Embed Size (px)
Citation preview

Optimization of Beam Spectrum and Dose for Lower-Cost CT
by
Mary Esther Braswell
Graduate Program in Medical Physics Duke University
Date:_______________________ Approved:
___________________________
James Dobbins, Supervisor
___________________________ Anuj Kapadia
___________________________
Robert Reiman
___________________________ Paul Segars
Thesis submitted in partial fulfillment of the requirements for the degree
of Master of Science in the Graduate Program in Medical Physics in the Graduate School
of Duke University
2016

ABSTRACT
Optimization of Beam Spectrum and Dose for Lower-Cost CT
by
Mary Esther Braswell
Graduate Program in Medical Physics Duke University
Date:_______________________ Approved:
___________________________
James Dobbins, Supervisor
___________________________ Anuj Kapadia
___________________________
Robert Reiman
___________________________ Paul Segars
An abstract of a thesis submitted in partial fulfillment of the requirements for the degree
of Master of Science in the Graduate Program in Medical Physics in the Graduate School of
Duke University
2016

Copyright by Mary Esther Braswell
2016

iv
Abstract In many parts of the developing world, easy access to volumetric imaging is not
available. A Lower-Cost CT setup was proposed and found feasible by Dobbins et al. [1],
but was not yet optimized to maximize image quality while minimizing radiation dose
to the patient. A combination of spectrum modeling and Monte Carlo simulations were
used to compare x-ray beam parameters to determine which combination was optimal.
The beam parameters considered were filter type, filter thickness, and tube peak
kilovoltage (kVp). The optimization was based on the differential signal-to-noise ratio
(dSNR) and the dose, using a factor referred to as dSNR Efficiency. After the three
different filter materials at three different thicknesses were compared across five
different kVp values, it was determined that one half-value-layer (HVL) of copper was
the best filter type and thickness to achieve maximum image quality for minimal patient
dose.
In order to verify that a good dSNR efficiency using the spectrum modeling and
Monte Carlo meant that the system would provide useable images, the extended
cardiac-torso (XCAT) phantom was used to simulate CT images, using a ray tracer, and
estimate dose, using a full LCCT Monte Carlo simulation. The ray-tracer produced x-ray
projections of the XCAT phantom which were then run through a Feldkamp
reconstruction algorithm to produce CT images. The full LCCT Monte Carlo simulation

v
modeled the LCCT setup using the XCAT phantom to determine the dose to the patient.
From the reconstructed CT images, it was determined that for image studies that favor
air contrast higher kVp values, such as 140 kVp, are optimal. For studies that favor bone
contrast, however, the lower kVp values, such as 60 or 80 kVp, are optimal. For 140 kVp
images, the average effective dose, calculated using the ICRP 103 protocol, was 2.31 ∗
10'( mSv per mAs. The average effective dose for 60 kVp was 8.24 ∗ 10'+ mSv per mAs,
and the average effective dose for 80 kVp was 1.41 ∗ 10'( mSv per mAs. Further work is
needed to determine optimal mAs values for different imaging studies. The LCCT setup
can provide volumetric imaging to developing parts of the world that currently have no
volumetric imaging, which would greatly improve the quality of readily available
medical care.

vi
Dedication
This thesis is dedicated to my parents, Randy and Claire Braswell, for their
unconditional love and support through every stage of my life; my siblings, Sarah, Luke
and his wife, Brianne, and Anna Braswell, for always looking out for me and pushing
me to be my best; and my countless friends, for being there when I needed them. This
thesis is also dedicated to my nephew Elijah, to hopefully inspire him to never let
anything get in the way of his dreams.

vii
Contents
Abstract .......................................................................................................................................... iv
List of Tables ................................................................................................................................. ix
List of Figures ................................................................................................................................ x
List of Abbreviations ................................................................................................................. xiii
Acknowledgements ................................................................................................................... xiv
1. Introduction ............................................................................................................................... 1
1.1 Lower-Cost CT .................................................................................................................. 2
1.2 Image Quality .................................................................................................................... 3
1.2.1 Contrast ......................................................................................................................... 4
1.2.2 Signal to Noise Ratio ................................................................................................... 5
1.2.3 Resolution ..................................................................................................................... 6
1.2.4 Image Quality and Dose ............................................................................................. 6
1.3 Spectrum Modeling .......................................................................................................... 7
1.4 Monte Carlo ..................................................................................................................... 10
1.5 XCAT ................................................................................................................................ 12
2. Parameter Optimization ......................................................................................................... 16
2.1 Spectrum Modeling Methods ....................................................................................... 16
2.1.1 DXSPEC ...................................................................................................................... 18
2.1.2 Penelope ...................................................................................................................... 20
2.2 Spectrum Modeling Results .......................................................................................... 23

viii
2.2.1 Dose, Signal, and Noise Results .............................................................................. 23
2.2.2 dSNR and dSNR Efficiency Results ........................................................................ 34
2.3 Spectrum Modeling Discussion and Conclusions ..................................................... 43
2.3.1 DXSPEC and Penelope Dose, Signal, and Noise Comparisons .......................... 43
2.3.2 DXSPEC and Penelope dSNR Comparisons ......................................................... 44
2.3.3 Final Spectrum Modeling Discussion and Conclusions ...................................... 45
3. CT Dose Simulation and Image Reconstruction ................................................................. 48
3.1 Simulation and Reconstruction Methods .................................................................... 48
3.1.1 XCAT Projector Methods ......................................................................................... 48
3.1.2 Image Reconstruction Methods ............................................................................... 50
3.1.3 LCCT Simulation Methods ...................................................................................... 51
3.2 Simulation and Reconstruction Results ...................................................................... 53
3.2.1 Imaging Results ......................................................................................................... 53
3.2.2 Simulation Results ..................................................................................................... 56
3.3 Simulation and Reconstruction Conclusions and Discussion ................................. 59
4. Conclusions .............................................................................................................................. 61
References .................................................................................................................................... 63

ix
List of Tables Table 1: 1 and 2 HVL thicknesses for copper, aluminum, and gadolinium. ...................... 19
Table 2: XCAT Projector Input Parameters ............................................................................. 49
Table 3: XCAT Phantoms used in the XCAT projector. ........................................................ 50
Table 4: MATLAB CT reconstruction input parameters. ...................................................... 51
Table 5: TCM Simulation Input Parameters ............................................................................ 52
Table 6: Dose to Lung and Effective Dose results for each phantom and kVp value combination. ................................................................................................................................ 56

x
List of Figures Figure 1: Example DXSPEC output file. .................................................................................... 9
Figure 2: Example projection from XCAT projector. ............................................................. 14
Figure 3: Example reconstructed CT image from 180 XCAT projections. .......................... 15
Figure 4: Penelope geometry setup from both the (a) beam’s eye view and (b) the side. 21
Figure 5: The dose to 25 cm of tissue from an x-ray beam filtered by 1 HVL of aluminum......................................................................................................................................................... 24
Figure 6: Dose to 25 cm tissue from an x-ray beam filtered by 1 HVL of copper. ............. 24
Figure 7: Dose to 25 cm of tissue from an x-ray beam filtered by 1 HVL of gadolinium. 25
Figure 8: Dose to 25 cm of tissue from an unfiltered beam. ................................................. 25
Figure 9: Dose to the detector for the tissue setup and 1 HVL aluminum filter. ............... 26
Figure 10: Dose to the detector for the tissue setup and 1 HVL copper filter. ................... 26
Figure 11: Dose to the detector for the tissue setup and 1 HVL gadolinium filter. ........... 27
Figure 12: Dose to the detector for the tissue setup and no filter. ....................................... 27
Figure 13: Dose to the detector for the bone setup and 1HVL aluminum filter. ............... 28
Figure 14: Dose to the detector for the air setup and 1HVL aluminum filter. ................... 28
Figure 15: Dose to the detector for the bone setup and 1HVL copper filter. ..................... 29
Figure 16: Dose to the detector for the air setup and 1HVL copper filter. ......................... 29
Figure 17: Dose to the detector for the bone setup and 1HVL gadolinium filter. ............. 30
Figure 18: Dose to the detector for the air setup and 1HVL gadolinium filter. ................. 30
Figure 19: Dose to the detector for the bone setup and no filter. ......................................... 31
Figure 20: Dose to the detector for the air setup and no filter. ............................................. 31

xi
Figure 21: Tissue setup detector noise for 1 HVL aluminum filter. .................................... 32
Figure 22: Tissue setup detector noise for 1 HVL copper filter. ........................................... 33
Figure 23: Tissue setup detector noise for 1 HVL gadolinium filter. .................................. 33
Figure 24: Tissue setup detector noise for no filter. ............................................................... 34
Figure 25: dSNRbone values for 1 HVL aluminum filter. ........................................................ 35
Figure 26: dSNRbone values for 1 HVL copper filter. .............................................................. 35
Figure 27: dSNRbone values for 1 HVL gadolinium filter. ...................................................... 36
Figure 28: dSNRbone values for no filter. ................................................................................... 36
Figure 29: dSNRair values for 1 HVL aluminum filter. .......................................................... 37
Figure 30: dSNRair values for 1 HVL copper filter. ................................................................. 37
Figure 31: dSNRair values for 1 HVL gadolinium filter. ........................................................ 38
Figure 32: dSNRair values for no filter. ..................................................................................... 38
Figure 33: Calculated dSNRbone Efficiency values from DXSPEC for 1 HVL filters. .......... 39
Figure 34: Calculated dSNRbone Efficiency values from Penelope for 1 HVL filters. ......... 40
Figure 35: Calculated dSNRair Efficiency values from DXSPEC for 1 HVL filters. ............ 40
Figure 36: Calculated dSNRair Efficiency values from Penelope for 1 HVL filters. ........... 41
Figure 37: Calculated dSNRbone Efficiency values from DXSPEC for 2 HVL filters. .......... 42
Figure 38: Calculated dSNRair Efficiency values from DXSPEC for 2 HVL filters. ............ 42
Figure 39: Combined dSNRbone efficiencies for 1 HVL filters. .............................................. 46
Figure 40: Combined dSNRair efficiencies for 1 HVL filters. ................................................. 47
Figure 41: Reconstructed CT images for Female 1 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp. .................................................................................... 54

xii
Figure 42: Reconstructed CT images for Female 2 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp. .................................................................................... 54
Figure 43: Reconstructed CT images for Male 1 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp. .................................................................................... 55
Figure 44: Reconstructed CT images for Male 2 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp. .................................................................................... 55
Figure 45: dSNRbone Efficiencies calculated using lung dose for each phantom. ............... 57
Figure 46: dSNRbone Efficiencies calculated using effective dose for each phantom. ......... 58
Figure 47: dSNRair Efficiencies calculated using lung dose for each phantom. .................. 58
Figure 48: dSNRair Efficiencies calculated using effective dose for each phantom. ........... 59

xiii
List of Abbreviations CT Computed Tomography
OECD Organization for Economic Co-operation and Development
LCCT Lower-Cost CT
CBCT Cone-Beam CT
Gy Gray
kVp Peak Kilovoltage
SNR Signal to Noise Ratio
dSNR Differential Signal to Noise Ratio
mA Milliamperes
s Second
CsI Cesium Iodide
XCAT Extended Cardiac-Torso Phantom
NCAT 4-D NURBS-Based Cardiac-Torso Phantom
NURBS
ED
mSv
Nonuniform Rationale B-splines
Effective Dose
Millisievert

xiv
Acknowledgements I would like to express my sincerest thanks to: Dr. James Dobbins for being my
advisor; Dr. Anuj Kapadia for being my co-advisor; Dr. Paul Segars for helping me with
the XCAT phantom and serving on my committee; Dr. Robert Reiman for serving on my
committee; Dr. Jered Wells for helping me with CT reconstructions; Dr. Greeshma
Agasthya, Yakun Zhang, and Wanyi Fu for helping me with Penelope; Brian Harrawood
for helping me fix computer problems; Karen Kenna for scheduling all my meetings
with Dr. Dobbins and for being an encouragement every time I saw her; and finally, the
Duke Medical Physics and RAI Lab communities for fostering a collaborative work
environment. Thank you.

1
1. Introduction The advances in healthcare in the past century have been phenomenal. In just the
last fifty years, specifically in the area of medical imaging, many new imaging
modalities have been invented and implemented in state-of-the-art healthcare facilities
[2]. One of the most notable of these modalities is Computed Tomography (CT). CT is a
volumetric imaging modality that uses x-rays to acquire projection images at different
angles around the patient, then uses a reconstruction algorithm to produce an image in
the transverse plane. With CT images, physicians can distinguish between structures
that would appear overlapped and indistinguishable on conventional x-ray radiograph
images. For some cases, an x-ray radiograph is sufficient to diagnose patients; however,
there are many cases in which the x-ray radiograph does not have enough information
to correctly diagnose a patient. Volumetric imaging, specifically CT imaging, provides
better patient care through better diagnostic abilities.
Most healthcare facilities in the United States have access to at least one CT
scanner; in fact, according to data from the Organization for Economic Co-operation and
Development (OECD), in 2013 there were 43.4 CT scanners per million people in the
United States [3]. Compared to the other countries surveyed by OECD in 2013, the
United States had the second highest number of CT scanners per million people, second
only to Australia. The trend of easily accessible CT scanners is a common theme in the
developed world; the developing world, however, does not have this capacity at

2
present. According to the Global Health Observatory through the World Health
Organization, in 2013 out of the 37 African countries surveyed only 9 countries had 1 or
more CT scanners per million people and 3 countries had no CT scanners at all [4].
CT scanners are less predominant in developing countries primarily because of
their cost. A state-of-the-art CT scanner can cost upwards of $2.5 million. However,
people in the developing world often don’t have easy access to a CT scanner which
limits the ability to provide optimum medical care for them unless they travel great
distances to a facility that does have CT. These trips can be costly and difficult and cause
hardships for the patients and their families. The proposed solution to this problem is a
Lower-Cost CT (LCCT), which would make volumetric imaging more easily accessible
in the developing world.
1.1 Lower-Cost CT
One of the most expensive parts of a CT scanner is the slip-ring gantry which
allows the x-ray source to rotate continuously around the patient. A potential solution
has been proposed: instead of using a fan beam and rotating the source and detector
around the patient, use a stationary source and detector and rotate the patient between
the source and the detector, acquiring the images with cone beam CT (CBCT) [1]. The
rotation is accomplished through a rotating stage, which a patient stands or sits on,
which makes 1 rotation in approximately 10 seconds. The source and detector are set up
like a conventional x-ray setup, with the rotating stage in the middle. Previous work [1]

3
on this design has found that this is a feasible setup; however, when the initial feasibility
study was performed, there were two main concerns.
The first concern is patient motion. One patient rotation takes 10 seconds, which
makes it very difficult for the patient to remain completely still. Patient motion can cause
artifacts in the image, which could potentially cause the images to be no more or
possibly even less useful than conventional x-ray images. An algorithm has been
developed that reduces image artifacts due to patient movement [5]. This algorithm uses
markers on the patient to track patient movement, then makes the adjustments in the
reconstruction, so the images appear as if the patient had not moved.
The second concern is patient dose. Absorbed dose is defined as the amount of
energy absorbed in a unit mass of a tissue and has units of gray (Gy). Effective dose
(ED), which is a better index of overall risk to the patient, is a weighted average of organ
absorbed doses. It is important to know if the LCCT setup delivers a dose that falls
within an accepted clinical dose range. In order to help the system operate within these
dose limits, the spectrum can be optimized to achieve the best image quality for the
lowest dose to the patient.
1.2 Image Quality
In order to optimize the dose, the beam parameters that affect dose have to be
optimized. However, the beam parameters that affect dose also affect the image quality.

4
By definition, image quality is a measurement of the usability of an image. There are
several different measures of image quality.
1.2.1 Contrast
One measure of image quality is the contrast. Contrast is defined as the relative
difference between the measured signal in an object and the measured signal in the
background, as seen in Equation 1. Contrast allows the differentiation of objects in an
image. The higher the contrast the more easily objects can be distinguished from other
objects.
𝐶𝑜𝑛𝑡𝑟𝑎𝑠𝑡 =𝑆𝑖𝑔𝑛𝑎𝑙𝑖𝑛𝑇𝑎𝑟𝑔𝑒𝑡 − 𝑆𝑖𝑔𝑛𝑎𝑙𝑖𝑛𝐵𝑎𝑐𝑘𝑔𝑟𝑜𝑢𝑛𝑑
𝑆𝑖𝑔𝑛𝑎𝑙𝑖𝑛𝐵𝑎𝑐𝑘𝑔𝑟𝑜𝑢𝑛𝑑 1
The amount of the x-ray beam that reaches the detector and gets measured as
signal is determined by how much of the beam gets attenuated in the body. Attenuation
coefficients for tissues are greater at lower energies than at higher energies [6]. This
means that at lower beam energies, the contrast is higher than it is at high energies. The
beam energy is determined by the x-ray tube peak kilo-voltage (kVp) and the amount of
filtration in the beam, from both the externally imposed filter material and the patient.
Although the contrast increases as kVp decreases, if the kVp is too low, most of
the photons from the x-ray beam are attenuated in the patient and few make it to the
detector. This means there is not enough signal to create a useful image unless dose is
unnecessarily high.

5
1.2.2 Signal to Noise Ratio
Another measure of image quality is the signal to noise ratio (SNR). The SNR
compares the signal of the image to the amount of noise in the image, as seen in
Equation 2. Image noise limits the ability to discern objects of interest the image. Usually
noise makes an image look grainy, or mottled, which is caused by the fluctuations of
incident photons on the detector [7]. Noisy images are not very useful because the noise
makes it difficult to distinguish objects in an image.
𝑆𝑁𝑅 =𝑅𝑎𝑤𝑆𝑖𝑔𝑛𝑎𝑙𝑁𝑜𝑖𝑠𝑒
2
SNR is a good measure of image quality; it provides information on the visibility
of the actual image compared to the noise in that image, but it doesn’t provide any
information on the difference between the signal in two different objects in the image.
The differential SNR (dSNR), as seen in Equation 3, measures the difference between
signal in an object and its background, or between two objects, and then compares that
difference in signal to the noise in the image, providing information about the SNR of
the anatomical object of diagnostic interest.
𝑑𝑆𝑁𝑅 =𝑆𝑖𝑔𝑛𝑎𝑙𝑖𝑛𝑂𝑏𝑗𝑒𝑐𝑡1 − 𝑆𝑖𝑔𝑛𝑎𝑙𝑖𝑛𝑂𝑏𝑗𝑒𝑐𝑡2
𝑁𝑜𝑖𝑠𝑒 3
The signal in the detector is affected by the x-ray tube output. The parameters
that contribute to x-ray tube output are the kVp, tube current, measured in milliamperes
(mA), and how long the beam stays on, measured in seconds (s). In diagnostic imaging,
the product of tube current and beam time is referred to as the mAs.

6
Since the noise increases as the raw signal increases, in order to generate the
best images, the optimal dSNR must be found. The optimal dSNR will maximize the
differential signal while minimizing noise.
1.2.3 Resolution
Spatial resolution is a measure of how easily small features that are close
together can be distinguished from each other. At high spatial resolution small features
are more easily distinguished than those same features are at low spatial resolution.
Although spatial resolution is important, it was not considered in this spectrum
optimization study.
1.2.4 Image Quality and Dose
As stated earlier, the same parameters that affect image quality also affect dose.
Patient dose depends on tube output parameters, such as kVp and mAs. Other
parameters that affect dose and image quality are beam filter type and beam filter
thickness. Putting a filter in the beam can harden the beam by removing the low-energy
portions of the x-ray spectrum that is produced by the x-ray tube, or, in the case of a k-
edge filter, can lower the average beam energy. Beam hardening increases the beam
mean energy, which decreases the dose for a given detected signal, because greater
absorption of lower energy photons in the filter reduces their absorption in the patient.
The filter type and thickness determine how much of the beam is removed from the
spectrum.

7
In order to find the optimal spectrum, there must be a way to compare the image
qualities of different x-ray spectra while also taking into consideration the amount of
radiation dose the patient is receiving. One way to do this is to calculate the efficiency,
which is defined here as the ratio of the squared dSNR to the patient dose This factor is
referred to as dSNR efficiency. This efficiency value allows for simultaneous
optimization of image quality and dose.
1.3 Spectrum Modeling
The x-ray beam spectrum affects both image quality and patient dose. The beam
spectrum represents the number of photons found at each energy in the x-ray beam. The
shape of the spectrum is effected by the filter material, the filter thickness, the tube kVp,
and the tube mAs. Each parameter produces a spectrum that has a different shape.
These different shapes cause the beam to interact differently through the patient. For
example, a spectrum that has a peak at lower energies, has a lower mean energy which
causes a higher patient dose and lower signal than if the peak in the spectrum had been
at a higher energy. The spectrum needs to be optimized in order to reduce unnecessary
patient dose and achieve the best image.
In order to compare many different beam parameter combinations and determine
the optimal dSNR Efficiency without having to physically run each combination, a
spectrum modeling program can be used. A spectrum modeling program uses a
mathematical method to estimate the x-ray spectrum based on given parameters. The

8
mathematical method uses tabulated attenuation coefficients of the relevant materials in
the beam to determine the beam spectrum as it passes through the various filters and the
patient.
DXSPEC is a spectrum modeling program designed specifically for diagnostic x-ray
spectra developed by Ergun et al. in 1977 [8]. DXSPEC accounts for Compton and
coherent scattering and photoelectric effect. DXSPEC also models secondary
interactions, such as k-fluorescence and single Compton cascades. Originally DXSPEC
was used to model a general x-ray tube x-ray spectrum including bremsstrahlung and
characteristic x-rays, but was later modified by Dobbins to include empirical tube
spectra that had been modeled by Boone and Seibert [9, 10]. Dobbins also modified
DXSPEC to generate an estimate of expected noise, calculated by summing the energy
weighted variances from each energy bin [9].
The modified version of DXSPEC can be used to estimate the signal, noise, and dose
for any filter combination. DXSPEC outputs the attenuated exposure, fluence, and mean
energy; the transmitted exposure, fluence, and mean energy; and the energy absorption
noise, dose, and mean energy for each material placed in the beam as seen in Figure 1.
DXSPEC considers every material placed in the beam a filter. By inputting the target
material, thicknesses of various tissues, and detector composition, such as cesium iodide
(CsI), the dSNR can be calculated from the values that DXSPEC outputs.

9
Figure 1: Example DXSPEC output file.
DXSPEC outputs “absorbed energy (*)” and “absorbed energy (**)” estimates for
each filter. The “absorbed energy (*)” value assigns the absorbed energy to the bin of the
incident photon, while the “absorbed energy (**)” value assigns absorbed energy to the
composite total of estimated initial and secondary absorption events. This means that
the expected dose and signal in real-life will likely fall between these two points. In
previous studies using DXPEC, DXSPEC was found to be accurate for attenuation
values, but the noise and tissue dose values had not been validated.
Since the dose values had not been validated, and dose is a very important aspect of
this work, it was necessary to validate the DXSPEC dose results. An established
technique to accurately estimate dose is Monte Carlo.

10
1.4 Monte Carlo
The “Monte Carlo” method uses random numbers to model very complex
mathematical processes. The term was first used by scientists in the 1940s who were
working on nuclear weapons. Monte Carlo is used in many fields, including physics, to
model complex equations and problems. In physics it can be used to model the path of a
particle through a material.
Monte Carlo simulations can use the probability distribution of interactions
between a particle and a material to estimate the interactions of multiple particles. The
Monte Carlo code is set up to use a random number each time something different could
happen. For example, a Monte Carlo code following a photon interacting in water would
use a random number to determine the energy of the photon, then use another random
number to determine whether the photon was absorbed in the water, then another
random number to determine if there were any secondary reactions, and so on until
there are no more possible interactions.
The decisions made by the random numbers are based on the probabilities supplied
to the Monte Carlo code. For example, consider the interaction of an x-ray beam with
water. The energy of each randomly-generated photon would be determined from the
input spectrum, and whether the photon was absorbed by the water would be
determined using the probability distribution of the photoelectric and Compton
attenuation coefficients for water.

11
Many Monte Carlo packages, which are already set up to model interactions of
particles with materials, are available. One available Monte Carlo package is
PENELOPE, which stands for Penetration and Energy Loss from Positrons and
Electrons. PENELOPE was developed in 2001 by Salvat et. al. to model electron and
photon transport [11]. PENELOPE is very useful for diagnostic imaging and radiation
therapy dosimetry simulations because it effectively models photon and electron
transport through the body at those energies to high accuracy. Like everything, Monte
Carlo has limitations. The main limitation of PENELOPE is that it is not an ideal way to
acquire projection data because it would take much longer than other programs, such as
ray tracing programs, to simulate enough particles to generate an image.
Since DXSPEC does not produce as sophisticated a model of dose as does Monte
Carlo methods, PENELOPE can be used to model the same simple setup as DXPEC to
produce a more accurate measurement of dose. This allows the dSNR efficiency to be a
more accurate measure than if only DXSPEC was used in its calculation.
PENELOPE can also be used to model the entire LCCT setup, so that an estimate of
dose to a phantom from a LCCT scan can be obtained. The PENELOPE simulation can
be set up to model a CBCT x-ray tube output to rotate around a phantom and take
projections at 180 different angles. This allows the dose to the phantom to be calculated.
The geometry package that is included with PENELOPE allows a user to specify
geometries made of quadratic surfaces. This geometry package makes it difficult to

12
generate complicated phantoms, such as the human body, however, PENELOPE can
also use a pre-generated voxelized phantom. This means that an anthropomorphic
phantom can be incorporated into the simulation and the dose to a person can be
estimated with high precision.
1.5 XCAT
There are three main types of anthropomorphic phantoms: mathematical,
voxelized, and hybrid. The mathematical phantom can model motion, but is a very
crude rendering of human anatomy. Voxelized phantoms, on the other hand, are
developed from patient CT data, so they model human anatomy very well, but they do
not model motion and they do not exist for a wide variety of patient body types and
sizes. The hybrid phantom is made up of the best qualities of the mathematical and
voxelized phantoms; it models human anatomy very well and models motion.
One such hybrid phantom developed by Segars et al. is called the extended
Cardiac-Torso (XCAT) phantom [12]. The XCAT is an extended version of the 4-D
NURBS-Based Cardiac-Torso (NCAT) phantom. NURBS, or nonuniform rational B-
splines, are used in computer graphics to model complicated surfaces, making it
possible to model complex anatomical structures correctly. The NCAT phantom was
developed using the Visible Human data from the National Library of Medicine. The
NCAT only models the torso, but allows for cardiac and respiratory motion. The NCAT
can be male or female; however, was only modeled from the male Visible Human data

13
set. The female phantom adds breast models to the male torso. The NCAT has the ability
to model different patient sizes by scaling the anatomy of the Visible Human data set.
The XCAT expands the NCAT to include the entire body. Although it was also
modeled using the Visible Human data, there are variations of the XCAT to model
different humans, based on clinical CT data. The XCAT models anatomical surfaces
better than the NCAT by using subdivision surfaces along with NURBS surfaces. The
subdivision surfaces better model certain structures in the brain and breast by taking a
rough polygon mesh and subdividing it until the surface becomes smooth. A female
XCAT was developed from the female Visible Human data and patient CT scans, and
better breast models have been developed through high resolution dedicated breast CT
data. The XCAT phantom also improves the NCAT phantom by using a higher
resolution heart motion data set and a higher resolution lung motion data to model
heart and respiratory motion.
The XCAT can easily be used in Monte Carlo simulations, like PENELOPE, and can
be easily imaged. A CT simulation for the XCAT phantom has been developed by Segars
et al. [13]. The CT simulation uses ray tracing to produce projections of the XCAT
phantom from different angles. This CT simulation models parallel, fan, and cone beam
CT. The CT parameters can be changed to simulate any CT setup, including the LCCT
[12-14]. An example projection image of the XCAT CT simulation can be found in Figure
2.

14
Figure 2: Example projection from XCAT projector.
The projections from the CT simulator can be used to generate a CT image using a
CT reconstruction algorithm, such as a Feldkamp algorithm [15]. The Felkamp
algorithm developed by Feldkamp et al. in 1984, is a filtered back projection
reconstruction algorithm specifically designed for CBCT. The Feldkamp reconstruction
algorithm generates volumetric images using x-ray projection data. The XCAT CT
simulator projections are run through the Feldkamp algorithm to produce CBCT images
such as the image in Figure 3.

15
Figure 3: Example reconstructed CT image from 180 XCAT projections.

16
2. Parameter Optimization The first part of this work was to determine the optimal beam parameters using
spectrum modeling. The spectrum modeling program DXSPEC was used as well as the
penmain program included in the 2006 version of Penelope.
2.1 Spectrum Modeling Methods
Previous work with DXSPEC determined that the optimal kVp and filter for x-
ray imaging for chest radiography using a CsI detector are 100kVp and 1 half-value
layer (HVL) copper (Cu) filter. [9] Taking these findings into consideration, the
following parameters were tested for the LCCT setup: filter type, filter thickness, and
kVp. One main parameter that affects image quality that was not tested was mAs,
however, mAs is limited by the tube loading. This means that the optimal mAs will have
to be determined after the LCCT system is operational.
The different filter types tested were aluminum, copper, and gadolinium.
Aluminum and copper were used because they are inexpensive and are common filter
materials. Gadolinium was chosen because it has a k-edge of 50.3 keV that creates a
spectrum with two well-defined peaks, which could impact the image quality and dose.
These filters provide a varying range of attenuation, with aluminum being the least
attenuating and gadolinium being the most attenuating per filter thickness.

17
These filters were simulated with thicknesses of 0 half value layer (HVL), 1 HVL,
and 2 HVL. An HVL thickness is the thickness of material it takes to attenuate half of the
particles incident on that material. For monoenergetic sources the HVL can be found by
𝐻𝑉𝐿 =ln 2𝜇
(4)
where µ is the linear attenuation coefficient. This equation is derived from the
attenuation equation
𝑁 = 𝑁O𝑒'PQ (5)
where N0 is the number of photons incident on the material, N is the number of photons
that are transmitted through the material, and x is the thickness of material. For
polyenergetic beams, the HVL must be found experimentally. 0 HVL means no
attenuation, 1 HVL thickness of material attenuates half of the incident photons, and 2
HVL thickness of material attenuates three fourths of the incident photons. Using these
thicknesses provides a good range of attenuation.
The kVp values that were simulated were: 60, 80, 100, 120, and 140 kVp. At
kilovoltage values lower than 60 kVp, most of the beam is attenuated by the patient
which means that usable signal per patient dose is not optimum for most imaging needs.
At kVps higher that 140 kVp, the dSNR does not greatly improve because contrast is
greater at lower energies.

18
2.1.1 DXSPEC
After the parameters that would be tested were chosen, the HVL for each filter
was found for each kVp value. Since DXSPEC outputs the attenuated fluence and the
transmitted fluence, the HVL can be found fairly easily. First the material was specified
in DXSPEC as a filter with a thickness of several centimeters, broken into 0.1 cm steps.
DXSPEC was run for each kVp value, then using the output files, the attenuated and
transmitted fluence at each 0.1 cm step were examined to find the thickness where the
difference between the attenuated and transmitted fluence was minimized. The 0.1 cm
step that had the closest transmitted and attenuated fluence was rerun through DXSPEC
at 0.01 cm increments, then 0.001 cm increments, so that the HVL to the nearest 0.01 mm
could be found. The HVLs found by DXSPEC can be found in Table 1. This method was
not the most efficient method to find the HVL thicknesses. The standard protocol and
more efficient way is to test several thicknesses, plot the transmission vs. thickness, and
interpolate using a logarithmic curve fit to find the HVL; however, the former approach
is potentially more accurate when significant spectral shaping occurs.

19
Table 1: 1 and 2 HVL thicknesses for copper, aluminum, and gadolinium.
Material Energy(kVp) 1HVL(mm) 2HVL(mm)Copper 60 0.13 0.26
80 0.22 0.44100 0.32 0.64120 0.41 0.82140 0.5 1
Aluminum 60 3.72 7.4480 5.31 10.62100 6.64 13.28120 7.68 15.36140 8.5 17
Gadolinium 60 0.09 0.1880 0.09 0.18100 0.1 0.2120 0.11 0.22140 0.12 0.24
After the HVLs for each filter type and kVp were found, the optimization was
started. Each filter type, filter thickness, and kVp combination was run through three
different setups in DXSPEC. The first setup included the filter, then 25 cm of tissue, then
the detector. This setup was the tissue setup. The second setup had the filter, 24 cm of
tissue, 1 cm of bone, then the detector. This setup was the bone setup. The final setup
was the air setup, it had the filter, 24 cm of tissue, then the detector.
After each filter type, filter thickness, and kVp combination was run through
DXSPEC for each setup, the dSNRs were calculated. The dSNR for tissue vs. bone
contrast, or dSNRbone was found by
𝑑𝑆𝑁𝑅STUV =𝐼STUV − 𝐼XYZZ[V
𝑁XYZZ[V(6)

20
where Ibone is the dose to the detector, or signal, for the bone setup, Itissue is the signal for
the tissue setup, and Ntissue is the detector noise for the tissue setup. Likewise, the dSNR
for tissue vs. air contrast, or dSNRair was found by
𝑑𝑆𝑁𝑅]Y^ =𝐼]Y^ − 𝐼XYZZ[V𝑁XYZZ[V
(7)
where Iair is the signal in the air setup. The dSNR Efficiencies could then be calculated by
𝐸𝑓𝑓𝑖𝑐𝑖𝑒𝑛𝑐𝑦 =𝑑𝑆𝑁𝑅c
𝐷XYZZ[V
(8)
where the Dtissue is the Dose to the tissue in the tissue setup. After the dSNR Efficiencies
are calculated, the different parameters can be compared to each other.
2.1.2 Penelope
The Penelope subroutine, included with Penelope 2006, called penmain was used
to validate the DXSPEC results. The DXSPEC signal results have been previously
experimentally validated [9], however, the dose results have not. DXSPEC gives results
in keV/(kJ*cm2), so in order to model the three DXSPEC setups in Penelope, the same
thicknesses were used, but each thickness had a face that was 1 cm by 1 cm. The
geometry can be found in figure 4. Figure 4a shows the setup in the beam’s eye view,
while Figure 4b shows the setup from the side.

21
Figure 4: Penelope geometry setup from both the (a) beam’s eye view and (b) the side.
In order to be consistent, the x-ray tube output spectrum, the spectrum with
nothing in the beam, from DXSPEC was used as the energy spectrum of the photons in
Penelope. Unlike DXSPEC, which outputs energy per tube output per square centimeter,
Penelope results are in units of energy per photon, specifically eV per photon. To make
the results comparable, the results from Penelope were multiplied by the fluence of the
tube output in number of photons per tube output energy per square centimeter and eV
was converted to keV, this made all the results in the same units: keV/(kJ*cm2). This is
not a conventional unit for dose, however, it can be easily converted. The units for dose

22
are gray (Gy), where 1 Gy equals 1 J/kg. Converting keV/(kJ*cm2) to Gy/kJ, or dose per
tube output begins by converting keV to J, then cm2 must be converted to kg. The
conversion factor for keV to J is keV equals 1.602*10-16 J. The square centimeters can be
converted to grams by using the depth of material and the density as shown in equation
(6).
𝑐𝑚c ∗ 𝑑𝑒𝑝𝑡ℎ 𝑐𝑚 ∗ 𝑑𝑒𝑛𝑠𝑖𝑡𝑦𝑔𝑐𝑚h = 𝑚𝑎𝑠𝑠 𝑔 (9)
Mass in grams can then be converted to kg. The complete conversion can be found in
equation (7).
𝑅𝑒𝑠𝑢𝑙𝑡𝑠𝑘𝑒𝑉
𝑘𝐽 ∗ 𝑐𝑚c ∗1.602 ∗ 10'kl 𝐽
𝑘𝑒𝑉𝑑𝑒𝑝𝑡ℎ 𝑐𝑚 ∗ 𝑑𝑒𝑛𝑠𝑖𝑡𝑦 𝑔
𝑐𝑚h ∗ .001 𝑘𝑔𝑔
= 𝑅𝑒𝑠𝑢𝑙𝑡𝑠𝐺𝑦𝑘𝐽
(10)
Even though units of Gy are more conventional, the units for this part of the project
were left in units of keV/(kJ*cm2), because the doses were only used for comparisons.
Unlike DXSPEC, Penelope does not output a measure of noise, so in order to find
the dSNR values from Penelope, the noise had to be calculated. Within the Penelope
input file, an energy detector can be defined from one of the objects in the geometry file.
The energy detector output gives the probability density of photons in defined energy
bins. This probability density can be used to calculate the theoretical noise. Finding the
standard deviation of the number of photons detected gives an estimate of noise. By
definition, the standard deviation is the square root of the variance. In counting, or
Poisson, statistics, the variance of a number of counts equals the number of counts. Since

23
each energy bin has its own counts, the variance for each energy bin was calculated. The
total Penelope noise was then calculated using
𝑁𝑜𝑖𝑠𝑒 = 𝐸Yc𝜎Yc (11)
where Ei is energy of an energy bin and si is the standard deviation in that energy bin.
After the noise was calculated for Penelope, the dSNR and dSNR efficiency values could
be calculated and compared to the dSNR and dSNR efficiency values for the
corresponding DXSPEC setups. The propagation of error can then be used to find the
uncertainty in the noise and dSNR.
2.2 Spectrum Modeling Results
2.2.1 Dose, Signal, and Noise Results
Figures 5 through 8 display the dose results for DXSPEC absorbed energy (*),
DXSPEC absorbed energy (**), and Penelope for the 1 HVL Aluminum, 1 HVL Copper, 1
HVL Gadolinium, and no filter cases, for 25 cm of tissue.
The DXSPEC absorbed energy (*), absorbed energy (**), and Penelope results for
the tissue setup dose to the detector, or signal, for 1 HVL aluminum filter, 1 HVL copper
filter, 1 HVL gadolinium filter, and 0 HVL, or unfiltered, can be found in Figures 9
through 12, respectively.

24
Figure 5: The dose to 25 cm of tissue from an x-ray beam filtered by 1 HVL of aluminum.
Figure 6: Dose to 25 cm tissue from an x-ray beam filtered by 1 HVL of copper.
0.00E+00
5.00E+09
1.00E+10
1.50E+10
2.00E+10
2.50E+10
3.00E+10
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
Doseto25cmTissue1HVLAluminumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+00
5.00E+09
1.00E+10
1.50E+10
2.00E+10
2.50E+10
3.00E+10
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
Doseto25cmTissue1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

25
Figure 7: Dose to 25 cm of tissue from an x-ray beam filtered by 1 HVL of gadolinium.
Figure 8: Dose to 25 cm of tissue from an unfiltered beam.
0.00E+00
5.00E+09
1.00E+10
1.50E+10
2.00E+10
2.50E+10
3.00E+10
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
Doseto25cmTissue1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+00
1.00E+10
2.00E+10
3.00E+10
4.00E+10
5.00E+10
6.00E+10
7.00E+10
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
Doseto25cmTissue0HVL
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

26
Figure 9: Dose to the detector for the tissue setup and 1 HVL aluminum filter.
Figure 10: Dose to the detector for the tissue setup and 1 HVL copper filter.
0.00E+005.00E+071.00E+081.50E+082.00E+082.50E+083.00E+083.50E+084.00E+084.50E+085.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
TissueSetupDetectorDose1HVLAluminumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+005.00E+071.00E+081.50E+082.00E+082.50E+083.00E+083.50E+084.00E+084.50E+085.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
TissueSetupDetectorDose1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

27
Figure 11: Dose to the detector for the tissue setup and 1 HVL gadolinium filter.
Figure 12: Dose to the detector for the tissue setup and no filter.
The detector doses for both the air setup and the bone setup followed the same
trends as the tissue setup. The only difference is that for the air setup, the doses are
0.00E+005.00E+071.00E+081.50E+082.00E+082.50E+083.00E+083.50E+084.00E+084.50E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
TissueSetupDetectorDose1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+00
1.00E+08
2.00E+08
3.00E+08
4.00E+08
5.00E+08
6.00E+08
7.00E+08
8.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
TissueSetupDetectorDose0HVLFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

28
shifted slightly higher, and for the bone setup, the doses are shifted slightly lower. The
detector doses for the bone and air setups are displayed in Figures 13-20.
Figure 13: Dose to the detector for the bone setup and 1HVL aluminum filter.
Figure 14: Dose to the detector for the air setup and 1HVL aluminum filter.
0.00E+005.00E+071.00E+081.50E+082.00E+082.50E+083.00E+083.50E+084.00E+084.50E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
BoneSetupDetectorDose1HVLAluminumFilter
Series1
Series2
Series3
0.00E+00
1.00E+08
2.00E+08
3.00E+08
4.00E+08
5.00E+08
6.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
AirSetupDetectorDose1HVLAluminumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

29
Figure 15: Dose to the detector for the bone setup and 1HVL copper filter.
Figure 16: Dose to the detector for the air setup and 1HVL copper filter.
0.00E+005.00E+071.00E+081.50E+082.00E+082.50E+083.00E+083.50E+084.00E+084.50E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
BoneSetupDetectorDose1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+00
1.00E+08
2.00E+08
3.00E+08
4.00E+08
5.00E+08
6.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
AirSetupDetectorDose1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

30
Figure 17: Dose to the detector for the bone setup and 1HVL gadolinium filter.
Figure 18: Dose to the detector for the air setup and 1HVL gadolinium filter.
0.00E+00
5.00E+07
1.00E+08
1.50E+08
2.00E+08
2.50E+08
3.00E+08
3.50E+08
4.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
BoneSetupDetectorDose1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+00
1.00E+08
2.00E+08
3.00E+08
4.00E+08
5.00E+08
6.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
AirSetupDetectorDose1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

31
Figure 19: Dose to the detector for the bone setup and no filter.
Figure 20: Dose to the detector for the air setup and no filter.
0.00E+00
1.00E+08
2.00E+08
3.00E+08
4.00E+08
5.00E+08
6.00E+08
7.00E+08
8.00E+08
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
BoneSetupDetectorDose0HVLFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+001.00E+082.00E+083.00E+084.00E+085.00E+086.00E+087.00E+088.00E+089.00E+081.00E+09
60 80 100 120 140
Dose
(kev/(kJ*cm^2))
kVp
AirSetupDetectorDose0HVLFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

32
The calculated noise from Penelope and the noise results from DXSPEC for 1
HVL of aluminum, 1 HVL copper, 1 HVL gadolinium, and no filter can be found in
Figures 21 through 24, respectively. The noise is only shown for the tissue setup because
the noise in the other two setups is not used to compute the dSNR or dSNR efficiency.
Figure 21: Tissue setup detector noise for 1 HVL aluminum filter.
0.00E+002.00E+044.00E+046.00E+048.00E+041.00E+051.20E+051.40E+051.60E+051.80E+05
60 80 100 120 140
Noise
(keV
/sqrt(k
J*cm
^2))
kVp
TissueSetupNoise1HVLAluminum
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

33
Figure 22: Tissue setup detector noise for 1 HVL copper filter.
Figure 23: Tissue setup detector noise for 1 HVL gadolinium filter.
0.00E+002.00E+044.00E+046.00E+048.00E+041.00E+051.20E+051.40E+051.60E+051.80E+05
60 80 100 120 140
Noise
(keV
/sqrt(k
J*cm
^2))
kVp
TissueSetupNoise1HVLCopper
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
0.00E+002.00E+044.00E+046.00E+048.00E+041.00E+051.20E+051.40E+051.60E+051.80E+05
60 80 100 120 140
Noise
(keV
/sqrt(k
J*cm
^2))
kVp
TissueSetupNoise1HVLGadoliinium
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

34
Figure 24: Tissue setup detector noise for no filter.
2.2.2 dSNR and dSNR Efficiency Results
The results of the DXSPEC and Penelope dSNRbone calculations for 1 HVL of each
filter type and no filter can be found in Figures 25-28. The dSNRair calculations for 1 HVL
of each filter type and no filter can be found in Figures 29-32.
0.00E+00
5.00E+04
1.00E+05
1.50E+05
2.00E+05
2.50E+05
60 80 100 120 140
Noise
(keV
/sqrt(k
J*cm
^2))
kVp
TissueSetupNoiseNoFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

35
Figure 25: dSNRbone values for 1 HVL aluminum filter.
Figure 26: dSNRbone values for 1 HVL copper filter.
120140160180200220240260280300320
60 80 100 120 140
dSNR
kVp
dSNRbone1HVLAluminumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
120140160180200220240260280300
60 80 100 120 140
dSNR
kVp
dSNRbone1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

36
Figure 27: dSNRbone values for 1 HVL gadolinium filter.
Figure 28: dSNRbone values for no filter.
120140160180200220240260280300
60 80 100 120 140
dSNR
kVp
dSNRbone1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
120
170
220
270
320
370
420
470
60 80 100 120 140
dSNR
kVp
dSNRboneNoFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

37
Figure 29: dSNRair values for 1 HVL aluminum filter.
Figure 30: dSNRair values for 1 HVL copper filter.
120
220
320
420
520
620
60 80 100 120 140
dSNR
kVp
dSNRair1HVLAluminumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
120
220
320
420
520
620
60 80 100 120 140
dSNR
kVp
dSNRair1HVLCopperFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

38
Figure 31: dSNRair values for 1 HVL gadolinium filter.
Figure 32: dSNRair values for no filter.
120
220
320
420
520
620
60 80 100 120 140
dSNR
kVp
dSNRair1HVLGadoliniumFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE
120220320420520620720820
60 80 100 120 140
dSNR
kVp
dSNRairNoFilter
AbsorbedEnergy(**)
AbsorbedEnergy(*)
PENELOPE

39
The dSNRbone efficiencies for 1 HVL filters from DXSPEC and Penelope can be
found in Figures 33 and 34. The dSNRair efficiencies for 1 HVL filters from DXSPEC and
Penelope can be found in Figures 35 and 36.
Figure 33: Calculated dSNRbone Efficiency values from DXSPEC for 1 HVL filters.
0.00E+00
1.00E-06
2.00E-06
3.00E-06
4.00E-06
5.00E-06
6.00E-06
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRboneEfficienciesDXSPEC1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter

40
Figure 34: Calculated dSNRbone Efficiency values from Penelope for 1 HVL filters.
Figure 35: Calculated dSNRair Efficiency values from DXSPEC for 1 HVL filters.
0.00E+001.00E-062.00E-063.00E-064.00E-065.00E-066.00E-067.00E-068.00E-069.00E-06
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRboneEfficienciesPenelope1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter
0.00E+00
2.00E-06
4.00E-06
6.00E-06
8.00E-06
1.00E-05
1.20E-05
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRairEfficienciesDXSPEC1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter

41
Figure 36: Calculated dSNRair Efficiency values from Penelope for 1 HVL filters.
The 2 HVL filter thicknesses were run on DXSPEC, analyzed, then only the
“best” filter was run through Penelope. The 2 HVL DXSPEC dSNR efficiencies can be
found in Figures 37 and 38.
0.00E+00
5.00E-06
1.00E-05
1.50E-05
2.00E-05
2.50E-05
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRairEfficienciesPenelope1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter

42
Figure 37: Calculated dSNRbone Efficiency values from DXSPEC for 2 HVL filters.
Figure 38: Calculated dSNRair Efficiency values from DXSPEC for 2 HVL filters.
0.00E+00
1.00E-06
2.00E-06
3.00E-06
4.00E-06
5.00E-06
6.00E-06
7.00E-06
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRbone EfficienciesDXSPEC2HVLFilters
Aluminum
Copper
Gadolinium
0.00E+00
2.00E-06
4.00E-06
6.00E-06
8.00E-06
1.00E-05
1.20E-05
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
dSNRair EfficienciesDXSPEC2HVLFilters
Aluminum
Copper
Gadolinium

43
2.3 Spectrum Modeling Discussion and Conclusions
2.3.1 DXSPEC and Penelope Dose, Signal, and Noise Comparisons
The DXSPEC and Penelope results for the dose, signal, and noise results were
considered in light of anticipated findings. For the dose to the tissue, it was expected
that DXSPEC absorbed energy (*) would underestimate dose, and DXSPEC absorbed
energy (**) would overestimate dose. When comparing the results from the DXSPEC
runs and the Penelope runs, the Penelope dose fell in between the two DXSPEC doses,
thus confirming expected results.
When the DXSPEC code was previously validated, the results showed that the
signal measured in DXSPEC was lower than the signal measured experimentally [9].
This was attributed to incomplete modeling of Auger electrons and other secondary
reactions within the detector thickness. The signal results from Penelope showed a
greater signal in the detector than the two sets of DXSPEC results. This is due to the
better modeling of Auger electrons and secondary reactions over short distances in
Penelope than in DXSPEC.
The calculated noises from Penelope for 60, 80, and 100 kVp are slightly higher
than the noises calculated within DXSPEC; however, the noises calculated in Penelope
for 120 kVp are very similar to the DXSPEC absorbed energy (**) noise calculations, and
the 140 kVp calculated noise from Penelope falls between the absorbed energy (*) and

44
the absorbed energy (**) noises. The noise calculated from Penelope for each filter type
followed this trend.
2.3.2 DXSPEC and Penelope dSNR Comparisons
As seen in Figures 25 through 32 above, the dSNR values vary more between the
different beam filters than any of the other results. The dSNR values, both bone and air,
from DXSPEC follow the same general shape for each filter, but the Penelope results do
not. The Penelope dSNRbone values for both 1 HVL of copper and 1 HVL of aluminum
follow very closely with the calculated dSNRbone values from DXSPEC absorbed energy
(**). In fact, for these two filters, the absorbed energy (**) dSNRbone values lie within the
error bars of the Penelope dSNRbone values. The dSNR error was calculated using the
propagation of error. The propagation of error for a given function R=R(x,y,…) is
defined as,
𝜎o =𝜕𝑅𝜕𝑥
𝜎Qc
+𝜕𝑅𝜕𝑦
𝜎sc
+ ⋯ (12)
where sR is the error, or standard deviation in the function R, sx is the standard
deviation of x, and sy is the standard deviation of y. Applying this to the dSNR
equation, the error in the dSNR is defined as
𝜎uvwo =1𝑁S
𝜎xc+
1𝑁S
𝜎xSc+
𝐼 − 𝐼S𝑁Sc
𝜎wS
c
(13)
where I refers to the signal in the target, Ib refers to the signal in the background, Nb
refers to the noise in the background, and s refers to standard deviation. The target

45
refers to either the bone or air setup and the background refers to the tissue setup. The
statistical uncertainty within the Penelope results was used as the standard deviation for
each signal measurement, while the standard deviation of the noise was calculated
based on the propagation of error of the calculated noise.
The dSNRbone values for both 1 HVL gadolinium filter and no filter don’t follow
either DXSPEC result closely, instead, the lowest kVp values show the Penelope
dSNRbone values to be closer to the absorbed energy (*) results. At 80 kVp, the Penelope
dSNRbone values and the absorbed energy (**) dSNRbone values are almost equal, but then
for 100, 120, and 140 kVp the Penelope dSNRbone values are higher than the absorbed
energy (**) values. The 1 HVL gadolinium and no filter Penelope dSNRair values follow
the same trend as the dSNRbone values for the same filter materials. The 1 HVL
aluminum and copper Penelope dSNRair have the same basic shape as the gadolinium
and no filter, only shifted to above the absorbed energy (**) values.
2.3.3 Final Spectrum Modeling Discussion and Conclusions
The major source of difference between the Penelope dSNR calculations and the
DXSPEC dSNR calculations is the noise estimation from Penelope. Although the
DXSPEC signal results were shown to be too low, the ratios between the results have
previously been validated [9]. On the other hand, Penelope Monte Carlo is a well-
established way to calculate dose, while the DXSPEC dose calculations have not been
previously validated. This means, that in order to get a better understanding of dSNR

46
Efficiency, the dSNR values from DXSPEC can be used in equations (3) and (4) with the
dose values from Penelope. Combining the two different methods gives dSNR
efficiencies that can be found in Figures 39 and 40.
Figure 39: Combined dSNRbone efficiencies for 1 HVL filters.
0.00E+00
1.00E-06
2.00E-06
3.00E-06
4.00E-06
5.00E-06
6.00E-06
7.00E-06
8.00E-06
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
CombineddSNRbone Efficiencies1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter

47
Figure 40: Combined dSNRair efficiencies for 1 HVL filters.
Figures 39 and 40 clearly show that copper has the highest dSNR efficiency for all
but one kVp value. For this reason, copper was chosen as the optimal filter to use for
both the full CT dose simulations and image acquisition and reconstruction.
After copper was chosen to be the best for all of the 1 HVL filters, it could be
compared to 2 HVL copper filter. The DXSPEC dSNR values for the 2 HVL filters as seen
in figures 37 and 38, shows copper to be the best 2 HVL filter. Comparing 1 HVL of
copper to 2 HVL of copper does show a slight increase in the dSNR efficiencies.
However, doubling the filter thickness would mean having to douple the tube loading,
which for the LCCT system is not feasible. Therefore, a 1 HVL copper filter was
determined to be the optimal filter for the LCCT system.
0.00E+00
2.00E-06
4.00E-06
6.00E-06
8.00E-06
1.00E-05
1.20E-05
1.40E-05
1.60E-05
60 80 100 120 140
Efficiency
((kJ*cm
^2)/keV)
kVp
CombineddSNRair Efficiencies1HVLFilters
Aluminum
Copper
Gadolinium
NoFilter

48
3. CT Dose Simulation and Image Reconstruction After the optimal filter type and thickness were found, the CT images could be
acquired using the XCAT projector, reconstructed using a Feldkamp algorithm, and the
dose could be calculated using Penelope.
3.1 Simulation and Reconstruction Methods
3.1.1 XCAT Projector Methods
The XCAT projector developed by Segars et al. [13] is an accurate way to acquire
projection images, which can then be used to reconstruct CT images. The projector uses
computer graphic ray tracing techniques to accurately calculate the CT projections for
the XCAT phantom. The projector program uses input parameters to model different CT
scanners and setups. This allowed for the XCAT projector to produce projections for the
LCCT setup.
The required CT setup input parameters and corresponding LCCT parameters
can be found in table 2. The LCCT setup source to patient distance is 153 cm and the
source to detector distance is 180 cm, which means that the patient to detector distance is
27 cm. The detector used is 41 cm by 41 cm, this models an available detector that can be
used with the LCCT setup. The number of rows and channels determine the number of
pixels in the detector, and using 512 by 512 will be sufficient for the purpose of this
study. The fan angle of the LCCT system is 14.96 degrees; this was calculated from the
LCCT setup to irradiate 40 cm of the patient. The mAs per projection was set at 0.05. As

49
stated above, this project included no mAs optimization, because of power and tube
loading constraints that will be present for the actual system. Because of this, a low
value of mAs was chosen and used for each kVp value so that the all of the images could
be compared. The geometric efficiency of the detector was set to 0.8, the detector shift
was set to -0.25, the electronic noise was turned off by setting the variance to 0, and the
subvoxel index was set to 1.
Table 2: XCAT Projector Input Parameters
LCCTParameterValue NeededProjectorInputParameter0 :output_type(0=log_transformed,1=intensity_output,2=both)0 :organ_to_center_projection(0=body)
1530 :distance_to_source(mms)270 :distance_to_detector(mms)410 :height(mms)410 :width(mms)512 :num_rows512 :num_channels7.48 :Half_fan_angle0.05 :mAs_per_projection0.8 :Geometric_efficiency_detector
-0.25 :detector_shift0 :variance_of_electronic_noise1 :subvoxel_index
In order to produce a projection with the XCAT projector, along with the
parameter file that defines the above parameters, a phantom file, a spectrum file, and a
projection angle are needed. The phantom file is generated from the XCAT phantom.
The desired phantom can be scaled or shifted as desired. For the LCCT system, four
different XCAT phantoms were chosen: two female and two male. The phantoms chosen

50
can be found in Table 3. These phantoms were chosen to model a range of diverse
patient sizes.
Table 3: XCAT Phantoms used in the XCAT projector.
Label Age Weight(kg) WeightPercentile Height(cm) BMIFemale1 66 66.4 48.8 162 25.3Female2 16.8 50.5 28 158.7 20.05Male1 31 77.9 49.1 185.2 22.71Male2 15 42.2 4 162.5 15.98
The spectrum files that were used as inputs for the projector, were the spectra
generated by DXSPEC for 60, 80, 100, 120, and 140 kVp beams filtered by 1 HVL of
copper. The projector was run for even angles from 0 to 358. Previous work with the
LCCT setup determined that a sufficient image could be reconstructed from 180
projections, and the fewer projections taken, the lower the dose.
3.1.2 Image Reconstruction Methods
After all of the projections had run, there were 180 projections for each kVp value
for each patient. These projections were then reconstructed using a Feldkamp algorithm.
The Feldkamp algorithm has been implemented into a MATLABTM (MathWorks, Natick,
MA) code. This MATLAB code was used to generate all the CT images for this thesis.
The MATLAB Feldkamp code needed inputs are shown in Table 4 with the
corresponding LCCT parameters. The projection angles in Table 3 start at 90 and end at -
268 because the XCAT projector and the reconstruction algorithm have a different
definition of 0 degrees and rotate in the opposite directions.

51
Table 4: MATLAB CT reconstruction input parameters.
Variable LCCTValue VariableExplinationtheta 90:-2:-270 ProjectionAnglesu_off 256.5 Locationofthecenterintheudirectionv_off 256.5 Locationofthecenterinthevdirectionweights 1 WeightofeachprojectionN_proj 180 NumberofprojectionsN_row 512 NumberofrowsN_col 512 NumberofColumnsdu 0.0801 PixelThicknessintheudirectiondv 0.0801 PixelThicknessinthevdirectionSAD 153 SourcetoPt.CenterDistanceSDD 180 SourcetoDetectorDistanceIAD 27 Pt.CentertoDetectorDistance
After the input parameters and the projection data are put into MATLAB the
filtered back projection Feldkamp reconstruction algorithm for flat panel detectors was
run and the CT images were acquired.
3.1.3 LCCT Simulation Methods
The Penelope code used to model the full LCCT setup was a modified version of
the tube current modulation (TCM) code developed and validated. The adaptations of
the TCM code were made in the input files. The TCM Penelope code was designed to
simulate CT scans in which the tube current is modulated across the patient to reduce
dose. For the LCCT simulation, the modulation was turned off and the other parameters
were changed to reflect the LCCT setup. First, the four phantoms that were used in the
image acquisition, were reconfigured to be compatible with the TCM simulation
package. The phantoms were saved as two raw files, one with the organ labels

52
embedded and the other with the material labels embedded. The updated input
parameters can be found in Table 5.
Table 5: TCM Simulation Input Parameters
Variable Value Explination#patient pt001 PatientIdentifier--uniqueforeachsimulation
inplane_resmm 3.45 PhantomPixelDimensionslongaxis_resmm 3.45 PhantomPixelDimensions
Norg 53 NumberofOrgansorgfile Female1_org_202_475_101.raw OrganFileNmat 24 NumberofMaterialsmatfile Female1_mat_202_475_101.raw MaterialFilematdata 42pts.mat MaterialDataYstart 128 StartingPixelLocationintheYdirection
start_offset(cm) 1Yend 128 EndingPixellocationintheYdirection
end_offset(cm) 1gantry_angle_dist_file na ModulationFile
kVp 60spcfile 60kVpCu1HVL.txt SpectrumFileSID(cm) 153 DistancefromtheSourcetoCenterofthePt.
FanAng(deg) 14.96 FullFanAnglecolli(mm) 0 CollimationThickness
EffBeamWidth(mm) 402 EffectiveBeamWidthattheCenterofthePt.pitch 0
sta_ang(deg) 0 StartAngleXdim 202 PhantomDimensionsYdim 475 PhantomDimensionsZdim 101 PhantomDimensionsXcenter 101 CenterXPixelZcenter 50 CenterZPixel
The patient identifier was changed for each run of the simulation. The phantom
pixel dimensions were in reference to the phantom used in the simulation. Because this

53
simulation usually models traditional CT, the y-direction is the direction from head to
foot, which in the LCCT setup is the z-direction. The modulation was turned off, so the
modulation file was not included. The spectrum file and kVp values changed to run the
simulation through each of the five kVp values for each of the four phantoms. The
collimation was originally used to determine scan length, but for the LCCT system, the
scan length is zero because there is no patient translation throughout the scan. The
effective beam width is the width of the beam at the center of the patient.
Each phantom/kVp combination was run through the simulation 15 times in
parallel, to reduce overall run time. The dose results from the 15 runs were then
averaged together to produce the final dose results for each phantom/kVp combination.
The dose in units of mGy per mAs, was then converted to mSv per mAs using the tissue
weighting factors from ICRP 103.
3.2 Simulation and Reconstruction Results
3.2.1 Imaging Results
The reconstructed CT images for the phantom Female 1 are found in figure 41.
The reconstructed CT images for Female 2 are found in figure 42. Male 1 reconstructed
CT images are found in figure 43. Male 2 reconstructed CT images are displayed in
figure 44.

54
Figure 41: Reconstructed CT images for Female 1 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp.
Figure 42: Reconstructed CT images for Female 2 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp.

55
Figure 43: Reconstructed CT images for Male 1 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp.
Figure 44: Reconstructed CT images for Male 2 phantom for (a) 60 kVp, (b) 80 kVp, (c) 100 kVp, (d)120 kVp, and (e) 140 kVp.

56
3.2.2 Simulation Results
The dose to the lungs calculated for each phantom and kVp combination are
displayed in Table 6.
Table 6: Dose to Lung and Effective Dose results for each phantom and kVp value combination.
Phantom kVp LungDose(mGy/mAs) EffectiveDose(mSv/mAs)60 1.59E-04 8.63E-0580 2.73E-04 1.47E-04
100 3.57E-04 1.94E-04120 4.10E-04 2.24E-04140 4.47E-04 2.44E-0460 1.74E-04 1.07E-0480 2.97E-04 1.78E-04
100 3.89E-04 2.29E-04120 4.44E-04 2.61E-04140 4.85E-04 2.85E-0460 1.53E-04 5.36E-0580 2.67E-04 9.71E-05
100 3.49E-04 1.29E-04120 4.03E-04 1.52E-04140 4.39E-04 1.66E-0460 2.03E-04 8.22E-0580 3.34E-04 1.40E-04
100 4.21E-04 1.82E-04120 4.78E-04 2.09E-04140 5.17E-04 2.28E-04
Female1
Female2
Male1
Male2
In order to calculate the dSNR for the reconstructed images, the signal in the
different tissue types and the noise in the image needed to be determined. To find the
noise, each image was generated twice, once with the noise turned off, then with noise
turned on. The image with no noise was subtracted from the noisy image to find the

57
noise print. The standard deviation of the pixel values in the noise print was used as the
noise. To find the signals in each of the tissue types, regions of interest were drawn.
These regions of interest corresponded to the different tissue types. The average signal
within these regions of interest was used as the signal from that tissue type. After the
signals and noise were found, the dSNR was calculated, then used along with the doses
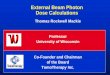
in Table 6 to calculate the dSNR efficiencies. The dSNRbone efficiencies for lung dose for
each phantom can be found in figures 45 and the dSNRbone efficiencies using effective
dose (ED) can be found in Figure 46. The dSNRair efficiencies using lung dose can be
found in Figure 47 and the dSNRair efficiencies using ED can be found in Figure 48.
Figure 45: dSNRbone Efficiencies calculated using lung dose for each phantom.
0.00E+00
1.00E+06
2.00E+06
3.00E+06
4.00E+06
5.00E+06
6.00E+06
7.00E+06
8.00E+06
60 80 100 120 140
Efficiency
(mAs/m
Gy)
kVp
dSNRboneLungDoseEfficiency
Female1
Female2
Male1
Male2

58
Figure 46: dSNRbone Efficiencies calculated using effective dose for each phantom.
Figure 47: dSNRair Efficiencies calculated using lung dose for each phantom.
0.00E+00
2.00E+06
4.00E+06
6.00E+06
8.00E+06
1.00E+07
1.20E+07
1.40E+07
60 80 100 120 140
Efficiency
(mAs/m
Sv)
kVp
dSNRBoneEDEfficiency
Female1
Female2
Male1
Male2
0.00E+00
1.00E+06
2.00E+06
3.00E+06
4.00E+06
5.00E+06
6.00E+06
60 80 100 120 140
Efficiency
(mAs/m
Gy)
kVp
dSNRAirLungDoseEfficiency
Female1
Female2
Male1
Male2

59
Figure 48: dSNRair Efficiencies calculated using effective dose for each phantom.
3.3 Simulation and Reconstruction Conclusions and Discussion
The CT images in Figures 41 through 44 show that the main contributing factor
to poor image quality is the under-sampling artifacts caused by only using 180
projections. For dSNRbone efficiency, the lower kVp values have a higher efficiency than
the higher kVp values. However, for dSNRair the efficiencies for the higher kVp values
are higher than the lower kVp values.
The average ED for a clinical diagnostic chest CT scan is about 7 millisieverts
(mSv), with a range of 4 - 18 mSv [16]. In order to produce a dose close to 7 mSv, the
LCCT system would have to be operated at almost 50,000 mAs. Although this project
did not explore optimal mA settings, running the system at 50,000 mAs does not seem
feasible due to the available power sources in the places these system will be used.
0.00E+001.00E+062.00E+063.00E+064.00E+065.00E+066.00E+067.00E+068.00E+069.00E+061.00E+07
60 80 100 120 140
Efficiency
(mAs/m
Sv)
kVp
dSNRAirEDEfficiency
Female1
Female2
Male1
Male2

60
Which means that the patients scanned on the LCCT system will receive a dose that falls
within clinically accepted dose.
The optimal kVp to run the LCCT system at to get the optimal beam spectrum
and dose depends on what is being imaged. For studies that favor bone contrast, such as
lung studies, the optimal dSNR efficiency occurs at the lower kVp values such as 60 and
80 kVp. For studies that favor air contrast, the optimal dSNR efficiency occurs at higher
kVp values, such as 140 kVp.

61
4. Conclusions The results from this thesis show that the optimal beam parameters for the LCCT
setup are 1 HVL filter of copper and 60 or 80 kVp for studies favoring bone contrast and
140 kVp for studies favoring air contrast, such as chest scans. Although the images
produced by these parameters are inferior to state-of-the-art CT images, they provide for
the first time volumetric imaging feasible for much of the developing world. The LCCT
could provide the developing world a more affordable way to acquire volumetric
imaging. Although the mAs was not optimized in this work, in order to produce doses
similar to state-of-the-art CT scanners, the LCCT system would have to be run at almost
50,000 mAs. Detectability studies need to be performed in order to determine the
optimal mAs setting, but it should be less than 50,000 mAs, which means that the LCCT
system will not introduce the patients to any more radiogenic risk than a state-of-the-art
CT.
Moving forward, the next likely step for the LCCT development is to build a
working prototype. This way, the tube loading concerns can be explored and the mAs
can be optimized. Another logical step is to look further into comparing the
reconstructed CT images. For this work, the CT images were not looked at by
radiologists, and were solely judged on physical measures of image quality. For
radiologists, a physical metric of image quality value does not always correspond to the
clinical utility of an image. Giving radiologists the images for each kVp value and asking

62
them to select the most useful image would allow additional data for determining which
image is the best.
After the best images have been determined by radiologists, the prototype has
been built, and the mAs optimized, the LCCT system can begin to be implemented in
developing countries. When the LCCT system is implemented in developing countries,
the quality of medicine readily available can start improving. And as the quality of
medicine starts improving, so does the quality of life.

63
References 1. Dobbins III, J.T., et al. Initial investigation into lower-cost CT for resource limited
regions of the world. in SPIE Medical Imaging. 2010. International Society for Optics and Photonics.
2. Doi, K., Diagnostic imaging over the last 50 years: research and development in medical imaging science and technology. Physics in medicine and biology, 2006. 51(13): p. R5.
3. OECD. Computed Tomography (CT) scanners. 2016 October 13, 2016]; Available from: https://data.oecd.org/healtheqt/computed-tomography-ct-scanners.htm.
4. WorldHealthOrganization. Medical Equipment Data by country. Global Health Observatory data repository 2016; Available from: http://apps.who.int/gho/data/node.main.510.
5. Wells, J.R., Correlated Polarity Noise Reduction: Development, Analysis, and Application of a Novel Noise Reduction Paradigm. 2013, Duke University.
6. Hubbell, J.H. and S.M. Seltzer, Tables of X-ray mass attenuation coefficients and mass energy-absorption coefficients 1 keV to 20 MeV for elements Z= 1 to 92 and 48 additional substances of dosimetric interest. 1995, National Inst. of Standards and Technology-PL, Gaithersburg, MD (United States). Ionizing Radiation Div.
7. Huda, W., Review of Radiologic Physics. 2010: Lippincott Williams & Wilkins.
8. Ergun, D., et al., DXSPEC: a computer program for diagnostic x-ray spectral filtration studies. Madison, Wis: University of Wisconsin-Madison Department of Medical Physics, 1977.
9. Dobbins, J.T., et al., Chest radiography: optimization of x-ray spectrum for cesium iodide–amorphous silicon flat-panel detector 1. Radiology, 2003. 226(1): p. 221-230.

64
10. Boone, J.M. and J.A. Seibert, An accurate method for computer-generating tungsten anode x-ray spectra from 30 to 140 kV. Medical physics, 1997. 24(11): p. 1661-1670.
11. Salvat, F., J.M. Fernández-Varea, and J. Sempau. PENELOPE-2006: A code system for Monte Carlo simulation of electron and photon transport. in Workshop proceedings. 2006.
12. Segars, W., et al., 4D XCAT phantom for multimodality imaging research. Medical physics, 2010. 37(9): p. 4902-4915.
13. Segars, W.P., et al., Realistic CT simulation using the 4D XCAT phantom. Medical physics, 2008. 35(8): p. 3800-3808.
14. Segars, W.P. and B.M. Tsui, MCAT to XCAT: The evolution of 4-D computerized phantoms for imaging research. Proceedings of the IEEE, 2009. 97(12): p. 1954-1968.
15. Feldkamp, L., L. Davis, and J. Kress, Practical cone-beam algorithm. JOSA A, 1984. 1(6): p. 612-619.
16. Mettler Jr, F.A., et al., Effective doses in radiology and diagnostic nuclear medicine: a catalog 1. Radiology, 2008. 248(1): p. 254-263.