Embed Size (px)
Citation preview

March 12, 201512:30 PM – 1:45 PMHouston, TX
Educational Partner
Sponsored by pmiCME
Optimizing the Diagnosis, Treatment, and Management ofIrritable Bowel Syndrome

Session 4
Session 4: Optimizing the Diagnosis, Treatment, and Management of Irritable Bowel Syndrome Learning Objectives
1. Diagnose IBS and differentiate from other bowel disorders using established clinical guidelines. 2. Summarize the efficacy and safety of pharmacologic and nonpharmacologic treatment options for IBS. 3. Implement patient-specific methods for managing IBS symptoms and improving function and quality of life.
Faculty
Brooks D. Cash, MD Professor of Medicine University of South Alabama Mobile, Alabama Dr Brooks Cash is a professor of medicine at the University of South Alabama (USA), Mobile, Alabama; where he has held a faculty position since 2013. He was previously a professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Maryland. He currently serves as the director of the motility and physiology service at the USA Digestive Health Center. Prior to his relocation to USA, Dr Cash served in the United States Navy for 24 years, retiring in 2013 at the rank
of captain, as the deputy commander for medicine at Walter Reed National Military Medical Center, Bethesda, Maryland. Dr Cash received his undergraduate degree in business administration (finance) with honors from The University of Texas at Austin. He earned his medical degree from the Uniformed Services University of Health Sciences and completed his internship, residency, and gastroenterology fellowship at the National Naval Medical Center, Bethesda. Dr Cash is a diplomate of the American Board of Gastroenterology. He is a fellow of the American College of Physicians, American College of Gastroenterology (ACG), American Gastroenterological Association, and the American Society for Gastrointestinal Endoscopy. Dr Cash serves on the Rome Foundation committee for functional gastrointestinal disorders and has authored multiple articles and book chapters on a variety of gastrointestinal topics, including irritable bowel syndrome and chronic constipation, colorectal cancer screening, CT colonography, acid peptic disorders, Barrett esophagus, and evidence based medicine. He serves as an associate editor for The American Journal of Gastroenterology and is an editorial board member and reviewer for numerous internal medicine and gastroenterology medical journals. Dr Cash most recently served as the governor of ACG’s military region.
Spencer Dorn, MD, MPH, MHA Vice Chief Gastroenterology Assistant Professor of Medicine University of North Carolina Chapel Hill, North Carolina Dr Spencer Dorn works to improve quality of care, operational efficiency, and patient experiences as vice chief of the University of North Carolina (UNC) division of gastroenterology and hepatology. As assistant professor of medicine, he conducts clinical trials for functional GI disorders, performs health services research, and examines the impact of health policy and regulations on gastroenterology. His clinical practice focuses on functional GI and motility disorders.
Dr Dorn graduated with highest distinction from the University of Michigan, Ann Arbor and summa cum laude from the State University of New York at Brooklyn College of Medicine. He earned a master of public health (epidemiology) degree and later a master of healthcare administration (health policy and management) from UNC. Dr Dorn completed his internal medicine training at Brigham and Women's Hospital, Boston, Massachusetts; where he was a clinical fellow at Harvard Medical School. He subsequently trained at UNC as a National Institutes of Health postdoctoral research fellow in digestive diseases epidemiology and functional GI disorders, and later as a clinical fellow in gastroenterology and hepatology.

Session 4
Faculty Financial Disclosure Statements The presenting faculty reports the following: Dr Cash receives Consulting fees from Zx Pharma; Medical Advisory Board fees from Forest, Ironwood, Paion, Salix, and Takeda; Speakers Bureau honorarium from Forest, Ironwood, Salix, and Takeda.
Dr Dorn is an ad hoc consultant to investors and marketers.
Education Partner Financial Disclosure Statement The content collaborators at Miller Medical Communications, LLC have no financial relationships to disclose.
Suggested Reading List Brandt LJ, Chey WD, Foxx-Orenstein AE, et al; for the American College of Gastroenterology Task Force on Irritable Bowel Syndrome. An evidence-based position statement on the management of irritable bowel syndrome. Am J Gastroenterol. 2009;104 (Suppl 1):S1-S35. Canavan C, West J, Card T. The epidemiology of irritable bowel syndrome. Clin Epidemiol. 2014;6:71-80. Chey WD, Maneerattaporn M, Saad R. Pharmacologic and complementary and alternative medicine therapies for irritable bowel syndrome. Gut Liver. 2011;5(3):253-266. Drossman DA, Morris CB, Schneck S, et al. International survey of patients with IBS: symptom features and their severity, health status, treatments, and risk taking to achieve clinical benefit. J Clin Gastroenterol. 2009;43(6):541-550. Engsbro AL, Begtrup LM, Kjeldsen J, et al. Patients suspected of irritable bowel syndrome--cross-sectional study exploring the sensitivity of Rome III criteria in primary care. Am J Gastroenterol. 2013;108(6):972-980. Harkness EF, Harrington V, Hinder S, et al. GP perspectives of irritable bowel syndrome--an accepted illness, but management deviates from guidelines: a qualitative study. BMC Fam Pract. 2013;14:92. Jarrett ME, Cain KC, Burr RL, et al. Comprehensive self-management for irritable bowel syndrome: randomized trial of in-person vs. combined in-person and telephone sessions. Am J Gastroenterol. 2009;104(12):3004-3014. Jellema P, van der Windt DA, Schellevis FG, van der Horst HE. Systemic review: accuracy of symptom-based criteria for diagnosis of irritable bowel syndrome in primary care. Aliment Pharmacol Ther. 2009;30(7):695-706. Ladabaum U, Boyd E, Zhao WK, et al. Diagnosis, cormorbidities, and management of irritable bowel syndrome in patients in a large health maintenance organization. Clin Gastroenterol Hepatol. 2012;10(1):37-45. Lee V, Guthrie E, Robinson A, et al. Functional bowel disorders in primary care: factors associated with health-related quality of life and doctor consultation. J Psychosom Res. 2008;64(2):129-138. Lembo AJ, Conboy L, Kelley JM, et al. A treatment trial of acupuncture in IBS patients. Am J Gastroenterol. 2009;104(6):1489-1497. Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-1491. MacPherson H, Tilbrook H, Bland JM, et al. Acupuncture for irritable bowel syndrome: primary care based pragmatic randomised controlled trial. BMC Gastroenterol. 2012;12:150. McKenzie YA, Alder A, Anderson W, et al. British Dietetic Association evidence-based guidelines for the dietary management of irritable bowel syndrome in adults. J Hum Nutr Diet. 2012;25(3):260-274. National Institute for Health and Care Excellence (NICE). Irritable bowel syndrome in adults: diagnosis and management of irritable bowel syndrome in primary care. February 2008;CG61. Accessed January 30, 2015.

Session 4
Rao S, Lembo AJ, Shiff SJ, et al. A 12-week, randomized, controlled trial with a 4-week randomized withdrawal period to evaluate the efficacy and safety of linaclotide in irritable bowel syndrome with constipation. Am J Gastroenterol. 2012;107(11):1714-1724. Spiegel BM, Farid M, Esrailian E, Talley J, Chang L. Is irritable bowel syndrome a diagnosis of exclusion? A survey of primary care providers, gastroenterologists, and IBS experts. Am J Gastroenterol. 2010;105(4):848-858. Wilkins T, Pepitone C, Alex B, Schade RR. Diagnosis and management of IBS in adults. Am Fam Physician. 2012;86(5):419-426. Yoon SL, Grundmann O, Koepp L, Farrell L. Management of irritable bowel syndrome (IBS) in adults: conventional and complementary/alternative approaches. Altern Med Rev. 2011;16(2):134-151.
SESSION 412:30 – 1:45pm
Optimizing the Diagnosis, Treatment, and Management of Irritable Bowel Syndrome
SPEAKERSBrooks D. Cash, MD
Spencer Dorn, MD, MPH, MHA
Presenter Disclosure Information
►Dr Cash receives Consulting fees from Zx Pharma; Medical Advisory Board fees from Forest, Ironwood, Paion, Salix, and Takeda; Speakers Bureau honorarium from Forest, Ironwood, Salix, and Takeda.
►Dr Dorn is an ad hoc consultant to Gerson Lehrman Group, Guidepoint Global and Coleman Research Group.
The following relationships exist related to this presentation:
Off-Label/Investigational Discussion
► In accordance with pmiCME policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
Learning Objectives
After participating in this educational activity the participant should be able to:
• Diagnose IBS and differentiate from other bowel disorders using established clinical guidelines
• Summarize the efficacy and safety of pharmacologic and nonpharmacologic treatment options for IBS
• Implement patient-specific methods for managing IBS symptoms and improving function and quality of life
3
4
Generic Name Trade Name
Alosetron Lotronex
Amitriptyline Elavil, Endep, Vanatrip
Cholestyramine Cholestyramine Light, Prevalite, Questran, Questran Light
Citalopram CeleXA
Desipramine Norpramin
Dicyclomine Bentyl
Diphenoxylate‐atropine Lomotil
Doxepin Adapin, Silenor, Sinequan
Elobixibat Elobixibat
Eluxadoline Eluxadoline
Fluoxetine Prozac, Sarafem
Hyoscyamine Anaspaz, Cystospaz, Donnamar, Levsin
Imipramine Tofranil, Tofranil‐PM
Generic Name Trade Name
Ispaghula Fybogel, Ispagel
Linaclotide Linzess
Loperamide Imodium, Imodium A‐D, Kaopectate II, Maalox Anti‐Diarrheal Caplets, Pepto Diarrhea Control
Lubiprostone Amitiza
Mesalamine/Mesalazine Apriso, Asacol, Lialda, Pentasa
PEG 3350+E Colyte, GaviLyte‐C, GolytelyGlycoLax,MiraLax
Paroxetine Paxil, Paxil CR, Pexeva
Plecanatide Plecanatide
Prucalopride Resolor
Psyllium Konsyl, Metamucil, Reguloid
Rifaximin Xifaxan
Brooks D. Cash, MDProfessor of MedicineUniversity of South AlabamaMobile, Alabama
10
Worldwide prevalence: 7% to 10%
1.5 times more prevalent in women
More commonly diagnosed in patients <50 years of age
More common in lower socioeconomic groups
Patients with IBS have more physician visits, hospitalizations, missed workdays, prescriptions, and diagnostic tests than those without
11
IBS=irritable bowel syndrome.

12
Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis
Onset associated with a change in frequency of
stool
Onset associated with a change in form of stool
Recurrent abdominal pain or discomfortat least 3 days/month in the last 3 months
associated with ≥2 of the following:
Improvement with defecation
Additional IBS “testing,” including routine laboratory tests and colonoscopy, unnecessary unless alarm features present
13
IBS-C IBS-M
IBS-U IBS-D
100
75
50
25
0
0 25 50 75 100
Loose or watery stools (%)
Hard or Lumpy Sto
ols (%)
IBS‐C: Constipation‐predominant IBS
IBS‐D: Diarrhea‐predominant IBS
IBS‐M: Mixed IBS (hard and loose stools over periods of weeks and months)
IBS‐U: Unsubtyped IBS
Abdominal pain – 29% state this is the predominant symptom
Misinformation 15% believe IBS will turn into cancer 30% believe IBS increases risk for IBD 17% believe IBS will lead to malnutrition
Lack of information Prevalent physician belief IBS due to anxiety (80.5%) or
depression (63.2%) Only 2/3 of patients recognize that IBS does not shorten
life expectancy
14
LemboT et al. Am J Gastroenterol. 1999;94(5):1320–1326. ; Lacy et al. Am J Gastroenterol. 2005;100(s9):S324; Noddin et al. Am J Gastroenterol. 2005;100(s9):S323; Lee et al. Am J Gastroenterol. 2005;100(s9):S336.
IBD=inflammatory bowel disease.
Enteric nervous system dysfunction Gastrointestinal
dysmotility Visceral hypersensitivity
Disordered CNS pain processing
Post‐infectious
Small intestinal bacterial overgrowth Dysbiosis
Food intolerance
Genetics
Mast cell dysfunction
Somatization
CNS=central nervous system.
18
Gastrointestinal
Colorectal cancer
Diverticular disease
Gynecologic
Ovarian cancer Endometriosis
Drugs
Opiates
Anticholinergics
Antidepressants
Metabolic/Endocrine
Hypothyroidism
Diabetes
Neurologic
Parkinson disease
Multiple sclerosis
Autonomic neuropathy
Other
Amyloidosis
Scleroderma
19
Dietary factors
Lactose Gluten Other FODMAPs
Drugs
Infection
Giardiasis Amebiasis C difficile
Malabsorption
Celiac disease
Inflammatory bowel disease
Crohn’s disease Ulcerative colitis Microscopic colitis
Psychological
Panic disorder Somatization Depression
FODMAPs=fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.
20

IBS is a syndrome—a collection of symptoms
Diagnosis possible via a thorough history of symptoms and physical examination
Because symptoms are non‐specific, must consider alternative organic diagnoses
Serious organic illnesses typically produce alarm symptoms (eg, bleeding, weight loss, etc)
21
302 Danish patients aged 18‐50 years referred from primary care. No alarm features. Randomized to:
▪ Exclusionary strategy: Blood work, stool samples, lower endoscopy with biopsy
▪ Positive strategy: CBC and CRP only
Followed for 1 year
No difference in any outcome measure (symptoms, HRQL, use of health care resources, etc)
No cases of IBD, CRC, or celiac disease identified
Exclusionary strategy more expensive▪ Direct costs: $863 greater▪ Mean total costs: $1915 greater
Begtrup LM et al. ClinGastroenterol Hepatol. 2013;11(8):956‐962.
CBC=complete blood count; CRC=colorectal cancer; CRP=C‐reactive protein; HRQL=health‐related quality of life.
22
8
72
Co
nsi
der
IB
S a
Dia
gn
osi
s o
f E
xclu
sio
n,
%
IBS Experts(n=27)
Community Clinicians(n=281)
Clinicians who believed IBS was a diagnosis of exclusion ordered 1.6 times more tests and spent $364more on diagnostic tests per patient (P<.0001)
Clinicians who believed IBS was a diagnosis of exclusion ordered 1.6 times more tests and spent $364more on diagnostic tests per patient (P<.0001)
23
Histologic Findings in IBS Patients and Controls;Populations Not Matched for Age or Sex
LesionIBS Patients
n=466 (%)
Controlsn=451 (%)
P Value
Adenomas 36 (7.7) 118 (26.1) <.0001
Hyperplastic polyps 39 (8.4) 52 (11.5) NS
Cloorectal adenocarcinoma 0 (0.0) 1 (0.2) NS
IBD 2 (0.4) 0 (0.0) NS
Microscopic colitis 7 (1.5) N/A N/A
Microscopic colitis was more common in a subset of patients with IBS‐D who were ≥45 years (2.3%).
N/A, not applicable; NS=not significant.
24
There is a paucity of evidence guiding radiologic imaging in IBS
Imaging study should be influenced by predominant symptoms
Data suggest very low yield of CT and U/S
Definitive recommendations must await further research
O’Connor OJ et al. Radiology. 2012;262(2):485‐494.
U/S=ultrasonography.
25 26

Up to 10% of chronic idiopathic abdominal pain Entrapment of anterior cutaneous branch of thoracic intercostal nerve
Sharply localized pain and superficial tenderness + Carnett sign: accentuated localized tenderness with abdominal wall tensing
Reassurance and avoidance of precipitating causes often sufficient
Anesthetic/corticosteroid injection effective in ≈ 75%▪ Also serves as diagnostic confirmation
Srinivassan R, et al. Am J Gastroenterol. 2002;3(4):824‐30.
27
1% of the adult population; 25% of those diagnosed with IBS‐D
Tests that directly assess bile acid malabsorption (SeHCAT, 14C‐glycocholate breath tests, serum C4, fecal bile acids) either not available in United States or not validated
Therapeutic trial only option Bile acid sequestrants
Vijayvargiya P et al. ClinGastroenterol Hepatol. 2013;11(10):1232‐1239.
SeHCAT= 75selenium homotaurocholic acid test.
28
Crohn’s disease, ulcerative colitis, undifferentiated IBD
IBS symptoms ARE common in IBD patients in “remission”
35% overall; higher in Crohn’s disease
Opinion divided as to what they mean
Unrecognized [latent] IBD
Real or coincident IBS; linked to psychosocial issues
29
Halpin SJ, et al. Am J Gastroenterol. 2012;107(10):1474‐1482.Keohane J et al. Am J Gastroenterol. 2010;105(8):1789‐1794. Quigley EM, et al. Am J Gastroenterol. 2012;107(10):1483‐1485. Vivinus‐NébotM et al. Gut. 2014;63(5):744‐752.Jonefjäll B et al. Neurogastroenterol Motil. 2013;25(9):756‐e578 Berrill JW et al. Aliment PharmacolTher. 2013;38(1):44‐51.
“Post‐diverticulitis IBS” 2204 subjects at Los Angeles Veterans Administration medical center
who had an episode of diverticulitis and followed for 6.3 years▪ Almost 5 times more likely to be diagnosed with IBS later
Symptomatic uncomplicated diverticular disease (SUDD) 229 treated with mesalazine ± L casei vs L casei alone vs placebo for 10
days per month for 12 months▪ Higher remission rates in treatment groups▪ Symptomatic diverticulitis in 6 on placebo and 1 in probiotic group
345 patients with uncomplicated diverticulitis
Mesalamine 3 g daily vs placebo for 48 weeks % recurrence‐free at 48 weeks: 68% mesalamine, 74% placebo
30Cohen E et al. ClinGastroenterol Hepatol. 2013;11(12):1614‐1619.TursiA. et al. DDW 2013. KruisW. et al. DDW 2013
General Practice Research Database in the United Kingdom Celiac patients were 3 times more likely to have a prior
diagnosis of IBS, even for 10 years previously
38% of celiac disease patients have IBS symptoms; especially if non‐adherent with gluten free diet
Should you screen for celiac disease? YES
Mohseninejad L et al. Eur J Health Econ. 2013;14(6):947‐957.
NOCash BD et al. Gastroenterology. 2011;141(4):1187‐1193.
31Card TR et al. Scand J Gastroenterol. 2013;48(7):801‐807. Sainsbury A et al. ClinGastroenterol Hepatol. 2013;11(4):359‐365.
IBS patients (physician diagnosis)Positive for both tTGA and EMACeliac disease not biopsy‐proven
Non‐constipated IBS patients (Rome II)Biopsy‐proven celiac disease
32
Case‐Control Study Prospective Study
0.5
1
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Patients w
ith celiac
disease (%)
0.4 0.4
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Patients w
ith celiac
disease (%)
N=566N=555
Controls IBS Patients
Saito‐Loftus Y, et al. Am J Gastroenterol. 2008;103(suppl 1):S472. Abstract 1208; Cash BD et al. Gastroenterology. 2011;141(4):1187‐1193.
N=492N=458
Controls IBS Patients
P=NS P=NS
Prospective study: 7.3% IBS and 4.8% controls had at least 1 abnormal gluten‐directed serology (most often IgG AGA)

Adapted from Verdu EF et al. Am J Gastroenterol. 2009;104(6):):1587‐1594.
CD=celiac disease. 33
IBS symptoms Spectrum of CD
Is it IBS, Celiac Disease or Something in Between?
Motility / visceral sensationBrain – gut interactionsImmune activationAltered gut microbiome
Potential / asymptomatic CD
Symptomatic CD
Non‐celiac glutenor
wheat sensitivity
Routine laboratory tests: CBC, CMP, TSH, stool O&P, abdominal imaging not recommended
Serologic testing for celiac disease (IBS‐D/M)
strongly consider
Lactose breath testing selected cases
Colonoscopy recommended if ≥50 years of age, with biopsies in refractory IBS‐D (to exclude microscopic colitis)
ACG=American College of Gastroenterology; CMP=Comprehensive Metabolic Panel; TSH=thyroid‐stimulating hormone.
American College of Gastroenterology Task Force on Irritable Bowel Syndrome; Brandt LJ et al. Am J Gastroenterol. 2009;104 suppl 1:S1‐S35. 34
Refractory or worsening abdominalsymptoms
Older patient (≥50 years of age;≥45 years of age if black) at onset
Blood in stools (hematochezia)
Anemia
Weight loss (unintentional)
Anorexia
Family history of organic GI disease
Further investigation warranted
35
Only 1% to 9% with IBS diagnosed with an alternative organic GI disorder after 30 years of follow‐up
Long‐term follow‐up: 2% to 18% worse, 30% to 50% of patients unchanged
Prior surgery (1 study), higher somatic scores (1 study), higher baseline anxiety (2 studies), depression (1 study) predicted worse symptoms during long‐term follow‐up
Short duration and constipation: better outcome
El‐Serag HB et al. Aliment PharmacolTher. 2004;19(8):861‐870.36
Identify IBS symptoms, presence of alarm features
Meets criteria, no alarm features make diagnosis of IBS
Does not meet criteria, has alarm features look for alternative diagnosis
Symptomatic treatment for predominant symptoms
Assess response to treatment
Good response continue Rx Poor response reassess
LongstrethGF et al. Gastroenterology. 2006;130(5):1480‐1491; Erratum in: Gastroenterology. 2006;131(2):688; American College of Gastroenterology Task Force on Irritable Bowel Syndrome; Brandt LJ et al. Am J Gastroenterol. 2009;104 suppl 1:S1‐S35.
Poor response reassess
37
Spencer Dorn, MD, MPH, MHAUniversity of North Carolina School of MedicineChapel Hill, North Carolina
38
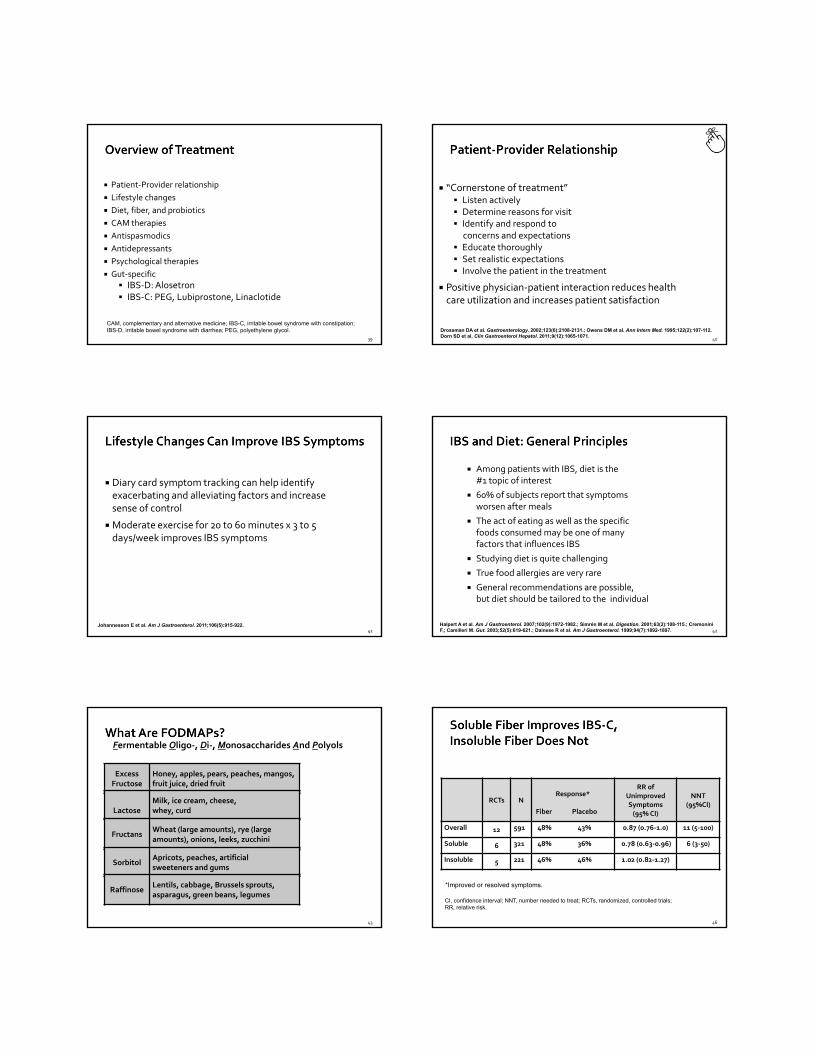
Patient‐Provider relationship
Lifestyle changes
Diet, fiber, and probiotics
CAM therapies
Antispasmodics
Antidepressants
Psychological therapies
Gut‐specific
IBS‐D: Alosetron IBS‐C: PEG, Lubiprostone, Linaclotide
CAM, complementary and alternative medicine; IBS-C, irritable bowel syndrome with constipation; IBS-D, irritable bowel syndrome with diarrhea; PEG, polyethylene glycol.
39
“Cornerstone of treatment” Listen actively Determine reasons for visit Identify and respond to
concerns and expectations Educate thoroughly Set realistic expectations Involve the patient in the treatment
Positive physician‐patient interaction reduces health care utilization and increases patient satisfaction
Drossman DA et al. Gastroenterology. 2002;123(6):2108-2131.; Owens DM et al. Ann Intern Med. 1995;122(2):107-112.Dorn SD et al, Clin Gastroenterol Hepatol. 2011;9(12):1065-1071.
40
Diary card symptom tracking can help identify exacerbating and alleviating factors and increase sense of control
Moderate exercise for 20 to 60 minutes x 3 to 5 days/week improves IBS symptoms
Johannesson E et al. Am J Gastroenterol. 2011;106(5):915-922.41
Among patients with IBS, diet is the#1 topic of interest
60% of subjects report that symptoms worsen after meals
The act of eating as well as the specific foods consumed may be one of many factors that influences IBS
Studying diet is quite challenging
True food allergies are very rare
General recommendations are possible, but diet should be tailored to the individual
Halpert A et al. Am J Gastroenterol. 2007;102(9):1972-1982.; Simrén M et al. Digestion. 2001;63(2):108-115.; CremoniniF,; Camilleri M. Gut. 2003;52(5):619-621.; Dainese R et al. Am J Gastroenterol. 1999;94(7):1892-1897. 42
Excess Fructose
Honey, apples, pears, peaches, mangos, fruit juice, dried fruit
LactoseMilk, ice cream, cheese,whey, curd
FructansWheat (large amounts), rye (large amounts), onions, leeks, zucchini
SorbitolApricots, peaches, artificial sweeteners and gums
RaffinoseLentils, cabbage, Brussels sprouts, asparagus, green beans, legumes
Fermentable Oligo‐, Di‐, Monosaccharides And Polyols
43
RCTs NResponse*
Fiber Placebo
RR of Unimproved Symptoms(95% CI)
NNT(95%CI)
Overall 12 591 48% 43% 0.87 (0.76‐1.0) 11 (5‐100)
Soluble 6 321 48% 36% 0.78 (0.63‐0.96) 6 (3‐50)
Insoluble 5 221 46% 46% 1.02 (0.82‐1.27)
*Improved or resolved symptoms.
CI, confidence interval; NNT, number needed to treat; RCTs, randomized, controlled trials; RR, relative risk.
46

Probiotics: live or attenuated microorganisms that have beneficial effects in humans
Meta‐analysis of 35 RCTs (n=3452) determined: “Probiotics are effective therapies for IBS” (global symptoms, pain, bloating, and gas) (NNT=7)
“We found evidence to support the use of combinations of probiotics as a group, although not for any of the different combinations studied individually.”
47
Up to 50% of all patients with IBS use some sort of CAM
Few CAM therapies have been rigorously evaluated for IBS: Peppermint – Safe and moderately efficacious for pain Acupuncture – Real and sham both more efficacious than
placebo
48
Smooth muscle relaxants with other anticholinergic effects Examples: dicyclomine, hyoscamine
Meta‐analysis of 22 RCTs comparing 12 different antispasmodics vs placebo (n=1778 patients) Significant heterogeneity among studies
Symptoms persist in 39% of patients receiving antispasmodics vs 56% of placebo‐treated patients (RR: 0.68; 95% CI: 0.57‐0.81)
Appear most useful for abdominal pain
Overall, these agents are cheap, widely available, and moderately efficacious for treating pain and bloating (and, possibly, urgency)
Ford AC et al. BMJ. 2008;337:b1881. 49
Tricyclic Antidepressants (TCAs): 9 studies (N=319 drug vs 256 control) Imipramine*, desipramine*, amitriptyline*, doxepin*; doses 10‐150 mg Meta‐analysis favors treatment
Selective Serotonin Reuptake Inhibitors (SSRIs): 5 studies (N=113 drug vs 117 control) Fluoxetine*, paroxetine*, citalopram*; dose 10‐40 mg Meta‐analysis favors treatment
Putative mechanisms include: Central effects (antinociception, +/‐ anxiolysis and antidepressive) Peripheral effects (SSRIs reduce gut transit, TCAs are modestly
anticholinergic)
Anecdotally, it is essential to (a) discuss the rationale for these medications, (b) explain that patients may not see benefits for 4 to 6 weeks and that the dose may need to be adjusted
Ford AC et al. Gut. 2009;58(3):367-378.
*These agents are not currently US Food and Drug Administration approved for IBS.50
RR NNTTrials N 95% CI 95% CI
Cognitive behavioral 7 491 0.60 3therapy 0.42‐0.87 2‐7
Relaxation 5 234 0.82
training 0.63‐1.08
Dynamic 2 273 0.60 3.5psychotherapy 0.39‐00.93 2‐25
Hypnotherapy 2 40 0.48 20.26‐0.87 1.5‐7
Anecdotally, it is critical to (a) identify appropriate candidates and (b) explain the rationale for psychological therapy
Ford AC et al. Gut. 2009;58(3):367-378.51
Study NFemale
%Response:
Alosetron, %Response: Placebo, %
Therapeutic
Gain, %
Camilleri1 370 53 60 33 27
Camilleri2 647 100 41 29 12
Camilleri3 626 100 43 26 17
Lembo4 801 100 73 57 16
Jones5 623 100 58 48 10
52

Female patients with chronic, severe IBS‐Dwho failed other treatments
Patient education regarding possible serious adverse effects of severe constipation or ischemic colitis
0.95 cases of ischemic colitis/1000 patient‐years
0.36 cases of severe constipation/1000 patient‐years
If ischemic colitis occurs, it is usually within the first month of therapy
Prescribing program mandated by US Food and Drug Administration
Requires patient to sign attestation form
53
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
# SBMs Pain Level
Placebo (n=71)
PEG 3350+E (n=68)
PEG is an alcohol that is not absorbed through the gut lumen. It creates an osmotic gradient that drives water into the lumen
139 adults with IBS‐C were randomized to placebo or PEG 3350 plus electrolytes (PEG 3350+E)
During week 4 of treatment, PEG improved number of SBMs (P<.0001), but not pain in IBS‐C patients
SBMs, spontaneous bowel movements.
54
12‐week treatment period
Overall responder: Monthly responder for at least 2 of 3 months
Monthly responder: At least moderate relief for 4/4 weeks or significant relief for 2/4 weeks
Ov
era
ll R
es
po
nd
ers
(%
)
n=387n=780
Lubiprostone8 µg bid
Placebo
*P=.001
17.9
10.1
0
25
50
Drossman DA et al. Aliment Pharmacol Ther. 2009;29(3):329-341. 56
Mean SBM Frequency per Month
8
7
6
5
4
3
2
1
01 2 3 4 5 6 7 8 9 10 11 12 13Baseline
Phase 3Studies
RandomizedWithdrawal/Extension Studies
Month of Treatment
Abdominal Pain/Discomfort
‐0.25
Month of Treatment
13121110987654321
‐0.50
‐0.75
‐1.00
‐1.25
‐1.50
Change From Base
line
P/L Group(n=179)
L/P/L Group(n=80)
L/L Group(n=261)
N=520 IBS‐C patients who completed 12 or 16 weeks of a placebo‐controlled phase 3 trial;patients enrolled in the extension study all received lubiprostone 8 µg bid.
P, placeboL, lubiprostone57
Most common AE diarrhea (19.7% vs 2.5%)
Chey WD et al. Am J Gastroenterol. 2012;107(11):1702-1712.
49.1
25.1
0
20
40
60
80
Lin 290 mcg Placebo
% A
deq
uat
e R
elie
f: IB
S S
ymp
tom
s
*P<.0001NNT=4.2
N=403N=401
AE, adverse event.
58
Patient‐Provider relationship
Lifestyle changes
Diet, fiber, and probiotics
CAM therapies
Antispasmodics
Antidepressants
Psychological therapies
Gut‐specific IBS‐D: Alosetron IBS‐C: PEG, Lubiprostone, Linaclotide
60