Embed Size (px)
Citation preview
+
Anna Padoa, MD
Urogynecology Service
Dept of Ob & Gyn
Assaf Harofe Medical Center
Operative
Vaginal
Delivery and
Pelvic Floor
Trauma
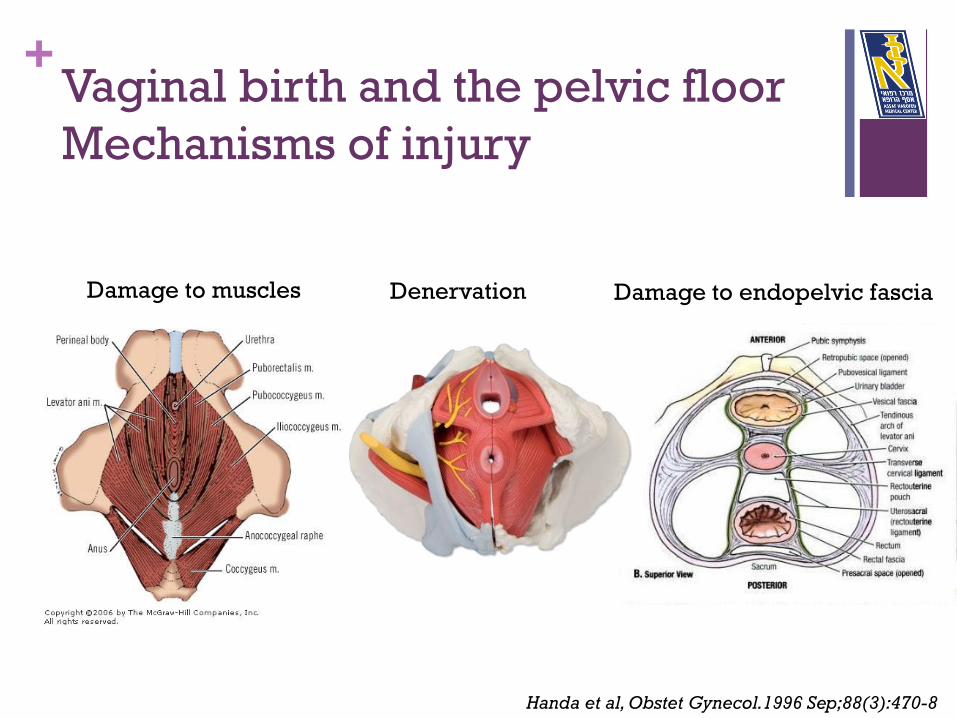
+ Vaginal birth and the pelvic floor
Mechanisms of injury
Damage to muscles Denervation Damage to endopelvic fascia
Handa et al, Obstet Gynecol.1996 Sep;88(3):470-8
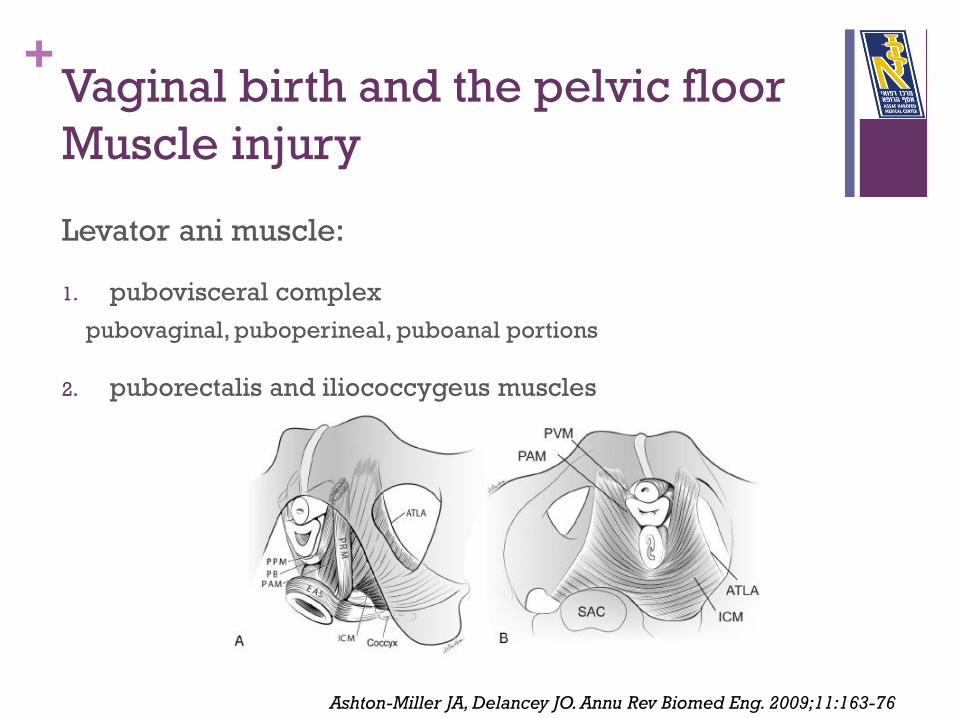
+ Vaginal birth and the pelvic floor
Muscle injury
Levator ani muscle:
1. pubovisceral complex
pubovaginal, puboperineal, puboanal portions
2. puborectalis and iliococcygeus muscles
Ashton-Miller JA, Delancey JO. Annu Rev Biomed Eng. 2009;11:163-76
+ Vaginal birth and the pelvic floor
Muscle injury
The load acting normal to the pelvic floor is approximately 37 N
in quiet standing and 19 N in the supine posture
During a maximum cough: peak load of 129 N
Straining at stool: 92 N
expulsive forces on the fetal head: 16 N at rest, 54 N during a
uterine contraction, and 120 N during a volitional push
Vacuum device: additional traction force of up to 113 N
Forceps: additional traction force can reach 200 N
Ashton-Miller JA, Delancey JO. Annu Rev Biomed Eng. 2009;11:163-76
+ Vaginal birth and the pelvic floor
Muscle injury
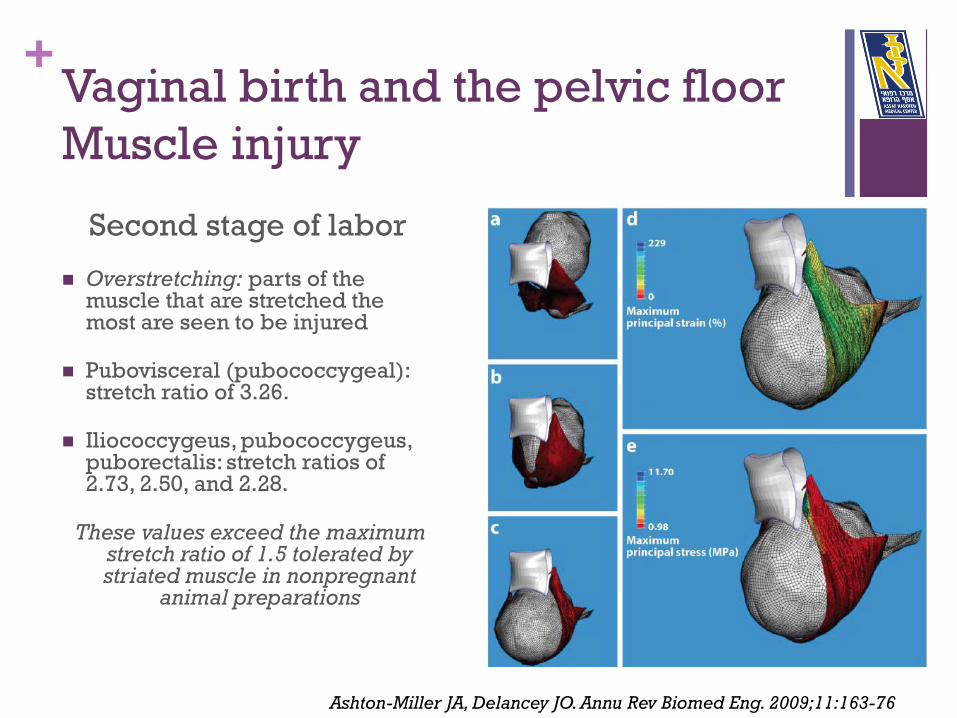
Second stage of labor
Overstretching: parts of the muscle that are stretched the most are seen to be injured
Pubovisceral (pubococcygeal): stretch ratio of 3.26.
Iliococcygeus, pubococcygeus, puborectalis: stretch ratios of 2.73, 2.50, and 2.28.
These values exceed the maximum stretch ratio of 1.5 tolerated by striated muscle in nonpregnant
animal preparations
Ashton-Miller JA, Delancey JO. Annu Rev Biomed Eng. 2009;11:163-76
+ Vaginal birth and the pelvic floor
Muscle injury
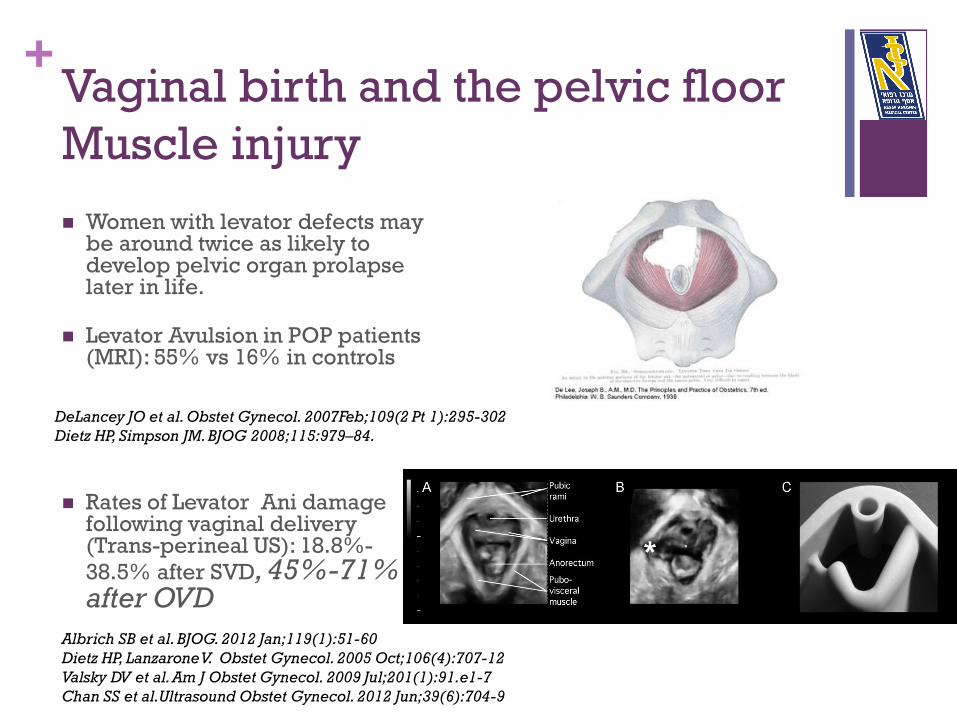
Women with levator defects may be around twice as likely to develop pelvic organ prolapse later in life.
Levator Avulsion in POP patients (MRI): 55% vs 16% in controls
Rates of Levator Ani damage following vaginal delivery (Trans-perineal US): 18.8%-
38.5% after SVD, 45%-71% after OVD
Albrich SB et al. BJOG. 2012 Jan;119(1):51-60
Dietz HP, Lanzarone V. Obstet Gynecol. 2005 Oct;106(4):707-12
Valsky DV et al. Am J Obstet Gynecol. 2009 Jul;201(1):91.e1-7
Chan SS et al.Ultrasound Obstet Gynecol. 2012 Jun;39(6):704-9
DeLancey JO et al. Obstet Gynecol. 2007Feb;109(2 Pt 1):295-302
Dietz HP, Simpson JM. BJOG 2008;115:979–84.
+ Vaginal birth and the pelvic floor
Muscle injury
When a passive muscle is stretched, its force depends on two
factors:
the strain rate
the product of the strain times the strain rate.
An order-of-magnitude increase in the strain rate can
increase the peak force by 25%.
Hence, a physician performing an instrumented delivery is
probably wise to keep the rate of pelvic muscle
stretch as low as possible by delivering the fetal
head as slowly as is reasonable
Ashton-Miller JA, Delancey JO. Annu Rev Biomed Eng. 2009;11:163-76
+ Vaginal birth and the pelvic floor
Nerve injury
PUDENDAL NERVE STRETCH DURING VAGINAL BIRTH:
the inferior rectal branch exhibited the maximum strain: 35%
which varied by 15% from least perineal descent to most perineal
descent
branches innervating the posterior labia and urethral sphincter
reached values of 15% and 13%
nerves innervating the anal sphincter are stretched beyond the 15%
strain threshold known to cause permanent damage in nonpregnant
appendicular nerve
Lien KC et al. Am J Obstet Gynecol. 2005May;192(5):1669-76
+ Vaginal birth and the pelvic floor
Endopelvic fascia
Isolated breaks in the endopelvic fascia: implicated in the
genesis of cystoceles, vaginal support defects and SUI.
After an acute injury new collagen is formed, which is never
as strong as the original connective tissue.
Following levator ani avulsion, loss of support exposes the
endopelvic fascia to gradual stretching and weakening
In a computerized model simulating vaginal delivery, Lepage
et al found the uterosacral ligaments to be submitted to
traction: for a medium-sized fetal head, uterosacral ligaments
undergo a deformation near 30 %
Lepage J et al.Int Urogynecol J. 2015 Apr;26(4):497-504.
+ Operative Vaginal Delivery and the
Pelvic Floor
Possible damage to pelvic floor function caused by operative
vaginal delivery:
1. Anal sphincter Disruption/ OASIS
2. Urinary Incontinence
3. Pelvic Organ Prolapse
+ Operative Vaginal Delivery and
anal incontinence
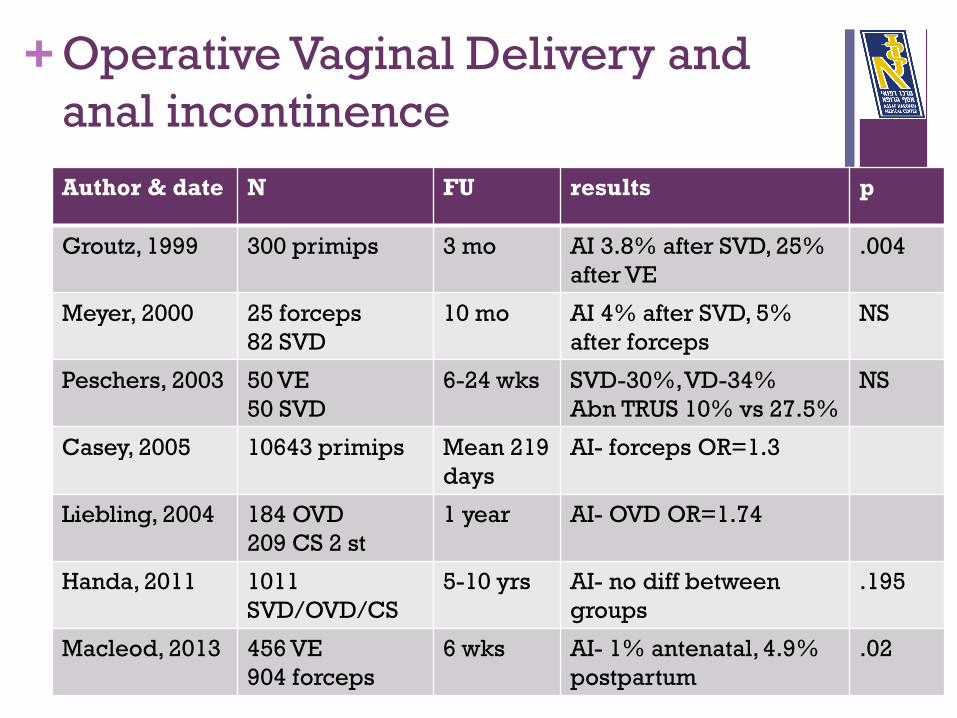
Author & date N FU results p
Groutz, 1999 300 primips 3 mo AI 3.8% after SVD, 25%
after VE
.004
Meyer, 2000 25 forceps
82 SVD
10 mo AI 4% after SVD, 5%
after forceps
NS
Peschers, 2003 50 VE
50 SVD
6-24 wks SVD-30%, VD-34%
Abn TRUS 10% vs 27.5%
NS
Casey, 2005 10643 primips Mean 219
days
AI- forceps OR=1.3
Liebling, 2004 184 OVD
209 CS 2 st
1 year AI- OVD OR=1.74
Handa, 2011 1011
SVD/OVD/CS
5-10 yrs AI- no diff between
groups
.195
Macleod, 2013 456 VE
904 forceps
6 wks AI- 1% antenatal, 4.9%
postpartum
.02
+ Operative Vaginal Delivery and
OASIS/ Anal incontinence
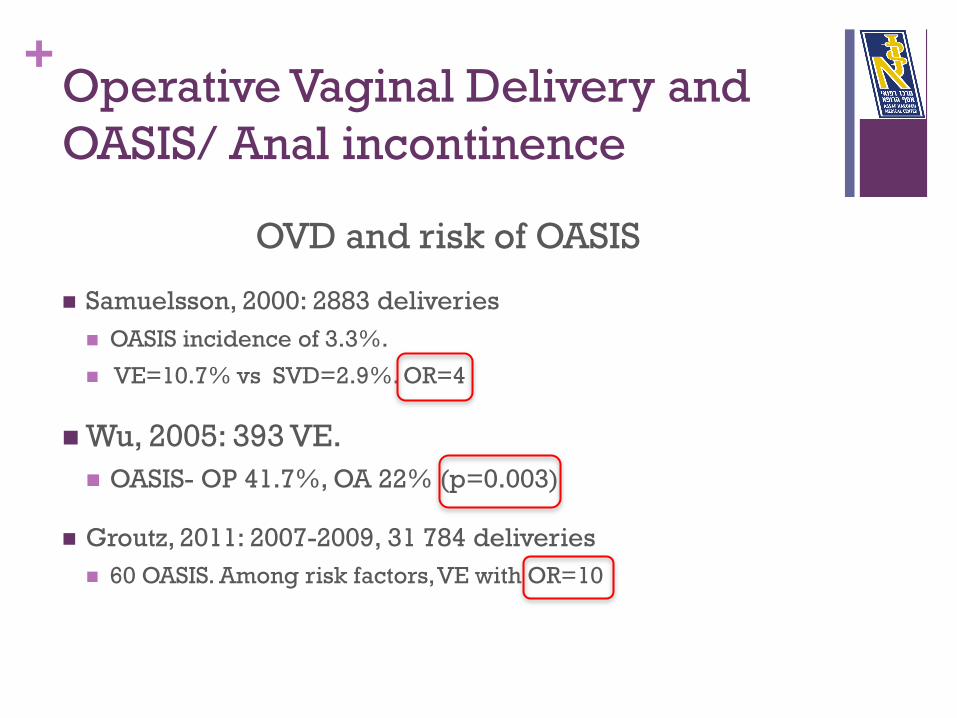
OVD and risk of OASIS
Samuelsson, 2000: 2883 deliveries
OASIS incidence of 3.3%.
VE=10.7% vs SVD=2.9%. OR=4
Wu, 2005: 393 VE.
OASIS- OP 41.7%, OA 22% (p=0.003)
Groutz, 2011: 2007-2009, 31 784 deliveries
60 OASIS. Among risk factors, VE with OR=10
+ Operative Vaginal Delivery and
OASIS/ Anal incontinence
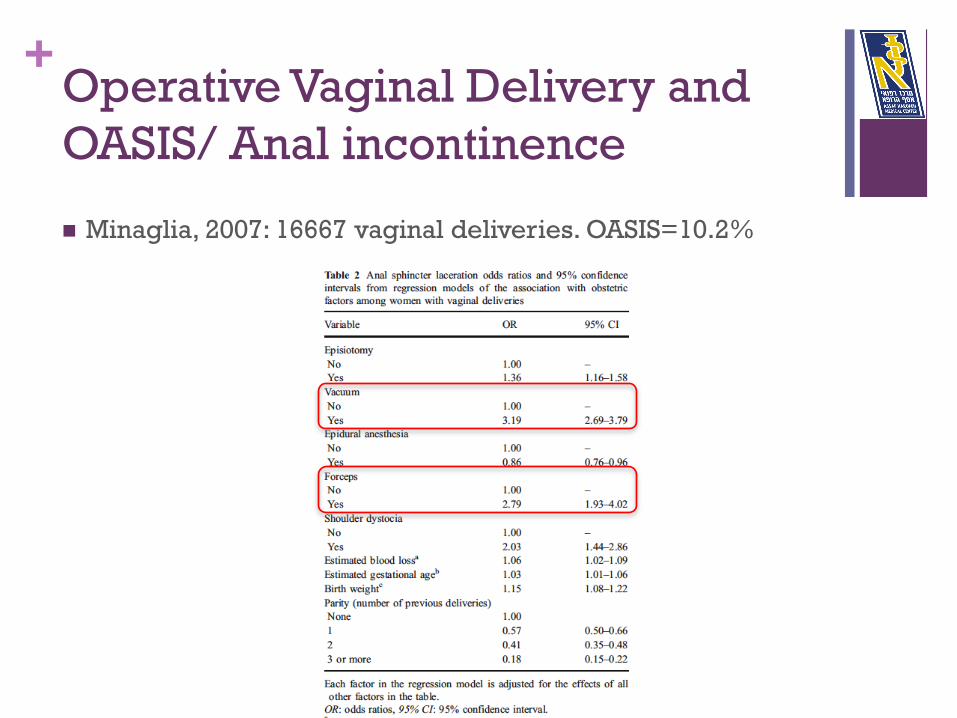
Minaglia, 2007: 16667 vaginal deliveries. OASIS=10.2%
+ Operative Vaginal Delivery and
OASIS/ Anal incontinence
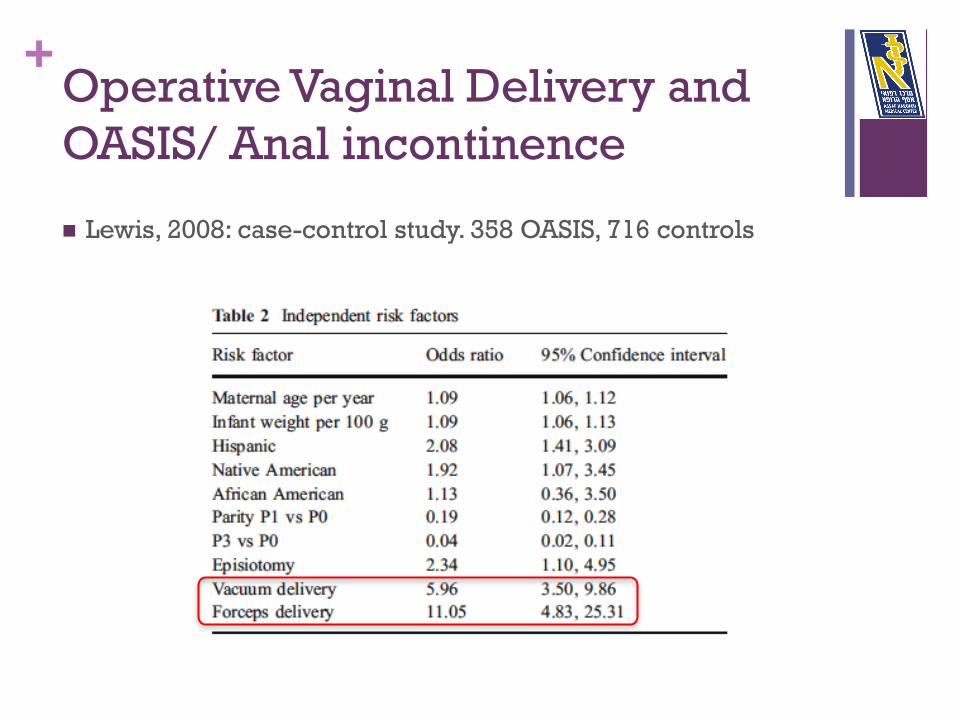
Lewis, 2008: case-control study. 358 OASIS, 716 controls
+ Operative Vaginal Delivery and
OASIS- VE vs forceps
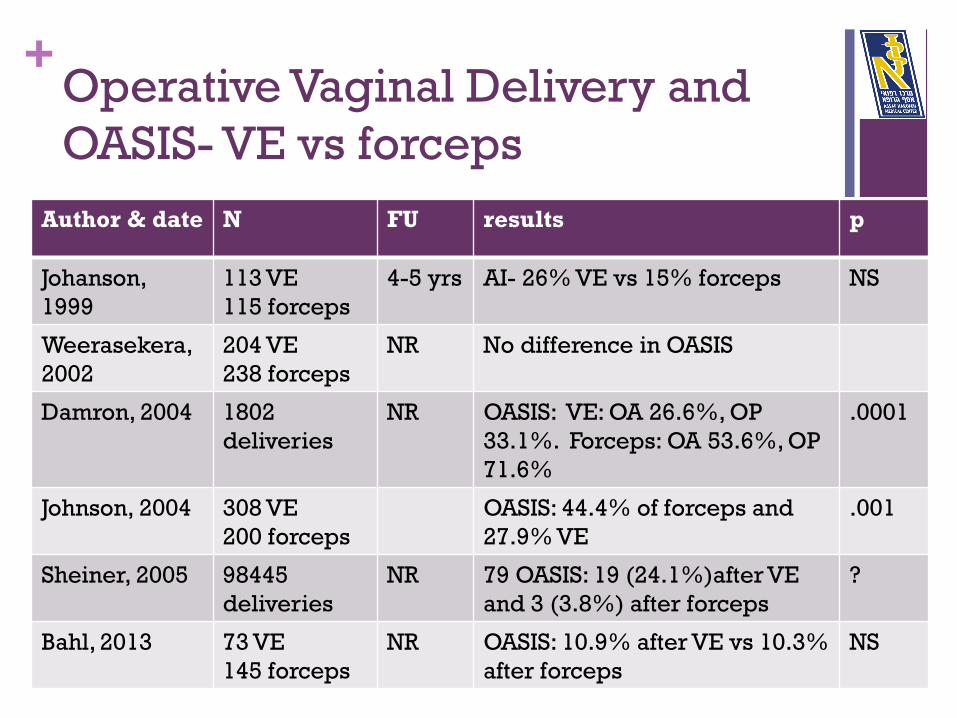
Author & date N FU results p
Johanson,
1999
113 VE
115 forceps
4-5 yrs AI- 26% VE vs 15% forceps NS
Weerasekera,
2002
204 VE
238 forceps
NR No difference in OASIS
Damron, 2004 1802
deliveries
NR OASIS: VE: OA 26.6%, OP
33.1%. Forceps: OA 53.6%, OP
71.6%
.0001
Johnson, 2004 308 VE
200 forceps
OASIS: 44.4% of forceps and
27.9% VE
.001
Sheiner, 2005 98445
deliveries
NR 79 OASIS: 19 (24.1%)after VE
and 3 (3.8%) after forceps
?
Bahl, 2013 73 VE
145 forceps
NR OASIS: 10.9% after VE vs 10.3%
after forceps
NS
+ Operative Vaginal Delivery and
OASIS/ Anal incontinence
Sequential Instruments (forceps>>VE) and OASIS
De Leeuw, 2001: Dutch national registry 1994-1995. 238,503
SVD and 46,280 OVD. Overall risk: 1.94%.
OR: fundal pressure 1.23, FP+VE 1.64, FP+forceps 3.04, VE
1.79, forceps 2.73, VE+forceps 4.58
Murphy, 2011: 1360 primiparae.
Sequential use of instruments: greater maternal morbidity than
single instrument use (anal sphincter tear 17.4% versus 8.4%,
adjusted OR 2.1, 95% CI 1.2–3.3)
+ Operative Vaginal Delivery, OASIS
and episiotomy
Author & date N FU results p
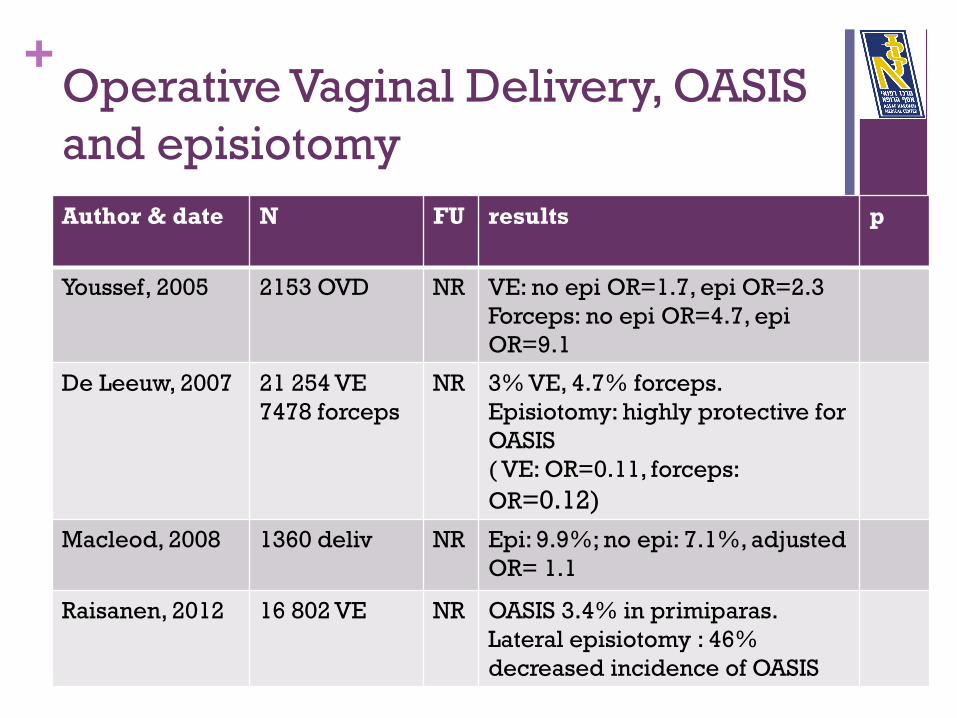
Youssef, 2005 2153 OVD NR VE: no epi OR=1.7, epi OR=2.3
Forceps: no epi OR=4.7, epi
OR=9.1
De Leeuw, 2007 21 254 VE
7478 forceps
NR 3% VE, 4.7% forceps.
Episiotomy: highly protective for
OASIS
( VE: OR=0.11, forceps:
OR=0.12)
Macleod, 2008 1360 deliv NR Epi: 9.9%; no epi: 7.1%, adjusted
OR= 1.1
Raisanen, 2012 16 802 VE NR OASIS 3.4% in primiparas.
Lateral episiotomy : 46%
decreased incidence of OASIS
+ Operative Vaginal Delivery, OASIS
and episiotomy
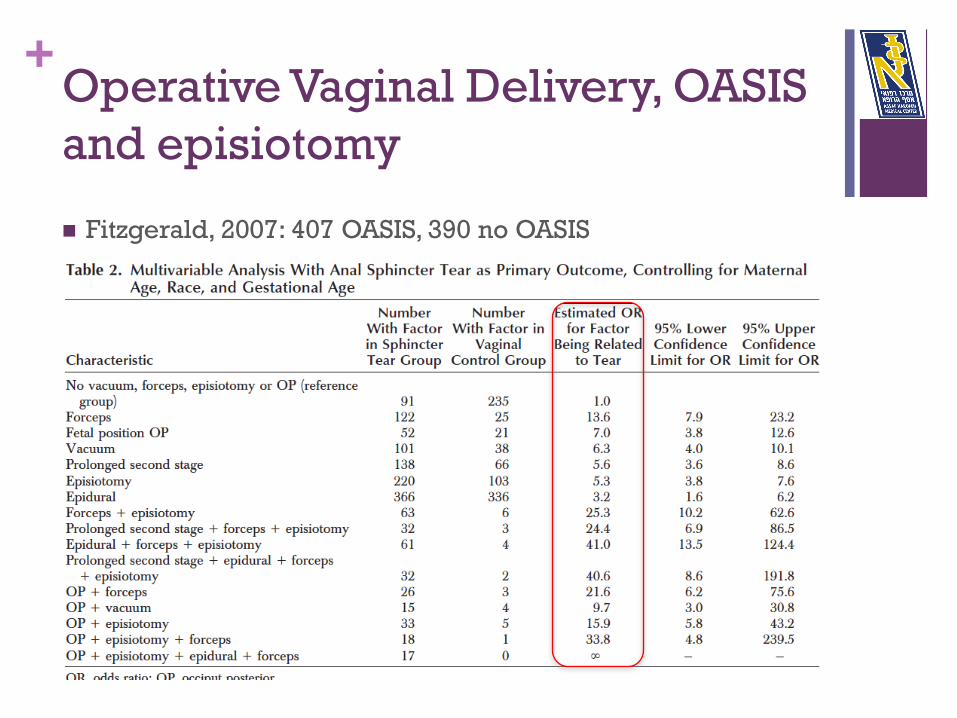
Fitzgerald, 2007: 407 OASIS, 390 no OASIS
+ Operative Vaginal Delivery, OASIS
and episiotomy
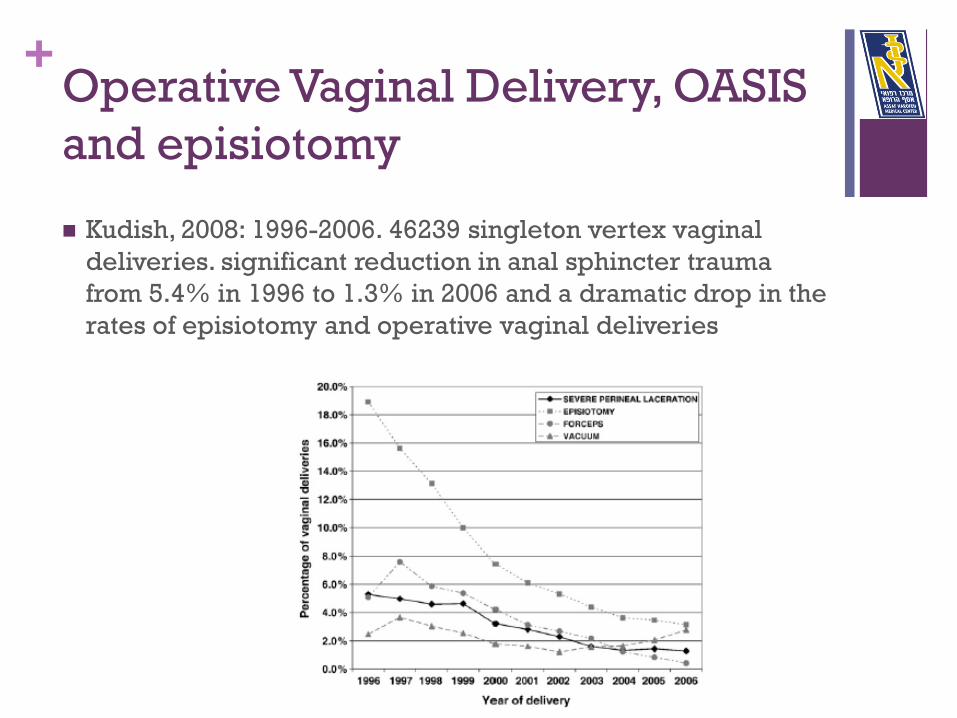
Kudish, 2008: 1996-2006. 46239 singleton vertex vaginal
deliveries. significant reduction in anal sphincter trauma
from 5.4% in 1996 to 1.3% in 2006 and a dramatic drop in the
rates of episiotomy and operative vaginal deliveries
+ Operative Vaginal Delivery is a
risk factor for LUTS
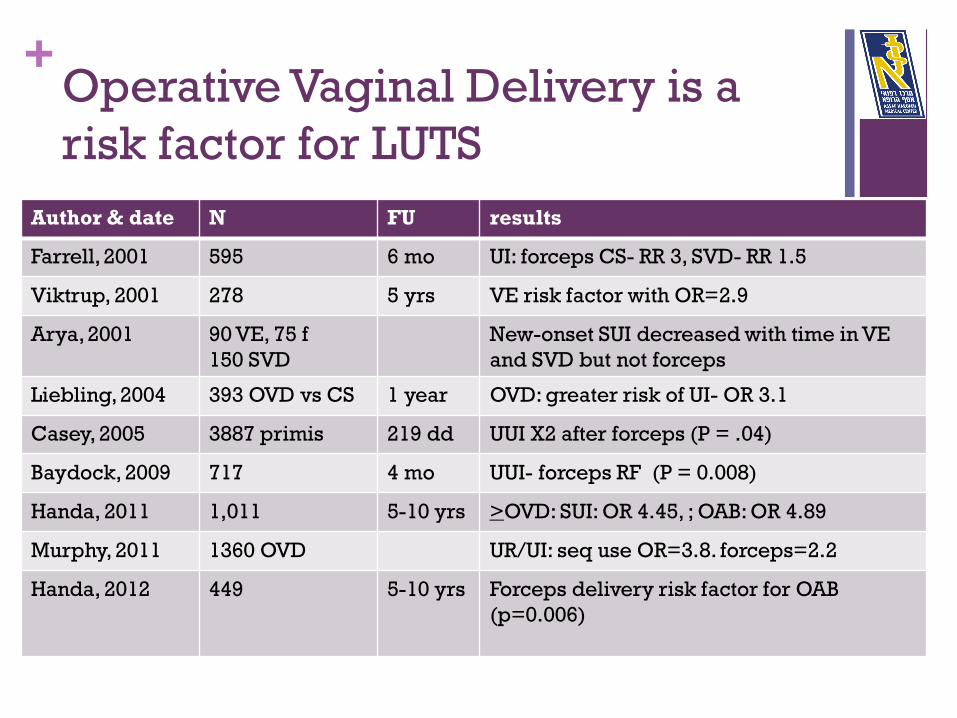
Author & date N FU results
Farrell, 2001 595 6 mo UI: forceps CS- RR 3, SVD- RR 1.5
Viktrup, 2001 278 5 yrs VE risk factor with OR=2.9
Arya, 2001 90 VE, 75 f
150 SVD
New-onset SUI decreased with time in VE
and SVD but not forceps
Liebling, 2004 393 OVD vs CS 1 year OVD: greater risk of UI- OR 3.1
Casey, 2005 3887 primis 219 dd UUI X2 after forceps (P = .04)
Baydock, 2009 717 4 mo UUI- forceps RF (P = 0.008)
Handa, 2011 1,011 5-10 yrs >OVD: SUI: OR 4.45, ; OAB: OR 4.89
Murphy, 2011 1360 OVD UR/UI: seq use OR=3.8. forceps=2.2
Handa, 2012 449 5-10 yrs Forceps delivery risk factor for OAB
(p=0.006)
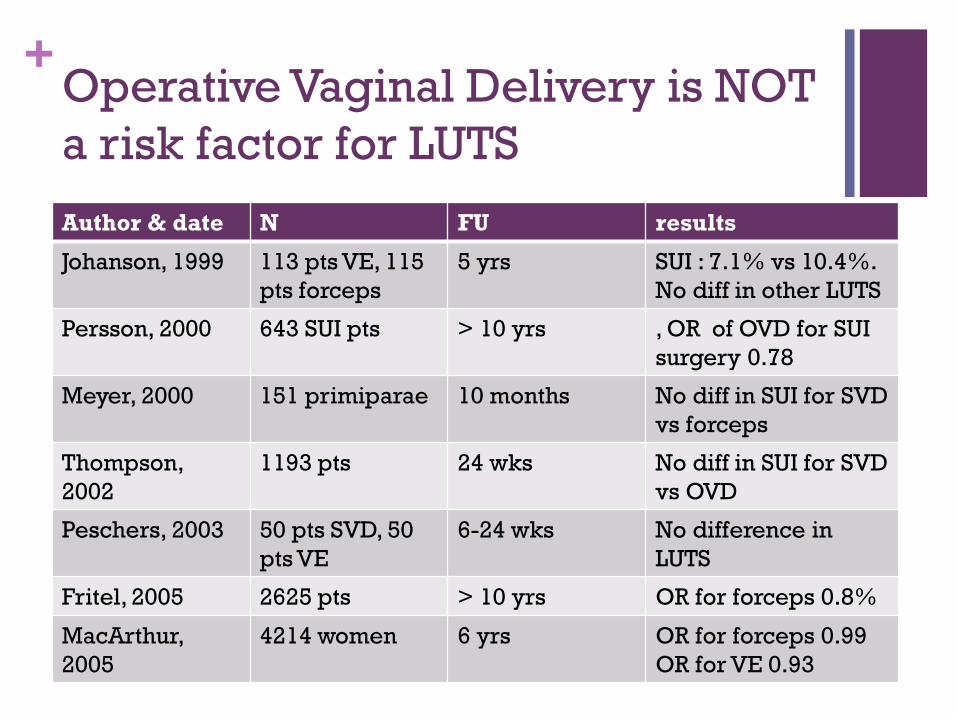
+ Operative Vaginal Delivery is NOT
a risk factor for LUTS
Author & date N FU results
Johanson, 1999 113 pts VE, 115
pts forceps
5 yrs SUI : 7.1% vs 10.4%.
No diff in other LUTS
Persson, 2000 643 SUI pts > 10 yrs , OR of OVD for SUI
surgery 0.78
Meyer, 2000 151 primiparae 10 months No diff in SUI for SVD
vs forceps
Thompson,
2002
1193 pts 24 wks No diff in SUI for SVD
vs OVD
Peschers, 2003 50 pts SVD, 50
pts VE
6-24 wks No difference in
LUTS
Fritel, 2005 2625 pts > 10 yrs OR for forceps 0.8%
MacArthur,
2005
4214 women 6 yrs OR for forceps 0.99
OR for VE 0.93
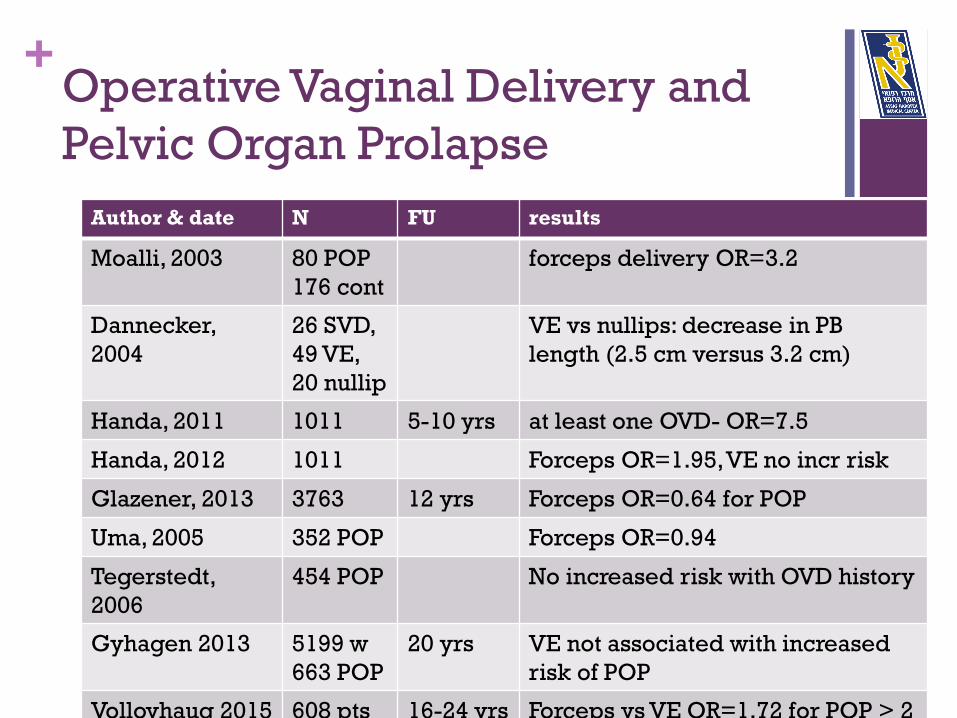
+ Operative Vaginal Delivery and
Pelvic Organ Prolapse
Author & date N FU results
Moalli, 2003 80 POP
176 cont
forceps delivery OR=3.2
Dannecker,
2004
26 SVD,
49 VE,
20 nullip
VE vs nullips: decrease in PB
length (2.5 cm versus 3.2 cm)
Handa, 2011 1011 5-10 yrs at least one OVD- OR=7.5
Handa, 2012 1011 Forceps OR=1.95, VE no incr risk
Glazener, 2013 3763 12 yrs Forceps OR=0.64 for POP
Uma, 2005 352 POP Forceps OR=0.94
Tegerstedt,
2006
454 POP No increased risk with OVD history
Gyhagen 2013 5199 w
663 POP
20 yrs VE not associated with increased
risk of POP
Volloyhaug 2015 608 pts 16-24 yrs Forceps vs VE OR=1.72 for POP > 2
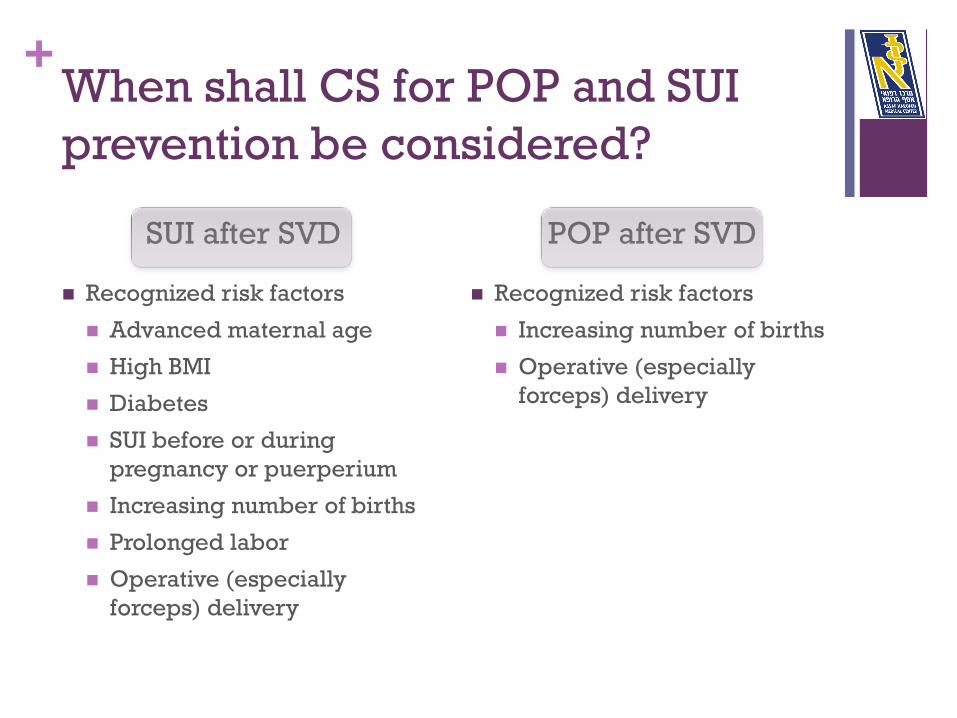
+ When shall CS for POP and SUI
prevention be considered?
SUI after SVD
Recognized risk factors
Advanced maternal age
High BMI
Diabetes
SUI before or during
pregnancy or puerperium
Increasing number of births
Prolonged labor
Operative (especially
forceps) delivery
POP after SVD
Recognized risk factors
Increasing number of births
Operative (especially
forceps) delivery

+
Thank you for your continence!
















![Pelvic floor muscle training versus no treatment, or inactive … - 2010.pdf · 2012. 11. 28. · [Intervention Review] Pelvic floor muscle training versus no treatment, or inactive](https://img.pdfslide.net/doc/110x75/5fcc55cc5a78f165476e42b3/pelvic-floor-muscle-training-versus-no-treatment-or-inactive-2010pdf-2012.jpg)












