension• Obstruction of the ureters with renal
insufficiency earliest and most common organ involvement.
• Aims in management : • Preserve renal function • Reduce morbidity • Suppress inflammatory processes.


SOURCES
• Previous slides from Addla/Lewin with Shackley as supervisor
• Pubmed• EAU Guidelines• AUA course