Embed Size (px)
Citation preview

TRUST BOARD AGENDA(open to members of the public and the press)
DATE: Wednesday 23 November 2016
TIME: 1300 -1400 (approx.)
VENUE: Boardroom, executive officees, 2nd
floor, Royal Free Hospital
Distribution
CHAIR: Dominic Dodd Chairman of the trust board
TRUST BOARDMEMBERS:
Stephen Ainger Non-executive director
Deborah Oakley Non-executive directorJenny Owen Non-executive directorVacant Non-executive directorDavid Sloman Chief executive
Caroline Clarke Chief finance officer and deputy chief executive
Prof Stephen Powis Medical director
Deborah Sanders Director of nursingKate Slemeck Chief operating officer
INVITED TO ATTENDDr Mike Greenberg Divisional director of women’s and children’s
servicesDavid Grantham Director of workforce and organisational
developmentDr Robin Woolfson Divisional director of transplant and specialist
servicesEmma Kearney Director of corporate affairs and communicationsAndrew Panniker Director of capital and estatesPeter Ridley Director of planningDr Steve Shaw Divisional director of urgent careAlison Macdonald Board secretary (minutes)Dr Chris LaingMM Devaney
Associate medical director – patient safetyHead of patient safety(for item 2016/199 only)
APOLOGIES Prof Anthony Schapira Non-executive directorProf George Hamilton Divisional director of surgery and associated
servicesCOPY FORINFORMATION:
Governors (agenda only)
Angela Attah Interim trust secretary

TRUST BOARD MEETING1
The next meeting of the trust board will take place on Wednesday 23 November 2016 at 1300 in the boardroom,executive offices, 2nd floor, Royal Free Hospital.
Dominic DoddChairman
A G E N D A
ITEM LEAD PAPER
ADMINISTRATIVE ITEMS
2016/194 Apologies for absence – A Schapira, George Hamilton D Dodd
2016/195 Declaration of interests D Dodd 1.
2016/196 Minutes of meeting held on 19 October 2016 D Dodd 2.
2016/197 Matters arising report D Dodd 3.
2016/198 Record of items discussed at the Part II board meeting on 19October 2016
D Dodd 4.
PATIENT SAFETY AND EXPERIENCE
2016/199 Quality improvement/patient safetyPatient safety programme overview and update
S PowisC LaingMM Devaney
2016/200 Patients’ voices S Powis
ORGANISATIONAL AGENDA
2016/201 North Central London sustainability and transformation plan P Ridley 5.
2016/202 Nursing/midwifery staff monthly report (September 2016) D Sanders 6.
OPERATIONAL AGENDA
2016/203 Chair’s and chief executive’s report D Dodd /D Sloman
7.
2016/204 Trust performance dashboard K Slemeck 8.
2016/205 Financial performance report C Clarke 9.
Governance and regulation: reports from board committees
2016/206 Shadow group board (13 October and 10 November 2016) D Dodd 10.
2016/207 Finance, investment and performance committee (18 October and15 November 2016)
D Dodd 11.
2016/208 Patient and staff experience committee (17 October 2016) J Owen 12.
2016/209 Audit committee (10 November 2016) D Oakley Verbal
1 In accordance with the Health & Social Care Act 2012, all Trust Board meetings must be held in public. All decisions which require the board’scollective approval can only be made at a Trust Board (or a Part II meeting held in closed session to discuss confidential matters).
OTHER BUSINESS
2016/210 Questions from the public D Dodd
2016/211 Any other business D Dodd
2016/212 Date of next meeting – 22 December 2016 D Dodd

Paper 1
Register of interests – trust board November 2016 1
REGISTER OF INTERESTS OF MEMBERS OF THE BOARD OF DIRECTORS
Executive summary
The trust constitution requires trust board members to declare interests which are relevant andmaterial to the NHS board of which they are a member. The register of interests is presented ateach board meeting.
The chief executive has made some additional declarations since the last board meeting.
Action required
Board members are asked to provide an update if they have any other changes in interests notnoted in the attached.
Board members are asked to declare any interests which are relevant to matters on the boardagenda.
The board is asked to ratify the updated register, subject to any further changes made.
Public Patient andCarer involvement
The register will be made available to the public.
Report From Dominic Dodd, chairmanAuthor(s) Alison Macdonald, board secretaryDate 15 November 2016
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 1
Version 9Updated 14/11/16
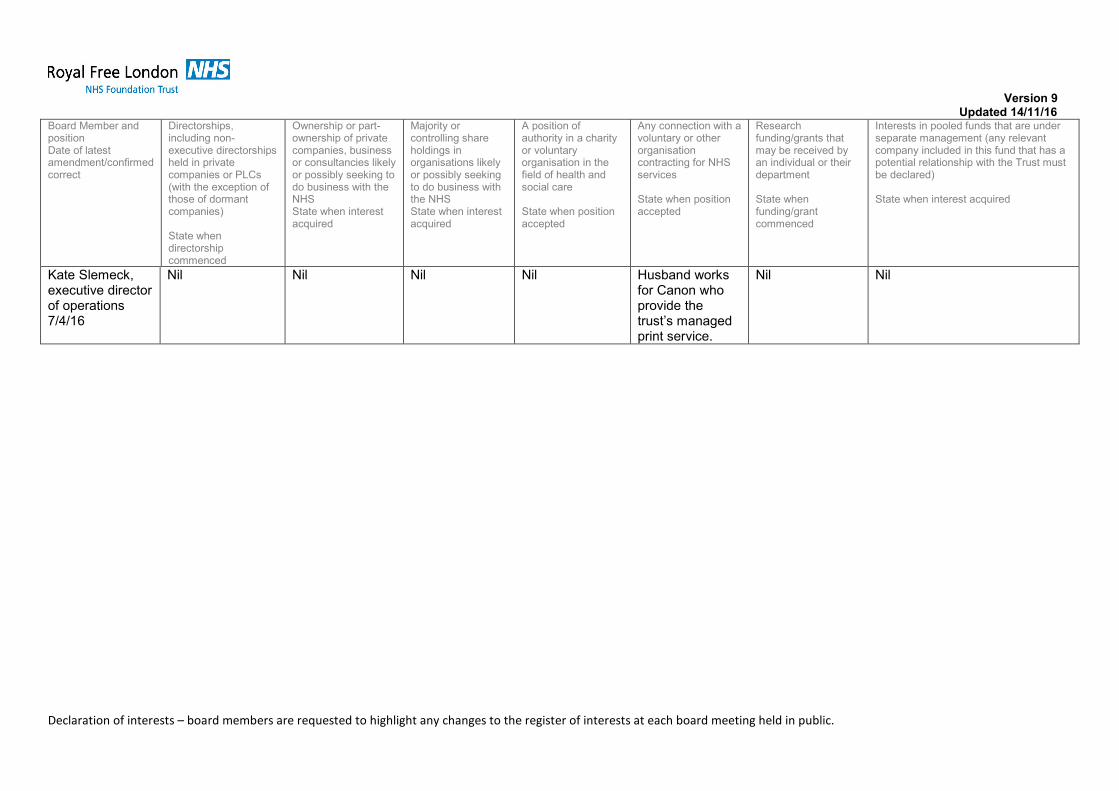
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
REGISTER OF THE INTERESTS OF MEMBERS OF THE TRUST BOARD
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Dominic Dodd,Chair8/4/16
UCLPartners1
Director of ownconsultancy firm
ImprovementDirector for trust inNHSI’s financialspecial measuresprogramme,assigned toCroydon HealthServices.Assignmentequivalent to circa5 days, to becompleted by endOctober 2016.Paid position.
Member of NHSI’sChairs’ AdvisoryGroup. Unpaidposition.
Nil Nil Nil Nil
1The Company’s constitutional documents have been drafted in accordance with charity law and Charity Commission guidance, so that the Company can apply for charitable status in the
future as and when its Board of Directors considers this appropriate.

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Non-executive directors
Stephen AingerNon-executivedirector5/1/16
Chair DownshireHill Residents’Association.
Nil Nil Nil Nil Nil Nil

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Deborah Oakley,non-executivedirector13/5/16
Medicines andHealthcareProductsRegulatoryAgency Non-ExecDirector
Nil Nil Nil Medicines andHealthcareProductsRegulatoryAgency Non-Exec Director
Nil I work for Veritas InvestmentManagement. The firm investsmoney on behalf of clients. Clientportfolios are invested in varioushealthcare companies whichmay do business with the trustand with the NHS more broadly.These investments include butare not limited to: SonicHealthcare; Roche; Novartis;GlaxoSmithKline, United Health,Alphabet, Oracle and others.Clients also invest in pooledfunds which are managedexternally and invest in a broadrange of healthcare companieswhich may do business with thetrust and the NHS.I and my family have personalholdings in pooled funds whichare managed externally andinvest in a broad range ofhealthcare companies whichmay do business with the trustand the NHS.I do not have any directinvestments in companies whichmay do business with the trust orwith the NHS.

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Jenny Owen,non-executivedirector6/4/16
Nil Nil Nil Board memberof Housing andCare 21
Trustee ofAlzheimer’sSociety
Housing 21 andCare 21
Alzheimer’sSociety
Nil Nil
ProfessorAnthony SchapiraNon-executivedirector13/5/16
Upper HampsteadWalk Residents’Association.AHV Schapira Ltd
Non-executivedirector, Ministryof Justice
Nil Nil Parkinson’sDisease SocietyResearchStrategy Group
Nil MedicalResearchCouncil,Wellcome Trust,Parkinson’sDisease Societyand othercharitablesources ofresearch funding
Nil
Executive directors
Caroline ClarkeDeputy chiefexecutive &director offinance11/4/16
Member, AdvisoryBoard to TheLearning Clinic
Nil Nil Trustee
Royal FreeCharity (1/4/16)
Nil Nil Nil

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Professor
Stephen Powis,
medical director
16/5/16
Director of HSL
(appointed by
RFL)
Nil Nil Employee of
UCL
Trustee
Peter Samuel
Trust
Trustee
Healthcare
Management
Trust
Trustee
Moorhead Renal
Trust
Trustee
Royal Free
Charity (1/4/16)
Member ofgoverning body,Merton NHSClinicalCommissioningGroup
Trustee
Healthcare
Management
Trust
Moorhead RenalTrust and variousother sources ofcharitable fundingheld bycolleagues withinthe academicrenal department
No individualfunding butcollaborate onresearch withinacademicresearchdepartmentfunded by avariety of sourceseg MRC, KidneyResearch UK.
Nil
Deborah SandersDirector ofnursing16/1/13
Nil Nil Nil Board member,The Royal FreeHospital Nurses’Home of RestTrust
Nil Nil Nil
Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Kate Slemeck,executive directorof operations7/4/16
Nil Nil Nil Nil Husband worksfor Canon whoprovide thetrust’s managedprint service.
Nil Nil

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
David SlomanChief executive15/11/16
Director,
UCLPartners2
Trustee/Non-executive director,Skills for Health
Chair of North
Central London
Sustainability and
Transformation
Plan
Nil Nil LondonProcurementPartnershipboard member.
Relative whoworks for Ernst &Young
Member of HSJ’sProduct AdvisoryBoard
Member of NHSImprovementCEO AdvisoryGroup (January2016)
Membership ofDeloitteAcademy
Member ofinternationaladvisory board ofThe NationalInstitute forHealth ResearchCollaboration forLeadership inApplied HealthResearch andCare (NIHRCLAHRC)
Nil Nil
2The Company’s constitutional documents have been drafted in accordance with charity law and Charity Commission guidance, so that the Company can apply for charitable status in the
future as and when its Board of Directors considers this appropriate.

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Non-voting directors
David Grantham
Director of
Workforce and
OD
7/4/16
Nil Nil Nil Board Member
and Treasurer
London
Healthcare
People
Management
Academy –
March 2013
Chair of NHS
Employers
Medical
Workforce
Forum – August
2010
Board MemberHealth EducationNorth and EastLondon(HENCEL) – July2014Board Memberand TreasurerLondonStreamliningProgramme(s) –March 2014
Nil Nil
Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
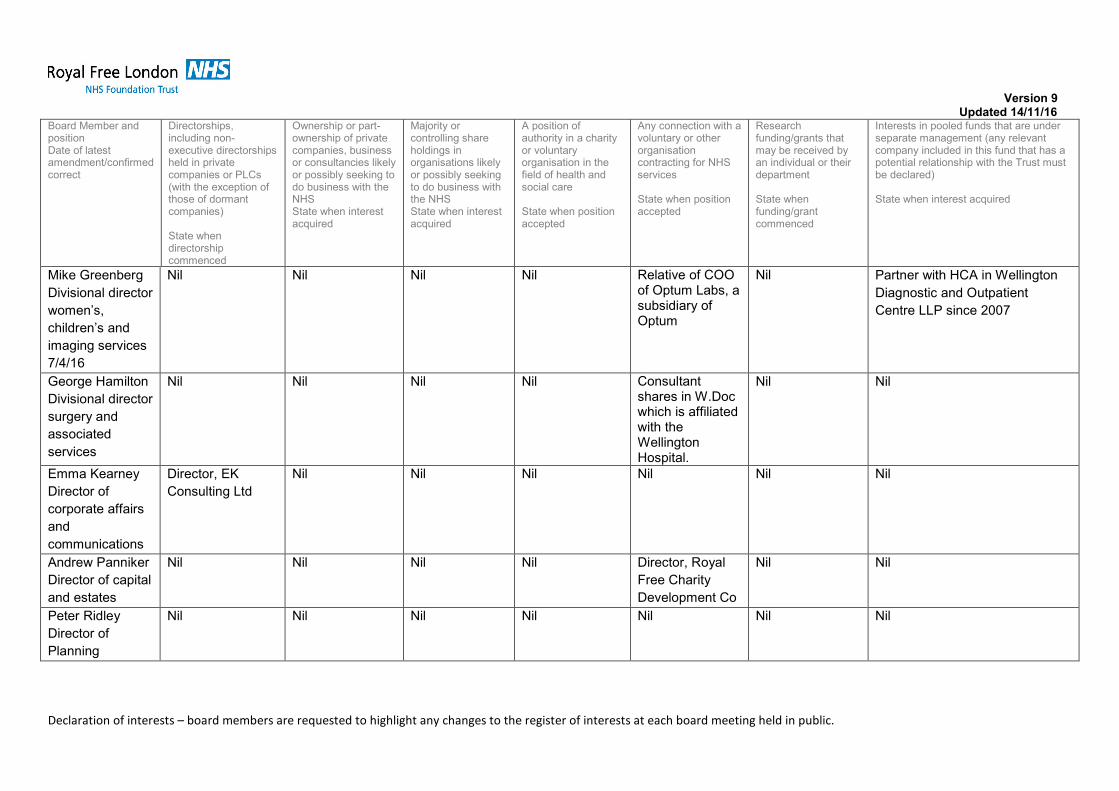
Mike Greenberg
Divisional director
women’s,
children’s and
imaging services
7/4/16
Nil Nil Nil Nil Relative of COOof Optum Labs, asubsidiary ofOptum
Nil Partner with HCA in Wellington
Diagnostic and Outpatient
Centre LLP since 2007
George Hamilton
Divisional director
surgery and
associated
services
Nil Nil Nil Nil Consultantshares in W.Docwhich is affiliatedwith theWellingtonHospital.
Nil Nil
Emma Kearney
Director of
corporate affairs
and
communications
Director, EK
Consulting Ltd
Nil Nil Nil Nil Nil Nil
Andrew Panniker
Director of capital
and estates
Nil Nil Nil Nil Director, Royal
Free Charity
Development Co
Nil Nil
Peter Ridley
Director of
Planning
Nil Nil Nil Nil Nil Nil Nil

Version 9Updated 14/11/16
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member andpositionDate of latestamendment/confirmedcorrect
Directorships,including non-executive directorshipsheld in privatecompanies or PLCs(with the exception ofthose of dormantcompanies)
State whendirectorshipcommenced
Ownership or part-ownership of privatecompanies, businessor consultancies likelyor possibly seeking todo business with theNHSState when interestacquired
Majority orcontrolling shareholdings inorganisations likelyor possibly seekingto do business withthe NHSState when interestacquired
A position ofauthority in a charityor voluntaryorganisation in thefield of health andsocial care
State when positionaccepted
Any connection with avoluntary or otherorganisationcontracting for NHSservices
State when positionaccepted
Researchfunding/grants thatmay be received byan individual or theirdepartment
State whenfunding/grantcommenced
Interests in pooled funds that are underseparate management (any relevantcompany included in this fund that has apotential relationship with the Trust mustbe declared)
State when interest acquired
Steve Shaw
Divisional director
urgent care
7/4/16
Nil Nil Nil Nil Nil Nil Nil
Will Smart
Chief information
officer
8/4/16
Nil Nil Nil Nil Nil Nil Nil
Robin Woolfson,
Divisional director
transplant and
specialist
services
Nil Nil Nil Nil Nil Nil Nil

Paper 2
1
MINUTES OF THE TRUST BOARD
HELD ON 19 OCTOBER 2016
Present
Mr D DoddMr S AingerMs C ClarkeMs D OakleyMs J OwenProf S PowisMs D SandersProf A SchapiraMs K SlemeckMr D Sloman
ChairmanNon-executive directorChief finance officer and deputy chief executiveNon-executive directorNon-executive directorMedical directorDirector of nursingNon-executive directorChief operating officerChief executive
Invited to attendMr D GranthamDr M GreenbergProf G HamiltonMs E KearneyMr A PannikerMr P RidleyDr S ShawMs A Macdonald
Director of workforce and organisational development (from 2016/158)Divisional director for women’s, children’s and imaging servicesDivisional director for surgery and associated servicesDirector of corporate affairs and communicationsDirector of capital and estatesDirector of planningDivisional director – urgent careBoard secretary (minutes)
Others in attendanceDr Anja DrebesMs H Wain
Ms Yvonne CarterMr David MyersCllr Peter Zinkin
Consultant haematologist and clinical lead for thrombosis and anticoagulation (foritem 2016/178)Deputy director of patient safety and risk (for item 2016/178)Head of infection prevention and control nursing (for item 2016/181)Elected patient governorAppointed governor
2016/173 APOLOGIES FOR ABSENCE AND WELCOME Action
Apologies for absence were received from:
Dr R Woolfson Divisional director, transplant and specialist services
The chairman welcomed those present to the meeting.2016/174 DECLARATION OF INTERESTS
The report on the register of interests was noted and entries confirmed to becorrect. No director had any further interests to declare.
2016/175 MINUTES OF MEETING HELD ON 28 SEPTEMBER 2016
The minutes were accepted as an accurate record of the meeting, subject to thefollowing amendment:

Paper 2
2
2016/169 Audit committee
Amend 5th bullet point to read: “The committee self-evaluation had beendiscussed, which had been generally positive but raised the issue of thecomposition of the committee. The committee noted that the trust was in theprocess of recruiting two non-executive directros and would await the outcome ofthe recruitment process before making a recommendation to the board.”
2016/176 MATTERS ARISING REPORT
The matters arising report was noted.2016/177 RECORD OF ITEMS DISCUSSED AT PART II BOARD MEETING ON 28
SEPTEMBER 2016
The report was noted.
2016/178 QUALITY IMPROVEMENT/PATIENT SAFETY – VENOUSTHROMBOELMBOLISM (VTE) PREVENTION PROGRAMME
Dr Anja Drebes, consultant haematologist and clinical lead for thrombosis andanticoagulation, and Ms H Wain, deputy director of patient safety and risk, were inattendance for this item.
Dr Drebes explained that there had been significant under-recognition of venousthromboembolism (VTE) which was an acute problem leading to significantissues. It was thought to account for 25,000 deaths each year and about 10% ofhospital deaths. In 2005 the Health Select Committee had investigated hospital-acquired thrombosis, and made a series of recommendations to reduce it.
Following this, locally, a thrombosis committee had been established and a riskassessment tool had been implemented, which was used for all inpatients,completed daily and reported upon to the thrombosis committee. A 95% targethad been set for completion of risk assessments and was the subject of a CQUINwith a value of £1.6m The trust had met this within 12-18 months. The target wasnow part of the NHS contract.
Another strand of the work was that all hospital acquired thrombosis cases wereidentified and subject to root cause analysis.
In 2015/16 there had been 27 cases at the Royal Free Hospital out of admissionsof circa 200,000. This was compared with 38 cases in 2011/12.
Concluding her presentation, she stated that the trust had done well with the VTEprogramme but given the expanded organisation this might be a challenge tomaintain and improve upon.
Ms Oakley, non-executive director asked whether the introduction of electronicprescribing would help. Dr Drebes responded that it would still require clinicalreview and intervention but that a promising start had been made working withCerner to build VTE prevention into the system.
Mr Ainger, non-executive director, asked if benchmark data was available. DrDrebes responded that hospital acquired thrombosis had not been systematicallyrecorded prior to the introduction of the CQUIN, but that the number of cases had

Paper 2
3
reduced since this.
Ms Owen, non-executive director, asked whether in view of the capacity issuesand the need for more patient education and information, there was a role forpatient support groups. Dr Drebes responded that if patients had questions orconcerns it was important that they receive advice from a healthcare professionaland that this was an integral part of the care delivered by ward staff.
The chairman thanked Dr Drebes for coming to the board and providing such aninteresting and informative presentation.
2016/179 PATIENTS’ VOICES
The divisional director – urgent care read out a complaint and a compliment.
The compliment was from a patient who had been admitted to the Royal FreeHospital through the emergency department under the care of thegastroenterology team. They said that they had received nothing but the bestcare from the doctors and the team supporting them – nurses, technicians andauxiliary staff. They also thanked the hospital for saving their daughters life whenshe was admitted for a pulmonary embolism.
The complaint was from the daughter of a patient with dementia who had come tothe emergency department at the Royal Free. She explained that her motherwould find having an X ray very traumatic, but this was ignored and her motherbecame even more distressed, which was not dealt with appropriately resulting inher mother becoming even more distressed.
The medical director would present this item next time. Medicaldirector
2016/159 NURSING AND MIDWIFERY STAFFING MONTHLY REPORT
The director of nursing presented the report which covered August 2016 andnoted planned versus actual hours was 1% less actual than planned across allthree sites. There had been five shifts or part shifts where the nurse: patient ratiowas below 1:8 on a day shift or 1:11, with no patient safety incidents reported.
The board had noted the family and friends test (FFT) scores on Adelaide andCapetown wards at the last meeting. Capetown had improved but Adelaide’sAugust score was 57%. This was based on 7 responses, with two of the threenegative responses referring to noise on the ward at night and the other to theresponse of staff to patients’’ needs. Improvement actions were in place. Thetrust would also be developing new ways to measure patient satisfaction,informed by work at Northumbria Healthcare NHS Foundation Trust which hadbeen presented to the patient and staff experience committee.
The year to date spend on nursing and midwifery agency was £97K above plan,with particular issues in the emergency departments and intensive care. Therewas a good recruitment pipeline for emergency care but the position for ITU wasmore worrying with 32 nurses in the pipeline. ITU was experiencing a highnumber of admissions and high acuity with units full most of the time. Howevershe was pleased to report that all agency rates were now under the cap.

Paper 2
4
Additional controls had been put in place for approval of agency staff and a newlevel of scrutiny would be given to study leave, with some difficult decisions to bemade.
Regarding recruitment, two assessment centres and one open day were beingheld every month and a careers clinic had started with the aim of encouraging andsimplifying internal staff transfers. So far six nurses had taken advantage of this,who would otherwise have left the trust. The trust had also been identified as oneof 11 test sites for developing the nurse associate role.
In answer to a question from Ms Oakley, non-executive director, she respondedthat the net recruitment position was probably just positive, but she would includefurther information in the next report.
Mr Ainger, non-executive director, asked whether any impact from Brexit wasbeing seen. The director of nursing responded that some nurses who had beenrecruited from the EU had changed their minds. Mr Ainger then asked about fallson Juniper and ward 8 West and the director of nursing advised that none ofthese had been falls with harm.
Ms Owen, non-executive director, asked the director of nursing to think about howFFT could be captured in the emergency department, and the director of nursingagreed to take this forward.
Ms Owen then asked about the outcome of the nurse shift pattern consultation.The director of nursing stated that the outcome document was being publishedthat day. As a result to the response to consultation, a short life group would beset up to look at how to ensure staff were able to take their breaks. In addition formost departments the shift pattern would be harmonised to staff working 14 shiftsa month, but for staff in the emergency department, maternity, neonates and ITUthey would work 13 shifts one month and 14 shifts the next. Although the primaryaim had not been to save money, the original proposal would have savedapproximately £3m per annum; the revised arrangements would still result in asaving albeit reduced.
The board agreed that the report provided sufficient assurance that the nursestaffing levels were meeting the needs of patients and providing safe care.
Directorofnursing
Directorofnursing
2016/181 DIRECTOR OF INFECTION PREVENTION AND CONTROL QUARTERLYREPORT
The head of infection prevention and control nursing was in attendance for thisitem.
The director of nursing reported that the trust had been under trajectory for C.diffin quarter 1 with 15 cases; however in quarter 2 there had been 23 cases whichwas 5 above trajectory. Two lapses in care had been identified, both on Cedarward and transmission cases. Actions included removing clutter, increasedcleaning, decontamination using vaporised hydrogen peroxide (VHP) andincreased practice educator input. She also reported that surgical site infectionsurveillance above mandatory requirements had been commenced as a newappointment had been made.
There was discussion about airflow in the operating theatres at Chase Farm

Paper 2
5
Hospital and it was noted that tests would be carried out six monthly, rather thanannually, and more frequently if the minimum 75% air change was not beingachieved.
The director of nursing reported that uptake of the flu vaccine was currently 21%which was not as good as she wanted it to be. However there were more peervaccinators trained then previously and the vaccination team were undertaking acomprehensive programme of vaccinations.
Ms Oakley asked if more information about the antibiotic CQUIN could beincluded in the next report.
Ms Owen, non-executive director, asked about cleaning standards at BarnetHospital. The director of capital and estates advised that this was part of the PFIcontract and delivered by Medirest. The trust had concerns about the standards,methodology and products used and these were being pursued with the company.The PFI contract was also being reviewed, with independent advice. Ms Owenasked for further information on this to be provided to the board.
The board noted the report.
Directorofnursing
Directorof capitalandestates
2016/182 MEDICAL APPRAISAL SIX MONTHLY REPORT
The medical director presented the report. He commented that he would bereviewing the way the data was presented to the board to make the overallappraisal rate clearer. Currently the focus was on doctors whose appraisal hadbeen either been missed or delayed the previous year.
The board noted the report.2016/183 CHAIR AND CHIEF EXECUTIVE’S REPORT
The chief executive highlighted the following points from the report:
• The Chase Farm Hospital redevelopment was slightly ahead of scheduleand on budget. In answer to a question he said that the cost reductionsfrom staff changes were also ahead of plan.
• The RFH outpatients refurbishment had commenced and was beingfunded by the Royal Free Charity. Refurbishment of the ground floorpublic toilets had also commenced.
• The patient transport service continued to be an improvement on theprevious position but was still being closely managed.
The board noted the report.
2016/184 TRUST PERFORMANCE DASHBOARD
The chief operating officer noted that the A&E and cancer remained particularperformance challenges. A&E performance was being driven by a combination ofincreased attendances and patient flow issues, particularly a high number ofdelayed transfers of care. The trust was launching the ‘safer faster better’programme which was directed at streaming within the emergency departmentand improving flow through the hospital. There would also be changes in thefront end at Barnet Hospital and the trust was working with the CCG to introduce

Paper 2
6
discharge to assess. Regarding cancer, a trajectory was in place, and the trustwas on track, to return to compliance by December 2016. She noted thatapproximately half the tumour sites were compliant, but some of the high volumesites were not yet compliant.
The board noted the report.
2016/163 FINANCIAL PERFORMANCE REPORT
The chief finance officer reported the trust was £30m adverse to plan at the end ofquarter 2. A large part of this was due to the loss of prior year income of £17m,alongside under-achievement of the private patients unit income,underperformance against activity income, pay overspends and a high level ofoutsourcing costs. The trust’s cash position was also a matter for seriousconcern. The trust executive committee had a detailed discussion of the financialposition earlier in the week and had agreed a series of actions to improve theposition and a revised year end forecast would be required.
The board noted the report.
2016/186 SHADOW GROUP BOARD REPORTThe chairman did not have anything to report from the committee in advance ofthe written report which would be provided to the next board meeting.
2016/187 FINANCE INVESTMENT AND PERFORMANCE COMMITTEE REPORT
The board agreed to discuss the governance statements in the context of thefinancial position in the confidential board meeting and that the statements wouldthen be noted in the minutes.
[Post meeting note
The board could not confirm the statement that:
The board anticipates that the trust will continue to maintain a financialsustainability risk rating of at least 3 over the next 12 months.
The board anticipated that it would have an overall rating of 1 for Q2 (with a riskrating of 2 for quarter 3 and a risk rating of 1 for quarter 4).
The board confirmed the statement that:
The board is satisfied that plans in place are sufficient to ensure: ongoingcompliance with all existing targets (after the application of thresholds) as set outin Appendix A of the Risk Assessment Framework, other than the 62 day cancertarget and the A&E target; and a commitment to comply with all other knowntargets going forwards.]
2016/188 PATIENT SAFETY COMMITTEE REPORT
The board noted the report from the committee.

Paper 2
7
2016/189 PATIENT AND STAFF EXPERIENCE COMMITTEE REPORT
The committee chair provided a verbal report on the previous meeting had beengiven over to a seminar on patient engagement and experience with the patientexperience and engagement lead from Northumbria. There had been a very goodturnout and the presentation had been inspirational. The trust had massivelyincreased the number of staff who thought that improving the patients experiencewas the top priority and had also developed very effective ways of gaining ‘realtime’ and ‘right time’ feedback.
The committee had also agreed to recommend to the board that the followingrisks be removed from the board assurance framework:
• 1b/3b – Patient transport – now being monitored as BAU.
• 2b – General staff experience risk – specific areas of concern are
highlighted elsewhere e.g. 2a/2c
• 6b – Overhead coverage for specialised services – risk abated following
agreement of 2016/17 contracts
The board agreed to this.2016/190 AUDIT COMMITTEE
The board noted the report from the committee.
2016/191 QUESTIONS FROM THE PUBLIC
Cllr Zinkin, appointed governor, asked about parking at Barnet Hospital. Thedirector of capital and estates advised that the trust was required to provide amasterplan for Barnet Hospital including key worker accommodation and a multi-storey carpark. In the meantime the trust was going to investigate the removal ofcycling lanes on the site in order to create more parking spaces. There washowever inconsistency between London Borough of Barnet and Greater LondonAuthority in terms of requirements for cycling lanes.
Mr Myers, patient governor, noted that DeepMind was on the part II agenda. Heexpressed strong support for the trust working with DeepMind having attendedthe DeepMind event for patients and seen the huge potential benefits for patients.The chairman noted that there were commercial and contractual reasons for theboard discussing the contract in private but this would be brought into the publicdomain as soon as possible.
2016/192 ANY OTHER BUSINESS
There was no other business.2016/193 DATE OF NEXT MEETING
The next trust board meeting would be on 23 November 2016 at 1300 in theboardroom, executive offices, 2nd floor, Royal Free Hospital.
Agreed as a correct record
Signature …………………………………..date 23 November 2016…………………………….Dominic Dodd, chairman

Paper 3
Matters arising – trust board 23 November 2016
Trust BoardMatters Arising report as at 23 November 2016
Actions completed since last meeting of the Trust Board
MinuteNo
Action Lead Complete Board date/agenda item
Outstanding
FROM TRUST BOARD HELD ON 19 OCTOBER 20162016/180 NURSING AND MIDWIFERY STAFFING
MONTHLY REPORTInclude further information on net recruitmentposition in the next report.
Consider how FFT could be captured in theemergency department.
D Sanders Update to be provided at board meeting.
2016/181 DIRECTOR OF INFECTION PREVENTION ANDCONTROL QUARTERLY REPORTMs Oakley asked if more information about theantibiotic CQUIN could be included in the nextreport.
Ms Owen, non-executive director, asked for moreinformation about the review of the PFI contract
D Sanders
A Panniker
Next report due January 2017
Review in progress, update to be provided toboard in December 2016
FROM TRUST BOARD HELD ON 28 SEPTEMBER 20162016/170 Questions from the public – falls information
Raise this at CQRG S Powis/D Sanders
FROM TRUST BOARD HELD ON 27 APRIL 20162016/77 Patient safety committee report
Board to receive training on corporatemanslaughter
S Powis Programmed for November 2016 meeting

Paper 3
Matters arising – trust board 23 November 2016
FROM TRUST BOARD HELD ON 6 APRIL 20162016/54 Chairman and chief executive’s report
Progress reports on pathology joint venture to theshadow group board and finance and performancecommittee.
M Dinan Agreed at May shadow group board that thisshould be programmed for July, following acustomer/investor annual review. Deferred toSeptember as HSL annual accounts notreceived. Report discussed at financeinvestment and performance committee inSeptember and further work required. Nowprogrammed for December trust boardmeeting.

Paper 4
Confidential trust board meeting update – trust board 19 October 2016
ITEMS DISCUSSED AT THE CONFIDENTIAL BOARD MEETING HELD ON 19 OCTOBER2016
Executive summary
Decisions taken at a confidential trust board are reported where appropriate at the next trustboard held in public. Those issues of note and decisions taken at the trust board’s confidentialmeeting held on 19 October 2016 are outlined below.
• North Middlesex University Hospital partnership update
The board also had a detailed discussion of the trust’s financial position and discussed the trustperformance report.
Action required
For the board to note.
Report From D Dodd, chairmanAuthor(s) A Macdonald, board secretaryDate 10 November 2016
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 4

Paper 5
Page 1 of 4
North Central London (NCL) sustainability and transformation plan (STP): 30 June
submission
Introduction
This report provides an overview of the published North Central London (NCL) Sustainabilityand Transformation Plan (STP).
The documents submitted are appended to this cover note and are:• The draft NCL STP strategic narrative submitted to NHS England on 21 October
2016;• NCL STP summary document
Sustainability and Transformation Plan
The draft Sustainability and Transformation Plan (STP) has been produced by all the mainhealthcare organisations and local authorities within North Central London. It sets out plansto meet the challenges faced locally and to deliver high quality and sustainable services inthe years to come.
The vision for the STP is for North Central London to be a place with the best possible healthand wellbeing, where no one gets left behind.
The clinical case for change within the STP describes the changing health and care needs oflocal people and the key issues facing health and care services in North Central London. Itwill be used to guide the transformation of local services over the next five years.
The clinical case for change in the STP is aligned to address the gaps identified in the FiveYear Forward Plan for health and wellbeing, care and quality, and finance.
To support delivery of the vision for the STP and address the clinical case for change aprogramme of transformation has been designed with four fundamental aspects:• Prevention: We will increase our efforts on prevention and early intervention to improve
health and wellbeing outcomes for our whole population;• Service transformation: To meet the changing needs of our population we will transform
the way that we deliver services;• Productivity: We will focus on identifying areas to drive down unit costs, remove
unnecessary costs and achieve efficiencies, including working together acrossorganisations to identify opportunities to deliver better productivity at scale;
• Enablers: We will build capacity in digital, workforce, estates and new commissioning anddelivery models to enable transformation.
Delivering these plans will result in improved outcomes and experience for the localpopulation, increased quality of services and significant savings.
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 5

Paper 5
Page 2 of 4
The STP is still work in progress. Despite the development of the plans for prevention,service transformation, productivity and enablers the draft STP submitted on 21 October2016 showed an overall £75m deficit in 2020/21 across NHS organisations. A number ofareas for further work have been identified between now and Christmas where additionalsavings can be found to address this residual gap.
To ensure overall delivery as a system, a robust governance structure is being developed toenable NHS and local government partners to work together in new ways to driveimplementation.
It is crucial that the whole system is aligned around delivery of the STP and work isunderway to ensure that the development of the two-year health contracts that are being putin place for 2017/18 - 2018/19 are consistent with the STP strategic framework.
There is more work to do to finalise the granular detail of our delivery plans and address theresidual challenge forecast. Development of plans in more detail will involve full engagementof people who use services and the public to ensure those plans are reflective of their needs.There is a commitment to being radical in approach, to focusing on improving populationhealth and delivering the best care in London. Our population deserves this, and we areconfident that we can deliver it.
The draft North Central London Sustainability and Transformation Plan therefore articulates:
• The health and social care landscape, and its complexity;• The collective understanding of the challenges faced through the clinical case for change;• The vision for health and care in NCL in 2020/21;• The plans to deliver the vision and address the challenges, and the delivery framework
that will enable implementation of those plans;• The impact expect to be achieved through the delivery of the plans;• Supporting governance arrangements;• Plans for securing broader public support and engagement with the STP proposals;• Next steps for further developing proposals and responding to our residual financial gap.
Workstream delivery plans
Submission of the draft NCL Sustainability and Transformation Plan is supported by thedevelopment of workstream delivery plans.
The workstreams focus on identified priorities for joint working across North Central Londonand focus on:
1. Prevention: We will increase our efforts on prevention and early intervention to improvehealth and wellbeing outcomes for our whole population:• This includes a focus on population health, particularly in areas that will support
improved outcomes and reduced costs within the five-year period of the STP –smoking, alcohol ,obesity, falls and sexual health (use of long-term contraception andearlier diagnosis of HIV);
• A focus on a workforce for prevention including mental health first aid, dementiaawareness, and the making every contact count programme;
• A focus on healthier environments including workplace wellbeing and an environmentto help reduce childhood obesity.
2. Service transformation: To meet the changing needs of our population we will transformthe way that we deliver services:• A focus on developing out of hospital services and providing health and care closer to
Paper 5
Page 3 of 4
home. This includes the development of urgent care and primary care services;• Development of mental health services for adults and children;• Urgent and emergency care including an integrated urgent care system;• Optimising elective care pathways including outpatient activity;• Consolidation and/or networking of services following the previous template in London
for stroke and trauma services;• Cancer pathways including earlier diagnosis and improving patient experience.
3. Productivity: We will focus on identifying areas to drive down unit costs, removeunnecessary costs and achieve efficiencies, including working together acrossorganisations to identify opportunities to deliver better productivity at scale through a focuson:• Workforce (skill-mix; shared recruitment and bank functions, increase retention);• Reducing operational and clinical variation including a response to recommendations in
the Carter Report;• Procurement efficiencies by acting at scale;• Sharing back office functions;• Reducing contract and transaction costs including new commissioning and contract
models;• Cost improvement schemes including theatre productivity.
4. Enablers: We will build capacity in digital, workforce, estates and new commissioning anddelivery models to enable transformation. This will be dome through workstreams for:• Workforce including the use of integrated employment models, developing new roles
to support new models of care, and enabling productivity opportunities;• Digital maturity including interoperability across providers as envisaged with the “Care
My Way” programme in Islington;• Estates including developing an overarching estates strategy, optimising the use and
quality of estate across health and care services, supporting delivery of new models ofcare by delivering linked improvements to the health and care estate, and creatingpartnership working between commissioners and providers to align incentives forestate release and support delivery of devolved estates powers for the NHS andpartners.
5. Patient & public engagement: We have a commitment to work in an open and transparentway. The STP summary has been produced to support further engagement, in recognitionthat the full STP is a technical planning document. All organisations involved in the STP areasked to publish the full strategic narrative and summary on their websites to stimulatefeedback and engagement with patients, the public, staff and other stakeholders. Werecognise that engagement on the overall STP to date has been limited to the stakeholdermeetings held in each borough in September, although individual STP workstreams such asmental health have also engaged users of service in the development of their plans. We willnow develop an STP workstream on communications and engagement to ensure we buildactive and effective engagement into the further development and delivery of the STP.
Action required/recommendation:
• NOTE the North Central London Sustainability and Transformation Plan• SUPPORT the direction of travel and priorities for improving services and
outcomes set out in the STP.• COMMENT on next steps
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
1. Excellent outcomes – to be in the top 10% of our peers on

Paper 5
Page 4 of 4
outcomes
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the
organisation for the future
Risks attached to this project/initiative and how these will be managed (assurance)
Equality analysis
• No identified negative impact on equality and diversity
Report from David Sloman, chief executive
Author(s) Peter Ridley, Director of Planning
Date 15 November 2016
North Central London
Sustainability and Transformation Plan
A summary
North Central London
N C L

2NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
IntroductionHospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform the care we deliver to our patients.
On a scale never seen before, health and social care services in the region are working on the ‘North and Central London (NCL) Sustainability and Transformation Plan (STP)’.
Our work covers the five boroughs of Camden, Islington, Haringey, Barnet and Enfield – an area that is home to nearly 1.5 million people.
We know that the health and social care needs of our local people are changing, and that there are serious issues facing health and care services in NCL. People receive different standards of care depending on where they live: waiting times for services and health outcomes vary, and the quality of care and people’s experience of health and social services is sometimes not as good as it should be.
We must improve and we can only do this if we all work closely together – with each other and with our local residents.
It does not mean doing less for patients or reducing the quality of care provided. It means more preventative care - finding new ways to meet people’s needs, and identifying ways to do things more efficiently. We want to ensure that everybody we care for has greater control of their health and wellbeing and receives the support they need to live longer, healthier lives. Many of these ambitions are not new, but are based on what local people have told us they want.
The plan is currently work in progress. We are looking to engage with as many people as possible over the next few months to develop our ideas further.
John, age 62 is a lifetime smoker who was recently diagnosed with chronic bronchitis. His GP ad-vised him to stop smoking but John said he could not cope without his cigarettes and refused the offer of nicotine replacement therapy (NRT). John contracted a chest infection, went to A&E and was admitted. He stayed for several days, was given some NRT on the ward to cope with his cravings for cigarettes. In future, when John is admitted to hospital his respiratory physician will discuss the importance of stopping smoking as a treatment for his bronchitis. He will be prescribed NRT to relieve his cravings and on discharge he will be offered a referral to specialist stop smoking support for heavily addict-ed smokers. John will then get a call the next day from the specialist stop smoking advisor who will arrange a home visit for the following day. John will be supported by the specialist advisor in weekly visits to help him to reduce or stop smoking altogether.

3NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
What is the Sustainability and Transformation Plan (STP)?To make sure everybody receives the care they need when they need it, we have to change the way we do things.
Our draft plan sets out how we will work together to deliver high quality, sustainable services in the years to come and how we can meet the financial challenges and increasing pressures on our services over the next five years.
The North Central London area has a growing population and people are also living longer, often with long term health problems.
The growth in our funding over the next five years will not match the expected increases in population and the resulting growth in demand for health services. NHS services already have deficits and, if nothing changes, it is anticipated that the combined deficit of health services alone will be nearly £900million by 2020/21. Local authorities are also facing significant financial pressures on their social care budgets. We need to change how we provide services, reduce the amount of time and treatment spent in hospitals, boost prevention and offer more local people the care they need closer to home.

4NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
Enfield CCG / Enfield Council~320,000 GP registered pop~324,000 resident pop49 GP practices
Barnet CCG / Barnet Council~396,000 GP registered pop~375,000 resident pop62 GP practices
Haringey CCG / Haringey Council~296,000 GP registered pop ~267,000 resident pop45 GP practices
Islington CCG / Islington Council~233,000 GP registered pop~221,000 resident pop34 GP practices
Camden CCG / Camden Council~260,000 GP registered pop~235,000 resident pop35 GP practices
London Ambulance Service East of England Ambulance Service
Total health spend £2.5bn
Total care spend £800m
Primary care spend
£~180m
Specialist commissioning
spend £~730m
NHS England
Note: registered pop data shows 2014 figures. Source: ONS
Barnet Enfield and Haringey Mental Health NHS Trust (main sites, incl Enfield community)
Camden and Islington NHS Foundation Trust (and main sites)
North Middlesex University Hospital NHS Trust The Royal Free London NHS Foundation Trust University College London Hospitals NHS
Foundation Trust Whittington Health NHS Trust
(incl Islington and Haringey Community) Central and North West London NHS Foundation
Trust (Camden Community) Central London Community Healthcare NHS
Trust (Barnet Community) Specialist providers
Other specialist providers out of scope: Great Ormond Street Hospital, Moorfields Eye Hospital, Tavistock and Portman Foundation Trust, Royal National Orthopaedic Hospital
North Central London overview

5NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
What are we going to do to?There are a wide range of health problems in the region including high rates of childhood obesity and mental illness. Too many people are treated in hospital for long term conditions when they could be better cared for in the community. Waiting times to see a specialist and for diagnostic tests are long. Attendance levels at A&E departments are high and it’s difficult to recruit staff. We want to create a health and social care system which delivers positive outcomes in all of these areas, no matter where you live.
To help us achieve this, over the next five years we aim to:
Invest more in prevention to stop people getting ill
Work with people to help them remain independent and manage their own health
Give children the best possible start in life
Provide care closer to home so that people will only need to go to hospital when it is clinically necessary
Give mental health services equal priority to physical health services
Improve cancer services
Make the best standards available to all and reduce variation
Make north central London an attractive place to work so that we have the right workforce to deliver high quality services
Modernise our buildings and make greater use of digital technology
Ensure value for tax payers’ money through increasing efficiency and productivity, and consolidating and specialising where appropriate
PreventionWe aim to do more to promote and empower people to live healthy lives so we can stop the onset of disease, and keep people out of hospital. We want to increase investment in prevention and ensure that the places where people live and work promote good health.
We want to support residents, families and communities to look after their own health. We will work to diagnose residents with clinical risk factors and long term conditions much earlier to increase life expectancy.

6NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
Care closer to homeWe aim to deliver more health and care closer to home, so that people are treated in the best possible environment and do not have to go to hospital unless they really need to.
This would be achieved through local networks which bring different services together and improving access to GPs or other primary care professionals.
We aim to provide 24/7 access to specialist opinion in primary care, ranging from an advice only service to admission to an acute assessment unit. We will also review the existing provision across NCL of GP presence in emergency departments.
We will look to develop special falls emergency response services to help support older people to remain at home after a fall, as well as helping to educate them about the risks.
What will be different for patients
GP servicesMs Sahni is 87 and has four chronic health problems. She currently has to book separate appointments with different doctors to have all of the relevant check-ups and appointments that she needs.
In future, Ms Sahni will be in a special “stream” of patients who will have all of their care co-ordinated by a very experienced GP. This will allow her to see the specialist heart or diabetic nurses at the integrated care centre at her GPs surgery. There will also be a care navigator in the team who can help sort things out for her at home including community support.
What will be different for patientsPrevention and care closer to home John, age 62 is a lifetime smoker who was recently diagnosed with chronic bronchitis. His GP advised him to stop smoking but John said he could not cope without his cigarettes and refused the offer of nicotine replacement therapy (NRT). John contracted a chest infection, went to A&E and was admitted. He stayed for several days and was given some NRT on the ward to cope with his cravings for cigarettes.
In future, when John is admitted to hospital his respiratory physician will discuss the importance of stopping smoking as a treatment for his bronchitis. He will be prescribed NRT to relieve his cravings and on discharge he will be offered a referral to specialist stop smoking support for heavily addicted smokers. John will then get a call the next day from the specialist stop smoking advisor who will arrange a home visit for the following day. John will be supported by the specialist advisor in weekly visits to help him to reduce or stop smoking altogether.

7NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
Achieving the best start in lifeBetter education for children is crucial to our plan. We need to put health and wellbeing on the map at the earliest opportunity. We need to create healthy environments, promote active travel, sport and play in schools.
We have identified areas of focus – from prevention to acute care – which will improve health and outcomes for children and young people
This will include a focus on maternal health which evidence strongly suggests has an impact on child and adult health – for example obesity, diabetes and cardiovascular disease.
We want to address mental health in children as early as possible, supporting mothers with mental health problems both before and after birth. We also want to provide services for parenting support and health visiting which focus on vulnerable, high risk families.
Mental healthWe will give equal priority to physical and mental illness and aim to reduce demand on hospital care and mental health inpatient beds.
Our plans include increasing access to primary care mental health services and improving how we manage acute mental health problems, building community capacity to enable people to stay well; and investing in mental health liaison services – for example ensuring that more people in hospitals have their mental health needs supported. We will also look to strengthen perinatal and child and adolescent mental health services (CAMHS).
What will be different for patients
Mental health liaison Maisie suffers from dementia, and is cared for by her husband Albert. Previously, after falling at home Maisie was admitted to hospital. Due to the accident and change of surroundings, Maisie was agitated and more confused than normal.
In future, as the hospital will have Core 24 liaison psychiatry, the liaison team will be able to help the hospital support both Maisie’s physical and mental health needs. As Maisie will receive holistic care it will mean that she is ready to be discharged sooner than if only her physical health needs were supported. Maisie’s husband Albert will also be supported by the dementia service, allowing him to continue to care for Maisie at home.

8NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
Urgent and emergency careOver the next five years, we aim to provide a consistent urgent and emergency care service. Patients should be seen by the most appropriate professional for their needs, which may include directing them to an alternative emergency or urgent care service. There is strong evidence that getting patients to the right specialist service, even if that might not be their local hospital, improves outcomes.
We want to develop high quality ambulatory care services across NCL – so patients can be assessed, diagnosed, treated and able to go home on the same day without needing a hospital admission.
For those patients who do need emergency treatment, we aim to have services in place that help them to leave hospital as quickly as possible and rehabilitate closer to their home if appropriate
Planned careWe want to reduce variation in the way that we deliver planned care across north central London. This includes some key areas for improvement, such as making sure patients can access the right expertise locally and that their experience of surgery is seamless, smooth and efficient.
We aim to have clear ‘pathways’ for patients across the region, with consistent approaches, so that we become more efficient and there is less variation in outcomes and experience.
We want to improve patients’ access to information and help people manage conditions without surgical intervention where possible. We will ensure patients spend as little time as possible in hospital.
CancerOur aim is to save lives and improve patient experience for people who have cancer. The priority areas we have identified for improvement are getting earlier diagnosis and better provision of radiotherapy and chemotherapy.
Targeting colorectal and lung cancers are a particular focus given the high percentage of patients receiving late stage diagnosis, often in emergency departments.
We are also developing a case for a single provider model for radiotherapy in NCL.
We want to improve palliative care so that patients have a better quality of life in their final weeks.

9NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
Social careSocial care is a crucial part of many elements of our plan, in particular in delivering care closer to home and improving mental health services. We want to ensure that health and social care services work well together to deliver well-coordinated care for local people. We will improve collaboration between local authorities and hospitals – for example, focusing on earlier discharge of hospital patients where safe and appropriate. We will build on the experience and expertise of social care and public health in the development of new models of care.
We recognise that many social care providers of services such as residential, nursing home and home care services are under great pressure. We aim to focus on strengthening the supply of the workforce for these services to address risks around their staffing capacity.
The role of social workers will also be essential to delivering our model for health and care closer to home, in addition to the role of home care workers, personal assistants and the blended role between district nurses and care workers. We will focus on recruiting to these posts and developing career opportunities in these areas.
Bringing services togetherWe will work out where it makes sense to bring services together or create networks across organisations to improve the experience of our patients. We are already collaborating across the region with positive results in cardiac/cancer; pathology; neurosurgery; stroke; and many other services.
We can learn from our experience in these areas and more work is planned to identify areas where some form of consolidation may be worth considering.
What will be different for patientsCancerPreviously Margaret, aged 60, went to see her GP with persistent gastric pain for several weeks. She was otherwise well, and did not have reflux, diarrhoea, vomiting or weight loss. Over the course of the next three weeks, Margaret's GP organised tests and ruled out any inflammation, heart problem, or gallstones that could cause the pain. He gave Margaret tablets to try to reduce inflammation from acid on her stomach lining. However, Margaret's pain was more persistent this time and she was still worried.
In the new system, Margaret’s GP will be able to refer her to a Multidisciplinary Diagnostic Centre at UCLH despite the fact that her symptoms are not considered “red flag”. Here, Margaret will be assessed for vague abdominal symptoms. A clinical nurse specialist will see her four days after referral. The team will identify that Margaret has early stage pancreatic cancer and because it was picked up early she can access potentially curative keyhole surgery.
10NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
WorkforceWe want to attract the highest quality staff to deliver the best possible care we can for local people. Therefore as well as creating the most positive environment for our patients, we want NCL to be a place where we offer the best opportunities for people to develop their careers.
Our aim is to attract, develop and retain people who work in and support health and social care in north central London. We want to create attractive careers with a workforce fit for purpose in the changing healthcare landscape – so we have the right skills in the right place for patients.
Digital and estatesWe want to use the power of digital communications and IT systems to share information and support the provision of better care and treatment for patients. We aim to promote changes so that patients can use technology to receive and share information, get treatment and prescriptions through e-referrals and e-consultations. Sharing high quality data between health and care professionals will mean people don’t have to retell their stories. Digital technologies will help ensure care is delivered in the right place at the right time by the right person.
We also want to modernise the buildings we work from and our equipment to make sure they are fit for purpose. We already have major investments planned at University College Hospital and Chase Farm Hospital and would look to develop plans for investment to improve facilities so we can deliver more care closer to home and improve mental health services.
Reducing costsWe think the changes we have set out will help us reduce waste in the health and care system. For example we can reduce cost of care by:
– treating people right first time and improving the co-ordination of services.
– avoiding unnecessary admissions to hospital .
– speeding up discharge when people are ready to go home.
– being less reliant on agency and temporary staff.
– avoiding unnecessary duplication of services between organisations.
However our plans at the moment do not achieve financial balance over the next five years, so we will continue to look for other opportunities to improve our efficiency.

11NCL | Sustainability and Transformation plan – a summary
N C LNorth Central London
EngagementWe are committed to being open and transparent about our plan as it develops. We need engagement from all of our partners, patients and local residents if we are to succeed
This means:
Early engagement on the issues before any decisions are made
Stakeholders and the public help to devise the solution
Ensuring decision-making is transparent and people know what to expect when
Each stage of the process is informed by ongoing dialogue.
As we add more detail to our plans, we will ensure that we undertake formal public consultation where appropriate. We will work with the North Central London Joint Health Overview and Scrutiny Committee to agree when we need to do this and how we best do this.
Next stepsThe draft Sustainability and Transformation Plan sets out our proposed approach to achieve sustainable health and care services in north central London. It is still work in progress. There is much more to do before we finalise the detail of these plans.
We want to fully engage patients and the public in our thinking to make sure we get this right. The various NHS organisations and local authorities will be looking at this draft plan over the next few months and they will arrange events to raise awareness of the proposals and get people’s feedback.
In the meantime if you want to feed in ideas or comments please contact the NCL STP office at [email protected]

1
NorthCentralLondonSustainabilityandTransformationPlan21October2016DRAFT
KeyinformationNameoffootprintandnumber:NorthCentralLondon,no.28Nominatedleadofthefootprint:DavidSloman,ChiefExecutive,TheRoyalFreeNHSFTOrganisationswithinfootprint:CCGs:Camden,Barnet,Islington,Haringey,EnfieldLAs:Camden,Barnet,Islington,Haringey,EnfieldProviders:Barnet,EnfieldandHaringeyMentalHealthNHSTrust,CamdenandIslingtonNHSFT,CentralLondonCommunityHealthcareNHSTrust,CentralandNorthWestLondonNHSFT,MoorfieldsEyeHospitalNHSFT,NorthMiddlesexUniversityHospitalNHSTrust,RoyalFreeLondonNHSFT,RoyalNationalOrthopaedicHospitalNHSTrust,TavistockandPortmanNHSFT,UniversityCollegeLondonHospitalsNHSFT,WhittingtonHealthNHSTrust
2
Contents
1 Foreword..........................................................................................................................................................3
2 Executivesummary...........................................................................................................................................5
3 Context.............................................................................................................................................................7
4 Caseforchange:ourchallengesandpriorities.................................................................................................104.1 Healthandwellbeinggap...........................................................................................................................104.2 Careandqualitygap...................................................................................................................................114.3 Baselinefinancialgap.................................................................................................................................13
5 Vision..............................................................................................................................................................15
6 Strategicframework........................................................................................................................................166.1 Prevention.................................................................................................................................................176.2 Servicetransformation...............................................................................................................................19
6.2.1 Achievingthebeststartinlife.......................................................................................................................196.2.2 Healthandcareclosertohome.....................................................................................................................216.2.3 Mentalhealth................................................................................................................................................256.2.4 Urgentandemergencycare..........................................................................................................................286.2.5 Socialcare......................................................................................................................................................296.2.6 Optimisingtheelective(plannedcare)pathway...........................................................................................306.2.7 Consolidationofspecialties...........................................................................................................................346.2.8 Cancer............................................................................................................................................................366.2.9 Specialisedcommissioning............................................................................................................................37
6.3 Productivity................................................................................................................................................386.3.1 Commissionerproductivity(BAUQIPP).........................................................................................................386.3.2 Providerproductivity(BAUCIP)andsystemproductivity.............................................................................39
6.4 Enablers.....................................................................................................................................................406.4.1 Digital.............................................................................................................................................................406.4.2 Estates............................................................................................................................................................436.4.3 Workforce......................................................................................................................................................466.4.4 Newcommissioninganddeliverymodels.....................................................................................................48
6.5 Measuringoursuccess...............................................................................................................................49
7 Deliveryplans..................................................................................................................................................50
8 Bridgingthefinancialgap................................................................................................................................518.1 Normalisedforecastoutturnbyyear..........................................................................................................528.2 2017/18forecastoperatingplan.................................................................................................................538.3 Capitalexpenditure....................................................................................................................................538.4 Nextstepstoaddressthefinancialgap......................................................................................................54
9 Howwewilldeliverourplan...........................................................................................................................599.1 Deliverythrough2yearcontractsinNCL....................................................................................................599.2 Decisionmakingintheprogramme............................................................................................................60
9.2.1 CollectivegovernancearrangementsforCCGs..............................................................................................609.3 Programmearchitecture............................................................................................................................61
9.3.1 Futureprogrammearchitecture....................................................................................................................629.3.2 Healthandwellbeingboards.........................................................................................................................639.3.3 Overviewandscrutinycommittees...............................................................................................................63
9.4 Programmeresourcing...............................................................................................................................63
10 Engagement....................................................................................................................................................6510.1 Ourfutureplans.........................................................................................................................................6510.2 Publicconsultation.....................................................................................................................................6710.3 Equalitiesanalysisandimpactassessment.................................................................................................67
11 Conclusionandnextsteps...............................................................................................................................68

3
1 ForewordWelcometotheSustainabilityandTransformationPlan(STP)forthehealthandsocialcareservicesthatservethepopulationofNorthCentralLondon(NCL).TheaimoftheSTPistoensureNCL isaplacewiththebestpossiblehealthandwellbeing,wherenoonegets leftbehind.This STP is awork in progress andwewelcome your comments and input aswe furtherdeveloptheplans.Forthefirsttime,wehavecometogetherashealthandsocialcarepartnerstoplanhowwewilldeliverexcellent,future-proofedservicesforourlocalpopulationoverthenext5years.Weknowthatthehealthandsocialcareneedsofour localpeoplearechanging,andthatthereareseriousissuesfacinghealthandcareservicesinNCL.Peoplereceivedifferentcaredependingonwhere theygo toobtain it:waiting times for servicesandhealthoutcomesvary, and the quality of care and people’s experience of health and social services issometimesnotasgoodasitcouldbe.On top of this, our financial situation remains challenging. Demand for health and socialcarecontinuestogrowyearonyearandthegrowth indemandisrunningfasterthanthegrowth in funding. Ifwe do nothing,we estimate thatwewould face an unprecedentedfinancial gap in relation to health services alone of nearly £900m in NCL by 2020/21. Inaddition,asiswellknown,thetrendisforpeopletolivelongerandinturnthisiscreatingpressureonsocialcareservicesandfunding.We believe the best approach tomeeting these challenges is towork together to tacklethemheadon,workingtogethertofindsolutionsatscaleandaligningasasystemaroundthe interestsof localpeople rather thansolely focusingonour individualorganisations. Ittakestimetobuildrelationshipsandtrustinthecontextofasystemthatisfragmentedandunderincreasingpressure,butwearecommittedtothisjointendeavouracrossthewholepartnership.TheSTPsetsoutourcommitmenttotransformingcaretodeliverthebestpossiblehealthoutcomesforourlocalpopulation;shiftingourmodelofcaresothatmorepeoplearecaredforinoutofhospitalsettings-throughprevention,moreproactivecare,andnewmodelsofcare delivery – and reducing reliance use of secondary care. We have made significantprogress indevelopingourspecific ideas forhowwewillachieve this.Wehavesetup13differentworkstreamsandhaveworkedhardontheseoverthelastfewmonthstodevelopthinking, building on evidence and involving hundreds of members of staff drawn fromeveryorganisationinNCL.Wehaveheldpublicmeetingsineachoftheboroughstostarttodevelopadialoguewiththelocalcommunity,althoughwerecognisethereismuchmoretodoonengagementinthemonthsahead.
4
The plan sets out a mixture of both radical service transformation and incrementalimprovements we believe we need to make in order to deliver real benefits for ourpopulation: increasingtheemphasisonprevention;shiftingcareclosertohometoreducedemand on hospitals; reducing variation in quality; improving productivity and reducingwaste.But theplanas it standsdoesnothaveall theanswers.Therearesomepartsof theplanwhichwehavenothadtimetodevelop indetail thatrequiresignificantlymorework.Werecognise thesheerscaleof thechanges thatwesetoutcurrently in theplanwill stretchourcapacitytodeliver,soweneedtostresstesttheplantoensurewefocusonthemostimportant improvement first. And fundamentally the plan does not yet balance thefinances,eithernextyearorby2020/21.Unlesswecandoso,wewillnotbeabletoaffordalloftheinvestmentsandimprovementsweaspiretodeliver.Asaresultweknowthatwemay face some really tough decisions about where we can invest for improvement andwherewewillneedtoprioritiseormakechoices.Weneed to resolve thesequestionsbetweennowandChristmas.Wewill ensureweareprioritising the areas which will add the most value (in terms of increasing health andwellbeingforpeople; improvingthequalityofcarepeoplereceive;andensuringvaluefortaxpayers’money) to focusourenergiesonachievingmaximumbenefit.Thiswill includetrying to attract as much investment into NCL as possible. We will continue to developfurtherideasinthepartsoftheplanwhicharenotfullydeveloped.Andwewillreviewthephasing of our specific priorities for the first 2 years of our plan in the context of thesignificantfinancialchallengeweface,seekingspecificallytoidentifyareaswherewecangofurtherandfaster,andareaswherewecandeferourinvestmentoreffort.Werecognisethere ismuchmoreworktodo,and it iscrucial thatour localresidentsareinvolved in this. We are at the beginning of truly transforming care for our population,whichwill require significant input and contribution from thepeoplewhouse services inNCL. We look forward to working with our local population to make designing andimplementingtheplanasuccessasitevolves.

5
2 Executivesummary
TherearesomeexcellenthealthandcareservicesinNorthCentralLondon(NCL).However,servicesarenotconsistentandthereareexamplesofpoorpractice.Wealsofacesignificantchallengesoverthenextfiveyearsandneedtoshiftourmodelofcaresothatmorepeopleare cared for inoutofhospital settings. This SustainabilityandTransformationPlan (STP)has been produced by all themain healthcare organisations and local authorities withinNCL.Itsetsouthowweareplanningtomeetthechallengeswefaceanddeliverhighqualityandsustainableservicesintheyearstocome.
Weknowfromourtrackrecordthatwehavethecapabilitytodeliverexcellentservicesandtodeliversignificantchange.However,wearenotcurrentlyabletodeliverservicesacrossNCL consistently to the standards we would like. We also face a number of significantchallengesaroundthehealthandwellbeingoflocalpeople;andthecareandqualityofourservices.Our current system is focussedondealingwith illness, rather thanorientated topreventionandhelpingpeopletolivewell.ThereisasubstantialfinancialchallengefacinghealthorganisationsinNCL;thehealthsystemisalreadyindeficitand,ifnothingchanges,thiswill worsen over the next 5 yearsmeaning that by 2020/21we estimatewewill bec.£900m in deficit. Local authorities are also facing significant financial pressures due todemographic changesandpolicy inflation:by2020/21 the combinationsofpressuresandcontinuedlossoffundingwillresultinacombinedsocialcarebudgetgapofc.£300m.
OurvisionisforNCLtobeaplacewiththebestpossiblehealthandwellbeing,wherenoonegetsleftbehind.Todeliveronourvision,wehavedesignedaprogrammeoftransformationwith4fundamentalaspects:
1. Prevention: We will increase our efforts on prevention and early intervention toimprovehealthandwellbeingoutcomesforourwholepopulation.
2. Service transformation: To meet the changing needs of our population we willtransformthewaythatwedeliverservices.
3. Productivity:Wewill focus on identifying areas to drive down unit costs, removeunnecessary costs and achieve efficiencies, including working together acrossorganisationstoidentifyopportunitiestodeliverbetterproductivityatscale.
4. Enablers: We will build capacity in digital, workforce, estates and newcommissioninganddeliverymodelstoenabletransformation.
Delivering these plans will result in improved outcomes and experience for our localpopulation,increasedqualityofservicesandsignificantsavings.
Despitethis,wecurrentlyexpectthattheoverallfinancialpositionofNHSorganisationswillbe a £75m deficit in 2020/21. We have identified a number of areas for further workbetweennowandChristmaswherewebelievetheremaybeadditionalsavingstobefoundthatwouldaddressthisresidualgap.

6
Toensureweareabletodeliverasasystem,buildingontheprogresswehavemadetodatewewill develop a robust governance structurewhich enablesNHS and local governmentpartners to work together in new ways to drive implementation. We will put in placededicated resources to support delivery. It is crucial thatwhole system is aligned arounddeliveryoftheSTPandwewillensurethatthedevelopmentofthe2yearhealthcontractsthat are being put in place for 2017/18 - 2018/19 are consistent with the STP strategicframework.
Werecognisethereismoreworktodotofinalisethegranulardetailofourdeliveryplansandaddresstheresidualchallengeweareforecasting.Todevelopourplansinmoredetailwewanttofullyengagepeoplewhouseservicesandthepublic inourthinkingtoensurethey are reflective of their needs. We are committed to being radical in our approach,focusing on improving population health and delivering the best care in London. Ourpopulationdeservesthis,andweareconfidentthatwecandeliverit.

7
3 Context
NorthCentral London (NCL) comprises fiveClinicalCommissioningGroups (CCGs):Barnet,Camden,Enfield,HaringeyandIslington,eachofwhichiscoterminouswiththelocalLondonBoroughs.Approximately1.45m1liveinthe5boroughs.Wespendc.£2.5bnonhealthandc.£800m2onadultandchildren'ssocialcareandpublichealth.Thepopulationisdiverseandhighlymobile,withalargenumberofpeoplelivingindeprivation3.
TherearefouracutetrustswithinNCL:TheRoyalFreeLondonNHSFoundationTrust(sitesincludeBarnetHospital, Chase FarmHospital and theRoyal FreeHospital inHampstead),University College London Hospitals NHS Foundation Trust, North Middlesex UniversityHospital NHS Trust, and Whittington Health NHS Trust. There are two single specialisthospitals: Moorfields Eye Hospital NHS Foundation Trust and the Royal NationalOrthopaedicHospitalNHSTrust.GreatOrmondStreetHospitalforChildrenNHSFoundationTrust iswithin theNCLgeography,but currentlyoutof the scopeof theSTP.Communityservices are provided by Central and North West London NHS Foundation Trust, theWhittingtonHealthNHSTrust,andCentralLondonCommunityHealthcareNHSTrust.
Mentalhealthservicesareprovidedby theTavistockandPortmanNHSFoundationTrust,Camden and Islington NHS Foundation Trust and Barnet, Enfield and Haringey MentalHealthNHSTrust.Thereare2204GPpractices,andtheout-of-hoursservicescontractwasrecentlyawarded to theLondonCentralandWestUnscheduledCareCollaborative.Thereare497activesocialcaresitesregisteredacrossNCL, including273registeredcarehomes(47ofwhichprovidenursing)5.CarehomesareparticularlyhighinnumbersinthenorthofNCL,forexampleinEnfieldwherethereare97registeredcarehomes(incontrasttothe12carehomes registered inCamden)6. In addition, thereare214 registereddomiciliary careproviders7.
TheorganisationofservicesinNCLmakestheareaquiteuniqueandthishasramificationsforplanning:thereisaparticularlyhighconcentrationofspecialisedservicesacrossmultipleproviderscoveringasmallgeographicarea.ThismeansmanyofthepatientstreatedinNCLdo not live in NCL and consequentially, a large proportion of the income paid to ourproviderscomesfromcommissionersoutsideofthearea.
AsindividualorganisationsinNCL,wehaveahistoryofworkingtogetherindifferentwaysto meet the needs of our population, and there are numerous excellent examples ofcollaboration as a result.However,working collectively across all organisations remains arelativelynewendeavourandwecontinuetobuildthetrustrequiredtoenableustodoso.
1ONS,Mid-yearpopulationestimates,201522015/16 3Officefornationalstatistics,IMD20154LatestfiguresfromNHSEngland,updatedsincepublicationoftheNCLcaseforchange5LocalAuthorityCareQualityCommissionreports,20166LocalAuthorityCareQualityCommissionreports,20167LocalAuthorityCareQualityCommissionreports,2016

8
We are home to 4 national Vanguards: The Royal Free London NHS Foundation Trust isdeveloping a provider chainmodel; University College London Hospitals NHS FoundationTrustVanguardisfocusedonwhatcanbedonetoimprovetheend-to-endexperienceforpeople with cancer; Moorfields Eye Hospital NHS Foundation Trust is developing anophthalmology specialty chain; and, theRoyalNationalOrthopaedicHospitalNHSTrustisoneof13partnersdevelopingaUK-widechainoforthopaedicproviders.NCLisalsohometotwodevolutionpilots:oneseekingtooptimisetheuseofhealthandsocialcareestate,andanother focusedonprevention inHaringey. Inprimarycare,GPpracticesarealreadyworking together in a number of GP Federations to provide extended services to ourresidents.
InNCL,everyboroughhas itsownuniqueidentityandlocalassetswecanbuildon.Manypeopleleadhealthylives,butiftheydogetsickwecanoffersomeofthebestcareinthecountry.Wehaveareputationforworldclassperformanceinresearchandtheapplicationof innovation and best practice, and we can harness the intellectual capacity of ourworkforcetoensurethebestoutcomesaredelivered.Therearemanyexamplesofexcellentpracticeacrosshealthand social care inourarea,whichwe intend touse tohelpensurethatexcellentpracticecanbeofferedtoallourresidents.
Ourtrackrecorddemonstratesthatwehavethecapabilitytodeliverexcellentservicesandalsotosignificantlychangeourserviceswhenneeded.Ourambitionisthateveryoneisabletogetthecaretheyneedwhentheyneedit.Thismeansensuringpeoplehavethebeststartinlife,andsupportingthemtolivehealthylives.Whenpeopledoneedspecialistcare,wewantthemtobeabletoaccessitquicklyandinthemostappropriatesetting,andtobefullysupportedtorecoverinthesettingmostsuitedtotheirneeds.
However,wearenotconsistentlydeliveringourambitiontothestandardswewould like.We face significant challenges around the health and wellbeing outcomes for ourpopulation,thequalityofourservicesandthefinancialsustainabilityofthehealthandcaresystem. These are outlined in this document and set out in more detail in our case forchange8.
ThenationalrequirementtoproduceanSTPisanopportunityfortheNCLsystemtoaddressthesechallengestogetherandwidenthescopeofourcollaborativeworking.Thisdocumentarticulates:
• ourcollectiveunderstandingofthechallengesweface• ourvisionforhealthandcareinNCLin2020/21• theplanstodeliveronourvisionandaddressthechallenges• thedeliveryframeworkwhichwillenableustoimplementourplan• theimpactweexpecttoachievethroughthedeliveryofourplans• ourplansforsecuringbroaderpublicsupportandengagementwithourproposals• our next steps for further developing proposals and responding to our residual
financialgap.
8https://www.uclh.nhs.uk/News/Documents/NCL%20case%20for%20change.September%202016.pdf

9
Exhibit1:OverviewofNCL
Source:Populationfiguresfrom2014ONSdata.
London Ambulance ServiceEastofEnglandAmbulanceService
Barnet,EnfieldandHaringeyMentalHealthNHSTrust(mainsites,incl EnfieldCommunity)CamdenandIslingtonNHSFT(andmainsites)NorthMiddlesexUniversityHospitalNHSTrustTheRoyalFree LondonNHDFTUniversityCollegeLondonHospitalsNHSFTWhittingtonHealthNHSTrust(incl IslingtonandHaringeyCommunity)CentralandNorthWestLondonNHSFT(CamdenCommunity)CentralLondonCommunityHealthcareNHSTrust(BarnetCommunity)Specialistproviders
EnfieldCCG/EnfieldCouncil~320kGPregisteredpop.~324kresidentpop.49GPpracticesBarnetCCG/BarnetCouncil~396kGPregisteredpop.~375kresidentpop.62GPpracticesHaringeyCCG/HaringeyCouncil~296kGPregisteredpop.~267kresidentpop.45GPpracticesIslingtonCCG/IslingtonCouncil~233kGPregisteredpop.~221kresidentpop.34GPpracticesCamdenCCG/CamdenCouncil~260kGPregisteredpop.~235kresidentpop.35GPpractices

10
4 Caseforchange:ourchallengesandpriorities
InNCLwesharemanyofthesamechallengesfacedbyhealthandcareorganisationsacrossthe UK (and indeed internationally). We have undertaken significant work to identify,articulateandquantifythespecificgapsinhealthandwellbeing;careandquality;andourbaselinefinancialposition.Acrossthesystemwehavealignedbehindthisworkandweallagreeon thenature and scaleof the challenge,whichwehavedescribed inour case forchangewhichwaspublishedinSeptember2016.
4.1 Healthandwellbeinggap
Wehaveadiverseandhighlymobilepopulation. Therearepeople froma rangeofBlackand Minority Ethnic (BME) groups: these groups have differing health needs and healthrisks. A quarter of our local people do not have English as their main language9, whichcreateschallengesfortheeffectivedeliveryofhealthandcareservices.Themobilityofourpopulation,with8%oflocalpeoplemovingintooroutofNCLeachyear10,hasasignificantimpactonaccesstoservicesanddelivery.
Poverty is a crucial determinant of health, and is widespread among both adults andchildrenlivingintheboroughsthatmakeupNCL11.Significantinequalitiesexist,whichneedtobeaddressed;forexample,meninthemostdeprivedareasofCamdenliveonaverage10yearsfewerthanthoseintheleastdeprivedareas12.Wefacechallengesinaddressingotherwider determinants of health, for example, there are high levels of homelessness andhouseholds in temporary housing with all five boroughs in the top 10% for number ofhouseholds in temporary accommodation13. Social isolation also remains a critical issueacrossthesub-region.
ThechildrenofNCLdonotalwaysgetthebeststarttolife.30%ofchildrengrowupinchildpovertyand6%liveinhouseholdswherenooneworks.60childrentakeupsmokingeveryday14.Althoughtherehavebeensomeimprovementsrecently,Londonasawholehasthehighestratesofobesitynationally:1in3childrenareobeseinYear6(age11)andweneedtodomoretotacklethis,particularlyworkingwiththeschoolsinNCL15.Althoughmanyofour residents are healthy and people are living for longer, good health does not alwayspersistintooldage.Ourolderpeoplearelivingthelast20yearsoftheirlifeinworsehealththantheEnglandaverage16.
Almosthalfofpeople inNCLhaveat leastone lifestyle-related clinicalproblem (e.g.highbloodpressure)thatisputtingtheirhealthatrisk17.However,theyhavenotyetdeveloped
9NCLcaseforchange,201610ONSmid-yearpopulationestimates201411Census201112IMD2015,ONS13https://www.gov.uk/government/statistical-data-sets/live-tables-on-homelessness14CENSUS201115Publichealthoutcomesframeworktool,2015 16 OfficeforNationalStatistics,HSCICCCGIndicators,2014-15 17CamdenandIslingtonGPLinkedDatasetprojectedtoNCLlevel

11
a long term health condition. Many of these lifestyle-related clinical problems are riskfactorsforNCL’sbiggestkillers-circulatorydiseasesandcancer.Thesediseasesarealsothebiggestcontributorstothedifferenceswhichexistinlifeexpectancy.
TherearehighratesofmentalillnessamongstbothadultsandchildreninNCL18,andmanyconditionsgoundiagnosed19.50%ofallmental illness inadultsbeginsbefore14yearsofageand75%by1820.Childrenwithmotherswithmentalillhealtharemuchmorelikelytodevelopmentalhealthissuesthemselves.Threeofourboroughshavethehighestratesofchildmental health admissions in London21 There are high rates of early death amongstthosewithmentalhealthconditions22,particularlyinHaringeyandIslington,andtherateofinpatientadmissionsamongstthispopulationisabovethenationalaverage.Astrongfocusonmentalhealthiscentraltoourapproachwithaclearaimoftreatingmentalandphysicalillhealthinajoinedupwayandwith“parityofesteem.”
4.2 Careandqualitygap
Currently, our systemdoesnot sufficiently invest in thosepeoplewith a life-style relatedclinical problem, which would help stop them from developing the long term conditionswhichinaggregateareahugeburdenonourhealthandcaresystem.Only3%ofhealthandsocialcarefundingisspentonpublichealthinNCL23,andthatisdespiteevidenceshowingthat between 2012 and 2014 around 20% (4,628) of deaths in NCL could have beenprevented24.Thereisa largeopportunity inrefocusingoureffortstowardspreventionandmaking every contact count. This focus should also address the wider determinants ofhealthsuchaspoverty,housingandemployment,allofwhichhaveasignificantimpactonindividuals’healthandwellbeing.
Diseaseand illness couldbedetectedandmanagedmuchearlier, andmanagedbetter incommunity.Itisthoughtthattherearearound20,000peopleinNCLwhodonotknowtheyhavediabetes,while13%ofthepopulationarethoughttobelivingwithhypertension25.Itislikely thatpeoplearebeing treated inhospital for long termconditions (LTCs)when theycouldbebettermanagedbyindividualsthemselveswiththesupportofprofessionalsinthecommunity.ManypeoplewithLTCs–over40%inBarnet,HaringeyandEnfield–donotfeelsupported to manage their condition26. This would help avoid the high levels ofhospitalisationweexperiencefortheelderlyandthosewithchronicconditions.
One of the disease specific challenges we face is in the provision of cancer care. Latediagnosisof cancers is aparticular issue, alongside low levelsof screening for cancerandlowawarenessofthesymptomsofcancerinsomeminorityethnicgroups.Waitingtimesto 18QOFdata2014/1519NHSEnglandDementiaDiagnosisMonthlyWorkbook,April201620DunedinMultidisciplinaryHealth&DevelopmentResearchUnit.WelcometotheDunedinMultidisciplinaryHealthandDevelopmentResearchUnit(DMHDRU).21Fingertips,2014/1522HealthyLives,HealthyPeople201023Basedon2015/16publichealthbudgetofeachNCLcouncil24PublicHealthProfilesDataTool,PHE,2012-1425QOF2014/1526OfficeforNationalStatistics,HSCICCCGIndicators,2014-15

12
seeaspecialistarelong,andsoarewaitingtimesfordiagnostics.Additionally,referralstospecialists have almost doubled in five years. There is a huge shortfall in diagnosticequipment and workforce, and a lack of services in the community, particularly atweekends.Afurtherissueisthatsomehospitalsareseeingsmallnumbersofpatientswithsometypesofcancer,insomecaseslessthantwoperweek.
Therearesomechallengesinprimarycareprovision,however,thisisamixedpicturewhichcreatesinequity.TherearetoofewGPsinBarnet,EnfieldandHaringey,andlownumbersofregistered practice nurses per person across all areas, but particularly in Camden andHaringey.
There are high levels of A&E attendances across NCL compared to national and peeraverages27,andveryhigh levelsof firstoutpatientattendances28,which indicatepotentialgaps in primary care provision. Acute providers are not consistently meeting emergencystandards.
Intheacutesettingtherearedifferencesinthewaythatplannedcareisdeliveredandthisneedstobeaddressed,withvariationbasedondifferences inclinicalpracticerather thanpatientneed.ThenumberofpeopleseenasoutpatientsinNCLishighandthereisvariationinthenumberofreferralsbetweenconsultantsinthesamehospital,thenumberoffollow-upoutpatientappointmentsandtheproportionofplannedcarethatisdoneasadaycase.
Weareusinghospitalbedsforpeoplewhocouldbecaredforathome,orinalternativecaresettings. 59% of acute bed days are used by people with stays over 10 days, and themajorityof thesepeopleareelderly. 85%of thementalhealthbeddays inNCLare frompatients stayingover30days.Delayeddischargesarealsohigh in somehospitals. Stayinglonger than necessary in hospital is not good for people’s health, especially the elderlywhosehealthandwellbeingcandeterioraterapidlyinanacuteenvironment.29
We face challenges inmentalhealthprovision.Peopledonotalwayshaveeasyaccess toinformation and community based support, and community mental health services areunderhugepressure.Thereisalsonohighqualityhealth-basedplaceofsafetyinNCL.Manypeople receive their first diagnosis of mental illness in Emergency Departments. Highnumbersofpeopleareadmittedtohospital–manyundertheMentalHealthAct.Thereisvariableaccess to liaisonpsychiatry,perinatalpsychiatryandchildandadolescentmentalhealth services (CAMHS) within urgent care: most of the liaison psychiatry and CAMHSservices in hospitals in NCL do not see children within one hour at weekends andovernight30.ThereislimitedperinatalcommunityserviceinNCL,inthenorthernboroughsthereisnospecialistteamandinthesouthernboroughstheservicedoesnotmeetnationalstandards31.
27RightCareAtlasofVariationinHealthcare,September201528NHSEnglandActivityData2014-1529Philipetal. (2013)Reducinghospitalbeduseby frailolderpeople: results fromasystematic reviewof the literature.
InternationalJournalofintegratedcare.30 MentalhealthcrisiscareEDaudit,NHSEngland(London),201531MaternalMentalHealthEveryone’sBusiness

13
Our use of information and technology does not currently support integrated health andsocialcareacrossNCL.Thereisavariablelevelofdigitalmaturityacrossprovidersandmostbeingbelowthenationalaveragefordigitalcapabilities,particularlytheircapabilitytoshareinformationwithothers.
Someofourbuildingsarenotfitforpurposeandthereareopportunitiestouseourestatesbetter.11sitesinNCLhavefacilititesmanagementcostsatleast10%morethantheCarterbenchmark(£319psq.m),withafurther3siteswithin10%ofthebenchmark.8siteshavea higher proportion of unutilised space than the 2.5% benchmark contained within theCarterreport,andoverhalfofthesitesanalysedwerefoundtohaveahigherproportionofnon-clinicalspacethantheCarterbenchmark(35%).
We have significant workforce challenges across health and social care, including a highturnover across a range of professions, an over reliance on agency staff and HR policieswhicharenottransferableacrossorganisations.
There is consensus across the system that the current approach to commissioning andprovidinghealthandsocialcareservicesacrossNCLcouldbebetteralignedtosupporttheimplementation of our emerging vision for the STP. In particular, the delivery of apopulationhealthapproachandgenuinelyintegratedcareissignificantlyconstrainedby:
• therigidseparationofcommissioningandprovidingresponsibilitieswithintheNHS• thelimitedexistingintegrationbetweenhealthandsocialcare• thefragmentationofprovidersofhealthandcareintomanysovereignorganisations• increasedfinancialrisksacrossCCGsandproviders• stretchedcapacityandcapabilityinthecurrentorganisationalform.
We need to design new commissioning and delivery models that enable us to delivertransformedcareinawaythatissustainable.
4.3 Baselinefinancialgap
Ourpopulationisgrowinganddemandisrising:peopleaccesshealthcaremoreoften,andare–positively–livinglonger,butoftenwithoneormorelongtermconditions.Meanwhile,theNHS’scostsarerisingmorethaninflationacrosstheUKeconomy(towhichallocationsarelinked).Theupshotofthisisthatnotonlyisthesystemrespondingtogreaterdemand,butalsothatthesumcostofactivityisgrowingfasterthanallocations.
Putsimply,fundingincreasesinNCLof£269moverthenext5yearswillnotmeetthelikelyincreasesinnumbersoflocalpeopleandgrowthindemandforhealthservicesofc.£483m,plusincreasesinthecostofdeliveringhealthcareofc.£404m.
ThismeansthatthereisasubstantialfinancialchallengefacinghealthorganisationsinNCL.Health commissioners and providers were already £121m in deficit in 2015/16 and, ifnothingchanges,thiswillgrowto£876mindeficitby2020/21.

14
Exhibit2:The‘donothing’financialgapforNCL
The‘donothing’specialisedcommissioningfinancialchallenge isestimatedat£137m(thisestimate is currently being validated). This excludes Great Ormond Street Hospital NHSTrustandtheRoyalNationalOrthopaedicHospitalNHSFoundationTrustwhichwouldaddafurther£49mand£10mrespectively.Thespecialisedcommissioningchallengeisdrivenbyadvances in science; an increasingly ageing population with LTCs; and rising publicexpectationandchoiceforspecialisedtreatment. Inadditionthereareincreasingfinancialpressuresforspecialisedservices,includingtheincreasingvolumeofexpensivenewdrugs.Spendingonspecialisedserviceshas increasedatmuchgreatera rate thanotherpartsoftheNHS,andthisisexpectedtocontinue.
The current combined net budgets for the 5 boroughs in NCL is £760m for Adults andChildren's Social Care (CSC) and Public Health services. However,we know that between2010/11and2020/21theaveragereductioninboroughspendingpowerwillbe35%.AdultSocial Care (ASC) budget reductions during this period will total at least £154.5m. Thisreductioninfundingrequiresthatasignificantsavingsprogrammebedelivered.
Thecollective2016/17forecastbudgetpressuresforthe5boroughsinASCandCSCis£39m(£26mASC,£13mCSC).BothASCandCSCwill continue faceconsiderablepressures fromdemographic growth, inflation and increasingly complex care needs. By 2020/21 thecombinations of pressures and continued loss of fundingwill result in a combined socialcarebudgetgapofc.£308m,whichisequivalenttoa28%reductiononthecurrentCouncils'totalbudget.Councilsmayhave theoption to raisea2%precept for social care in futureyears,butthiswillbesubjecttopoliticalagreementandwillnotcomeclosetoclosingthegap.

15
5 Vision
DevelopingourvisioninNCLhastakentime,andwehaveharnessedourhighqualityclinicalandpractitionerleadershipateverystageoftheprocess.ThevisionforNCLinitiallydrewonexistinglocalworkwhichwasunderwaybeforetheSTPprocessstarted.LeadersacrossthesystemtheniteratedthevisionataneventinSeptember2016.Thisprocess,alongsidetheseriesofborough-basedpublicengagementeventsinSeptemberandOctober,hasensuredthatourvision iscollectivelyownedacrossthesystem.Wearecommittedtofulfillingourvisionthroughthisplan,andhaveidentifiedasetofcoreprinciplestosupportourambition.
Ourcoreprinciples
• Wewillworkinanewwayasawholesystem;sharingrisk,resourcesandreward.• Health and social care will be integrated as a critical enabler to the delivery of
seamless,joinedupcare.• Wewillmovefrompilotsandprojectsto interventions forwholepopulationsbuilt
aroundcommunities,peopleandtheirneeds.Thiswillbeunderpinnedbyresearchbaseddeliverymodelsthatmove innovation in laboratoriestofrontlinedeliveryasquicklyaspossible.
• Wewillmakethebestthestandardforeveryone,byreducingvariationacrossNCL.• Intermsofhealthwewillgivechildrenthebeststartinlife,andworkwithpeopleto
helpthemremainindependentandmanagetheirownhealthandwellbeing.• Intermsofcarewewillworktogethertoimproveoutcomes,providecarecloserto
home,andpeoplewill onlyneed togo tohospitalwhen it is clinicallyessentialoreconomicallysensible.
• We will ensure value for tax payers’ money through increasing efficiency andproductivity,andconsolidatingserviceswhereappropriate.
• Todoallofthiswewilldothingsradicallydifferentlythroughoptimisingtheuseoftechnology.
• Thiswillbedeliveredbyaunified,highqualityworkforceforNCL.
OurvisionisforNorthCentralLondontobeaplacewiththebestpossiblehealthandwellbeing,whereno-onegetsleftbehind.

16
6 Strategicframework
TodeliveronourvisionandachievethetripleaimassetoutintheFiveYearForwardView(toincreasehealthandwellbeing;meetthehigheststandardsofcareandquality;andimproveproductivityandefficiency),wehavedesignedaprogrammeoftransformationwith4aspects:
1. Prevention: Much of the burden of ill health, poor quality of life and healthinequalities inNCL is preventable.Wewill increase our efforts on prevention andearly intervention to improve health and wellbeing outcomes for our wholepopulation,whichwillreducehealthinequalities,andhelppreventdemandformoreexpensivehealthandcareservicesinthelongerterm.
2. Service transformation: To meet the changing needs of our population we willtransform the way that we deliver services. This involves taking a “populationhealth” approach: giving children the best possible start in life; strengthening theoffersandprovisioninthelocalcommunitytoensurethatwherepossiblecarecanbe provided out of hospital and closer to home – reducing pressure on hospitalservices;rethinkingtherelationshipsbetweenphysicalandmentalhealthtoensurethat mental health care is holistic and person-centred; and, reducing variation inservicesprovidedinhospital.Socialcareplaysakeyroleinservicetransformation.
3. Productivity: Inordertoensuresustainability,wewill focuson identifyingareastodrive down unit costs, remove unnecessary costs and achieve efficiencies. Forproviders,thisincludesimplementingrecommendationsfromtheCarterReviewandworking together across organisations to identify opportunities to deliver betterproductivityatscale.
4. Enablers:We will focus on delivering capacity in key areas that will support thedelivery of transformed care across NCL. This includes digital, workforce, estates,andnewcommissioninganddeliverymodels.
Exhibit3:TheNCLSTPstrategicframework
ServicetransformationImprovespopulationhealthoutcomes;Reduces
demand;Improvesqualityofservices1.Prevention
2.Healthandcareclosertohome
3.Mentalhealth
4.Urgentandemergencycare
5.Optimising theelectivepathway
6.Consolidationofspecialties
ProductivityReducesnonvalue-addingcost
EnablersFacilitatesthedeliveryofkeyworkstreams
A B
8. Productivity• BAUQIPP• BAUCIP• Systemproductivity
7.Cancer
C
9.Healthandcareworkforce10.Healthandcareestates11.Digital12.Newdeliverymodels13.Commissioningarrangements

17
6.1 Prevention
Wewillembedpreventionandearlyinterventionacrossthewholehealthandcaresystemand deliver effective preventative interventions at scale. As a result, we will improvepopulationhealthoutcomesandreducehealthinequalitiesbyharnessingassetswithinandacross communities for example, from Council services, including social care and thevoluntary and community sector. This will positively impacting on the lives of residents,theirfamilies,andourcommunities.
Ourpreventionplansfocusoninterventionsandsystemchangeacrossthewholespectrumof prevention (exhibit 4), where there is strong evidence of effectiveness and return oninvestment within the 5 year period of the STP32. In addition, we have identifiedopportunitieswherewe could rapidlybuildupon successful local initiatives acrossNCL toachieveeconomiesofscale.
32 InterventionshavebeenidentifiedfromthePublicHealthEngland(PHE)SupportingPackforSTPsandthereturnoninvestmentworkundertakenforHealthyLondonPartnershipsbyOptimity.
Afrinlivesinhostelaccommodationandisdependentonalcohol.Heexperiencesseizuresalmostdaily.Afrinhasinthepast,withsupportfromtreatment,managedtogainabstinencebuthadarelapsewhichisduetodepressionbroughtonbyunstablehousingandeconomiccircumstances.Afrinhashadmanyunscheduledhospitaladmissionsinthelast6months.Infuture,onadmissiontohospitalAfrinwillbereferredtoanalcoholassertiveoutreachworker(AAOT)bythehospitalalcoholliaisonworker.Thissupportwillenablehimtoputinplacefoundationsthatwillhelphimtowardsabstinenceandrecovery.Afrinwillbesupportedtogiveupdrinking,withinputfromanaddictionsdoctoratacommunityalcoholservice.Aslowreductionplan,thatisachievableandminimisestheriskofseizureswhichinthepasthaveledtohospitaladmission,willbeputinplace.Afrinwillhaveregular1-2-1appointmentswithhisAAOT,whichwillincludepsychologicalhelp.

18
Exhibit4:Approachtoprevention
Wewillconcentrateoureffortson:
• Creating a ‘workforce for prevention’ so that every member of the local publicsectorworkforceinNCLisachampionforprevention.Specific interventions:MakingEveryContactCount(MECC);MentalHealthFirstAid(MHFA);dementiaawareness
• Ensuring that the placeswhere residents and employees live andwork promotegood health. This will include: reversing the upwards trend in childhood obesity;supportingpeoplewithmental ill healthandother long termconditions to stay inwork;pioneeringnewapproachestotacklinggambling,alcoholmisuseandsmoking;and supporting the workforce across NCL (including our own staff) to becomehealthier.Specific interventions: Haringey Devolution Pilot; improving employmentopportunitiesforpeoplewithmentalillhealththroughindividualplacementsupport(IPS);HealthyWorkplaceCharter;HealthyEarlyYears/HealthySchoolsaccreditation
• Supportingresidents,familiesandcommunitiestolookaftertheirhealth:smokinganddrinkingless,eatingmorehealthily,andbeingmoreactive,aswellaslookingaftertheirsexualhealthandmentalhealthwellbeing.Thiswillall reducehospitaladmissions from preventable causes such as smoking, alcohol, and falls, andreductionsinassociatedillhealthandearlydeaths.Wewillprotectandensurehighqualityuniversalservicesforvulnerablefamiliesbystartingdirectconversationswithschools to proactively identify who these families are, and collaborating to mapacross primary care, social care, early years, therapies, paediatrics and secondarycare. We will ensure that smoking cessation programmes are embedded across

19
maternityservicesandservicesforchildrenandyoungpeople,targetingparentsandolder children.Drawingon theexperienceofour local authorities in running largescale campaigns, we will design and delivera campaign across NCL to address avarietyofwellbeingor long termconditions througha singlepreventativemessagewithcommonNCLbranding. Specific interventions: smoking cessation; alcohol screening, liaison and outreachteams; weight management programmes; diabetes prevention programme;multifactorial falls intervention; long-acting reversible contraception; communityresilience;increasedaccesstomentalhealthservicesforchildrenandnewmothers;London’sdigitalmentalhealthprogramme.
• Diagnosing residents with clinical risk factors and long term conditions muchearlier to increase lifeexpectancy.Oncediagnosed,empowering themtomanagetheir own condition(s) alongsideproactivemanagementbyhealthprofessionals topreventthedevelopmentoffurtherconditionsandcomplications.Specific interventions: increasing awareness and case finding (including nationalcancerscreeningandHIVtesting)andappropriatemedicationstocontrolconditionsfor people with high blood pressure, diabetes, atrial fibrillation; self-care andstructured self-management for long term conditions; reablement offers in socialcareandcarenavigation.
WewillbuilduponontheindividualstrengthsthateachpartofthepublicsectorinNCLcanbringtopreventingdiseaseand illhealth. Aswellastraditional ‘healthprofessionals’ thisalsomeansworkingwithlocalauthorityhousingofficersandtheLondonFireBrigadein,forexample, preventing falls. We also recognise the key contribution that voluntary andcommunity sector organisations can make in achieving disproportionately greaterimprovementsinhealthforresidentswithmentalillhealthandlearningdisabilities,specificBME groups, and those in the most deprived communities, and we are committed toworkingmorecollaborativelywiththeseorganisations.
6.2 Servicetransformation
Tomeet thechangingneedsofourpopulationwewill transformtheway thatwedeliverservices, shifting the balance of care from reactive to proactive. This will be throughensuringpeopleachieve thebest start in life,developingour care closer tohomemodel,creating a holistic approach to mental health services, improving urgent and emergencycare, optimising the elective pathway, consolidating of specialtieswhere appropriate andtransformingcancerservicestoimprovetheend-to-endexperience.Socialcareplaysakeyroleinallaspectsofservicetransformation.
6.2.1 Achievingthebeststartinlife
Childrenmakeupbetween25%and30%ofthepopulationacrosstheNCLfootprintwhichmeansthatservicetransformationmustincludeaspecificfocusonourchildrenandyoungpeople.We recognise thatproviding childrenwith thebest start in life is critical for theirdevelopmentandhealth long term.Wehave identified interventionsacross thepathway,

20
from prevention to acute care, that are focussed specifically on improving health andoutcomesforchildrenandyoungpeople.
In the context of a considerable body of research suggesting that fetal exposure to anadverse environment in-utero sets the trajectory for child and adult health in terms ofcongenital malformations, obesity, diabetes and cardiovascular disease, we will explorewaystolinkprimarycare,publichealthandmaternityservicestooptimisematernalhealthbefore, during and after pregnancy. In particular, smoking cessation, weight reduction,optimisation of blood sugar control in diabetics and improvement of diet in women ofreproductiveagehasthepotentialtoreducethehealthneedsofchildren.Wewillleveragethe work of our NCL Maternity Network to ensure that our local maternity systemimplements the findings of the nationalMaternity review: Better Births.We are keen totakepartintheNationalMaternityTransformationprogrammeasanEarlyAdopter.
Wewillpromoteactivetravel,sportandplayforchildreninschools,forexampleinvolvingschoolstodelivertheTake10,Active15,Walkadailymileinitiativesthatotherpartsofthecountryhaveadopted to support this.By2020/21,our aim is that4outof 5early years’settingsandschools inNCLwillbeaccreditedaspartofthehealthyschools,healthyearlyyearsorsimilarlyaccreditedprogrammeforpromotinghealthylives.
Wewilladdressmentalillhealthinchildrenasearlyaspossible:developingantenatalandpostnatalinterventionsformotherswithmentalillhealth;improvingservicesforparentingsupport, health visiting, and signposting; and creating targeted services that focus onvulnerablehighriskfamilies.WewillcapitaliseontheuniversalservicesofMIND,Place2Beand voluntary sector initiatives like Hope Tottenham that are already established andworkingdirectlywithfamiliesandyoungpeople.AspartofourChildandAdolescentMentalHealthServices(CAMHS)andperinatalinitiativeledthroughthementalhealthworkstream,wewill:
1. Develop a shared dataset for CAMHS to enable comparison and shared learningacrossthe5boroughs
2. Tackleeatingdisordersbyestablishingdedicatedeatingdisorderteamsinlinewiththewaitingtimestandard,servicemodelandguidance
3. Upskillourworkforcetomeetthementalhealthandpsychologicalwellbeingneedsof children and young people, including developing a children and young people’sIAPTworkforcecapabilityprogramme
Tai,14,suffersfromseveredepression.WiththeinvolvementofTai,hisfamily,andhisCAMHSpractitioners,TaihasbeenadmittedintoaTier4unitonaplannerbasis.Previously,itwaslikelythatTaiwouldhavebeenplacedfarfromhome.Infuture,withthelocalcommissioningofTier4hewillbeabletobeplacedclosetohome.ThiswillenablebetterlinkagewiththelocalCAMHScommunityteam,whichwillhavealsobeenenhanced.Together,thesefactorswillmeanTaihasabetterexperienceofcareandstaysinhospitalforashorterlengthoftime.WhenTaiisdischargedbackintothecommunity,hewillhaveanenhancedcareplantosupporthimtokeepwell.

21
4. BuildonourTransformingCareinitiativebysupportingchildrenandyoungpeoplewith challenging behaviour in the community in order to prevent the need forresidentialadmission
5. Improve perinatal mental health services by developing a specialist communityperinatalmentalhealthteamthatservestheNCLpopulationandthephysicalhealthacutetrustswithinNCL
6. ImplementaChildHousemodelfollowingbestpracticetosupportabusedchildren7. Create a 24/7 crisis pathway for children and young people, including local
commissioning of Tier 4 CAMHS to eliminate out of area placements for non-specialistacutecareby2020/21;andreviewofS136
8. Developaco-commissioningmodelforyouthjusticeworkingwithNHSEngland.
TheprinciplesofTHRIVEwillbeusedasanoverarchingapproachtoourCAMHSwork,withthe aim that at least 32% of children with a diagnosable condition are able to accessevidence-basedservicesbyApril2019assetoutintheMentalHealthTaskforce.
6.2.2 Healthandcareclosertohome
Healthandcarewillbeavailableclosertohomeforall,ensuringthatpeoplereceivecareinthebestpossiblesettingatalocallevelandwithlocalaccountability.Wealreadyhavemanyhigh quality services outside acute settings acrossNCL, but our health and care closer tohomemodelwillfocusonscalingtheseservicesup,reducingvariationandmakingthisthedefault approach to care. Social carewill play a key role in the design, development andexpansionofthefuturemodel.
Wewilladdressthesustainabilityandqualityofgeneralpractice, includingworkforceandworkload issues. It is recognised that for some people, health and care being deliveredclosertotheirhomeisnotalwaysthebestchoice,andthereforehighqualityhospital-basedandcarehomeserviceswillcontinuetobeavailablewhenneeded.
Attheheartofthecareclosertohomemodelisa‘place-based’populationhealthsystemofcaredeliverywhichdrawstogethersocial,community,primaryandspecialistservices.Thiswillbeunderpinnedbyasystematicfocusonpreventionandsupportedself-care,withtheaimofreducingdemandonthesystemovertime.Wewilldelivertherightcareattherighttimetothewholepopulation.Thecareclosertohomemodelisoneofthekeyvehiclesby
MsSahniis87andhasfourchronichealthproblems.Previously,shehadtobookseparateappointmentswithdifferentprimarycareprofessionalstohavealloftherelevantcheck-upsandappointmentsthatsherequired.Infuture,MsSahniwillbeinaspecial“stream”ofpatientswhowillhavealloftheircareco-ordinatedbyaveryexperiencedGP.ThiswillallowhertoseethespecialistheartordiabeticnursesattheIntegratedCareCentrelocatedatherGPsurgery.Therewillalsobeacarenavigatorintheteamwhocanhelptosortthingsoutforherathome,includingcommunitysupportwhensheneedsit.

22
which we will contribute towards the overall delivery of the Better Health for Londonoutcomes.
Exhibit 5:Deliveryof theBetterHealth for Londonoutcomes through thehealthand careclosertohomemodel
Specificinterventionsthatmakeupthescopeofthecareclosertohomemodelinclude:
• Developing ‘Care Closer to Home Integrated Networks’ (CHINs): CHINs may bevirtualorphysical,andwillmostlikelycoverapopulationofc.50,000people.Theywillbehometoanumberofservicesincludingthevoluntaryandcommunitysectorto provide a more integrated and holistic, person-centred community model,including health and social care integrated multi-disciplinary teams (MDTs), careplanningandcarecoordinationforidentifiedpatients.Interventionsfocussedonthestrengthsofresidents,familiesandcommunities;improvingqualityinprimarycare;andreducingunwarrantedvariationwillalsooperatefromCHINs, includingQualityImprovementSupportTeams(QIST)toprovidehands-onpracticalhelpforindividualGPpracticestoensureaconsistentqualitystandardandoffertoallpatients.Thiswillincludesupportforcasefindingandproactivemanagementofhighbloodpressure,atrial fibrillation and diabetes. We have already piloted CHINs, for example theBarnetIntegratedLocalTeam(BILT)33hubwhichprovidescoordinatedcareforolderresidentswithcomplexmedicalandsocialcareneeds,aswellasprovidingsupport
33 BarnetintegratedCareLocalityTeam,2016
Thereismoreopportunity todevelopskills
Lessstressasservicesworkbetter together
Moreopportunitytodevelopandimproveservicestomeettheneedsofpatients
Greaterassuranceaboutthequalityandsafetyofcare
Servicesareeasiertounderstand
Moreservicesareavailableclosertomyhome/work
Physicalandmentalhealthneedscanbemetoutsideofhospital
TheNHSandthelocalauthoritiesprovidecaretogether
Thehealth andcaresystemisfinanciallysustainable
Moreplannedcareinthecommunity
Greater confidenceinthesystemtosupport familiesandcommunities
Improvedoutcomes andreduced inequalities
ENABLERS:• JointlydesignedcarepathwaysthatconsistentlyWorkforcedevelopmentincluding joint training• Deliveryprioritised inpeoples’ jobplans• IM&T:ITinteroperability
ENABLERS:• Engagementofthepublicandusers• Engagementofallrelevantserviceproviderse.g.voluntarysector,schools, others• IM&T:Electronicrecordsharing
ENABLERS:• Supportive contracting &commissioning• Upfront investmenttodevelopOOHservices• Systemsfortimelymonitoring ofperformance enablingrapidlearningandadaptionofservices
Morecaregiveninthecommunity
Increasedworkforce andcapabilities
Greaterdiversityofstaffandservices
Morejointworking
Greatercapabilityforinnovation
Peoplelookingaftermeworktogether andknowmycareplan
Abletoaccesscareclosertomyhome/workandinlotsofdifferentways
Differentservicesavailableclosetohome
Peopleareinformed abouttheir ownhealthandkeepingwell
Servicesplannedtodeliverhighqualitycareforbestvalue
Professionals
Individualsusingservices
Populations

23
tocarers.TheBILThubhasbeenopensinceApril2016andisajointfundedhealthandsocialcarepilot.
• Extendingaccesstoprimarycare:patientswillbeabletoaccessconsultationswithGPs or other primary care professionals in their local area for pre-bookable andunscheduledcareappointmentsbetween8amand8pm7daysaweek.
• Supportinghealthierchoices:inlinewithourpreventionagenda,thecareclosertohome model will include upscaling our smoking cessation activities by 9-fold toreduce prevalence and hospital admissions; increasing alcohol screening and thecapacityofalcoholliaisonservicesandalcoholassertiveoutreachteamsacrossNCL;scalingupweightmanagementprogrammeswithintegratedphysicalandwellbeingactivities;andreducingunplannedpregnanciesbyincreasingtheofferanduptakeoflongactingreversiblecontraception.
• Improving access through technology and pathways: telephone triage, virtualconsultationsandonlinebookingsystemswillbeavailableforallpatients.
• Supporting patients through social prescribing and patient education: the carecloser to home model will include a greater emphasis on social prescribing andpatienteducation.Supportwillbeavailableforpatients,carersandprofessionalstobeconfidentusersofinformationandITsolutionsthatenableself-managementandcare,aswellascarenavigationsupporttodirectpatientstotherightservices.
• 24/7 access to specialist opinion in primary care: primary care will be able toprovide more complex patients with a number of options for specialist opinionoutside of the hospital itself. These range from: 1) advice only 2) an urgent 'hotclinic' appointment in an out-patient clinic 3) assessment in an ambulatoryemergency care facilityand4) admission toanacuteassessmentunit. Inaddition,consultant-led clinical assessment and treatment services offered in CHINs willenablemorepatients tobemanaged in theprimary care setting. Specialties tobeconsidered include gynaecology; ENT; urology; dermatology;musculo-skeletal; andophthalmology.
• GP front door model in Emergency Departments: we will review the existingprovision acrossNCLofGP led triage, treatment and streaming for all ambulatorypatients will be provided at the front door of Emergency Departments. GPs andnursesonthedoormakedecisionsaboutwherethepatientisbesttreated–whichcould be in the urgent care centre or emergency department, or redirection toalternativeservices.
• Falls emergency response team and multifactorial intervention: multifactorialinterventions combining regular exercise, modifications to people’s homes andregular reviewofmedicationswill prevent people from falling in the first place. Ifthey do fall, falls partnership ambulance vehicleswill be availablewith advanced,multi-disciplinary practitioners. In addition, a specific falls service will supportpatientstoremainathomeafterafall.
• Enhancedrapidresponse(ERR):arapidresponseteamwillpreventanadmissiontohospital for those in crisis, providing enhanced therapy, nursing and social worksupporttosupportpeopletostayintheirownhome.

24
• Acute care at home: where there is a medical need, acute clinical care will beprovided at home by aMDT to provide the best possible patient experience andoutcomes,andenablethepatienttobenefitfromholisticintegratedcare.
• Frailtyunits:adedicatedservice, suchas thatalready inplaceat theWhittington,that will be focussed on rapid assessment, treatment and rapid discharge of frailolderpeoplethatcouldpotentiallybeco-locatedwithintheEmergencyDepartment.Thiswillenableambulatorycareforpeopleagedover65.ThesewouldberolledoutacrossNCL.
• Enhancedcarehomesupport: provided to stabiliseand /or treat residents in thecarehomewhereappropriatetherebyreducingthelevelofconveyances,unplannedattendancesandadmissionstosecondarycare.Thecareclosertohomemodelwillpreventemergency readmissions fromcarehomes throughdevelopmentofa carehomebundle, includingaproactiveapproachtopreventionandearly identificationofcomplications.
• Endof life care:wewill supportpeopleat theendof life to receive the care thatthey need to enable them to die in their place of choice via rolling out the Co-ordinateMyCare(CMC)careplanningprogramme,andensuringthenewIntegratedUrgentCareservice(seesection6.2.4)hasaccesstoCMCplans.
Acheivingcareclosertohomewillneedtobeunderpinnedbystrongresilientcommunitiesthat are able to support residents live independently at home, where that support isneeded. The supportmay be needed from families, carers, neighbours or from voluntaryandcommunitygroupsallofwhomhavecentralrolestoplay.
We plan to bring together the funding currently used for Locally Commissioned Services(LCS)and the premium spent on Personal Medical Services (over and above GMS) andestablish one LCS contract framework for the whole of NCL. This LCS contract will haveagreed outcomes which are shared with the Health And Care Closer to Home Networks(CHINs) and the Quality Improvement Support Teams (QISTs) so that all local GPs areprovided with the necessary funding and incentives to fully engage with these vitalcomponents of the health and care closer to home work.Delivery of this whole systemalignment is partly dependentonNHSEngland (London)delegating commissioningof thePMSpremiumtotheCCGswhichiscurrentlyunderdiscussionwithallkeyparties.
In support of delivering our health and care closer to home model, Islington CCG hasexpressedaninterestinbecominganIntegratedPersonalCommissioning(IPC)siteinordertoimprovehealthandwellbeingoutcomesthroughpersonalisedcommissioning,improvedcareandsupportplanninganddevelopinganassetbasedapproachtosupportsolutions.
TheIPCsitewill:
• improve outcomes for patients with care delivered closer to home, and aim toreduceunplannedadmissions
• realign service provision in light of new service developments related to IPC andPersonalHealthBudgets
• reviewexistingcontractstoassessimpactandidentifyopportunitiesforrealignmentbasedonanumberofotherdevelopmentssuchasNewCareModelsandIPC.

25
Improving outcomes will be the crucial measure of success of the care closer to homemodel. Using national and international evidence, we have estimated that some of theoutcomesthatourhealthandcareclosertohomemodelcouldpotentiallydeliverare:
• 70%ofpeopleattheendoftheirlifewillhaveacareplantosupportthemtodieintheirplaceofchoice
• 4%decreaseinunplannedpregnancies• a reduction in alcohol consumption with 10% fewer alcohol-related hospital
admissions• upto150,000feweremergencydepartmentattendances• 63,000fewernon-electiveadmissions• 35,000feweroutpatientattendances• 10%reductioninfalls-relatedhospitaladmissions• ahalvingofthenumbersoflateHIVdiagnoses• 50,000weightmanagementreferralsleadingtoareductioninexcessweight• 66%ofpeoplewithhighbloodpressurehaveitdiagnosedandcontrolled• 55%ofpeoplewithatrialfibrillationarereceivinganti-coagulants• 69%ofpeoplewithdiabeteshavecontrolledbloodglucose.
6.2.3 Mentalhealth
Wewilldevelopa‘stepped’modelofcare(seeexhibit6)supportingpeoplewithmentalillhealth to livewell, enabling them to receive care in the least restrictive setting for theirneeds.34Werecognisethekeyroleandaccountabilitiesofsocialcareforpeoplewithlong-standingmentalillhealthanddrawingonthiswillbecentraltothesuccessofthesteppedmodel.
Exhibit6:Thementalhealth‘stepped’modelofcare
34 AsidentifiedintheMentalHealthTaskforceReport

26
Weaimtoreducedemandontheacutesectorandmitigatetheneedforadditionalmentalhealthinpatientbeds.ThiswillimproveoverallmentalhealthoutcomesacrossNCL,reduceinequalities for thosewithmental ill health, enablemore people to livewell and receiveservicesclosertohomeandensurethatwearetreatingbothphysicalandmentalillhealthequally.Wewillachievethekeymentalhealthaccessstandards:
• more than50%ofpeopleexperiencinga firstepisodeofpsychosiswill commencetreatmentwithaNICEapprovedcarepackagewithin2weeksofreferral
• 75% of people with common mental health conditions referred to the ImprovedAccesstoPsychologicalTherapies(IAPT)programmewillbetreatedwithin6weeksofreferral,with95%treatedwithin18weeks.
Initiativeswillcovermentalhealthsupportforallagegroupsandinclude:
• Improvingcommunityresilience:bothforthegeneralpopulation,andthoseatriskof developing mental ill health or of it becoming more severe. For the generalpopulationthisincludesapromotionaldriveaimedatincreasingbasicmentalhealthawareness includingself-awareness,normalisingmentalhealthneedsandreducingstigma.Fortheatriskpopulationfocuswillbegiventoimprovingaccessandsupportthrough training of non-mental health specialists to recognise mental ill healthsymptoms, improving service navigation, development of open resources, andprovisionof individualandgrouptherapies;employmentsupporttohelppeopletomaintainandgetback intowork includingthrough IndividualPlacementSupport35;and suicide prevention work to strengthen referral pathways for those in crisis,linkedtothelocalmultiagencysuicidepreventionstrategies.36ThiswillbedeliveredinconjunctionwithotherregionalandnationalschemessuchastheLondondigitalwellbeingplatform.Wewillcontinuetobuilduponcurrentwork;forexampleBarnetCCGandlocalauthorityarealreadyworkingtowardsadementiafriendlyboroughbyproviding lunch clubs, reminiscent therapy and engagingwith local shops to raiseawareness.
• Increasingaccesstoprimarycarementalhealthservices:ensuringmoreaccessiblementalhealthsupportisdeliveredlocallywithinprimarycareservices,developedaspart of the CHINs; enabling both physical health and mental health needs to be
35FiveYearForwardView-29,000morepeoplelivingwithmentalillhealthshouldbesupportedtofindorstayinwork(~725withinNCL)36FiveYearForwardView-Reducesuicideby10%
Maisiesuffersfromdementia,andiscaredforbyherhusbandAlbert.Previously,afterfallingathome,Maisiewasadmittedtohospital.Duetotheaccidentandchangeofsurroundings,Maisiewasagitatedandmoreconfusedthannormal.Infuture,thehospitalwillhaveCore24liasionpsychiatrymeaningthattheliaisonteamwillbeabletohelpthehospitalsupportbothMaisie’sphysicalandmentalhealthneeds.AsMaisiewillreceiveholisticcareitwillmeanthatsheisreadytobedischargedsoonerthanifonlyherphysicalhealthneedsweresupported.Maisie’shusbandAlbertwillalsobesupportedbythedementiaservice,allowinghimtocontinuetocareforMaisieathome.

27
supportedtogether37.WewilloffersupportdirectlytopatientsandsupporttoGPsand other professionals; enablingmore people to access evidenced basedmentalhealthservices38,andmorecaretobeofferedthroughCHINsratherthanrequiringreferraltosecondarycarementalhealthservices.ServiceswillincludeincreasingtheIAPToffertoreach25%ofneed.39
• Improvingtheacutementalhealthpathway:buildingcommunitycapacitytoenablepeople to stay well and reduce acute presentations. This includes developingalternatives to admission by strengthening crisis and home treatment teams;reviewingHealthBasedPlaceof Safety (HBPoS) provisionwith the view to reducethenumberofunitsandtohaveasectorwideprovisionthatmeetsallrequirements;and investing in longer term supported living arrangements to ensure effectivedischarge,enablingmorepeopletolivewellinthecommunity.
• Developing a Female Psychiatric Intensive Care Unit (PICU): we will ensure localprovisionofinpatientservicestofemalepatientsrequiringpsychiatricintensivecare,where currently there is none. This will enable patients to remain close to theircommunities,with amore streamlined and effective pathway ensuring a focus onrecovery.40
• Investing inmental health liaison services: scalingup24/7 all-age comprehensiveliaison tomorewards and EmergencyDepartments, ensuring thatmore people inEmergencyDepartmentsandoninpatientwardswithphysicalhealthproblemshavetheirmentalhealthneedsassessedandsupported.
• CAMHSandperinatal:initiativesassetoutinsection6.2.1.• InvestinginadementiafriendlyNCL: lookingatpreventionandearly intervention,
supportingpeople to remainathome longerand supporting carers toensure thatwemeetnationalstandardsarounddementia,includingadementiadiagnosisrateofatleasttwo-thirdsoftheestimatednumberofpeoplewithdementia.
AnimportantenablerofanumberourinitiativesistheredevelopmentofboththeBarnet,Enfield and Haringey Mental Health Trust St Ann’s site and the Camden and IslingtonFoundationTrustStPancrassite(inconjunctionwiththeproposedrelocationofMoorfieldsEyeHospitalFoundationTrusttotheStPancrassite).
TheproposeddevelopmentsoftheStAnn’sandStPancrassiteswould:• transform the current inadequate acutemental health inpatient environments on
bothsites• providemoretherapeuticandrecoveryfocussedsurroundingsforpatientsandstaff• improveclinicalefficiencyandgreaterintegrationofphysicalandmentalhealthcare• release estate across the trusts, to enable development of community-based
integratedphysicalandmentalhealthfacilities• developworldclassresearchfacilitiesformentalhealthandophthalmologyenabling
practicetoreflectthebestevidence 37FYFV–atleast280,000peoplewithseverementalillhealthhavetheirphysicalhealthneedsmet(~7,000withinNCL)38FiveYearForwardView-moreadultswithanxietyanddepressionhaveaccesstoevidencebasedpsychologicaltherapies(~15,000withinNCL)39FiveYearForwardView40FiveYearForwardView-inappropriateoutofareatreatmentsforacutementalhealthcareshouldbeeliminatedinallareasby2020/21.

28
• provide landforbothprivateandaffordablehousing,aswellassupportedhousingforserviceusersandhousingforkeyworkers.
6.2.4 Urgentandemergencycare41
Overthenextfiveyears,wewilldeliverurgentandemergencycare(UEC)servicesthatarereliable,workwelltogetherandareeasilyunderstood.Ourserviceswillbeconsistentandinspire confidence in patients and professionals; supported by the use of an integrateddigitalcarerecordthatcanbeaccessedacrossorganisations.Thefirst2yearswillfocusonreducingvariation inour servicesand the latter yearswill focuson transformationof theurgentandemergencycaresystem,aligningcloselywiththecareclosertohomemodel.
Ouraimsareto:
• Create a consistent UEC service across NCL: all UEC services in NCL will meetNational and London-wide quality standards42 which will promote consistency inclinical assessmentand theadoptionofbestpractice.Patientswill be seenby themostappropriateprofessionalfortheirneeds,whichmayincludedirectingthemtoanalternativeemergencyorurgentcareservice.
• Develop and implement a high quality integrated UEC service: all urgent careservicesacrossNCL (includingNHS111,GPoutofhours,UrgentCareCentres)willwork together tooffer consistent care.These serviceswillbe renamed ‘Integrated
41 ThisworkstreamincludesallaspectsofUrgentandEmergencyCareprovisiondeliveredintheacutesetting,includingsupportforpeopletoleavehospital.Alsoinscopeisthedevelopmentofahighquality,integratedurgentcaresystem. 42AsdefinedbytheNHSEUECdesignationprocess
Maryis83yearsoldandlivesathomewithherhusband.Maryhadafallathomeandinjuredherankle.Herhusbandwasunabletohelphergetupsohecalled999foranambulance.MarywastakentothenearestA&Eandadmittedtohospital,wheresheisdiagnosedwithaurinarytractinfection(UTI).Shewasreviewedbytheconsultant:aplanwasputinplacefortreatmentofherUTIandphysiotherapywasrecommendedforherankle.Overtheweekend,Mary’sUTIimproved,buttherewasnoconsultanttoreviewherconditionorphysiotherapisttoprovidehercare,soMarywasunabletogohome.Whengoingtothetoiletinthenight,Maryfellagainandstayedinhospitalforafurther2weeks.Marybecameincreasinglylessmobileandmorefrailanddependent.
InfuturewhenMaryfalls,herhusbandwilldial999,andaparamedicwillbedispatched.Whentheclinicalassessmentdoesnotsuggestanyfractures,thecrewwillaccessthelocaldirectoryofserviceswhilstonsceneandelectronicallyreferMarytotheAcuteCareatHomeservicewithrequestfora12hourresponse.MarywillthenbevisitedathomebythefallsteamthenextdaywhowilldesignapackageofcareforMaryincludingreablement,allowingMarytostayathome.ThefallsteamwillbeabletodetectifthereisanythingunusualaboutMary’sbehaviour,andmakearapidappointmentwithherGPiftheysuspectaUTI.Marywillthengettheantibioticssheneedstoresolvethisatanearlystage.
29
Urgent Care’. We have commissioned a joined up new Integrated Urgent Careserviceprovidedbyoneprovider,LCW,whichgoesliveinOctober2016.ThisservicecombinestheNHS111andGPOut-of-Hours(OOH)services,andallowspatientstoaccessawiderskillmixofspecialisedcliniciansinanewNHS111clinicalhub.
• Develop high quality, responsive 7-day hospital UEC services: people will besupported to leave hospital as quickly as possible through building close linksbetweenacutecareprovidersandsocialcare.Wewillsupportshorterhospitalstaysby operating a simplified discharge or integrated ‘discharge to assess’ model:planning post-acute care in the community, as soon as the acute episode iscomplete,ratherthaninhospitalbeforedischarge.Thiswillbethedefaultpathway,withnon-acutebeddedalternatives for thevery fewpatientswhocannotmanagethis.
• Develophighquality,responsive7-daycommunityservices:wherepossible,peoplewillbesupportedandtreatedathomebycommunityandambulanceservices.Forthose people who do require ambulance transfer, the ambulance services will beabletouseanyUECservicesthatmeetsthepatient’sneed.
• DevelophighqualityambulatorycareservicesacrossNCL:wewilldevelopaservicethat reduces avoidable, unplanned admissions to hospital, such as that already inplace at the Whittington. All UEC services will create consistent ambulatory carepathways that support people to have their care on a planned basis, whereverpossible. This will provide same day emergency care to support patients to beassessed, diagnosed, treated and able to go home the same day without anovernightadmission.ThismodelwillberolledoutacrossNCL.
The focus on urgent and emergency care services will reduce the number of unplannedadmissions tohospital and supportpeople togohome fromhospital as soonaspossible.Thiswill improvepatientexperience, improveoutcomesandmake sure thatpeoplehavetheircareonaplannedbasiswhereverpossible.
6.2.5 Socialcare
Social care isacrucialpartofmanyofourworkstreams,particularlycarecloser tohome,TransformingCare,andmentalhealth,aswellaschildren'sandpublichealthinterventions.WeareconsideringhowlocalauthoritiescanworkwiththeworkforceleadsacrossNCLtodesign and develop proposals specifically for social care, including a focus on thesustainability of provider workforce, the sustainability of the registered workforce andstimulating the personal assistant workforce. We will ensure that our plans factor inpracticalstepsthatwecantakeaspartners toaddressproviderfailureandthehugerisksaroundcapacityandqualityinthedomiciliarymarket.
Theroleofsocialworkerswillbeessential todeliveringonourmodel forhealthandcareclosertohome,inadditiontotheroleofhomecareworkers,personalassistants,blendedrole between district nurses and care workers. The workforce workstream will considerthesecareerpathways,makingcareersintheseareasmoreattractivetosupportincreasedsustainabilityof theworkforce.Wewill quantify any investment thatmightbeneeded inworkforce from a social care point of view e.g. increasing numbers of domiciliary care

30
workers and, drawing on learning from elsewhere, we will quantify the return oninvestment.
Social care is also built into our mental health model, including a broader dimension ofpublic service support suchas employment supportworkers. Learningdisabilities is a keyareaof focus given thathalf of social care spend is on this group, and that childrenwithspecialeducationalneedsandlearningdisabilitieshaveworselongtermoutcomesinbothhealth and education. We need to start supporting thosewith learning disabilities fromearly childhood to ensure early detection and appropriate intervention. Many of ourinterventions, including health visiting, early years, community paediatrics, CAMHS, andworkingdirectlywithschoolswillensurethatwebettersupportthesechildren.WeplantoscaleupourTransformingCareworktoimplementenhancedcommunityprovision;reduceinpatientcapacity;upgradeaccommodationandsupportforthosewithlearningdisabilities;androlloutcareandtreatmentreviewsinlinewithpublishedpolicytoreducelonglengthsofstayinhospitalsandimproveindependence.
AspartofourSTPwewillexplorecollaborationandconsolidationopportunitiesbetweenlocal authorities in areas such as the hospital discharge pathway and the mental healthenablementprocess.Wewillconsiderwhatcanbecommissioneddifferentlyand/oratscale- particularly across health and social care, for example nursing homes.Wewill focus onrampingup theuseofdataanalysisand risk stratification;workingcohesivelywithpublichealthacross thepatch; leveraging telecare;andsharingof ideasand learningaboutbestpracticeintermsofhealthandsocialcareintegration.Ourpan-NCLbedstateanalysiswillconsidernon-healthbeds,includingthe6,440carehomebedsinNCL,sothatwegainanin-depthunderstandingofwhypeopleendupinthesebedsandhowbesttheirneedscouldbemetelsewhere(aswellastheresourcesitwouldtaketodothis).
We recognise the co-dependencies between health and social care: any change in eithersectormayhaveasignificantimpactontheother.Aswecontinuetodevelopourplans,wewill ensure local authorities are involved throughout so that we can mitigate any risksaroundthistogether,andtransformthesystemsothatitistrulyintegrated.
6.2.6 Optimisingtheelective(plannedcare)pathway
Building on the opportunities identified through RightCare, we will reduce unwarrantedvariation in elective (planned) care across providers in NCL. This will include reducingvariation in the length of stay in hospital and the number of outpatient appointmentsreceived by patients with similar needs. Optimised pathways will ensure patient safety,qualityandoutcomes,andefficientcaredelivery.

31
Wewilldrawon localexamplesofbestpractice, suchas theSouthWest LondonElectiveOrthopaedic Centre; and international best practice, such as Intermountain’s hipreplacement pathway redesign, which reduced the cost of total hip replacement by aquarter.43 Building on the evidence, we will redesign pathways with local clinicians,responding to local needs and opportunities. We will initially focus on areas with highvolume or high variability, where there is opportunity to achieve high impact bymakingchanges,suchasorthopaedics.
Wewillleveragethefollowingopportunitiesforimprovementtoelectivepathways:
• expertfirstpointofcontact:makingsurepeoplehaveaccesstotherightexpertisefromtheirfirstappointmentinprimarycare
• one-stop services: so that people do not need to attend multiple outpatientappointmentsbeforetheirprocedure
• efficientsurgicalpathways:toensuremaximumuseofstaffandtheatres• timelydischargeplanning:toreduceunnecessarytimeinhospital.
Todeliverontheabove,aseriesof interventionswillbeput inplaceateachstageoftheelectivepathway.Theseareillustratedinexhibit7.
43JamesandSavitz(2011).HowIntermountainTrimmedHealthCareCostsThroughRobustQualityImprovementEfforts�.HealthAffairs
Previously,John(whois75andhaspaininhisknee)madeanappointmentwithhisGP.TheGPreferredhimtothehospitalwherehewasseeninoutpatientsandsentforanMRIscan.AconsultantestablishedthatJohnneededakneereplacement.JohnwasabouttogoonatriptovisitfamilyintheUSAfor2months,sotheconsultantsenthimbacktohisGP.WhenhereturnedJohnsawtheGPagainaswellastheconsultant,whosenthimtopreoperativeassessment.Hewasfoundtohavehighbloodpressure,andwassentbacktotheGPfortreatment.Oncehisbloodpressurewasundercontrol,Johnwaslistedandthenadmittedforsurgery.Hespentabout5daysinhospital,andthenreturnedhome.Inthefuture,JohnwillseeanextendedscopephysiotherapistattheGPsurgeryforhiskneepain.ThephysiowillarrangetheMRI,anddiscusstheresultswithJohn.ThephysiowillidentifythatJohnhasraisedbloodpressurewhilecompletinghiselectronicreferraltemplatetotheconsultantatthehospital,andliaisewiththeGPtomakesurethisistreatedbeforeheisreferred.Johnwillhavehishospitalappointmentandpre-operativeassessmentonthesameday,andwillbegivenalltheinformationheneedstoprepareforaftertheoperation.
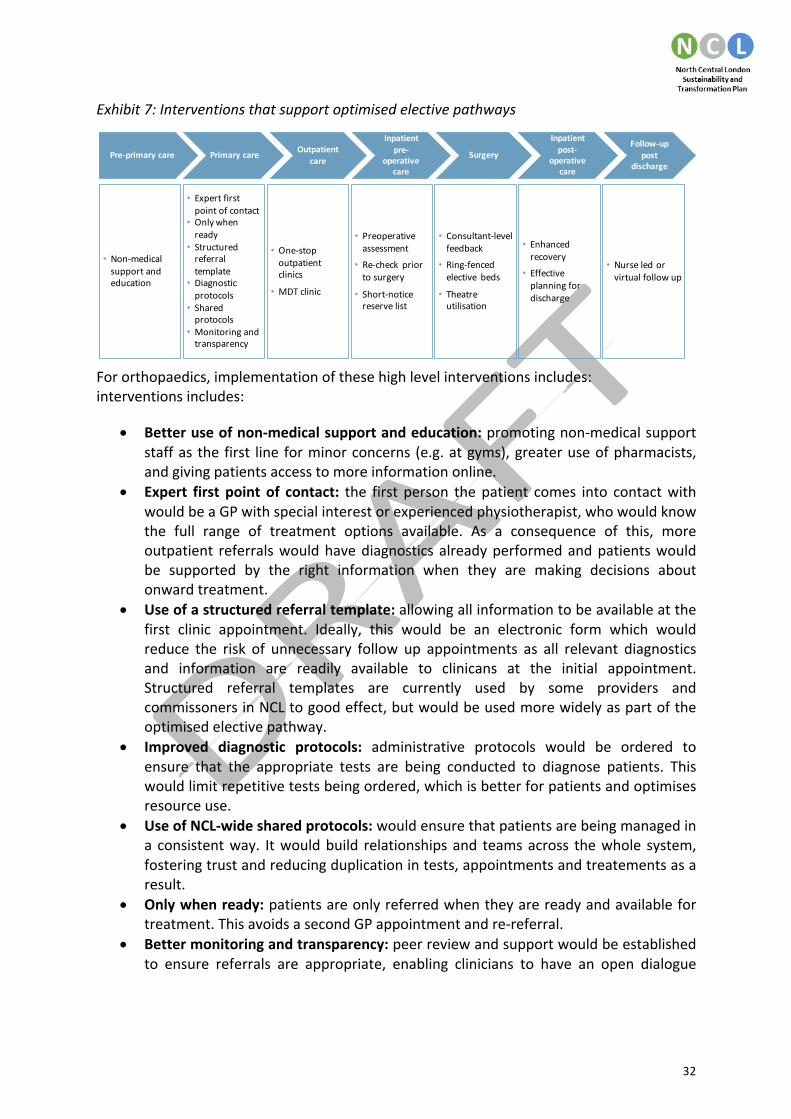
32
Exhibit7:Interventionsthatsupportoptimisedelectivepathways
Fororthopaedics,implementationofthesehighlevelinterventionsincludes:interventionsincludes:
• Betteruseofnon-medicalsupportandeducation:promotingnon-medicalsupportstaffas the first line forminorconcerns (e.g.atgyms),greateruseofpharmacists,andgivingpatientsaccesstomoreinformationonline.
• Expert first point of contact: the first person thepatient comes into contactwithwouldbeaGPwithspecialinterestorexperiencedphysiotherapist,whowouldknowthe full range of treatment options available. As a consequence of this, moreoutpatient referralswouldhavediagnosticsalreadyperformedandpatientswouldbe supported by the right information when they are making decisions aboutonwardtreatment.
• Useofastructuredreferraltemplate:allowingallinformationtobeavailableatthefirst clinic appointment. Ideally, this would be an electronic form which wouldreduce the risk of unnecessary follow up appointments as all relevant diagnosticsand information are readily available to clinicans at the initial appointment.Structured referral templates are currently used by some providers andcommissonersinNCLtogoodeffect,butwouldbeusedmorewidelyaspartoftheoptimisedelectivepathway.
• Improved diagnostic protocols: administrative protocols would be ordered toensure that the appropriate tests are being conducted to diagnose patients. Thiswouldlimitrepetitivetestsbeingordered,whichisbetterforpatientsandoptimisesresourceuse.
• UseofNCL-widesharedprotocols:wouldensurethatpatientsarebeingmanagedina consistentway. Itwouldbuild relationshipsand teamsacross thewhole system,fosteringtrustandreducingduplicationintests,appointmentsandtreatementsasaresult.
• Onlywhenready:patientsareonlyreferredwhentheyarereadyandavailablefortreatment.ThisavoidsasecondGPappointmentandre-referral.
• Bettermonitoringandtransparency:peerreviewandsupportwouldbeestablishedto ensure referrals are appropriate, enabling clinicians to have an open dialogue
Thekeyinterventionsmaptodifferentstagesalongtheelectivepathway
Pre-primarycare Outpatientcare
Inpatientpre-
operativecare
Follow-uppost
discharge
Inpatientpost-
operativecare
Surgery
• Non-medicalsupportandeducation
• One-stopoutpatientclinics
• MDTclinic
• Consultant-levelfeedback
• Ring-fencedelective beds
• Theatreutilisation
• Enhancedrecovery
• Effectiveplanningfordischarge
• Nurseledorvirtualfollowup
• Preoperativeassessment
• Re-check priortosurgery
• Short-noticereservelist
Primarycare
• Expertfirstpointofcontact
• Onlywhenready
• Structuredreferraltemplate
• Diagnosticprotocols
• Sharedprotocols
• Monitoringandtransparency

33
regarding the quality of referrals and continuously improve their own referralpractices.
• One-stopoutpatientclinics:access tosimultaneouspre-assessmentandadditionaldiagnosticsinasingleplace,reducingtheneedforunnecessaryfollowups.
• Multi-disciplinary team (MDT) clinics: clinics which consist of multiple differentpeople working together to triage to the most appropriate clinician. Consultants,extendedscopephysiosandGPswithspecialinterestswouldallworkingtogetherinasinglesettingtoformtheMDT.
• Pre-operative assessments conducted at the first outpatient appointment: ifpatientsarenotfoundtobefit,thentheirplanisreviewedthesameday.Thiswouldbesupportedbygreateruseofe-selfassessmentbypatients intheirhome.Rehabandpost-operative packages of carewould be arrangedprior to referral, enablingpatients who are at risk of staying for long lengths of time in hospital to beproactivelyidentified.
• Re-check prior to surgery: patients will be contacted 48-72 hours before theirsurgery to reduce the riskof latecancellations.This checkwillensurepatientsarestillwellenoughforsurgery,andwanttogoaheadwiththeplannedprocedure.
• Short-notice reserve list: to ensure that gaps caused by late cancellation can befilledbypatientswhoarereadyfortreatmentwhichallowstheatrestobeusedmostefficiently.
• Consultant-levelfeedback:transparencyoflistutilisationandcasevolumesperlist.This allows for peer challenge to take place between consultants, to ensure thehighestqualityandmostefficientpracticesarebeingmaintained.
• More effective planning for discharge: discharge planning serviceswill be offeredearlierintheprocess,beforepatientsareadmittedtohospital.Thiswillgivegreateraccesstocommunitysupportservices,andreducedelaysindischarge.
• Enhanced recovery pathways will be consistently applied: patients will have agreaterunderstandingoftheirexpectedlengthofstaywhentheyareadmitted,andbeadvisedonthebestcourseofactiontoavoidstayingforlonger.
• Ring fenced elective beds will be available: to reduce wasted theatre time, anddiminishtheriskofinfectionforelectivepatients.
• Theatreutilisationwillbeoptimised:byschedulingcasesandensuringthatcriticalequipmentisproperlyscheduledtomaintaintheorderandrunningoflists.
Inadditiontotheimprovementsbeingworkedthroughfororthopaedics,furtherspecialtieshavebeenidentifiedforfocusedpathwaydesign.Theseare:
• Urology• Generalsurgery• Colorectalsurgery• Hepatobiliaryandpancreaticsurgery• Uppergastrointestinalsurgery• Gynaecology• Gynaecologicaloncology• Ear,NoseandThroat(ENT)

34
• Vascularsurgery• Breastsurgery• Musculoskeletal(MSK)• Ophthalmology• Generalmedicine• Gastroenterology• Endocrinology
As well as delivering efficiency savings, reducing variation in planned care will improvepatientoutcomesandexperiencethrough:
• improved access to information and support to help people manage conditionswithoutsurgicalintervention
• supportforpeopletoaccesstotherightprofessionalexpertisethefirsttime,ratherthanbeingreferredbetweenseveraldifferentprofessionals
• improvedaccesstosurgicalinterventionsascapacitywillbefreedup• patients receive a single outpatient appointment rather than needing to make
severalattendances• lesstimespentinhospital,meaninglesschanceofacquiringinfectionsandreducing
theriskoflostindependence• ensuring access to the right post-operative support, helping patients get back to
normallifemorequickly.
Reducingvariationwillalsoimprovestaffexperience,includingensuringaccesstotherightprofessional expertise when needed, better access to high quality diagnostics, improvedrelationships between professionals in different care settings and increasing sharing andlearningfrombestpracticeacrossthelocalprofessionalcommunities.
6.2.7 Consolidationofspecialties
We will identify clinical areas that might benefit from being organised differently (e.g.managingmultiple services as a single service), networking across providers, or providerscollaboratingand/orconfiguringinanewwayinordertodeliverhighimpactchangestomajor services. While changes of this sort can be challenging to implement andcontroversial with the public, we should not shy away from consideringmaking changes
InLondon,twothirdsofearlydeathsinpeopleunder75arefromcancerandheartdisease,thereisahighriskofheartdiseaseamongthelocalpopulationandthenumberofpeoplediagnosedwithcancerisgrowing.Specialists,technologyandresearcharespreadacrosstoomanyhospitalstoprovidethebestround-the-clockcaretoallpatients.IfweweretoimprovelocalsurvivalratesforheartdiseaseandallcancersinlinewithatleasttherateforEngland,over1,200livescouldbesavedeachyear.(Source:UCLHnews,14March2014)UCLH,BartsHealth,theRoyalFreeandanumberofothernorthLondontrustsimplementedasignificantservicereconfigurationtoaddresstheseissues.CardiovascularcareservicesprovidedatTheHeartHospital,TheLondonChestHospitalandStBartholomew’sHospitalwerecombinedtocreateanintegratedcardiovascularcentreinthenewbuildingatStBartholomew’s.For5complexorrarecancers,specialisttreatmentisprovidedincentresofexcellenceacrossthearea.Servicesforothertypesofcancerandgeneralcancerservices,suchasmostdiagnosticsandchemotherapy,continuedtobeprovidedlocally.

35
wherewearesurethatsignificantimprovementsinthequalityofcarecanbeachieved.
We are not starting from scratch in this area: considerable service consolidation andspecialisationhasalreadytakenplaceinNCL.Recentexampleswherewehavesuccessfullydonethisinclude:
• Cardiac/cancer(seecaseexamplebox)• Neurosurgery• PathologyJointVenture• Renalmedicine• Hepatologyandhepatobiliarysurgery• Neurosurgery• Vascularsurgery• Ear,NoseandThroat(ENT)• BoneMarrowtransplantation• Uppergastrointestinal• Malignantgynaecology• Cardiology• Majortraumaservices• Strokeservices• Plasticsurgery• Respiratorysub-specialties• Cancer services including: pancreatic cancer, renal cancer, skin cancer, prostate
cancer,headandneckcancer
However, we recognise that theremay be other service areas which are or will becomevulnerable in the future. There aremany reasonswhy consolidation of servicesmight beconsideredas apossibleopportunity for improvement. First and foremost,weagree thatimprovingquality should be the key driver for exploring consolidation, particularlywherethere is clear evidence of patients achieving better outcomes.Where there is a ‘burningplatform’and it iswidely accepted that a serviceneedsurgent attention (forexample, inaddressing issuesofworkforcesustainability),consolidationwillbeexploredasanoption.Releasingcostsavingstosupportoverallsystemsustainabilityisanotherdriverforexploringpotentialconsolidationopportunities.
Thisworkisatanearlystage.Nodecisionshavebeenmade,butwehaveidentifiedserviceswherewewillreviewwhethersomeformofconsolidationmaybeworthconsideration.Itisrecognised that fundamental, large scale reorganisationmay take longer than the 5 yearstrategic horizon of the STP. As such,we havemade no assumptions of financial benefitfromthiswork.
To understandwherewe should focus furtherwork, senior clinicians have systematicallyassessedservicesbasedonwhetherconsolidationoralternativenetworkingisrequiredand/orcouldbebeneficial.Thishasenabledustoidentifyalonglistofservicespotentiallyinscopeforfurtherworkoverthe5yearperiod,forexample:

36
• Emergencysurgery(outofhours)• Maternityservices,inthecontextoftheBetterBirthsinitiative(seesection6.2.1)• Electiveorthopaedics• Mentalhealthcrisiscareandplaceofsafety• Mentalhealthacuteinpatientservices• Histopathology• Generaldermatologyservices
Overthenextyeareachoftheseserviceswillbereviewed in lightofwhethertheywouldbenefitfromconsolidationornetworking.Weareintheprocessofdevelopingproposalstobring together some mental health inpatient services in order to drive significantimprovementsinqualityandpatientexperienceassetoutinthementalhealthworkstream(seesection6.2.3).Inaddition,workisunderwaytounderstandpotentialopportunitiesforconsolidationofmentalhealthplacesofsafety. 6.2.8 Cancer
WewillsavelivesandimprovepatientexperienceforthosewithcancerinNCLandbeyond.CommissionersandprovidersacrossNCL joinedtogethertoformourCancerVanguard, inpartnershipwithManchesterCancerandRoyalMarsdenPartners,withtheaimofachievingearlier cancer diagnosis, ensuring effective use of cancer outcomes information andadoptionofrecognisedbestpracticeacrossthefullspectrumofcancerpathways.
OurcancerworkstreamisderivedfromtheVanguardagendaandencompassesarangeofimprovementstocurrentpractice.Thekeyareasoffocusinclude:
• Earlydiagnosis:toaddressimpactoflatediagnosisonsurvivaloutcomesacrossNCL,wewill targetspecificcausesof latediagnosisandpoordetectionrates.Targetingcolorectal and lung pathways are a particular focus given the high percentage ofpatients receiving late stagediagnoses, often in EmergencyDepartments.Wewillroll out the Multi-disciplinary Diagnostic Clinic model for vague abdominalsymptoms,promoteadoptionofstraighttotestmodelsanddeliveraprogrammeto
PreviouslyMargaret,aged60,wenttoseeherGPwithpersistentepigastricpainforseveralweeks.Shewasotherwisewell,anddidnothavereflux,diarrhoea,vomitingorweightloss.Overthecourseofnext3weeks,Margaret'sGPorganisedtestsandruledoutanyinflammation,heartproblem,orgallstonesthatcouldcausethepain.HealsostartedMargaretonatablet(lansoprazole)totrytoreduceinflammationfromtheacidonherstomachlining.However,Margaret'spainwasmorepersistentthistimeandshewasstillworried.Inthenewsystem,Margaret’sGPwillbeabletoreferhertotheMultidisciplinaryDiagnosticCentreatUCLHdespitethefactthathersymptomsarenotconsidered“redflag”.Here,Margaretwillbeassessedforvagueabdominalsymptoms.Aclinicalnursespecialistwillseeher4daysafterreferral.TheteamwillidentifythatMargarethasearlystagepancreaticcancerandbecauseitispickedupearlyshewillbeabletoaccesspotentiallycurativekeyholesurgery.

37
improveawarenessofcancersymptomsinprimarycare.• Newmodels of care: we are developing the case for a single providermodel for
radiotherapy in NCL, to help achieve financial sustainability, reduce variation inclinical protocols and improve patient access to research and clinicalinnovations. This is being explored between the North Middlesex UniversityHospitals NHS Trust, the Royal Free NHS Foundation Trust and University CollegeLondon Hospitals NHS Foundation Trust and also links with the hospital chainsVanguardledbytheRoyalFree.Wewill increaseprovisionofchemotherapycloserto home, establishing a quality kitemark for chemotherapy and supporting self-management. The first patient treatment in the home for breast cancer will beavailablebytheendofSeptember2016.
• Centre for Cancer Outcomes (CCO): to deliver robust outcomes data, improvepathway intelligence and address important population health research questionswewillproducebalancedscorecardswhichcanmadeavailabletoMDTs,providersandcommissionersthroughafreetoaccesswebbasedplatform.
• Researchandcommercialisation:wewill leverageouruniquepositionnationallyincancertoimprovecareforpeoplewithcancer,generateadditionalrevenuesacrossthesystem,andgenerateefficienciesbyavoidingunnecessaryinterventions.
6.2.9 Specialisedcommissioning
Specialisedservicesarethoseprovided inrelatively fewhospitals/providers,accessedbycomparatively smallnumbersofpatientsbutwithcatchmentpopulationsofusuallymorethanonemillion. These services tend tobe located in specialisedhospital trusts that canrecruit a team of staff with the appropriate expertise and enable them to develop theirskills.InNCL,themainprovidersofspecialisedacuteservicesareUniversityCollegeLondonHospitalsNHSFoundationTrust (with income totaling£317m)and theRoyalFreeLondonNHS Foundation Trust (with income totaling £273m). A further 10 providers receive anadditional £128m in income for the delivery of specialised services. This includes threespecialisthospitals:RoyalNationalOrthopaedicHospitalNHSTrust,MoorfieldsEyeHospitalNHS Foundation Trust, andGreatOrmond Street Hospital NHS Trust. Barnet, Enfield andHaringeyMentalHealthNHS Trust and the Tavistock and PortmanNHS Foundation Trustprovidesspecialisedmentalhealthservices.Aswellascaring for the localpopulation, thespecialised services provided by hospitals in north central London are also accessed by apopulationfromoutsideofNCL.
We recognise that planning for specialised services canhave an impact across the region(and potentially nationally), and are thereforeworking closelywithNHS England, Londonregion to develop plans in this area. At a pan-London level, 11 priority transformationinitiativesforspecialisedserviceshavebeenidentified.Theseare:
• Paediatrics• Cardiovascular• Neuroscienceandstroke• Renal• Cancer

38
• Adultmentalhealth• ChildandAdolescentMentalHealthServices(CAMHS)• Trauma• Womenandchildren• Bloodandinfection• Medicinesoptimisation
On reviewof thesepan-London initiatives,our clinical leadership identified5areaswhichresonated strongly as opportunities where we could lead the way in transformingspecialisedservices.Weareintheprocessofprogressingplansinthefollowing5areas:
• Highcostdrugs:thisinvolvesreviewingandstrengtheningadherencetostartingandstopping rules forall high costdrugs. There is alreadyworkongoing inNCL in thisarea,whichhasrevealedthatcliniciansaregoodatstartingpeopleonthesedrugsbut poor at stopping them.Wewill set clear criteria around the use of high costdrugsatanNCLlevel.Inaddition,wewillreducethespendoncancerdrugsthroughthe Cancer Vanguard Pharma Challenge process, which includes programmes onbiosimilars,homeadministrationandsystemintelligence.
• Elective spinal surgery:wewill rapidly progress work on assessment, pre-surgicalpathways and stratification to ensure patients are directed to the best possibleplace.Thiswillhelpusbalancedemandandcapacitymoreeffectively.
• End of life chemotherapy: we will undertake a comprehensive review ofchemotherapyusage close to theendof life.Using theevidenceonwhen to stopendoflifechemotherapy,wewilldevelopprotocolsaroundthis.Wewillworkacrossthewholepathwayonthisissue,andlinkstoppingacutechemotherapytoendoflifediscussionsinprimarycare,workingcloselywiththeCancerVanguardtodeliverthis.
• Imaging: we will contain growth in imaging costs by eliminating the need for re-acquisition due to inadequate or unavailable scans. For patients, thiswill increasethespeedofdiagnosisandresult inareduction induplicatedcontrastorradiationexposure.Implementinganetworkingapproachtoimagingwillhelpustodeliveronthis,aswellasuseofinformationmanagementandtechnologytoenableproviderstoshareinformationonthescanswhichhavealreadytakenplace.
• Spinal cord injury: we will redesign the pathway locally to address patients arecurrentlywaiting in Intensive Care Unit (ICU) beds to access specialist spinal cordinjury rehabilitation services. Waiting in ICU beds can cause the onset of othersymptomsleadingtoworseoutcomesforpatientsandhighcostsforthesystem.
Werecognise thatourplanningonspecialisedservices is lessdevelopedthanmanyotherpartsoftheSTP.WewillcontinuetoworkwiththespecialisedcommissioningteaminNHSEngland,LondonRegiontodevelopmoredetailedplansinthisarea.
6.3 Productivity
6.3.1 Commissionerproductivity(BAUQIPP)
Wewillcontinuetodeliversignificant“businessasusual”efficienciesthroughoutthe5yearperiod. Business as usual (BAU) QIPP (Quality, Innovation, Productivity and Prevention)

39
comprisessavingscommissionersexpecttodeliveraspartoftheirnormalactivities.Theseareefficiencies inareasofCCGspendnotcoveredbyourotherworkstreamsand includeopportunitiesinthefollowingareas:
• Mental health: this includes ongoing non-transformational efficiencies, consistentwith parity of esteem requirements. Examples of mental health QIPP are themanagement of out of sector placements and streamlining the pathways withspecialistcommissioningacrossforensicandmentalhealthservices.
• Community: spend on community services was c.£133m in 2015/16. There is anassumption of increased efficiency equivalent to 1.5% per annum supported bybenchmarkingworkandtransitiontonewmodelsofcare.
• Continuing care: spend on continuing care was c.£90m in 2015/16. There is anassumption of increased efficiency equivalent to 2.1% per annum supported byexistingframeworkagreements.
• Primarycareprescribing:spendonprimarycareprescribingwasc.£205min15/16.There is an assumption of increased efficiency equivalent to 2.5% per annumincludingtheadoptionofgenericdrugswherepossible,theadoptionoflocalqualityschemestoimproveconsistencyandeffectiveness.Thisisinthecontextofassumedgrowthof5-7%perannum.
• Programme costs (including estates): this includesmeasures to reduce void costsand better alignment of health and care services to reduce the overall estatefootprintwhilstmaintainingandimprovingservicequality.
6.3.2 Providerproductivity(BAUCIP)andsystemproductivity
Significantlyimprovingproviderproductivityisanessentialpartoftheworktoaddressourfinancial challenge. Our plans assume significant delivery of CIP (Cost ImprovementProgrammes),improvingproviderproductivity.
Wehaveidentifiedopportunitiesforsystemproductivity(definedasthoseareaswhereCIPdelivery is dependent on trusts working together) to deliver financial savings whilstmaintaining or improving quality. Our plans also assume savings from improvements tocontractingbetweenCCGsandtrustswhichwillberealisedsystemwide.
Specificinitiativestoimproveproductivityinclude:
• Workforce: we will establish a shared recruitment and bank function acrossprovidersmeaning thatstaffcanbedeployedbetweenproviders in thesystem;aswellasimprovingretentionofcurrentstaffandupskillingthehealthandsocialcareworkforcetoenabledeliveryofnewmodelsofcare.WecommittocomplyingwiththemaximumtotalagencyspendandhourlyratessetoutbyNHSImprovement.
• Procurement:wewillreducepurchasingunitcostswithincreasedvolumeandscaleacrossallprovidersbyreducingclinicalvariationinproductchoiceandundertakingjointactionondrugsandmedicinesmanagement.
• Back office:wewill create centralised functions for payroll and pensions, financeand estates in order to reduce our overheads and improve service resilience. Inadditionwewill:

40
o Consolidate IT services to reduce costswhilst improving the resilience andqualityofservices
o Enhance the existing share procurement arrangements to reduce non-paycosts
o Pool our legal budgets and resources, considering options to consolidateoutsourcedresourcesorappointanin-houselegalteam.
• Operationalandclinicalvariation:wewillcollectivelyreduceaveragelengthofstay,maximisetheatreutilisationandstreamlineclinicalprocesses,inadditiontothechangesproposedthroughtheelectiveworkstream.
• Contractandtransactioncosts:Releasingsavingsfromstreamliningtransactionsandcontracting.Thiswillbedeliveredthroughimplementingnewcommissioningarrangements(whichmayfacilitatejointprocurementofservicesfromtheCommissioningSupportUnit(CSU),forexample)andleveragingtheopportunitiesassociatedwithjointcommissioningbetweenlocalauthoritiesandCCGs.
• Other:Additionalexistingproviderproductivityschemes:estates,clinicaladminredesign,servicetransformation,incomeetc.
6.4 Enablers
6.4.1 Digital
Wewillusedigitaltechnologiesandinformationtomovefromourcurrentmodelsofcaretodeliverproactive,predictive,participatory,person-centredcareforthepopulationweserve. Thereissignificantandimmediateopportunityfordigitaltotransformourcurrentdeliverymodels and seed completely new, integrated models of health and social care. Werecognise the strength of both the clinical and financial case for digital and its potentialimpact in strengtheningproductivity, providing easeof access to our services,minimisingwasteandimprovingcare.Ourambitionistobecomeanationalleaderinpopulationhealthmanagementenabledbyinformatics,toreducevariationandcostandimprovecare.Wewillprioritiseand increasepaceofappropriatedigital technologyadoptionwithinourorganisations, realigning the demand on our services by reducing the emphasis ontraditionalfacetofacecaremodels.Inaddition,wewillexplorenewdigitalalternativesthatwill transformour services,with the aimofmoving care closer to home, enabling virtualconsultationsandprovidingourpatientswiththeinformationandresourcestoself-manageeffectively, facilitating co-ordinated and effective out of hospital care. We will utiliseopportunities for real-time, fully interoperable information exchanges to provide new,flexibleandresponsivedigitalservicesthatdeliverintegrated,proactivecarethatimprovesoutcomesforourpatients.Our digital programme proposes the creation of an NCL Population HealthManagementSystem(exhibit8),whichsupportsprevention,servicetransformationandproductivity,andwouldenableustomeetthenationalmandateofoperatingpaperfreeatthepointofcareby2020.Through this systemwewillmove froma landscapeofdiversityandvariation tooneofsharedprinciples,consolidationandjointworkingforthebenefitofthepopulation.

41

42
Exhibit8:NCLPopulationHealthSystemManagement
The6workstreamsthatmakeupourdigitalstrategyare:
• Activate: We will provide our citizens with the ability to transact with healthcareservices digitally, giving themaccess to their personal health and care informationand equipping them with tools which enable them to actively manage their ownhealthandwellbeing.
• Analyse:Wewill use data collected at the point of care to identify populations atrisk,monitortheeffectivenessofinterventionsonpatientswithestablisheddiseaseanddeliverwholesystemsintelligencesothattheneedsofourentirepopulationcanbepredictedandmet.
• Link:Wewill enable information to be shared across the health and care systemsseamlessly.
• Share:Wewillcreateandsharecarerecordsandplansthatenable integratedcaredeliveryacrossorganisations.
• Digitise:Wewillsupportourproviderstomoveawayfrompapertofullydigitalcareprocesses;includingdocumentation,ordering,prescribinganddecisionsupporttoolsthathelptomakecaresafer.
• Enable:Wewillprovideinfrastructurewhichenablesourcareprofessionalstoworkandcommunicateeffectively,anywhereatanytime,andfacilitatenewandenhancedmodelsofcareclosertohome.
Todeliveronourdigitalstrategywewillneedtoinvest£159m,withafurther£21min2020/21(seesection8.3).
Enable
Digitise
Link
Share
Analyse
Activate
InfrastructureNetwork; wifi; unified comms; email; collaboration tools; end user technology; virtual care services
Integration and messaging
Applications
Health Information Exchange; information and messaging standards; document, image and data exchange
Electronic health records; clinical documentation; ePrescribing and closed loop medication management; orders and results; device integration; alerts and decision support
Integrated care
Insights driven health system
Shared health and care records; care plans
Health system benchmarking; cohort stratification; patient tracking; case management; whole pathway decision support; predictive modelling
Digitally activated population Personal Health Record; Self management; remote monitoring; digital transactions
Info
rmat
ion
Gov
erna
nce
Dat
a Q
ualit
y an
d Va
lidat
ion
CCGs
Primary care
Social care
Acute, community, mental health and specialist providers
Care homes
NCL
Dig
ital
Del
iver
y M
odel

43
6.4.2 Estates
Ourvisionistoprovideafitforpurpose,cost-effective,integrated,accessibleestatewhichenablesthedeliveryofhighqualityhealthandsocialcareservicesforourlocalpopulation.Theprioritiesfordevelopmentofourestatesstrategyare:
• torespondtoclinicalrequirementsandchangesindemandbyputtinginplaceafitforpurposeestate
• toincreasetheoperationalefficiencyoftheestate• toenhancedeliverycapability• toenablethedeliveryofaportfolioofestatestransformationprojects.
Thereanumberofbarrierstoachievingthis,including:
• thecomplexityoftheestatessysteminNCL,includingthenumberoforganisationsand the differences in governance, objectives and incentives between eachorganisation,whichoftenresultsinorganisationsworkinginsilos
• misalignedincentives,whichdonotencourageoptimalbehaviour• lack of affordability, specifically the inability for trusts to retain capital receipts,
budget “annuality” and the difficulty of accessing capital investment for re-provision
• thecomplexityofdevelopingbusinesscasesintermsofgettingtherightbalanceofspeed and rigour, and the different approvals processes facing differentorganisation types (for example, there are different capital approval regimesoperatingacrosstheNHSandlocalgovernment).
WeareworkingaspartoftheLondondevolutionprogrammetopilotdevolvedpowers inrelationtothehealthandcareestate.Aspartofthis,weareaskingfor:
• local prioritisation and investment of capital receipts, including those thatwouldotherwiseberetainednationally
• NHScapitalbusinesscaseapprovaltobeacceleratedandconsolidatedthroughtheimplementation of a jointly owned and collaborative NCL / national process (ordevolvedtosub-regionalorLondon-level)
• development of enhanced and revised definitions of value for money, whichconsider social value, wider community benefit and system sustainability at thesub-regionallevel
• new approaches for the accounting treatment of multi-year projects for non-foundationtrustproviders,insupportofourplans
• developinglocalflexibilitiesintermsandconditionsfortheprimaryandcommunityhealthestatetoimprovequalityandutilisation
• supporttoagreetheLondon-levelandNCLdeliveryoptionstoenhanceourwork• abilitytopayoffPFIsusingmoneyraisedfromcapitalsalesand/oracommitment
bynationalpartners to renegotiationof suchagreements,where theyhavebeenidentifiedasasignificantbarriertofinancialsustainabilityand/orthefacilityislessthan50%utilisedandnootherutilisationsolutionwilladdresstheissue.
Weanticipatethefollowingbenefits:

44
• a whole system approach to estates development across NCL, with differentpartners working together on projects and developing a shared view of therequiredinvestmentanddevelopmenttosupportclinicalchange
• the ability to undertake better local health economy planning, includingestablishingestatesrequirements
• increasedaffordabilityofestateschangeacrossNCL• greaterincentivestodisposeofsurplusproperty,releasinglandforhousing• focused action on the development of the estates requirements to deliver care
closertohome• greater efficiency and flexibility in the estate, reducing voids and improving
utilisationandco-locationwhichwillsupportfinancialsavings
AcrossthesitesofMoorfields,StPancras,StAnn’swearebeginningtoevidencequalitativebenefits ofworking together to deliver estates value and improvement. The sector for anumberofyearshashadunresolvedestatesissuesrelatingtopoormentalhealthinpatientaccommodationandpotentiallysaleableandhighvalueestateatStPancrasHospital.The3providers are working together on this strategic estates project which aligns estatesprioritiesbetweenall3trusts.
Theproposedprogramme,which is still subject toconsultation,wouldseesalesproceedsfromsurplusassetsusedtodelivernewpurposebuiltmentalhealthaccommodation,andthe eventual relocation of Moorfields Eye Hospital to the St Pancras site. ClinicalimprovementswouldbeprioritisedthroughthebuildingofanewInstituteofMentalHealthand an integrated EyeHospital and Institute of Ophthalmology at the current St PancrasHospitalsite.
Thethreetrustsarecurrentlyrefiningtheiroutlinebusinesscases,withBoarddecisionsduein late 2016 and early 2017. Subject to consultation, further testing of economic viabilityandplanningpermission,thespecificbenefitsoftheworkwillinclude:
• development of a new world class research, education and clinical care facilityhousing an integrated Moorfields Eye Hospital and UCLH’s Institute ofOphthalmology, transforming ophthalmology facilities that are at present aconstraintoncontinuousimprovement
• improvementstotheestatetomeetCQC“mustdos”includingnewmentalhealthinpatients facilities forCamdenand IslingtonNHSFoundationTrust (includingtheintegration of physical and mental health and social care through an integratedpractice unit at St Pancras). Also, new facilities for Barnet, Enfield & HaringeyMentalHealthTrustatStAnn’sHospital,Tottenham
• a world class UCLH Institute of Mental Health and associated patient care andeducationalfacilitiesatStPancrasHospital
• potentialtodeliverc.1,500newhousingunitsinLondon,significantlycontributingtotheNHStargetforreleaseoflandforresidentialdevelopment
• improvements to environmental sustainability, as the new builds will deliver abalancebetweenBREEAMratingsfor‘green’initiatives,thecostofthecapitalbuildrequirementstodeliverthemandthewholelifecyclebenefitsintermsofcostsand
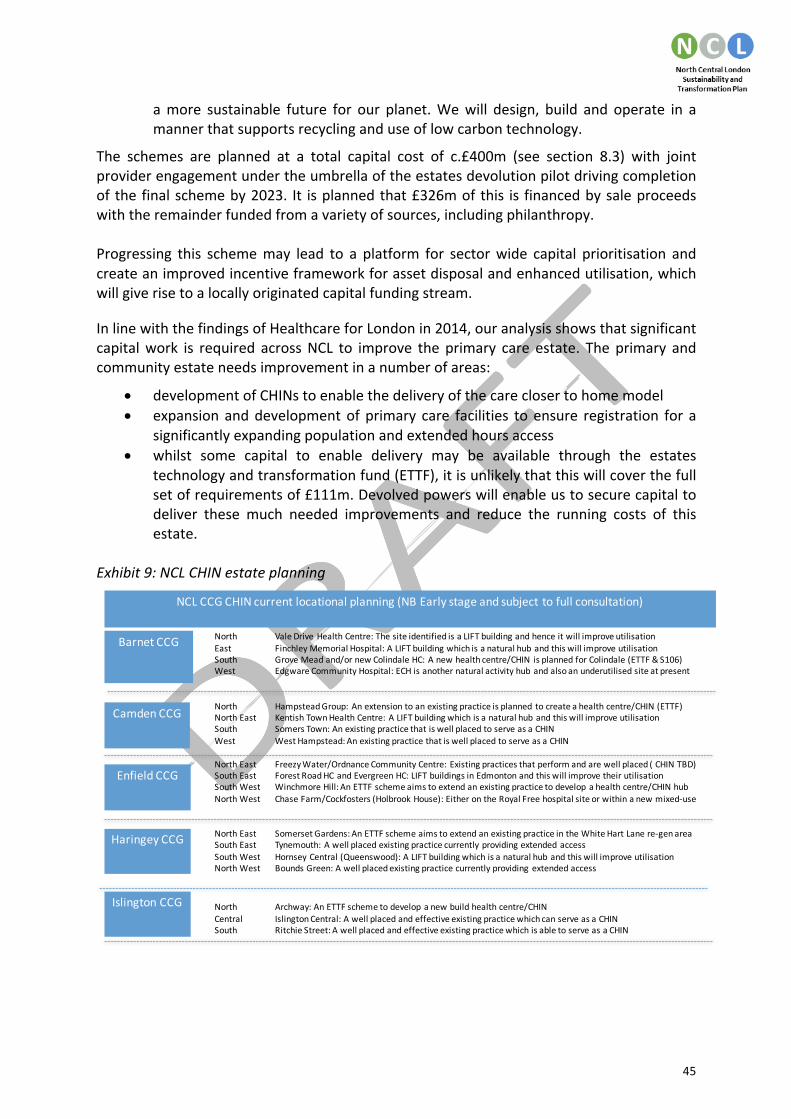
45
amore sustainable future for our planet.Wewill design, build and operate in amannerthatsupportsrecyclinganduseoflowcarbontechnology.
The schemes are planned at a total capital cost of c.£400m (see section 8.3) with jointproviderengagementundertheumbrellaoftheestatesdevolutionpilotdrivingcompletionof thefinalschemeby2023. It isplannedthat£326mofthis is financedbysaleproceedswiththeremainderfundedfromavarietyofsources,includingphilanthropy.Progressing this schememay lead to a platform for sectorwide capital prioritisation andcreateanimprovedincentiveframeworkforassetdisposalandenhancedutilisation,whichwillgiverisetoalocallyoriginatedcapitalfundingstream.
InlinewiththefindingsofHealthcareforLondonin2014,ouranalysisshowsthatsignificantcapitalwork is required acrossNCL to improve the primary care estate. The primary andcommunityestateneedsimprovementinanumberofareas:
• developmentofCHINstoenablethedeliveryofthecareclosertohomemodel• expansionanddevelopmentofprimary care facilities toensure registration for a
significantlyexpandingpopulationandextendedhoursaccess• whilst some capital to enable delivery may be available through the estates
technologyandtransformationfund(ETTF),itisunlikelythatthiswillcoverthefullsetofrequirementsof£111m.Devolvedpowerswillenableustosecurecapitaltodeliver these much needed improvements and reduce the running costs of thisestate.
Exhibit9:NCLCHINestateplanning
North ValeDriveHealthCentre:ThesiteidentifiedisaLIFTbuildingandhenceitwillimproveutilisationEast FinchleyMemorialHospital:ALIFTbuildingwhichisanaturalhubandthiswillimproveutilisationSouth GroveMeadand/ornewColindaleHC:Anewhealthcentre/CHIN isplannedforColindale(ETTF&S106)West EdgwareCommunityHospital:ECHisanothernaturalactivityhubandalsoanunderutilisedsiteatpresent
North HampsteadGroup:Anextensiontoanexistingpracticeisplanned tocreateahealthcentre/CHIN(ETTF)NorthEast KentishTownHealthCentre:ALIFTbuildingwhichisanaturalhubandthiswillimproveutilisationSouth SomersTown:AnexistingpracticethatiswellplacedtoserveasaCHINWest WestHampstead:AnexistingpracticethatiswellplacedtoserveasaCHIN
NorthEast FreezyWater/OrdnanceCommunityCentre:Existingpracticesthatperformandarewellplaced(CHINTBD)SouthEast ForestRoadHCandEvergreenHC:LIFTbuildingsinEdmontonandthiswillimprovetheirutilisationSouthWest WinchmoreHill:AnETTFschemeaimstoextendanexistingpracticetodevelopahealthcentre/CHINhubNorthWest ChaseFarm/Cockfosters(HolbrookHouse):EitherontheRoyalFreehospitalsiteorwithinanewmixed-use
NorthEast SomersetGardens:AnETTFschemeaimstoextendanexistingpracticeintheWhiteHartLanere-genareaSouthEast Tynemouth:AwellplacedexistingpracticecurrentlyprovidingextendedaccessSouthWest HornseyCentral(Queenswood):ALIFTbuildingwhichisanaturalhubandthiswillimproveutilisationNorthWest BoundsGreen:Awellplacedexistingpracticecurrentlyprovidingextendedaccess
North Archway:AnETTFschemetodevelopanewbuildhealthcentre/CHINCentral IslingtonCentral:AwellplacedandeffectiveexistingpracticewhichcanserveasaCHINSouth RitchieStreet:AwellplacedandeffectiveexistingpracticewhichisabletoserveasaCHIN
NCLCCGCHINcurrentlocationalplanning(NBEarlystageandsubjecttofullconsultation)
BarnetCCG
CamdenCCG
EnfieldCCG
HaringeyCCG
IslingtonCCG

46
6.4.3 Workforce
WeaimtoensurethatNCLbecomestheplaceofchoicetotrain,workandlivehealthylives.This includes co-creating, communicatingandcollaborativelydeliveringa compellingoffertoattract,developretainandsustainacommunityofpeoplewhoworkinhealthandcareinNCL. Our workforce needs tomove further towards a person-centred approach and thismeansdevelopingawholerangeofnewskills,trainingmodalitiesandnewroles.Our vision is for staff to be part of the wider NCL workforce, not just part of a singleorganisation.Throughthiswewillachieveefficienciesinemploymentbymanagingservicescollectively across the footprint. We will create sustainable career pathways to attract,developandsupportaworkforcefitforpurposeinthechanginghealthandcarelandscape.We will work with NCL organisations across all care settings (including social care) tosupport their collaborative efforts to be excellent employers – employers of choice,committed to looking after the wellbeing of staff whilst also preparing them to begindelivering the new caremodels. Thiswill supportNCL organisations to recruit and retainstaff, particularly where employee turnover rates are high or where there are staffshortages.Careerpathwayswillnotbelimitedtoasinglecaresettingandwillofferourstaffopportunities to experience a wide range of different opportunities which fit their ownaspirations. This processwill allowus towork towards thedevelopmentof an integratedemploymentmodelandapersonalcareerpassportforstafftodeveloptheircareeroverthelong-termwithinNCL.We aim to improve employee wellbeing and reduce avoidable sickness absence cost-effectively, therefore increasing lifetime productivity.Wewill focus on implementing thehealthyworkplacecharterinNHSorganisations,localauthoritiesandinsmallandmediumsizedbusinesses.
Throughequippingtheexistingworkforcewithnewskillsandwaysofworking,wewillbothensurethatourpeopleareworkingtothebestoftheirabilityaswellasadaptingrolestomeet the changing requirements of our services.We will support some of those peoplecurrentlyworkinginhospitalsettingswiththeskillsandconfidencetoworkacrossthecarepathway,reachingoutintocommunitycaresettingsanddeliveringthecareclosertohomemodel. We will similarly enhance the capabilities of those currently working in social,community and primary care. We will equip all our existing and future staff withmotivational and coaching skills, competence in promoting self-care and prevention, andtheenhancementofemotionalresilienceinthemselves,theirteamsandtheirpatients.AllfrontlineNHSandlocalauthoritystaffwillbetrainedonlineinMakingEveryContactCount(MECC),withkeyfrontlinestaffalsoreceivingface-to-facetraining.Allnon-medicalfrontlinestaffwillreceivetraininginMentalHealthFirstAid(MHFA).AllNHSandsocialcarestaffwillbetrainedinbasicdementiaawareness,withmoreadvancedtrainingforfrontlinestaffwhoaremorelikelytoencounterpeoplelivingwithdementia.
WhilemostofthepeoplewhowillbeengagedindeliveringtheNCLvisionarealreadywithus,workinginroleswhichwillneedtoadaptorchangeinsomeway,wewillalsosupportthe establishment of a small number of new roles, such as physician’s associates, care

47
navigatorsandadvancedclinicalpractitioners.Wewillundertakeexpertstrategicworkforceplanningand redesign,andcommission training for skill enhancement, rolediversificationandnewroleimplementation.
To enable transformation, we will deliver system-level organisational development,supportingsystemleadersasindividualsandasteamsthroughthetransformationjourneytoenablepersonalresilienceandcourageousaction.Inaddition,wewilltraineveryoneinasingle approach to continuous quality improvement to create a culture of continuousimprovementtodeliverclinicalexcellenceandqualitycare.
Health,socialcareandpublichealthdeliveryisnotlimitedtoemployeesofourtraditionalemployers,andournotionofworkingwiththe‘widerworkforce’extendstothenumerouscarers,volunteersandcitizenswhoimprovethelifeofourpopulation.Inordertoimprovethegeneralwellbeingofourpopulationandmakeuseofthesubstantialsocialcapitalacrossourfootprint,wewilleducateandsupportpatients,carersandthoseintheircommunitiesin areas such as self-care, self-management, dementia and mental health awareness.Buildingonour‘widerworkforce’visionandaligningwithinitiativessuchastheAlzheimer’sSociety ambition for London to be a dementia friendly city by 2020,wewill support thetrainingofgroupssuchasbarbers,hairdressers, librariansandteacherstogatherabetterunderstanding of dementia andother long term conditions. AcrossNCL,wehave alreadybuiltfivestrongCommunityEducationProviderNetworks(CEPNs),andthesewillprovideaneffective vehicle for delivery of this aim. We will review the provision of learning anddevelopmentacrossNCLtoensurewemakethebestuseofexistingassets toencompassthewiderhealthcarecommunityincludingpatientsandcarers.Ourimmediateaimswillbetostandardiseandstreamlinestatutoryandmandatorytraining,align inductionandsharein-houselearninganddevelopmentcapacity.
Exhibit10:Integratedworkforcemodel

48
6.4.4 Newcommissioninganddeliverymodels
As part of the STP development process, and in response to the changing healthcarelandscape in NCL, the 5 CCGs have been exploringways ofworkingmore collaborativelytogetherwhilst also seeking to strengthen joint commissioningwith local authorities.Wehave concluded that a more formalised degree of cooperation between the 5 CCGs willimprovehealthcommissioning,particularlyinresponseto:
• thedevelopmentofnewmodelsofcare,includinglargerproviderorganisationssuchtheRoyalFreeVanguard.
• increasingfinancialrisk• stretchedcapabilityandcapacity.
Our work has covered the development of a proposal for joint governance of strategiccommissioningdecisions(seesection9.2.1);thedevelopmentofacommoncommissioningstrategy and financial strategy; and, a review of CCGmanagement arrangements, with aviewtoshapingnewwaysofcommissioning.Withafocusonpopulationhealthsystemsandoutcomes and the transition to newmodels to deliver these, our objective is to furtherstrengthen strategic commissioningover thenext 2 years.Wehave agreed that anynewcommissioning arrangements need to balance the importance of local relationships andexistingprogrammesofworkwiththeneedtocommissionatscale.The governing bodies of each of the CCGs have agreed to the need for new executivemanagementarrangementsincludingsharedrolesacrosstheCCGs:anAccountableOfficer;aChiefFinanceOfficer;aDirectorofStrategy;and,aDirectorofPerformance.Additionally,inordertoensurethecontinuedroleofeachCCGinrespecttoitslocalcommissioningandjointworkwithlocalgovernment,localDirectorswithresponsibilityforlocalfunctionsandserviceshavebeenproposed.ThesenewleadershippositionswillworkwitheachoftheCCGs,aswellasthenewsharedgovernancestructuredescribedinsection9.2.1,toensurethathealthcommissioninginNCLdeliversthebestpossiblehealthandwellbeingforthelocalpopulationwhilstensuringvalueformoney.ThearrangementswillbefurtherconsideredbygoverningbodiesinNovemberwiththeexpectationthatthenewleadershipwillbeinplacenolaterthan1April2017.
Inparallel,commissionersandprovidersacrossthesystemhavebeenworkingtogethertodefineourdirectionoftravelintermsofnewdeliverymodels.Wealreadyhavesignificantwork we can build on relating to this, including the Royal Free London’s provider chainmodel; the UCLH Cancer Vanguard; theMoorfields Eye Hospital ophthalmology specialtychain; and, the Royal National Orthopaedic Hospital NHS Trustchain of orthopaedicproviders.
Wehaveconsultedwiththeleadersofallorganisationsacrossthesystemtogetviewsonthe different options for new deliverymodels, and the broad consensus includesmovingtowards:

49
• wholesystemworkingwithapopulationratherthanindividualorganisationalfocus• a deeper level of provider collaboration, including collaboration between primary
care, community services, acute services, mental health services and social careservices.
• theestablishmentofsomeformof‘newdeliveryvehicle’or‘newdeliverysystem’tosupportthisprovidercollaboration.
• atransferovertimeofsomeelementsofwhatwecurrentlyconsidercommissioningfunctions(forexample,pathwayredesign)intothesenewdeliveryvehicles.
• a move towards some sort of population based capitated budget for the newdeliveryvehicles.
• the retention of a strategic commissioning function responsible for holding thedelivery vehicles to account, with accountability for outcomes rather than inputsbasedonprinciplesofcommissioningforvalue.
Further work needs to be done to resolve issues and differences of view around thefollowing:
• theorganisationalformforthenewdeliveryvehicles• theoptimalpopulationsizeforpopulationhealthmanagement• thegeographyoverwhichnewdeliveryvehiclesshouldoperate• theformandgovernanceofthestrategiccommissioningfunction• which commissioning functions should remain with the strategic commissioning
functionandwhichshouldbeundertakenthroughthenewdeliveryvehicle.• thescopeofthenewdeliveryvehicles• unresolved issues such as how tomanage patient choice, specialised services and
other flows outside of the delivery vehicle and a full understanding of the legalframeworkwhichmightimpactonimplementation
• speedofimplementation.
Discussions continue across health and care commissioners and providers in NCL toestablish agreement about the nature and scale of new delivery vehicles. Different caremodels are still being considered, and this work is being steered through the STPgovernanceframework.
6.5 Measuringoursuccess
We have established the anticipated impact of each of our workstreams to ensure weremainontracktoclosethekeygapsassetoutinourcaseforchange.However,toensurethat the breadth of our workstreams collectively meet the scale of our ambition, 11overarching outcomes have been developed by the London Health Commission for theBetterHealthforLondonstrategy.ThesehavebeenadaptedforNCLandendorsedbytheclinicalcabinetforourSTP.Wewillknowifwehavebeensuccessfulbymeasuringimpactagainsttheseoutcomesoverthenext4years.
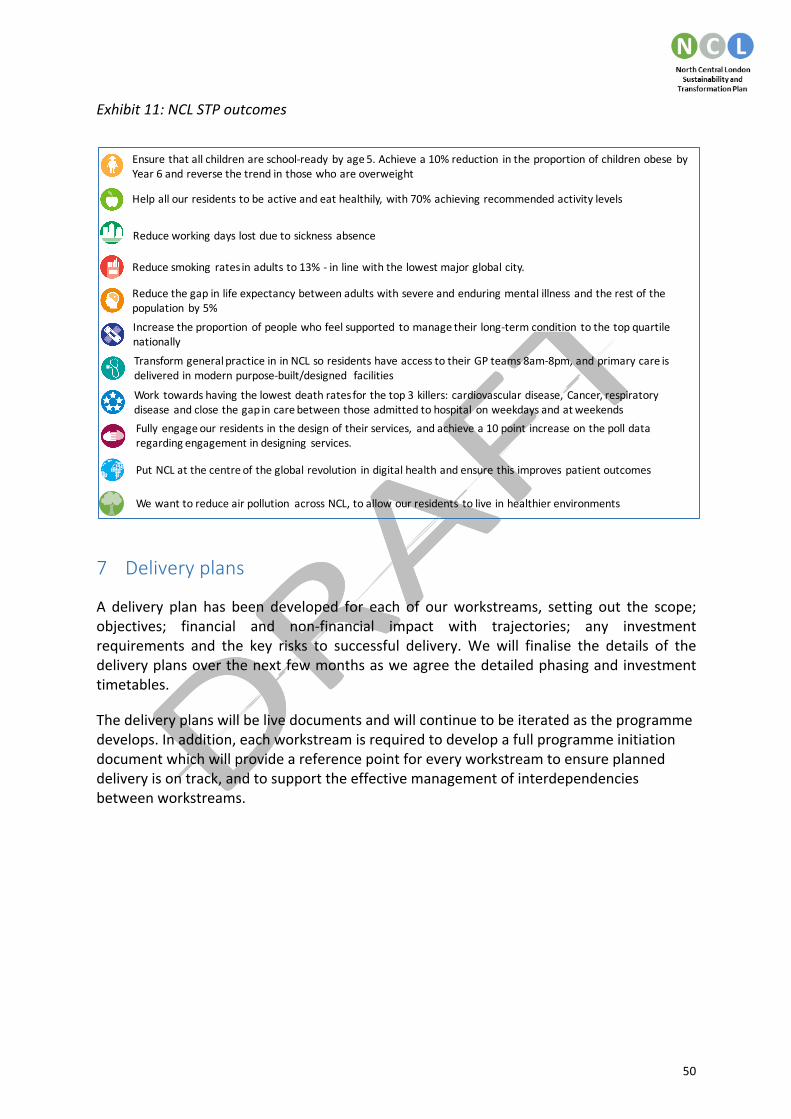
50
Exhibit11:NCLSTPoutcomes
7 Deliveryplans
A delivery plan has been developed for each of ourworkstreams, setting out the scope;objectives; financial and non-financial impact with trajectories; any investmentrequirements and the key risks to successful delivery.We will finalise the details of thedeliveryplansoverthenextfewmonthsasweagreethedetailedphasingandinvestmenttimetables.
Thedeliveryplanswillbelivedocumentsandwillcontinuetobeiteratedastheprogrammedevelops.Inaddition,eachworkstreamisrequiredtodevelopafullprogrammeinitiationdocumentwhichwillprovideareferencepointforeveryworkstreamtoensureplanneddeliveryisontrack,andtosupporttheeffectivemanagementofinterdependenciesbetweenworkstreams.
Ensurethatallchildrenareschool-ready byage5.Achievea10%reduction intheproportionofchildrenobese byYear6andreversethetrendinthosewhoareoverweight
Helpallourresidentstobeactiveandeathealthily,with70%achievingrecommendedactivitylevels
Reduceworkingdayslostduetosickness absence
Reducesmoking ratesinadultsto13%- inlinewiththelowestmajorglobalcity.
Reducethegapinlifeexpectancybetweenadultswithsevereandenduringmentalillness andtherestofthepopulation by5%
Increasetheproportionofpeoplewhofeelsupported tomanagetheirlong-termcondition tothetopquartilenationally
TransformgeneralpracticeininNCLsoresidentshaveaccesstotheirGPteams8am-8pm,andprimarycareisdeliveredinmodernpurpose-built/designed facilities
Work towardshavingthelowestdeathratesforthetop3 killers:cardiovasculardisease, Cancer,respiratorydisease andclosethegapincarebetweenthoseadmittedtohospital onweekdaysandatweekends
Fully engageourresidentsinthedesignoftheirservices, andachievea10pointincreaseonthepolldataregardingengagementindesigning services.
PutNCLatthecentreoftheglobalrevolution indigitalhealthandensurethisimproves patientoutcomes
Wewanttoreduceairpollution acrossNCL,toallowourresidents toliveinhealthierenvironments

51
8 Bridgingthefinancialgap
The financial analysis that we have undertaken (see exhibit 2) shows the significant gapbetweenanticipatedgrowthindemand(andthereforecostgrowth)fortheNHSinNCLandthegrowthinfundingthattheNHSexpectstoreceiveoverthe5yearsoftheSTP.Withoutchangingthewaythatweworktogetherasasystemtoprovideamoreefficient,joinedupservice across organisations, this would leave us with an estimated £876m deficit in2020/2021.
TheSTP inNCLhasbroughttogetherorganisationsacrosshealthandsocialcareto jointlydiscusshowwecanaddressthisfinancialchallengeaswellasmakingprogressinimprovingthequalityof,andaccess,toservices.Basedontheplansandanalysissetout inthisSTP,which have been developedwith and by local clinical experts,wewill reduce the annualdeficitoverthenextfiveyearsto£75m(exhibit12)–whilstthisaddressesmorethan90%ofthefinancialgap,werecognisethatfurtherworkisneeded.
Thekeyelementsof theplanaresetout indetailelsewhere in thisdocument.Exhibit12showshowthesecontributetotheimprovementintheannualfinancialpositionoftheNCLsystemover5years.Thekeyareasofworkare:
• Careclosertohome:savingsof£114mhavebeenestimatedfromimprovingaccesstoprimarycare;proactively identifyingneedandearly intervention toavoid crisis;rapid response to urgent needs to prevent hospital admissions; providingcommunity-basedandambulatory-basedcare;andreducingdelaystodischarge.
• Prevention and the support of healthier choices: this is estimated to result insavingsof£10m.
• Mentalhealthoutreachandliaison:thisisestimatedtoresultinsavingsof£6m.• Optimising the elective pathway: savings of £55m have been estimated from
benchmarkingagainstbestpractice;workingcloselywithclinicians;optimisingflowthroughtheatres(increasingthroughput);andreducinglengthofstay-inadditiontotheexcellentworkthatourhospitalsandotherprovidersdotoimproveproductivityeachyear.
• AdditionalplansarebeingdevelopedrelatingtotheUCLHCancerVanguardschemeandRoyalFreeHospitalChainVanguardwhichareestimatedtodeliver£35m.
• Systemlevelproductivitysavingsof£98mareplannedtobeachievedalongsidethe‘business asusual’ cost improvementsacrossproviders inNCLof£218mand localcommissionerbusinessasusualefficiencies(QIPP)of£57m.
• We have identified a potential saving of £24m per year through ‘buying out’ anumber of Private Finance Initiative hospitals, bringing management of thesefacilities back within the public sector. We will continue to work with theDepartmentofHealthandotherstodeveloptheseplans,recognisingthatthereareanumberofconstraints.
• Althoughdetailedplanshavenotyetbeendeveloped,wehavebeenadvisedbyNHSEnglandtoassumethattheNCLproportionoftheLondonAmbulanceService(LAS)financial gap of £10m and the estimated specialised commissioning pressure of£137mwill be fully addressedby LASandNHSEngland respectively.NCLhospitalsprovideaverysignificantamountofspecialistcareanditisthereforeessentialthatNHSEnglandworkstogetherwiththeSTPonhowtheseservicescanflourishwhilst

52
also addressing the financial pressures associated with the growth in specialistactivity(whichinmostdevelopedeconomiesishigherthangrowthinotherservicesduetonewtechnologies,drugsandclinicalinterventions).
• Furtherworkisongoinginrelationtodevelopingafullerunderstandingofthesocialcare financial position and pressures. At present no financial values have beenincluded as advised by NHS England, but this has not prevented the STP fromworkingverycloselyacrossbothhealthandsocialcare.InparticulartheNHSwithinNCL is seeking to learn from local authority colleagues best practice in relation toreducingcostwhilst improving theexperienceofpeoplewhouse servicesand thepublic.
These improvements cannot be achieved without investment. The plan is based oninvestmentof£64minpreventionandcareclosertohome,and£4minelectivecare.Wehave also assumed that £31m of our indicative £105m share of the Sustainability andTransformationFundwillberequiredtofundnationalpolicyprioritiesoverandabovetheseinvestments,inadditiontothatalreadyassumedwithinthe‘donothing’scenario.
Thesavingssetoutabovearepredicatedstronglyuponreducingsignificantactivityinacutehospitals, in particular reducing demand for inpatient care.We know that realising suchsavings can be difficult in practice and are contingent upon removing or re-purposingcapacitywithinacutehospitals.Assuch,throughworkingwiththeclinicalcabinetofclinicalleaderswithinNCLwehaveassumedthatthecostsavingsthatwillberealisedfromeachavoideddayofacutehospitalcarewillbesignificantlylowerthantheaveragetariffthatiscurrentlypaidtoprovidersbycommissionersforthiscare.This isreflectedina£53m‘riskadjustment’inthefinancialanalysis.
8.1 Normalisedforecastoutturnbyyear
Eachyeartherewillbeanumberofone-offcostsandincomestreamstothecommissionersand providers within NCL. Our 5 year financial analysis is initially based upon the“normalised”(orunderlying)financialpositionin2016/17whichisthenprojectedforward.Weestimatethat2016/17outturnwillbeanormaliseddeficitof£216m(£101monanin-yearbasis).Significantone-offfigureswithinthisincludeUCLH’stransitionalfundingthatitis receivingtocompensateforthefinancial impactofmovingcardiacservicestothenew,worldclasscentreatBartshospital,andtheRoyalFree’stransitionalfundinginrelationtothe merger with Barnet and Chase Farm. The underlying figure also includes a £40madjustment which is an estimate of the combined risk to the NHS provider andcommissioner forecast outturn. This has arisen as a result of potentially differentassumptions between NHS commissioners and providers about the value of workundertakenby theendof2016/17.Wehave reachedanagreedviewon forecastoutturnactivityandwillcontinuetoworkurgently toensureconsistencyofpaymentassumptionsbetweendifferentpartsoftheNHSwithinNCL.Allpartieshaveagreedamore‘openbook’approachtocontractagreementsthatwillensureaconsistent,system-basedapproach.
TheSTPplanshowsagradualimprovementinthefinancialpositionoverthe5yearsoftheSTP (exhibit 13). The normalised position improves year on year. This pattern is in partcausedbytherequirementformajorityoftheinvestmentintheearlyyearsoftheSTP,withbenefitsaccruinginthelateryears.

53
8.2 2017/18forecastoperatingplan
In2017/18weestimate thatour in-yearpositionwillbea£95mdeficit forNCLagainstadraftsystemcontroltotalof£13msurplus(whichweanticipatewillchangeoverthecomingweeksduetoanumberoftechnicalissues).ThisincorporatessignificantinvestmentduringtheyearonservicetransformationanddeliveryoftheFiveYearForwardView:
• investmentinservicetransformation:£25m.Thisrelatestothecareclosertohome(£23.5m),elective(£0.8m)andoutpatient(£0.4m)workstreams
• otherrecurrentinvestmentbyCCGsandtrusts–includedwithintheCCGandtrustcostmovements it is estimatedat £25m in17/18 todeliver elementsof the5YFVpriorities
• othernon-recurrentcosts(estimatedat£20min17/18)forinvestmentinVanguardcosts,ITdigitalcosts,andSTPprogrammecosts.
InlinewithNHSEguidancewehavealsoassumedthatwewillreceiveour‘fairshare’ofthenationalSustainabilityandTransformationFund(£105m)in2017/18.Thiscomparestothe£52m currently notified to NHS providers, and additional a further £53m improves ourrevisedforecastoperatingplanpositiontoadeficitof£62m–seeexhibit14.8.3 Capitalexpenditure
We recognise that the national capital budget for theNHS is highly constrained over thecourse of this parliament, and will continue to work hard to minimise the need forsignificantcapitalinvestmentunlessthereisastrongreturnoninvestment.NCLalsohasanumber of creative proposals thatwill seek tomaximise disposal proceeds from sites nolonger required, and use these to reinvest in the priority areas of the STP aswell as thepotentialtoprovideadditional,much-neededhousingfortheresidentsofNCL.
There are a number of large capital schemes that are already approved and underwaywithintheSTPand,whilst far frombeing ‘businessasusual’ theseare included inthe ‘donothing’ scenario as their approval pre-dates the STP work. Total capital, before specificSTP-relatedinvestment,is£1.2bnoverthe5years.Thisincludes:
• UCLHnewclinicalfacilities:haematology-oncologyandshortstaysurgery–(£137m);Proton-beamtherapy(£130m),ENTanddentalfacilitytoconsolidatetwoexistinghospitalsontothemainUniversityCollegeHospitalcampus(£98m)andothermoreminorschemes.UCLHhaveapprovedDHfundingof£278m(£51mpublicdividendcapital(PDC)and£227mDHLoan)aswellasanticipated,ring-fenceddisposalproceedstofinancethesedevelopments
• RoyalFree-ChaseFarmredevelopment:(£183m),whichincludes£93mofapprovedDHfunding(£80mPDCand£13mDHLoan).
In addition to thesemajor developments there is of course significant business as usualcapital investment such as equipment replacement and building maintenance, fundedthroughdepreciation,cashreservesandothersourcesoffunding(includingdisposals).
54
TheadditionalgrosscapitalrequirementstoimplementthetransformationprogrammesetoutintheSTPtotals£542m,withamuchsmallernetinvestmentrequirementaftertakingintoaccountdisposals,donationsandgrants:
• Estates redevelopment: relating to our St Pancras/St Anns/Moorfields proposals:£404m, assumed to be funded through disposals £326m), DH loans (£39m) andDonations (£37m), of which £272m (including short term bridging loans andrepayments)occurwithintheperiodcoveredbythisSTP(i.e.before2020/21)andisincludedabove.Thisscheme,includinganassumptionofDHloanfunding,hasyettobe agreed, and will be subject to normal Business Case processes through NHSImprovement.
• PrimaryCareforCareClosertoHomeand5YFVinvestment:£111massumedtobefunded predominantly through ETTF (£60m – all bids submitted), s106/CIL/GPcontributions(£26m),grantsandothersources.
• ITinvestment:£159mwithafurther£21min2021/22.AllassumedtobefundedbyETTF(circa£10m–bidssubmittedforthePersonHeldRecord/IDCR)orthroughthecentralDigitalTransformationFund.
Werecognisethatfurtherworkisneededtodevelopfullbusinesscasesfortheabove,andatpresent these figuresareestimated-particularly in relationtoprimarycareanddigitalinvestment. In developing these schemes we will seek to maximise the use of existingbuildingsandotherassets,andminimisetheneedfornewcapitalinvestment,togetherwithapplying a robust requirement for return on investment for each scheme. However, wefundamentallybelieve that investment inprimarycareanddigital technology iscentral tothetransformationofservicesthatisneededinNCLtoaddressthegapsinservicequality,accessandfinance,andwhollyconsistentwiththeFiveYearForwardViewandrequirementto be paper-free at the point of care by 2023. It would be wrong to assume that suchinvestment is not required and will not deliver value simply because of the stage indevelopmentoftheseplansthatNCLiscurrentlyin.TheestatesredevelopmentrelatingtoStPancras,StAnn’sandMoorfields,andtheestatesdevolution work, offers an exciting and compelling vision as to how existing assets,disposals, redevelopment and construction of new facilities can be financially efficient aswellasdeliveringsignificantbenefitstopatients,serviceusersandthewiderpopulation.In addition,wewill continue to engage as an STPwith thework being led by Sir RobertNaylor inrelationtopropertystrategyacrosstheNHS,tofurtherunderstandhowbeingapilotareainthiscanhelpNCLmakebestuseofitscurrentassetstosupportthedeliveryofourSTPvision.8.4 Nextstepstoaddressthefinancialgap
Weareveryclearthatwehavemoretodotoclosethefinancialgapsfortheremainderof2016/17andacrossthenext4yearsoftheSTP.Wewillthereforeundertakeaperiodoffurtherintensiveworkoverthenext8weeksbothto improve confidence in delivery of current estimates, whilst concurrently working onother areas to further improve the position. As far as possiblewewill aim to do this by

55
Christmas,sothatouroperatingplansubmissionimprovesonthissubmission.However,wedo believe that there is a risk that the gap will not be fully closed in every year whilstensuringthatwecontinuetoprioritisequalityofandaccesstoservices,particularlyaswebalance theneed to invest in the early years to deliver transformational benefits in lateryears. It is alsoessential that STPs and their constituentorganisations and leadership aregiventheregulatoryheadroomtodeveloplongertermplans,andthatthe‘newmodelsofcare’ being developed give clarity of financial accountability to support the financialchallengesthattheSTPfaces.Wehaveidentifiedanumberofimmediateactionstoimproveourcurrentfinancialposition,whichinclude:
• earlydeliveryofhighimpactcareclosertohomeinterventions• accelerateddeliveryofstretchtargetsforhighimpactelectivepathways• increased effort in terms of delivering efficiencies through provider productivity
schemes• reducinganynon-valueaddedcontractingcosts• implementationof payharmonisation and sharedprinciples aroundusageof bank
andagencystaff• leveragingexistingcapacityinNHSproviderstoreduceoutsourcingofactivitytothe
independentsector• othernon-recurrentsavingsmeasures• assessingandincorporatingtheimpactof2017/18tariffchanges.
Therearealsoanumberofareasthatwewillexplorefurtheraswebelievetheremaybesignificantsavingstobefound.Theseinclude:
• maximising clinical productivity across providers, for example introducing sharedclinicalrotas
• developing alternative pathways for the London Ambulance Service to avoidconveyancetoEmergencyDepartments
• rollingoutstandardisedpathwaystoallspecialities• identifyingopportunitiestoreducethelengthofstayforpatientsreceivingspecialist
services• reviewinganyplansthatrequirecapitalandhavenotyetbeenagreedtoestablish
themostcosteffectivewaytodeliveragreedoutcomes• rapidimplementationofcancerinitiatives,includingearlydiagnosis,newmodelsof
care,endoflifeinterventionsandresearchandinnovation• re-providingcosteffectiveservicesforthec.20%ofpeopleweestimatearecurrently
inhospitalbedsbutaremedicallyfittoleave• putting in place a peer review challenge approach across all areas of spend to
identifyfurtheropportunitiestoreduceoravoidspend,andtoaidcollectivedeliveryofplans.

56
Exhibit12:Bridgingthefinancialgapto2020/21

57
Exhibit13:Normalisedforecastoutturnbyyear

58
Exhibit14:Forecast2016/17outturncontroltotalto2017/18forecastoperatingplan
Note:The16/17 inyearFOTof£101mtogetherwith the£107m16/17normalizingadjustments represents thenormalized16/17positionexcluding thespecialist trusts
(RNOH,T&P).Includingthespecialisttrustsnormalised16/17position(£8m)bringsthecombined16/17normaliseddeficitto£216m(showninexhibit13).

59
9 Howwewilldeliverourplan
9.1 Deliverythrough2yearcontractsinNCL
Delivering the STP is a priority for health and care commissioners and providers inNCL -thereforeitisessentialthatcommissioningintentionsandcontractsreflectthis.Inlinewithnational guidance, we are entering into a planning round for 2 year contracts covering2017/18and2018/19.Wewillusethisopportunitytoensureallcontractsarestrategicallyaligned to the STP, thus enabling its delivery. Whilst we recognise that implementationmightlookdifferentindifferentlocalareas,weknowthatitwillonlybepossibletodeliveron the STP if we are all pulling in the same direction. Setting up 2 year contracts basedaroundourSTPdeliveryplanswillbothenablerapidimplementationandsupportalongerterm move to new relationships between commissioners and providers, reducingtransactionalcostsandbuildingthefoundationforthedevelopmentofnewcommissioninganddeliveryarrangements.
Exhibit15:Highlevelplanfor2yearplanningroundtosupportdeliveryoftheSTP
We have developed a proposed process and a set of draft principles for managing thecontractnegotiations thatwill takeplaceover thenext coupleofmonths.Our leadershipgroup will meet regularly (every 2 to 3 weeks) to ensure leadership alignment, assessprogressonoperatingplans,andtoensurethatthebehavioursofteamsreflecttheagreedNCLapproach.
WehaveagreedthatoperatingplansandcontractswillneedtobestrategicallyconsistentwiththeSTP.Toachievethis,allfinanceandactivityalignmentwillbeoverseenbytheSTPfinanceandactivitymodellinggroup,withoverallplanalignmenttobeoverseenbytheNCLwideplanninggroupledbytheCCGs.All interimfinanceandactivitysubmissionsbyCCGsand trustsbetween21Octoberand23Decembershould thereforebealignedacrossNCL
60
beforesubmission.WhilstorganisationswillindividuallyfollowupquerieswithNHSEnglandorNHSImprovementon2017/18controltotals,noorganisationwillagreetheir individualtargetunlessanduntilthereisapan-NCLplanagreed.
Therisksofdeliveryofoperatingplanswillbe identifiedand jointlyownedandmanaged,withthefollowingprinciples:
• simplicity• reducingtransactioncosts• incentivisingthechangesincaredeliveryassetoutintheSTP• incentivisingthedeliveryinimprovedproductivityassetoutintheSTP• locatingriskwhereitcanbestbemanaged• anopenbookapproach• useofagreedsourcesofdata.
Inthecurrentcontextofthefinancialpositionandmanagementcapacityacrossthesystem,wewillensureinthefirst2yearsoftheSTPthatweareprioritisingoureffortsintheareaswhich will add the most value in terms of increasing health and wellbeing for people;improvingthequalityofcarepeoplereceive;andensuringvaluefortaxpayers’money.Wewill focus our energies on achievingmaximumbenefit andwewill seek to identify areaswherewecanfurtherandfastertobuildconfidenceandmomentum.
Wewillidentifyresourcestotakeforwardareasoffurtherpotentialbenefit.Inaddition,wewill set up a process for independent peer review challenge of all areas of discretionaryspendinprovidersandCCGstoidentifyfurtheropportunitiestoreduceoravoidspendandtoaidthecollectivedeliveryofplans.
9.2 Decisionmakingintheprogramme
TheSTPisacollaborationbetweenarangeofsovereignorganisationsinNCL,eachwithitsown governance and decision-making structures. We have not to date introduced anycollectivedecision-makingstructures.HoweverwehaveworkedtogethertoproduceboththeCaseforChangeandtheSTP.
The STP is a work in progress and therefore has not been signed off by any of theorganisationswithintheSTP.WewilltakethisSTPthroughthepublicsessionsofeachoftheNHS provider boards, CCG governing bodies and Local Authorities for their support andinputintothenextsteps.
9.2.1 CollectivegovernancearrangementsforCCGs
Going forward, in order to support amore collaborative commissioning approach acrossNCL, the 5 CCGswill need amechanism for collective decisionmaking.Governing BodieshaverecognisedthisrequirementandhaveagreedtheprincipleofestablishingajointNCL-widegovernancestructureforsomeelementsofcommissioning.
Further work is being done on the details of the proposed joint governance structure.Engagementon thedesignhasbeenongoingduringOctober2016andwill continuewithfurtherdetailstobepresentedatGoverningBodymeetingsinNovember2016.
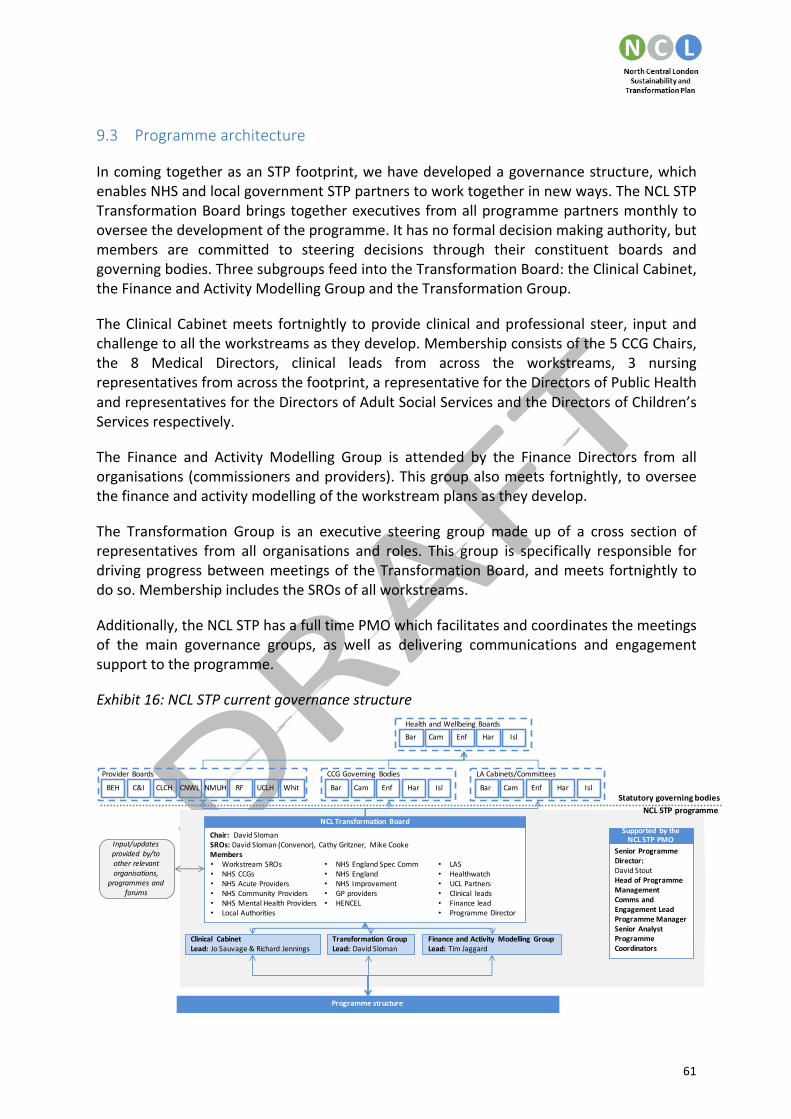
61
9.3 Programmearchitecture
IncomingtogetherasanSTPfootprint,wehavedevelopedagovernancestructure,whichenablesNHSandlocalgovernmentSTPpartnerstoworktogetherinnewways.TheNCLSTPTransformationBoardbringstogetherexecutivesfromallprogrammepartnersmonthlytooverseethedevelopmentoftheprogramme.Ithasnoformaldecisionmakingauthority,butmembers are committed to steering decisions through their constituent boards andgoverningbodies.ThreesubgroupsfeedintotheTransformationBoard:theClinicalCabinet,theFinanceandActivityModellingGroupandtheTransformationGroup.
TheClinicalCabinetmeets fortnightly toprovideclinicalandprofessional steer, inputandchallengetoalltheworkstreamsastheydevelop.Membershipconsistsofthe5CCGChairs,the 8 Medical Directors, clinical leads from across the workstreams, 3 nursingrepresentativesfromacrossthefootprint,arepresentativefortheDirectorsofPublicHealthandrepresentativesfortheDirectorsofAdultSocialServicesandtheDirectorsofChildren’sServicesrespectively.
The Finance and Activity Modelling Group is attended by the Finance Directors from allorganisations(commissionersandproviders).Thisgroupalsomeetsfortnightly,tooverseethefinanceandactivitymodellingoftheworkstreamplansastheydevelop.
The Transformation Group is an executive steering groupmade up of a cross section ofrepresentatives from all organisations and roles. This group is specifically responsible fordrivingprogressbetweenmeetingsof theTransformationBoard,andmeets fortnightly todoso.MembershipincludestheSROsofallworkstreams.
Additionally,theNCLSTPhasafulltimePMOwhichfacilitatesandcoordinatesthemeetingsof the main governance groups, as well as delivering communications and engagementsupporttotheprogramme.
Exhibit16:NCLSTPcurrentgovernancestructure
Programmestructure
StatutorygoverningbodiesNCLSTPprogramme
Cam Enf Har IslBar
LACabinets/Committees
Cam Enf Har IslBar
CCGGoverning Bodies
Cam Enf Har IslBar
HealthandWellbeingBoards
Provider Boards
NMUHCLCH CNWL RFBEH C&I UCLH Whit
NCLTransformation BoardChair:DavidSlomanSROs:DavidSloman(Convenor), CathyGritzner, MikeCookeMembers
• NHSEnglandSpecComm• NHSEngland• NHSImprovement• GPproviders• HENCEL
• LAS• Healthwatch• UCLPartners• Clinical leads• Financelead• ProgrammeDirector
• Workstream SROs• NHSCCGs• NHSAcuteProviders• NHSCommunityProviders• NHSMentalHealthProviders• LocalAuthorities
FinanceandActivityModelling GroupLead:TimJaggard
Transformation GroupLead: DavidSloman
Clinical CabinetLead:JoSauvage&RichardJennings
Input/updatesprovided by/tootherrelevantorganisations,
programmesandforums
SeniorProgrammeDirector:DavidStoutHeadofProgrammeManagementComms andEngagementLeadProgrammeManagerSeniorAnalystProgrammeCoordinators
Supported bytheNCLSTPPMO

62
The component workstreams of the NCL STP feed into the overarching governanceframework.Theworkstreamsareresponsiblefordevelopingproposalsanddeliveryplansinthe core priority areas. Every workstream has its own governance arrangements andmeeting cycleswhichhavebeendesigned tomeet their respective specific requirements,dependingonthecorestakeholdersinvolved.
9.3.1 Futureprogrammearchitecture
We recognise that as we move from planning to implementation that we will need toamendourprogrammearchitecturetoensurethat it is fit forpurpose.WewillworkwiththeTransformationBoardtoagreeanyrequiredchangestotheprogrammearchitecturesothatwearereadytomoveforwardwithimplementationfromthenewyear.
Ourinitialproposalfordiscussionissetoutinexhibit17.
Exhibit17:Proposedfutureprogrammearchitecture
Thisstructurewouldcomprisethefollowingnewgroups:
• STPOversightGroup:ThisoversightgroupwouldbemadeupofChairsandpoliticalleaders and would go some way to address the current ‘democratic deficit’ andrepresentationofviewsofthelocalpopulation.It isproposedthatthisgroupmeetquarterlyandmightbenefit fromanappointed IndependentChair.MembershipofthisgroupwouldensurescrutinyofthedeliveryofSTPdeliveryandensureabetterconnectionwiththeNHSboards,governingbodiesandlocalauthorityleadership.
• STPDeliveryProgrammeBoard:TodriveandoverseetheprogressionanddeliveryoftheSTP.Itisproposedthatthedeliveryboardmeetmonthly.ThiswouldreplacetheTransformationGroup.
NCLSTPDELIVERYPROGRAMMEBOARDChair:DavidSloman
AllSROsFrequency:Monthly
NCLSTPOVERSIGHTGROUPNHSChairs/Political Leaders/Healthwatch
Chair: Independent Chair,TBAFrequency: quarterly
ClinicalCabinet Finance&ActivityModellingGroup
NCLExecutive/Stakeholder
Leadershipevents
Workstreams
NCLSTPPMOSnrProgramme
Director

63
• Executive leadership events: CEOs and other relevant executive directors andstakeholder representativeswouldmeet periodically as requested by the DeliveryBoardinordertoresolvedeliveryissues.
9.3.2 Healthandwellbeingboards
CCGsarerequiredtoinvolvetheirlocalHealthandWellbeingBoard(HWB)whenpreparingtheircommissioningplansothatHWBscanconsiderwhethertheirdraftplanstakeproperaccountofthelocalhealthandwellbeingstrategy.AsCCGcommissioningplanswillbesetwithinthecontextoftheSTP,itwillbeimportantthatweengagewithHWBsaswedeveloptheSTP.EngagementofHWBswillalsobeanimportantmeansofensuringengagementoflocalpoliticalleadershipintheSTPprocess.
9.3.3 Overviewandscrutinycommittees
Localauthoritieshavearoleinreviewingandscrutinisingmattersrelatingtotheplanning,provisionandoperationofhealthservicesintheirlocalarea.CommissionersandprovidersofNHSservices(includingNHSEngland,CCGs,NHStrusts,NHSfoundationtrustsandprivateproviders)mustconsult the localauthoritywhere theyareconsideringanyproposal forasubstantialdevelopmentorvariationofthehealthserviceinthearea.Ordinarily,wheretheservices inquestionarecommissionedbyNHSEnglandorCCGs (as thecasemaybe), thecommissioners carry out this exercise on behalf of providers. Providers of public healthservicescommissionedbythelocalauthorityarealsorequiredtoconsultthelocalauthorityinthesamewayascommissionersandprovidersofNHSservices.
ThelocalauthoritymayscrutinisesuchproposalsandmakereportsandrecommendationstoNHSEnglandandtheSecretaryofState forHealth.Legislationprovides forexemptionsfromthedutytoconsultincertaincircumstances,forexamplewherethedecisionmustbetaken without allowing time for consultation because of a risk to safety or welfare ofpatientsorstaff.Aspartoftheoverviewandscrutinyprocess,thelocalauthoritywillinvitecomment from interested parties and take into account relevant information available,includingthatfromHealthwatch.
WehaveaJointHealthOverviewandScrutinyCommittee(JHOSC)inplaceacrossNCLwhichhas already put the STP on its agenda as a standing item.Wewill ensure that we liaisecloselywith the JHOSCas theSTPplansdevelop so thatwecanplanahead forany likelyneed for public consultation. In addition, we will discuss plans with any relevant localauthorityoverviewandscrutinycommitteesaswemovetowardslocalimplementation.
9.4 Programmeresourcing
Wehavededicated resources inplace to support thedeliveryof the STP,withanagreedoverallprogrammebudgetof£5m in2016/17.EachworkstreamhasaSeniorResponsibleOfficer(SRO).Someworkstreamshavesharedleadership,whereamixedskillsetisrequired.All of these individuals are senior Executive level - Chief Executives,Medical Directors orFinanceDirectors -ensuring leadershipof thehighestquality.EachSRO is supportedbyadedicated programme manager, and in some cases a broader team of support. Aprogrammebudget for2016/17hasbeenallocated toeachof theworkstreamsbasedon

64
theirproposedrequirements.STPpartnerorganisationsarealsogivinginkindtoeachoftheworkstreamstoensurehighqualityplanscanbedeliveredatpace.
Wewillreviewtherequirementsfor2017/18andbeyondaswefinalisethedeliveryplansandphasingofimplementation.A£10mresourcerequirementtodelivertheplanhasbeenfactoredintoourfinancialmodelling.

65
10 Engagement
Wehavecomealongwaysincebeingaskedtocometogetheras22healthandsocialcareorganisationswithdisparateviews lastDecember. It takestimetobuildtrustanddevelopsharedasharedvisionofthefuturebetweenpeopleandorganisations,andtogeteveryoneworkingtowardsthesamegoals.Wearenowallalignedbehindacollectiveagendaandarereadytoshareitmorewidely,seekinginputandfeedbackonourdraftplanstodate.
Themost importantpeopleweneedtoengagewitharethosewhouseourservices–theresidents ofNCL.We have specifically created a shared core narrative for this purpose –ensuringitisinpatient-focusedandaccessibleinlanguagetobegintoinvolvepeopleintheprocess.Nowthatweareinapositiontocommunicateourcollectivethoughtseffectively,our intention is to engage residents, local Councillors, our workforce and other keystakeholderstogetfeedbackonourplans.Wehaveheldinitialpublicmeetingsineachofthe5boroughs tobegin theprocessof co-designwithpatients,peoplewhouse services,carers,familiesandHealthwatch.
Ourapproachgoing forwardwillbe tocollaboratemoreextensivelywithpeoplewhouseservicesandcarers,localpoliticalstakeholdersaswellasmembersofthepublic,toensurethatourresidentshelpinformourdecisions.Thisapproachisguidedbythefollowingcoreprinciples (often called the “Ladder of Citizen Participation”).Wewill undertake differenttypesofengagementassetoutontheladderasappropriate:
1. ‘inform’stakeholders2. ‘engage’withstakeholdersinopendiscussions3. ‘co-design/co-produce’serviceswithstakeholders
Feedbackfromourlocalresidentswillbefundamentaltoourdecisionmakingandwillhelpusshapethewaythefinalplanisimplemented.
10.1 Ourfutureplans
Wewillnowbuildonthesuccessofourinitialpublicengagementeventsby:
• holdingaquarterlyforumineachborough• holdingpan-NCLeventsonspecific issuesthatmayarise insupportoftheborough
levelevents• hostingmeetingswiththepubliconfocussedtopicssuchasurgentandemergency
care,primarycare,andmentalhealthtogetin-depthinputfromthecommunity• organising‘Tweetchats’onspecificareasofinterest• developingadesignatedYouTubechannelandpopulatingitwithrelevantresources.• using partner digitalmedia channels – Twitter, Facebook, Instagram– to promote
our public engagement programmes and information. We will also use thesechannelstotestideasandprogressonlocalprioritieswhichwillhelpusdevelopourplansfurther.

66
Todothis,wewill:
• use Healthwatch, other patient representative groups and resident’s associations,localauthorityengagementnetworksandtherangeofothernetworksavailabletoreachouttothepublicandshareourdraftplans
• work inpartnershipwith communications teamsacrossNCLorganisationsandusetheirwide rangeofcommunitychannels to socialise theSTP, forexampleCamdenCCG’scitizens’panelandEnfield’sPatientParticipationGroupsNetwork.
• useexistingonlineengagementtoolsthatCCGs,localauthoritiesandprovidershaveto engage specific audiences and reach those who may be unable to attend ourevents.
Werecognise it iscrucial toensureour localpoliticalstakeholdersareactively involved intheoversightoftheplansastheydevelop.Weareplanningondoingthisby:
• planning regular face to facemeetingsbetween theSTP leadership teamand localcouncillorsandMPs,alongwithMinistersintheDepartmentforHealthifrequiredtoseektheirregularadviceonallproposedchanges
• continuingtoshareprogressupdatesoftheSTPatallmeetingsattheJointHealthOverview and Scrutiny Committee (JHOSC)ensuring that all political channelsthroughCCGs,localauthoritiesandprovidersarekeptfullybriefedontheSTPasitdevelopsandanypublicconcernsfortheregularengagementtheyundertakewithelectedleaders
• loggingallmediastoriesandregularlyupdatingtheTransformationBoardandthosemeetingwithelectedmembersontheSTPas itdevelops,mediadevelopmentandanypublicconcerns.
Thereisalsoaneedtoengagemoreofourownworkforceintheplanningprocess.Wewilldothisvia:
• the weekly STP newsletter that we have set up for those working within theorganisationsoftheSTP
• providingpeopleworkingwithinourorganisationswithregularupdatesonprogressthrough internal newsletters and bulletins, weekly / monthly updates from ChiefExecutives
• hosting sessions with a wider set of clinicians and social care practitioners to gettheir input intotheprioritiesanddeliveryareas.Thiswill includeworkingwithourGPFederationstoengageprimarycareproviderstoensureourworkforceisadriverandownerofchange
• runningeventswithinourmembershiporganisationstoshowcasetherangeofworkwhichishappeningacrossNCLandtoensurestaffunderstandthecurrentplans,andhowtheymayaffectthemasweprogressintoimplementation.
We will continue to build our communications and engagement capabilities across thesystem.Weareplanningtohostaworkshopwithcommunicationsleadsfromacrosssectorstoco-designthefutureengagementstrategy,havingnowidentifiedthekeyaudiencesthatweneed toengagewith across the5boroughs.The strategywill include thedesignofaprogrammeofdeliberative-styleeventswhichwillbringtogetherdifferentgroupstomore

67
directly shapeourplans.Wewillestablishadesignatedcommunicationsandengagementworkstream to oversee delivery of the strategy, with a Senior Responsible Officer forengagement.
10.2 Publicconsultation
Aformalpublicconsultationisnotneededforeveryservicechange.However,itislikelytobeneededshouldsubstantialchangestotheconfigurationofhealthservicesinalocalareabeproposedasourplansdevelopandwearecommittedtoensuringweconsultwidelyandeffectively.
Wearealreadybeginningtodevelopacomprehensivepictureof localviewsandconcernsthroughourearlyengagement,buildinganextensivestakeholderandcommunitydatabaseand contacts which will enable us to develop a detailed plan of those affected by anyproposedchanges.
We also have an existing relationship with both general and specialist media outlets(includingdigital).WearealreadyworkingonSTPstorieswiththesestakeholdersandwillcontinuetodosowhetherformalconsultationisrequiredornot.
10.3 Equalitiesanalysisandimpactassessment
UndertheEqualityAct2010,wearerequiredtoanalysetheeffectand impactoftheNCLSTPinrelationtoequality.Wearecommittedtocarryingoutanequalityimpactassessmentto ensure our plan does not discriminate against disadvantaged or vulnerable people, orotherprotectedgroups.
Our equality analysis will consider the effect on different groups protected fromdiscrimination by the Equality Act to ensure any changes are fully effective for all targetgroups and mitigate against any unintended consequences for some groups. We arecommittedtoundertakinganEqualitiesImpactAssessmentasourplansbecomemorefullydeveloped.
WealreadyhaveagoodoverviewandanalysisofequalityinformationfromacrosstheNCLfootprint through our existing and ongoing partnershipworkwith the 5 local authorities,CCGs, providers and other representative organisations.We are building on local regularequalityauditsofresidents,patientsandstafftoensuregoodengagementwithprotectedgroups and others, so that we can better understand the actual or potential effect ofchanges to functions, policies or decisions through the STP. This will help us to identifypracticalstepstotackleanynegativeeffectsordiscrimination, toadvanceequalityandtofostergoodrelations.
Throughout our engagement to date, and building on the insight above, we have takenadvice on best practice to ensure that all our public facing work is as fully accessible aspossible,includingsharinginformationinavarietyofformatstoensureourweareabletoengageallourresidents,using interpretersorEasyReadmaterialwhererequired.Wewillcontinue to hold events andmeetings in accessible locations (accessible for people withdisabilities and easily reached on public transport, with adaptationsmade for attendees’

68
communicationneeds).OuraimistoenabledifferentgroupstobefullyinvolvedastheSTPprogresses.
11 Conclusionandnextsteps
TheSTPisworkinprogressandwerecognisethatwehavemuchmoreworktodotodeliverthevisionwehavesetout.
TheimmediatenextstepsbetweennowandChristmasareto:
• totakestepstostabiliseourfinancialposition,developingmoredetailedideasintheareaswehavenotyetfullyexplored
• agreetheprioritiesforimplementationinthefirst2yearsoftheSTPtoensurethatwe focus initially on the improvements which will make the most impact on ourtripleaimsmostquickly.
Atthesametime,weareclearthatwewillnotlosefocusonthelongertermtransformationthatwillsupportsustainability.
Thereremainmanyissuestoresolveandweknowwedonothavealltheanswers.Butweare determined to succeed andwill continue toworkwith peoplewho use services, thepublicandourstafftofindsolutionsinthemonthsandyearsahead.

Page 1 of 2
Monthly report of Nursing staffing levels September 2016
Executive summary – including resource implications
The overall trust summary of planned versus actual hours for September was 1.5% lessactual hours than planned:
Site specific data is as follows:
• Barnet hospital 0.5% less actual hours than planned
• Chase Farm hospital 1.5% less actual hours than planned
• Royal Free hospital 2% less actual hours than planned
In September out of a minimum of 3,000 shifts there were 13 shifts reported where the nurse:patient ratio dropped below 1:8 on a day shift or 1:11 on a night shift. There were no patientsafety incidents reported on these occasions
Action required
The board is requested to
• consider if the report provides sufficient assurance that the nurse staffing levels aremeeting the needs of patients and providing safe care
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
1. Excellent outcomes – to be in the top 10% of our peers on
outcomes
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the
organisation for the future
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 6

Page 2 of 2
CQC outcomes supported by this paper
1 Respecting and involving people who use services
4 Care and welfare of people who use services
5 Meeting nutritional needs
7 Safeguarding people who use services from abuse
8 Cleanliness and infection control
9 Management of medicines
13 Staffing
14 Supporting staff
Risks attached to this project/initiative and how these will be managed (assurance)
Equality analysis
• No identified negative impact on equality and diversity
Report from Deborah Sanders, Director of Nursing
Author(s) Deborah Sanders, Director of Nursing
Date 16 November 2016
References: Supporting NHS providers to deliver the right staff, with the right skills, in theright place at the right time – Safe, sustainable and productive staffing, July 2016,https://www.england.nhs.uk/ourwork/part-rel/nqb/

Paper 6
1
IntroductionThis report provides information on planned versus actual nurse staffing for September 2016
and an update on progress with the reduction in use of agency nursing and midwifery staff.
Planned versus actual staffingThe overall trust summary of planned versus actual hours for September was 1.5% lessactual hours than planned:
Site specific data is as follows:• Barnet hospital 0.5% less actual hours than planned• Chase Farm hospital 1.5% less actual hours than planned• Royal Free hospital 2% less actual hours than planned
Planned versus actual staffingThe tables below show that planned versus actual hours by ward for registered nurses and
midwives and healthcare assistants.
Ward Beds
Registered nurse to
patient ratio
Day Shift
Percent of actual vs
total planned shifts
(RN days)
Percent of actual vs
total planned shifts
(RN nights)
Percent of actual vs
total planned shifts
(HCA days)
Percent of actual vs
total planned shifts
(HCA nights)
FallsAttributable
CdiffFFT Score
9 West 33 1:4 93% 98% 110% 67% 6 0 96%
9 North 33 1:4.7 85% 91% 85% 73% 6 0 88%
11 West 22 1:4.8 103% 128% 158% 253% 2 1 100%
11 South 19 1:3.8 87% 99% 122% 328% 0 0 91%
11 East 24 1:4.8 88% 100% 92% 110% 3 0 94%
10 East 24 1:3.4 94% 97% 88% 100% 3 0 84%
10 South 25 1:6.25 94% 103% 85% 108% 1 2 80%
5 East B 24 1:5 90% 100% 92% 105% 1 0 83%
Mulberry 13 1:5 85% 100% 136% n/a 2 0 96%
Transplantation and Specialist Services September 2016
Ward Beds
Registered nurse to
patient ratio
Day Shift
Percent of actual vs
total planned shifts
(RN days)
Percent of actual vs
total planned shifts
(RN nights)
Percent of actual vs
total planned shifts
(HCA days)
Percent of actual vs
total planned shifts
(HCA nights)
FallsAttributable
CdiffFFT Score
5 north A 18 1:4.5 97% 99% 94% 93% 0 0 92%
7East A 20 1:5 91% 100% 110% 115% 2 0 100%
7 East B 13 1:4.3 89% 100% 100% 117% 4 0 90%
7 West 32 1:4 93% 100% 100% 110% 7 0 86%
7 North 24 1:4.7 102% 106% 103% 103% 4 0 95%
Beech 24 1:6 103% 100% 97% 96% 2 0 70%
Canterb'y 25 1:6.25 81% 65% 62% 97% 3 0 95%
Cedar 24 1:4 70% 97% 153% 146% 3 1 94%
Damson 24 1:6 85% 100% 124% 145% 2 0 90%
Wel'gton 39 1:6.5 81% 61% 75% 120% 0 0 96%
Surgery and Associated Services September 2016
Ward Beds
Registered nurse to
patient ratio
Day Shift
Percent of actual vs
total planned shifts
(RN days)
Percent of actual vs
total planned shifts
(RN nights)
Percent of actual vs
total planned shifts
(HCA days)
Percent of actual vs
total planned shifts
(HCA nights)
FallsAttributable
CdiffFFT Score
6 North 20 1:4 98% 99% 100% n/a 0 0 n/a
5 South 31 1:8 87% 92% 84% 95% 0 0 89%
Neona te RFH vary 87% 100% 100% 100% 0 0 n/a
Galaxy 30 1:4 63% 82% 85% 30% 1 0 n/a
Neona te BH vary 80% 77% n/a n/a 0 0 n/a
Willow 16 1:5.3 117% 151% 108% 70% 5 0 94%
Victoria 48 1:8 103% 100% 148% 97% 0 0 95%
Womens and Childrens September 2016

Paper 6
2
Safe staffing
In September out of a minimum of 3,000 shifts there were 13 shifts reported where the
nurse: patient ratio dropped below 1:8 on a day shift or 1:11 on a night shift. There was one
night shift on Juniper where there was a ratio of 1:12. Capetown had 6 late shifts and 2 long
days with a ratio of 1:9. On Damson there were 2 part shifts where there was a 1:12 ratio, 1
early and 1 late and a night shift and long day with a 1:12 ratio. There were no reported
patient safety incidents reported on these occasions.
Registered nurse agency staff
On 1 September 2015 Monitor wrote to the trust advising of the rules for nursing agency
spending and setting out the spending ceiling for the trust. The rules are an annual ceiling
for total nursing agency spending for each trust and a mandatory use of approved
frameworks for procuring agency staff. The rules apply to all NHS trusts, NHS foundation
trusts receiving interim support from the Department of Health and NHS foundation trusts in
breach of their licence for financial reasons. All other NHS foundations trusts have been
strongly encouraged to comply.
On 19 October 2015 Monitor wrote to the trust confirming that the agreed ceiling of nurse
agency pay as a % of total nurse pay for the Royal Free London was 9.8% by March 2016
with a further reduction in April 2016. The further reduction % of nursing pay by agency has
not yet been issued rather the trust has been sent an overall control total of £29 million on
agency pay (all staff groups).
Ward Beds
Registered nurse to
patient ratio
Day Shift
Percent of actual vs
total planned shifts
(RN days)
Percent of actual vs
total planned shifts
(RN nights)
Percent of actual vs
total planned shifts
(HCA days)
Percent of actual vs
total planned shifts
(HCA nights)
FallsAttributable
CdiffFFT Score
10 North 32 1:5.3 97% 100% 97% 98% 5 0 85%
8 West 36 1:5.1 99% 107% 94% 97% 7 0 89%
8 North 32 1:4 92% 98% 93% 100% 1 2 89%
10 West 27 1:5 103% 116% 108% 146% 2 0 90%
8 East 26 1:4.3 95% 92% 94% 97% 1 0 76%
6 South 28 1:4 94% 100% 97% 99% 4 1 83%
ITU (RF) vary 1:1/1:2 99% 99% 113% 89% 0 0 n/a
ED (RF) n/a n/a 105% 113% 77% 91% 0 0 83%
ED(BH) n/a n/a 96% 102% 96% 99% 2 0 80%
UCC (CF) n/a n/a 106% 100% 77% n/a 0 0 n/a
Adelaide 25 1:6.25 71% 91% 97% 206% 1 0 50%
Capetown 36 1:5.1 98% 124% 148% 216% 1 0 80%
CCU 8 1:2 95% 99% n/a n/a 0 0 100%
CDU 24 1:4.8 90% 94% 118% 183% 0 0 100%
ITU (BH) vary 1:1/1:2 105% 101% 87% 80% 0 0 n/a
Juniper 24 1:4.8 105% 106% 98% 93% 3 0 88%
Larch 22 1:5.5 104% 107% 95% 97% 0 0 50%
Olive 22 1:5.5 93% 100% 96% 88% 4 0 88%
Palm 22 1:5.5 85% 99% 95% 73% 5 0 89%
Quince 24 1:4.8 104% 115% 123% 206% 4 1 75%
Rowan 24 1:4.8 82% 97% 132% 113% 2 0 90%
Spruce 24 1:6 93% 97% 98% 107% 0 0 50%
Walnut 24 1:6 89% 102% 114% 203% 2 0 81%
Urgent Care September 2016
Ward Beds
Registered nurse to
patient ratio
Day Shift
Percent of actual vs
total planned shifts
(RN days)
Percent of actual vs
total planned shifts
(RN nights)
Percent of actual vs
total planned shifts
(HCA days)
Percent of actual vs
total planned shifts
(HCA nights)
FallsAttributable
CdiffFFT Score
12 Wesr 15 vary 97% 100% 78% 98% 0 0 n/a
12 South 16 1:4 99% 100% 99% 98% 4 0 100%
12 Eas t B 12 vary 98% 100% 90% 95% 0 0 75%
Private Practice September 2016

Paper 6
3
The divisional nurse directors, heads of nursing and matrons have further increased controls
over agency usage and this combined with the new starters has led to a sustained decrease
in the use of agency staff.
E-rostering has now been rolled out to all inpatient and critical care areas across the Trust,
with all areas now liked to payroll. Areas with 15 or less nursing staff are now being moved
to E-rostering. A recommendation of Lord Carter is that nursing rotas should be approved
and published 6 weeks before the start date of the rota. The new policy has been introduced
and the new rotas under this time frame were due this month. 23% met the 6 week deadline
so further focus remains on this. When the e-roster roll out started there were only 18% of
wards that published their rota’s at 4 weeks so progress is being made.
Recruitment
A key driver to reducing agency cost is recruitment to substantive posts. Induction was
moved to the Peter Samuel Hall due to the large number of new nurses and midwives
starting with the trust.

Paper 6
4
There are currently 308 nursing and midwifery recruits in the pipeline, 96 have agreed start
dates and 224 are being processed. We continue to hold 2 assessment centres a month
alongside one open day a month

Paper 7
1X:\ Chair and CEO report 23 November 2016
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
Executive summary
This is a combined chairman’s and chief executive’s report containing items ofinterest/relevance to the board.
Action required
The board is asked to note the report.
Report From D Dodd, chairman and D Sloman, chief executiveAuthor(s) A Macdonald, board secretaryDate November 2016
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 7

Paper 7
2X:\ Chair and CEO report 23 November 2016
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
A TRUST DEVELOPMENTS
NORTH MIDDLESEX UNIVERSITY HOSPITAL NHS TRUST (NMUH)
The board will recall that David Sloman was appointed as Accountable Officer at NorthMiddlesex University Hospital (NMUH) at the same time as Libbie McManus was appointedchief executive at the trust. The chief executive of NHS Improvement has recently written tothank David Sloman for his personal support in stabilising the leadership situation at NMUHand assisting NHS Improvement secure key leadership roles for the trust’s executive team.David Sloman’s role as Accountable Officer will now cease, as Libby McManus has beenappointed Accountable Officer for the trust.
CHASE FARM HOSPITAL REDEVELOPMENT UPDATE
The Chase Farm Redevelopment build programme is continuing at pace with the concreteframe complete up to the second floor and a topping out ceremony planned for January2017. Construction is running on time and on budget. Contracts have been exchanged withLinden Homes for the sale of Parcel A, and the sale is due to be completed by 31st October.Revenue savings are being tracked on a monthly basis, and the savings on site are currentlyahead of plan. Detailed workforce and efficiency plans are being worked up as part of thetrust’s overall financial improvement plan.
ROYAL FREE HOSPITAL EMERGENCY DEPARTMENT UPDATE
The Royal Free emergency department redevelopment is being undertaken under twocontracts. The first has been completed, which provided a new dedicated paediatrics'emergency department and waiting area, new staff facilities and office accommodation and anew ambulatory care unit.
Contract 2 started on the 26 September 2016 and will be comprised of three phases. Thefirst phase of the construction works will deliver Part 1 of majors, a new reception desk, andthe rapid assessment and treatment area including new LAS handover facilities. Phase 2will provide a new imaging facility including two x-ray rooms and one CT suite, and a sixbedded resuscitation unit. The final phase completes the majors facility and delivers a new30 bedded CDU, which replaces the temporary facility. Contract 2 is programmed forcompletion in March 2018. This stage of the development scheme is particularly challengingfrom both a build and operations perspective due to the live nature of the environment, theadjacencies of the MRI and the challenges of the infrastructure. The clinical and projectteams are working closely to maintain clinical operations at all times. Projected expenditureand programme is currently in line with the approved business case.
B REGULATION
NHS IMPROVEMENT SINGLE OVERSIGHT FRAMEWORK
NHS Improvement (NHSI) is the operational name for the organisation which brings togetherMonitor and the NHS Trust Development Authority.
NHSI published its new Single Oversight Framework (SOF) in September 2016, following aconsultation period over the summer. The SOF introduced a new mechanism of categorisingtrusts according to their performance against a number of metrics across five themes (quality

Paper 7
3X:\ Chair and CEO report 23 November 2016
of care; finance and use of resources; operational performance; strategic change; leadershipand improvement capability). This segmentation replaces the previously used risk ratings byMonitor through its Risk Assessment Framework, and categories used by the NHS TrustDevelopment Authority through its Accountability Framework. The purpose of the singleoversight framework and segmentation is to help NHSI identify what support providers need.
Since the publication of the SOF NHSI has undertaken a shadow segmentation processbased on performance and other intelligence gathered over recent months. The results ofthis process have now been published. The shadow segment provides a starting point foruse of the single oversight framework. Formal segmentation (ie. non ‘shadow) willcommence from November onwards based on actual data collected under the SOF.
The majority (60 per cent) of providers are in segments one and two. However when brokendown by trust type the figures demonstrate that the ambulance and acute sector are facingthe extreme pressure, with two thirds of acute trusts and half of ambulance trusts insegments three and four.
RFL’s shadow segmentation is 2 (where 1 is the best rating and 4 is the worst). This meansthat NHSI will offer targeted support in areas where the trust is challenged. The trust hasbeen placed in segment 2 based primarily upon financial concerns around both surplus andcash. The segmentation will be reviewed on a monthly basis. The trust will have access toall NHSI’s universal support, guidance, tools etc which will be released on an ongoing basis,as well as targeted support to improve in areas identified under the SOF.
C BOARD AND COUNCIL MATTERS
NON EXECUTIVE DIRECTOR APPOINTMENTS
The board will recall the decision to appoint an additional non-executive director and theresignation of Dean Finch created a vacancy. The council of governors consideredrecommendations from the nominations committee for the appointment of two non-executivedirectors at its meeting on 15 November. The recruitment process included advertising andsearch activities; a long-listing discussion by the nominations committee, drawing up ashortlist and shortlisted candidates being briefed by the chairman and either chief executiveor deputy chief executive. The process concluded with the five shortlisted candidates havinga formal interview with members of the nominations committee – (Chairman, Judy Dewinterand Peter Atkin (elected patient governors) and Hans Stauss (appointed governor) togetherwith an external panel member, Yvonne Coghill, joint Director for NHS Workforce RaceEquality Standard Implementation at NHS England. The council of governors approved thenominations committee’s recommendations for two new appointments, further details will beprovided as soon as the appointments have been accepted.
Both appointments will commence 1 December 2016.
COUNCIL OF GOVERNORS
Aivet Phiri, elected public governor – rest of England, has resigned from the council ofgovernors and arrangements will be put in train to fill the vacancy created.

Paper 7
4X:\ Chair and CEO report 23 November 2016
D LOCAL NEWS AND DEVELOPMENTS
CYBER SECURITY
The Royal Free London has taken a number of steps to minimise the threat posed by Cyberattacks. These include regular penetration testing of the network to highlight security gaps,security patching of firewalls and encrypting data in flight. The Trust has also commissionedan external cyber security review and the recommendations from the report are beingimplemented. Governance of this is through the information governance group, with theaudit committee also maintaining oversight.
FLU VACCINATION CAMPAIGN
Every year, the influenza vaccination is offered to NHS staff as a way to reduce the risk ofstaff contracting the virus and transmitting it to their family members as well as patients.Healthcare workers may transmit the illness to patients even if they are mildly or sub-clinically infected as flu is a highly transmissible infection.
The occupational health department are leading the delivery of the vaccinations across thetrust.
Vaccination clinics are being held on all sites, and staff are offered the vaccination atinduction days and chief executive’s briefing meetings. There is also a daily walk-invaccination clinic at the occupational health departments at RFH and CFH. Peervaccinators have been recruited to vaccinate colleagues.
The ‘jabometer’ displayed on the landing page of Freenet is shown below, with the overallvaccination rate as at 8 November being 33% of staff.

Paper 7
5X:\ Chair and CEO report 23 November 2016
.INSTITUTE FOR HEALTHCARE IMPROVEMENT (IHI) QUALITY IMPROVEMENTDIAGNOSTIC
The trust’s quality strategy centres on embedding quality improvement across the trust’sdaily work. Embedding improvement into everyone’s routine in a systematic way will deliversubstantial benefits for patients (safer care, better outcomes, better patient experience), forstaff and better use of resources. It represents a significant and multi-year organisationaltransition. In late June the trust undertook a three-day on-site improvement readinessdiagnostic with the Institute for Healthcare Improvement (IHI). The diagnostic included 73sessions with over 500 staff across a broad range of professional groups (both clinical andnon-clinical) from all major trust sites, as well as patients, external stakeholders, and asession for governors. IHI’s recommendations can be grouped into six areas: settingcontext, leading and reinforcing, reducing red tape, data and analytics, engaging acrossboundaries and partnering with patients.
In November IHI will facilitate two one-day improvement workshops, one for the trust board,the other for around 120 senior clinical and other leaders. A working group is underway tooperationalise the strategy. IHI’s report is also informing work in related areas – for example,the trust’s analytic and data review, and a renewed emphasis on patient experience and co-production led by the patient and staff experience committee.
THE MARSDEN LECTURE
Professor Jason Leitch, the national clinical director for the Scottish Government, will begiving the Marsden Lecture at the Royal Free Hospital in the Sir William Wells Atrium at 5pmon 17 November 2016.
The Royal Free London holds the Marsden Lecture annually – it is named in honour of DrWilliam Marsden, who founded the Royal Free in 1828. Governors have been invited toattend.
Professor Leitch will be talking about Scotland’s approach to quality improvement –improving the quality of the care delivered to patients. Members of the public are welcome toattend the talk.
Improving the quality of healthcare has been at the heart of NHS Scotland’s Quality Strategysince it was published in 2010 and Scotland is unique in its ambitious attempts to implementquality improvement across a while national healthcare system.
Professor Leitch will describe how the Scottish patient safety programme has expanded fromthe acute hospital setting to include paediatric and neonatal care, maternity, mental healthservices and primary care. He will also explain how the early years collaborative is workingwith community health partnerships to improve outcomes for Scotland’s children, and howthe raising attainment for all programme is improving the educational outcomes for children.
The trust’s own quality improvement strategy centres on embedding improvements in to allstaff members’ routines in order to deliver benefits for patients such as safer care and abetter patient experience.

Paper 7
6X:\ Chair and CEO report 23 November 2016
PATIENT FRIENDS AND FAMILY TEST (FFT) UPDATE
The NHS friends and family test (FFT) was introduced in 2013 to enable patients to feedback on their care and treatment to enable hospitals and other providers to improveservices. It asks patients whether they would recommend hospital wards, A&E departmentsand maternity services to their friends and family if they needed similar care or treatment.
The FFT results are reviewed by the patient and staff experience committee and reported toevery public meeting of the trust board.
The tables below show the combined scores for all sites and then the results by site forOctober 2016.
Royal Free Londoncombined data
% likely/extremely likely torecommend October 2016
(range: 0 – 100%)
Number of patient responses
In-patient 90% 1351
A&E 81% 4907
Barnet Hospital % likely/extremely likely torecommend September 2016
(range: 0 – 100%)
Number of patient responses
In-patient 84% 426
A&E 80% 2564
Antenatal care 79% 29
Labour and birth 99% 86
Postnatal hospital ward 94% 88
Postnatal community care 98% 64
Out-patients 94% 83
Chase Farm Hospital % likely/extremely likely torecommend September 2016
(range: 0 – 100%)
Number of patient responses
In-patient 94% 151
Out-patients 95% 198

Paper 7
7X:\ Chair and CEO report 23 November 2016
Royal Free Hospital % likely/extremely likely torecommend – September 2016
(range: 0 – 100%)
Number of patient responses
In-patient 92% 774
A&E 83% 2343
Antenatal care 89% 38
Labour and birth 96% 81
Postnatal hospital ward 91% 81
Postnatal community care 98% 64
Out-patients 90% 344
COMMUNICATIONS REPORT
Media coverage
Positive
During October the trust featured positively in the local media as the communications teaminvited The Sunday Mirror and Barnet Press to photograph a dialysis patient’s 104th birthdaycelebration at Barnet Hospital. The Barnet Press then included this story on their front page.The Camden New Journal also ran a story on a new book by Barbara Wren, consultantpsychologist and Schwartz round lead.
In the national press, the Evening Standard mentioned the trust positively in a story aboutclinical trials taking place at the Royal Free Hospital. Tottenham Hotspur Football Club alsopublished a story about opening the Green Gym at Chase Farm Hospital, the story featuredpositive updates about the redevelopment and the health activities taking place at ChaseFarm Hospital.
Negative
The Ham & High included a negative story on their front page about five patient letters whichthe Royal Free Hospital sent to the wrong address. ITV News also included the Royal FreeLondon in a list of trusts which car parking charges. The Evening Standard, Telegraph andother local papers picked this story up. The Ham & High ran another story about the patientswho were infected with HIV at the Royal Free Hospital during the 80s and the Mail Onlinementioned the trust in a neutral story about ambulance waiting times.
Figure 1 shows the number of positive stories that the trust had during October. The trustwas mentioned in 26 positive stories for October.

Paper 7
8X:\ Chair and CEO report 23 November 2016
Figure 1
Figure 2 shows how much this positive coverage would cost if these pieces were paid foradvertorials, the total cost would be £18,770.25 for October
Figure 2
Figure 3 shows the sentiment of our press mentions split as positive, neutral and negative.The sentiment of our coverage is analysed through the tone of our mentions.
£10,882.86
£6,673.31
£1,214.08
£0.00
£2,000.00
£4,000.00
£6,000.00
£8,000.00
£10,000.00
£12,000.00
Royal Free Hospital July Barnet Hospital July Chase Farm Hospital July
RFL value October 2016
Royal Free Hospital July Barnet Hospital July Chase Farm Hospital July
13
9
6
0
2
4
6
8
10
12
14
Royal Free Hospital Barnet Hospital Chase Farm Hospital
Royal Free Hospital Barnet Hospital Chase Farm Hospital

Paper 7
9X:\ Chair and CEO report 23 November 2016
Figure 3
October Royal FreeHospital
BarnetHospital
Chase FarmHospital
Total
Positive 13 9 6 28
Neutral 344 23 4 371Negative 49 1 0 50
Total 406 33 10 921
Figure 4 shows how many media requests the trust received and how many statements andwebsite stories the external and digital communications team issued during the month ofOctober.
Figure 4
Figure 5 shows the daily breakdown of the trust’svolume of news stories compared to how manypeople they reached. Reach can be calculated ashigher if the trust is mentioned in national coveragecompared to local. There is a spike on Friday 7October as the trust was mentioned in stories about
Pauline Cafferkey. There is a spike on Friday 14 November as the trust was mentioned inan ITV News story about car parking costs.
Figure 5
October Trust total
Statements 10Mediarequests
33
Websitestories
12

Paper 7
10X:\ Chair and CEO report 23 November 2016
Figure 6 shows the number of reactions (likes) and comments our posts received, and thenumber of times they were shared across the month of October.
Figure 6
• The spike on 14 October shows the reaction to a post about Dr Nick Murch,
consultant in acute medicine, becoming the fifth person in the world and only the
second person in the UK to successfully swim Lake Geneva . This post reached
9,603 people.
• The spike on 19 October shows the reaction to a post about nurses at Barnet
Hospital helping a 104-year-old dialysis patient celebrate his birthday. This post
reached 7,015 people.
• The spike on 24 October shows the reaction to a post about new research, carried
out by Dr Victoria Male at the Royal Free Hospital, uncovering a new kind of immune
cell. This post reached 2,598.
Twitter activity - October• Total number of followers: 11,588• Increase of 210 compared to September 2016• Percentage increase YOY: 28.43%• No. of posts: 215• Most retweeted tweet: Consultant psychologist writes
book about helping #NHS staff to overcome theemotional challenges of their work (9 retweets)
• Most clicked tweet: Consultant psychologist writesbook about helping #NHS staff to overcome theemotional challenges of their work (43 clicks)
• Most liked tweet: One of our consultants,@AcuteMedEd, has become the 5th person tosuccessfully swim Lake Geneva (13 likes)
• The book tweet reached 1,472 people and theconsultant tweet reached 2,297 people.

Paper 7
11X:\ Chair and CEO report 23 November 2016
LinkedIn activity
Figure 7 shows the number of clicks our posts received over October.
Figure 7
• The spike on 5 October shows the reaction to a post advertising our senior digital
communications manager vacancy. This post reached 3,128 people.
• The spike on 19 October shows the reaction to a post about how the trust was
celebrating NHS Fab Change Day. This post reached 5,877 people.
• The spike on 28 October shows the reaction to a post advertising our occupational
therapist vacancy. This post received reached 3,882 people.
Internal communications
Figure 8 shows a breakdown of how many items the internal communications teamuploaded to our staff intranet, Freenet, during July, August and October.
Figure 8
Landing page newsLanding page
noticesFreenet news Events
August 22 18 28 7
September 38 28 46 12
October 35 19 39 17
0
10
20
30
40
50
RFL Intranet three months

Paper 7
12X:\ Chair and CEO report 23 November 2016
Figure 9 shows how many stories and notices the internal communications team publishedin the monthly staff magazine, Freepress and the weekly staff e-letter Freemail.
Figure 9
October Total stories andnotices
Freenet 110
Freepress 17
Freemail 67
Managers’ briefing 19
Figure 10 shows how many briefings and visits the internal communications team arrangedduring the month of October.Figure 10
October Total amount
Chief executivebriefing
5
Executive shadowing 1
Go-see visits 5
In this time the internal communications team also:
• Provided internal communication support for key trust improvement projects, the 2020
vision transformation programme and the financial improvement programme.
• Promoted the launch of the 2016 NHS staff survey and the actions taken to date in
response to the last two years’ feedback as part of the staff experience retention plan.
• Launched the winter flu campaign to help achieve the trust’s target of vaccinating 75%
of staff.
• Worked closely with the relevant staff groups to promote Healthy Living Week and
launch a range of activities to celebrate Black History Month in October.
• Continued to support the redevelopment of Chase Farm Hospital.

Paper 8
Page 1 of 2
Trust performance report
Risk Assessment Framework Ratings Summary
Performance summary 2016/17The Royal Free London NHS Foundation Trust recorded a Green rating under Monitor’s riskassessment framework in quarter one 2016/17.
September 2016With all data now available for September, apart from C. difficile, the trust failed two targetsduring the month:
1. A&E 4-hour standard2. Cancer 62 days from GP referral
This therefore equates to three non-compliant standards and therefore compliance againstthe governance regime with a Green rating achieved for the month.
This therefore equates to three non-compliant standards and therefore compliance againstthe governance regime with a Green rating achieved for the month.
Action required
For information and agreement
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
1. Excellent outcomes – to be in the top 10% of our peers on
outcomes
X
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
X
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
X
5. A strong organisation for the future – to strengthen the
organisation for the future
X
CQC Regulations supported by this paper
Regulation 8 ⃰ General
Regulation 9 Person-centred care
Regulation 10 Dignity and respect
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 8

Paper 8
Page 2 of 2
Regulation 12 Safe care and treatment
Regulation 17 Good governance
Regulation 18 Staffing
Regulation 20A⃰ Requirement as to display of performance assessments
Risks attached to this project/initiative and how these will be managed (assurance)
Failure to achieve and maintain compliance against Monitor risk assessment framework
standards and targets.
Equality analysis
• No identified negative impact on equality and diversity
Report from Kate Slemeck, chief operating officer
Author(s) Amy Caldwell-Nichols, head of performance; Temi Salam, information analyst
Date 17 November 2016

October 2016
Monitor Risk Assessment Framework
Performance for
2015/2016 Outturn
and
October 2016
Produced 7th November 2016

Monitor Risk Assessment Framework
Table of Contents
Section Pages
Monitor risk assessment framework dashboard 2015/16 Pages 3 - 4
Monitor governance risk rating 2015/16 - Royal Free London NHS Foundation Trust Page 5
Monitor governance risk rating 2015/16 - Royal Free Hospital Site Page 6
Monitor governance risk rating 2015/16 - Barnet Hospital Site Page 7
Monitor governance risk rating 2015/16 - Chase Farm Hospital Site Page 8
Monitor governance risk rating 2015/16 - Other Hospital Sites Page 9
Recovery trajectory compliance Page 10
Monitor high risk ratings Pages 11 - 24
Monitor low risk ratings Pages 25 - 26

October 2016
Section 1
Monitor Risk Assessment Framework Dashboard
Access Targets & Outcome Objectives
Operational Standards & Targets
October 2016 and Quarter 2

Monitor Risk Assessment DashboardMonth: October 2016
Summary
Risk Assessment Framework Summary A&E Performance against 95% Standard
Month Trend QTD Month Trend QTD
Royal Free London NHS FT Green1
Green1
Royal Free London NHS FT R R
Royal Free Hospital Green1
Green1
Royal Free Hospital R R
Barnet Hospital & Chase Farm Hospital Green1
Green1
Barnet Hospital & Chase Farm Hospital R R
C. difficile Performance against Trajectory 18-weeks RTT Performance
Month Trend QTD Month Trend QTD
Royal Free London NHS FT G G Royal Free London NHS FT G G
Royal Free Hospital G G Royal Free Hospital G G
Barnet Hospital & Chase Farm Hospital G G Barnet Hospital & Chase Farm Hospital G G
Cancer Performance against Targets2
Month Trend QTD
Royal Free London NHS FT R R
Royal Free Hospital R R
Barnet Hospital & Chase Farm Hospital R R
1Monitor framework adjustment applies
218-weeks RTT and
Cancer are reported for August 16
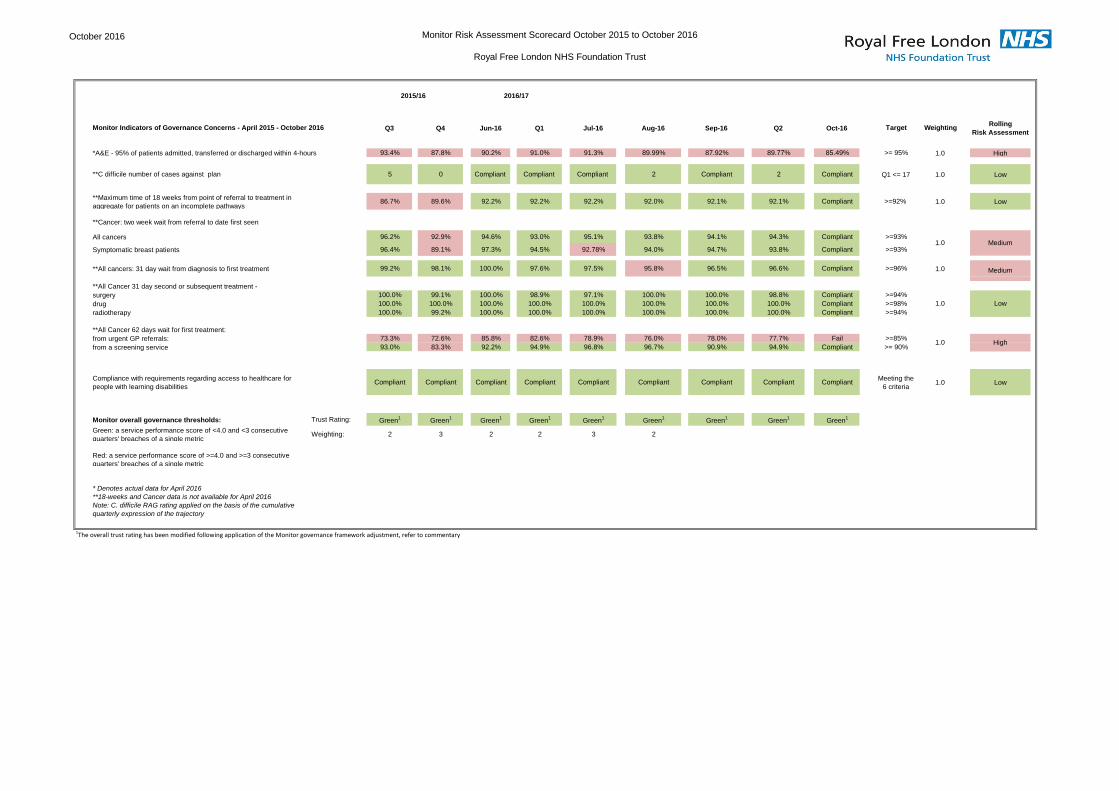
October 2016 Monitor Risk Assessment Scorecard October 2015 to October 2016
Royal Free London NHS Foundation Trust
Monitor Indicators of Governance Concerns - April 2015 - October 2016 Q3 Q4 Jun-16 Q1 Jul-16 Aug-16 Sep-16 Q2 Oct-16 Target WeightingRolling
Risk Assessment
*A&E - 95% of patients admitted, transferred or discharged within 4-hours 93.4% 87.8% 90.2% 91.0% 91.3% 89.99% 87.92% 89.77% 85.49% >= 95% 1.0 High
**C difficile number of cases against plan 5 0 Compliant Compliant Compliant 2 Compliant 2 Compliant Q1 <= 17 1.0 Low
**Maximum time of 18 weeks from point of referral to treatment in
aggregate for patients on an incomplete pathways86.7% 89.6% 92.2% 92.2% 92.2% 92.0% 92.1% 92.1% Compliant >=92% 1.0 Low
**Cancer: two week wait from referral to date first seen
All cancers 96.2% 92.9% 94.6% 93.0% 95.1% 93.8% 94.1% 94.3% Compliant >=93%
Symptomatic breast patients 96.4% 89.1% 97.3% 94.5% 92.78% 94.0% 94.7% 93.8% Compliant >=93%
**All cancers: 31 day wait from diagnosis to first treatment 99.2% 98.1% 100.0% 97.6% 97.5% 95.8% 96.5% 96.6% Compliant >=96% 1.0
**All Cancer 31 day second or subsequent treatment -
surgery 100.0% 99.1% 100.0% 98.9% 97.1% 100.0% 100.0% 98.8% Compliant >=94%
drug 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=98%
radiotherapy 100.0% 99.2% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=94%
**All Cancer 62 days wait for first treatment:
from urgent GP referrals: 73.3% 72.6% 85.8% 82.6% 78.9% 76.0% 78.0% 77.7% Fail >=85%
from a screening service 93.0% 83.3% 92.2% 94.9% 96.8% 96.7% 90.9% 94.9% Compliant >= 90%
Compliance with requirements regarding access to healthcare for
people with learning disabilitiesCompliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant
Meeting the
6 criteria1.0 Low
Monitor overall governance thresholds: Trust Rating: Green1
Green1
Green1
Green1
Green1
Green1
Green1
Green1
Green1
Green: a service performance score of <4.0 and <3 consecutive
quarters' breaches of a single metricWeighting: 2 3 2 2 3 2
Red: a service performance score of >=4.0 and >=3 consecutive
quarters' breaches of a single metric
* Denotes actual data for April 2016
**18-weeks and Cancer data is not available for April 2016
Note: C. difficile RAG rating applied on the basis of the cumulative
quarterly expression of the trajectory
2015/16
1The overall trust rating has been modified following application of the Monitor governance framework adjustment, refer to commentary
Low
High
1.0 Medium
1.0
1.0
2016/17
Medium

September 2016 Monitor Risk Assessment Scorecard October 2015 to September 2016
Royal Free London Hospital
Monitor Indicators of Governance Concerns - April 2015 - October 2016 Q3 Q4 Q1 Jul-16 Aug-16 Sep-16 Q2 Oct-16 Target WeightingRolling
Risk Assessment
*A&E - 95% of patients admitted, transferred or discharged within 4-hours 93.3% 89.5% 90.7% 92.1% 92.7% 84.9% 89.9% 84.1% >= 95% 1.0 High
**C difficile number of cases against plan 4 0 Compliant Compliant Compliant Compliant Compliant Compliant Q1 <= 8 1.0 Low
**Cancer: two week wait from referral to date first seen
All cancers 98.7% 97.4% 96.9% 96.4% 96.2% 96.7% 96.5% Compliant >=93%
Symptomatic breast patients 98.8% 95.0% 98.2% 94.4% 96.3% 96.6% 95.7% Compliant >=93%
**All cancers: 31 day wait from diagnosis to first treatment 98.5% 96.5% 95.5% 95.0% 92.8% 93.0% 93.6% Fail >=96% 1.0
**All Cancer 31 day second or subsequent treatment -
surgery 100.0% 100.0% 98.1% 92.3% N/A 100.0% 96.2% Compliant >=94%
drug 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=98%
radiotherapy 100.0% 99.2% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=94%
**All Cancer 62 days wait for first treatment:
from urgent GP referrals: 72.6% 69.8% 79.7% 71.1% 68.6% 71.6% 70.4% >=85%
from a screening service 92.6% 92.6% 91.7% 100.0% 94.1% 76.5% 89.1% Compliant >= 90%
Compliance with requirements regarding access to healthcare for people with
learning disabilitiesCompliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant
Meeting the 6
criteria1.0 Low
Monitor overall governance thresholds: Trust Rating: Green1
Green1
Green1 Red Green
1Green
1Green
1Green
1
Green: a service performance score of <4.0 and <3 consecutive quarters'
breaches of a single metricWeighting: 2 3 3 4 3
Red: a service performance score of >=4.0 and >=3 consecutive quarters'
breaches of a single metric
* Denotes actual data for April 2016
**18-weeks and Cancer data is not available for April 2016
Note: C. difficile RAG rating applied on the basis of the cumulative quarterly
expression of the trajectory
2015/16
1The overall trust rating has been modified following application of the Monitor governance framework adjustment, refer to commentary
1.0 Low
1.0 Low
1.0 High
High

October 2016 Monitor Risk Assessment Scorecard October 2015 to October 2016
Barnet Hospital
Monitor Indicators of Governance Concerns - April 2015 - October 2016 Q3 Q4 Q1 Jul-16 Aug-16 Sep-16 Q2 Oct-16 Target WeightingRolling
Risk Assessment
*A&E - 95% of patients admitted, transferred or discharged within 4-hours 91.5% 82.2% 91.3% 87.6% 84.5% 86.5% 86.5% 86.2% >= 95% 1.0 High
**C difficile number of cases against plan 1 0 Compliant Compliant 2 Compliant 2 Compliant Q1 <= 7 1.0 Low
**Cancer: two week wait from referral to date first seen
All cancers 94.5% 91.0% 91.7% 94.6% 92.2% 92.5% 93.1% Fail >=93%
Symptomatic breast patients 94.3% 81.5% 89.6% 91.4% 90.6% 95.7% 92.5% Compliant >=93%
**All cancers: 31 day wait from diagnosis to first treatment 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=96% 1.0
**All Cancer 31 day second or subsequent treatment -
surgery 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=94%
drug 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=98%
radiotherapy N/A N/A N/A N/A N/A N/A N/A Compliant >=94%
**All Cancer 62 days wait for first treatment:
from urgent GP referrals: 76.0% 75.5% 80.0% 79.7% 80.6% 83.0% 81.0% Fail >=85%
from a screening service 100.0% 91.7% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >= 90%
Compliance with requirements regarding access to healthcare for people with
learning disabilitiesCompliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant
Meeting the 6
criteria1.0 Low
Monitor overall governance thresholds: Trust Rating: Green1
Green1 Red Green
1Green
1Green
1Green
1Green
1
Green: a service performance score of <4.0 and <3 consecutive quarters'
breaches of a single metricWeighting: 2 3 4 3 3 3 3 3
Red: a service performance score of >=4.0 and >=3 consecutive quarters'
breaches of a single metric
* Denotes actual data for April 2016
**18-weeks and Cancer data is not available for April 2016
Note: C. difficile RAG rating applied on the basis of the cumulative quarterly
expression of the trajectory
2015/16
1The overall trust rating has been modified following application of the Monitor governance framework adjustment, refer to commentary
1.0 High
1.0 Low
1.0 High
Low
2016/17

Octoberber 2016 Monitor Risk Assessment Scorecard October 2015 to October 2016
Chase Farm Hospital
Monitor Indicators of Governance Concerns - April 2015 - October 2016 Q3 Q4 Q1 Jul-16 Aug-16 Sep-16 Q2 Oct-16 Target WeightingRolling
Risk Assessment
*A&E - 95% of patients admitted, transferred or discharged within 4-hours 99.9% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% >= 95% 1.0 Low
**C difficile number of cases against plan 0 0 Compliant Compliant Compliant Compliant Compliant Compliant Q1 <= 0 1.0 Low
**Cancer: two week wait from referral to date first seen
All cancers 95.5% 90.8% 89.9% 94.1% 93.9% 93.7% 93.9% Compliant >=93%
Symptomatic breast patients 96.6% 91.7% 92.5% 93.2% 96.2% 89.7% 93.4% Fail >=93%
**All cancers: 31 day wait from diagnosis to first treatment 100.0% 99.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=96% 1.0 Low
**All Cancer 31 day second or subsequent treatment -
surgery 100.0% 96.3% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=94%
drug 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >=98%
radiotherapy N/A N/A N/A N/A N/A N/A N/A N/A >=94%
**All Cancer 62 days wait for first treatment:
from urgent GP referrals: 69.1% 72.3% 80.4% 91.9% 83.9% 83.3% 86.9% Fail >=85%
from a screening service 80.0% 52.9% 100.0% 100.0% 100.0% 100.0% 100.0% Compliant >= 90%
Compliance with requirements regarding access to healthcare for people with
learning disabilitiesCompliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant
Meeting the
6 criteria1.0 Low
Monitor overall governance thresholds: Trust Rating: Green1
Green1
Green1
Green1
Green1
Green1
Green1
Green1
Green: a service performance score of <4.0 and <3 consecutive quarters'
breaches of a single metricWeighting: 1 2 2 0 2
Red: a service performance score of >=4.0 and >=3 consecutive quarters'
breaches of a single metric
* Denotes actual data for March 2016
**18-weeks and Cancer data is not available for March 2016
Note: C. difficile RAG rating applied on the basis of the cumulative quarterly
expression of the trajectory
2015/16
1The overall trust rating has been modified following application of the Monitor governance framework adjustment, refer to commentary
1.0 High
1.0 Low
1.0 High

October 2016 Monitor Risk Assessment Scorecard October 2015 to October 2016
Other Satellite Sites
Monitor Indicators of Governance Concerns - April 2015 - October 2016 Q3 Q4 Q1 Jul-16 Aug-16 Sep-16 Q2 Oct-16 Target WeightingRolling
Risk Assessment
*A&E - 95% of patients admitted, transferred or discharged within 4-hours >= 95% 1.0
**C difficile number of cases against plan Q1 <= 0 1.0
**Maximum time of 18 weeks from point of referral to treatment in
aggregate for patients on an incomplete pathways>=92% 1.0
**Cancer: two week wait from referral to date first seen
All cancers 93.4% 79.7% 82.8% 96.6% 89.3% 90.3% 92.0% Fail >=93%
Symptomatic breast patients 91.7% 42.9% 80.0% N/A 100.0% 100.0% 100.0% Compliant >=93%
**All cancers: 31 day wait from diagnosis to first treatment 100.0% 100.0% 100.0% 100.0% N/A N/A 100.0% Compliant >=96% 1.0 Low
**All Cancer 31 day second or subsequent treatment -
surgery >=94%
drug >=98%
radiotherapy >=94%
**All Cancer 62 days wait for first treatment:
from urgent GP referrals: 50.0% 84.8% 100.0% 100.0% N/A 0.0% 75.0% Fail >=85%
from a screening service 94.8% 100.0% 91.4% 90.0% 96.7% 97.2% 95.3% Compliant >= 90%
Compliance with requirements regarding access to healthcare for people with
learning disabilitiesCompliant Compliant Compliant Compliant Compliant Compliant Compliant Compliant
Meeting the
6 criteria1.0 Low
Monitor overall governance thresholds: Trust Rating:
Green: a service performance score of <4.0 and <3 consecutive quarters'
breaches of a single metricWeighting: 2 2
Red: a service performance score of >=4.0 and >=3 consecutive quarters'
breaches of a single metric
* Denotes actual data for April 2016
**18-weeks and Cancer data is not available for April 2016
Note: C. difficile RAG rating applied on the basis of the cumulative quarterly
expression of the trajectory
2016/172015/16
1The overall trust rating has been modified following application of the Monitor governance framework adjustment, refer to commentary
1.0 High
1.0
1.0 High

April 2016 Performance against Recovery Trajectory
Royal Free London NHS Foundation Trust Royal Free London NHS Foundation Trust Royal Free London NHS Foundation Trust
A&E 95% Trajectory 92% of patients with incomplete pathways waited less than 18-weeks RTT 52 week breaches
The A&E trajectory delivers compliance against the 95% standard from June 16 and
each month thereafter to September 16, from October 16 the trust returns to non-
compliance (as a result of winter pressures) for the remainder of 2016/17. The trust's
Chief Operating Officer is currently reviewing the delivery date of June 16 against the
quarter 1 forecast delivery-risk, following this review the trajectory may be amended.
Royal Free London NHS Foundation Trust Royal Free London NHS Foundation Trust
Cancer - 62 day wait from urgent GP referral 99% of patients on a diagnostic pathway within 6 weeks
The Cancer 62 day trajectory delivers compliance against the 95% standard from
June 16 and each month thereafter to the end of 2016/17. The trust's Chief Operating
Officer is currently reviewing the delivery date of June 16 against the quarter 1
forecast delivery-risk, following this review the trajectory may be amended.
Performance measured against trajectory
The graphs presented below represent the trust's actual performance ("measure") against externally submitted trajectories ("trajectory") during the course of 2015/16 and those trajectories submitted in respect of 2016/17. For 2016/17 the data will be
refreshed with each month's actual performance against trajectory. Where a negative variance (underperformance) is recorded against trajectory, or important contextual information is required, this will appear beneath each relevant chart.
90%
92%
94%
96%
98%
100%
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
De
c-1
6
Jan
-17
Feb
-17
Mar
-17
Patients with diagnostic pathways to have waited less than 6-weeks - Percentage of Trust Compliance
Measure Trajectory
60%
65%
70%
75%
80%
85%
90%All Cancer 62 Days Wait for First Treatment
Urgent GP Referrals
Measure Trajectory
80%
85%
90%
95%
100%
A&E - 95% of patients admitted, transferred or discharged within 4-hours
Measure Trajectory
80%
82%
84%
86%
88%
90%
92%
94%
Patients with incomplete pathways to have waited less than 18-weeks - Percentage of Trust Compliance
Measure Trajectory
0
50
100
150
200
250
No of 52 week Breaches
Measure Trajectory

April 2016 High Risk Ratings
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
A&E 95% Standard A&E 95% Standard A&E 95% Standard A&E 95% Standard
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet & Chase Farm Hospital Chase Farm Hospital
92% of patients with incomplete pathways waited less than 18-weeks 92% of patients with incomplete pathways waited less than 18-weeks 92% of patients with incomplete pathways waited less than 18-weeks 92% of patients with incomplete pathways waited less than 18-weeks
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
All Cancer 2 week wait All Cancer 2 week wait All Cancer 2 week wait All Cancer 2 week wait
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
Symptomatic breast 2-week wait Symptomatic breast 2-week wait Symptomatic breast 2-week wait Symptomatic breast 2-week wait
Risk Rating - High
86%
88%
90%
92%
94%
Oct
-14
No
v-14
Dec
-14
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-15
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Patients with incomplete pathways to have waited less than 18-weeks - Percentage of Trust Compliance
Measure Target
86%
88%
90%
92%
94%Patients with incomplete pathways to have waited less than 18-weeks
- Percentage of Trust Compliance
Measure Target
80%
85%
90%
95%
100%
A&E - 95% of patients admitted, transferred or discharged within 4-hours
Measure Target
80%
85%
90%
95%
100%
A&E - 95% of patients admitted, transferred or discharged within 4-hours
Measure Target
80%
85%
90%
95%
100%
A&E - 95% of patients admitted, transferred or discharged within 4-hours
Measure Target
88%
90%
92%
94%
96%
98%
100%
Cancer: 2 week wait (All Cancer)
Measure Target
84%
86%88%90%92%
94%96%98%
Cancer: 2 week wait (All Cancer)
Measure Target
88%
90%
92%
94%
96%
98%
Cancer: 2 week wait (All Cancer)
Measure Target
70%
75%
80%
85%
90%
95%
100%
Cancer: 2 week wait (Symptomatic Breast)
Measure Target
70%
75%
80%
85%
90%
95%
100%
Cancer: 2 week wait (Symptomatic Breast)
Measure Target
75%
80%
85%
90%
95%
100%
Cancer: 2 week wait (Symptomatic Breast)
Measure Target
79%
84%
89%
94%
Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16
Patients with incomplete pathways to have waited less than 18-weeks - Percentage of Trust Compliance
Measure Target
80%
85%
90%
95%
100%
A&E - 95% of patients admitted, transferred or discharged within 4-hours
Measure Target
84%
86%88%90%92%
94%96%98%
Cancer: 2 week wait (All Cancer)
Measure Target
70%
75%
80%
85%
90%
95%
100%
Cancer: 2 week wait (Symptomatic Breast)
Measure Target

April 2016 High Risk Ratings
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
Cancer - 62 day wait from urgent GP referral Cancer - 62 day wait from urgent GP referral Cancer - 62 day wait from urgent GP referral Cancer - 62 day wait from urgent GP referral
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
Cancer 62 days from screening Cancer 62 days from screening Cancer 62 days from screening Cancer 62 days from screening
60%
70%
80%
90%
100%
All Cancer 62 Days Wait for First Treatment Urgent GP Referrals
Measure Target
55%
65%
75%
85%
95%
All Cancer 62 Days Wait for First Treatment Urgent GP Referrals
Measure Target
60%
65%
70%
75%
80%
85%
90%
All Cancer 62 Days Wait for First Treatment Urgent GP Referrals
Measure Target
60%
70%
80%
90%
100%
Cancer 62 Days Wait for First Treatment Screening
Measure Target
60%
70%
80%
90%
100%
Cancer 62 Days Wait for First Treatment Screening
Measure Target
0%
20%
40%
60%
80%
100%
Cancer 62 Days Wait for First Treatment Screening
Measure Target
50%
60%
70%
80%
90%
100%
All Cancer 62 Days Wait for First Treatment Urgent GP Referrals
Measure Target
0%
20%
40%
60%
80%
100%
Cancer 62 Days Wait for First Treatment Screening
Measure Target

April 2016 Low Risk Ratings
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
Number of C. difficile infections against plan Number of C. difficile infections against plan Number of C. difficile infections against plan Number of C. difficile infections against plan
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
All cancers: 31 day wait from diagnosis to first treatment All cancers: 31 day wait from diagnosis to first treatment All cancers: 31 day wait from diagnosis to first treatment All cancers: 31 day wait from diagnosis to first treatment
Royal Free London NHS Foundation Trust Royal Free Hospital
All Cancer 31 day second or subsequent treatment for radiotherapy All Cancer 31 day second or subsequent treatment for radiotherapy
Risk Rating - Low
Summary:
The following indicators have been rated Low risk primarily on the basis that at trust level there is good headroom against the standard. However the trust requires compliance to be achieved at every hospital every month and quarter. The C. difficile charts have a black line
separating the data pre and post April 15, this reflects the change in counting methodology applied by Monitor from that date. From April 15 only infections relating to "lapses in care" are included for the purposes of the Monitor risk assessment.
86%88%90%92%94%96%98%
100%
All Cancers: 31 Day Wait from Diagnosis to First Treatment
Measure Target
90%92%94%96%98%
100%
All Cancer 31 Day Second or Subsequent Treatment Radiotherapy
Measure Target
94%
95%
96%
97%
98%
99%
100%
All Cancers: 31 Day Wait from Diagnosis to First Treatment
Measure Target
90%
92%
94%
96%
98%
100%
All Cancer 31 Day Second or Subsequent Treatment Radiotherapy
Measure Target
92%
94%
96%
98%
100%
All Cancers: 31 Day Wait from Diagnosis to First Treatment
Measure Target
0
1
2
3
4
5
C-Difficile
Measure Target
0
1
2
3
4
C-Difficile
Measure Target
01234567
C-Difficile
Measure Target
94%
95%
96%
97%
98%
99%
100%
All Cancers: 31 Day Wait from Diagnosis to First Treatment
Measure Target
0
1
2
C-Difficile
Measure Target

April 2016 Low Risk Ratings
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
All Cancer 31 day second or subsequent drug treatment All Cancer 31 day second or subsequent drug treatment All Cancer 31 day second or subsequent drug treatment All Cancer 31 day second or subsequent drug treatment
Royal Free London NHS Foundation Trust Royal Free Hospital Barnet Hospital Chase Farm Hospital
All cancer 31 day Second or Subsequent Treatment Surgery All cancer 31 day Second or Subsequent Treatment Surgery All cancer 31 day Second or Subsequent Treatment Surgery All cancer 31 day Second or Subsequent Treatment Surgery
97%
98%
98%
99%
99%
100%
100%
All Cancer 31 Day Second or Subsequent Treatment Drug
Measure Target
97%98%98%99%99%
100%100%
All Cancer 31 Day Second or Subsequent Treatment Drug
Measure Target
97%
98%
98%
99%
99%
100%
100%
All Cancer 31 Day Second or Subsequent Treatment Drug
Measure Target
0%
20%
40%
60%
80%
100%
All Cancer 31 Day Second or Subsequent Treatment Surgery
Measure Target
90%
92%
94%
96%
98%
100%
All Cancer 31 Day Second or Subsequent Treatment Surgery
Measure Target
90%
92%
94%
96%
98%
100%
All Cancer 31 Day Second or Subsequent Treatment Surgery
Measure Target
0%
20%
40%
60%
80%
100%
All Cancer 31 Day Second or Subsequent Treatment Drug
Measure Target
80%
85%
90%
95%
100%
All Cancer 31 Day Second or Subsequent Treatment Surgery
Measure Target

High Risk Indicators Commentary and Exception Report
Month: September 2016
Risk Assessment Framework - commentary
Trust performance overview
The table below summarises the performance against standard by site and by trust. Compliance is being delivered against all standards with the exception
of:
• A&E
• 62 day cancer
Period
Reported Indicator Description Standard STF All
Royal
Free Barnet
Chase
Farm Other
Oct-16 AE Patients admitted, transferred or discharged
within 4 hours
95% 92% 85.5% 84.1% 81.8% 100.0%
Oct-16 C Difficile
Cases
Lapses in care <=0 0 Compliant Compliant Compliant Compliant Compliant
Sep-16 RTT Patients on incomplete pathways waiting
less than 18weeks
92% 92% 92.1%
Sep-16 Cancer 2 week waits - All cancers
93% 94.1% 96.7% 92.5% 93.7% 90.3%
2 week waits - Symptomatic breast
93% 94.7% 96.6% 95.7% 89.7% 100.0%
31 day waits diagnosis to first treatment - All
cancers
96% 96.5% 93.0% 100.0% 100.0%
31 day waits diagnosis to first treatment –
Surgery
94% 100.0% 100.0% 100.0% 100.0%
31 day waits diagnosis to first treatment -
Drug
98% 100.0% 100.0% 100.0% 100.0%
31 day waits diagnosis to first treatment -
Radiotherapy
94% 100.0% 100.0%

High Risk Indicators Commentary and Exception Report
Month: September 2016
62 day waits from GP referral to treatment
85% 74.4% 78.0% 71.6% 83.0% 83.3% 0.0%
62 day waits from screening service referral
to treatment
90% 90.9% 76.5% 100.0% 100.0% 97.2%
Our focus remains on our areas of sustained non-compliance in A&E and Cancer. RTT performance has been compliant since June and we are progressing
with the next phase of development for the RTT patient tracking list (PTL). Diagnostics continues to be compliant with the 6 week standard in September,
including a return to standard for the Cystoscopy modality.
The Strategic Transformation Fund (STF)
For 2016/17 NHS Improvement has allocated additional funding from the STF to trusts delivering against agreed target recovery trajectories. Our
trajectories for all indicators are summarised in the table below – green indicates that we have met the trajectory, red that we have not.
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
A&E 4 hour standard 90% 92% 93% 95% 95% 95% 92% 90% 91% 91% 92% 92%
18-weeks RTT Incomplete Pathways 90% 91% 91% 92% 92% 92% 92% 92% 92% 92% 92% 92%
18-weeks RTT Volume of 52 Weeks
Breaches 5 5 5 5 5 5 0 0 0 0 0 0
99% of Diagnostic Pathways to be
Seen within 6-weeks 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%
Cancer 62 days from GP Referral 79.7% 75.2% 76.1% 77.4% 78.1% 74.4% 78.2% 83.8% 85.2% 85.3% 85.2% 85.2%

High Risk Indicators Commentary and Exception Report
Month: September 2016
A&E
We have now launched our Safer, Faster, Better programme, focusing on the areas for improvement as recommended by NHS Improvement. We are
currently working with teams to agree plans, performance measures and revise our 4 hour performance trajectory accordingly.
We are currently still on track to open the Barnet AAU development in mid-December, which should provide extra capacity to support A&E performance at
the front door. We have also launched our new Discharge to Assess pathways with local partners – this is low numbers to start with, but we expect
incremental increases over the next two weeks.
Cancer 62 day
Cancer 62 day performance for September was above our STF trajectory. We have progressed with our improvement plans, including:
• Resolving our renal theatre capacity issues, and
• Implementing our Infoflex merge project, bringing together the IT databases used to manage cancer services across RFH and BCF.
Our Q2 validation exercise has also been completed this month, which shows that we have been compliant in Q2 against all standards except 62 days.
There are remaining risks around:
• Our capacity to manage any unexpected increases in demand, including any resulting from potential changes to the breast cancer service at The
Whittington,
• Resolving remaining issues resulting from our Infoflex merge project,
• Implementing straight-to-test pathways for our Lower GI service, and
• Ensuring sufficient histopathology capacity to deliver improved turnaround times.
This is a key area of focus for operational teams as we aim for compliance in December.

Paper 9
FINANCE PERFORMANCE REPORT 2016/17 – Month 7
Executive summary
The Trust delivered an actual deficit of £34.8m at end of October; this was £38.3m worse than itsplanned surplus of £3.5m. Key factors driving the year to date variance from plan are
1. Income adjustments relating to prior year of £17.5m
2. Income provisions relating to this financial year of £3.1m
3. Under performance in clinical activity income
4. Over spend on pay mainly relating to use of agency to cover medical pay vacancies
5. Over spend on non-pay mainly due to outsourcing. We also have increased patient transportcosts due to change of supplier.
6. Under recovery of PPU income resulting in reduced contribution
7. Slippage against savings target
8. STF funding loss of £6.1m
Action required/recommendation
For Discussion
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk number(s)
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
CQC Regulations supported by this paper
Regulation 13 Financial position
Risks attached to this project/initiative and how these will be managed (assurance)
Equality analysis
• No identified negative impact on equality and diversity
Report from Caroline Clarke
Author(s) Senior Finance Team
Date 11th November 2016
Report to Date of meeting Attachment number
Trust board public 23 November 2016 Paper 9

Financial Performance ReportOctober 2016
1

FINANCIAL PERFORMANCE EXECUTIVE SUMMARY
October 2016
Measure Description Status Position Trend Variation
Normalised
Net Surplus /
(Deficit)
Net income and
expenditure excluding
profit from fixed asset
disposals and fixed asset
impairments
Net surplus/(deficit) in month:
Plan £1.1m, Actual (£6.3m),
Variance (£7.5m) adverse
Net surplus/(deficit) YTD:
Plan (£13.6m), Actual
(£51.9m), Variance (£38.3m)
deficit
NHS Clinical Income: The year to date (YTD) clinical income values as at 31st
October shows an under performance positon of (£28.4.m) which primarily relates
to prior year credit notes issued.
Other Income: (£2.1m) adverse from plan in month and (£7.7m) adverse YTD. The
adverse variance relates primarily to private patient reduced activity and pharmacy
wholesaling.
Pay excluding Integration: (£0.8m) adverse from plan in month and (£4.8m)
adverse YTD. Overspend is mainly due to use of agency to cover medical pay
vacancies and unallocated CIP targets.
Non-Pay excluding Integration & TEDD: £0.1m favourable from plan in month and
(£7.1m) YTD. Key overspent areas are outsourcing, patient transport and
unallocated CIP targets.
Integration: £0.3m favourable in month and £1.5m favourable YTD.
CIP Savings
Savings against the
recurrent CIP savings
plan. The plan includes
both cost efficiency or
income generation
schemes.
CIP in month:
Plan £2.8m, Actual £2.7m,
Variance (£0.1m) adverse
CIP year to date:
Plan £8.2m, Actual £10.4m,
Variance £2.2m favourable
Actual delivery of plans in M7 was of £2.7m, which is £0.1m adverse when
compared to plan.
Capital
Expenditure
Year to date cumulative
expenditure in non-
current assets.
CAPEX in month:
Plan £6.0m, Actual £4.4m,
Variance £1.6m favourable
CAPEX year to date:
Plan £48.7m, Actual £40.4m,
Variance £8..3m favourable
Capital expenditure for the month is £4.4m which is £1.6m less than plan.
All programmes are back on track and forecast to be witin CAPEX limit.
Cash
Cash held with the
government banking
service and in commercial
banks.
Cash flow in month:
Plan (£1.0m), Actual £6.8m,
Variance £7.8m favourable
Cash balance:
Plan £15.5m, Actual £13.7m,
Variance (£1.7m) adverse
The cash balance is below the planned levels in October due to the lower than
expected receipts of the planned prior year NHS over performance. In addition the
GP Lead programme that the Trust is hosting continues to impact cash due to non-
payment and late receipts for GP salaries.
The £13.8m cash balance reflects the Income and Expenditure deficit position and
non-recovery of NHS debts.
2015/16
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Capital Service Cover 1 1 1 1 1 1 2 3
Liquidity 4 4 4 4 2 2 4 4
Normalised I&E Margin 1 1 1 1 1 1 1 2
I&E Margin Plan Variance 2 2 2 2 3 1 4 4
Overall 2 2 2 2 2 1 2 3
Monitor
Financial
Sustainability
Risk Rating
(FSRR)
Monitor measures an
organisations financial
risk on a scale of 1-4 with
4 being the lowest risk
and 1 the highest risk.
2016/17 Actual 2016/17 Plan
Monitor FSSR: Trusts with a Normalised I&E margin of less than -1% are rated as 1
for this metric. A rating of 1 on any metric means the overall rating cannot exceed
2.
0
2
4
6
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
£m
Plan
Actual
0
2
4
6
8
10
12
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-1
6
Ap
r-1
6
May
-1
6
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
£m
Plan
Actual
0
50
100
150
No
v-1
5
Dec
-1
5
Jan
-16
Feb
-1
6
Mar
-1
6
Ap
r-1
6
May
-1
6
Jun
-1
6
Jul-
16
Au
g-1
6
Sep
-1
6
Oct
-1
6
£m
Plan
Actual
-30
-25
-20
-15
-10
-5
0
5
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
£m
Plan
Actual
A
R
G R
A
R
2

Paper 10
Shadow group board report – Board November 2016
SHADOW GROUP BOARD REPORT (OCTOBER)
Executive summary
The Shadow Group Board (SGB) met on 13 October 2016. The key issues discussed were:
• Update on partners and system stakeholders• New commissioning and delivery models in NCL• Group implementation, structures and processes• Group growth strategy• Google Deepmind• CSSD business case• Key worker accommodation
Members were advised that a paper on the Group BAF would be brought to a near futuremeeting.
Action required
To note.
Trust strategic priorities and businessplanning objectives supported by this paper
Board assurance risk number(s)
3. Excellent financial performance – to be inthe top 10% of relevant peers on financialperformance
5. A strong organisation for the future – tostrengthen the organisation for the future
CQC Regulations supported by this paper
Regulation 12 Statement of purposeRegulation 13 Financial position
Equality impact assessment
No identified negative impact on equality and diversity
Report From Dominic Dodd, chairmanAuthor(s) Mark Redhead, head of planningDate 28 October 2016
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 10

Paper 11
1
Report from finance, investment and performance committee - 15 November 2016 and 18 October 2016
Executive summary The finance, investment and performance committee met on 15 November 2016. The key points of note and items for discussion were as follows: Finance performance – Month 7
The committee considered the financial position as at Month 7, noting the ongoing serious financial situation.
The trust delivered an actual deficit of £34.8m at the end of October; this was £38.3m worse than the planned surplus of £3.5m. The committee noted the key factors driving the year to date variance, such as income adjustments related to prior year, income provisions related to 2016/17, under performance in clinical activity income, and overspend on pay.
Deteriorating performance was also having an adverse impact on the trust’s cash position which, at the end of October, was £13.8m against a plan of £15.5m.
Financial improvement plan (FIP) 2016/17
An update was given on the status of the trust’s FIP. A total of £10.4m of FIP savings had been delivered in the seven months against a target of £8.3m for the same period. A number of FIP plans had identified savings of £14.4m with a further £16.8m of savings identified in the pipeline plans; work was ongoing to ensure that the former could be delivered with confidence and that the latter were converted to concrete plans as soon as possible. Executive sponsors for the pharmacy, radiology and theatre workstreams attended the meeting to talk through their current FIP status and business performance year to date. The committee discussed the work being undertaken and planned to improve their financial position with specific focus on the action being taken to close the financial gap. After deliberation, the committee considered a greater focus on productivity was needed; that the electronic prescribing business case benefits should be taken through the committee; and that it would seek greater clarity on what additional contingent actions the trust could take to ensure that it hit the CIP target that year.
Accessing the Department of Health’s (DH) revolving working capital facility
In light of the trust’s deteriorating financial position and the detrimental impact on the cash position, the committee was asked to support access to DH’s revolving working capital facility. The committee were in support, noting that the trust executive committee had discussed the position in depth at its meeting the previous week where the chief executive had been delegated authority to agree the submission (board resolution) to the DH with the chairman. The committee did ask, however, that a statement outlining the trust’s
Report to
Date of meeting Attachment number
Trust Board
23 November 2016 Paper 11
Paper 11
2
compliance with the terms and conditions against the capital facility be circulated to the board for completeness.
Agreement of the 2017/18 and 2018/19 control totals
The committee was asked to discuss its options in regards to the 2017/18 and 2018/19 control totals. The chair considered the committee was not in a position to agree its approach at the meeting as a greater understanding was needed on what would be achievable and what the associated assumptions alongside that would be. The committee agreed to debate the options in more detail at the November board meeting when the additional information requested would be available.
Finance, investment and performance committee held on 18 October 2016 The finance, investment and performance committee met on 18 October 2016. A verbal report from that meeting was provided at the trust board on 19 October 2016 but for completeness a written report is attached (Annex 1).
Action required The board is asked to note report.
Equality impact assessment No negative impact on equality or diversity.
Report From Dominic Dodd, non-executive director and chair of the committee Author(s) Veronica Jackson, committee secretary Date 16 November 2016

Paper 11
3
Annex 1
Finance, investment and performance committee held on 18 October 2016 The finance, investment and performance committee met on 18 October 2016. A verbal report from that meeting was provided at the trust board on 19 October 2016 but for completeness a written report follows: Financial performance – Month 6
The committee considered the financial position as at Month 6, noting the ongoing serious financial situation.
The trust had delivered an actual deficit of £28.4m at the end of September; this was
£30.7m worse than its planned surplus of £2.4m. The committee noted the key factors driving the year to date variance from plan. It also noted the challenging position on cash.
The committee noted the Month 6 activity and income position, and was updated on the
current state of negotiations with NHS England and local Clinical Commissioning Groups to settle outstanding amounts owed.
An update was given on the status of the trust’s financial improvement plan (FIP). At the
half year point, the trust had achieved £7.7m in FIP savings which met the target set for that period. For the full year, forecast savings were £17.9m against the £46.3m target. Total pipeline ideas totalled £22m, but it was noted that the pace of converting ideas into concrete plans had to quicken, with immediate focus given to the biggest wins.
The committee noted the new requirements being imposed on agency staff by NHS
Improvement (NHSI). Trusts were required to report to NHSI to a granular level of detail on agency staffing, and there was a new requirement to apply for prospective approval for higher cost interim staff.
Monitor risk assessment framework
The committee noted that the two main performance challenges remained the cancer 62 standard and the A&E 4-hour standard. The trust was working to be compliant with the cancer target by December but this would be challenging. It was noted that the trust’s ‘safer, faster, better’ programme was due to be launched. The programme was designed to improve A&E processes and flow through the hospital.
Quarter 2 2016-17 NHSI (formerly Monitor) submission
The committee agreed to recommend to the board that it confirm the following statements for submission to NHSI: For finance that the board could not confirm the statement that the trust would
continue to maintain a financial sustainability risk rating of at least 3 over the next 12 months.
For governance that the board was satisfied that plans in place were sufficient to ensure: ongoing compliance with all existing targets (after the application of thresholds) as set out in Appendix A of the risk assessment framework, other than the 62 day cancer target and the A&E target; and a commitment to comply with all other known targets going forward.
The committee noted that from Quarter 3 2016-17 onwards the trust would be operating under the new single oversight framework had had been given a shadow rating.
Capital expenditure report
The committee noted that in-month project activity had been good, and the trust was on target to meet its capital year end spend target.

Paper 11
4
Progress updates in relation to the redevelopment of Chase Farm Hospital and the
refurbishment of the Royal Free Hospital’s emergency department were received.
It was noted that the capital programme was under review. This would be taken through the capital management group and the finance, investment and performance committee thereafter.

Paper 12
Page 1 of 2FINAL 15/11/16
Report from the patient and staff experience committee held on 17 October 2016
Executive summary
The patient and staff experience committee (PSEC) met on 17 October 2016. A verbalupdate was provided at the trust board meeting held on 19 October 2016 but forcompleteness a written report follows.
Part I - Public and patient engagement and involvement
The first part of the meeting had been given over to a seminar on public and patientengagement and involvement.
The director of patient experience from Northumbria Healthcare NHS Foundation Trust (FT)gave a presentation on how her trust had prioritised involvement and how it had went aboutgetting staff and patients enthused and involved. She explained how the trust had massivelyincreased the number of staff who thought that improving the patient’s experience was thetop priority, and had also developed very effective ways of gaining ‘real time’ and ‘right time’feedback.
The chair considered the presentation and subsequent discussion to be extremely insightful,and which provided a good baseline for the RFL in helping it consider further it’s aspirationsin this area. It was clear that the Northumbria Healthcare FT was well ahead in this regards,and the chair was keen continue to collaborate with the trust in sharing learning, knowledgeand expertise.
The detail of the presentation and discussion is reported in full in the minutes of the meeting.
Part II - The second part of the meeting was business as usual
Change to committee membershipThe committee noted that the chief executive had stood down as a member of PSEC due tocommitments with his role as chair of the North Central London Sustainability andTransformation Plan programme. The chair requested that the committee formally record itsthanks to the chief executive for his helpful contributions during his time as a member.
The committee recommended that the director of quality become a regular attendee of thecommittee and therefore be formally invited to attend future meetings.
Non-emergency patient transport (NEPT) updateThe committee noted that a new service provider, DHL Supply Chain, had taken over theservice provision for the trust’s NEPT on 21 August 2016 with support from SpecialistAmbulance Transport Services (SATs) for all specialist ambulance provisions. It was notedthat the overall the transition had gone well with minimal impact on service delivery and
Report to Date of meeting Attachment number
Trust Board 23 November 2016 Paper 12

Paper 12
Page 2 of 2FINAL 15/11/16
patient experience, there had been good engagement and team working, and a reductionhad been seen in the number of incidents and PAL complaints compared to the same periodthe previous year. The chair was pleased to note the smooth transition thus far and alsothanked the director of facilities for his efforts in this area.
On an associated issue, the committee reviewed the trust board assurance framework(BAF). It agreed to recommend to the board that risk 1b/3b in relation to patient transport beremoved as the director of facilities reported that his department had undertaken its ownreview of this risk and agreed it could be downgraded. It was now monitored by way of itsinclusion on the trust risk register.
Action required
The board is asked to note the report.
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
x
CQC Regulations supported by this paper
Regulation 9 Person-centred care
Regulation 10 Dignity and respect
Regulation 11 Need for consent
Regulation 12 Safe care and treatment
Regulation 13 Safeguarding service users from abuse and improper treatment
Regulation 16 Receiving and acting on complaints
Regulation 18 Staffing
Risks attached to this project/initiative and how these will be managed (assurance)
Not applicable.
Equality analysis
• No identified negative impact on equality and diversity
Report from Jenny Owen, non-executive director and chair of the patient and staff
experience committee
Author(s) Veronica Jackson, committee secretary
Date 15 November 2016