Embed Size (px)
Citation preview
Paul C. Coelho, MD Board Certified PM&R
Subspecialty Certified Pain Medicine
Opioid Risk Stratification: Identifying The Central Pain
Phenotype
Disclosures
Paul Coelho,MD: No financial relationships to disclose. I will not be discussing any off-label use.
Table Of Contents
1. Traditional Opioid Risk Stratification Tools 2. Musculoskeletal Pain Phenotypes 3. Tools to Identify the Central Pain/Central Sensitivity (CS) Phenotype 4. Pain Phenotyping As A Proxy For Risk Stratification 5. Treatment of Central Sensitivity 6. Sample Case
CDC Guidelines Recommend Opioid Risk Stratification
https://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm

Traditional Opioid Risk Stratification Instruments
http://www.opioidrisk.com/node/774
1. ORT: Opioid Risk Tool 2. DIRE: Diagnosis, Intractability, Risk, Efficacy 3. SOAPP-R: Screener & Opioid Risk
Assessment for Patients in Pain 4. SISAP: Screening Instrument for Substance
Abuse Potential
Risk Stratification Instruments Fail
http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm
“Unfortunately the predictive utility for predicting opioid misuse was inconsistent and poor for the ORT, SOAPP-R, and SOAPP version 1. Usually the instruments performed better in the initial study and more poorly when someone else tried to validate it. A couple of recent studies have also looked at a new instrument called the Brief Risk Instrument which also did not perform very well. The DIRE and the SISAP have not been evaluated in terms of predictive utility (at least not in studies that met our inclusion criteria).”
Roger Chou
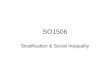
Identifying Musculoskeletal Pain Phenotypes

MSK Pain PhenotypesNociceptive Neuropathic Central
Primarily due to inflammation or mechanical damage in periphery.
Damage or entrapment of peripheral nerves.
Primarily due to a central disturbance in pain processing.
NSAID, Opioid Responsive
Responds to both peripheral and central pharmacological therapy.
Responsive to Tricyclic Compounds. Opioid effectiveness questioned
Responds to procedures Does not respond to procedures
Does not respond to procedures
Behavioral factors minor. Behavioral factors minor. Behavioral factors more prominent.
Examples: Osteoarthritis, Rheumatoid Arthritis, Cancer Pain
Examples: Diabetic neuropathy, Post-herpetic neuralgia.
Examples: FMS, IBS, Tension HA, idiopathic LBP
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1829161/
Central Pain (CS) Is Not Opioid Responsive
http://www.ncbi.nlm.nih.gov/pubmed/26975749
American Pain Society American Academy of Pain Medicine American Academy of Neurology European League Against Rheumatism Canadian Pain Society Canadian Rheumatology Association British Pain Society
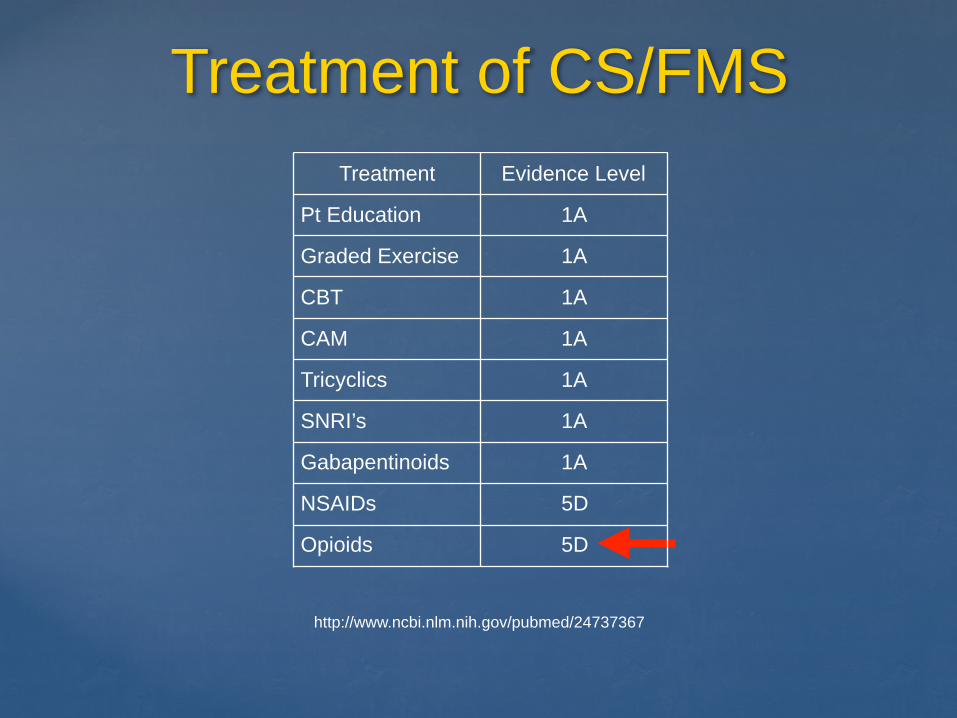
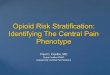
Treatment of CS/FMS
http://www.ncbi.nlm.nih.gov/pubmed/24737367
Treatment Evidence Level
Pt Education 1A
Graded Exercise 1A
CBT 1A
CAM 1A
Tricyclics 1A
SNRI’s 1A
Gabapentinoids 1A
NSAIDs 5D
Opioids 5D
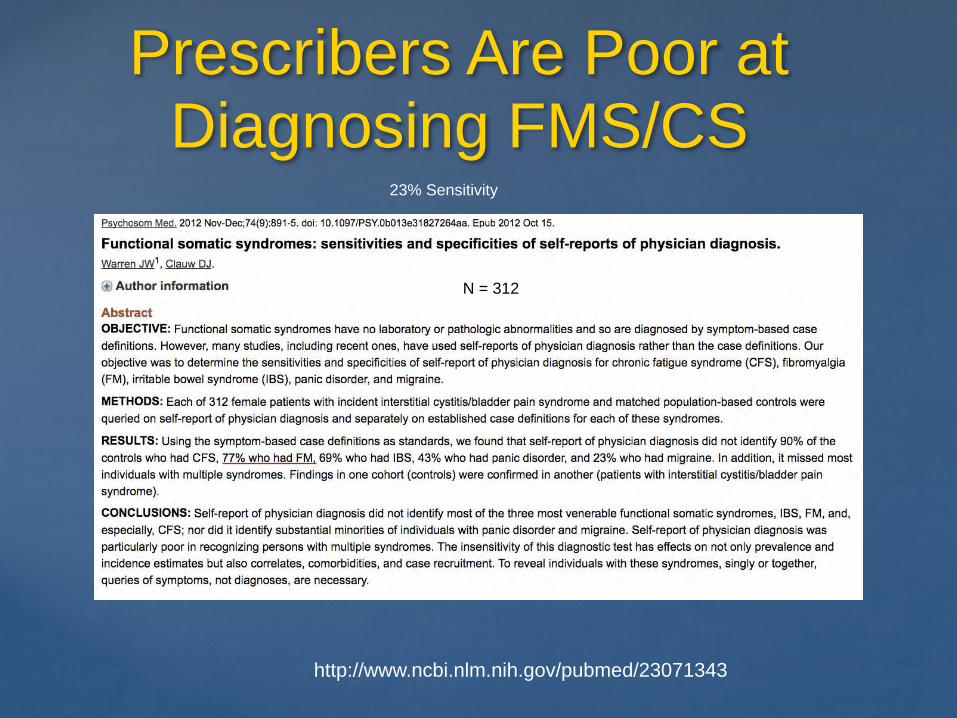
Prescribers Are Poor at Diagnosing FMS/CS
http://www.ncbi.nlm.nih.gov/pubmed/23071343
23% Sensitivity
N = 312
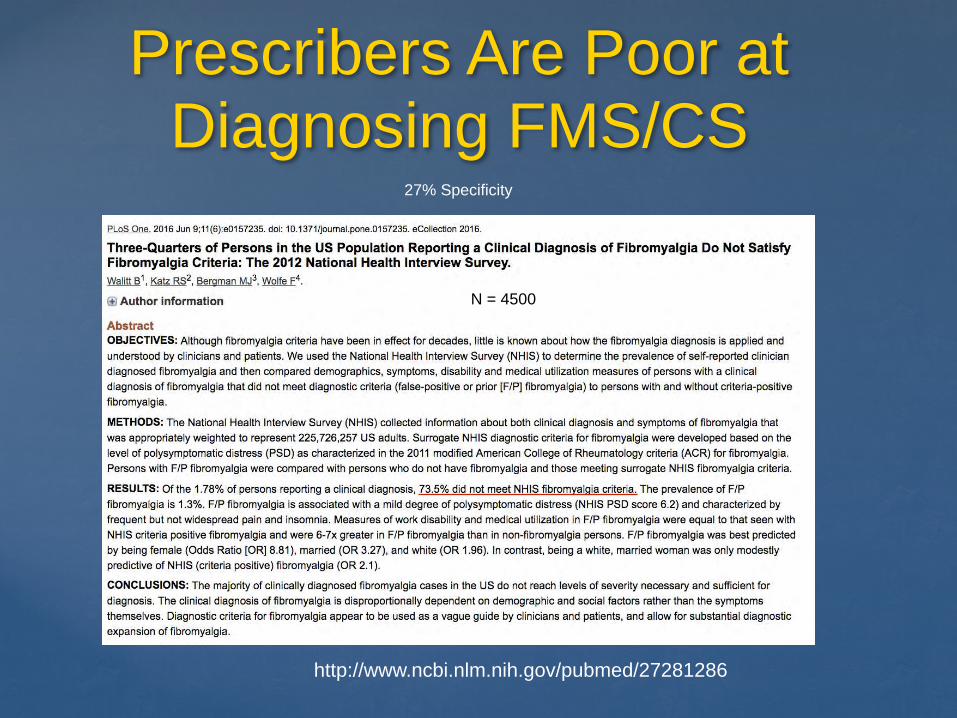
Prescribers Are Poor at Diagnosing FMS/CS
http://www.ncbi.nlm.nih.gov/pubmed/27281286
27% Specificity
N = 4500
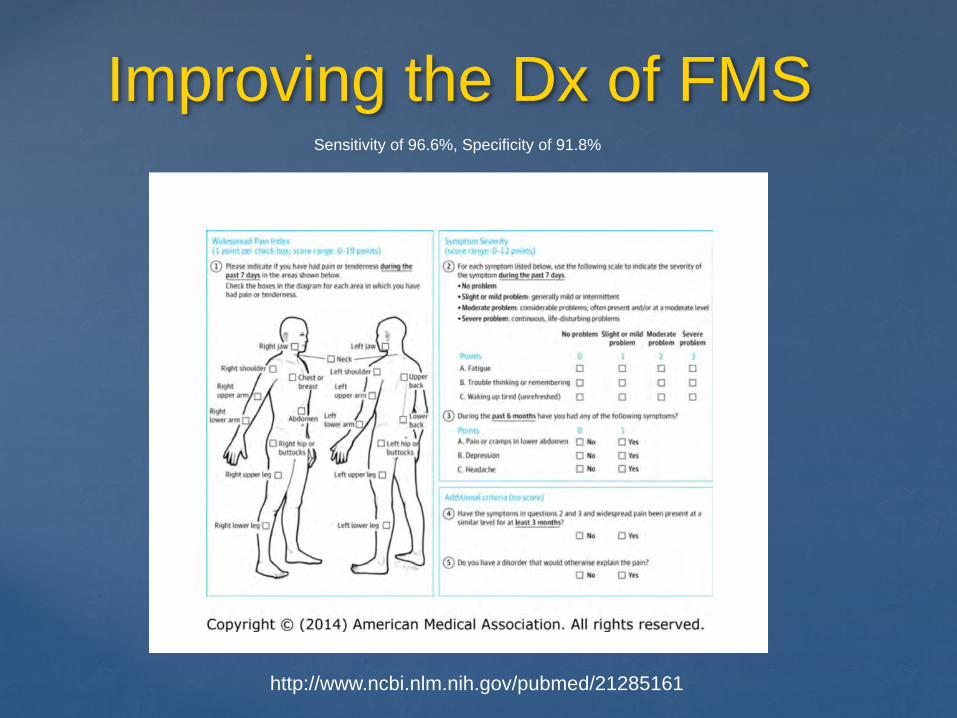
Improving the Dx of FMS
http://www.ncbi.nlm.nih.gov/pubmed/21285161
Sensitivity of 96.6%, Specificity of 91.8%
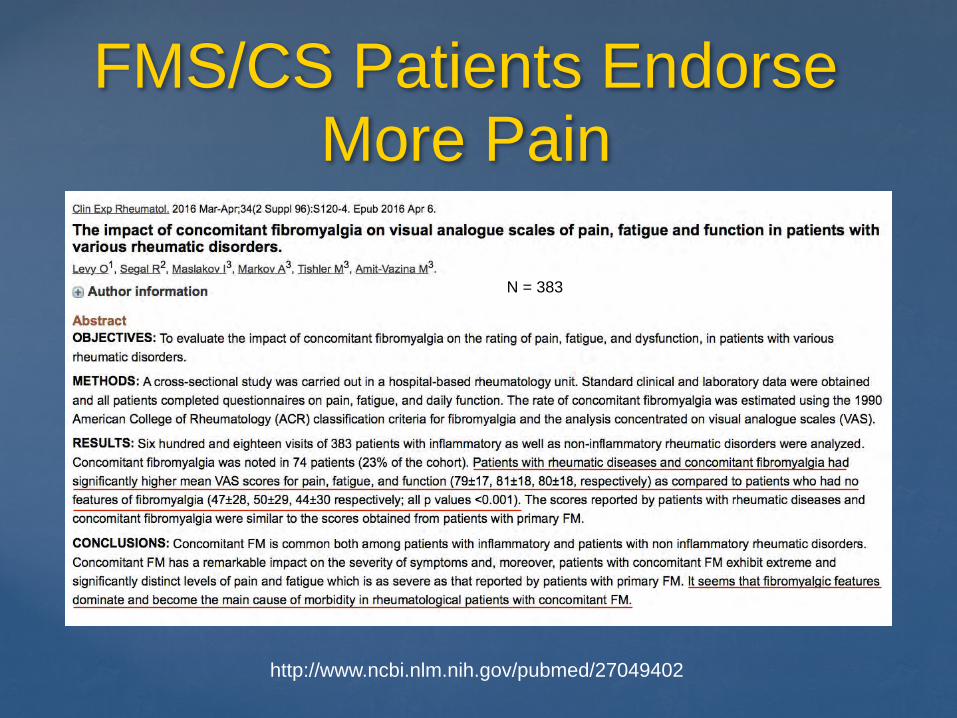
FMS/CS Patients Endorse More Pain
http://www.ncbi.nlm.nih.gov/pubmed/27049402
N = 383
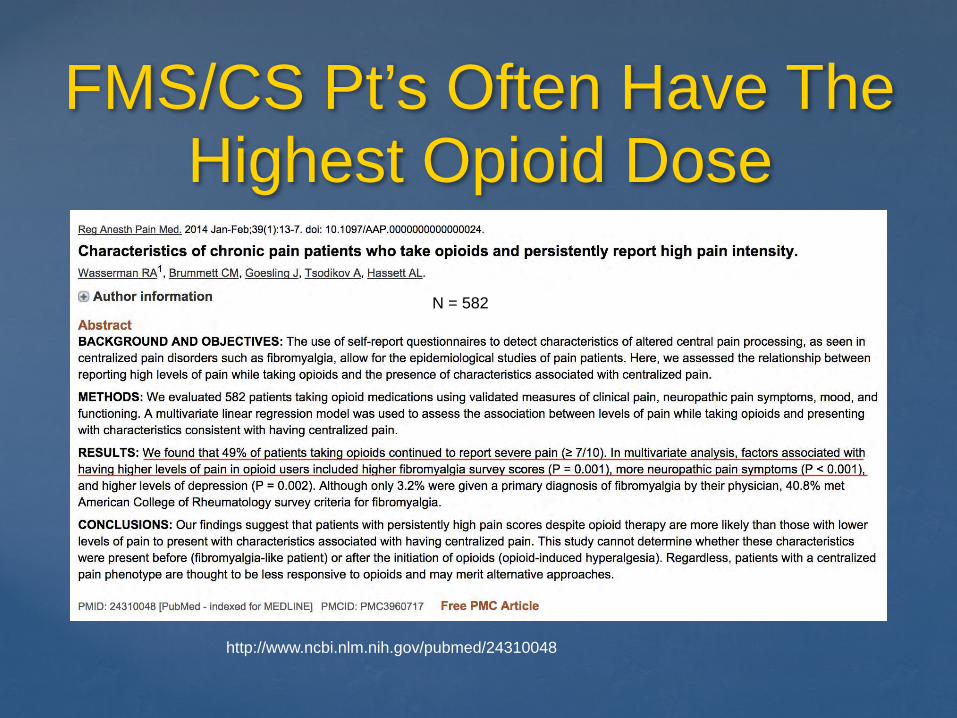
FMS/CS Pt’s Often Have The Highest Opioid Dose
http://www.ncbi.nlm.nih.gov/pubmed/24310048
N = 582
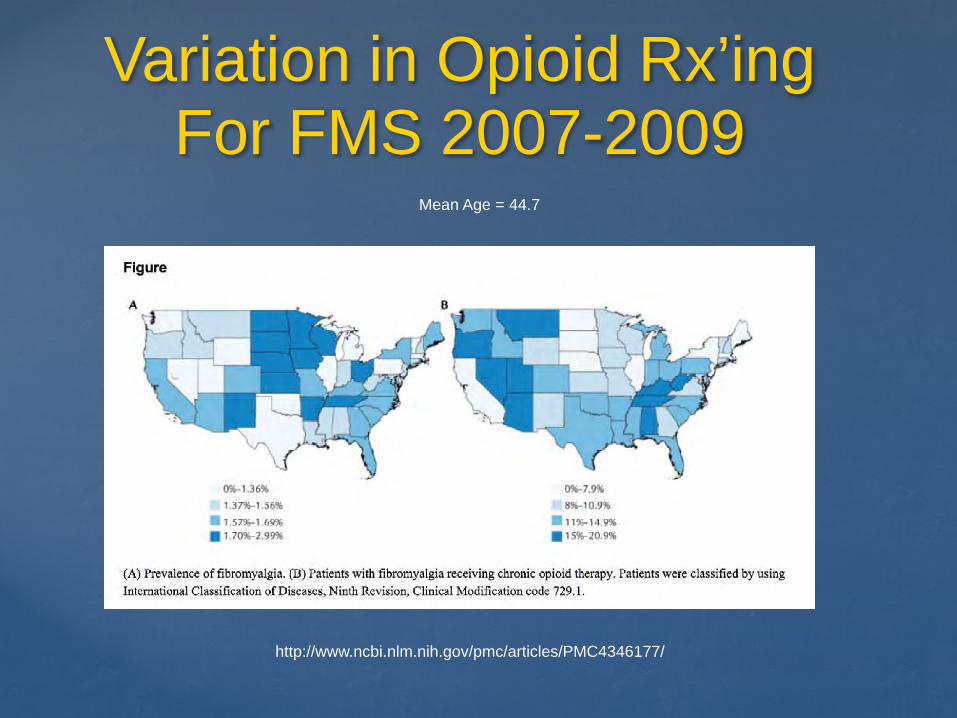
Variation in Opioid Rx’ing For FMS 2007-2009
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4346177/
Mean Age = 44.7
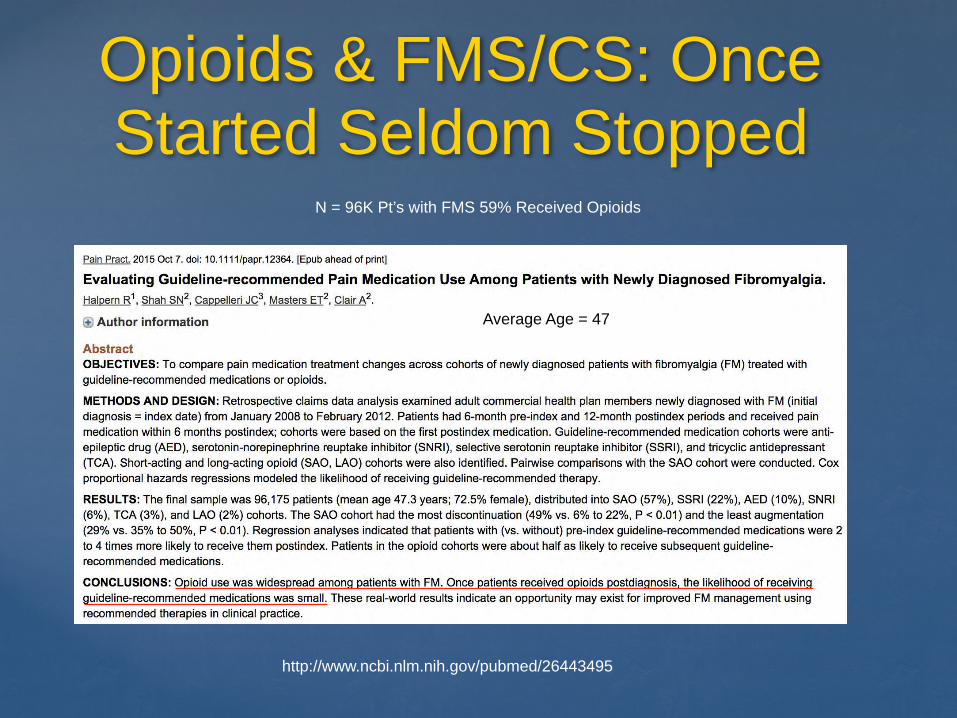
Opioids & FMS/CS: Once Started Seldom Stopped
http://www.ncbi.nlm.nih.gov/pubmed/26443495
Average Age = 47
N = 96K Pt’s with FMS 59% Received Opioids

Central Sensitivity is a Spectrum Disorder
http://www.ncbi.nlm.nih.gov/pubmed/23272983
Many Species in the Genus
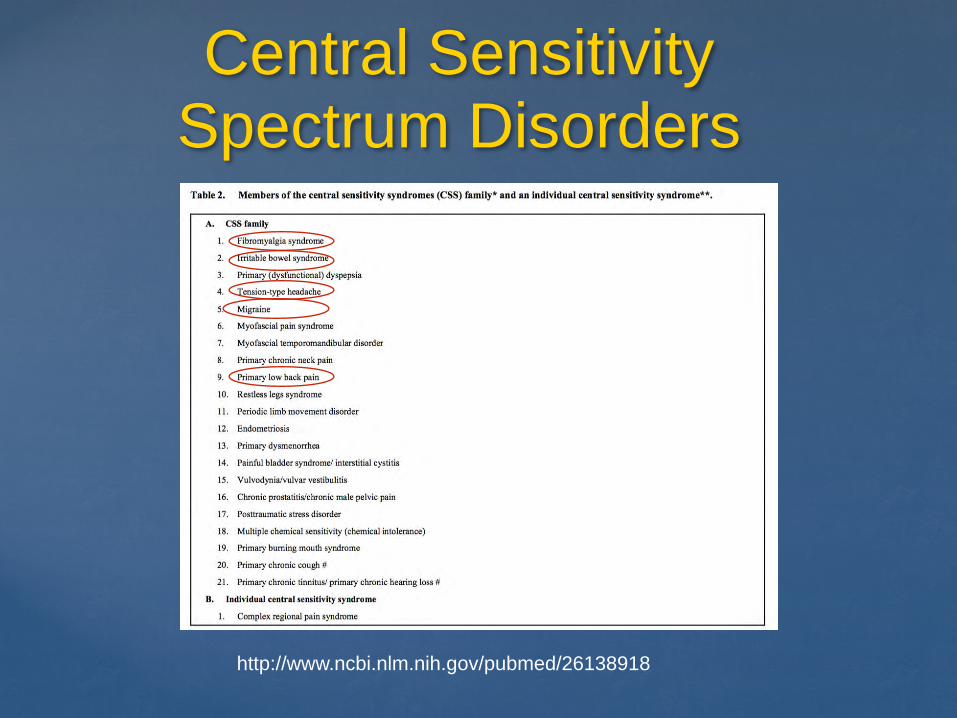
Central Sensitivity Spectrum Disorders
http://www.ncbi.nlm.nih.gov/pubmed/26138918
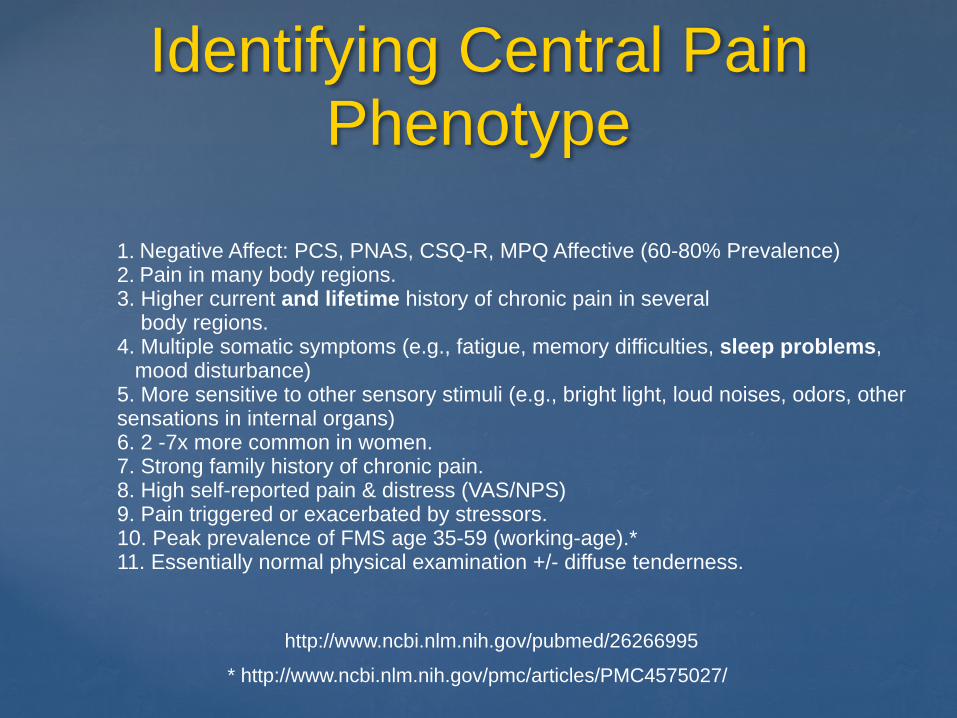
Identifying Central Pain Phenotype
http://www.ncbi.nlm.nih.gov/pubmed/26266995
1. Negative Affect: PCS, PNAS, CSQ-R, MPQ Affective (60-80% Prevalence) 2. Pain in many body regions. 3. Higher current and lifetime history of chronic pain in several body regions. 4. Multiple somatic symptoms (e.g., fatigue, memory difficulties, sleep problems, mood disturbance) 5. More sensitive to other sensory stimuli (e.g., bright light, loud noises, odors, other sensations in internal organs) 6. 2 -7x more common in women. 7. Strong family history of chronic pain. 8. High self-reported pain & distress (VAS/NPS) 9. Pain triggered or exacerbated by stressors. 10. Peak prevalence of FMS age 35-59 (working-age).* 11. Essentially normal physical examination +/- diffuse tenderness.
* http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4575027/
Validated Instruments to Central Pain
“You cannot guess at the extent of fatigue, unrefreshed sleep, cognitive problems, multiplicity of symptoms, and extent of pain without a detailed interview.”
Frederick Wolfe
http://www.ncbi.nlm.nih.gov/pubmed/20461781
Validated Instruments to Detect Central Pain
Negative Affect: Pain Catastrophizing Scale (PCS) Fibromyalgia Screening Questionnaire (NHIS)
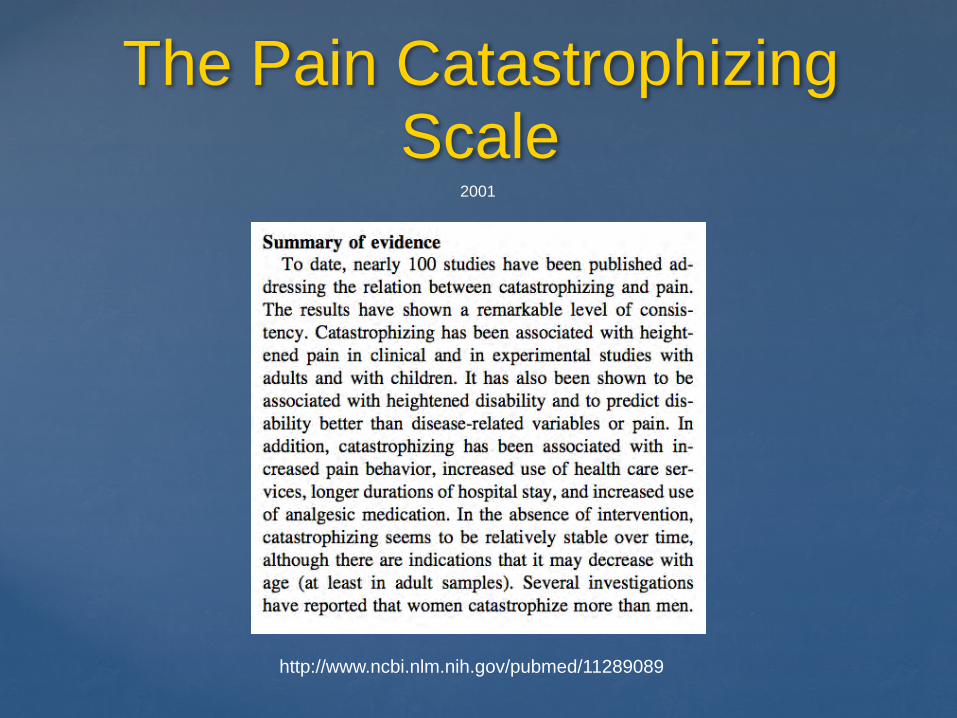
The Pain Catastrophizing Scale
http://www.ncbi.nlm.nih.gov/pubmed/11289089
2001
The PCS is a Validated Measure of Negative Affect
1. Published by Sullivan 1995 2. 13 Item Likert Scale 3. 5 min to Administer 4. 3 Sub-scales:
A. Helplessness [1,2,3,4,5,12] B. Rumination [8,9,10,11] C. Magnification [6,7,13]
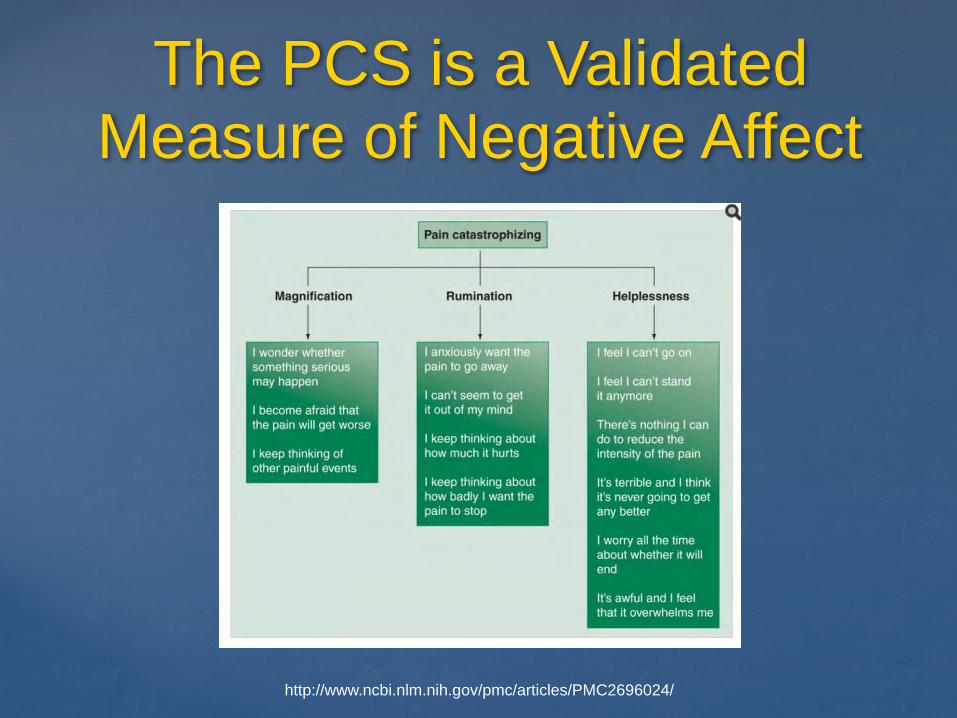
The PCS is a Validated Measure of Negative Affect
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696024/
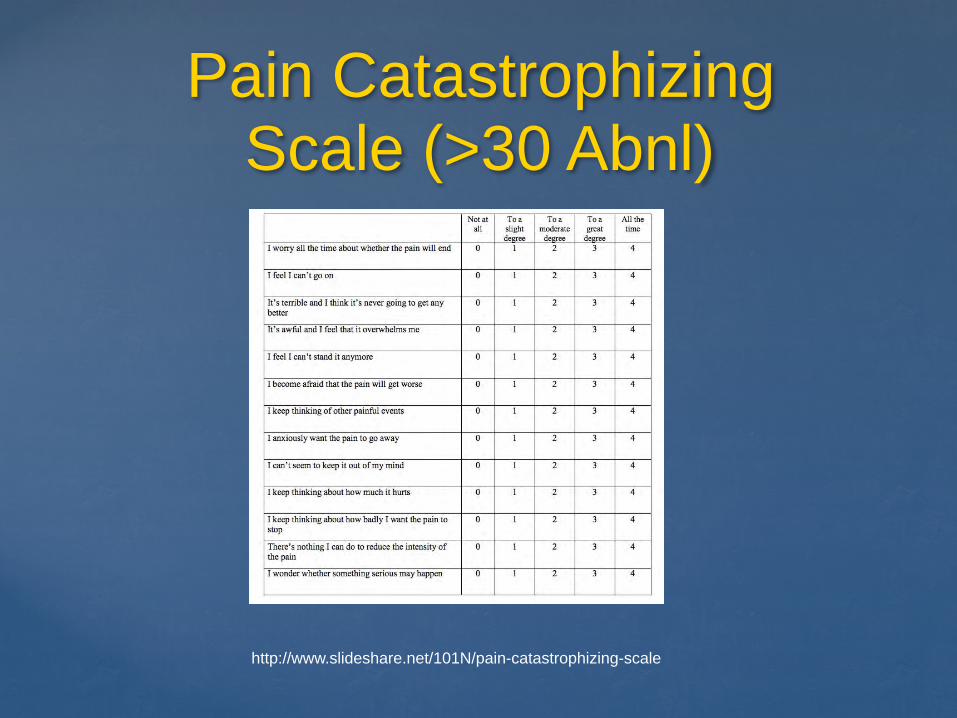
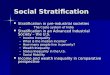
Pain Catastrophizing Scale (>30 Abnl)
http://www.slideshare.net/101N/pain-catastrophizing-scale
Heightened Pain Catastrophzing
What bearing does the diagnosis of heightened pain catastrophizing have upon opioid risk stratification?
Catastrophizing Predicts Opioid Misuse
http://www.ncbi.nlm.nih.gov/pubmed/23618767
N = 115

Catastrophizing Predicts Opioid Misuse
http://www.ncbi.nlm.nih.gov/pubmed/26235471
N = 215

Catastrophizing Predicts Opioid Misuse
http://www.ncbi.nlm.nih.gov/pubmed/27005461
N = 214
Catastrophizing Predicts Pain Sensitivity & Severity
http://www.ncbi.nlm.nih.gov/pubmed/11444718
N = 211
Catastrophizing Predicts Post-Op Opioid Use
http://www.ncbi.nlm.nih.gov/pubmed/25288368
N = 252
Catastrophizing Predicts Spinal Injection Failure
http://www.ncbi.nlm.nih.gov/pubmed/25817755
N = 386
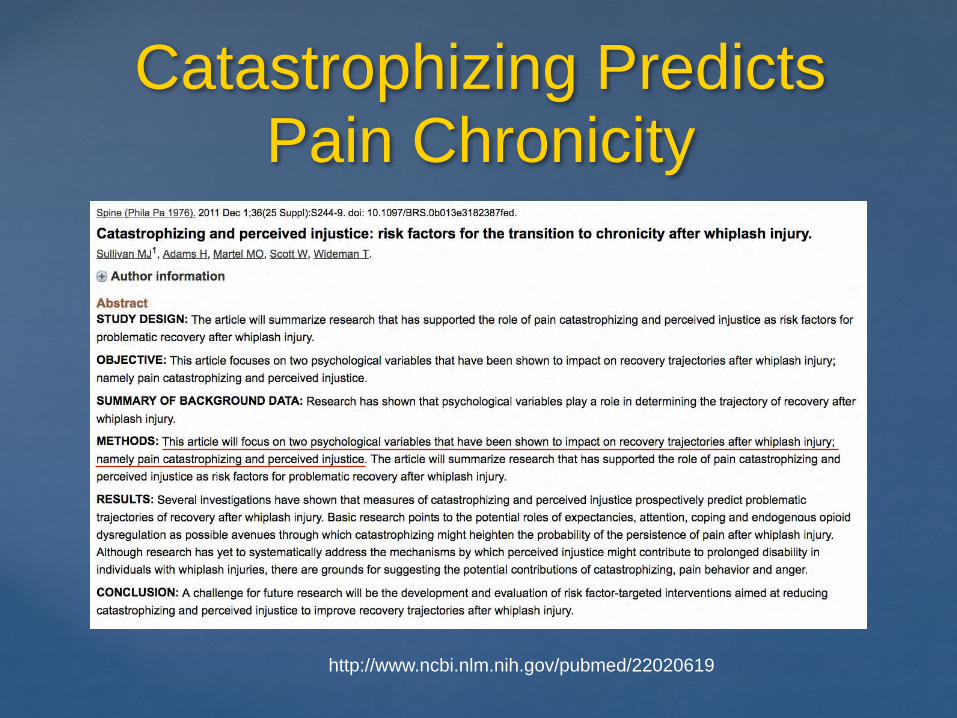
Catastrophizing Predicts Pain Chronicity
http://www.ncbi.nlm.nih.gov/pubmed/22020619
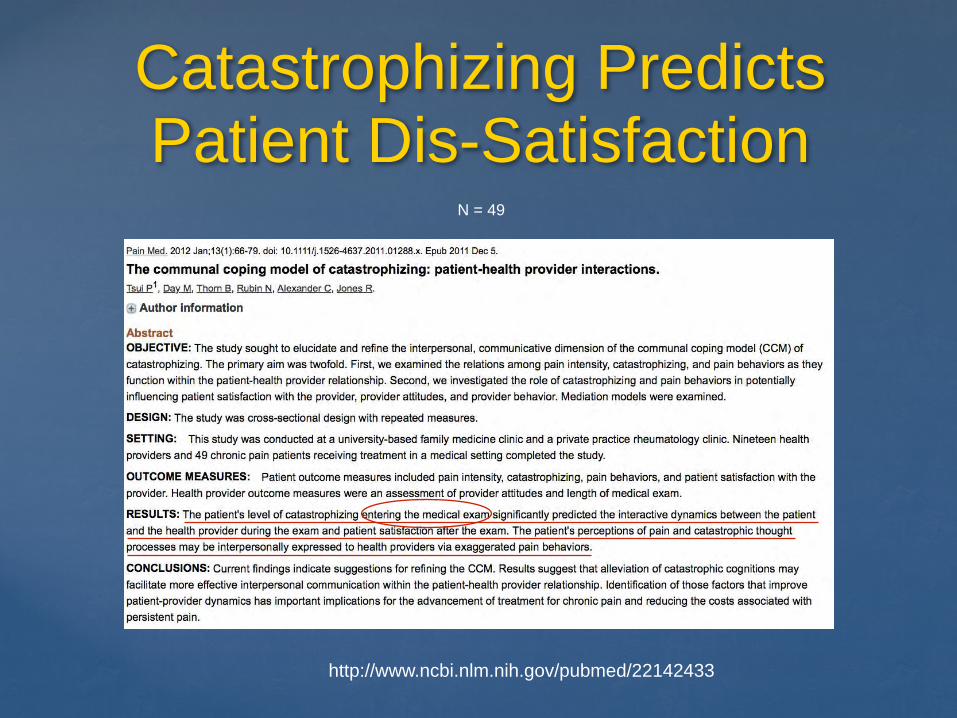
Catastrophizing Predicts Patient Dis-Satisfaction
http://www.ncbi.nlm.nih.gov/pubmed/22142433
N = 49
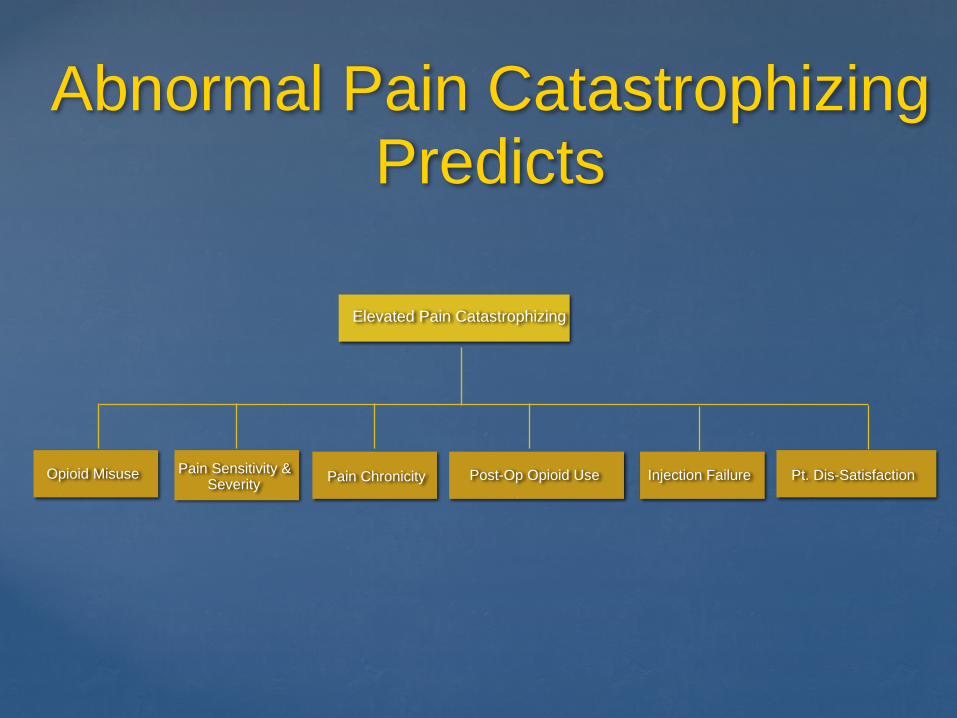
Abnormal Pain Catastrophizing Predicts
Injection Failure Pt. Dis-SatisfactionPost-Op Opioid UseOpioid Misuse Pain Sensitivity & Severity
Elevated Pain Catastrophizing
Pain Chronicity
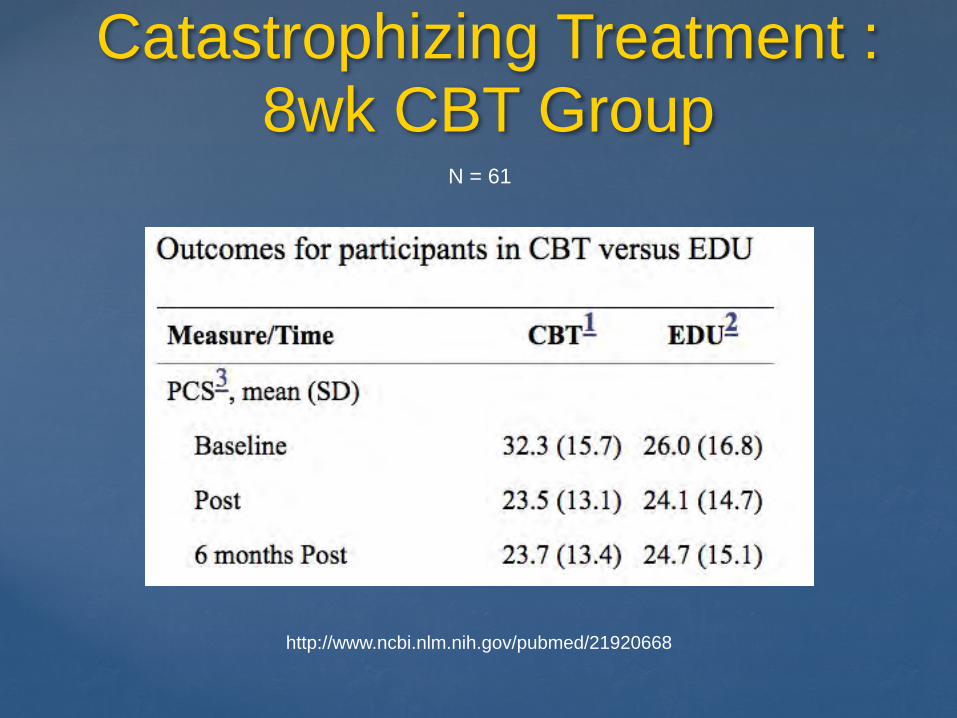
Catastrophizing Treatment : 8wk CBT Group
http://www.ncbi.nlm.nih.gov/pubmed/21920668
N = 61

Catastrophizing Treatment : 8wk Mindfulness Group
http://www.ncbi.nlm.nih.gov/pubmed/27445929
N = 29
Sample Case
Mrs. C: 50y/o WF with chronic low back pain and headache x 20yrs
FHX of chronic pain: + Mother & Sibling
Meds: HCTZ, IBU, topiramate & sumatriptan
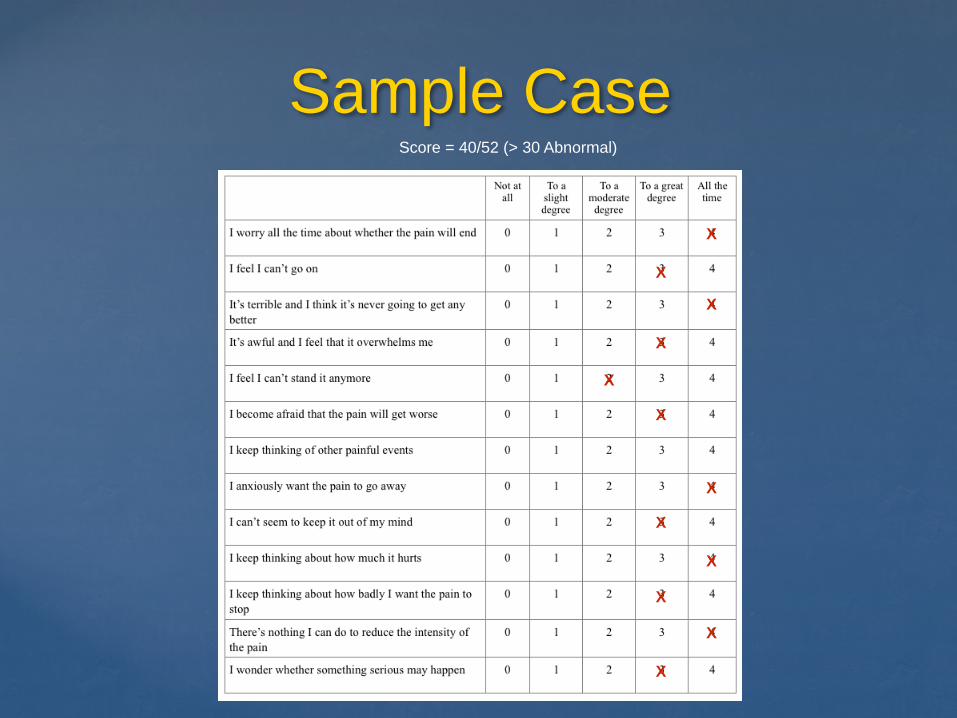
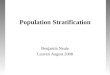
Sample Case
Score = 40/52 (> 30 Abnormal)
X
X
X
X
X
X
X
X
X
X
X
X

Sample Case
X
XX
XX
X
Score = 11 (FMS > 13)
X
X
X
N= 1
N= 10
References
Pain Catastrophizing Bibliography: https://www.slideshare.net/secret/D0Pddyn0y2LRgc
Pain Catastrophizing Scale: http://www.slideshare.net/101N/pain-catastrophizing-scale
2011 FMS Screener: http://www.slideshare.net/101N/fibromyalagia-survery-questionnaire
Catastrophizing theoretical perspectives: http://www.slideshare.net/101N/catastrophizing-trait-or-state
Thank You
www.supportprop.org