Embed Size (px)
Citation preview
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 1
ODESA NATIONAL MEDICAL UNIVERSITY
Department of Internal medicine №1 with the cardiovascular pathology course
APPROVED by
Head of department
_________(prof. Karpenko I.I)
“27” September 2021
METHODOLOGICAL RECOMMENDATION ON THE LECTURE
Course: IV Faculty: International
Academic discipline “Endocrinology”
Lecture №01 Topic “Diabetes mellitus. Modern classification, etiology,
pathogenesis, symptoms, diagnosis. Chronic complications of Diabetes”
Odesa – 2021 y.
The lecture was created by
Assistant
___________ (Blikhar O.V.)
The lecture was discussed at
the methodical meeting of the
department
«27» September 2021 y.
Protocol № 2.
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 2
Lecture № 01
Topic: “Diabetes mellitus. Modern classification, etiology, pathogenesis,
symptoms, diagnosis. Chronic complications of Diabetes”
The goals of the lecture : explain the essence of the Diabetes mellitus, causes, role
in the etiopathogenesis of various factors, approaches to diagnosis and prevention.
Specific objectives of the lecture:
- give a modern definition of Diabetes mellitus;
- present generalized and systematized material on etiopathogenesis based on the
results of modern controlled clinical trials;
- present the basic concepts of classification, clinical features and diagnostic
approaches;
- to determine the basic principles of differential diagnosis with further substantiation
of final diagnosis based on the analysis of patient complaints, anamnesis, physical
symptoms, laboratory and instrumental examination data;
- explain the principles of treatment of Diabetes mellitus provided by national clinical
guidelines;
- to present modern methods of determining the prognosis and expert assessment of
the patient's ability to work based on the recommendations of the Ministry of Health
of Ukraine;
- to demonstrate the principles of medical ethics and deontology, to promote the
formation of a professionally significant structure of the doctor's personality on the
example of the peculiarities of working with patients.
Key words: Diabetes mellitus, hyperglycemia, autoimmune disease, obesity, HbA1c,
oral glucose tolerance test
Lecture plan and organizational structure
№ The main stages of the lecture
and their content
Goals in
levels of
abstraction
Type of lecture,
methods and means
of activating
students, equipment
Time
distribution
І
1.
2.
Preparatory stage
Setting a learning goal
Providing positive motivation
І
І
In accordance with
the publication
"Guidelines for
planning,
preparation and
analysis of lectures"
5%
(5 min)
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 3
ІІ
3.
The main stage
Teaching lecture material
according to the plan:
1. Relevance of the topic
2. Definition
3. Classification
4. Etiology and main links of
pathogenesis
5. Symptoms and signs
6. Diagnostic criteria
7. Main syndromes and
differential diagnosis
8. Criteria for the severity of
disease
9. Treatment
10. Prevention
ІІ
ІІ
ІІ
ІІ
ІІ
ІІ
ІІ
ІІ
ІІ
ІІ
Slide presentation of
lecture material
Extracts from
medical histories of
patients. Excerpts
from clinical
protocols of the
Ministry of Health
of Ukraine for the
provision of medical
care to patients.
85%
(75 min)
ІІІ
4.
5.
6.
The final stage
Lecture summary, general
conclusions
Answers to possible questions
Tasks for self-training
ІІІ
ІІІ
ІІІ
References,
questions, tasks
10%
(10 min)
Content of the lecture
Diabetes is a chronic disease that occurs either when the pancreas does not
produce enough insulin or when the body cannot effectively use the insulin it
produces. Insulin is a hormone that regulates blood sugar. Hyperglycaemia, or raised
blood sugar, is a common effect of uncontrolled diabetes and over time leads to
serious damage to many of the body's systems, especially the nerves and blood
vessels.
In 2014, 8.5% of adults aged 18 years and older had diabetes. In 2019, diabetes was
the direct cause of 1.5 million deaths. To present a more accurate picture of the
deaths causes by diabetes, however, deaths due to higher-than-optimal blood glucose
through cardiovascular disease, chronic kidney disease and tuberculosis should be
added. In 2012 (year of the latest available data), there were another 2.2 million
deaths due to high blood glucose.
Between 2000 and 2016, there was a 5% increase in premature mortality from
diabetes. In high-income countries the premature mortality rate due to diabetes
decreased from 2000 to 2010 but then increased in 2010-2016. In lower-middle-
income countries, the premature mortality rate due to diabetes increased across both
periods.
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 4
By contrast, the probability of dying from any one of the four main
noncommunicable diseases (cardiovascular diseases, cancer, chronic respiratory
diseases or diabetes) between the ages of 30 and 70 decreased by 18% globally
between 2000 and 2016.
Diabetes is a complex, chronic illness requiring continuous medical care with
multifactorial risk-reduction strategies beyond glycemic control. Ongoing diabetes
self-management education and support are critical to preventing acute complications
and reducing the risk of long-term complications. Significant evidence exists that
supports a range of interventions to improve diabetes outcomes.
Classification
Diabetes can be classified into the following general categories:
1. Type 1 diabetes (due to autoimmune β-cell destruction, usually leading to absolute
insulin deficiency, including latent autoimmune diabetes of adulthood)
2. Type 2 diabetes (due to a progressive loss of adequate β-cell insulin secretion
frequently on the background of insulin resistance)
3. Specific types of diabetes due to other causes, e.g., monogenic diabetes syndromes
(such as neonatal diabetes and maturity-onset diabetes of the young), diseases of the
exocrine pancreas (such as cystic fibrosis and pancreatitis), and drug- or chemical-
induced diabetes (such as with glucocorticoid use, in the treatment of HIV/AIDS, or
after organ transplantation)
4. Gestational diabetes mellitus (diabetes diagnosed in the second or third trimester of
pregnancy that was not clearly overt diabetes prior to gestation)
Type 1 Diabetes
This form, previously called “insulin-dependent diabetes” or “juvenile-onset
diabetes,” accounts for 5–10% of diabetes and is due to cellular-mediated
autoimmune destruction of the pancreatic β-cells. Autoimmune markers include islet
cell autoantibodies and autoantibodies to GAD (GAD65), insulin, the tyrosine
phosphatases IA-2 and IA-2β, and zinc transporter 8 (ZnT8).
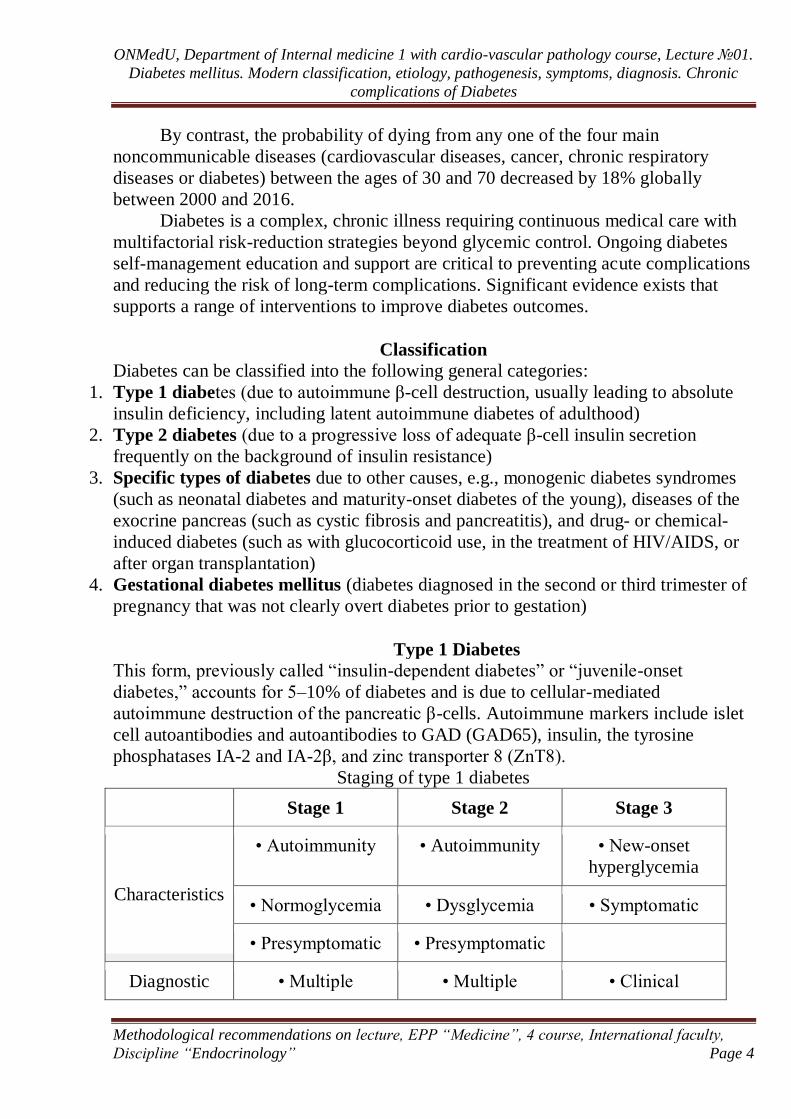
Staging of type 1 diabetes
Stage 1 Stage 2 Stage 3
Characteristics
• Autoimmunity • Autoimmunity • New-onset
hyperglycemia
• Normoglycemia • Dysglycemia • Symptomatic
• Presymptomatic • Presymptomatic
Diagnostic • Multiple • Multiple • Clinical
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 5
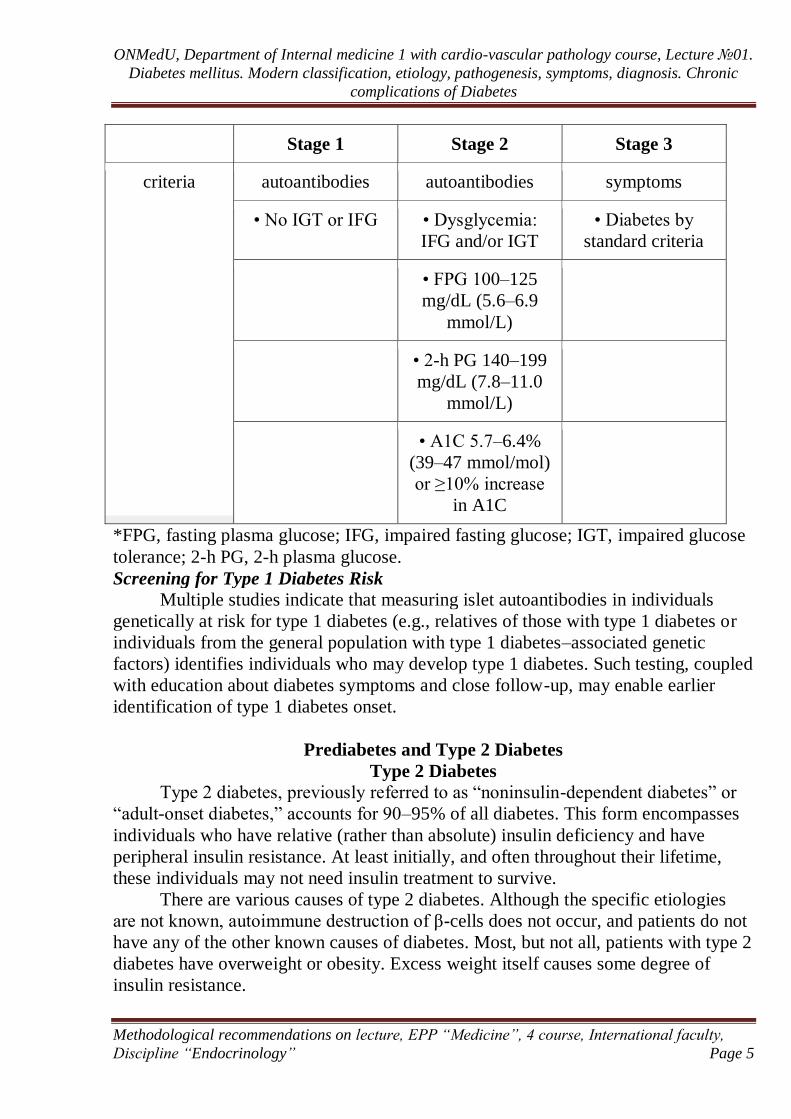
Stage 1 Stage 2 Stage 3
criteria autoantibodies autoantibodies symptoms
• No IGT or IFG • Dysglycemia:
IFG and/or IGT
• Diabetes by
standard criteria
• FPG 100–125
mg/dL (5.6–6.9
mmol/L)
• 2-h PG 140–199
mg/dL (7.8–11.0
mmol/L)
• A1C 5.7–6.4%
(39–47 mmol/mol)
or ≥10% increase
in A1C
*FPG, fasting plasma glucose; IFG, impaired fasting glucose; IGT, impaired glucose
tolerance; 2-h PG, 2-h plasma glucose.
Screening for Type 1 Diabetes Risk
Multiple studies indicate that measuring islet autoantibodies in individuals
genetically at risk for type 1 diabetes (e.g., relatives of those with type 1 diabetes or
individuals from the general population with type 1 diabetes–associated genetic
factors) identifies individuals who may develop type 1 diabetes. Such testing, coupled
with education about diabetes symptoms and close follow-up, may enable earlier
identification of type 1 diabetes onset.
Prediabetes and Type 2 Diabetes
Type 2 Diabetes
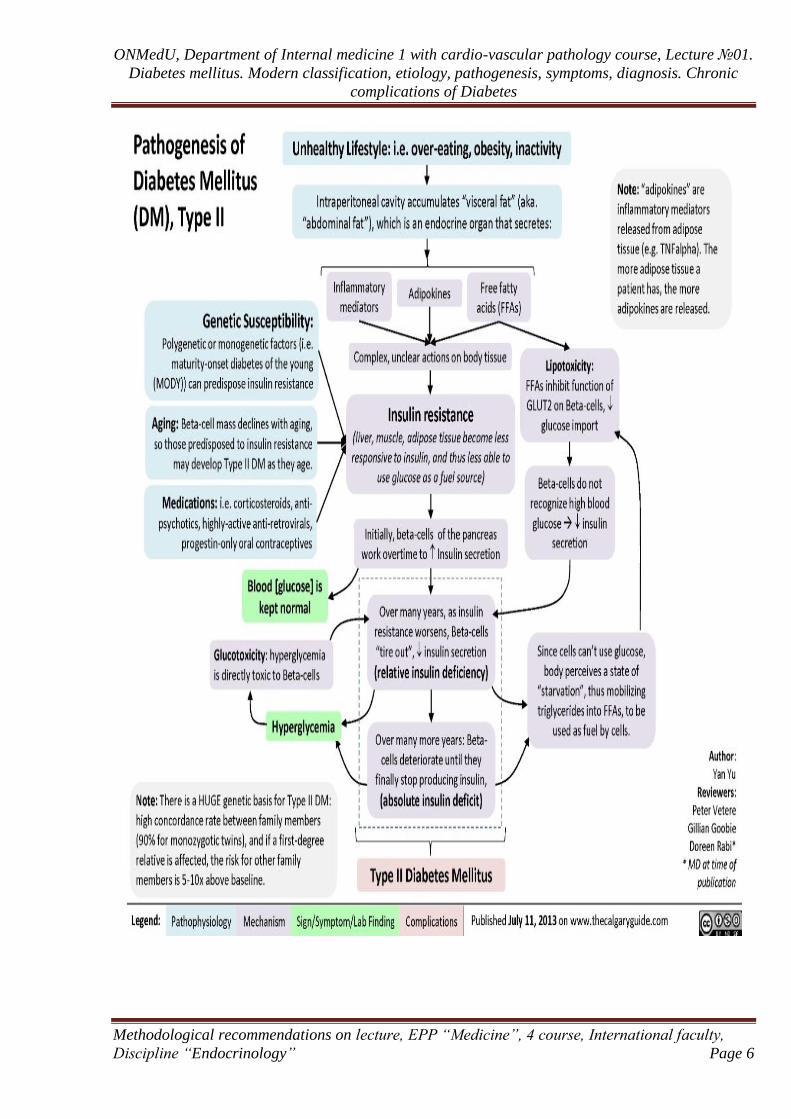
Type 2 diabetes, previously referred to as “noninsulin-dependent diabetes” or
“adult-onset diabetes,” accounts for 90–95% of all diabetes. This form encompasses
individuals who have relative (rather than absolute) insulin deficiency and have
peripheral insulin resistance. At least initially, and often throughout their lifetime,
these individuals may not need insulin treatment to survive.
There are various causes of type 2 diabetes. Although the specific etiologies
are not known, autoimmune destruction of β-cells does not occur, and patients do not
have any of the other known causes of diabetes. Most, but not all, patients with type 2
diabetes have overweight or obesity. Excess weight itself causes some degree of
insulin resistance.
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 6
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 7
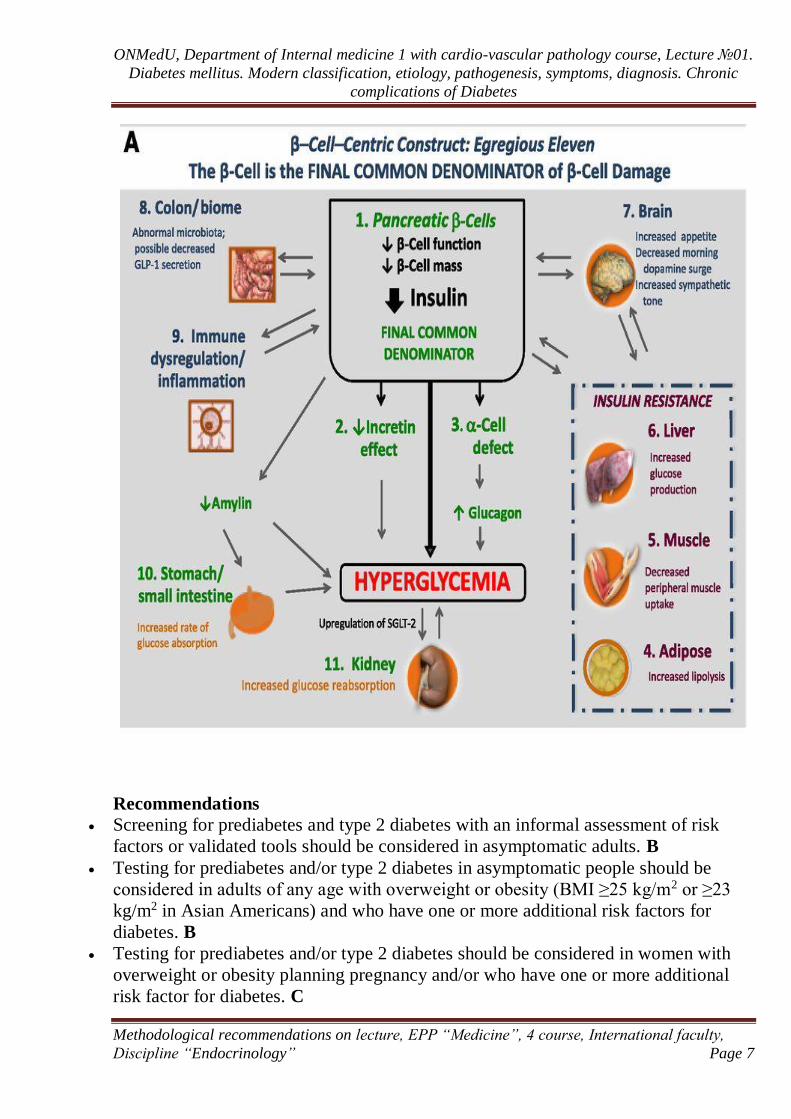
Recommendations
Screening for prediabetes and type 2 diabetes with an informal assessment of risk
factors or validated tools should be considered in asymptomatic adults. B
Testing for prediabetes and/or type 2 diabetes in asymptomatic people should be
considered in adults of any age with overweight or obesity (BMI ≥25 kg/m2 or ≥23
kg/m2 in Asian Americans) and who have one or more additional risk factors for
diabetes. B
Testing for prediabetes and/or type 2 diabetes should be considered in women with
overweight or obesity planning pregnancy and/or who have one or more additional
risk factor for diabetes. C
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 8
For all people, testing should begin at age 45 years. B
If tests are normal, repeat testing carried out at a minimum of 3-year intervals is
reasonable, sooner with symptoms. C
To test for prediabetes and type 2 diabetes, fasting plasma glucose, 2-h plasma
glucose during 75-g oral glucose tolerance test, and A1C are equally appropriate B
In patients with prediabetes and type 2 diabetes, identify and treat other
cardiovascular disease risk factors. A
Risk-based screening for prediabetes and/or type 2 diabetes should be considered
after the onset of puberty or after 10 years of age, whichever occurs earlier, in
children and adolescents with overweight (BMI ≥85th percentile) or obesity (BMI
≥95th percentile) and who have one or more risk factor for diabetes. B
Patients with HIV should be screened for diabetes and prediabetes with a fasting
glucose test before starting antiretroviral therapy, at the time of switching
antiretroviral therapy, and 3−6 months after starting or switching antiretroviral
therapy. If initial screening results are normal, fasting glucose should be checked
annually. E
Criteria for testing for diabetes or prediabetes in asymptomatic adults
1. Testing should be considered in adults with overweight or obesity (BMI ≥25
kg/m2 or ≥23 kg/m2 in Asian Americans) who have one or more of the following
risk factors:
• First-degree relative with diabetes
• High-risk race/ethnicity (e.g., African American, Latino, Native American,
Asian American, Pacific Islander)
• History of CVD
• Hypertension (≥140/90 mmHg or on therapy for hypertension)
• HDL cholesterol level <35 mg/dL (0.90 mmol/L) and/or a triglyceride level
>250 mg/dL (2.82 mmol/L)
• Women with polycystic ovary syndrome
• Physical inactivity
• Other clinical conditions associated with insulin resistance (e.g., severe
obesity, acanthosis nigricans)
2. Patients with prediabetes (A1C ≥5.7% [39 mmol/mol], IGT, or IFG) should be
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 9
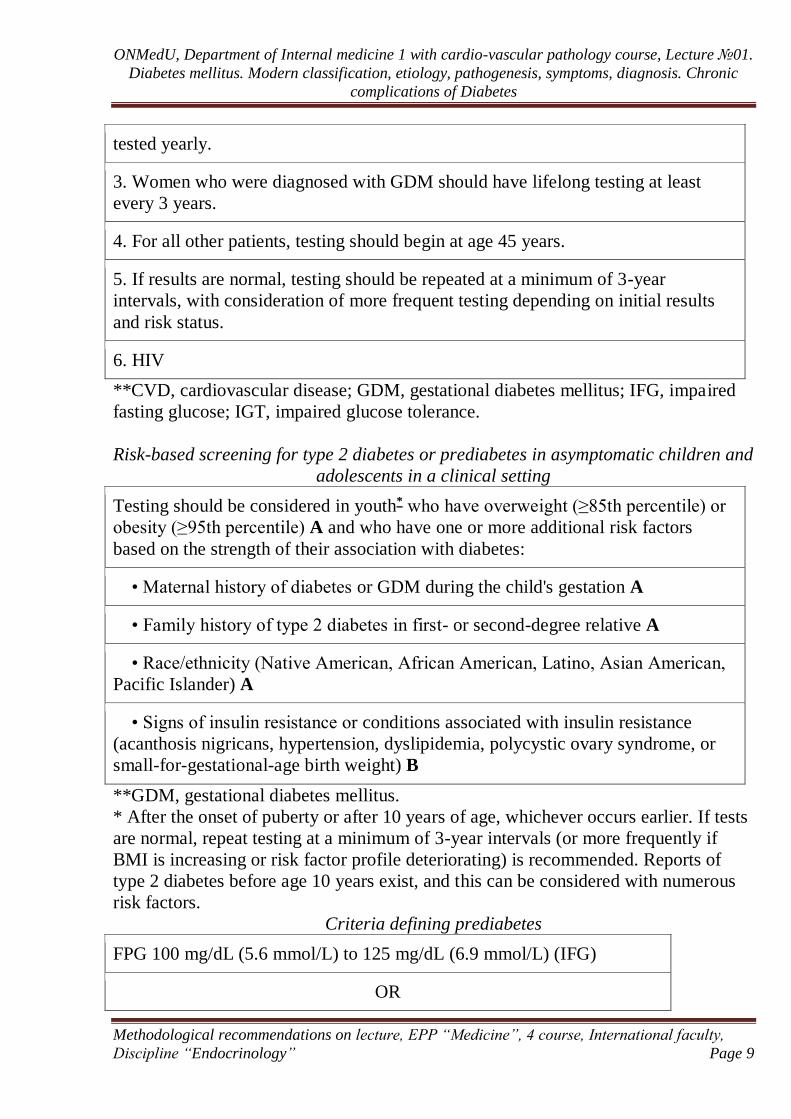
tested yearly.
3. Women who were diagnosed with GDM should have lifelong testing at least
every 3 years.
4. For all other patients, testing should begin at age 45 years.
5. If results are normal, testing should be repeated at a minimum of 3-year
intervals, with consideration of more frequent testing depending on initial results
and risk status.
6. HIV
**CVD, cardiovascular disease; GDM, gestational diabetes mellitus; IFG, impaired
fasting glucose; IGT, impaired glucose tolerance.
Risk-based screening for type 2 diabetes or prediabetes in asymptomatic children and
adolescents in a clinical setting
Testing should be considered in youth* who have overweight (≥85th percentile) or
obesity (≥95th percentile) A and who have one or more additional risk factors
based on the strength of their association with diabetes:
• Maternal history of diabetes or GDM during the child's gestation A
• Family history of type 2 diabetes in first- or second-degree relative A
• Race/ethnicity (Native American, African American, Latino, Asian American,
Pacific Islander) A
• Signs of insulin resistance or conditions associated with insulin resistance
(acanthosis nigricans, hypertension, dyslipidemia, polycystic ovary syndrome, or
small-for-gestational-age birth weight) B
**GDM, gestational diabetes mellitus.
* After the onset of puberty or after 10 years of age, whichever occurs earlier. If tests
are normal, repeat testing at a minimum of 3-year intervals (or more frequently if
BMI is increasing or risk factor profile deteriorating) is recommended. Reports of
type 2 diabetes before age 10 years exist, and this can be considered with numerous
risk factors.
Criteria defining prediabetes
FPG 100 mg/dL (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (IFG)
OR
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 10
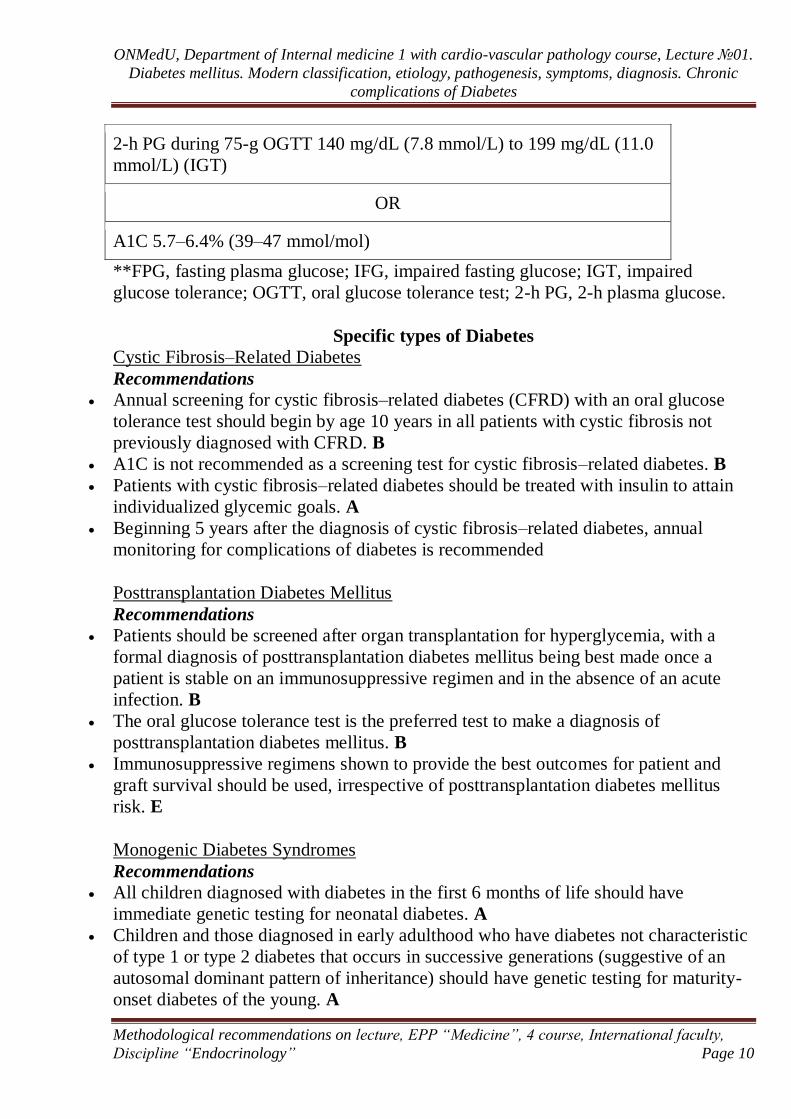
2-h PG during 75-g OGTT 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0
mmol/L) (IGT)
OR
A1C 5.7–6.4% (39–47 mmol/mol)
**FPG, fasting plasma glucose; IFG, impaired fasting glucose; IGT, impaired
glucose tolerance; OGTT, oral glucose tolerance test; 2-h PG, 2-h plasma glucose.
Specific types of Diabetes
Cystic Fibrosis–Related Diabetes
Recommendations
Annual screening for cystic fibrosis–related diabetes (CFRD) with an oral glucose
tolerance test should begin by age 10 years in all patients with cystic fibrosis not
previously diagnosed with CFRD. B
A1C is not recommended as a screening test for cystic fibrosis–related diabetes. B
Patients with cystic fibrosis–related diabetes should be treated with insulin to attain
individualized glycemic goals. A
Beginning 5 years after the diagnosis of cystic fibrosis–related diabetes, annual
monitoring for complications of diabetes is recommended
Posttransplantation Diabetes Mellitus
Recommendations
Patients should be screened after organ transplantation for hyperglycemia, with a
formal diagnosis of posttransplantation diabetes mellitus being best made once a
patient is stable on an immunosuppressive regimen and in the absence of an acute
infection. B
The oral glucose tolerance test is the preferred test to make a diagnosis of
posttransplantation diabetes mellitus. B
Immunosuppressive regimens shown to provide the best outcomes for patient and
graft survival should be used, irrespective of posttransplantation diabetes mellitus
risk. E
Monogenic Diabetes Syndromes
Recommendations
All children diagnosed with diabetes in the first 6 months of life should have
immediate genetic testing for neonatal diabetes. A
Children and those diagnosed in early adulthood who have diabetes not characteristic
of type 1 or type 2 diabetes that occurs in successive generations (suggestive of an
autosomal dominant pattern of inheritance) should have genetic testing for maturity-
onset diabetes of the young. A
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 11
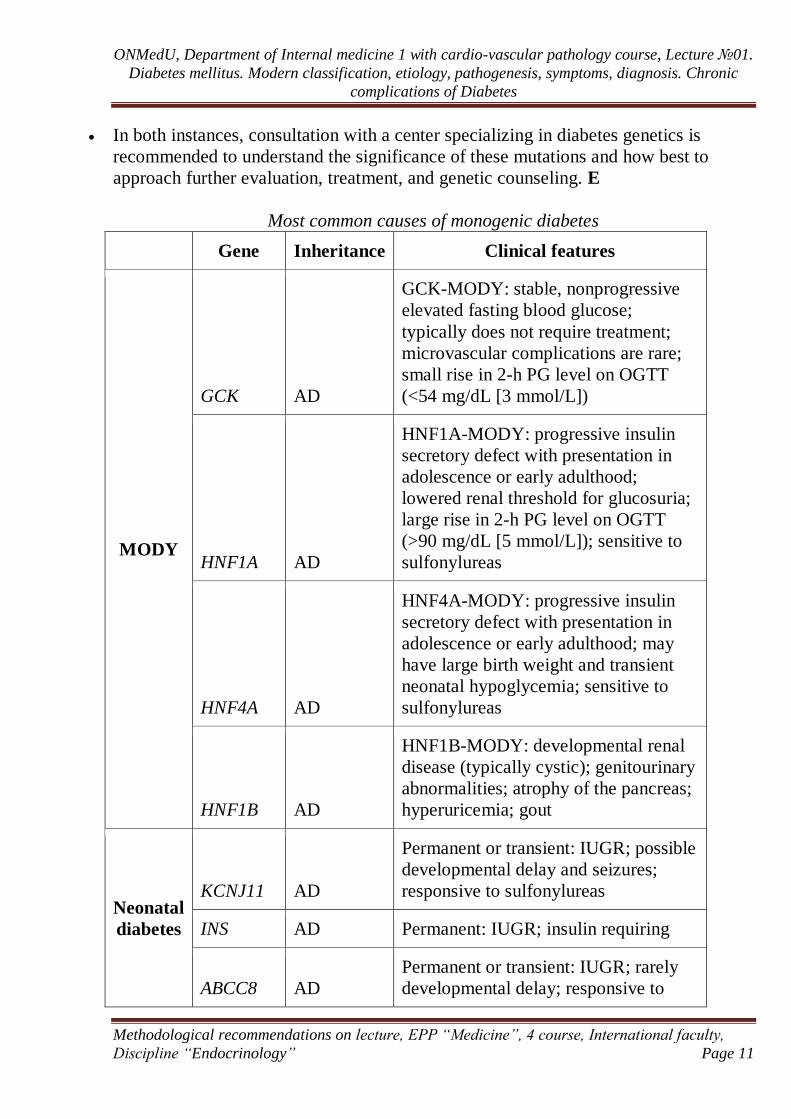
In both instances, consultation with a center specializing in diabetes genetics is
recommended to understand the significance of these mutations and how best to
approach further evaluation, treatment, and genetic counseling. E
Most common causes of monogenic diabetes
Gene Inheritance Clinical features
MODY
GCK AD
GCK-MODY: stable, nonprogressive
elevated fasting blood glucose;
typically does not require treatment;
microvascular complications are rare;
small rise in 2-h PG level on OGTT
(<54 mg/dL [3 mmol/L])
HNF1A AD
HNF1A-MODY: progressive insulin
secretory defect with presentation in
adolescence or early adulthood;
lowered renal threshold for glucosuria;
large rise in 2-h PG level on OGTT
(>90 mg/dL [5 mmol/L]); sensitive to
sulfonylureas
HNF4A AD
HNF4A-MODY: progressive insulin
secretory defect with presentation in
adolescence or early adulthood; may
have large birth weight and transient
neonatal hypoglycemia; sensitive to
sulfonylureas
HNF1B AD
HNF1B-MODY: developmental renal
disease (typically cystic); genitourinary
abnormalities; atrophy of the pancreas;
hyperuricemia; gout
Neonatal
diabetes
KCNJ11 AD
Permanent or transient: IUGR; possible
developmental delay and seizures;
responsive to sulfonylureas
INS AD Permanent: IUGR; insulin requiring
ABCC8 AD
Permanent or transient: IUGR; rarely
developmental delay; responsive to
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 12
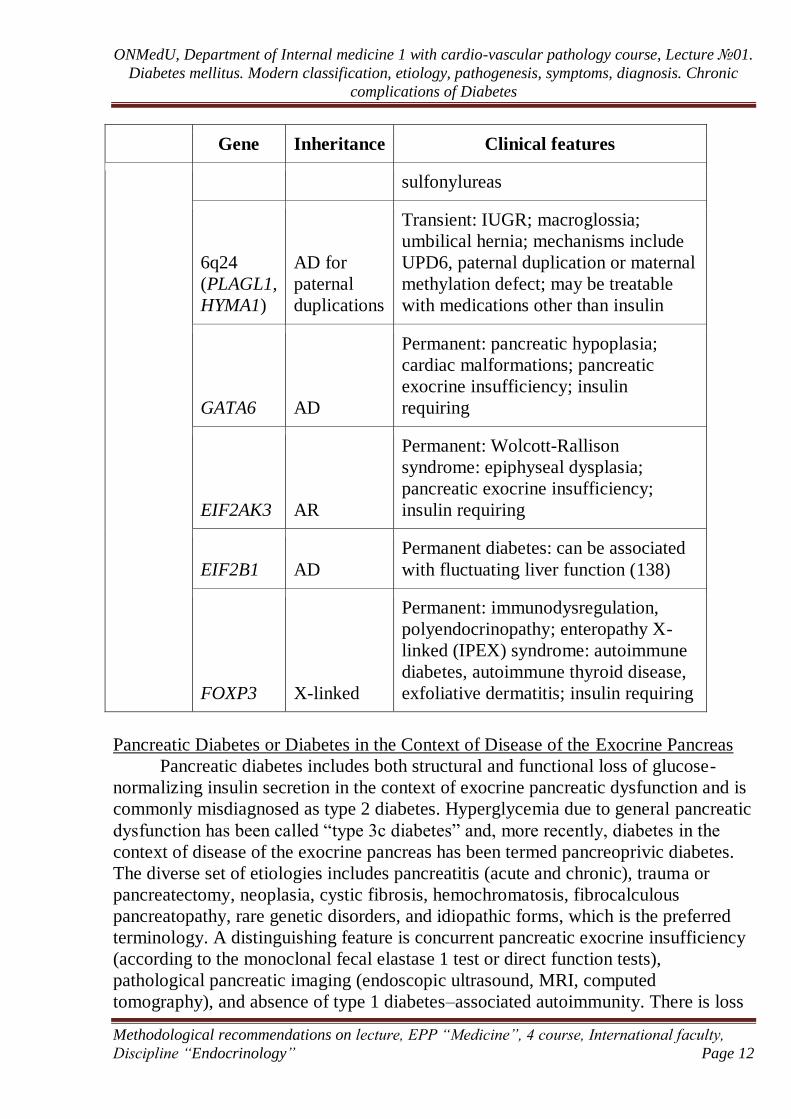
Gene Inheritance Clinical features
sulfonylureas
6q24
(PLAGL1,
HYMA1)
AD for
paternal
duplications
Transient: IUGR; macroglossia;
umbilical hernia; mechanisms include
UPD6, paternal duplication or maternal
methylation defect; may be treatable
with medications other than insulin
GATA6 AD
Permanent: pancreatic hypoplasia;
cardiac malformations; pancreatic
exocrine insufficiency; insulin
requiring
EIF2AK3 AR
Permanent: Wolcott-Rallison
syndrome: epiphyseal dysplasia;
pancreatic exocrine insufficiency;
insulin requiring
EIF2B1 AD
Permanent diabetes: can be associated
with fluctuating liver function (138)
FOXP3 X-linked
Permanent: immunodysregulation,
polyendocrinopathy; enteropathy X-
linked (IPEX) syndrome: autoimmune
diabetes, autoimmune thyroid disease,
exfoliative dermatitis; insulin requiring
Pancreatic Diabetes or Diabetes in the Context of Disease of the Exocrine Pancreas
Pancreatic diabetes includes both structural and functional loss of glucose-
normalizing insulin secretion in the context of exocrine pancreatic dysfunction and is
commonly misdiagnosed as type 2 diabetes. Hyperglycemia due to general pancreatic
dysfunction has been called “type 3c diabetes” and, more recently, diabetes in the
context of disease of the exocrine pancreas has been termed pancreoprivic diabetes.
The diverse set of etiologies includes pancreatitis (acute and chronic), trauma or
pancreatectomy, neoplasia, cystic fibrosis, hemochromatosis, fibrocalculous
pancreatopathy, rare genetic disorders, and idiopathic forms, which is the preferred
terminology. A distinguishing feature is concurrent pancreatic exocrine insufficiency
(according to the monoclonal fecal elastase 1 test or direct function tests),
pathological pancreatic imaging (endoscopic ultrasound, MRI, computed
tomography), and absence of type 1 diabetes–associated autoimmunity. There is loss

ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 13
of both insulin and glucagon secretion and often higher-than-expected insulin
requirements. Risk for microvascular complications is similar to other forms of
diabetes. In the context of pancreatectomy, islet autotransplantation can be done to
retain insulin secretion. In some cases, autotransplant can lead to insulin
independence. In others, it may decrease insulin requirements.
Gestational Diabetes Mellitus
Recommendations
Test for undiagnosed prediabetes and diabetes at the first prenatal visit in those
with risk factors using standard diagnostic criteria. B
Test for gestational diabetes mellitus at 24–28 weeks of gestation in pregnant
women not previously found to have diabetes. A
Test women with gestational diabetes mellitus for prediabetes or diabetes at 4–
12 weeks postpartum, using the 75-g oral glucose tolerance test and clinically
appropriate nonpregnancy diagnostic criteria. B
Women with a history of gestational diabetes mellitus should have lifelong
screening for the development of diabetes or prediabetes at least every 3 years. B
Women with a history of gestational diabetes mellitus found to have
prediabetes should receive intensive lifestyle interventions and/or metformin to
prevent diabetes. A
Screening for and diagnosis of GDM
One-step strategy
Perform a 75-g OGTT, with plasma glucose measurement when patient is
fasting and at 1 and 2 h, at 24–28 weeks of gestation in women not previously
diagnosed with diabetes.
The OGTT should be performed in the morning after an overnight fast of at least
8 h.
The diagnosis of GDM is made when any of the following plasma glucose
values are met or exceeded:
• Fasting: 92 mg/dL (5.1 mmol/L)
• 1 h: 180 mg/dL (10.0 mmol/L)
• 2 h: 153 mg/dL (8.5 mmol/L)
Two-step strategy
Step 1: Perform a 50-g GLT (nonfasting), with plasma glucose measurement at
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 14
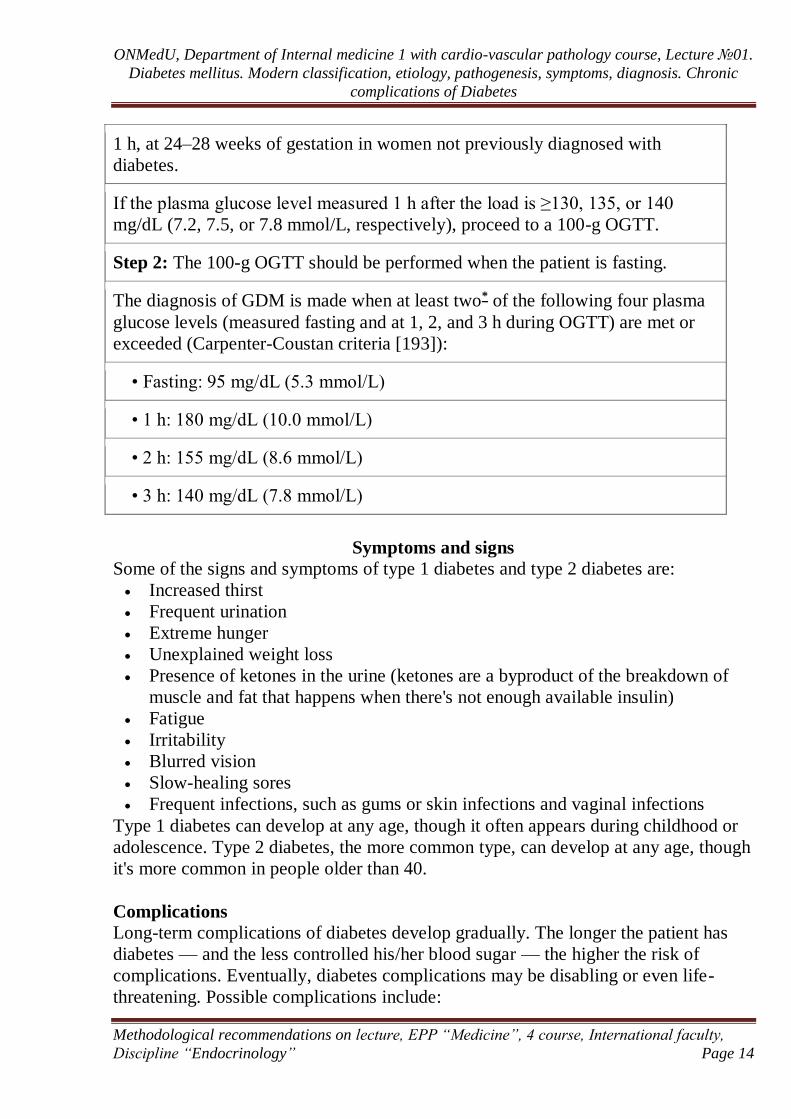
1 h, at 24–28 weeks of gestation in women not previously diagnosed with
diabetes.
If the plasma glucose level measured 1 h after the load is ≥130, 135, or 140
mg/dL (7.2, 7.5, or 7.8 mmol/L, respectively), proceed to a 100-g OGTT.
Step 2: The 100-g OGTT should be performed when the patient is fasting.
The diagnosis of GDM is made when at least two* of the following four plasma
glucose levels (measured fasting and at 1, 2, and 3 h during OGTT) are met or
exceeded (Carpenter-Coustan criteria [193]):
• Fasting: 95 mg/dL (5.3 mmol/L)
• 1 h: 180 mg/dL (10.0 mmol/L)
• 2 h: 155 mg/dL (8.6 mmol/L)
• 3 h: 140 mg/dL (7.8 mmol/L)
Symptoms and signs
Some of the signs and symptoms of type 1 diabetes and type 2 diabetes are:
Increased thirst
Frequent urination
Extreme hunger
Unexplained weight loss
Presence of ketones in the urine (ketones are a byproduct of the breakdown of
muscle and fat that happens when there's not enough available insulin)
Fatigue
Irritability
Blurred vision
Slow-healing sores
Frequent infections, such as gums or skin infections and vaginal infections
Type 1 diabetes can develop at any age, though it often appears during childhood or
adolescence. Type 2 diabetes, the more common type, can develop at any age, though
it's more common in people older than 40.
Complications
Long-term complications of diabetes develop gradually. The longer the patient has
diabetes — and the less controlled his/her blood sugar — the higher the risk of
complications. Eventually, diabetes complications may be disabling or even life-
threatening. Possible complications include:
ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 15
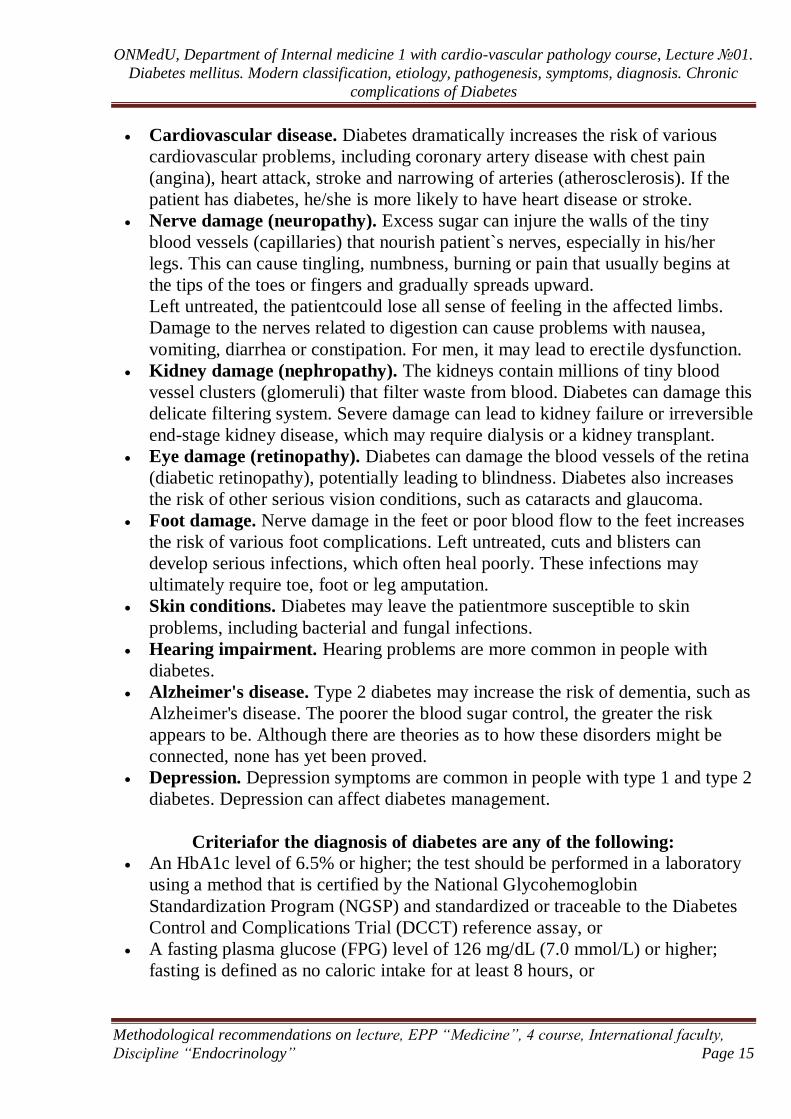
Cardiovascular disease. Diabetes dramatically increases the risk of various
cardiovascular problems, including coronary artery disease with chest pain
(angina), heart attack, stroke and narrowing of arteries (atherosclerosis). If the
patient has diabetes, he/she is more likely to have heart disease or stroke.
Nerve damage (neuropathy). Excess sugar can injure the walls of the tiny
blood vessels (capillaries) that nourish patient`s nerves, especially in his/her
legs. This can cause tingling, numbness, burning or pain that usually begins at
the tips of the toes or fingers and gradually spreads upward.
Left untreated, the patientcould lose all sense of feeling in the affected limbs.
Damage to the nerves related to digestion can cause problems with nausea,
vomiting, diarrhea or constipation. For men, it may lead to erectile dysfunction.
Kidney damage (nephropathy). The kidneys contain millions of tiny blood
vessel clusters (glomeruli) that filter waste from blood. Diabetes can damage this
delicate filtering system. Severe damage can lead to kidney failure or irreversible
end-stage kidney disease, which may require dialysis or a kidney transplant.
Eye damage (retinopathy). Diabetes can damage the blood vessels of the retina
(diabetic retinopathy), potentially leading to blindness. Diabetes also increases
the risk of other serious vision conditions, such as cataracts and glaucoma.
Foot damage. Nerve damage in the feet or poor blood flow to the feet increases
the risk of various foot complications. Left untreated, cuts and blisters can
develop serious infections, which often heal poorly. These infections may
ultimately require toe, foot or leg amputation.
Skin conditions. Diabetes may leave the patientmore susceptible to skin
problems, including bacterial and fungal infections.
Hearing impairment. Hearing problems are more common in people with
diabetes.
Alzheimer's disease. Type 2 diabetes may increase the risk of dementia, such as
Alzheimer's disease. The poorer the blood sugar control, the greater the risk
appears to be. Although there are theories as to how these disorders might be
connected, none has yet been proved.
Depression. Depression symptoms are common in people with type 1 and type 2
diabetes. Depression can affect diabetes management.
Criteriafor the diagnosis of diabetes are any of the following:
An HbA1c level of 6.5% or higher; the test should be performed in a laboratory
using a method that is certified by the National Glycohemoglobin
Standardization Program (NGSP) and standardized or traceable to the Diabetes
Control and Complications Trial (DCCT) reference assay, or
A fasting plasma glucose (FPG) level of 126 mg/dL (7.0 mmol/L) or higher;
fasting is defined as no caloric intake for at least 8 hours, or

ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 16
A 2-hour plasma glucose level of 200 mg/dL (11.1 mmol/L) or higher during a
75-g oral glucose tolerance test (OGTT), or
A random plasma glucose of 200 mg/dL (11.1 mmol/L) or higher in a patient
with classic symptoms of hyperglycemia (ie, polyuria, polydipsia, polyphagia,
weight loss) or hyperglycemic crisis
Questions for the self-control
1. What is Diabetes mellitus?
2. What types of DM do you know?
3. What is the role of glucagon-like peptide in our body?
4. What is the role of Sodium-glucose co-transporter 2 type in our body?
5. Describe the pathophysiological links of type 1 DM
6. Describe the pathophysiological links of type 2 DM
7. What are the criteria of pre-diabetes?
8. What are the criteria of gestation DM?
9. What are the reasons for polyuria?
10. What complication of DM is the most common?
References
1. https://care.diabetesjournals.org/
2. Davidson's Principles and Practice of Medicine, 23rd Edition, 2018.
3. Endocrinology: textbook /Ed. by prof. Petro M. Bodnar.- 4th ed. updated –
Vinnitsa: Nova Knyha, 2017. – 328 р.
4. USMLE Step 2 CK Lecture Notes 2017: Internal Medicine (Kaplan Test Prep). -
2016. - Published by Kaplan Medical. - 474 pages.
5. https://academic.oup.com/ndt/pages/General_Instruction
6. http://www.acc.org/guidelines#sort=%40foriginalz32xpostedz32xdate86069%20d
escending
7. http://www.asco.org/practice-guidelines/quality-guidelines/guidelines
8. https://www.asn-online.org/education/training/fellows/educational-
resources.aspx#Guidelines
9. https://cprguidelines.eu/
10. https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines
11. http://www.eagen.org/
12. http://www.ers-education.org/guidelines.aspx
13. http://www.enp-era-edta.org/#/44/page/home
14. https://www.eular.org/recommendations_management.cfm
15. http://www.esmo.org/Guidelines/Haematological-Malignancies
16. https://ehaweb.org/organization/committees/swg-unit/scientific-working-
groups/structure-and-guidelines/
17. http://www.oxfordmedicaleducation.com/

ONMedU, Department of Internal medicine 1 with cardio-vascular pathology course, Lecture №01.
Diabetes mellitus. Modern classification, etiology, pathogenesis, symptoms, diagnosis. Chronic
complications of Diabetes
Methodological recommendations on lecture, EPP “Medicine”, 4 course, International faculty,
Discipline “Endocrinology” Page 17
18. http://professional.heart.org/professional/GuidelinesStatements/UCM_316885_Gu
idelines-Statements.jsp
19. https://www.ueg.eu/guidelines/
20. http://www.diabetes.org
21. http://care.diabetesjournals.org
22. http://www.endocrinology.mif-ua.com
23. https://care.diabetesjournals.org/content/44/Supplement_1/S1
24. https://calgaryguide.ucalgary.ca/pathogenesis-of-diabetes-mellitus-dm-type-ii/
25. https://care.diabetesjournals.org/content/39/2/179.full
26. https://www.mayoclinic.org/diseases-conditions/diabetes/symptoms-causes/syc-
20371444
27. https://emedicine.medscape.com/article/117853-overview

![INTERNAL MEDICINE - Home | WMed Internal Medicine v2[1].pdf · the western michigan university homer stryker m.d. school of medicine (wmed) internal medicine residency program has](https://img.pdfslide.net/doc/110x75/5b4f1ed47f8b9a396e8ba16a/internal-medicine-home-internal-medicine-v21pdf-the-western-michigan.jpg)



























