Embed Size (px)
Citation preview

One Lung VentilationOne Lung Ventilation
Paul Alfille

Disclaimers and Commercial hSponsorships
• NoneNone
Andrea Pisano 1437 “The Creation of Eve”

Goals and ObjectivesGoals and Objectives
• What are the indications for one lungWhat are the indications for one lung ventilation
• What is best practice for managing one lung• What is best practice for managing one‐lung ventilationWh h h i f l• What are the techniques for one‐lung ventilation

Indications for Lung IsolationIndications for Lung Isolation
• Surgical exposure • Differential ventilationSurgical exposure• Lung resection• Airway protection
Differential ventilation– Post transplant– Giant blebAirway protection
– Hemoptysis– Infection
– Bronchopleural fistula– bronchial disruption
• Lung lavage

How to chooseHow to chooseSurgical exposure
Differential ventilation
Lavage Difficult airway
Small patient
Bronchial lesionexposure ventilation airway patient lesion
DLT √√ √√ √√ xx xx √√
Blocker √√ xx xx √√ √√ xx
Bronchialtube
√√ xx xx √√ √√ √√
Spontaneous √√ xx xx √√ √√ √√ptx

CarlensCarlens
• Left sidedLeft sided with carinalhookhook
• Right sided versionversion called the White tubeWhite tube

RobertshawRobertshaw
• Both left and rightBoth left and right sided version
• No carinal hook• No carinal hook• RUL window for right
iversion• Multiple modern designs

Right sided tubesRight sided tubes
• Asymmetric cuffhttp://www.sumi.com.pl/en/double‐lumen‐bronchial‐tube‐right‐sided/
Asymmetric cuff• RUL orifice• Often avoided by• Often avoided by the inexperienced
Mallincrodt

Bronchial lengths
•FOB, casts, cadavers
•Female slightly smaller
• Benumof JL Partidge BL Salvatierra C Keating J
g y
•Design of tube important
Benumof JL, Partidge BL Salvatierra C, Keating J.Margin of safety in positioning positioning modern double‐lumen endotracheal tubesAnesthesiology 1987 67:729

Tips for positioning


Is a RDLT time efficient?Is a RDLT time efficient?Right DLT Left DLT
Initial placement min 3.37 2.08
Left lung collapse min 13 10
FOB exams number 2 2
Surgical exposure ExcellentFair
19/190/19
19/201/20Fair 0/19 1/20
RUL expansion Post‐op Xray Full 17/17 Full 18/18
Campos JH, et al. The Incidence of Right Upperlobe Collapse When Comparing Right‐sided Double Lumen Tube Versus a Modified Left Double‐Lumen Tube for Left‐Sided Thoracic Surgery. Anesth Analg 2000; 90:535‐40

Porcine bronchusPorcine bronchus• Incidence < 1%• Some or all segments of RUL start above carina
• Very occasionally on L side, too.side, too.
• Contraindication for ipsilateral DLT (oripsilateral DLT (or blocker)

MallinckrodtMallinckrodt
• Left DLT– 28 32 35 37 39 41
• Right DLT– 35 37 39 4135 37 39 41
• Left with Hook35 37 39 41– 35 37 39 41
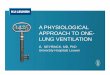
RÜSCHRÜSCH
• Left RobershawLeft Robershaw– 26 28 35 37 39 41
• Right Robershaw• Right Robershaw– 26 28 35 37 39 41
• Carlens– 35 37 39 41
• Dr. White– 35 37 39 41

PortexPortex
• Nicest design for theNicest design for the top of the tube

Phycon (Fuji Systems)Phycon (Fuji Systems)
• “Silbroncho”Silbroncho• Left and Right DLT
l ibl il i• Flexible silocone wire‐reinforced bronchial lumen
• 33,35,37,39 Fr• Less kinkingg

Endobronchial tubeEndobronchial tube
• Long tubeLong tube• Flexible wire‐reinforcedS ll ff• Small cuff
• Short distance cuff to tip• 5.5 6.5 7.5 mm I.D.
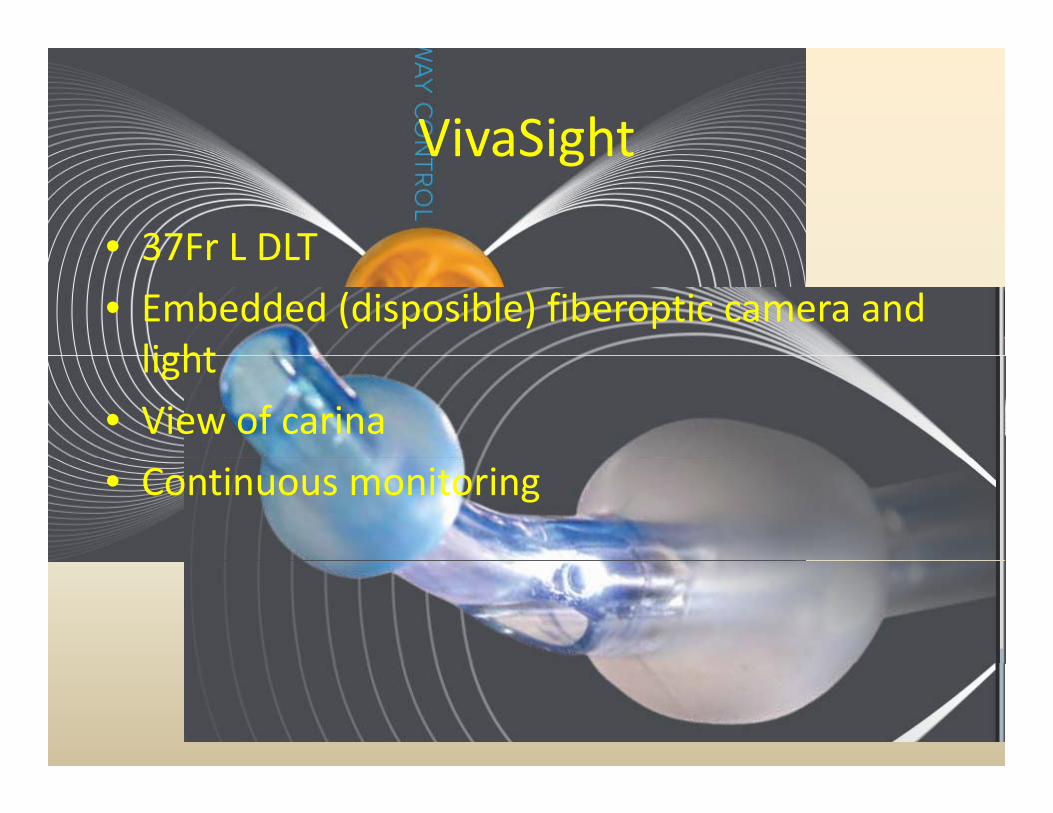
VivaSightVivaSight
• 37Fr L DLT37Fr L DLT• Embedded (disposible) fiberoptic camera and lightlight
• View of carina• Continuous monitoring

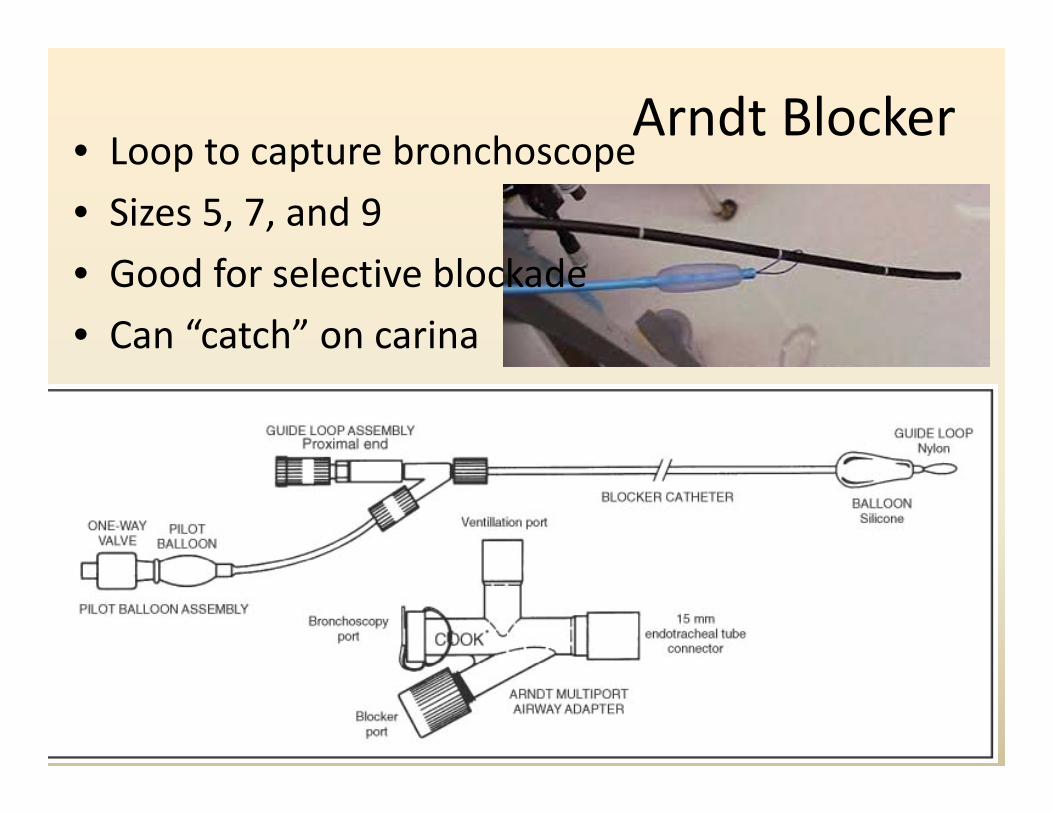
Arndt Blocker• Loop to capture bronchoscope• Loop to capture bronchoscope• Sizes 5, 7, and 9• Good for selective blockade• Can “catch” on carina

Endobronchial tubeEndobronchial tube
.

Fogarty Embolectomy CatheterFogarty Embolectomy Catheter
• No suction/CPAP lumenNo suction/CPAP lumen••• Various sizes• Connections difficult

Univent TubeUnivent Tube
• Integral blockerIntegral blocker


Tube variability – bronchial lumenTube variability bronchial lumen
W. J. RUSSELL, T. S. STRONG Dimensions of Double‐Lumen Tracheobronchial TubesAnaesthesia and Intensive Care, Vol. 31, No. 1, February 2003
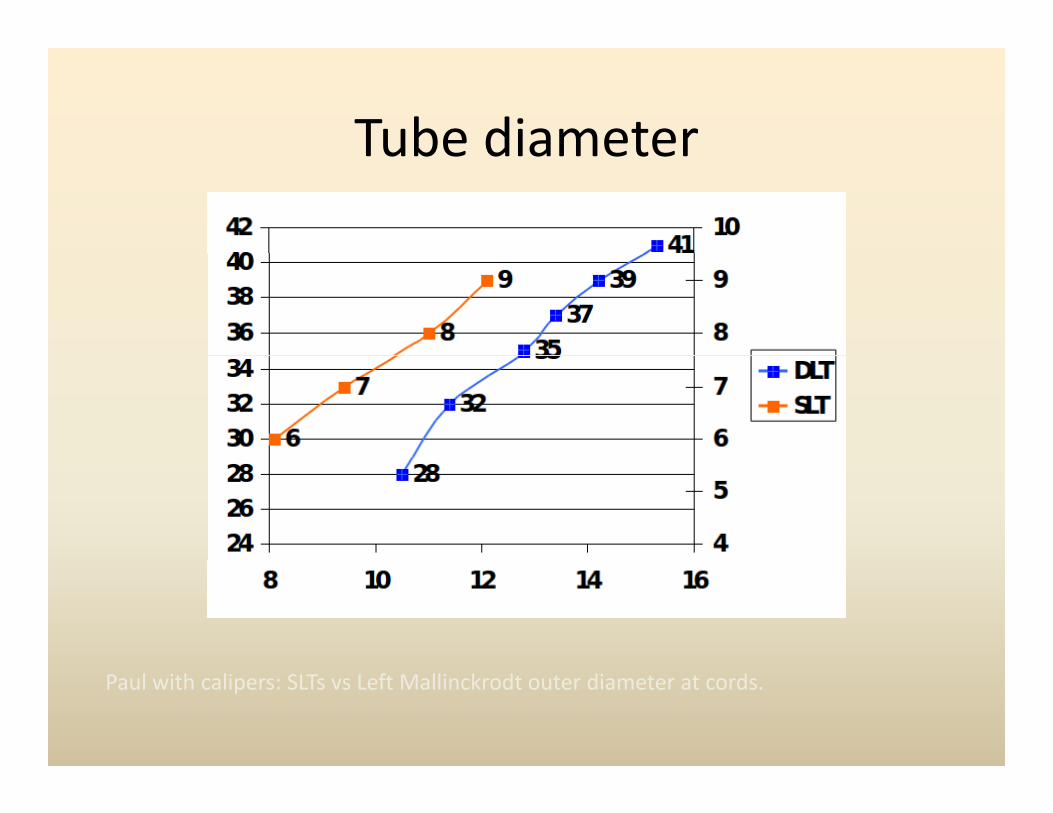
Tube diameterTube diameter
Paul with calipers: SLTs vs Left Mallinckrodt outer diameter at cords.

ResistanceResistanceChart TitleHigh resistance
8
10
12
4
6
8
0
2
Left Right
C 37 C 39 C 41 L RS sm L RS med L RS lgW 37 W 39 W 41 R RS sm R RS med R RS lg
Low resistance
Hammond JE, Wright DJ. Comparison of the Resistances of Double‐Lumen EndobronchialTubes. Be J Anaesth 1984; 56:299‐302

ResistanceResistance
• Overall resistance ~ 7 0 to 8 0 ETTOverall resistance 7.0 to 8.0 ETT– (both lumen)
• Better than Univent tube• Better than Univent tube• Unclear comparison with blockers
– (resistance to both lumen low and comparable)
• Use in ICU discouraged because of unfamiliarity rather than resistance.
Chiaranda M, et al. Measurement of the flow‐resistive properties of double‐lumen bronchial tubes in vitro. Anaesthesia 1989; 44:335‐40

Hypoxia and OLVHypoxia and OLV
• Unique is pure • Oxygenation vs LungUnique is pure anatomic shunt
• Definitions vary
Oxygenation vs Lung protection
y– 10% had Sat < 90
• Pre‐op conditionsp• Position• Ventilatione a o• FiO2• DrugsDrugs

Factors Effecting ShuntFactors Effecting Shunt
• Ventilated side:Ventilated side:– Improve gas exchange
– Keep low PVR• Non‐ventilated:
– Keep PVR high– Add O2
• Improve mixed venous O2

Shunt and oxygenationShunt and oxygenation
• Dependent onDependent on HPV
• FiO2 has littleFiO2 has little effect at high shunt fraction
• Cardiac output and mixed venous content important

Mixed venous concentrationMixed venous concentration
• More importantMore important at high shunt
• Metabolic rate• Metabolic rate• Anemia• Cardiac output

PositionPosition
• Gravity has pO2Gravity has strong effect on 1LV 200
250
300
on 1LV• Supine < Lateral
100
150
200
pO2
Lateral0
50
Ventilated below Supine Ventilated above
Szegedu LL, et al. Gravity is an important determinant of oxygenation during one‐lung il i hi l S d 20 0 6 0ventilation. Acta Aneasthiol Scand 2010; 6:744‐50

Cardiac OutputCardiac Output
• HigherHigher cardiac outputoutput improves oxygenationoxygenation
• Confounds some studiessome studies
Singer P, Scott WAC. Arterial Oxygenation during One‐lung ventilation. AnesthesiologySinger P, Scott WAC. Arterial Oxygenation during One lung ventilation. Anesthesiology 1995; 82:940‐6

AssymetryAssymetry
• Sicker non‐ventilatedSicker non ventilated lung helps
• Higher Δ between lung• Higher Δ between lung• Better oxygenation• Prior lobectomy
Yamamoto Y, et al. Gradient of bronchial end‐tidal CO2 during two‐lung ventilation in lateral decubitus position is predictive of oxygenation disorder during subsequent one‐lung ventilation. J Anesth 2009; 23:192‐7
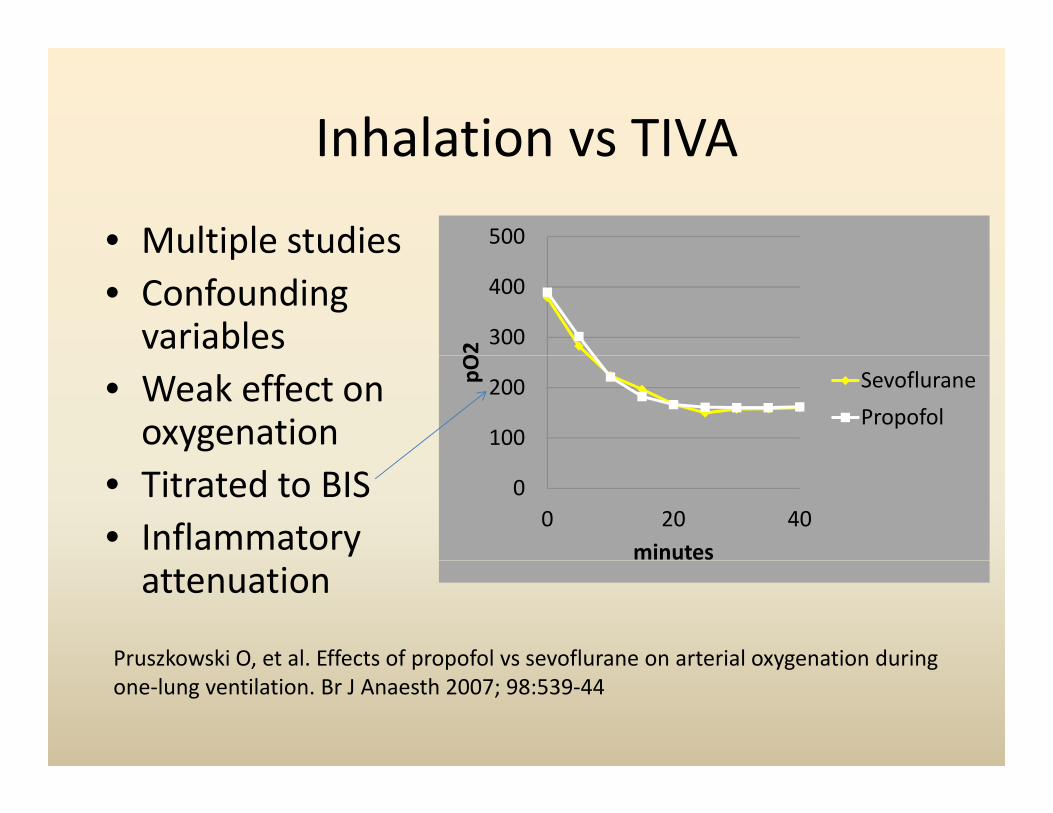
Inhalation vs TIVAInhalation vs TIVA500• Multiple studies
300
400
O2
u t p e stud es• Confounding variables
100
200pO SevofluranePropofol
• Weak effect on oxygenation
00 20 40
minutes
• Titrated to BIS• Inflammatory attenuation
Pruszkowski O, et al. Effects of propofol vs sevoflurane on arterial oxygenation duringPruszkowski O, et al. Effects of propofol vs sevoflurane on arterial oxygenation during one‐lung ventilation. Br J Anaesth 2007; 98:539‐44

Inflammation and Anesthetic
• BAL samples fromBAL samples from ventilated lung
• No difference in• No difference in oxygenationD i• Decrease in markers
• Clinical import unclear
Schilling T et al Effects of Volatile and Intravenous Anesthesia on the Alveolar and SystemicSchilling T, et al. Effects of Volatile and Intravenous Anesthesia on the Alveolar and Systemic Inflammatory Response in Thoracic Surgical Patients. Anesthesiology 2011; 115:65‐74

DexmedetomidineDexmedetomidine500
200
300
400
Dexmedetomidine
0
100
200 Control
0TLV OLV‐1 OLV‐2
Anesthetic sparing effect?
Kenman S. et al. Effects of dexmedetomidine on oxygenation during one‐lung ventilation for thoracic surgery in adults. J Minim Access Surg 2011; 7:227‐31

KetamineKetaminepO2/FiO2
100
150
200
0
50
Ketamine Ketamine Control
pO2/FiO2
Ketamine 1.0mg/kg
Ketamine 0.5mk/kg
Control
Iwata M, et al. Ketamine eliminates propofol pain but does not affect hemodynamics during induction with double‐lumen tubes. J Anesth 2010; 24:31‐7

VasopressorsVasopressors
• α‐block↓ HPVα block ↓ HPV• β‐block ↑ HPV• Epidural effect from• Epidural effect from α and β block
Brimioulle S, et al. Sympathetic modulation of hypoxic pulmonary vasoconstriction in intact dogs Cardiovasc Res 1997; 34:384‐92

EpiduralEpidural
354045
500
600
• Equivocal studies
20253035
300
400 BupivSufIV
Equivocal studies• Propofol GASi il O2
5101520
100
200IVBupiv Qs/QtSuf Qs/Qt
/
• Similar pO2• Similar Qs/Qt
05
0IV Qs/Qt
• Similar output
Jung SM, et al. The effect of thoracic epidural anesthesia on pulmonary shunt fraction andJung SM, et al. The effect of thoracic epidural anesthesia on pulmonary shunt fraction and arterial oxygenation during one‐lung ventilation. J Cardiothoracic Vasc Anesth 2010; 24:456‐62

AlmitrineAlmitrine

AlmitrineAlmitrine2.5
3
120
140
c
1.5
2
80
100ardiac
pO
Almitrine
Placebo
140
60
c
inde
O2 Almitrine2
Placebo2
0
0.5
0
20
1‐lung Load Maintainance
x
• Improves oxygenation• Little effect on cardiac outputpDailibon ND, et al. Treatment of Hypoxemia During One‐Lung Ventilation Using Intravenous Almitrine. Anesth Analg 2004; 98:590‐4

Nitric OxideNitric Oxide
• Dilates pulmonary vesselsDilates pulmonary vessels• Matched to ventilation
ff i O i l• No effect in OLV in normals• Perhaps in PAH
Pre, 40ppm, post
Rocca GD, et al. Inhaled Nitric Oxide Administration During One‐Lung Ventilation in Patients Undergoing Thoracic Surgery. J Cardiothor Vasc Anesth 2001; 15:218‐23

Tidal volumeTidal volume
• High TV improvesHigh TV improves oxygenation
• Higher PEEP may• Higher PEEP may balance (based on plateau pressureplateau pressure
• Lung injury
Kim SH, Jung KT, An TH. Effects of tidal volume and PEEP on arterial blood gases and pulmonary mechanics during one lung ventilation J Anesth 2012; 26:568 73pulmonary mechanics during one‐lung ventilation J Anesth 2012; 26:568‐73

Tidal volumeTidal volume
• Low TV protects lungLow TV protects lung• PEEP prevents collapse• Moderate FiO2Moderate FiO2• 3‐6 ml/kg for OLV

• ConventionalConventional– 10 ml/kg– FiO2 1.0– ZEEP
• Protective– 6 ml/kg– FiO2 0.5– 5 PEEP– 58% required ↑ FiO2
Yang M, et al. Does a Protective Ventilation Strategy Reduce the Risk of Pulmonary Complications After Lung Cancer Surgery. A Randomized Controlled Trial. Chest 2011; 139:530‐37

PEEPPEEP
• Variable effect on PVRVariable effect on PVR• Dependent lung at low volumevolume
• Optimal PVR and i FRCoxygenation at FRC
Simmons DH at al. Relation Between Lung Volume and Pulmonary Vascular Resistance. Circ Res 1961; 9:465‐71

PEEPPEEP
• Variable effect on PVRVariable effect on PVR• Dependent lung at low volumevolume
• Optimal PVR and oxygenation at FRC
Simmons DH at al. Relation Between Lung Volume and Pulmonary Vascular Resistance. Circ Res 1961; 9:465‐71

PEEPPEEP
V i bl lt• Variable results• 6 ml/kg TV• Recruitment• 12/41 improved12/41 improved• No Δ CO, MAP
Hoftman N, et al. Positive end expiratory pressure during one‐lung ventilation: Selecting ideal patients and ventilator settings with the aim of improving arterial oxygenation. Ann Card Anaesth 2011;14:183‐7.yg

RecruitmentRecruitment
• Applied prior to 600ControlApplied prior to
OLV• Improved pO2 300
400
500
pO2
ControlARS
• Improved pO2• Improved VD/VT
0
100
200
p
0TLV TLV 20 OLV 20 OLV 40 TLV
Unzeta C, et al. Alveolar recruitment improves ventilation during thoracic surgery: a randomized controlled trial. Br J Anaesth 2012; 108:517‐24

HypercapneaHypercapnea
• UnpublishedUnpublished• Therapeutic hypercapnea (exogenous CO2)
d d fl k• Reduced inflammatory markers

Limb ischemiaLimb ischemia• Limb Remote Ischemic Preconditioning Attenuates
Lung Injury after Pulmonary Resection under Propofol–Remifentanil Anesthesia: A Randomized Controlled Studyy
• Li, Cai M.D.; Xu, Miao M.D.; Wu, Yan M.D.; Li, Yun‐Sheng M.D.; Huang, Wen‐Qi M.D.; Liu, Ke‐XuanM.D., Ph.D.
• Anesthesiologygy• Issue: Volume 121(2), August 2014, p 249–259

CPAPCPAP
• Very effective 600
pO2 and CPAP
Very effective• Intact airwayS i fl d
300
400
500
pO2 2cm CPAP
5 CPAP• Start inflated• Surgical 0
100
200
2 lung 1 lung CPAP 2 lung
5cm CPAP
conditions• Inject O2jHogue CW. Effectiveness of Low Levels of Nonventilated Lung Continuous Positive Airway Pressure in Improving Arterial Oxygenation During One‐Lung Ventilation. A th A l 1994 79 364 7Anesth Analg 1994; 79:364‐7

Selective ventilation
500
pO2 and CPAP
Selective ventilation
• Selective lobar
200250300350400450
pO2 0 CPAP
5 CPAP
Selective lobar blockade
• Optionally
050100150200
2 lung 1 lung +/‐CPAP Lobar 2 lung
5cm CPAPOptionally CPAP only that lobe
Campos JH. Effects on Oxygenation During Selective Lobar Versus Total Lung Collapse With of Without Continuous Positive Airway Pressure. Anesth Analg 1997; 85:583‐6 850 2850‐2
• “rescue” blocker with DLT
Sumitani M, et al. Selective lobar bronchial blockade using a double‐lumen endotracheal tube and bronchial blocker. Gen Thorac Cardiovasc Surg 2007; 55:225‐7

Selective ventilationSelective ventilation
• BronchoscopeBronchoscope in lobe
• O2 carefully• O2 carefully
Ku CM, Slinger P, Waddell TK. A Novel Method of Treating Hypoxemia During One‐Lung Ventilation for Thoracoscopic Surgery. J Cardiothor Vasc Anesth 2009;23:850‐2

• Open airwayOpen airway• HFJV vs CPAP? CO• ? COPD
• Hemodynamics
El Tahan MR, et al. Effects of Nondependent Lung Ventilation With ContinuousEl Tahan MR, et al. Effects of Nondependent Lung Ventilation With Continuous Positive‐Pressure Ventilation on Right‐Ventricular Function During 1‐Lung Ventilation. Sem Cardiothor and Vasc Anesth 2010; 14:291‐300

• Sander’s injector• Hand control Sander’s• Vary driving pressure, rate, I:E ratioR i bl d t
Sander s
• Requires blender to alter FiO2
• No pressureNo pressure monitoring
• Risk of barotra mabarotrauma
• Risk of hypoventilationhypoventilation

Monsoon Automated JetMonsoon Automated Jet
Safety cut offidifi i d h iHumidification and heating
FiO2Consistent

Extreme measuresExtreme measures
• Pulmonary artery occlusionPulmonary artery occlusion• ECMOC• CPB

ECMOECMO
• Endobronchial intubtion• Marginal oxygenation• VV• Impro e o enation• Improve oxygenation• Less need for
anticoagulationg
Anesthetic Management of a Delayed Carinal Resection Following Traumatic DisruptionKevin A. Blackney, Paul H. Alfille. Open Journal of Anesthesiology, 2014, 4, 231‐235

AlgorithmAlgorithm
• Severe desaturationSevere desaturation– 2 lung ventilation
• GradualGradual– Check tube position, suction, vent settings– Increase FiO2Increase FiO2– Try Recruitment and PEEP– CPAP or selective ventilation– Intermittent inflation– Adjust hemodynamicsj y– Surgical occlusion of blood flow