Embed Size (px)
Citation preview
OPERATIVE RIB FIXATION AFTER BLUNT TRAUMA:
A PRACTICE MANAGEMENT GUIDELINE FROM EAST
George Kasotakis, MD MPH FACS Boston University School of Medicine
An Eastern Association for the Surgery of Trauma Practice Management Guideline (PMG)

Committee
Team Member Affiliation and expertise George Kasotakis, MD MPH Boston University, Trauma Surgery & SCC Louis Alarcon, MD Univ. of Pittsburgh, Trauma Surgery & SCC Patrick Bosarge, MD Univ. of Alabama, Trauma Surgery & SCC John J. Como, MD MPH Metro Health Medical Center, Trauma Surgery & SCC Erik A. Hasenboehler, MD Johns Hopkins Medicine, Orthopedic Surgery Elliott R. Haut, MD PhD Johns Hopkins Medicine, Trauma Surgery & SCC Joseph Love, DO Univ. of Texas at Houston, Trauma Surgery & SCC Mayur Patel, MD MPH Vanderbilt University, Trauma Surgery & SCC Nimitt Patel, MD Metro Health Medical Center, Trauma Surgery & SCC Erik Streib, MD Indiana University, Trauma Surgery & SCC
Conflict of Interest Disclosure
EAH is a paid consultant for DePuy Synthes Trauma.
Background • Thoracic trauma significant source of morbidity &
mortality – Directly associated with 25% of trauma-related mortality
– Indirectly associated with another 50%
• Chest wall trauma typically accompanies internal thoracic injuries – Range of severity
• Rib fx ORIF relatively new option that addresses chest wall-related morbidity
• Patients that benefit the most, and the outcomes that are improved the most not well characterized
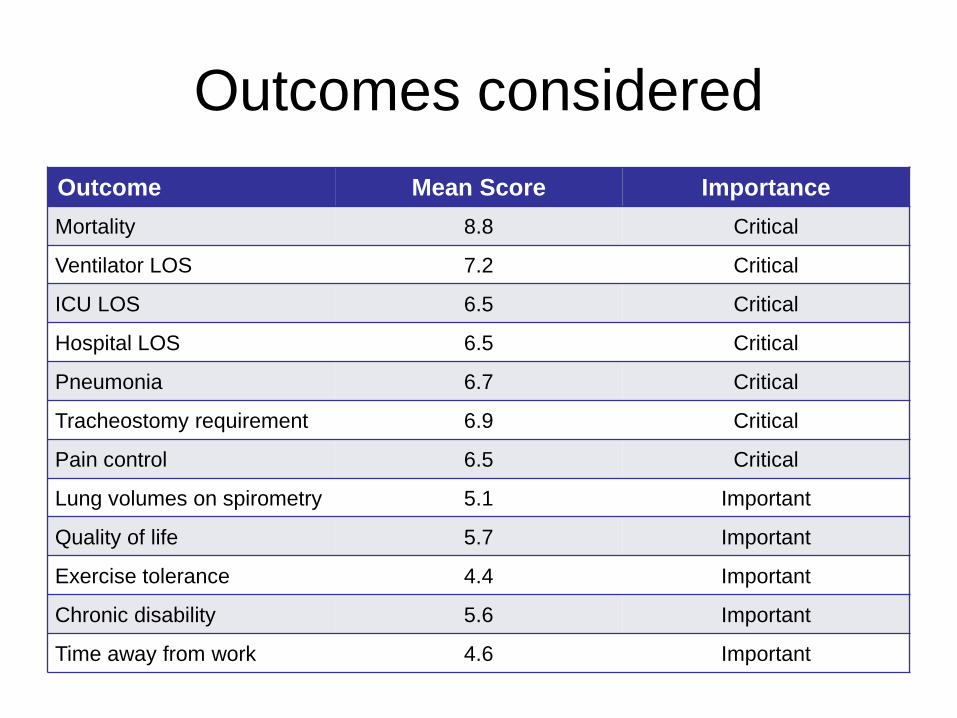
Outcomes considered Outcome Mean Score Importance Mortality 8.8 Critical
Ventilator LOS 7.2 Critical
ICU LOS 6.5 Critical
Hospital LOS 6.5 Critical
Pneumonia 6.7 Critical
Tracheostomy requirement 6.9 Critical
Pain control 6.5 Critical
Lung volumes on spirometry 5.1 Important
Quality of life 5.7 Important
Exercise tolerance 4.4 Important
Chronic disability 5.6 Important
Time away from work 4.6 Important
PICO Questions • PICO #1
– In adult patients with flail chest after blunt trauma (P), should rib ORIF be performed (I) (vs non-op mgt) (C) to improve mortality; shorten DMV, ICU LOS, and hospital LOS; decrease incidence of pneumonia and need for tracheostomy; and pain control (O)?
• PICO #2 – In adult patients with non-flail rib fractures after blunt trauma
(P), should rib ORIF (I) be performed (vs non-op mgt) (C) to improve mortality; shorten DMV, ICU LOS, and hospital LOS; decrease incidence of pneumonia and need for tracheostomy; and pain control (O)?
Methods
• Literature Review – PubMed, Embase, Cochrane
• Search Terms – (Rib fracture or flail chest) AND (surgical management/therapy/surgery
or fixation or plating or ORIF)
• Study Eligibility – Prospective, cohort & case-control studies
– Arms of rib ORIF vs non-op mgmt
– No language / year of publication restrictions
– Case reports, animal studies, reviews: excluded
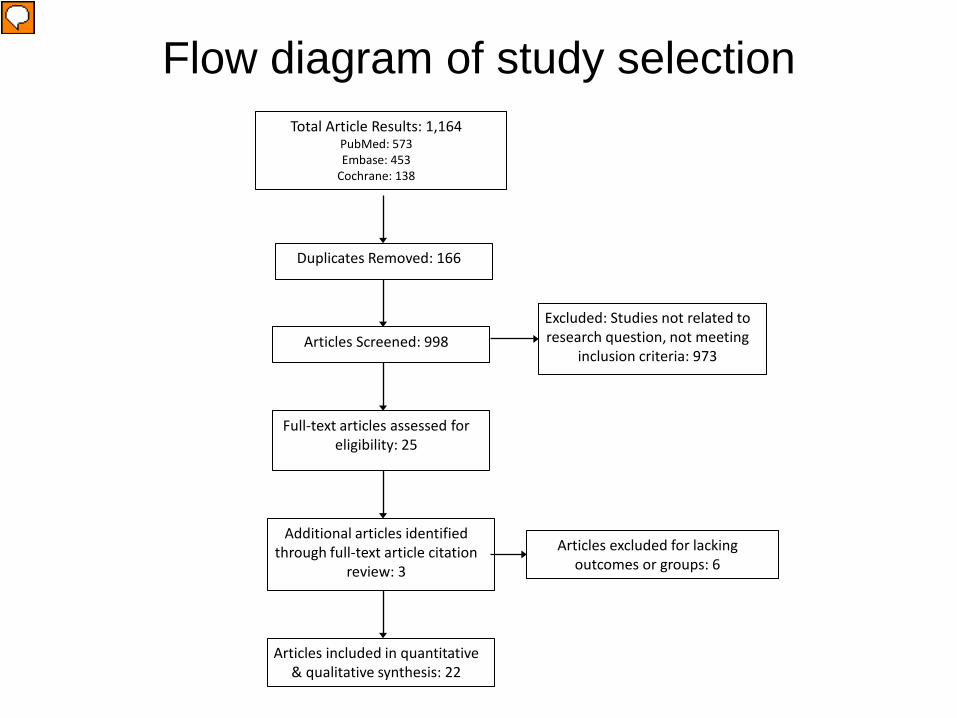
Flow diagram of study selection Total Article Results: 1,164
PubMed: 573 Embase: 453
Cochrane: 138
Duplicates Removed: 166
Articles Screened: 998
Full-text articles assessed for eligibility: 25
Additional articles identified through full-text article citation
review: 3
Articles included in quantitative & qualitative synthesis: 22
Excluded: Studies not related to research question, not meeting
inclusion criteria: 973
Articles excluded for lacking outcomes or groups: 6
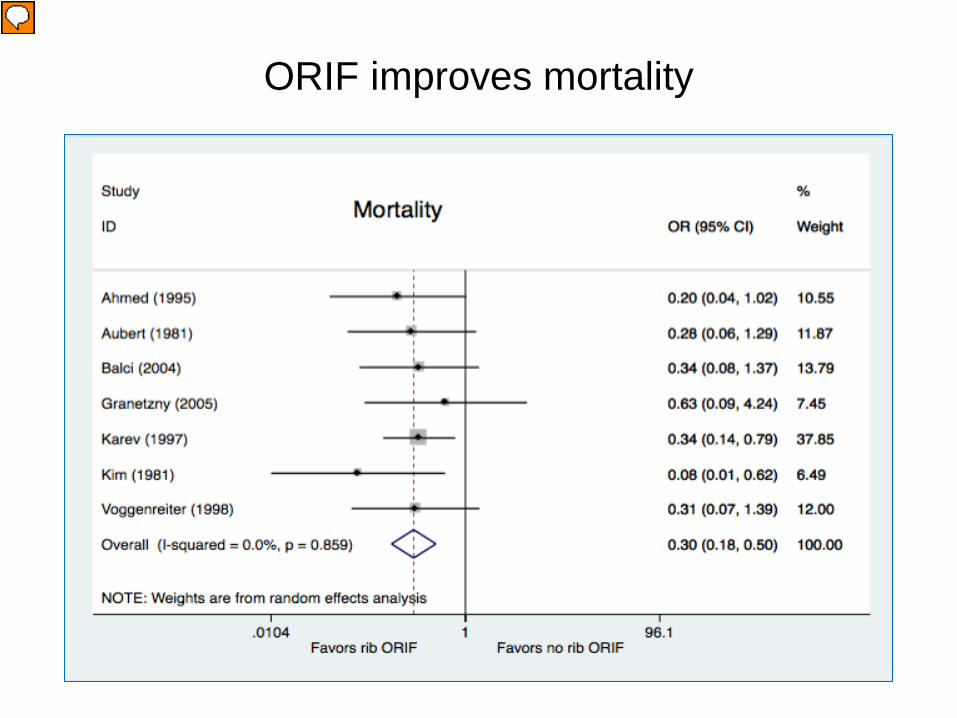
ORIF improves mortality
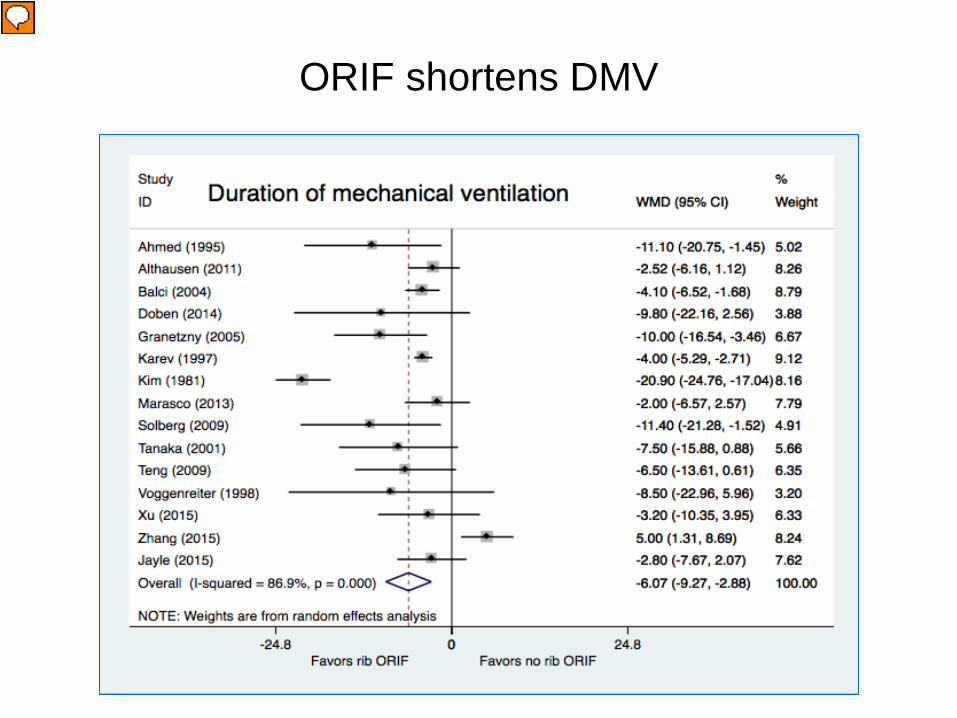
ORIF shortens DMV
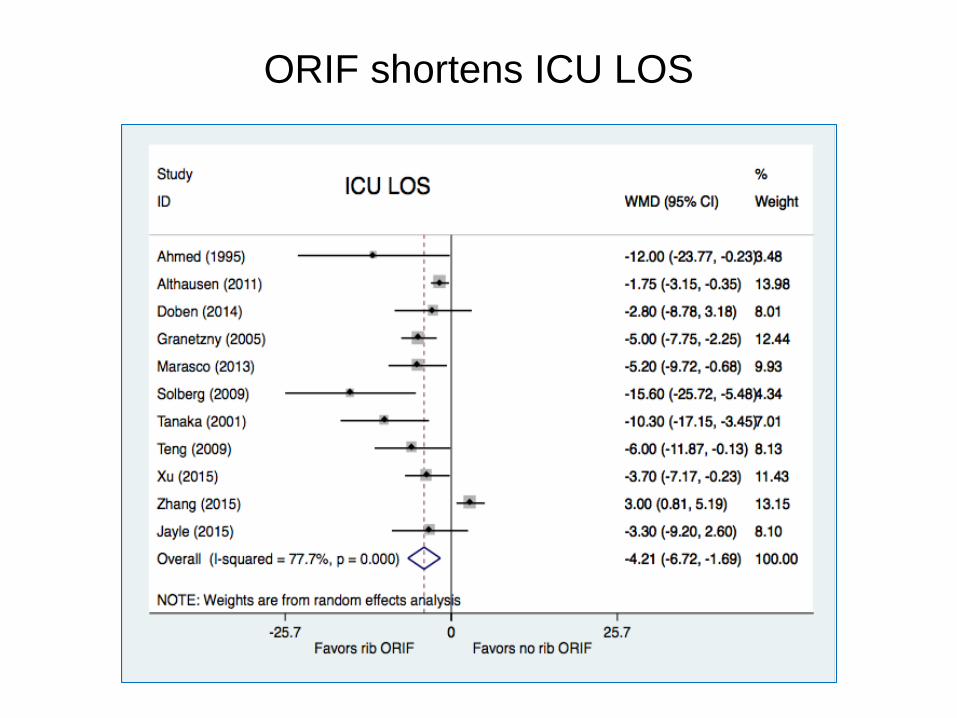
ORIF shortens ICU LOS
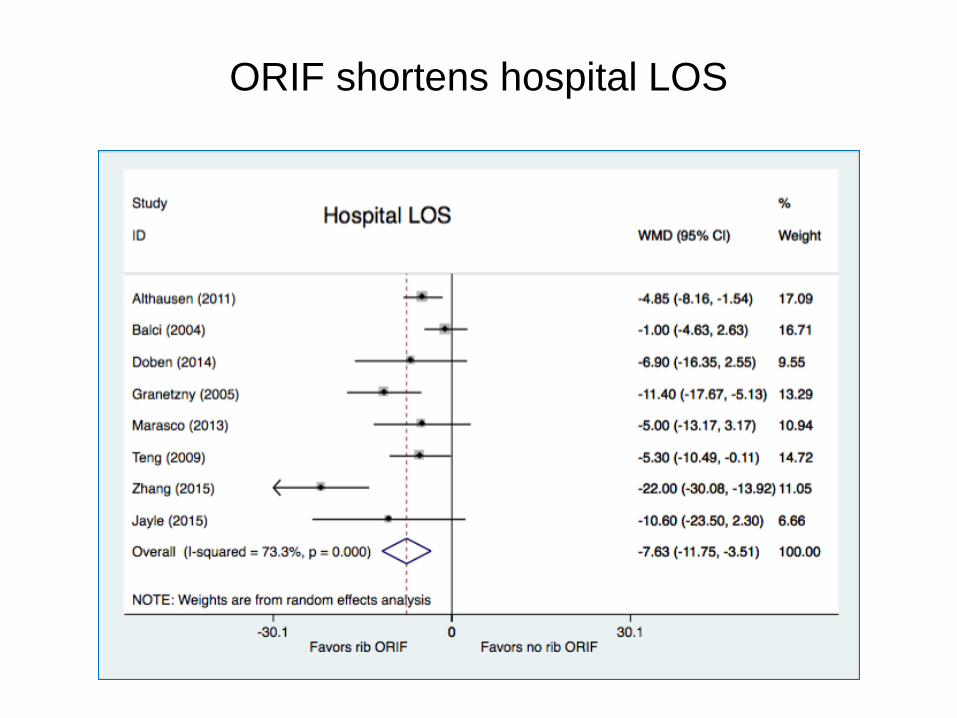
ORIF shortens hospital LOS
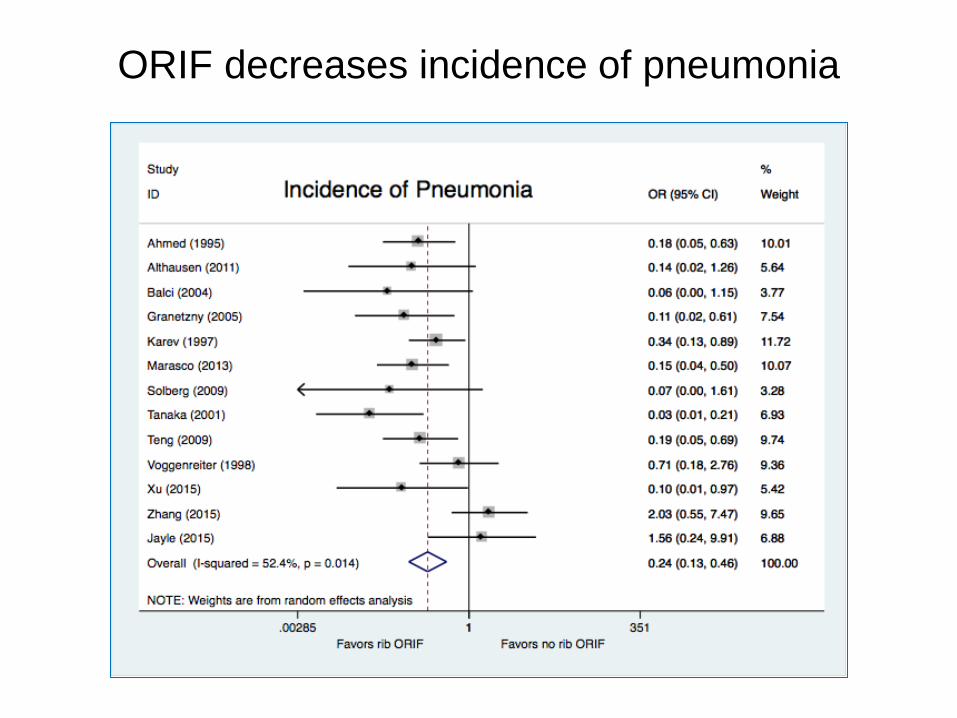
ORIF decreases incidence of pneumonia
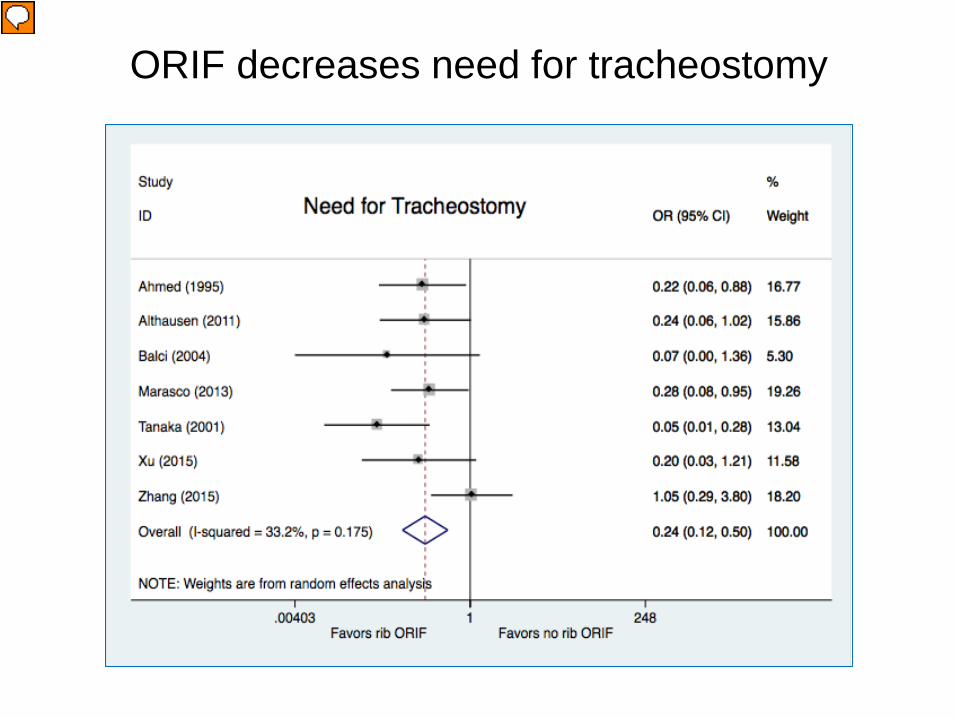
ORIF decreases need for tracheostomy
PICO #2
• No studies included only non-flail chest pts
• 5 studies included both flail & non-flail pts: – Nirula (2006): ORIF decreased DMV in pts requiring MV
– deMoya (2011): ORIF improved pain control
– Khandelwahl (2011) - ORIF improved pain control & allowed earlier return to activity
– Wu (2015): ORIF shortened ICU, hosp LOS, DMV; decreased pneumonia, need for tracheostomy
– Majercic (2015): ORIF shortened ICU LOS (& DMV, trach in non-TBI pts)
– Pieracci (2016): ORIF decreased DMV & need for tracheostomy
• No subgroup analyses in any of the above
Recommendations
PICO#1 – Flail chest:
• In adult patients with flail chest after blunt trauma, we conditionally recommend rib ORIF to decrease mortality; shorten duration of mechanical ventilation, ICU LOS and hospital LOS; incidence of pneumonia and need for tracheostomy.
• We cannot offer a recommendation for pain control with currently available evidence.
Additional Considerations in flail chest
• Rib ORIF should be undertaken early to maximize benefit. • Less pronounced benefit on DMV/ICU LOS if mod-severe
pulmonary contusions, or in those with other indications for prolonged ventilation.
• Most studies excluded patients with mod-severe TBI pts. • Most authors recommend ORIF of ribs 3-10. • A survival benefit cannot be consistently anticipated
(mortality benefit in <2004 studies)
Recommendations
PICO#2:
• In adult patients with non-flail rib fractures after blunt trauma, we cannot offer a recommendation for any of the outcomes with currently available evidence.
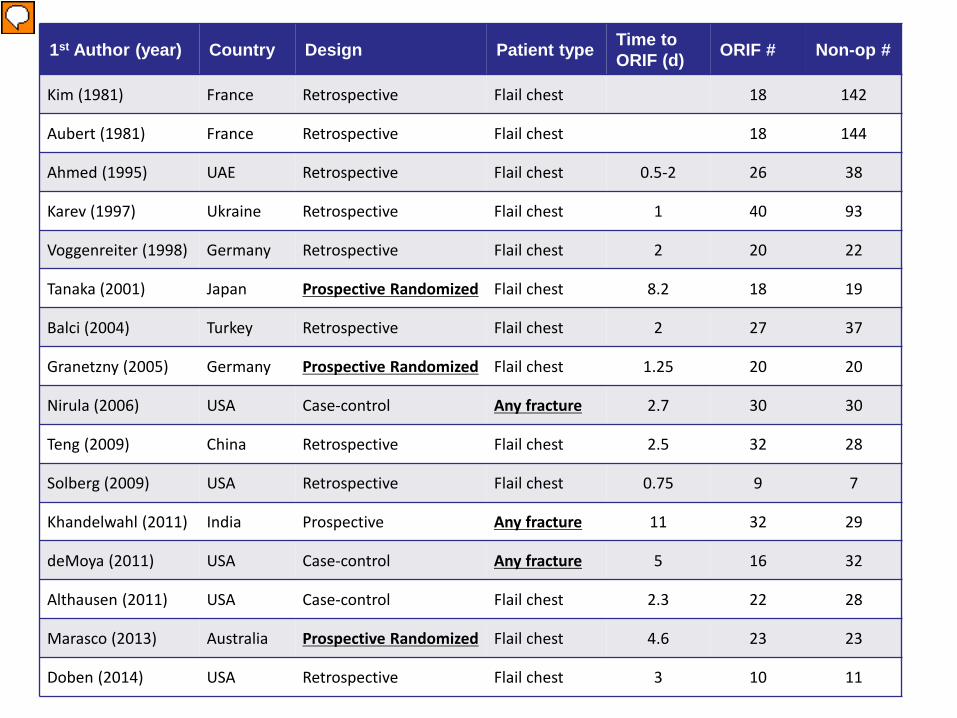
1st Author (year) Country Design Patient type Time to ORIF (d) ORIF # Non-op #
Kim (1981) France Retrospective Flail chest 18 142
Aubert (1981) France Retrospective Flail chest 18 144
Ahmed (1995) UAE Retrospective Flail chest 0.5-2 26 38
Karev (1997) Ukraine Retrospective Flail chest 1 40 93
Voggenreiter (1998) Germany Retrospective Flail chest 2 20 22
Tanaka (2001) Japan Prospective Randomized Flail chest 8.2 18 19
Balci (2004) Turkey Retrospective Flail chest 2 27 37
Granetzny (2005) Germany Prospective Randomized Flail chest 1.25 20 20
Nirula (2006) USA Case-control Any fracture 2.7 30 30
Teng (2009) China Retrospective Flail chest 2.5 32 28
Solberg (2009) USA Retrospective Flail chest 0.75 9 7
Khandelwahl (2011) India Prospective Any fracture 11 32 29
deMoya (2011) USA Case-control Any fracture 5 16 32
Althausen (2011) USA Case-control Flail chest 2.3 22 28
Marasco (2013) Australia Prospective Randomized Flail chest 4.6 23 23
Doben (2014) USA Retrospective Flail chest 3 10 11