Embed Size (px)
Citation preview
comprehensive review
Optimizing Management of Tumor Lysis Syndromein Adults with Hematologic Malignancies
Anne-Sophie Michallet, Sophie Tartas, Bertrand Coiffier
Key words: Alkalinization, Allopurinol, Hydration, Hyperuricemia,Rasburicase, Renal failure, Urate oxidase
Abstract
Tumor lysis syndrome (TLS), caused by the release of cellular components into the blood after rapid cell lysis, is a seriousproblem in patients with hematologic malignancies. It is characterized by hyperuricemia, hyperkalemia, hyperphosphatemia, andsecondary hypocalcemia, with serious clinical consequences including renal failure and death. Although TLS may occurspontaneously, it is more commonly caused by the destruction of malignant cells by chemotherapy. The risk of developing TLSis influenced by a number of characteristics including the type of malignancy, the type and intensity of anticancer treatment, andthe presence of preexisting conditions such as renal insufficiency. Particularly, high-risk patients who have malignancies with ahigh rate of cell turnover are highly sensitive to chemotherapy. The identification and prophylactic treatment of patients at highrisk of developing TLS is key to the management of TLS. This review provides a summary of the pathogenesis of TLS, risk factorsfor TLS, its associated incidence and clinical consequences, and pharmacologic options for prevention and treatment.
Hospices Civils de Lyon and Université Claude Bernard, Lyon, FranceAddress for correspondence: Bertrand Coiffier, MD, HematologyDepartment, Hospices Civils de Lyon and Université Claude Bernard, 69495Pierre-Benite Cedex, Lyon, FranceFax: 33-478-866566; e-mail: [email protected]
Submitted: Dec 15, 2004; Revised: Jan 26, 2005; Accepted: Feb 3, 2005Supportive Cancer Therapy, Vol 2, No 3, 159-166, 2005
Volume 2, Number 3 • April 2005
159
IntroductionTumor lysis syndrome (TLS) is a serious problem in
patients with hematologic malignancies.1,2 Beacause it iscaused by the release of cellular components into the bloodafter rapid cell lysis, TLS is characterized by hyperuricemia,hyperkalemia, hyperphosphatemia, and secondary hypocalce-mia. Crystallization of uric acid in the renal tubules con-tributes to impaired renal function. Serious clinical conse-quences of TLS include renal failure and death.3-5 AlthoughTLS may occur spontaneously, especially in patients with ahigh tumor burden, it is more commonly caused by the
destruction of malignant cells by chemotherapy,6-8 and itrarely precedes treatment.9 Therefore, preventing TLS is par-ticularly important in patients receiving chemotherapy forthe treatment of newly diagnosed malignancies.
Pathogenesis of Tumor Lysis Syndromeand Associated Renal Failure
Tumor-cell lysis releases an array of intracellular compo-nents into the blood stream,8,10 including potassium,11
Electronic forwarding or copying is a violation of US and International Copyright Laws.Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by Cancer Information Group, ISSN #1543-2912, provided the appropriate fee is paid directly to Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923 USA 978-750-8400.
Managing Tumor Lysis Syndrome in Adults
Supportive Cancer Therapy
160
phosphate,12 and purines from the breakdown of nuclear pro-teins.9,10 Purines are metabolized to hypoxanthine and xan-thine, which are further degraded in the liver by the enzymexanthine oxidase in order to produce uric acid.8,9 Normally,the serum levels of potassium, phosphate, and uric acid arecontrolled by excretion, primarily by the kidneys.13
However, during TLS, the massive release of potassium,phosphate, and uric acid into the blood overwhelms thebody’s capacity for clearance, resulting in hyperkalemia,hyperphosphatemia, and hyperuricemia.8,9 Uric acid is solu-ble in plasma but poorly soluble in acidic urine, so, as theconcentration of plasma uric acid rises, the potential for theprecipitation of uric acid crystals in the renal tubules alsoincreases.2,14 This deposition of excess uric acid and theresulting obstruction of the renal tubules is central to thedevelopment of renal insufficiency, leading to reducedglomerular filtration, oliguria, and eventually renal fail-ure.9,15 Hyperphosphatemia has also been implicated in thepathogenesis of kidney failure in patients with TLS.16 Excessphosphate in the plasma combines with calcium to form cal-cium–phosphate complexes (CaxP) that may be precipitatedin tissues such as the kidneys.2,10 In addition, removal of cal-cium from the plasma leads to secondary hypocalcemia.
The Incidence of Tumor Lysis SyndromeThe incidence of TLS and the administration of pro-
phylactic medication were evaluated in a retrospective studyof 788 patients, including 433 adults, with acute leukemiaor non-Hodgkin’s lymphoma (NHL).3 This study revealedthat adults were less likely to receive preventative measuresthan children. Overall, 66% of adults and 94% of childrenhad primary prophylaxis to avoid TLS, and 19.7% of
patients had slow-start chemotherapy to reduce the risk ofTLS. Even with this level of preventative treatment, 5% ofadult patients still developed TLS (biologic), and of these,45% had acute renal failure and 25% required hemodialysisor hemofiltration.3 The incidence of TLS is lower in adultswith solid tumors compared with adults with hematologicmalignancies, but it is still potentially fatal.17 In a recentreview of all available literature for TLS in patients withsolid tumors, only 45 cases of TLS were recorded, but themortality rate was 1 in 3.17 These results indicate that thelevel of use and the efficacy of prophylaxis could beenhanced.
Risk Factors for Tumor Lysis SyndromeThe risk of TLS is influenced by a number of characteris-
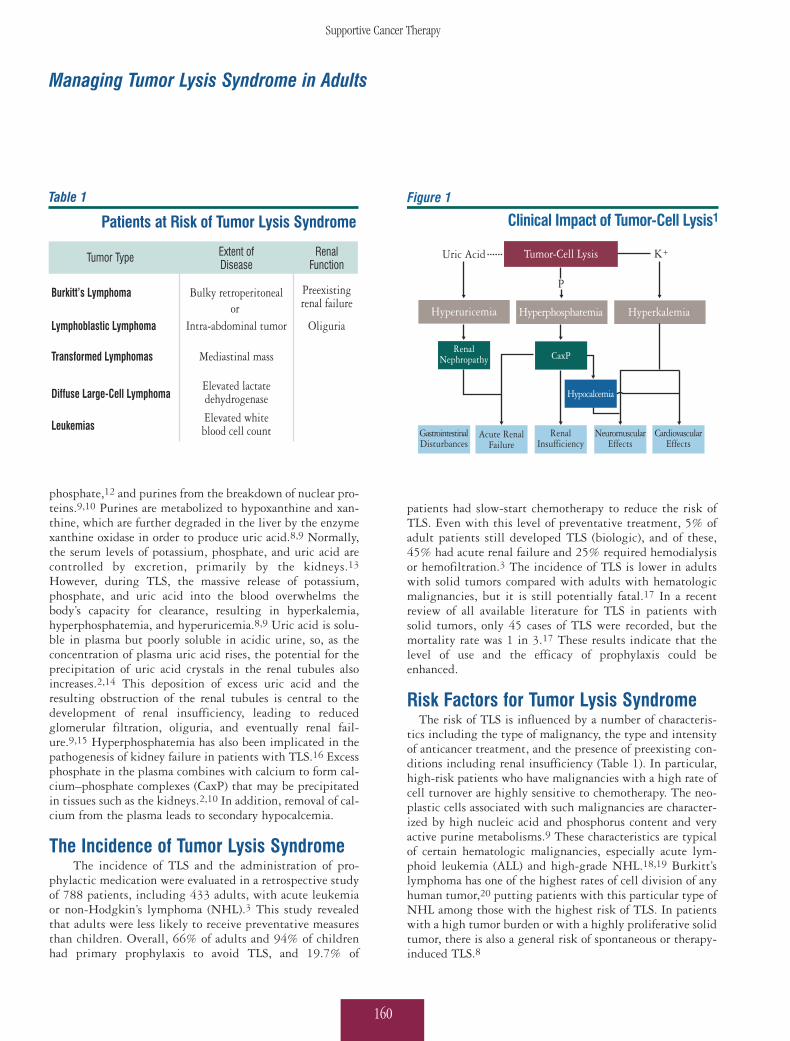
tics including the type of malignancy, the type and intensityof anticancer treatment, and the presence of preexisting con-ditions including renal insufficiency (Table 1). In particular,high-risk patients who have malignancies with a high rate ofcell turnover are highly sensitive to chemotherapy. The neo-plastic cells associated with such malignancies are character-ized by high nucleic acid and phosphorus content and veryactive purine metabolisms.9 These characteristics are typicalof certain hematologic malignancies, especially acute lym-phoid leukemia (ALL) and high-grade NHL.18,19 Burkitt’slymphoma has one of the highest rates of cell division of anyhuman tumor,20 putting patients with this particular type ofNHL among those with the highest risk of TLS. In patientswith a high tumor burden or with a highly proliferative solidtumor, there is also a general risk of spontaneous or therapy-induced TLS.8
Table 1
Patients at Risk of Tumor Lysis Syndrome
Extent ofDisease
RenalFunction
Tumor Type
Bulky retroperitonealor
Intra-abdominal tumor
Mediastinal mass
Elevated lactatedehydrogenase
Elevated whiteblood cell count
Preexistingrenal failure
Oliguria
Burkitt’s Lymphoma
Lymphoblastic Lymphoma
Transformed Lymphomas
Diffuse Large-Cell Lymphoma
Leukemias
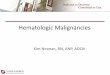
Figure 1
Clinical Impact of Tumor-Cell Lysis1
P
Uric Acid K+Tumor-Cell Lysis
Hyperuricemia
RenalNephropathy
GastrointestinalDisturbances
RenalInsufficiency
NeuromuscularEffects
CardiovascularEffects
Acute RenalFailure
CaxP
Hypocalcemia
HyperkalemiaHyperphosphatemia
Anne-Sophie Michallet et al
Volume 2, Number 3 • April 2005
161
Tumor lysis syndrome generally develops during the first3-4 days of chemotherapy/immunotherapy, and the typeand intensity of the anticancer treatment used influencesthe patient’s overall risk of developing TLS.6,21 Intensivechemotherapy regimens cause rapid and extensive tumor-cell lysis18 and are therefore associated with a particularlyhigh risk of TLS.
Individual therapy and malignancy combinations mayalso carry specific risks for TLS. Patients with chroniclymphocytic leukemia (CLL), for example, are generally atlow risk of developing TLS, but the use of fludarabine inthis particular leukemia may be associated with significantmorbidity and mortality in the small number of patientswho are susceptible to TLS.4 Radiation therapy is also asso-ciated with the development of TLS. For example, severeTLS was reported in a 30-year-old man who had refractoryT-cell ALL and received total body irradiation of only 4 Gyon the first day of reduced-intensity conditioning beforehematopoietic stem cell transplantation (HSCT).22 Thepatient developed extreme biochemical changes, cardiacand neurologic symptoms, and acute renal failure requir-ing dialysis.
A number of preexisting conditions, in particular thoselinked with renal insufficiency and reduced clearance ofuric acid, also increase the risk of TLS. These include dehy-dration, oliguria or anuria, preexisting hyperuricemia,acidic urine, which reduces the solubility and clearance ofuric acid, and renal conditions such as renal insufficien-cy.8,14,23,24
Clinical Consequences of Tumor Lysis Syndrome
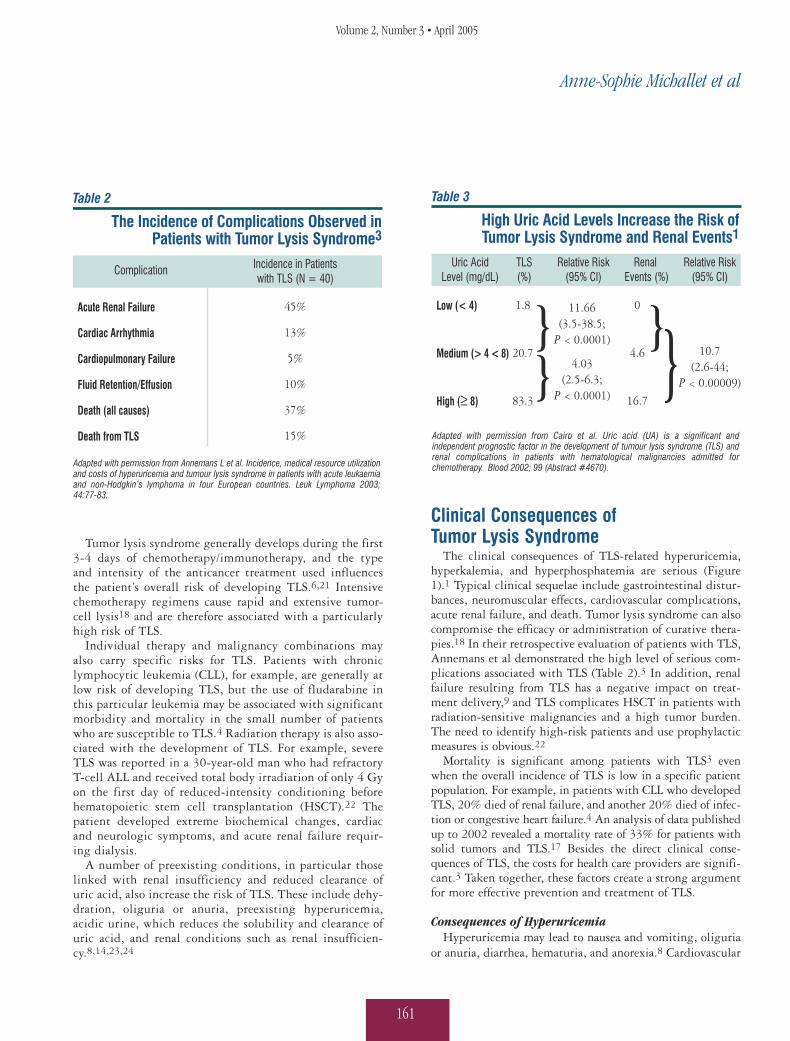
The clinical consequences of TLS-related hyperuricemia,hyperkalemia, and hyperphosphatemia are serious (Figure1).1 Typical clinical sequelae include gastrointestinal distur-bances, neuromuscular effects, cardiovascular complications,acute renal failure, and death. Tumor lysis syndrome can alsocompromise the efficacy or administration of curative thera-pies.18 In their retrospective evaluation of patients with TLS,Annemans et al demonstrated the high level of serious com-plications associated with TLS (Table 2).3 In addition, renalfailure resulting from TLS has a negative impact on treat-ment delivery,9 and TLS complicates HSCT in patients withradiation-sensitive malignancies and a high tumor burden.The need to identify high-risk patients and use prophylacticmeasures is obvious.22
Mortality is significant among patients with TLS3 evenwhen the overall incidence of TLS is low in a specific patientpopulation. For example, in patients with CLL who developedTLS, 20% died of renal failure, and another 20% died of infec-tion or congestive heart failure.4 An analysis of data publishedup to 2002 revealed a mortality rate of 33% for patients withsolid tumors and TLS.17 Besides the direct clinical conse-quences of TLS, the costs for health care providers are signifi-cant.3 Taken together, these factors create a strong argumentfor more effective prevention and treatment of TLS.
Consequences of HyperuricemiaHyperuricemia may lead to nausea and vomiting, oliguria
or anuria, diarrhea, hematuria, and anorexia.8 Cardiovascular
Table 2
The Incidence of Complications Observed in Patients with Tumor Lysis Syndrome3
Incidence in Patientswith TLS (N = 40)
Complication
Acute Renal Failure
Cardiac Arrhythmia
Cardiopulmonary Failure
Fluid Retention/Effusion
Death (all causes)
Death from TLS
45%
13%
5%
10%
37%
15%
Adapted with permission from Annemans L et al. Incidence, medical resource utilization and costs of hyperuricemia and tumour lysis syndrome in patients with acute leukaemia and non-Hodgkin’s lymphoma in four European countries. Leuk Lymphoma 2003; 44:77-83.
Table 3
High Uric Acid Levels Increase the Risk of Tumor Lysis Syndrome and Renal Events1
Relative Risk(95% CI)
Uric AcidLevel (mg/dL)
TLS(%)
Low (< 4)
Medium (> 4 < 8)
High (≥ 8)
11.66(3.5-38.5;
P < 0.0001)
4.03(2.5-6.3;
P < 0.0001)
Renal Events (%)
0
4.6
16.7
Relative Risk(95% CI)
10.7(2.6-44;
P < 0.00009)
1.8
20.7
83.3
Adapted with permission from Cairo et al. Uric acid (UA) is a significant and independent prognostic factor in the development of tumour lysis syndrome (TLS) and renal complications in patients with hematological malignancies admitted for chemotherapy. Blood 2002; 99 (Abstract #4670).

Managing Tumor Lysis Syndrome in Adults
Supportive Cancer Therapy
162
disease has also been linked with hyperuricemia.25 However,acute renal failure represents one of the most frequent, seri-ous clinical consequences of TLS and hyperuricemia.3Another study that analyzed the importance of uric acid inthe development of TLS used logistical regression to investi-gate evidence of renal events in 83 patients with NHL whowere admitted to the hospital for chemotherapy. High andeven normal levels of uric acid were significantly associatedwith an increased risk of TLS and renal events (Table 3).1 Forevery 1 mg/dL increase in uric acid, the risk of TLS increasedby a factor of 1.7 (95% confidence interval [CI] 1.41, 2.17;P < 0.0001), and risk of a renal event increased by 2.21 (95%CI, 1.32, 3.56; P = 0.0012). Overall, the incidence of renalevents (16.7%) in patients with high uric acid levels was signif-icantly higher than in those with low or normal uric acid levels(relative risk 10.7; 95% CI, 2.6-44; P < 0.00009).1 It is clearthat careful monitoring and management of uric acid levels areessential to the identification of patients at high risk of TLS.
Consequences of Hyperkalemia and HyperphosphatemiaHyperkalemia, hyperphosphatemia, and secondary hypo-
calcemia may lead to serious clinical consequences in additionto those caused by hyperuricemia. High potassium levels(plasma concentrations of > 6.5 mmol/L) can be life threaten-ing, potentially causing serious cardiac disturbances includ-ing arrhythmias, ventricular tachycardia, fibrillation, and car-diac arrest.8 High potassium levels may also cause neuromus-cular effects including muscle cramps and paresthesia. Highphosphate levels may lead to renal insufficiency, anuria, oroliguria because of the formation of CaxP in the kidneys,2,10
and the deposition of these complexes can cause renal failure.Secondary hypocalcemia can, in turn, lead to cardiovasculareffects such as arrhythmia and hypotension and neuromuscu-lar effects including tetany and muscle cramp.8
Prevention and Management of Tumor Lysis SyndromePrevention of Tumor Lysis Syndrome
Prevention is key to the management of TLS,8 and, despitethe serious clinical consequences of advanced TLS, it can beprevented in most patients.17 The best strategy for prevent-ing and treating TLS is careful monitoring and promptaction. Prophylaxis for TLS should begin before treatment forNHL or leukemia starts26 and continue for 3-7 days.27
Therapeutic Options to Prevent and Manage the Clinical Consequences of Tumor Lysis Syndrome
Tumor lysis syndrome–related hyperuricemia can be pre-vented and managed by vigorous hydration to increase elim-ination of uric acid, diuresis to maintain urine output, urinary
alkalinization to increase solubility of uric acid in urine, andthe use of agents such as allopurinol or recombinant urate oxi-dase (rasburicase) to reduce plasma uric acid levels.26-28
Alkalinization of urine is widely used but controversialbecause, although alkalinization reduces the likelihood of uricacid precipitation, it also increases the precipitation of CaxP.Although their role is not fully understood, these complexesmay contribute to nephropathy and lead to a reducedglomerular filtration rate and acute renal failure.
Brant reviewed the management of TLS-related hyperuri-cemia7 and found that management commonly included vig-orous intravenous (I.V.) hydration of 3-6 L/m2 per day; uri-nary alkalinization with 50-100 mEq/L of sodium bicarbon-ate to maintain the urine pH at 7-7.5; reduction of uric acidproduction with rasburicase (0.20 mg/kg per day for 5-7days) or allopurinol (200-400 mg/m2 per day I.V. or 300-800mg per day orally); and diuretics as needed to prevent fluidoverload. Urinary alkalinization using sodium bicarbonateenhances the excretion of uric acid in the urine,28 becausebuffering to ≥ pH 7 maintains uric acid in its ionized form,reducing deposition of uric acid crystals in the renal tubules.8However, the treatment strategies for managing TLS varysignificantly from country to country, with many countriesfollowing their own national guidelines. Even within thesame country, hematologists will use varying combinationsof the therapeutic options available to them. However, it isclear that each patient should be evaluated thoroughly,assessed for individual risk of developing TLS, and treatedearly and appropriately.
Although hydration is often used as the first option, thecourse of treatment determined by the physician will bedependent on the risk assessment. In our clinical practice, forexample, patients with early symptoms of TLS such as hyper-uricemia, hyperphosphatemia, or increased creatinine levelare treated with vigorous hydration (to maintain urine out-flow > 1 L every 6 hours) and rasburicase before beginningchemotherapy. For patients at risk but without early biolog-ic symptoms, the same regimen is used to maintain > 1 L ofurine outflow every 8 hours.
Allopurinol and rasburicase, the 2 agents that are current-ly available to reduce uric acid levels in patients with TLS,are discussed in further detail.
AllopurinolAllopurinol has been widely used for many years and is
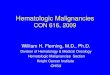
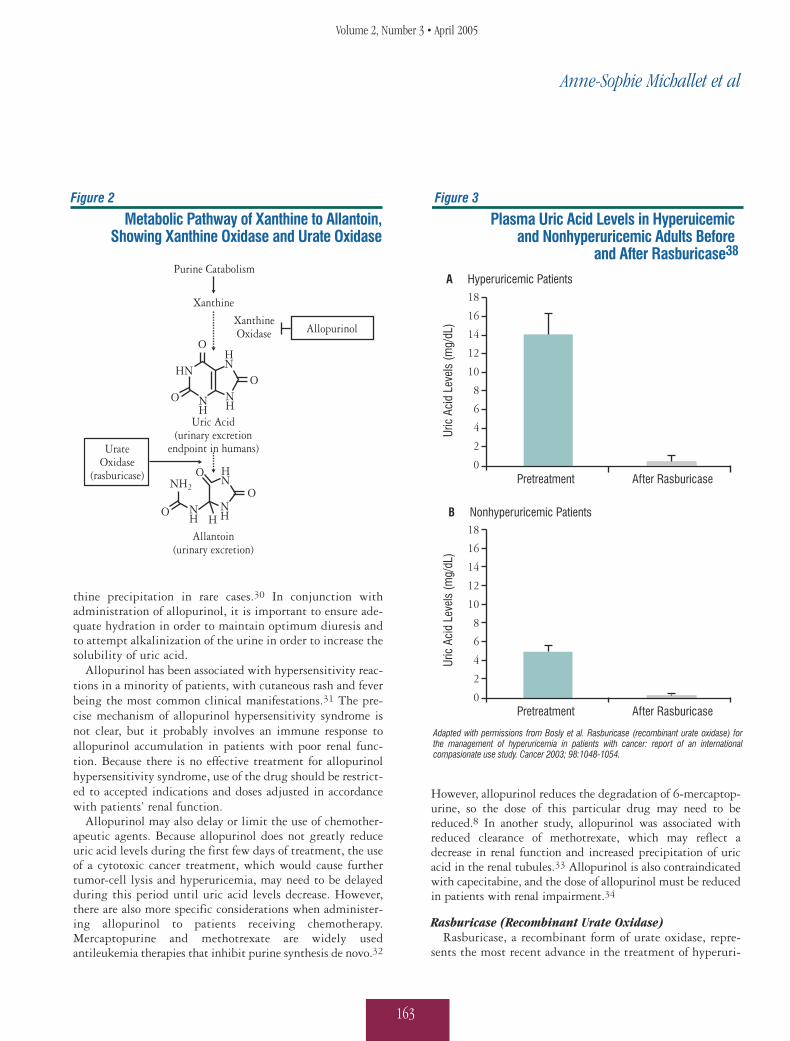
standard therapy in the United States for controlling hyper-uricemia in adult patients.29 Allopurinol, a structural ana-logue of the purine base hypoxanthine with a plasma half-lifeof 1-2 hours, reduces the formation of uric acid by inhibitingthe action of xanthine oxidase, the enzyme responsible for theconversion of hypoxanthine to xanthine and xanthine to uricacid (Figure 2). Because of the action of allopurinol, anaccumulation of xanthine may be observed leading to xan-
Anne-Sophie Michallet et al
Volume 2, Number 3 • April 2005
163
thine precipitation in rare cases.30 In conjunction withadministration of allopurinol, it is important to ensure ade-quate hydration in order to maintain optimum diuresis andto attempt alkalinization of the urine in order to increase thesolubility of uric acid.
Allopurinol has been associated with hypersensitivity reac-tions in a minority of patients, with cutaneous rash and feverbeing the most common clinical manifestations.31 The pre-cise mechanism of allopurinol hypersensitivity syndrome isnot clear, but it probably involves an immune response toallopurinol accumulation in patients with poor renal func-tion. Because there is no effective treatment for allopurinolhypersensitivity syndrome, use of the drug should be restrict-ed to accepted indications and doses adjusted in accordancewith patients’ renal function.
Allopurinol may also delay or limit the use of chemother-apeutic agents. Because allopurinol does not greatly reduceuric acid levels during the first few days of treatment, the useof a cytotoxic cancer treatment, which would cause furthertumor-cell lysis and hyperuricemia, may need to be delayedduring this period until uric acid levels decrease. However,there are also more specific considerations when administer-ing allopurinol to patients receiving chemotherapy.Mercaptopurine and methotrexate are widely usedantileukemia therapies that inhibit purine synthesis de novo.32
However, allopurinol reduces the degradation of 6-mercaptop-urine, so the dose of this particular drug may need to bereduced.8 In another study, allopurinol was associated withreduced clearance of methotrexate, which may reflect adecrease in renal function and increased precipitation of uricacid in the renal tubules.33 Allopurinol is also contraindicatedwith capecitabine, and the dose of allopurinol must be reducedin patients with renal impairment.34
Rasburicase (Recombinant Urate Oxidase)Rasburicase, a recombinant form of urate oxidase, repre-
sents the most recent advance in the treatment of hyperuri-
Figure 2
Metabolic Pathway of Xanthine to Allantoin,Showing Xanthine Oxidase and Urate Oxidase
Purine Catabolism
Xanthine
Uric Acid(urinary excretion
endpoint in humans)
Allantoin(urinary excretion)
UrateOxidase
(rasburicase)
XanthineOxidase
O
O
O
OH
OO
NH2
HN
HN
NHN
H
NH
NH
Allopurinol
HN
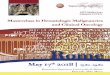
Figure 3
A Hyperuricemic Patients
B Nonhyperuricemic Patients
After RasburicasePretreatment
After RasburicasePretreatment
Uric
Aci
d Le
vels
(mg/
dL)
Uric
Aci
d Le
vels
(mg/
dL)
18
16
14
12
10
8
6
4
2
0
18
16
14
12
10
8
6
4
2
0
Adapted with permissions from Bosly et al. Rasburicase (recombinant urate oxidase) for the management of hyperuricemia in patients with cancer: report of an international compasionate use study. Cancer 2003; 98:1048-1054.
Plasma Uric Acid Levels in Hyperuicemic and Nonhyperuricemic Adults Before
and After Rasburicase38

Managing Tumor Lysis Syndrome in Adults
Supportive Cancer Therapy
164
cemia and appears to offer benefits over treatment withallopurinol or nonrecombinant urate oxidase. Although ras-buricase is not yet available in the United States to treatadult patients with TLS, it is used throughout Europe at 0.2mg/kg per day for 5-7 days in adult patients with hemato-logic malignancies.35 Rasburicase has a long plasma half-lifeof 17-21 hours and a rapid onset of action, reducing plasmauric acid levels within 4 hours.13 In contrast to allopurinol,which prevents the formation of uric acid, rasburicase cat-alyzes the conversion of uric acid to allantoin, which is sol-uble and easily excreted via the urine (Figure 2). Therefore,rasburicase has a faster onset of action than allopurinol andgenerally reduces uric acid levels to within normal parame-ters in 4-6 hours.
The safety and clinical efficacy of rasburicase have beendemonstrated in a number of studies. In one trial of 17 adultsand 90 children newly diagnosed with hematologic malig-nancies,36 the level of plasma uric acid decreased by > 25%just 4 hours after the administration of rasburicase, comparedwith baseline. By 48 hours after the first dose of rasburicase,uric acid levels were below the upper limit of normal in 99%of patients. The safety profile of rasburicase was shown to beacceptable in this study. Twenty-three patients developedTLS, but 11 of these were hyperuricemic at baseline. Nopatients needed dialysis, and there were no delays in admin-istration of induction chemotherapy.
Another study of 100 adult patients with NHL providedfurther evidence of the efficacy of rasburicase (GRAAL 1).37
All patients had ≥ 1 adverse prognostic factor (according tothe International Prognostic Index) in their first cycle ofchemotherapy. Response to rasburicase was defined as “thenormalization of uric acid levels maintained during chemo-therapy and associated with normalization of creatinine andother metabolites.” All patients who received ≥ 3 days oftreatment responded to rasburicase, and there was no inci-dence of increased creatinine or need for dialysis in anypatients. Rasburicase clearly provided rapid and dramaticdecreases of uric acid levels and control of metabolites inthese adult lymphoma patients receiving chemotherapy.Three days of rasburicase treatment controlled uric acid lev-els in 81% of patients, with another 10% controlled in 4days and another 4% controlled in 5-6 days. The safety pro-file of rasburicase was, again, acceptable.
Rasburicase was further investigated in an internationalcompassionate-use trial of patients from 8 countries(Australia, Belgium, Hong Kong, New Zealand, Malaysia,the Netherlands, Spain, and the United Kingdom) receivinginitiation chemotherapy and at risk of TLS.38 The study pop-ulation included 112 adults with hematologic malignancieswho received, at the discretion of the investigator, a medianof 6 doses of rasburicase if they presented with hyperuricemiaand a median of 5 doses of rasburicase for prophylaxis. In 27
hyperuricemic patients, rasburicase reduced the median plas-ma uric acid concentration from 14.2 mg/dL to 0.5 mg/dL(P < 0.001; Figure 3A).38 In 70 patients with normal plas-ma uric acid level at presentation, the median plasma uricacid concentration decreased from 4.9 mg/dL to 0.3 mg/dL(P < 0.001; Figure 3B). The response rate was 100% forhyperuricemic and nonhyperuricemic patients. Rasburicasewas well tolerated; 1 patient had a grade II allergic reactionwith fever but recovered without sequelae when rasburicasewas stopped. Another patient needed dialysis for acute renalfailure, despite the restoration of a normal uric acid level.Although occasional cases of hemolytic anemia and methe-moglobinemia have been reported with rasburicase treatmentin patients with glucose-6-phosphate dehydrogenase defi-ciency,12 in this study, grade III methemoglobinemia wasobserved in 1 patient, and no cases of hemolytic anemia wereobserved.38 The study investigators concluded that rasburi-case was safe and highly effective.
The final results of a second, large, rasburicase compassion-ate-use trial are now available.39 In this American compas-sionate-use trial, 379 adult patients received rasburicase. Allbut 3 patients had hematologic malignancy with a hightumor burden shown by markedly elevated lactate dehydro-genase and, in patients with leukemia, high leukocyte counts.Rasburicase was given at a dose of 0.2 mg/kg I.V. daily for 1-7 days and, if needed, every 12 hours for the first 72 hours.Uric acid levels decreased markedly from a median of 10.9mg/dL to 0.7 mg/dL (P < 0.001). All patients responded to amedian of 3 doses of rasburicase (range, 1-12 doses). Fivepatients had adverse events that were possibly related to ras-buricase, including hypersensitivity, severe backache, andmyalgia. This study confirms the efficacy and safety of rasbu-ricase for normalizing uric acid levels in adults with hyper-uricemia, maintaining uric acid levels after the start of chemo-therapy for hematologic malignancies, and maintaining uricacid levels in patients at high risk of hyperuricemia.
With the increasingly large body of evidence supportingthe use of rasburicase, it is not surprising that rasburicase isnow replacing allopurinol as the favored treatment for reduc-ing hyperuricemia and the risks of TLS.17,40 Recombinanturate oxidase is now the drug of choice in newly diagnosedpatients at high risk for TLS.40
However, as with all new therapies, the cost-effectivenessof rasburicase must be considered. A pan-European multi-center economic evaluation reported on the cost-effectivenessof rasburicase in the prevention and treatment of hyperurice-mia and TLS in patients with hematologic malignancies.41
Use of rasburicase to prevent hyperuricemia and TLS in chil-dren was associated with an incremental cost-effectivenessratio of €425-€3054 per life-year saved. In adults, preven-tion was more cost-effective in NHL and ALL than in acutemyeloid leukemia. Treatment with rasburicase was cost-

Anne-Sophie Michallet et al
Volume 2, Number 3 • April 2005
165
effective in adults and children in all malignancies and coun-ties examined. The researchers concluded that, besides itsclinical benefits, rasburicase is an economically attractivenew treatment for hyperuricemia and is cost-effective inadults with ALL and NHL.
ConclusionFor adults with hematologic malignancies, TLS is a serious
problem associated with considerable morbidity and anincreased risk of mortality. However, TLS is preventable andtreatable. Patients at high risk of TLS should be identifiedand prophylactic measures should be taken. Similarly,patients who develop hyperuricemia or TLS should be treat-ed promptly to reduce the risk of complications from TLS.Early identification of TLS is the key to effective manage-ment, and patients should be treated as soon as possible toavoid further complications.
The common management strategy for TLS-related hyper-uricemia is based around 4 interventions: I.V. hydration, uri-nary alkalinization with sodium bicarbonate, diuretics asrequired, and pharmacologic therapy for reduction of uricacid production. Hematologists currently have to make adecision between using allopurinol or rasburicase for thereduction of uric acid production.
Allopurinol has been available for many years and is stan-dard therapy in the United States. However, this treatmentdoes have drawbacks. Uric acid levels are not greatly reducedin the first few days of treatment; therefore, the use of cyto-toxic cancer treatment may need to be delayed. Interactionsof allopurinol have been noted with commonly used chemo-therapy agents (mercaptopurine and methotrexate) thatcould necessitate the use of reduced dosages. Allopurinol isalso contraindicated with capecitabine, and the dose of allop-urinol must be reduced in patients with renal impairment.
Rasburicase, the newly developed recombinant urate oxi-dase, has been shown to be clinically efficacious and cost-effective, with clear benefits over established therapies.Rasburicase provides faster management of hyperuricemia inhours instead of days. Also, in the studies conducted to date,treatment with rasburicase has been well tolerated.Therefore, rasburicase represents a significant developmentin the management of hyperuricemia and TLS.
References1. Cairo MS, Arikian S, Casciano R, et al. Uric acid (UA) is a significant
and independent prognostic factor in the development of tumour lysissyndrome (TLS) and renal complications in patients with hematologicalmalignancies admitted for chemotherapy. Blood 2002; 99 (Abstract#4670).
2. Ribeiro RC, Pui CH. Recombinant urate oxidase for prevention ofhyperuricemia and tumor lysis syndrome in lymphoid malignancies.Clin Lymphoma 2003; 3:225-232.
3. Annemans L, Moeremans K, Lamotte M, et al. Incidence, medical
resource utilisation and costs of hyperuricemia and tumour lysis syn-drome in patients with acute leukaemia and non-Hodgkin's lymphomain four European countries. Leuk Lymphoma 2003; 44:77-83.
4. Cheson BD, Frame JN, Vena D, et al. Tumor lysis syndrome: an uncom-mon complication of fludarabine therapy of chronic lymphocyticleukemia. J Clin Oncol 1998; 16:2313-2320.
5. Pui CH, Mahmoud HH, Wiley JM, et al. Recombinant urate oxidase forthe prophylaxis or treatment of hyperuricemia in patients withleukemia or lymphoma. J Clin Oncol 2001; 19:697-704.
6. Arrambide K, Toto RD. Tumor lysis syndrome. Semin Nephrol 1993;13:273-280.
7. Brant JM. Rasburicase: an innovative new treatment for hyperuricemiaassociated with tumor lysis syndrome. Clin J Oncol Nurs 2002; 6:12-16.
8. Jeha, S. Tumor lysis syndrome. Semin Hematol 2001; 38:4-8.9. Ribeiro RC, Pui CH. Hyperuricemia in patients with cancer. Am J
Cancer 2002; 1:409-422.10. Nicolin, G. Emergencies and their management. Eur J Cancer 2002;
38:1365-1377; discussion 1378-1369.11. Stapleton FB, Strother DR, Roy S 3rd, et al. Acute renal failure at onset
of therapy for advanced stage Burkitt lymphoma and B cell acute lym-phoblastic lymphoma. Pediatrics 1988; 82:863-869.
12. Cohen LF, Balow JE, Magrath IT, et al. Acute tumor lysis syndrome. Areview of 37 patients with Burkitt's lymphoma. Am J Med 1980;68:486-491.
13. Pui CH. Rasburicase: a potent uricolytic agent. Expert Opin Pharmacother2002; 3:433-452.
14. Hogan DK, Rosenthal LD. Oncological emergencies in the patient withlymphoma. Semin Oncol Nurs 1998; 14:312-320.
15. Rieselbach RE, Bentzel CJ, Cotlove E, et al. Uric acid excretion andrenal function in the acute hyperuricemia of leukemia. Am J Med 1964;37:872-884.
16. Zusman J, Brown DM, Nesbit ME. Hyperphosphatemia, hyperphos-phaturia and hypocalcemia in acute lymphoblastic leukemia. N Engl JMed 1973; 289:1335-1340.
17. Baeksgaard L, Sorensen JB. Acute tumor lysis syndrome in solidtumors–a case report and review of the literature. Cancer ChemotherPharmacol 2003; 51:187-192.
18. Levine AM. Challenges in the management of Burkitt's lymphoma. ClinLymphoma 2002; 3:S19-S25.
19. Ravindranath Y. Recent advances in pediatric acute lymphoblastic andmyeloid leukemia. Curr Opin Oncol 2003; 15:23-35.
20. Hecht JL, Aster JC. Molecular biology of Burkitt's lymphoma. J ClinOncol 2000; 18:3707-3721.
21. Jones DP, Stapleton FB, Kalwinsky D, et al. Renal dysfunction andhyperuricemia at presentation and relapse of acute lymphoblasticleukemia. Med Pediatr Oncol 1990; 18:283-286.
22. Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysissyndrome immediately after 4 Gy fractionated TBI as part of reducedintensity preparative regimen in a patient with T-ALL with high tumorburden. Bone Marrow Transplant 2003; 31:935-937.
23. Ezzone SA. Tumor lysis syndrome. Semin Oncol Nurs 1999; 15:202-208.24. Navolanic PM, Pui CH, Larson RA, et al. Elitek-rasburicase: an effec-
tive means to prevent and treat hyperuricemia associated with tumorlysis syndrome, a Meeting Report, Dallas, Texas, January 2002.Leukemia 2003; 17:499-514.
25. Watanabe S, Kanellis J, Nakagawa T, et al. Reducing uric acid as ameans to prevent cardiovascular and renal disease. Expert Opin TherPatents 2002; 12:193-199.
26. Sallan S. Management of acute tumor lysis syndrome. Semin Oncol 2001;28:9-12.
27. Patte C, Sakiroglu C, Ansoborlo S, et al. Urate-oxidase in the preven-tion and treatment of metabolic complications in patients with B-celllymphoma and leukemia, treated in the Societe Francaise d'OncologiePediatrique LMB89 protocol. Ann Oncol 2002; 13:789-795.

Managing Tumor Lysis Syndrome in Adults
Supportive Cancer Therapy
166
28. Cairo MS. Prevention and treatment of hyperuricemia in hematologicalmalignancies. Clin Lymphoma 2002; 3(suppl 1):S26-S31.
29. Smalley RV, Guaspari A, Haase-Statz S, et al. Allopurinol: intravenoususe for prevention and treatment of hyperuricemia. J Clin Oncol 2000;18:1758-1763.
30. Andreoli SP, Clark JH, McGuire WA, et al. Purine excretion during tumorlysis in children with acute lymphocytic leukemia receiving allopurinol:relationship to acute renal failure. J Pediatr 1986; 109:292-298.
31. Arellano F, Sacristan JA. Allopurinol hypersensitivity syndrome: areview. Ann Pharmacother 1993; 27:337-343.
32. Dervieux T, Brenner TL, Hon YY, et al. De novo purine synthesis inhi-bition and antileukemic effects of mercaptopurine alone or in combina-tion with methotrexate in vivo. Blood 2002; 100:1240-1247.
33. Crews KR, Evans WE, Pui CH. Methotrexate Pharmacokinetics fol-lowing hyperuricemic treatment with allopurinol vs urate oxidase inchildren with acute lymphoblastic leukemia (ALL). Blood 2001;98:113a (Abstract #474).
34. British National Formulary. Allopurinol. Available at http://www.bnf.org.Accessed November 1, 2004.
35. Easton J, Noble S, Jarvis B. Rasburicase. Paediatr Drugs 2001; 3:433-437.36. Lascombes F, Sommelet D, Gebhard F, et al. High efficacy of recombi-
nant urate oxidase in prevention of renal failure related to tumor lysissyndrome (TLS). Blood 1998; 92:237B (Abstract #4019).
37. Coiffier B, Mournier N, Bologna S, et al. Efficacy and safety of rasburi-case (recombinant urate oxidase) for the prevention and treatment ofhyperuricemia during induction chemotherapy of aggressive non-Hodgkin’s lymphoma: results of the GRAAL1 (Groupe d’Etude desLymphomes de l’Adulte Trial on Rasburicase Activity in AdultLymphoma) study. J Clin Oncol 2003; 21: 4402-4406.
38. Bosly A, Sonet A, Pinkerton CR, et al. Rasburicase (recombinant urateoxidase) for the management of hyperuricemia in patients with cancer:report of an international compassionate use study. Cancer 2003;98:1048-1054.
39. Jeha S, Kantarjian H, Irwin D, et al. Efficacy and safety of rasburicase,a recombinant urate oxidase (Elitek), in the management of malignan-cy-associated hyperuricemia in pediatric and adult patients: final resultsof a multicenter compassionate use trial. Leukemia 2005; 19:34-38.
40. Lowis S. Commentary. Eur J Cancer 2002; 38:1378-1379.41. Annemans L, Moeremans K, Lamotte M, et al. Pan-European multicen-
tre economic evaluation of recombinant urate oxidase (rasburicase) in pre-vention and treatment of hyperuricaemia and tumour lysis syndrome inhaematological cancer patients. Support Care Cancer 2003; 11:249-257.