Embed Size (px)
Citation preview
1
One Moment Please
One Moment PleaseOne Moment Please
Skin Cancer
Thomas Olencki, DO Thomas Olencki, DO
Today’s WebcastFriday, 09/09/11, Noon
,David Carr, MD
,David Carr, MD
2
New FeaturesNew FeaturesEnlargeSlidesEnlargeSlides
LinksLinks
Use the email function to let us know what you thinkUse the email function to let us know what you think
PollingPollingChaptersChapters

3
© The Ohio State University Medical Center, 2011© The Ohio State University Medical Center, 2011
The following program is a Continuing Medical Education Activity sponsored by The Ohio State University Medical Center. The design and production of this CME Activity is the sole responsibility of The Ohio State University Medical Center.
Accreditation Statement
The Ohio State University Medical Center, Center for Continuing Medical Education (CCME) is accredited by the Accreditation Council for Continuing Medical Education (ACCME®) to provide continuing medical education for physicians.
AMA Designation Statement
The Ohio State University Medical Center Center for Continuing Medical Education
The following program is a Continuing Medical Education Activity sponsored by The Ohio State University Medical Center. The design and production of this CME Activity is the sole responsibility of The Ohio State University Medical Center.
Accreditation Statement
The Ohio State University Medical Center, Center for Continuing Medical Education (CCME) is accredited by the Accreditation Council for Continuing Medical Education (ACCME®) to provide continuing medical education for physicians.
AMA Designation Statement
The Ohio State University Medical Center Center for Continuing Medical EducationThe Ohio State University Medical Center, Center for Continuing Medical Education designates this educational activity for a maximum of 1 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
As an enduring material this CME Activity is approved for three years from original release. Original release 09/09/11. Termination date 09/09/14.
CCME Disclosure Statement
As a provider of AMA PRA Category 1 Continuing Medical Education, it is the policy of CCME to adhere to the ACCME Standards for Commercial Support to avoid any
The Ohio State University Medical Center, Center for Continuing Medical Education designates this educational activity for a maximum of 1 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
As an enduring material this CME Activity is approved for three years from original release. Original release 09/09/11. Termination date 09/09/14.
CCME Disclosure Statement
As a provider of AMA PRA Category 1 Continuing Medical Education, it is the policy of CCME to adhere to the ACCME Standards for Commercial Support to avoid anyCCME to adhere to the ACCME Standards for Commercial Support to avoid any conflict of interest and/or commercial bias and must ensure balance, independence, objectivity and scientific rigor in all its sponsored educational activities. All individuals who are in a position to control content of an educational activity, including presenters, panel members and moderators, must to disclose any relevant financial relationships that create a conflict of interest.
Nothing in this program is intended to imply that any off-label or unapproved product use discussed is reimbursed by any government or private payor or that submission of a claim for such use is proper.
Presentation may include discussion of services and unapproved or off-label usage of commercial products or devices Log on to ccme osu edu for more information
CCME to adhere to the ACCME Standards for Commercial Support to avoid any conflict of interest and/or commercial bias and must ensure balance, independence, objectivity and scientific rigor in all its sponsored educational activities. All individuals who are in a position to control content of an educational activity, including presenters, panel members and moderators, must to disclose any relevant financial relationships that create a conflict of interest.
Nothing in this program is intended to imply that any off-label or unapproved product use discussed is reimbursed by any government or private payor or that submission of a claim for such use is proper.
Presentation may include discussion of services and unapproved or off-label usage of commercial products or devices Log on to ccme osu edu for more information
4
The following planning committee members have no relevant financial relationships with commercial interests to disclose:
Planning Committee DisclosuresPlanning Committee Disclosures
Jame Allen, MD
Barbara Berry
Derrick Freeman
The following planning committee members’ educational unit does not have a financial interest or affiliation with an organization that may receive direct benefit from the subject of the proposed CME activity, and they will not be personally compensated for their role in the planning or execution of this proposed CME activity by an
i ti th th Th Ohi St t U i itorganization other than The Ohio State University:
Jame Allen, MD
Barbara Berry
Derrick Freeman
Speaker DisclosuresSpeaker Disclosures• The following presenters for this educational activity disclose that they have the following relationships with commercial interests to disclose.
Thomas Olencki DOThomas Olencki, DO
Advisory Board Membership – GenentechGrants/Research support – Genentech, Bristol Myers-Squibb
David Carr, MD – Consultant – Healthy Advice
D Ol ki’ t ti ill i l d di i f• Dr. Olencki’s presentation will include discussion of unapproved or “off-label” usage of commercial products and/or services
Thomas Olencki, DO
David Carr, MD
5
Agenda Disclaimer
CCME presents this activity for educational purposes only. Participants are expected to utilize their own expertise and judgment while engaged in the practice of medicine The
Agenda Disclaimer
CCME presents this activity for educational purposes only. Participants are expected to utilize their own expertise and judgment while engaged in the practice of medicine Thejudgment while engaged in the practice of medicine. The content of the presentations is provided solely by presenters who have been selected for presentations of recognized expertise in their field.
No further reproduction or distribution is permitted by electronic transmission or any other means The presentations during this
judgment while engaged in the practice of medicine. The content of the presentations is provided solely by presenters who have been selected for presentations of recognized expertise in their field.
No further reproduction or distribution is permitted by electronic transmission or any other means The presentations during thistransmission or any other means. The presentations during this webcast are the intellectual property of the presenter and require his/her permission for further use.
This activity will review the treatment of Skin Cancer.
transmission or any other means. The presentations during this webcast are the intellectual property of the presenter and require his/her permission for further use.
This activity will review the treatment of Skin Cancer.
The Ohio State University Medical CenterMedical Center
Arthur G. James Cancer Hospital and Solove Research Institute
6
Skin CancerSkin Cancer
7
Thomas Olencki, DO David Carr, MD
Jim Allen, MDProfessor of Internal MedicineThe Ohio State University Medical Center
Jim Allen, MDProfessor of Internal MedicineThe Ohio State University Medical Center
8
ccme.osu.educcme.osu.eduCME tracking, 24/7, current therapies, post-tests
Madison, WisconsinPhoto by Dori
9
Skin CancerSkin Cancer
Thomas Olencki, DODavid Carr, MD
Thomas Olencki, DODavid Carr, MD
10
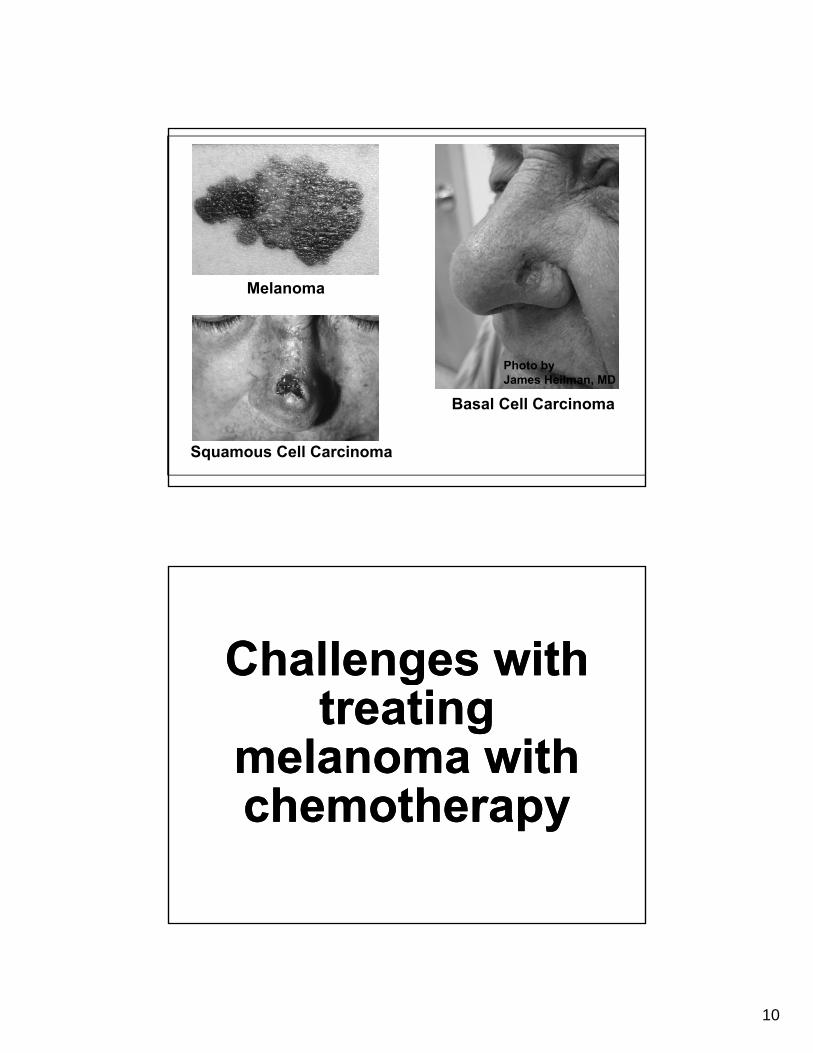
Melanoma
Photo by
Basal Cell Carcinoma
Squamous Cell Carcinoma
Photo byJames Heilman, MD
Challenges with Challenges with gtreating
melanoma with chemotherapy
gtreating
melanoma with chemotherapychemotherapychemotherapy
11
you are invited to participate
you are invited to participate
and email us with your questions
and email us with your questions
EMAILEMAIL
MohsMohs Surgery: Overview & Surgery: Overview & IndicationsIndications
MohsMohs Surgery: Overview & Surgery: Overview & IndicationsIndicationsIndicationsIndicationsIndicationsIndications
David Carr, MDAssistant Professor
Division of DermatologyThe Ohio State University College of Medicine
12
Video PresentationVideo Presentation
Mohs Surgery
Video PresentationVideo Presentation
Q & A with Dr. David Carr
13
Video PresentationVideo Presentation
Dr. David Carr’s Key Point
Prognosis ofPrognosis ofPrognosis of metastatic melanoma
Prognosis of metastatic melanoma
14
Review of 2 New Meds for Review of 2 New Meds for Therapy of Therapy of MetasticMetastic
MelanomaMelanoma
Review of 2 New Meds for Review of 2 New Meds for Therapy of Therapy of MetasticMetastic
MelanomaMelanomaMelanoma Melanoma Melanoma Melanoma
Thomas Olencki, DOClinical Professor of MedicineDivision of Medical Oncology
Ohio State University College of Medicine
FDA Approved Drugs For Treatment Of Metastatic Melanoma
FDA Approved Drugs For Treatment Of Metastatic Melanoma
• Dacarbazine (DTIC) – 1975
• Interleukin-2 (IL-2) – Jan 1998
• Yervoy (ipilimumab) – March 2010Yervoy (ipilimumab) March 2010
• Zelboraf (vemurafenib) – August 2011
15
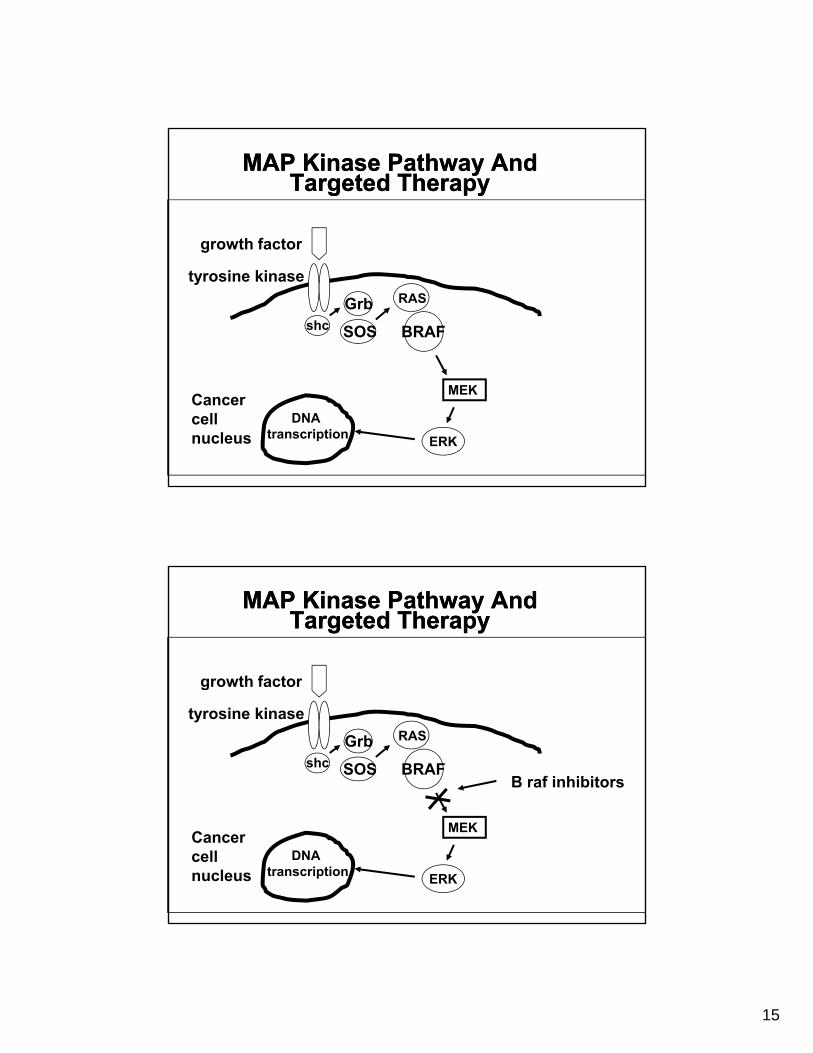
MAP Kinase Pathway And Targeted Therapy
MAP Kinase Pathway And Targeted Therapy
growth factor
shc
Grb
SOS
RAS
BRAF
growth factor
tyrosine kinase
MEKCancercellnucleus ERK
DNAtranscription
MAP Kinase Pathway And Targeted Therapy
MAP Kinase Pathway And Targeted Therapy
growth factor
shc
Grb
SOS
RAS
BRAF
growth factor
tyrosine kinase
B raf inhibitors
MEKCancercellnucleus ERK
DNAtranscription
16
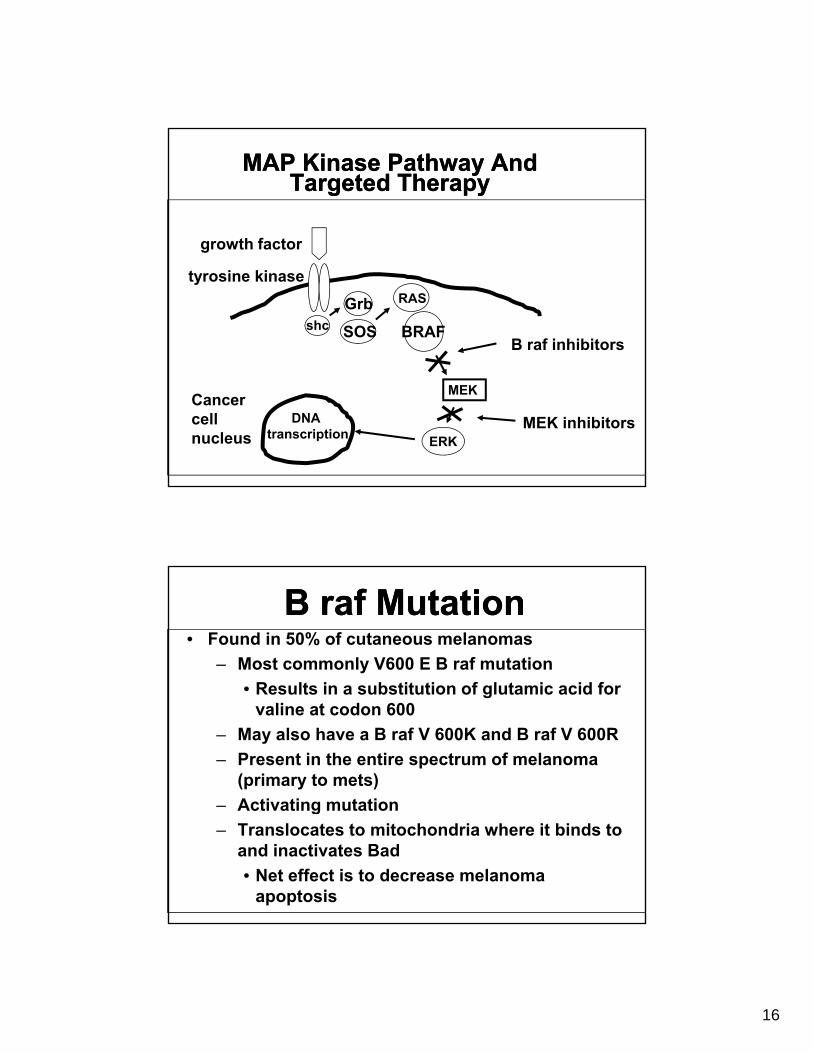
MAP Kinase Pathway And Targeted Therapy
MAP Kinase Pathway And Targeted Therapy
growth factor
shc
Grb
SOS
RAS
BRAF
growth factor
tyrosine kinase
B raf inhibitors
MEKCancercellnucleus ERK
DNAtranscription
MEK inhibitors
B raf MutationB raf Mutation• Found in 50% of cutaneous melanomas
– Most commonly V600 E B raf mutation
R lt i b tit ti f l t i id f• Results in a substitution of glutamic acid for valine at codon 600
– May also have a B raf V 600K and B raf V 600R
– Present in the entire spectrum of melanoma (primary to mets)
Activating mutation– Activating mutation
– Translocates to mitochondria where it binds to and inactivates Bad
• Net effect is to decrease melanoma apoptosis
17
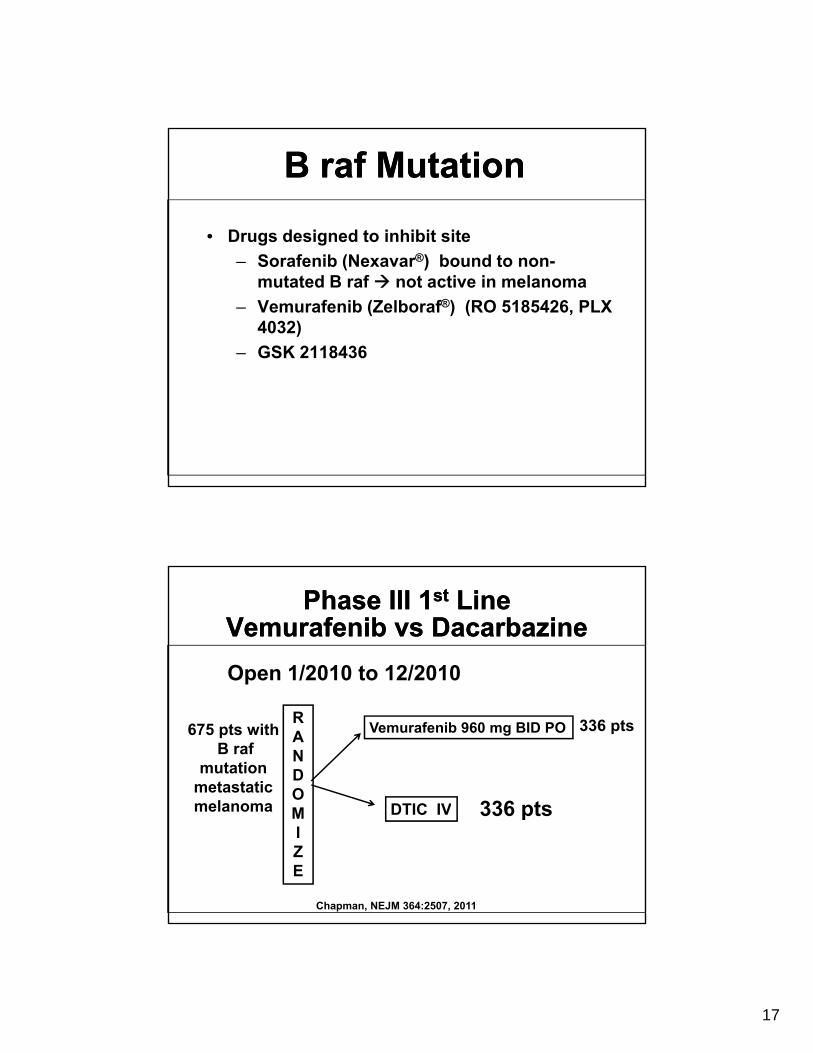
B raf MutationB raf Mutation
• Drugs designed to inhibit site
– Sorafenib (Nexavar®) bound to non-mutated B raf not active in melanoma
– Vemurafenib (Zelboraf®) (RO 5185426, PLX 4032)
– GSK 2118436
Phase III 1st Line Vemurafenib vs Dacarbazine
Phase III 1st Line Vemurafenib vs Dacarbazine
Open 1/2010 to 12/2010
RANDO
Vemurafenib 960 mg BID PO
DTIC IV
675 pts withB raf
mutationmetastatic melanoma
336 pts
336 ptsMIZE
DTIC IV
Chapman, NEJM 364:2507, 2011
melanoma 336 pts
18
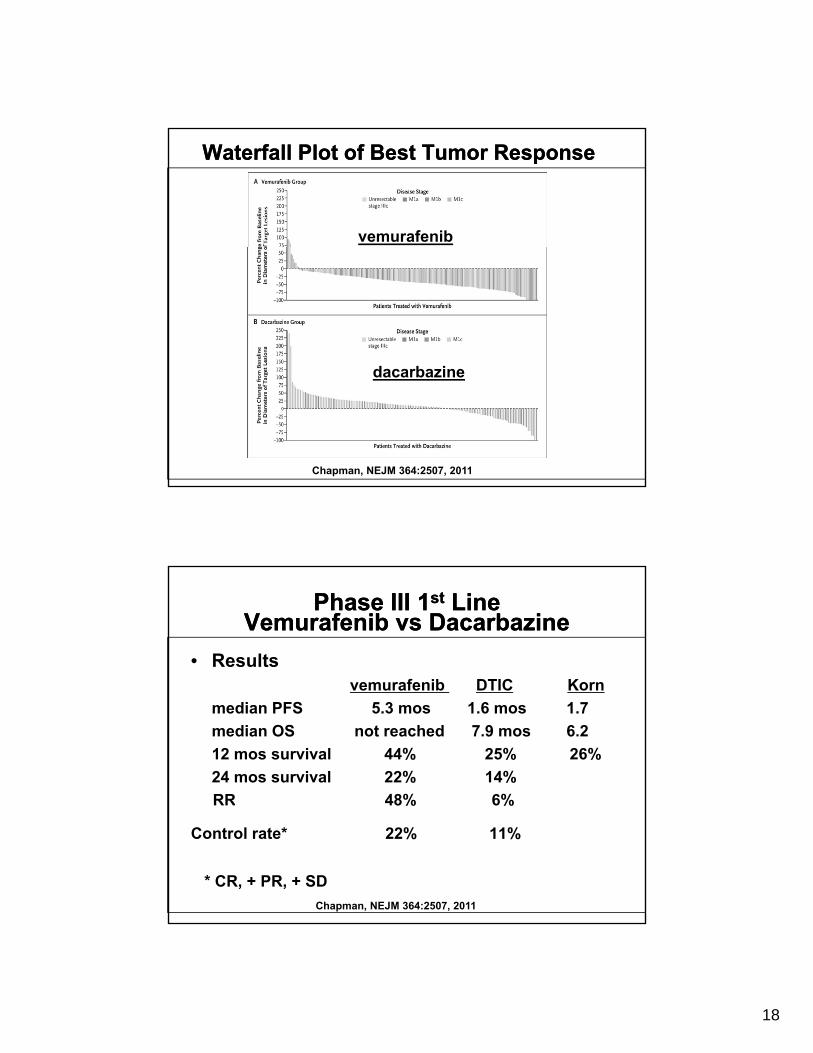
vemurafenib
Waterfall Plot of Best Tumor Response Waterfall Plot of Best Tumor Response
d b idacarbazine
Chapman, NEJM 364:2507, 2011
Phase III 1st Line Vemurafenib vs Dacarbazine
Phase III 1st Line Vemurafenib vs Dacarbazine
• Results vemurafenib DTIC Kornvemurafenib DTIC Korn
median PFS 5.3 mos 1.6 mos 1.7
median OS not reached 7.9 mos 6.2
12 mos survival 44% 25% 26%
24 mos survival 22% 14%
RR 48% 6%RR 48% 6%
Control rate* 22% 11%
* CR, + PR, + SD
Chapman, NEJM 364:2507, 2011
19
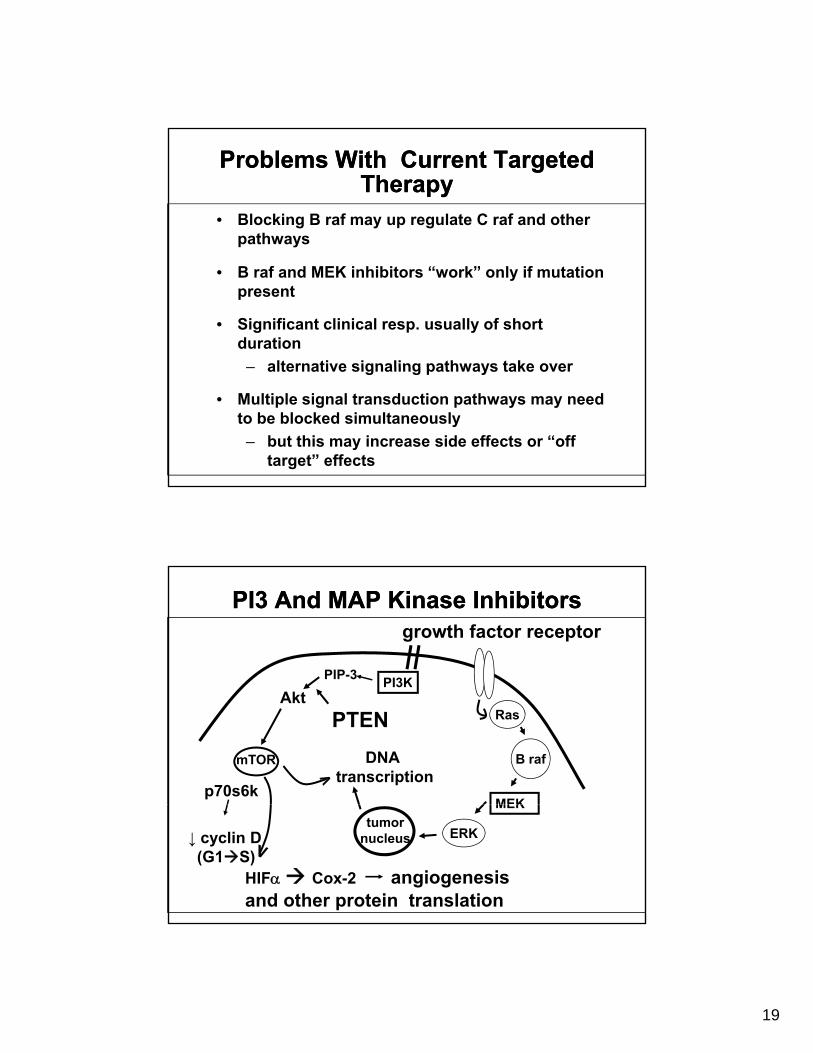
Problems With Current Targeted Therapy
Problems With Current Targeted Therapy
• Blocking B raf may up regulate C raf and other pathways
• B raf and MEK inhibitors “work” only if mutation present
• Significant clinical resp. usually of short duration
– alternative signaling pathways take over– alternative signaling pathways take over
• Multiple signal transduction pathways may need to be blocked simultaneously
– but this may increase side effects or “off target” effects
PI3 And MAP Kinase InhibitorsPI3 And MAP Kinase Inhibitors
PI3KPIP-3
growth factor receptor
PI3KAkt
mTOR
p70s6k
Ras
B raf
MEK
PTEN
DNAtranscription
↓ cyclin D(G1S)
HIF Cox-2 angiogenesisand other protein translation
MEK
ERKtumor
nucleus
20
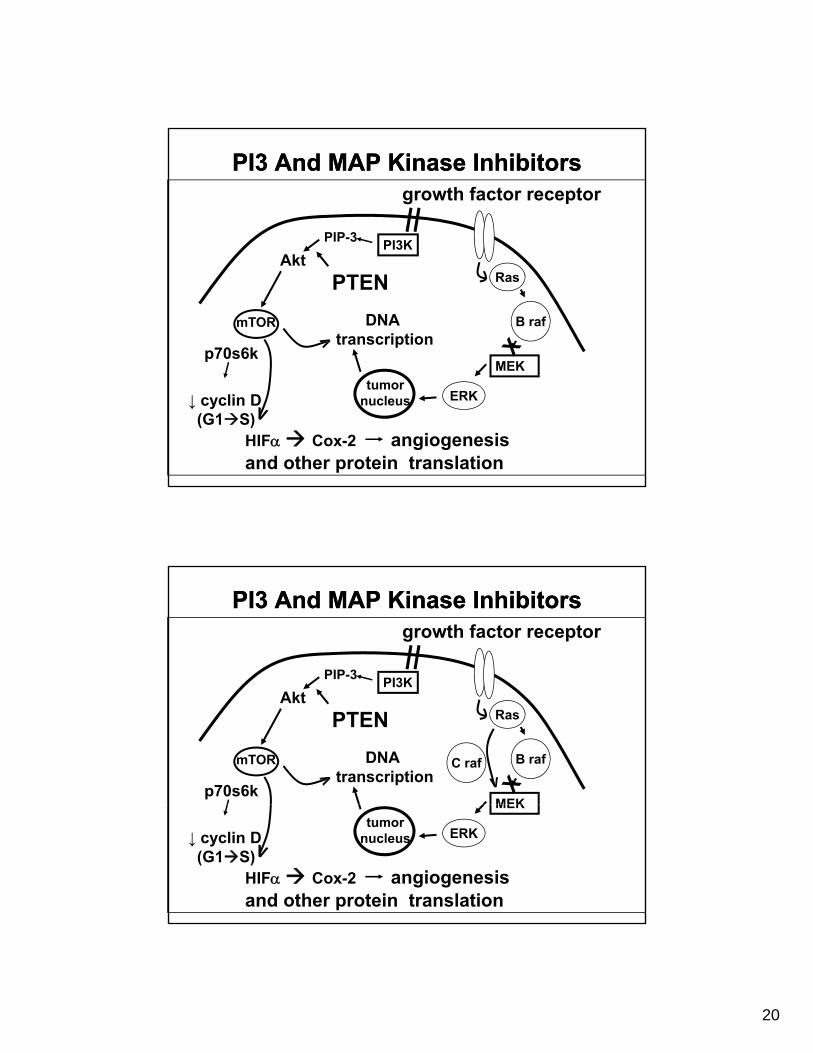
PI3 And MAP Kinase InhibitorsPI3 And MAP Kinase Inhibitors
PI3KPIP-3
growth factor receptor
PI3KAkt
mTOR
p70s6k
Ras
B raf
MEK
PTEN
DNAtranscription
↓ cyclin D(G1S)
HIF Cox-2 angiogenesisand other protein translation
MEK
ERKtumor
nucleus
PI3 And MAP Kinase InhibitorsPI3 And MAP Kinase Inhibitors
PI3KPIP-3
growth factor receptor
PI3KAkt
mTOR
p70s6k
Ras
B raf
MEK
PTEN
DNAtranscription
C raf
↓ cyclin D(G1S)
HIF Cox-2 angiogenesisand other protein translation
MEK
ERKtumor
nucleus
21
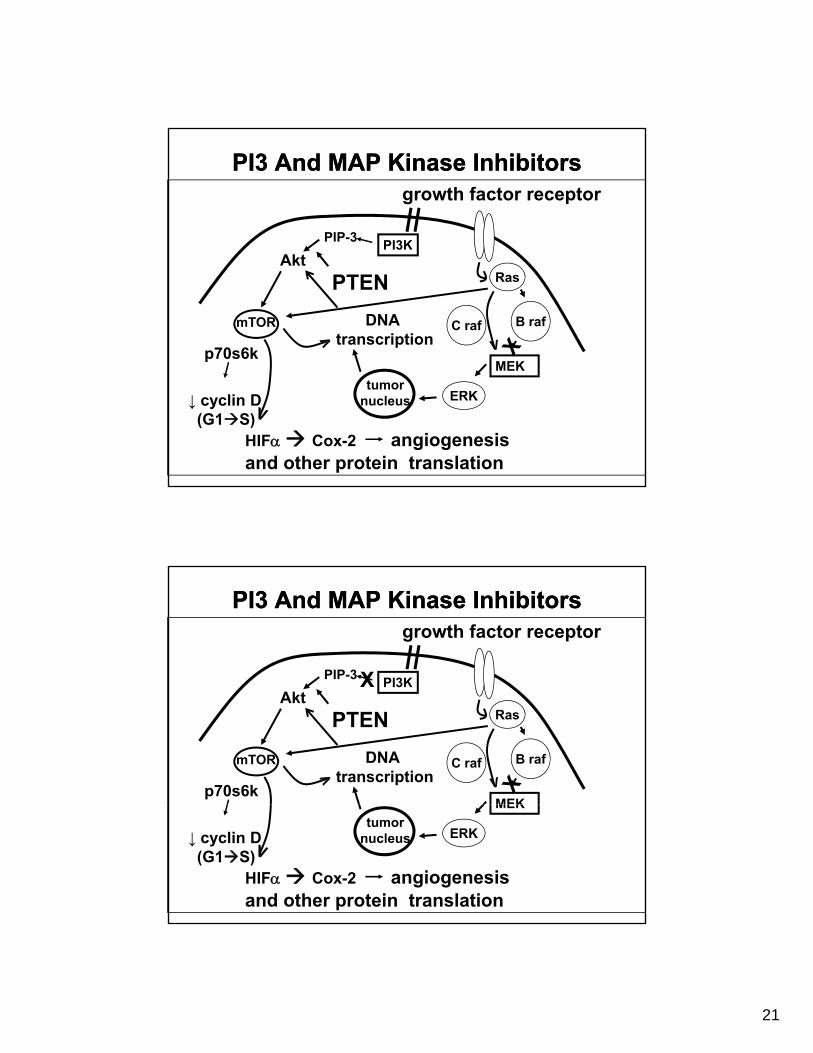
PI3 And MAP Kinase InhibitorsPI3 And MAP Kinase Inhibitors
PI3KPIP-3
growth factor receptor
PI3KAkt
mTOR
p70s6k
Ras
B raf
MEK
PTEN
DNAtranscription
C raf
↓ cyclin D(G1S)
HIF Cox-2 angiogenesisand other protein translation
MEK
ERKtumor
nucleus
PI3 And MAP Kinase InhibitorsPI3 And MAP Kinase Inhibitors
PI3KPIP-3
growth factor receptor
X PI3KAkt
mTOR
p70s6k
X
Ras
B raf
MEK
PTEN
DNAtranscription
C raf
↓ cyclin D(G1S)
HIF Cox-2 angiogenesisand other protein translation
MEK
ERKtumor
nucleus
22
So, what is all the news about?
ASCO 2010Sunday June 6, 2010
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
23
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
24
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag
CD 80 B 7.1CD 86 B 7.2
25
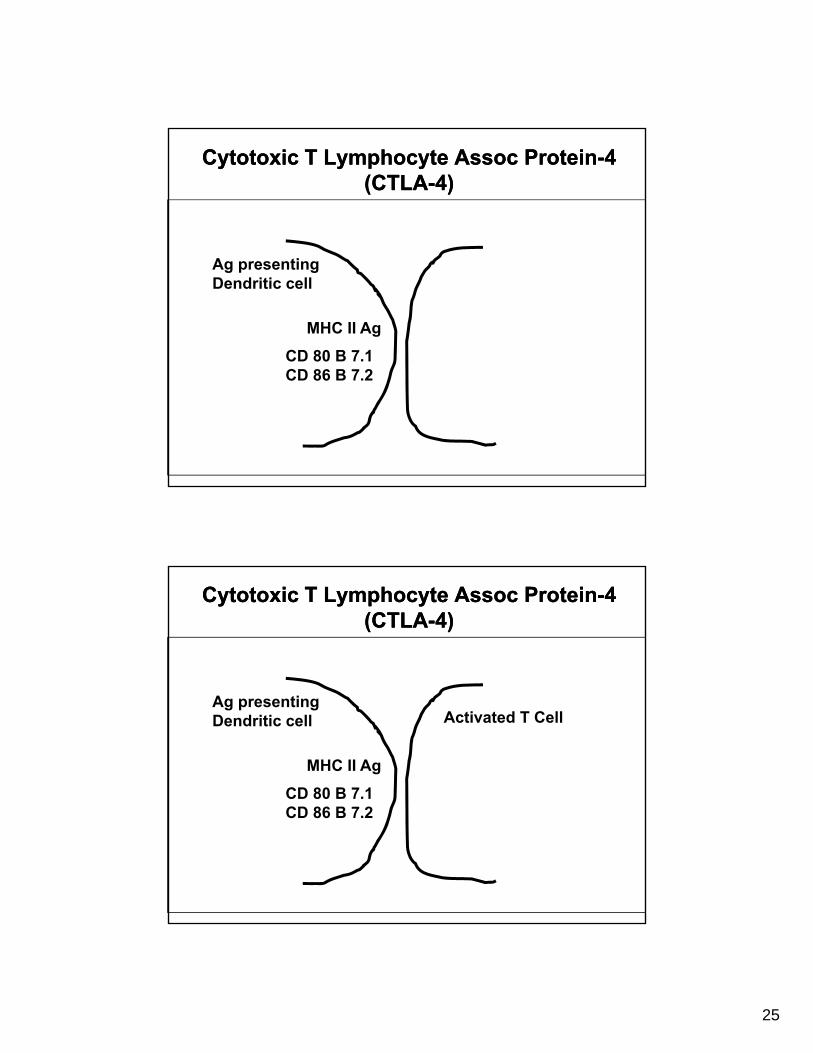
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag
CD 80 B 7.1CD 86 B 7.2
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag
CD 80 B 7.1
Activated T Cell
CD 86 B 7.2
26
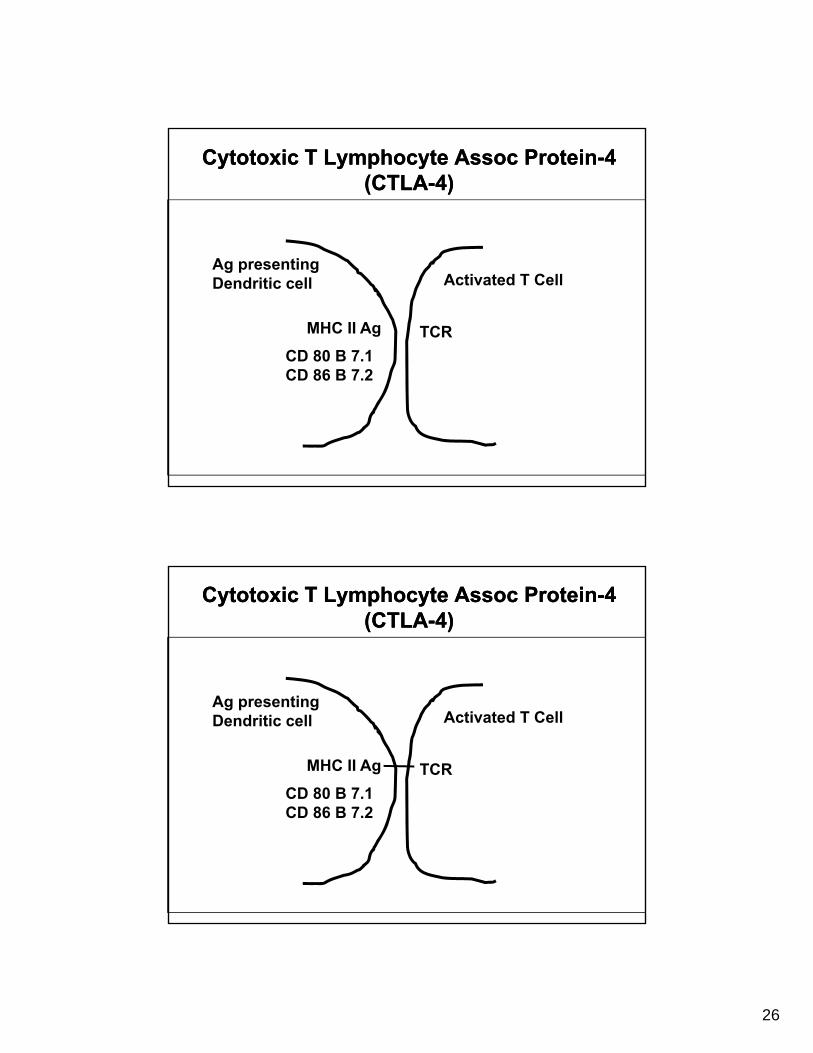
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCR
CD 80 B 7.1
Activated T Cell
CD 86 B 7.2
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCR
CD 80 B 7.1
Activated T Cell
CD 86 B 7.2
27
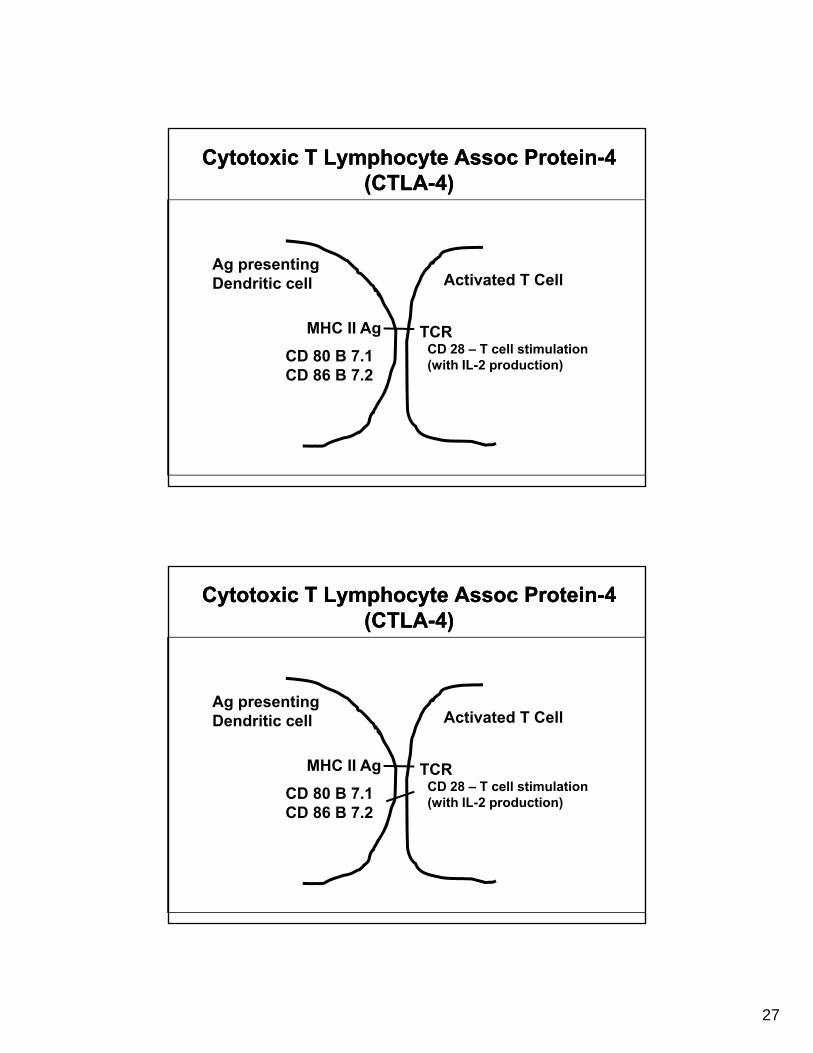
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – T cell stimulation (with IL-2 production)
CD 80 B 7.1
Activated T Cell
(with IL 2 production)CD 86 B 7.2
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – T cell stimulation (with IL-2 production)
CD 80 B 7.1
Activated T Cell
(with IL 2 production)CD 86 B 7.2
28
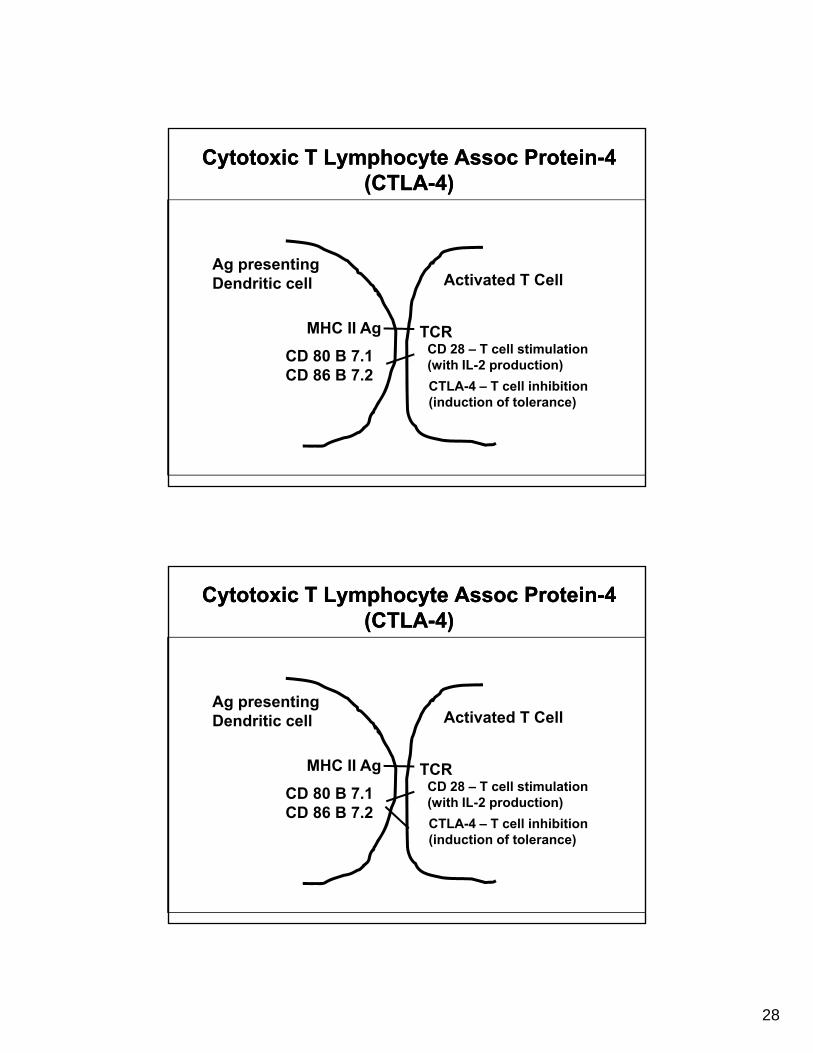
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – T cell stimulation (with IL-2 production)
CD 80 B 7.1
Activated T Cell
(with IL 2 production)CD 86 B 7.2
CTLA-4 – T cell inhibition (induction of tolerance)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – T cell stimulation (with IL-2 production)
CD 80 B 7.1
Activated T Cell
(with IL 2 production)CD 86 B 7.2
CTLA-4 – T cell inhibition (induction of tolerance)
29
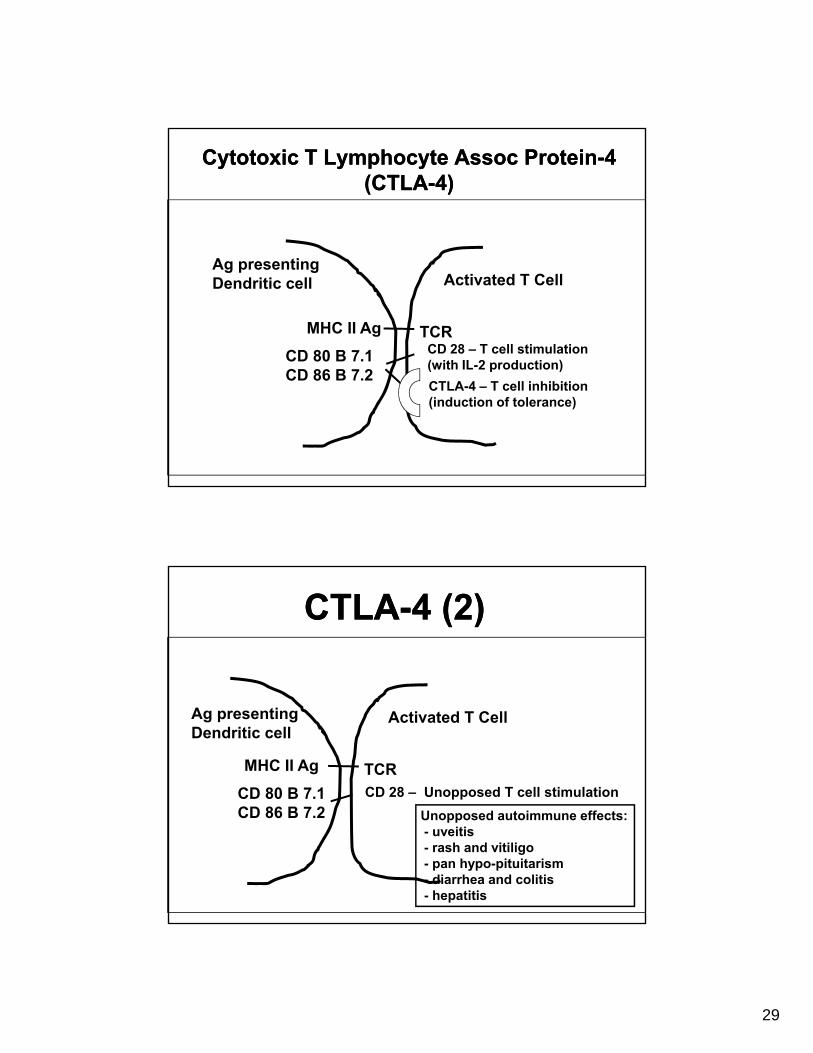
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Cytotoxic T Lymphocyte Assoc Protein-4 (CTLA-4)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – T cell stimulation (with IL-2 production)
CD 80 B 7.1
Activated T Cell
(with IL 2 production)CD 86 B 7.2
CTLA-4 – T cell inhibition (induction of tolerance)
CTLA-4 (2)CTLA-4 (2)
Ag presentingDendritic cell
MHC II Ag TCRCD 28 – Unopposed T cell stimulationCD 80 B 7.1
Activated T Cell
CD 86 B 7.2 Unopposed autoimmune effects:- uveitis- rash and vitiligo- pan hypo-pituitarism - diarrhea and colitis- hepatitis
30
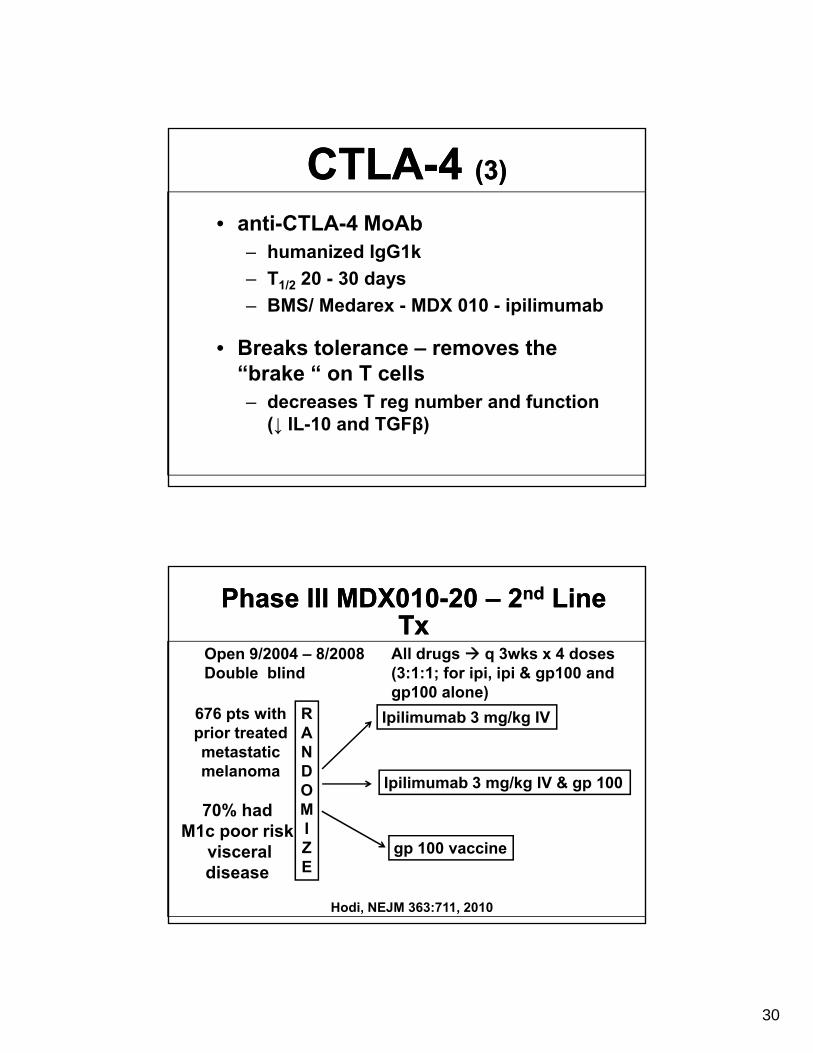
CTLA-4 (3)CTLA-4 (3)
• anti-CTLA-4 MoAbh i d I G1k– humanized IgG1k
– T1/2 20 - 30 days
– BMS/ Medarex - MDX 010 - ipilimumab
• Breaks tolerance – removes the “b k “ T ll“brake “ on T cells– decreases T reg number and function
(↓ IL-10 and TGFβ)
Phase III MDX010-20 – 2nd Line Tx
Phase III MDX010-20 – 2nd Line Tx
Open 9/2004 – 8/2008Double blind
All drugs q 3wks x 4 doses(3:1:1; for ipi, ipi & gp100 and
RANDOM
Ipilimumab 3 mg/kg IV
Ipilimumab 3 mg/kg IV & gp 100
gp100 alone)676 pts with prior treatedmetastatic melanoma
70% h d MIZE
Hodi, NEJM 363:711, 2010
70% hadM1c poor risk
visceral disease
gp 100 vaccine
31
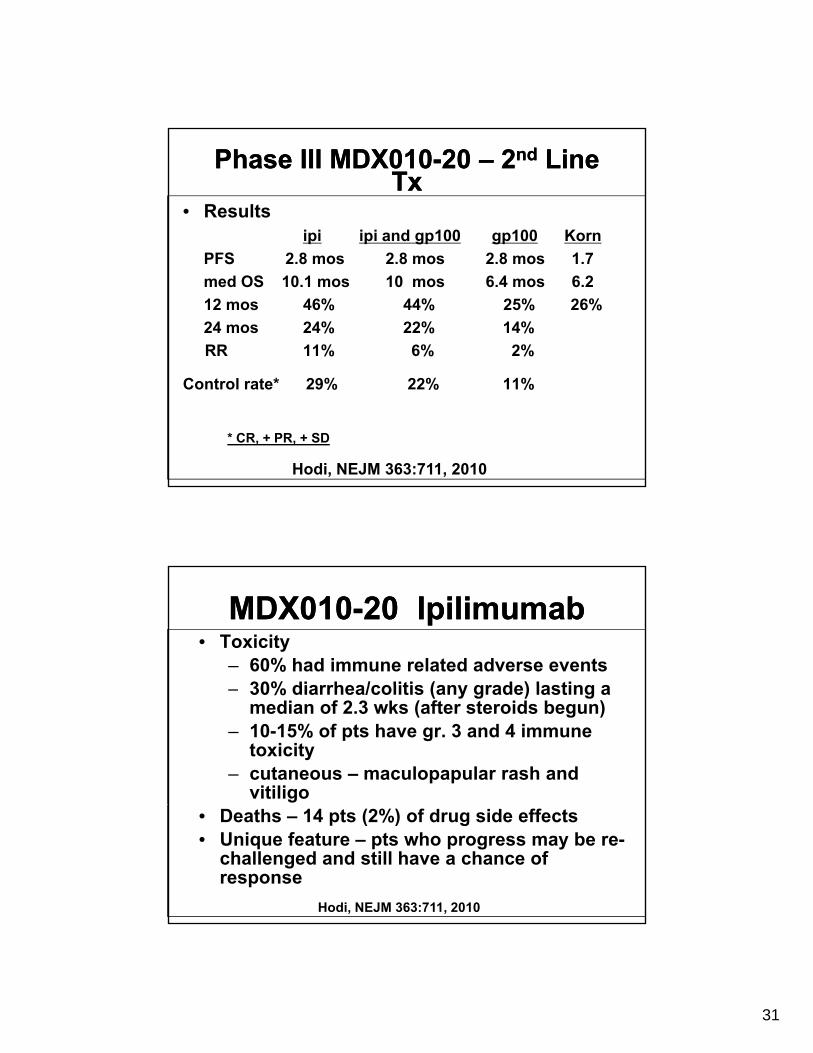
Phase III MDX010-20 – 2nd Line Tx
Phase III MDX010-20 – 2nd Line Tx
• Results ipi ipi and gp100 gp100 Korn
PFS 2.8 mos 2.8 mos 2.8 mos 1.7
med OS 10.1 mos 10 mos 6.4 mos 6.2
12 mos 46% 44% 25% 26%
24 mos 24% 22% 14%
RR 11% 6% 2%
Control rate* 29% 22% 11%
* CR, + PR, + SD
Hodi, NEJM 363:711, 2010
MDX010-20 IpilimumabMDX010-20 Ipilimumab• Toxicity
– 60% had immune related adverse events30% diarrhea/colitis (an grade) lasting a– 30% diarrhea/colitis (any grade) lasting a median of 2.3 wks (after steroids begun)
– 10-15% of pts have gr. 3 and 4 immune toxicity
– cutaneous – maculopapular rash and vitiligo
• Deaths – 14 pts (2%) of drug side effects• Unique feature – pts who progress may be re-
challenged and still have a chance of response
Hodi, NEJM 363:711, 2010
32
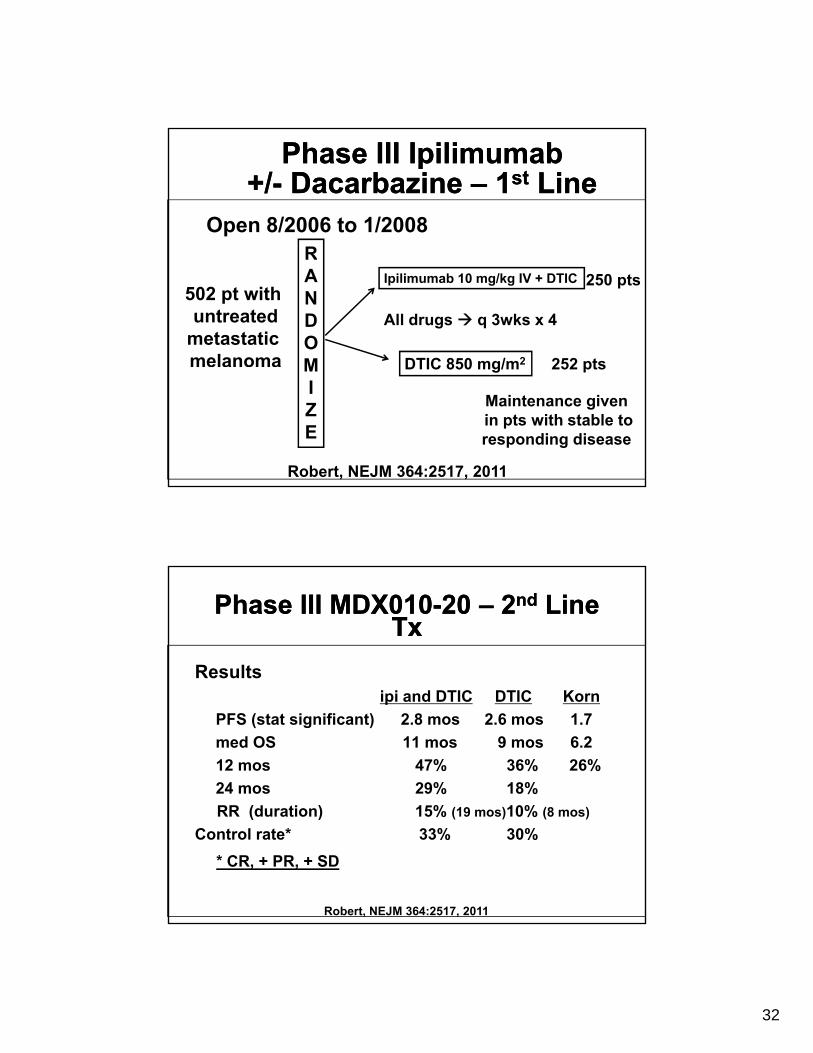
Phase III Ipilimumab +/- Dacarbazine – 1st Line
Phase III Ipilimumab +/- Dacarbazine – 1st Line
R
Open 8/2006 to 1/2008RANDOM
Ipilimumab 10 mg/kg IV + DTIC
DTIC 850 mg/m2
250 pts
252 pts
All drugs q 3wks x 4
502 pt with untreated
metastatic melanoma M
IZE
DTIC 850 mg/m 252 pts
Robert, NEJM 364:2517, 2011
Maintenance givenin pts with stable to responding disease
Phase III MDX010-20 – 2nd Line Tx
Phase III MDX010-20 – 2nd Line Tx
Results ipi and DTIC DTIC Korn
PFS (stat significant) 2.8 mos 2.6 mos 1.7
med OS 11 mos 9 mos 6.2
12 mos 47% 36% 26%
24 mos 29% 18%
RR (duration) 15% (19 mos)10% (8 mos)
Control rate* 33% 30%
* CR, + PR, + SD
Robert, NEJM 364:2517, 2011
33
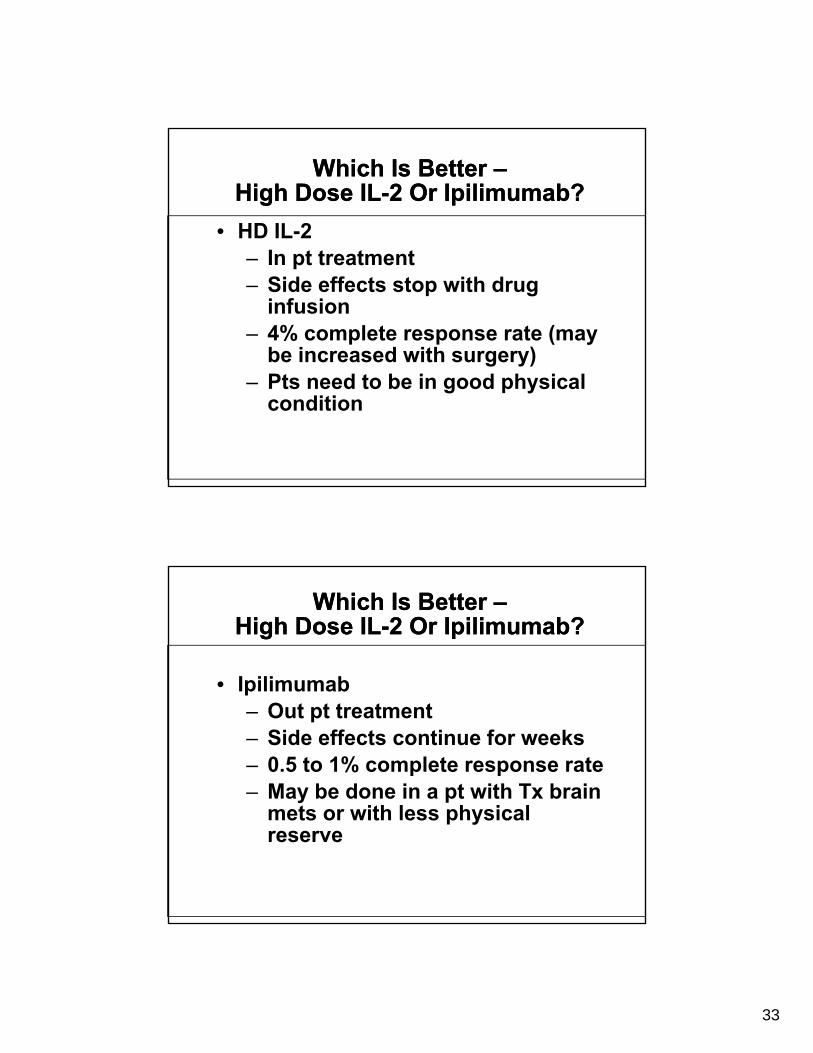
Which Is Better –High Dose IL-2 Or Ipilimumab?
Which Is Better –High Dose IL-2 Or Ipilimumab?
• HD IL-2– In pt treatment– Side effects stop with drug
infusion– 4% complete response rate (may
be increased with surgery)– Pts need to be in good physical
condition
Which Is Better –High Dose IL-2 Or Ipilimumab?
Which Is Better –High Dose IL-2 Or Ipilimumab?
• Ipilimumab• Ipilimumab– Out pt treatment– Side effects continue for weeks– 0.5 to 1% complete response rate– May be done in a pt with Tx brain
mets or with less physical reserve
34
ConclusionsConclusions• Because of short response and short survival
upon progression, B raf inhibitors will need to be given in combination or sequentially with be g e co b at o o seque t a y tother drugs
• Uncertainty remains – re the effect of dacarbazine given in
combination with ipi– whether ipi should be given 1st or 2 nd line
h th i i h ld b i i bi ti– whether ipi should be given in combination or sequentially with other drugs
• As optimal therapy remains lacking, pts should be treated on clinical trials as much as possible
Signs and Signs and gsymptoms of
recurrent melanoma
gsymptoms of
recurrent melanomamelanomamelanoma

35
Skin cancer Skin cancer prevention: Advice for patients
prevention: Advice for patientspatientspatients
Immuno-Immuno-Immuno-suppression and
skin cancer
Immuno-suppression and
skin cancer
36
Squamous cell carcinoma and
basal cell
Squamous cell carcinoma and
basal cellbasal cell carcinoma: the
role of the
basal cell carcinoma: the
role of the medical
oncologistmedical
oncologist
© The Ohio State University Medical Center, 2011© The Ohio State University Medical Center, 2011
37
Today’s Poll ResultsToday’s Poll Results
poll results will continue to be tabulated
poll results will continue to be tabulated
POLLINGPOLLING
To take the post test, please return to your account at ccme.osu.eduTo take the post test, please return to your account at ccme.osu.edu
Be sure to refresh (f5)
38
Skin CancerSkin Cancer





![[Also please see corrected entry at 2005-Ohio-62.] · [Also please see corrected entry at 2005-Ohio-62.] ... Detective Prochazka contacted Murton and Carter to discuss the ... banking](https://img.pdfslide.net/doc/110x75/5af143647f8b9a8c308e42f5/also-please-see-corrected-entry-at-2005-ohio-62-also-please-see-corrected-entry.jpg)




![[Vacated opinion. Please see 2017-Ohio-7727.]...2017-Ohio-4066.] [Vacated opinion. Please see 2017-Ohio-7727.] IN THE COURT OF APPEALS OF OHIO EIGHTH APPELLATE DISTRICT CUYAHOGA COUNTY](https://img.pdfslide.net/doc/110x75/5f61b87695ee716ead3e6859/vacated-opinion-please-see-2017-ohio-7727-2017-ohio-4066-vacated-opinion.jpg)

![[Please see vacated opinion at 2014-Ohio-5271.] … · [Please see vacated opinion at 2014-Ohio-5271.] ... Dr. Daniel Galita, a medical examiner in the Cuyahoga County Coroner’s](https://img.pdfslide.net/doc/110x75/5b942d2009d3f2130d8c2858/please-see-vacated-opinion-at-2014-ohio-5271-please-see-vacated-opinion.jpg)



![[Vacated opinion. Please see 2011-Ohio-2778.] Court of ...€¦ · [Cite as Johnson v.Cleveland City School Dist., 2011-Ohio-1917.] [Vacated opinion. Please see 2011-Ohio-2778.] Court](https://img.pdfslide.net/doc/110x75/603782b6cd803400ea07e545/vacated-opinion-please-see-2011-ohio-2778-court-of-cite-as-johnson-vcleveland.jpg)












