Embed Size (px)
DESCRIPTION
46th Annual Educational Conference & Exhibition Patient Access: The First Connection to a Lasting Impression September 23, 2014. Operationalizing New Transparency Requirements Katherine H. Murphy, FHAM, CHAM VP Revenue Cycle Consulting, Passport/Experian Health. What Patients Want. - PowerPoint PPT Presentation
Citation preview

Operationalizing New Transparency Requirements Katherine H. Murphy, FHAM, CHAM
VP Revenue Cycle Consulting, Passport/Experian Health
46th AnnualEducational Conference & Exhibition
Patient Access: The First Connection to a Lasting Impression
September 23, 2014

WHAT PATIENTS WANT• Designing Access is the Most Important Initiative
You Can Undertake
• Expertise from Y-O-U!
• They do not want to work hard for Access or Information
(“If you make me work hard to do business with you I will go somewhere else”)
They want to be W-E-L-L
Paul Roemer, VP Clinovations/Pale Rhino Consulting

TRANSPARENCY - DEFINED
• Generally implies openness, communication, and accountability. Transparency is operating in such a way that it is easy for others to see what actions are performed.
• “The perceived quality of intentionally shared information from a sender".
• Infusion of greater disclosure, clarity, and accuracy into their communications with stakeholders

Can we make a complicated process simple?
I think we
need to
schedule
another
appointment
…
Doc, What is Healthcare Transparency
?

TODAY’S LESSON
• Transparency Overviews• Best Practice
• Industry Best Practice recommendations• How to follow the recommendation
• Provider Journey• Provider success story: The start up & current state• Transparency future state
• Transparency Gone Wild! (Going the Extra Mile)• Technology• Patient Engagement• How to drill down estimates and be closer to the truth!

THE WAY WE WERE
04/20/23 6
So…Lola,what did you say a “dial tone” was for?

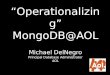
THE PATIENT BALANCE DEATH SPIRAL
04/20/23 7
$200
2005 2007
$250
$250
$265
2015
$312
$420*
-- CONSUMER TO PAYER -- -- CONSUMER TO PAYER --
Breakdown of U.S. Healthcare Consumer ResponsibilityU.S.$ billions, estimates
-- CONSUMER TO PROVIDER --
-- CONSUMER TO PROVIDER --
$450
$515
PROJECTED$732
*Source: 2007 & 2009 McKinsey analysis

8
If only Price Transparencywas this easy!

I know everyone will be excited about new ways not to get paid

TRANSPARENCY CAN OCCUR WHENEVER THERE IS COMMUNICATION BETWEEN ANY TWO OF:
- Insurer- Provider: hospital/physician/Patient Access & Patient- Primary Care Physician- Specialist- Ancillary testing facility- Post Acute Care
- Nursing Home- Home Health- Family Caregiver- Pharmacy

TODAY TRANSPARENCY ACROSS THE CONTINUUM! (NOT RELATED TO ANY ONE EPISODE)
. • Office Visit…
• Scheduling…Testing…
• Admission/Reg…
• Discharge…
• Billing…for svc you provided
• Payment
• Bill me
• Connected to EMR’s/ACOs
• Confirm appt / Pt Arrival/ Results
• PreService Clearance prior
• Phys office + specialists + Others
• Billing=combination of providers
• Bundled Payments
• Pay me
Old Paradigm – episode of care New Paradigm – Pop Health Mgmt

From To
Fee for Service Payment
Risk and/or Incentives for Keeping Patients Healthy. P4P (Pay for Performance), Shared Savings, Capitation
Care Not Coordinated Between Providers
Providers Managing Continuum of Care. Right Care at the Right Place/Time. Care Coordination, Transitions of Care leveraging community resources
No Shared Patient Information
Electronic Health Records enable information Sharing. Health Information Exchange
Doctors Wait for Sick People to Show Up
Predictive modeling, Proactive Monitoring and Outreach. Telemedicine, Patient Centered Medical Home, Home visits
Patients Wait for Providers to Tell Them What to Do
Patients Actively Engaged in Improving and Managing their Health. Personal Health Records, Home Monitoring Devices, Patient Engagement/Liability estimates
Moving from Volume to Value: What’s Moving from Volume to Value: What’s Different?Different?
Degree of Transparency!Degree of Transparency!
12

SO IT SHOULDN’T BE A SURPRISE THAT…
• Notice to Patients Required for Outpatient Facility Fees
• Posted: 24 Apr 2014 11:36 AM PDT (Effective Oct. 2014)• The Connecticut House of Representatives responded on Wednesday to medical billing
concerns patients expressed over undisclosed and unexpected facility fees by unanimously passing a bill that requires notice. Many patients expressed that the additional charges were a surprise when they received their bill. The legislation now moves to the state Senate for a vote.
The charges, often referred to as "facility fees" are charged to patients by medical offices that are owned by hospitals for outpatient care. These fees are separate from doctor fees. Facility fees range from several hundred to thousands of dollars.
The bill to require notice to patients about fees possible extra charges for outpatient care at medical offices owned by hospitals. The bill specifically requires that patients with scheduled appointments at medical offices where facility fees are charged receive notice about the fees in plain language before they receive treatments scheduled so long as the appointment is scheduled at least 10 days in advance. If the exact nature of the services or insurance coverage is unknown the patients would be provided with an estimate based on typical charges at the facility. Notice for patients receiving emergency care would need to be delivered as soon as practicable after the patient is stabilized. The bill does not impact the offices' ability to charge facility fees.
Other provisions in the bill are include requirements that the office prominently displays that the facility is connected to a hospital, what hospital the office is affiliated with, and states that the patient may incur higher charges than if they were treated at a facility that isn't hospital-based.

MASSACHUSETTS CHAPTER 224
The law aims to control health care cost growth through a number of mechanisms, including the creation of new commissions and agencies to monitor and enforce the health care cost growth benchmark, wide adoption of alternative payment methodologies, increased price transparency, investments in wellness and prevention, an expanded primary care workforce, a focus on health resource planning, and further support for health information technology

NEW BUSINESSESINVESTORS ARE DRAWN TO THE CONCEPT OF PRICE TRANSPARENCY, WITH SHARES RISING 139 PERCENT ON ITS FIRST DAY OF TRADING.
• Castlight is helping patients select the best price, and quality service. Are you ready?• If you’re not offering competitive prices and
high quality outcomes employers and patients may start taking their business elsewhere. Wall Street appears to have casted their vote in favor of patient consumerism.

CANARY – INFECTION TRANSPARENCY
“Using the breath biomarker, we can pick up the body getting ready to fight infection ... even before the patient is showing signs,”

SHAREPRACTICE - NEW WAY TO RATE TREATMENT?
Yelp for Doctors? over 5,000 health care providers using the app

TAPCLOUD

WHAT ARE WE TASKED WITH?
AND HOW DO WE ACCOMPLISH

ENTERPRISE TRANSPARENCY: PROVISION OF CARE
• Provider organizations will have clear policies on how to interact with patients with prior balances choosing to have elective or non-elective procedures. They will also have clear definitions for elective and non-elective procedures. These policies will be made available to the public.
• Brochures, Website, all documents
• Patients do not speak ABN, MSP, elective, In from Out!
• Lasix vs Furosemide

BEST PRACTICES FOR TRANSPARENCY
• Have defined processes for all patient types: EMR – OPT – INPT – Pre
• Discussion with Participants - not to disrupt workflow
• Patient Share Responsibility / Estimate / Navigation Counselor • When: Pre/Post Service, Emtala, Walk-ins
• Include Financial Screening along with Estimation * Use of consumer data * Toll Free number / Business Cards
• Appropriate Discussion Settings & Script
• Pre – Point - change in discharge process (fast pass?)

THE BEST PAYMENT PROMISE
• Know who is in front of them. I.D. your patient – Keep patient SAFE & STOP RETURN Mail
• Define the medical language in CONSUMER language• Have the correct insurance and benefit information.• Tell patients what they will owe at the time of service.• Enroll for Financial Assistance before rendering service.• Extend hospital charity to those who qualify.• Securely accept payment upfront for smaller balances.• Extend payment terms and fundraising options for larger balances.
04/20/23 22
Every patient leaves knowing what they owe & how their services will be paid for! Excellence in Patient Financial Triage includes determining the Patient’s Preferred method for future Communications!
Providers must…

WHO, WHERE, WHEN? HOW EASY IS THIS FOR YOU?
• Prior Balance Discussion
• Balances across their continuum of care
• Payment plans tailored to successful collection
• Summary of Care Document
• Annual Training of Registration – MSP, Collections, Payer Skills, Industry trends & updates

MEASUREMENT/COMMUNICATION
• Collections / accuracy• Consumer satisfaction Surveys / real time• Host Focus Groups• Define Medical and Legal terms and provide
access to them – See handout
• Access success – Reduction in Dups, return mail & patient complaints, cancellations, no-shows
• Increase – patient satisfaction scores, collections, employee satisfaction, positive internal relationships
•


• Display Confidence!
• Be sensitive to the situation (emotional intelligence)
• Be aware of cultural differences
• Be humane, respectful and honest
• Determine what leverage you have
• Be realistic – understand the strategy and policy
• Hire with these traits in mind

LISA TOZIER – ST JOSEPH’S STORY

PROVIDER OVERVIEW
• Faith Based organization• Bangor Maine, Population 33,000• St Joseph Hospital/Covenant Health System• Licensed for 112 beds• Self pay portions increased volume • Transparency & collection = new concept to
patients• Delicacy in rolling out the changes and
keeping within the mission

PATIENT ACCESS/REVENUE INTEGRITY
MANAGER
• Manage the day to day operations for a Patient Access staff of 30• Responsible for pre-reg, pre-cert, face to face reg and the ED• Manage the day to day operations for a Reimbursement staff of 3• Responsible for managing charging throughout the hospital • Responsible for managing RAC, MIC, ADR and 3rd party audits• Liaison between the revenue cycle departments• Lead our Revenue Integrity Team• Spend 2 hours a week working with Patient Accounts solving
issues• Spend 2 hours a week working with IS to ensure our revenue
cycle computer systems are running correctly. • Lead implementation coordinator for all revenue cycle software• Maintain security for revenue cycle software programs• Responsible for the overall maintenance of the hospital’s
chargemaster• Responsible for the expanded proration file

BENEFITS OFFERED
• Patient discounts from Providers
• Financial Counseling Services
• Card give to patient for Counseling hours
• Establishing a Physical Space and staffing in the ED (certified counselor for HIX) Key Factor: Physical Space

CENTRALIZED & DECENTRALIZED OVERSIGHT
• Challenges
• Training staff – 2 day with pre-reg staff and time with education trainers
• ipad swipes / kiosks (where, which patients)
• Outcome: More Transparency = shorter throughput

COMMUNICATION - LIAISON
• Role connectivity between rev cycle, ancillary and I.T. departments to make process improvements
• Automated process developed allows for Patient Access + PFS transparency.
• Dedicated price estimation line and dedicated Financial Counseling line.
• Keep it Simple - allow for Patient Engagement via patient portal, smartphones etc

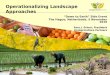
Patient Responsibility Deposit MatrixDepartment SJH employees and their family with Aetna
through the hospitalPatient % Liability with
Insurance or deductible from Passport or use amount below
Medicare Patients with no secondary Self Pay WE DO NOT COLLECT FROM THE FOLLOWING PEOPLE
Inpatient $150 (if admitted through ED there is no charge) $150.00 NONE $500.00MEDICARE PT WITH SECONDARY INS; ALSO, WHEN MEDICARE IS THE SECONDARY INSURANCE
Emergency Department$150 copay If they don’t have encourage payroll
deduction $50.00 or copay per passport/card $10.00 $200.00 PATIENTS WITH TWO OR MORE INSURANCES
Diabetes $10.00 $10.00 $10.00 $100.00MAINECARE PATIENTS WITH THE EXCEPTION OF THOSE THAT HAVE A CO-PAY
Nutrition $5.00 $5.00$30.00 unless PT has dx of diabetes or renal
disease then nothing $30.00 VA PATIENTS
Cardiology $10.00 $10.00 $10.00 $90.00 WORKER'S COMP PATIENTS
Cardiac Cath $50.00 $50.00 $50.00 $500.00 THIRD PARY LIABILITIES
ENDO (excludes colonscopies) $50.00 $50.00 $50.00 $500.00 MVA'S
Outpatient Surgery $50.00 $50.00 $50.00 $500.00 SCREENING MAMMOGRAMS
Pain Clinic $50.00 $50.00 $50.00 $500.00 COLONOSCOPY PATIENTS
RBCC Diagnositics $25.00 $25.00 $10.00 $200.00
RBCC Bone density $10.00 $10.00 $10.00 $70.00
X-RAY $15.00 $15.00 $10.00 $150.00
CT, MRI, NUC, US, Sleep Lab, EEG $20.00 $20.00 $10.00 $200.00
Wound Clinic $20.00 $20.00 $10.00 $100.00
Infusion Clinic $5.00 $5.00 $10.00 $50.00
Hyperbaric $20.00 $20.00 $50.00 $250.00
REMEMBER TO SMILE WHEN YOU SAY HOW WOULD YOU PREFER TO PAY FOR THAT TODAY

TACKLING PRICING TRANSPARENCY• CDM• Historical Claims Data• Complex Contract terms• Manipulating pricing/co-morbidities• Correct Insurance plan codes• Rich Eligibility Data(Web, COB, HIX)• Carve outs• Ability to Pay• Propensity to pay• Collection process• Payment plan creation• Portal payments• Ability to explain calculations
OUCH!

#1 : SUPPORT FROM INTERNAL RESOURCES
• ED and ancillary staff• Revenue Cycle Departments• Senior Management – on board• I.T.!• Working to budget much needed resources• Provider owner physician practices & entities• All staff physicians • Their Office staff • Marketing
Educating consumers and supporting the vision is everyone’s job.

QUALITY MANAGEMENT – IT’S WHAT’S UPFRONT THAT COUNTS!
• Without quality data you cannot be transparent with any sense of accuracy• Scrub accounts upfront• Auto scripting corrections means less
rekeying and less chance for error.• Snapshots of electronic trx and info kept for
audit trail• Reports! Communicate Success!
Ya Gotta Be a Team Player

GOALS FOR TRANSPARENCY IMPLEMENTATION
• ONE Integrated platform – Touchless processing! Lisa joined Exp/PP
• Work queues• Address verification USPS and Validation• Q.A.• Eligibility Verification• Scripting address & eligibility corrections/carrier codes• Medical Necessity• Automated Pre-Authorizations• Patient Liability Estimator • Payment Processing • Patient Portal & results tracking/reporting• Patient Kiosks & m devices (Pt check-in to streamline experience)2015 – Financial Screening, Automated Charity apps• Automated Physician Orders – legible/screened/ kick off!• PreClaim scrubber and new claims processing solution• New statements to better communicate bill, programs, even
coupons!

FUTURE STATE
• Kiosks in all areas• Scrubbing tool integrated with PFS• Patient Portal for test results/appts and
financial and clinical communications• Automated PreAuth• Work closely with Provider owned practices
to move processes even farther to the front of the patient experience• Physician liaison role to assist with the
physician office relationships• Automated phone calls to encourage pre-
processing

VENDOR SELECTION
vendor
39
vendor
Customer Support

COB SMART – WOW!

INCLUDE/EXCLUDE?(OUT OF POCKET OPTIONS)

DRILLING DEEPER INTO PRICING
• Use Historical Claims Data• Use CPT & ICD codes• Cross walk CPT to ICD• Combine Hospital & Physician liabilities• Consider specific physician and location• Establish high, average, low pricing• Adjust specific line items• Access readiness for ICD10 in
automated tool
Combined Estimates

I’ll splane our silver burger plan


ELIGIBILITY HIX RESPONSE

HOW CAN YOU DENY ME TODAY?
• Grace Period = claim denied? Claim paid?
• Collect from patient & refund later?
• If the deductible hasn’t been met can’t you collect payment anyway? It is not covered right?
• If the patient pays the premium…does this payment automatically trigger a payment to the hospital?
• Will the hospital have to track and monitor denials to rebill?
• How must administrative cost is there?

Benefit data
Contract Data
Cashiering Tools
Payment Estimate
HOW DO YOU MAKE THIS POSSIBLE?
Skills &
Patient
Satisfactio
n +
CHANGE
Financial Triage &
PIVAccurate Data & Denial
Prevention


Transparency Gone Wild!

50
SOMETIMES TRANSPARENCY IS WELL…
• Disclaimer verbiage• Communicate typical variances up front• Additional amount due vs. refund
Opague

WHY ESTIMATES HAVE TRANSPARENCY LIMITATIONS
• The user selected the wrong procedure• The wrong insurance code was selected and not
fixed before the estimate was run• A procedure was added on after the estimate• Not all of the same surgeries will be the same• Dealing with the unknown • Co-morbidities…..• Chargemaster updates • Contract updates• Benefits not always there• Co-insurance-moving target
04/20/23 51
GUESStimate

GUESSTIMATRON MAGIC

TRANSPARENCY NAVIGATOR

ESTIMATRON CLIFF NOTES

WHY PATIENTS CANNOT EASILY DO ESTIMATES?

CONSUMER FACING ESTIMATES

Key Components: (A-U-T-O-M-A-T-I-O-N)
•1. Screen: who should not be targeted for collections. Screen for bankruptcy, deceased, Medicaid & Commercial eligibility and charity eligibility.
•2. Segment: to prioritize inventory and produce optimal collection and treatment strategies.
•3. Route: assign accounts to the most appropriate role pre/post
WILDLY OPTIMIZING BEGINS AT THE VERY BEGINNING!

• 4. Performance Management: Real-time dashboards and to support and drive business decisions.
• 5. Collaboration, Consultation and Analytics: identify best practice collection strategies on going, evaluate reports for opportunities and anoint someone to oversee & champion process.
OPTIMIZATION

END GOAL
59
Healthy Happy Consumers A healthy Provider revenue cycle
04/20/23

WHAT OTHER KINDS OF WILD?
• Telemedicine
• Gamification applied to healthcare engagement (Let’s play a game…)
• Change your process to meet the needs for customers of all ages and tech savviness.
• Hospitals compete for patients by developing their expertise in niche markets. This could just be quality customer service, consumer friendly processes, and confidence in experiencing the latest technology in place right at the start.
• Servant Leader Management Style

TRY NEW THINGS! COLLABORATE WITH YOUR BUSINESS PARTNERS TO MANAGE THE NEW
MODELS
04/20/23 61Passport Health a Part of Experian

BE USER FRIENDLY & INTUITIVE.SHOW HEALTHCARE CONSUMERS
THE LOVE!
04/20/23 62
Wow…I can do this!
CHAM
Meaningful use: More than 50 percent of all unique patients online access to their health information.Precisely I.D. your patients and enroll in your Patient Portal!
500,000 known, verified fraud records
Transparency

EDUCATION / NAHAM/AFFILIATES
• Ham & Egg Breakfast
• The Chicken is invested
• The Pig is committed!
• Achieving Success comes at a price

Katherine H. Murphy, FHAM, CHAM, VP Revenue Cycle Consulting, Passport-a part of Experian
Congratulations and THANK YOU for another G--R-E-A-T CAHAM conference!
PATIENT ACCESS