Embed Size (px)
Citation preview

Dipti Itchhaporia, MD, FACC, FESCImmediate Past Trustee, American College of Cardiology
Director of Disease Management, Hoag HospitalRobert and Georgia Roth Endowed Chair for Excellence in
Cardiac CareJeffrey M. Carlton Heart and Vascular Institute
Assistant Clinical Professor, University of California, Irvine
Optimizing STEMI Systems of Care

I have no
disclosures
Disclosure
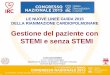
Time and Mortality in STEMI Patients
15.4
23.3
28.1
30.8
0
5
10
15
20
25
30
35
Mortality, %
0 to 60 min 61 to 120
min
121 to 180
min
181 to 360
min
Terkelsen CJ JAMA 2010;304:763-771
Longer D2B – higher mortality
Shorter time from door-to-balloon (PCI) leads to lower risk of mortality
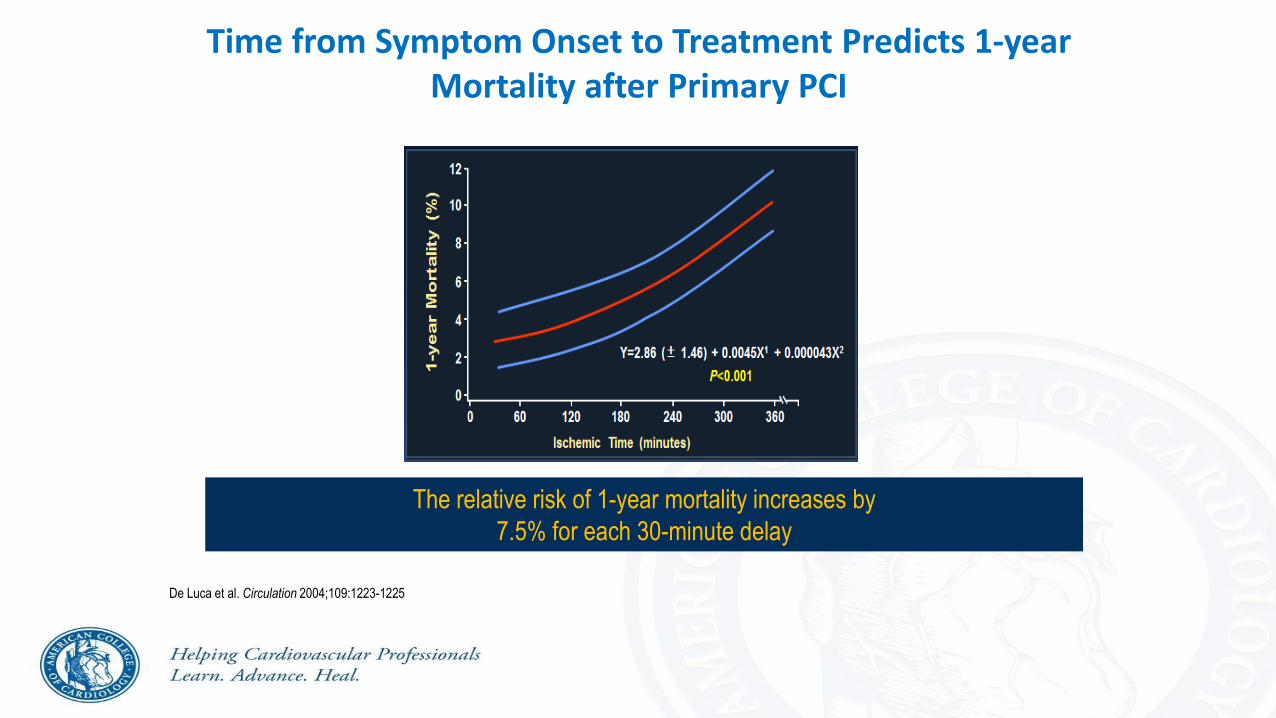
Time from Symptom Onset to Treatment Predicts 1-year Mortality after Primary PCI
De Luca et al. Circulation 2004;109:1223-1225
The relative risk of 1-year mortality increases by
7.5% for each 30-minute delay

Do whatever it takes to reduce time from symptom onset to ER arrival and time from ER arrival to PCI!
Public awareness of MI Sx
CAD centers of excellence with
lower DBTs and excellent outcomes
Regional coordination
Ambulance ECG telemetry
Ambulance/ER CCL activation
ICs sleep in hospital
Continual QI
Mehran, Roxana

Barriers to Timely Reperfusion• The patient
• Failure to promptly recognize symptoms• Hesitation to seek medical attention
• Time to transport• Mandated delivery to the closest hospital, regardless of PCI
capabilities• Long transport in rural areas
• Decision process on arrival• Clot-busting drugs vs. PCI• Off hours• Transfer to PCI facility
• Time to implement treatment– Procedural factors• Team assembly
6
The Reality of Today’s Patients• Not all STEMI patients call 9-1-1
• 50% of STEMI patients present to their local emergency department (ED)
• “Walk-in” patients • Rapid ECG
– CODE 10 Established – ECG in under 10 minutes from time of arrival (DOOR TIME)
– Operational Considerations• CODE 10 called overhead in ED• multiple available ECG machines • process in place to mobilize ECG machine and tech• training/ competency of Emergency Care Techs to perform
ECG• high priority of ED MD to read ECG
7

The Ideal Patient & System• Patients and the public:
• Recognize the symptoms of STEMI • Realize the importance of:
• Activating emergency medical services (EMS) via 9-1-1 promptly
• Getting treatment quickly
• The ideal system:• Promotes education efforts for the
Emergency Medical System, the Emergency department personnel, cath lab staff, physicians and the patients.
• Provides coordinated and patient-centered care
8

Transport: Patient to ED by Ambulance
• Coordination with Emergency Medical System
• 12 Lead ECG performed in field
– Appropriate ECG machines on ambulance capable of transmitting clean tracing
– Training/ competency of EMT to perform ECG
• EMS transmits to Base Hospital, BH contacts Cardiovascular Receiving Center (CVRC)
– Our institution is both a BH and CVRC
• Radio call to ED
– Notifies ED MD, ED RN, Activates CATH LAB –simultaneously
– ED MD contacts ED CALL PANEL On Call Interventional Cardiologist

The Ideal Emergency Medical System (EMS)• In an ideal system:
• Ambulances are equipped with 12-lead ECG machines• EMS providers are trained to:
• Use and transmit 12-lead ECGs• Care for STEMI patients• Provide feedback on performance and compliance
with guidelines• Standardized point-of-entry (POE) protocols define patient
transport rules• When there is STEMI, the cath lab is activated promptly• Patients transported to a STEMI-referral hospital remain
on the stretcher with EMS present pending a transport decision
• When “walk-in” patients present to a STEMI-referral hospital and require primary PCI, activation of EMS occurs
• Hospitals close the communication gap with EMS
10

PROCESS:STEMI Presentation: EMS v. Walk-In
EMS
• STEMI Recognition by EMS Pre-Hospital Prior to “DOOR”
– Education & Collaboration with EMS for timely and accurate 12 Lead ECG
• Pre-hospital activation of ED, CCU & CCL Team CODE STEMI
– 30 minute arrival time
• ED MD interprets ECG upon pt arrival, repeats if necessary.
11
Walk-In
• STEMI Recognition upon arrival of Walk–In CODE 10:
ECG within 10 min
• ED MD primary interpretation of ECG with simultaneousactivation of IC and CCL TEAM

STEMI Treatment
GOAL: Achieve D2B < 90 minutes <60 minutes• Key Criteria
– Early activation – Door to Data/ECG < 10 min– Door to Decision < 15 min– Door to Cardiac Cath Lab (CCL) < 30 minutes– CCL door to Ready for Stick < 10 min– CCL door to BLN < 45 min
12
13
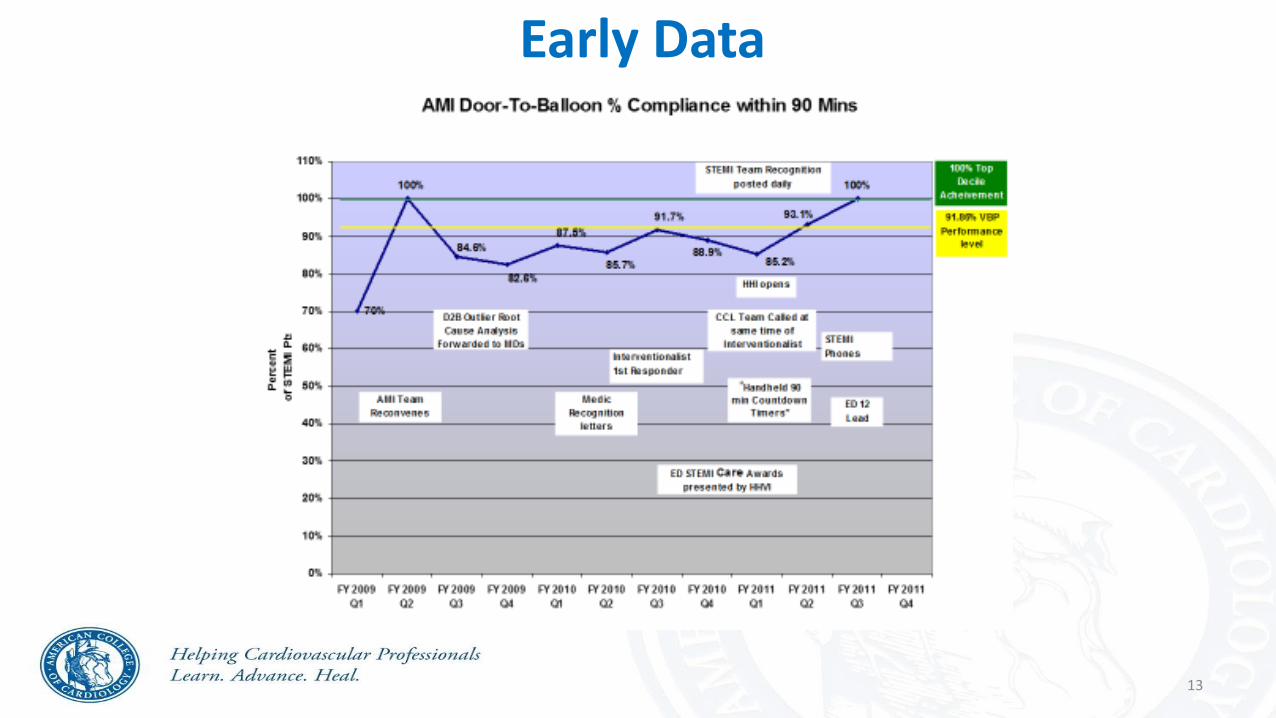
Early Data

14
Dedicated Mobile Phones in EDFor STEMI Notification
• Programmed with IC Cell Numbers
• ED MD speaks directly with IC • Program IC’s cell phones with
ED Cell identifier as “STEMI”
STEMI
STE
MI

Next StepsTracking Progress
Create evaluation mechanism to track progress and outcomes- and give feedback

16
Time
________
________
"Door to Data"
________ National Goal = 10 minutes
Hoag Goal < 10 minutes
________ "Door to Decision"
________ Hoag Goal < 15 minutes
Interventional Cardiologist: __________________
________
________
________ ED arrival to CVL arrival
Hoag Goal = < 40 minutes
"ED to lab"
________ Hoag Goal < 5 minutes
________ "CCL door to ready"
Hoag Goal < 10 minutes
________ "Lab ready to Stick Time"
Hoag Goal = 0 minutes
Artery Open (time of 1st balloon inflation) ________ "CCL arrival to balloon"
Culprit artery: ________________________ Hoag Goal = < 45 minutes
________
________
Goal D2B = < 90 minutes
Goal E2B = < 90 minutes
Primary PCI Data Collection FormThis is NOT a Permanent Part of the Patient's Record
Benchmark Time or Goal
REFERENCE
Date & time patient first arrives to Hoag:
ED calls Interventional Cardiologist
ED Physician: ____________________________
Please copy and attach:
1.) EMS field ECG,
2.) EMS run Sheet,
3.) ECG(s) from ED,
4.) ED triage sheet
Immediate post-procedure pt disposition &/or location:
_____________________________
Patient arrives in CCL from ED
(Please document if room not available.)
Local
Total ED door to balloon (D2B) time =
Patient ready - prepped & draped
Total EMS to balloon (E2B) time =
Hoag Goal = < 30 minutes
following notification
Initial ECG obtained: EMS____ Hoag______
STEMI? Yes______ No______
If EMS ECG, was the field interpretation confirmed?
Yes _____ No_____
Time 1st ECG obtained
Patient ready for transport to CCL:
Call Team arrival time to hospital:
Cardiologist arrival time to hospital:
ED calls Perfect Serve to activate Call Team
Data Element
"Door" ie.: Arrival to hospital
Card
iac C
ath
Lab
Resp
on
sib
ilit
y
Date AND Time ED notified of patient arrival:
Arrival by: EMS _____ BLS _____ Walk-In _____
OCS-EMS Identification (run) #:______________
Medical Record #:_________________________
Patient Age: _____ Male ____ Female_____
Em
erg
en
cy D
ep
art
men
t R
esp
on
sib
ilit
y
Hoag Goal = < 30 minutes
following notification
Primary PCI Data CollectionForm
• Initiated Dec 2010
• Completed by designated CCL RN’s
• Reviewed and reported by AMI Team Leaders
• Immediate, real-time feedback for all

Door 2 Balloon Time (in Minutes)
17

Partners for Success
• Patients and care givers
• EMS providers
• Physicians, nurses and other providers
• STEM-referral (non-PCI) hospitals
• STEMI-receiving (PCI-capable) hospitals
• Health systems
• Departments of health
• EMS regulatory authority / office of EMS
• Quality improvement organizations
• State and local policymakers
18
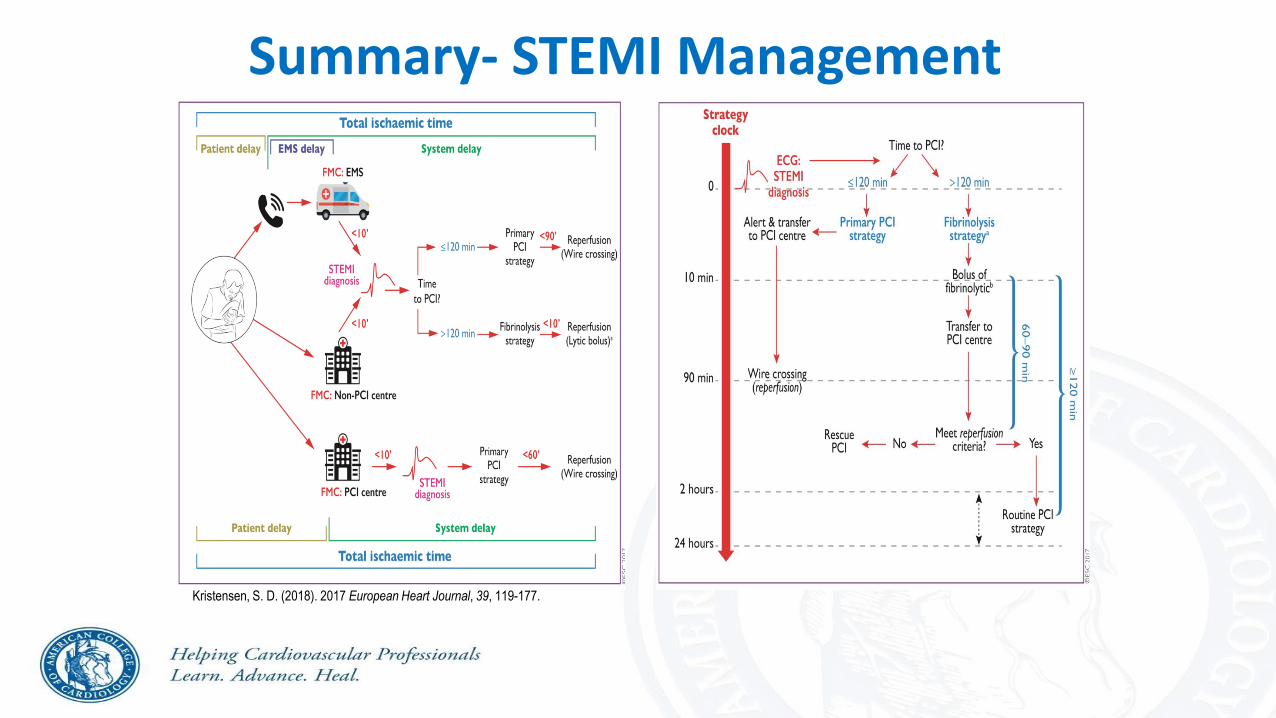
Summary- STEMI Management
Kristensen, S. D. (2018). 2017 European Heart Journal, 39, 119-177.