Embed Size (px)
Citation preview

Effectiveness and implementationof enhanced recovery after surgeryprogrammes: a rapid evidence synthesis
Fiona Paton,1 Duncan Chambers,1 Paul Wilson,1 Alison Eastwood,1 Dawn Craig,1
Dave Fox,1 David Jayne,2 Erika McGinnes2
To cite: Paton F,Chambers D, Wilson P, et al.Effectiveness andimplementation of enhancedrecovery after surgeryprogrammes: a rapidevidence synthesis. BMJOpen 2014;4:e005015.doi:10.1136/bmjopen-2014-005015
▸ Prepublication history andadditional material isavailable. To view please visitthe journal (http://dx.doi.org/10.1136/bmjopen-2014-005015).
Received 7 February 2014Revised 1 July 2014Accepted 4 July 2014
▸ http://dx.doi.org/10.1136/bmjopen-2014-005014
1Centre for Reviews andDissemination, University ofYork, York, UK2Leeds Teaching HospitalsNHS Trust, Leeds, UK
Correspondence toFiona Paton;[email protected]
ABSTRACTObjectives: To assess the evidence on the impact ofenhanced recovery programmes for patientsundergoing elective surgery in acute hospital settingsin the UK.Design: Rapid evidence synthesis. Eight databaseswere searched from 1990 to March 2013 withoutlanguage restrictions. Relevant reports and guidelines,websites and reference lists of retrieved articles werescanned to identify additional studies. Systematicreviews, RCTs not included in the systematic reviews,economic evaluations and UK NHS cost analysis,implementation case studies and surveys of patientexperience in a UK setting were eligible for inclusion.Primary and secondary outcome measures: Weassessed the impact of enhanced recoveryprogrammes on health or cost-related outcomes, andassessed implementation case studies and patientexperience in UK settings. Studies were qualityassessed where appropriate using the Centre forReviews and Dissemination Database of Abstracts ofReviews of Effects critical appraisal process.Results: 17 systematic reviews and 12 additionalRCTs were included. Ten relevant economic evaluationswere included. No cost analysis studies were identified.Most of the evidence focused on colorectal surgery. 14innovation case studies and 15 implementation casestudies undertaken in National Health Service settingsdescribed factors critical to the success of anenhanced recovery programme.Evidence for colorectal surgery suggests that
enhanced recovery programmes may reduce hospitalstays by 0.5–3.5 days compared with conventionalcare. There were no significant differences in reportedreadmission rates. Other surgical specialties showedgreater variation in reductions in length of stayreflecting the limited evidence identified. Findingsrelating to other outcomes were hampered by a lack ofrobust evidence and poor reporting.Conclusions: There is consistent, albeit limited,evidence that enhanced recovery programmes canreduce length of patient hospital stay withoutincreasing readmission rates. The extent to whichmanagers and clinicians considering implementingenhanced recovery programmes in UK settings canrealise savings will depend on length of stay achievedunder their existing care pathway.
INTRODUCTIONThe National Health Service (NHS) facessevere funding constraints now and in themedium term. The forecast reduction inresources provides an enormous challenge toNHS organisations and staff. Service redesigncan save money and improve quality butmuch depends on how care is co-ordinatedand the way services are implemented in alocal setting.1 2 NHS decisionmakers need toconsider not only the effectiveness and cost-effectiveness of any initiative but also effi-cient implementation. Enhanced recoveryprogrammes (also known as ERAS, fast track,multimodal, rapid or accelerated recoveryprogrammes) seek to deliver an optimal
Strengths and limitations of this study
▪ Enhanced recovery programmes have beenadopted with enthusiasm by the NHS as ameans to achieving productivity gains and costsavings. This evolution makes combining studiesover different periods and interpreting results ofearlier studies in relation to the current contextmore difficult.
▪ The evidence base to support such widespreadimplementation suggests possible benefits interms of reduced length of hospital stay, fewerpostoperative complications, reduced readmis-sions and improved patient outcomes.
▪ Although there is a reasonable volume of evi-dence evaluating enhanced recovery programmesin colorectal surgery, robust evidence is sparse.Optimal care is certainly the right thing to do,but the evidence does not identify whichenhanced recovery programme elements andcombinations of elements are most effective.
▪ Findings relating to other outcomes, costs ofenhanced recovery programmes, experience inusing the programmes, and patient experiencewere limited by generally poor quality evidenceand poor reporting. As such, conclusions onwhich combinations provide greatest gains andhow best to implement them cannot be made.
Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015 1
Open Access Research
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

pathway (covering the preoperative, intraoperative andpostoperative periods) that is focused on optimal recov-ery and discharge for patients. The approach was pio-neered in Denmark in the late 1990s for patientsundergoing colorectal surgery3 and is now spreading toother surgical pathways such as orthopaedic, urologyand gynaecology.Enhanced recovery programmes have been delivered
in the UK NHS since the early 2000s. Implementationhas to date been variable despite the support of theDepartment of Health and more recently the RoyalColleges. In 2011, 14 innovation sites were established aspart of the Enhanced Recovery Partnership Programme.These sites acted as pathfinders for implementation;some sites were self-selecting and others were encour-aged to join. The aim was to raise the profile, promotethe benefits and inform the uptake of enhanced recov-ery for elective surgical care across the NHS. These siteshad little or no experience in enhanced recovery path-ways. It is likely that this variation seen across these sitesreflects the complexity of enhanced recovery pro-grammes themselves and issues around implementingchange in established surgical pathways . Differences inprogramme implementation may also reflect differencesbetween surgical specialities. Set against the benefits ofenhanced recovery programmes are concerns that dis-charging patients too soon after surgery could increasecomplications and readmissions, thereby worseningpatient experience and potentially health outcomes, andincreasing pressure on primary and/or secondaryhealthcare services.Before embarking on adoption of an enhanced recov-
ery programme, NHS managers and clinicians need tobe fully aware of the strength of the underlying evi-dence. They need to have a clear understanding of howbest to implement such programmes and the likelyimplications for service delivery within finite budgetsand considering the need for equity of access. The aimof this project was to conduct a rapid synthesis of the evi-dence on the clinical and cost-effectiveness of enhancedrecovery programmes, and the implementation, deliveryand impact of such programmes in secondary care set-tings in the UK.
METHODSEight databases, including DARE, NHS EED andMEDLINE were searched to from 1990 to March 2013without language restrictions. The PROSPERO databasewas searched to identify ongoing systematic reviews.Relevant reports and guidelines were screened forfurther studies. Reference lists of retrieved articles,reviews and evaluations were scanned, and relevant indi-viduals contacted for additional evidence.Systematic reviews, RCTs not included in the system-
atic reviews, economic evaluations and UK NHS costanalysis studies were included if they evaluated theimpact of enhanced recovery programmes
(encompassing different combinations of the main pre-operative, intraoperative and postoperative pathway ele-ments described by the Enhanced Recovery PartnershipProgramme)4 on health-related or cost-related out-comes. Eligible studies included patients undergoingelective surgery in an acute hospital in the UK NHS or acomparable healthcare system. Comparators were onlyrelevant to clinical and cost-effectiveness evaluations,and included conventional (usual/standard) carewithout a structured multimodal enhanced recoverypatient pathway (as defined in the included studies).Case studies, impact assessments and surveys of patientexperience that documented the experience of imple-menting enhanced recovery in a UK setting were alsoeligible.Quality assessment of systematic reviews, RCTs and
economic evaluations was based on existing CRD criticalappraisal methods (http://www.crd.york.ac.uk/crdweb/HomePage.asp; CRD, 2009). Cost analysis studies,studies of patient experience and case studies of imple-mentation were not formally quality assessed.All stages of the review process were performed by
one researcher and checked by a second. Disagreementsbetween reviewers were resolved by discussion or byrecourse to a third reviewer where necessary.The type and range of evidence precluded meta-
analysis and we therefore performed a narrative synthesis,differentiating clinical outcomes (eg, mobilisation, mor-tality and morbidity and length of hospital stay), patient-reported outcomes (eg, patient experience and satisfac-tion), resource use in secondary care (eg, workforce util-isation and costs) and implementation case studies.
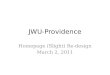
RESULTSSeventeen systematic reviews5–21 and 12 additionalRCTs22–34 were included in the evidence on clinicaleffectiveness (see figure 1: flow diagram). The quality ofthe systematic reviews varied and the additional RCTswere considered to be at high risk of bias (see tables 1and 2). One RCT was a four arm trial; this was the onlymulticentre trial, the remaining trials were small, singlecentre trials.35 We included 15 case studies of implemen-tation of ERAS in NHS settings, and evaluations of the14 Enhanced Recovery Partnership Programme innov-ation sites. In addition, 10 relevant economic evaluationswere also included (summary evidence tables are avail-able on request from the review authors). Most of theevidence focused on colorectal surgery.Where reviews reported the number of included
patients, sample sizes ranged between 99 and 5747patients in the ERAS group and between 99 and 1062 incomparator groups. Most individual RCTs analysed fewerthan 100 patients (range 44–597 patients). Where indi-cations for surgery were reported in systematic reviewsand individual RCTs, most trials were in patients withcancer. Where reported, patients were adults within
2 Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

similar age ranges. Follow-up was generally up to 30 dayspost discharge.The number and combination of ERAS elements
varied considerably across all types of evidence; rangingfrom 4 to 14 elements across systematic reviews and from10 to 14 elements across individual RCTs (see full reportfor details; in press). This highlights the lack of stand-ardisation across ERAS programmes and agreement onwhat constitutes an ERAS pathway, and will have implica-tions on the overall findings. Only one review assessedcompliance with ERAS elements.7 Ahmed et al7 notedthat, in general, compliance fell during the post-operative period in most of the studies (from around100% to around 20%). Use of epidural analgesia had
the highest levels of compliance across all studies (67–100%). Use of transverse incisions had the lowest levelsof compliance (around 25%). Reasons for differences incompliance and waning of compliance were not mea-sured in the reviews. None of the reviews assessedpatient compliance, including adherence to preopera-tive advice to ensure fitness for surgery.Despite the large number of studies, robust evidence
was sparse (see online supplementary tables S1 and S2;full outcome details are available in the full review; inpress). Seven reviews in colorectal surgery performedmeta-analyses and showed a significant mean reductionin primary or total length of stay that ranged from1.56 days (95% CI 0.50 to 2.61 days)19 to 3.75 days (95%
Figure 1 Study flow diagram.
Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015 3
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

CI 5.11 to 2.40 days).18 Evidence from individual RCTsin colorectal surgery also suggest reduced length of hos-tpital stay following an ERAS programme (mean lengthof stay 4.15 to 6.43 days) compared to conventional care(mean length of stay 6.6 to 11.7 days). There were nosignificant differences in reported readmission rates, butit was unclear how readmissions were defined and mea-sured in the reviews and RCTs.Other surgical specialties showed greater variation in
reported reductions in length of stay, but this is likely toreflect the greater uncertainty due to the more limited evi-dence base for these specialties. Statistical heterogeneityvaried between reviews and was often not formallyexplored, but may have reflected differences in ERAS pro-tocols, lack of compliance with important ERAS elements,and differences in surgical populations and procedures.Deaths were rare and no significant differences
between treatment groups were found in the systematicreviews and additional RCTs, regardless of surgical spe-cialty. Morbidity was defined differently across systematicreviews and RCTs; rates between treatment groups weresometimes inconsistent, but generally indicated no statis-tically significant differences.Mobilisation rates were inconsistent across systematic
reviews, but most reported no significant differences in timeto mobilisation between treatment groups. Mobilisation wasrarely reported as an outcome in the additional RCTs.
Where systematic reviews and additional RCTs assessedquality of life and patient experience/satisfaction,equivocal findings were reported. Evidence on reinter-vention rates, pain and resource use was lacking in sys-tematic reviews and RCTs.
Other reviewsA systematic review in colorectal surgery, identified afterthe last literature search, showed similar findings to thesystematic reviews discussed above.36 Mean length ofprimary hospital stay was statistically significantlyreduced in ERAS patients; mean difference (MD) −2.44(95% CI −3.06 to −1.83; 11 RCTs) but with significantstatistical heterogeneity (I2=88%). There was no evi-dence to suggest increased rates of readmissions, compli-cations and mortality. Some of the individual RCTresults for primary length of stay did not appear to beconsistent with results reported in other systematicreviews, and this may have impacted on the estimatedreduction in length of primary hospital stay.36
Two reviews37 38 focusing on individual ERAS elementswere identified, of which highlighted the lack of evi-dence on the full ERAS pathway and the lack of compli-ance with ERAS protocols. Details can be found in thefull review (in press).
Table 1 Systematic review risk of bias assessment
Author
Adequate
search
Risk of
bias
assessed
Quality
score
accounted
for in
analysis
Study details
reported and
differences
accounted
for
Statistical
heterogeneity
investigated
Gaps in
research
identified
Conclusions
justified
Colorectal/colon surgery
Adamina et al6 ✓ ✓ UC ✓ UC ✓ ✓Ahmed et al7 ✓ X X X X X ✓Eskicioglu et al10 ✓ ✓ X ✓ ✓ ✓ ✓Gouvas et al11 ✓ ✓ X ✓ ✓ ✓ ✓Khan et al13 ✓ ✓ X ✓ X ✓ ✓Lv et al21 ✓ ✓ X X ✓ ✓ ✓Rawlinson et al15 ✓ X X ✓ UC X UC
Spanjersberg
et al16✓ ✓ ✓ ✓ ✓ ✓ ✓
Varadhan et al17 ✓ ✓ X ✓ ✓ ✓ ✓Walter et al18 ✓ ✓ ✓ ✓ ✓ ✓ ✓Wind et al19 ✓ ✓ ✓ ✓ ✓ ✓ ✓
Gynaecological surgery
Lv et al20 ✓ X X X X ✓ ✓Liver/pancreatic surgery
Coolsen et al8 ✓ ✓ X ✓ X ✓ ✓Coolsen et al9
Link to66✓ ✓ ✓ ✓ ✓ ✓ ✓
Hall et al12 X X X ✓ X ✓ ✓Various surgical specialities
Lemmens et al14 ✓ X X ✓ X ✓ ✓Sturm et al5 ✓ X X ✓ UC ✓ ✓
UC, unclear reporting.
4 Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

Case studiesTen of 14 UK NHS innovation sites provided adequatedata for inclusion in this section.39–41 Fifteen casestudies of implementation of ERAS in NHS settings, and11 NHS trusts (mostly in colorectal surgery) providedevidence relating to the implementation of an ERASprogramme within their Trust. Full results and evidencetables are presented in the full review (in press).There were variations in practice in terms of numbers
and combinations of ERAS elements implemented; themost frequently implemented programme elements inthe case studies were preadmission information/counsel-ling and early postoperative mobilisation. Available evi-dence did not address which enhanced recoveryelements and combinations of elements were mosteffective. Substantial variation in what constitutes anenhanced recovery programme within and between dif-ferent surgical specialities, and difficulties in implement-ing certain ERAS components, suggest that theenhanced recovery pathway may be used as a frameworkand adapted to suit local situations. Evidence on compli-ance/adherence to enhanced recovery programmes waslacking.Case studies identified the factors believed to act as
barriers or facilitators to implementing an ERAS pro-gramme. Barriers to implementation included resistanceto change from patients and staff, lack of funding orsupport from management,39 42–44 staff turnover, pro-blems arising from poor documentation, the timerequired to complete documentation and other practicalissues.Facilitators included the presence of a dedicated
ERAS project lead/nurse to coordinate and sustainmultidisciplinary working and continuity of the pathway,a multidisciplinary team approach and continual educa-tion for staff and patients/patient representatives. Oneinnovation site mentioned that it did not offer a 7 dayservice for enhanced recovery due to staff resources.Patients operated on towards the end of the week mayhave to wait until after the weekend to be discharged ifthey need to be seen by any healthcare professionals orsocial services. The need to sustain multidisciplinaryworking means that, in the absence of 24/7 working forelective procedures, enhanced recovery programmes willtend to be front loaded into the start of the workingweek (typically Monday to Thursday). Recent evidencesuggests a higher risk of death for patients who haveelective surgical procedures carried out later in theworking week and at the weekend,45 the capcity toimplement ERAS throughout the working week mightensure continuity of best care and help mitigate againstsuch variation.We included two published studies of patient experi-
ence of ERAS.46 47 Each study used qualitative researchmethods to analyse audiotaped material. The two studiesprovided limited evidence suggesting that patients whowere willing to provide feedback took a positive view oftheir experience of treatment in an ERAS programme.
Table
2RCTqualityassessment
Author
Adequate
random
allocation
Adequate
allocation
concealm
ent
Blindingof
healthcare
professional
Blindingof
participants
Blinding
of
outcome
assessor
Unexpected
imbalancesin
dropouts
betw
een
groups
Imbalances
accounted/
adjustedfor
Intention-
to-treat
analysis
ITTappropriate
andappropriate
methodsused
toaccountfor
missingdata
Bariatric
surgery
Lemanuetal27
✓✓
XX
XX
NA
UC
UC
Colorectal/colonsurgery
Garcia-Botello
etal24
UC
XUC
XUC
XNA
UC
✓Ionescuetal25
✓✓
XX
UC
XNA
UC
UC
Leeetal26
✓✓
UC
XUC
XNA
UC
UC
Renetal29
✓✓
XX
✓X
NA
UC
UC
Wangetal31
UC
UC
UC
XUC
XNA
✓✓
Wangetal32
UC
UC
XX
✓UC
UC
UC
UC
Yangetal3334
✓UC
XX
UC
XNA
XX
Gastric
surgery
Chenetal22
UC
UC
X✓
✓X
NA
UC
UC
Kim
etal23
UC
UC
XX
XX
NA
UC
UC
Liu
etal28
UC
XX
XX
XNA
UC
UC
Wangetal30
UC
UC
XX
UC
XNA
XX
UC,unclearreporting;NA,notapplicable.
Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015 5
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

The studies suggested that patients were willing tocomment on their experience in a way that can helphealthcare providers to identify areas for improvement.
COST-EFFECTIVENESSTen economic evaluations in adult populations undergo-ing various surgical procedures evaluated costs andoutcomes over short-time horizons (see onlinesupplementary table S3).48–57 All of the evaluations sug-gested that programmes that achieve a reduction inlength of stay are cost saving, and are not to the detri-ment of patients in terms of complication rates, readmis-sion and health-related quality-of-life. The quality of theclinical studies on which these evaluations were based wasvariable, but generally poor. The generalisability of theresults of these evaluations was limited by a lack of trans-parency in reporting, and the disparity in standard proto-cols and what had been evaluated across the settingsmade it unfeasible to select a cost-effective programme.
DISCUSSIONStatement of principal findingsOverall, the systematic reviews and additional RCTs suggestthat length of hospital stay is reduced in ERAS patientscompared to patients receiving conventional care. The evi-dence was based mainly on colorectal surgery and theapplicability of findings to other surgical specialitiesremains less clear. Evidence for colorectal surgery suggeststhat enhanced recovery programmes may reduce hospitalstays by 0.5–3.5 days compared with conventional care.There were marked differences in length of stay across
reviews and individual studies regardless of specialty.These differences may reflect differences in ERAS proto-cols, compliance to ERAS programmes, healthcaresystems and procedures and/or outcome definitions.This raises questions regarding the magnitude of effectof the ERAS protocols on length of stay, which may beoverstated in some reviews.The evidence suggests that ERAS programmes do not
compromise patient morbidity, mortality and readmis-sion rates but outcome definitions varied across reviewsand individual studies. Such differences make it difficultto determine the reliability and generalisability of thefindings.Equivocal findings were reported for quality of life
and patient experience/satisfaction but the evidence wasbased on few studies, which utilised various methods tomeasure these outcomes. The limited evidence pre-cludes conclusions on the effects of ERAS protocols onpain, mobilisation and reintervention.The implementation evidence included resource use
in terms of the professionals involved in delivery ofenhanced recovery programmes, but details were verylimited and did not add to the evidence synthesis. Mostcase studies were uncontrolled and represent experi-ences of a sample of centres that chose to report theirdata; their outcomes may not be representative of those
achieved elsewhere in the UK NHS. Their main value asevidence is the light they shed on NHS clinicians’ per-ceptions of requirements for successful implementationand barriers to implementation of ERAS.The impact of surgical experience and surgical
volume on clinical outcomes was not explored and anyimplications of differences in these areas remainunknown. As enhanced recovery invariably targets thefitter, more mobile patient, frailer patients may notreceive parity of access to what may be consideredoptimal treatment and management. Managers and clin-icians considering implementing such programmesshould think about the likely implication on equity ofaccess. Whether inequity is an unintended outcome ofenhanced recovery, merits further investigation.Our review of the cost-effectiveness literature suggests
that enhanced recovery programmes that achieve areduction in length of stay may save costs without detri-mental effects on complication rates, readmission andhealth-related quality of life. However, generalisability ofthe results of the economic evaluations is limited by alack of transparency in reporting, use of different set-tings and populations and variable methodology in ana-lyses. Data were lacking for resource use associated withthe programmes evaluated and could not usefullyinform the review of economic evaluations. In addition,the clinical effectiveness of some of the programmesconsidered in economic evaluations was not based onrobust evidence.
Strengths and weaknessesThe main strength of this study was our use of multipleapproaches to acquire and synthesise evidence. Themain limitations were poor methodological quality andpoor reporting of the included studies, and the inherentdifficulty of reviewing a complex intervention in differ-ent healthcare systems and surgical specialities. Currentmethods for synthesising such complex interventions arelimited. The methodological limitations and are not dis-cussed here as this was outside the scope of this project,but have been addressed in previous publications.58
Another complication is that elements of early enhancedrecovery programmes have become accepted practicewithin conventional care. This evolution makes combin-ing studies over different periods and interpretingresults of earlier studies in relation to the currentcontext more difficult.We found a large number of systematic reviews but
there was substantial overlap in the included studies andevidence was not as abundant as the existence of multiplesystematic reviews suggested. Most of the RCTs were smalland not high quality. With the exception of one RCT, theremainder were single centre trials and therefore appearto have been undertaken to support implementation ofan enhanced recovery programme in a specific settingrather than being planned as research studies. Therewere significant clinical and methodological differencesbetween individual trials, and we therefore presented a
6 Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

narrative synthesis. Relatively few trials were conducted inthe UK and this may limit the generalisability of evidenceto UK NHS settings.Lack of evidence on important outcomes including
pain and quality of life is also an issue for research inthis field. Trials tended not to report on adherence tothe planned enhanced recovery programme. Assessingadherence to interventions and the impact this has onhealth outcomes is an important issue which is oftenoverlooked in studies, and is a limitation in the evidencebase in this review.Three additional systematic reviews of effectiveness
were brought to our attention during manuscript sub-mission. One systematic review incorporates RCTs incolorectal surgery (Greco, 2013),59 one incorporatesRCTs and cohort studies in abdominal surgery (Neville,2014)60 and one includes RCTs and quasi-RCTs acrossvarious surgical specialities (Nicholson, 2014).61 Thetrials included in Greco (2013)59 and Nicholson(2014)61 overlap with those included in this review andthe findings are consistent. The inclusion of these tworeviews would therefore not have significantly alteredthe findings from this review. Neville (2014)60 providessome additional data on patient-reported outcomes,including some evidence on post-discharge functionalstatus. However, these outcomes were not frequentlyreported, and the additional evidence was mainly fromstudy designs that would not have met the inclusion cri-teria for this review.An important feature of our review is the inclusion of
evidence on the implementation of enhanced recoveryprogrammes in the UK NHS. This evidence has notbeen synthesised previously and the original pro-gramme websites are archived, so future access is notassured. By summarising this evidence, we have ensuredthat the main findings continue to be publicly available.We sought evidence on the experience of health profes-sionals and patients of a broad range of sources andstudy types. Important themes emerged from this evi-dence that may be of value for implementing and sus-taining enhanced recovery programmes in UK NHSsettings. Owing to the rapid nature of the evidence syn-thesis, the list of sources searched to identify data onimplementation and delivery of enhanced recovery pro-grammes was not exhaustive and we acknowledge thatrelevant evidence may have been missed. Indeed, evi-dence from Scotland has been noted and eligible casestudies have been identified from the NHS ScotlandQuality Improvement Hub website. It should be notedthat these are as limited as those included in thereview. A qualitative study was brought to our attentionat peer review; the study was published after our finalsearch date. Pearsall et al62 conducted a qualitativestudy to explore the barriers and enablers in imple-menting an enhanced recovery after surgery pro-gramme in a University hospital in Canada. Thethemes identified are consistent with those reported inthis review.
However, case studies are susceptible to risk of bias.Use of a standard reporting format was a potentialstrength of the case studies but variation in what eachsite actually reported (particularly in terms of evidenceof benefit from the introduction of enhanced recoveryprogrammes) reduced the usefulness of the evidence.We sought to incorporate published and unpublished
evidence on patient experiences and views of enhancedrecovery programmes. Evaluation of patient experienceof care is increasingly important for the NHS, especiallyin view of unacceptable failures of care such as thosehighlighted in the Francis Report.63 Though the evi-dence was generally positive for enhanced recovery, itwas limited by a shortage of studies that used validatedmeasures of patient experience and by study designsthat could bias results in favour of enhanced recovery.A further strength of this study was the consideration
of cost-effectiveness evidence, but the nature of the evi-dence did not permit any analyses. There is a clear needto capture better evaluated data on costs and benefits ofenhanced recovery programmes from a clearly statedperspective. A systematic review of economic evalua-tions64 was brought to our attention during manuscriptpublication. The review confirmed the need for well-designed research to determine the cost-effectiveness ofenhanced recovery programmes from the institutionaland societal perspectives.
Implications for healthcareOverall, there is consistent, albeit limited, evidence thatenhanced recovery programmes can reduce length ofpatient hospital stay without increasing readmissionrates. Data on reintervention rates and patient-reportedoutcomes did not suggest significant differencesbetween enhanced recovery and conventional care, butthe evidence was very limited and based on smallnumbers of patients. The lack of evidence on patientoutcomes, resource use and costs precludes firm conclu-sions on the overall value of enhanced recoveryprogrammes.ERAS does not appear to reduce complication or
readmission rates; the only cost benefit may lie in areduction in post-operative bed days. Optimal care is cer-tainly the right thing to do, but the evidence does notidentify which enhanced recovery programme elementsand combinations of elements are most effective. Assuch, conclusions on which combinations provide great-est gains and how best to implement them cannot bemade.The extent to which managers and clinicians consider-
ing implementing enhanced recovery programmes canrealise reductions and cost savings will therefore dependon length of stays achieved under their existing carepathway. Important themes emerged from the relevantevidence identified on implementation, including therole of ERAS facilitators and the need for full supportfrom management. It appears that these componentsare essential for the successful implementation and
Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015 7
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

sustained delivery of enhanced recovery programmes inNHS settings. Consideration of potential benefit alsoneeds to take account of the costs of service redesign,the resource use associated with programmes of thisnature, the potential for improvement in patient out-comes and the impact on equity of access.
Implications for researchRCTs comparing an enhanced recovery programme withconventional care continue to be conducted and pub-lished, although mostly not in the UK. Given the avail-able evidence, further single centre RCTs of this kindare not a priority. Rather, what is needed is improvedcollection and reporting of how enhanced recovery pro-grammes are implemented, resourced and experiencedin NHS settings. Also, exploration into the effect thatvarying levels of surgical volume and surgical experienceand different discharge protocols might have on thesuccess of an enhanced recovery pathway and subse-quent outcomes.This will enhance our existing knowl-edge and understanding and provide evidence tosupport local decision-making about whether to adoptand how best to implement.The two groups of implementation case studies
included in our synthesis, although all were conductedin the UK, provide very limited information on howenhanced recovery programmes have actually beenimplemented in UK NHS settings. The standard report-ing format originally proposed by The EnhancedRecovery Partnership Programme would enhance thevalue of future case studies if adhered to. Knowledge ofhow well the intervention has been implemented (fidel-ity) is essential for understanding how and why the inter-vention works and hence how outcomes can be furtherimproved. Assessing fidelity may involve considering notonly adherence to the requirements of the programmebut also potential moderating factors, such as strategiesused to assist delivery of the intervention, quality ofdelivery and participant responsiveness to new prac-tices.65 It would be helpful if future innovation pro-grammes used standardised reporting. For multisiteprogrammes, a formal synthesis of findings from all par-ticipating sites should be undertaken as part of theevaluative process. This would ensure that the insightsand contextual information which can inform the widerspread and adoption (or indeed discontinuation) wouldbe systematically captured in a generalisable format.Adherence/compliance to elements by staff and
patients also requires further investigation. Rigorousdata on patients’ experiences of enhanced recovery pro-grammes are lacking. Validated tools should be usedand administered independently of those providing theservice. Efforts should be made to obtain data from rep-resentative samples of patients receiving conventionalcare as well as those treated with enhanced recovery pro-tocols, along with evidence on the experiences of theirfamilies/carers.
Evidence relating to the cost-effectiveness of enhancedrecovery programmes in UK NHS settings is lacking.While enhanced recovery programmes have the poten-tial to deliver cost savings, improved measurement ofcosts and benefits is crucial to help decisionmakersdecide how best to make optimal use of limitedresources.
Acknowledgements The authors would like to thank all the NHS staff thattook the time to respond and help us identify grey literature considered forinclusion in this review.
Contributors PW took overall responsibility for the rapid synthesis. AEprovided input at all stages. DC was involved in all stages of the economicevaluation including production of the final review write-up. DCh and FP wereinvolved in all stages of the rapid synthesis including production of the finalreview write-up. DF conducted literature searches and contributed to themethods section of the review. DJ and EMcG provided advice throughout therapid synthesis and commented on the draft review.
Funding This project was funded as part of a programme of research fundedby the NIHR Health Services and Delivery Research programme (Project ref:11/1026/04).
Disclaimer This report presents independent research funded by the NationalInstitute for Health Research (NIHR). The views expressed are those of theauthors and do not necessarily reflect those of the NIHR Health Services andDelivery Research programme or the Department of Health.
Competing interests
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license,which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, providedthe original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
REFERENCES1. Øvretveit J. Does improving quality save money? A review of
evidence of which improvements to quality reduce costs for healthservice providers. London: The Health Foundation, 2009.
2. Øvretveit J. Does improving care coordination save money: a reviewof research. London: The Health Foundation, 2011.
3. Kehlet H, Slim K. The future of fast-track surgery. Br J Surg2012;99:1025–6.
4. Enhanced Recovery Partnership Programme. Delivering enhancedrecovery–helping patients to get better sooner after surgery. London:Department of Health, 2010.
5. Sturm L, Cameron AL. Brief review: fast-track surgery and enhancedrecovery after surgery (ERAS) programs. Melbourne: AustralianSafety and Efficacy Register of New Interventional Procedures—Surgical (ASERNIP-S), 2009 Contract No:3.
6. Adamina M, Kehlet H, Tomlinson GA, et al. Enhanced recoverypathways optimize health outcomes and resource utilization: ameta-analysis of randomized controlled trials in colorectal surgery.Surgery 2011;149:830–40.
7. Ahmed J, Khan S, Lim M, et al. Enhanced recovery after surgeryprotocols—compliance and variations in practice during routinecolorectal surgery. Colorectal Dis 2012;14:1045–51.
8. Coolsen MM, Wong-Lun-Hing EM, van Dam RM, et al. A systematicreview of outcomes in patients undergoing liver surgery in anenhanced recovery after surgery pathways. HPB (Oxford)2013;15:245–51.
9. Coolsen MM, van Dam RM, van der Wilt AA, et al. Systematicreview and meta-analysis of enhanced recovery after pancreaticsurgery with particular emphasis on pancreaticoduodenectomies.World J Surg 2013;37:1909–18.
10. Eskicioglu C, Forbes SS, Aarts M-A, et al. Enhanced recovery aftersurgery (ERAS) programs for patients having colorectal surgery:
8 Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

a meta-analysis of randomized trials. J Gastrointest Surg2009;13:2321–9.
11. Gouvas N, Tan E, Windsor A, et al. Fast-track vs standard care incolorectal surgery: a meta-analysis update. Int J Colorectal Dis2009;24:1119–31.
12. Hall TC, Dennison AR, Bilku DK, et al. Enhanced recoveryprogrammes in hepatobiliary and pancreatic surgery: a systematicreview. Ann R Coll Surg Engl 2012;94:318–26.
13. Khan S, Wilson T, Ahmed J, et al. Quality of life and patientsatisfaction with enhanced recovery protocols. Colorectal Dis2010;12:1175–82.
14. Lemmens L, van Zelm R, Borel Rinkes I, et al. Clinical andorganizational content of clinical pathways for digestive surgery:a systematic review. Dig Surg 2009;26:91–9.
15. Rawlinson A, Kang P, Evans J, et al. A systematic review ofenhanced recovery protocols in colorectal surgery. Ann R Coll SurgEngl 2011;93:583–8.
16. Spanjersberg Willem R, Reurings J, Keus F, et al. Fast track surgeryversus conventional recovery strategies for colorectal surgery.Cochrane Database of Sys Rev 2011;16(2):CD007635.
17. Varadhan KK, Neal KR, Dejong CH, et al. The enhanced recoveryafter surgery (ERAS) pathway for patients undergoing major electiveopen colorectal surgery: a meta-analysis of randomized controlledtrials. Clin Nutr 2010;29:434–40.
18. Walter CJ, Collin J, Dumville JC, et al. Enhanced recovery incolorectal resections: a systematic review and meta-analysis.Colorectal Dis 2009;11:344–53.
19. Wind J, Polle SW, Fung Kon Jin PH, et al. Systematic review ofenhanced recovery programmes in colonic surgery. Br J Surg2006;93:800–9.
20. Lu D, Wang X, Shi G. Perioperative enhanced recovery programmesfor gynaecological cancer patients. Cochrane Database Syst Rev2012;12:CD008239b.
21. Lv L, Shao YF, Zhou YB. The enhanced recovery after surgery(ERAS) pathway for patients undergoing colorectal surgery: anupdate of meta-analysis of randomized controlled trials. Int JColorectal Dis 2012;27:1549–54.
22. Chen Hu J, Xin Jiang L, Cai L, et al. Preliminary experience offast-track surgery combined with laparoscopy-assisted radical distalgastrectomy for gastric cancer. J Gastrointest Surg 2012;16:1830–9.
23. Kim JW, Kim WS, Cheong JH, et al. Safety and efficacy of fast-tracksurgery in laparoscopic distal gastrectomy for gastric cancer: arandomized clinical trial. World J Surg 2012;36:2879–87.
24. Garcia-Botello S, Canovas de Lucas R, Tornero C, et al.Implementation of a perioperative multimodal rehabilitation protocolin elective colorectal surgery. A prospective randomised controlledstudy. Cir Esp 2011;89:159–66.
25. Ionescu D, Iancu C, Ion D, et al. Implementing fast-track protocol forcolorectal surgery: a prospective randomized clinical trial. World JSurg 2009;33:2433–8.
26. Lee TG, Kang SB, Kim DW, et al. Comparison of early mobilizationand diet rehabilitation program with conventional care afterlaparoscopic colon surgery: a prospective randomized controlledtrial. Dis Colon Rectum 2011;54:21–8.
27. Lemanu DP, Singh PP, Berridge K, et al. Randomized clinical trial ofenhanced recovery versus standard care after laparoscopic sleevegastrectomy. Br J Surg 2013;100:482–9.
28. Liu XX, Jiang ZW, Wang ZM, et al. Multimodal optimization ofsurgical care shows beneficial outcome in gastrectomy surgery.JPEN J Parenter Enteral Nutr 2010;34:313–21.
29. Ren L, Zhu D, Wei Y, et al. Enhanced recovery after surgery (ERAS)program attenuates stress and accelerates recovery in patients afterradical resection for colorectal cancer: a prospective randomizedcontrolled trial. World J Surg 2012;36:407–14.
30. Wang D, Kong Y, Zhong B, et al. Fast-track surgery improvespostoperative recovery in patients with gastric cancer: a randomizedcomparison with conventional postoperative care. J GastrointestSurg 2010;14:620–7.
31. Wang G, Jiang ZW, Xu J, et al. Fast-track rehabilitation program vsconventional care after colorectal resection: a randomized clinicaltrial. World J Gastroenterol 2011;17:671–6.
32. Wang Q, Suo J, Jiang J, et al. Effectiveness of fast-trackrehabilitation vs conventional care in laparoscopic colorectalresection for elderly patients: a randomized trial. Colorectal Dis2012;14:1009–13.
33. Yang DJ, Zhang S, He WL, et al. Fast track surgery accelerates therecovery of postoperative insulin sensitivity. Chin Med J2012;125:3261–5.
34. Yang DJ, Zhang S, He WL, et al. Fast-track surgery accelerates therecovery of postoperative humoral immune function in elective
operation for colorectal carcinoma: a randomized controlled clinicaltrial. Chin Med J 2012;92:1112–15.
35. Vlug MS, Wind J, Hollmann MW, et al. Laparoscopy in combinationwith fast track multimodal management is the best perioperativestrategy in patients undergoing colonic surgery: a randomizedclinical trial (LAFA-study). Ann Surg 2011;254:868–75.
36. Cheng-Le Z, Xing-Zhao Y, Xiao-Dong Z, et al. Enhanced recoveryafter surgery programs versus traditional care for colorectal surgery:a meta-analysis of randomized controlled trials. Dis Colon Rectum2013;56:667–78.
37. Arsalani-Zadeh R, Elfadl D, Yassin N, et al. Evidence-based reviewof enhancing postoperative recovery after breast surgery. Br J Surg2011;98:181–96.
38. Hoffmann H, Kettelhack C. Fast-track surgery—conditions andchallenges in postsurgical treatment: a review of elements oftranslational research in enhanced recovery after surgery. Eur SurgRes 2012;49:24–34.
39. Enhanced Recovery Partnership Programme Case Studies 2011:Gynaecology: Addenbrookes Hospital.
40. Enhanced Recovery Partnership Programme Case Studies 2011:Enhanced Recovery Programme: Yeovil District Hospital NHSFoundation Trust.
41. Enhanced Recovery Partnership Programme Case Studies 2011:Enhanced recovery for colorectal surgery: Yeovil District HospitalNHS Foundation Trust.
42. Enhanced Recovery Partnership Programme Case Studies 2011:Colorectal, Gynaecology, Urology, MSK: Medway NHS FoundationTrust.
43. Enhanced Recovery Partnership Programme Case Studies 2011:Colorectal surgery (all elective procedures) and most majoremergencies from decision to treat surgically: Royal BerkshireHospital.
44. Enhanced Recovery Partnership Programme Case Studies 2011:Enhanced recovery after colorectal surgery: Royal BerkshireHospital.
45. Aylin P, Alexandrescu R, Jen MH, et al. Day of week of procedureand 30 day mortality for elective surgery: retrospective analysis ofhospital episode statistics. BMJ 2013;346:8.
46. Blazeby JM, Soulsby M, Winstone K, et al. A qualitativeevaluation of patients’ experiences of an enhanced recoveryprogramme for colorectal cancer. Colorectal Dis 2010;12(10 Online):e236–42.
47. Taylor C, Burch J. Feedback on an enhanced recovery programmefor colorectal surgery. Br J Nurs 2011;20:286–90.
48. Reilly KA, Beard DJ, Barker KL, et al. Efficacy of an acceleratedrecovery protocol for Oxford unicompartmental knee arthroplasty: arandomised controlled trial. Knee 2005;12:351–7.
49. Archibald LH, Ott MJ, Gale CM, et al. Enhanced recovery after colonsurgery in a community hospital system. Dis Colon Rectum2011;54:840–5.
50. Sammour T, Zargar-Shoshtari K, Bhat A, et al. A programme ofenhanced recovery after surgery (ERAS) is a cost-effectiveintervention in elective colonic surgery. N Z Med J 2010;123:61–70.
51. King PM, Blazeby JM, Ewings P, et al. The influence of anenhanced recovery programme on clinical outcomes, costs andquality of life after surgery for colorectal cancer. Colorectal Dis2006;8:506–13.
52. Nielsen PR, Andreasen J, Asmussen M, et al. Costs and quality oflife for prehabilitation and early rehabilitation after surgery of thelumbar spine. BMC Health Serv Res 2008;8:209. http://www.biomedcentral.com/1472–6963/8/209
53. Jakobsen DH, Sonne E, Andreasen J, et al. Convalescence aftercolonic surgery with fast-track vs conventional care. Colorectal Dis2006;8:683–7.
54. McBride N, Farringdon F, Midford R. Implementing a school drugeducation programme: reflections on fidelity. Int J Health PromotEduc 2002;40:40–50.
55. Kariv Y, Delaney CP, Senagore AJ, et al. Clinical outcomes and costanalysis of a fast track postoperative care pathway for ilealpouch-anal anastomosis. A case control study. Dis Colon Rectum2007;50:137–46.
56. Salhiyyah K, Elsobky S, Raja S, et al. A clinical and economicevaluation of fast-track recovery after cardiac surgery. Heart SurgForum 2011;14:E330–4.
57. Yanatori M, Tomita S, Miura Y, et al. Feasibility of the fast-trackrecovery program after cardiac surgery in Japan. Gen ThoracCardiovasc Surg 2007;55:445–9.
58. Noyes J, Gough D, Lewin S, et al. A research and developmentagenda for systematic reviews that ask complex questions aboutcomplex interventions. J Clin Epidemiol 2013;66:1262–70.
Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015 9
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from

59. Greco M, Capretti G, Beretta L, et al. Enhanced Recovery Programin Colorectal Surgery: A Meta-analysis of Randomized ControlledTrials. World J Surg 2014;38:1531–41.
60. Neville A, Lee L, Antonescu I, et al. Systematic review of outcomesused to evaluate enhanced recovery after surgery. Br J Surg2014;101:159–71.
61. Nicholson A, Lowe MC, Parker J, et al. Systematic review and meta-analysis of enhanced recovery programmes in surgical patients. Br JSurg 2014;101:172–88.
62. Pearsall EA, Meghji Z, Pitzul KB, et al. A qualitative study tounderstand the barriers and enablers in implementing an enhancedrecovery after surgery program. Ann Surg 18 Mar 2014. Epub aheadof print.
63. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry(Chaired by Robert Francis QC). London: The Stationery Office,2013.
64. Lee L, Li C, Landry T, et al. A systematic review of economicevaluations of enhanced recovery pathways for colorectal surgery.Ann Surg 2014;259:670–6.
65. Carroll C, Patterson M, Wood S, et al. A conceptual framework forimplementation fidelity. Implement Sci 2007;2:40.
66. Coolsen MME, van Dam RM, van der Wilt AA, et al.Systematic review and meta-analysis of enhanced recovery afterpancreatic surgery with particular emphasis onpancreaticoduodenectomies: supplementary material. World J Surg2013;37:1909–18.
10 Paton F, et al. BMJ Open 2014;4:e005015. doi:10.1136/bmjopen-2014-005015
Open Access
on August 18, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-005015 on 22 July 2014. D
ownloaded from