Embed Size (px)
Citation preview
Optimizing Therapy for Vancomycin-Resistant Enterococci (VRE)Peter K. Linden, M.D.1
ABSTRACT
Enterococci are gram-positive, facultative bacteria with low intrinsic virulence butcapable of causing a diverse variety of infections such as bacteremia with or withoutendocarditis, and intra-abdominal, wound, and genitourinary infection. During the past2 decades the incidence of hospital-acquired enterococcal infection has significantly risenand is increasingly due to multidrug-resistant strains, primarily to the coacquisitionof genetic determinants that encode for the stable expression of high-level b-lactam,aminoglycoside, and glycopeptide resistance.
Because enterococci constitute part of the normal colonizing flora, careful clinicalinterpretation of cultures that grow enterococci is paramount to avoid unnecessary andpotentially deleterious antimicrobial therapy. Traditional antimicrobial treatment forampicillin- and glycopeptide-susceptible enterococcal infection remains a penicillin-,ampicillin-, semisynthetic penicillin–based regimen, or vancomycin in a penicillin-intol-erant individual. The need for a bactericidal combination with a cell-wall active agentcombined with an aminoglycoside is most supported for native- or prosthetic valveendocarditis but is unproven for the majority of infections due to enterococci. Theemergence of vancomycin-resistant enterococci prompted the clinical development ofseveral novel and modified antimicrobial compounds approved for VRE infection (quinu-pristin-dalfopristin, linezolid) and several approved for non-VRE indications (daptomycin,tigecycline).
There is a paucity of comparative clinical trial data with these new agents,although linezolid, based upon its efficacy and tolerability, appears to be the cornerstoneof current treatment approaches. Despite a relatively short period of clinical use, enter-ococcal resistance has now been described for quinupristin-dalfopristin and linezolid andmore recently even for daptomycin and tigecycline. Moreover, the optimal treatment ofendocarditis due to VRE strains is unknown because, with the exception of daptomycin,current treatment options only yield bacteriostasis. Nonantimicrobial measures to treatVRE infection, such as foreign body removal and percutaneous or surgical drainage ofclose-spaced infection, reduce both the need for and the duration of anti-enterococcaltreatment and the emergence of resistance to the newer antimicrobials.
KEYWORDS: Enterococcus, vancomycin, linezolid, antimicrobial resistance,
nosocomial infection
1Department of Critical Care Medicine, University of PittsburghMedical Center, Pittsburgh, Pennsylvania.
Address for correspondence and reprint requests: Peter K. Linden,M.D., Department of Critical Care Medicine, University of PittsburghMedical Center, 602 A Scaife Hall, 3550 Terrace St., Pittsburgh, PA15261 (e-mail: [email protected]).
Optimizing Antimicrobial Therapy for Serious Infections in theCritically Ill; Guest Editor, David L. Paterson, M.D., Ph.D.
Semin Respir Crit Care Med 2007;28:632–645. Copyright # 2007by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York,NY 10001, USA. Tel: +1(212) 584-4662.DOI 10.1055/s-2007-996410. ISSN 1069-3424.
632

INCIDENCE OF ENTEROCOCCALINFECTION AND RESISTANCE TRENDSEnterococci have become more common and problematicpathogens over the past 2 decades, with a rise in both theoverall incidence of enterococcal infection and multidrugresistance. In a nationwide surveillance study [Surveil-lance and Control of Pathogens of EpidemiologicalImportance (SCOPE)] between 1995 and 2002, enter-ococci were the third most frequent cause of nosocomialbloodstream infection, and high-level vancomycin-resistance was present in 60% of Enterococcus faeciumstrains but only 2% of E. faecalis strains.1 A Centers forDisease Control and Prevention (CDC) surveillanceprogram during the same time period showed that VREaccounted for 27.5% of intensive care unit (ICU) noso-comial bacteremic and nonbacteremic infections.2 Thevast majority of E. faecium strains are multidrug resistantwith high-level resistance to penicillin and ampicillin(MIC > 128 mg/mL) and high-level resistance togentamicin (MIC > 1000 mg/mL), which eliminatesthe potential for bactericidal ‘‘synergistic’’ treatment.The forces behind this important trend include theincreased prevalence and greater longevity of immuno-compromised hosts due to native or iatrogenic immuno-suppression, the increased use of antimicrobials thatare devoid of enterococcal activity (cephalosporins,quinolones) and thus selective for more resistant pheno-types, and, most importantly, the appearance of newresistance mechanisms (i.e., high-level vancomycinresistance), which confer resistance to previously effectiveantimicrobial classes.
ANTIMICROBIAL RESISTANCEMECHANISMS AMONG ENTEROCCI
Intrinsic Resistance Mechanisms
Enterococci possess several constitutive, nontransferableresistance mechanisms against a variety of antimicro-bials, which limits therapeutic options even for vanco-mycin-susceptible enterococci and magnifies the effectof superimposed intrinsic resistance traits (Table 1).Relative or absolute resistance to the b-lactams (pen-icillin, ampicillin, antipseudomonal penicillins, cephalo-
sporins) is expressed in all enterococci due to theexpression of inner-cell-wall penicillin-binding proteins(PBPs) with low affinity for these compounds.3 Expo-sure of such enterococcal strains to an effective b-lactamresults in inhibitory but not bactericidal activity asmeasured by time-killing kinetic curves.4
Low-level resistance to aminoglycosides is secon-dary to their low penetrability through the outer-perim-eter envelope of the organism, a property that can beovercome with the synergistic activity of an effective cellwall active agent such as a penicillin or vancomycin.5
Although the majority of enterococci exhibit in vitrosusceptibility to trimethoprim/sulfamethoxasole theirability to utilize exogenous folate in vivo precludesthe clinical utility of trimethoprim-sulfamethoxazole(TMP/SMX) and other agents that impair folate syn-thesis.6 A significant percentage of enterococci may alsopossess constitutive resistance to macrolides (erythromy-cin, azithromycin) and lincosamides (clindamycin) pri-marily mediated by modification of the ribosomalattachment site.7
Acquired Resistance Mechanisms
There are few other species of bacteria that have theproclivity and efficiency of the Enterococcus to acquirenew and multiple antimicrobial resistance mechanisms3,4
(Table 2). The genomic elements that encode for resist-ance are carried on plasmid or larger transposon elements,are stable, and often carry multiple resistance determi-nants that culminate in multidrug-resistant strains. Enter-ococci acquire resistance to chloramphenicol (mediated bychloramphenicol acetyltransferase), quinolones (by gyrasemutations), rifampin (by mutation of the gene that enc-odes for RNA polymerase), and tetracyclines (by a varietyof mechanisms).8 However, the most clinically importantantimicrobials to which enterococci have acquired resist-ance are discussed in more detail following here.
High-Level b-Lactam Resistance
Overproduction and/or mutation of the penicillin-binding protein 5 receptor leading to diminished affinityfor b-lactams has increased dramatically in E. faecium
Table 1 Intrinsic Resistance Mechanisms among Enterococci
Antimicrobial Mechanism(s) Comments
Ampicillin, penicillin Altered binding protein
Aminoglycosides (LL) Decreased permeability Altered
ribosomal binding
High-level gentamicin strains may be
susceptible to high-level streptomycin
Clindamycin Altered ribosomal binding
Erythromycin Altered ribosomal binding
Tetracyclines Efflux pump
Trimethoprim-sulfamethoxasole Utilize exogenous folate
LL, low level.
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 633

but remains uncommon (< 5%) among E. faecalisstrains.9,10 This property is expressed constitutively andcarried by resistance genes located on chromosomal ele-ments. E. faecium strains with acquired high-level ampi-cillin resistance have ampicillin MICs > 128 mg/mL andare neither inhibited nor killed by ampicillin, penicillin,or other b-lactams. The ubiquity of high-level ampicillinresistance has been a major step toward the eventualevolution of multidrug resistance among E. faecium asthe superimposition of other resistance traits haveappeared in such strains.
High-Level Aminoglycoside Resistance
The first reports of high-level gentamicin resistant(HLGR) strains in the United States were in 1979,appearing in both E. faecalis and E. faecium.11 More recentsurveillance data from the SCOPE program between theyears 1997 and 1999 showed 69 to 71% of all U.S.enterococcal strains were HLGR and 40% of all testedvancomycin-resistant enterococci (VRE) strains.12 Enter-ococci acquire resistance to aminoglycosides via (1)changes in the ribosomal attachment sites; (2) diminishedaminoglycoside transport into the cell; and (3)aminoglycoside-modifying enzymes (adenyltransferase,phosphotransferase, and bifunctional acetyl-phospho-transferase). Although the majority of HLGR strainsalso exhibit high-level streptomycin resistance, a minorityretain sensitivity to streptomycin; thus susceptibility test-ing to high-level streptomycin is worthwhile in HLGRstrains.13 No reliable bactericidal activity can be achievedwith any antimicrobial combination against strains withhigh-level aminoglycoside resistance.14
VANCOMYCIN AND OTHERGLYCOPEPTIDE RESISTANCE
Epidemiology
Without question, the appearance of E. faecium strainswith high-level vancomycin resistance in France and
England in 1986 was a major watershed mark in theevolution of enterococcal antimicrobial resistance andthe final step toward the subsequent establishment ofendemic multidrug-resistant enterococci.15,16 VREstrains did not first appear in the United States until1989, but thereafter their incidence rapidly increasedfrom 0.3% of all enterococci in 1989 to 7.9% in 1993.17
During this early period the majority of reported VREisolates were almost exclusively E. faecium, were mono-or pauciclonal in origin, and predominantly originatedfrom ICU patients in tertiary care centers, particularly inthe northeastern United States, where both vanA andvanB genotype outbreaks were observed; however, therewas no discernible epidemiologic or clinical differentia-tion between the two types. Local enhancement ofcontact precautions usually aborted or significantlymodified such outbreaks.
A more contemporaneous surveillance study ofbloodstream isolates has shown a steady decrease invancomycin susceptibility among E. faecium strainsfrom 60% in 1997 to only 39.1% in 2002, whereas thevast majority (96.1 to 99.4%) of E. faecalis strainscontinue to remain vancomycin susceptible over this5-year period.18 The incidence of VRE remains highestin the intensive care unit setting. It has increased to agreater relative extent on hospital floors and parahospitalcenters such as long-term acute care (LTAC) facilitiesand skilled-care nursing facilities, which often receivepatients from hospitals with endemic VRE epidemi-ology.19
Genetic Basis of Vancomycin Resistance
Six distinct glycopeptide resistance phenotypes havebeen discovered: VanA, VanB, VanC, VanD, VanE,and VanG, distinguished based upon gene content,glycopeptide minimum inhibitory concentrations(MICs), and inducibility and transferability properties20
(Table 3). The vanA and vanB phenotypes uniformlyconfer high-level vancomycin resistance (MIC > 64 mg/mL) and have the highest prevalence and clinical
Table 2 Acquired Resistance Mechanisms among Enterococci
Antimicrobial Mechanism(s) Comments
Ampicillin, penicillin (HL) Mutation of pbp-5 95% of E. faecium < 5% E. faecalis
Aminoglycoside (HL) Enzyme modification Plasmid mediated Some HL-gentamicin
R strains may be streptomycin S
Quinolones DNA gyrase mutation
Chloramphenicol Efflux pump
Glycopeptide Altered cell wall binding Transposon 1546
Quinupristin/dalfopristin Ribosomal modification Efflux pump ermB gene vatd, vate gene
Linezolid Single point mutation G2476U mutation
Daptomycin Unknown Described in E. faecalis, E. faecium,
and E. durans
HL, high level.
634 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007
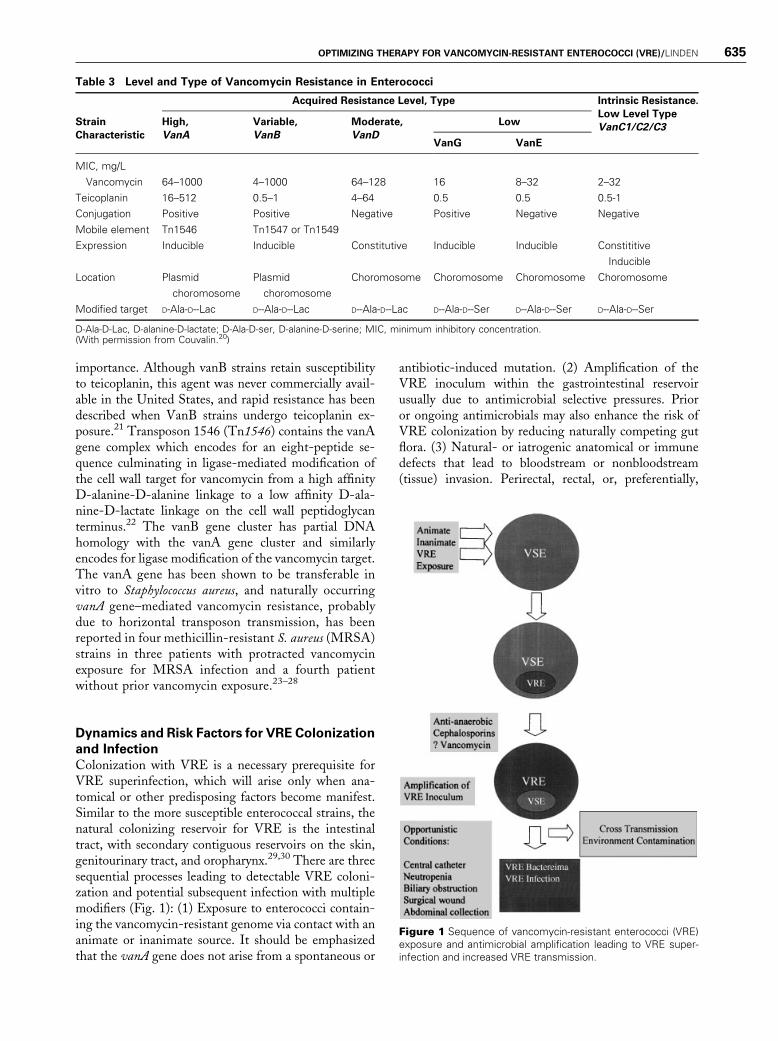
importance. Although vanB strains retain susceptibilityto teicoplanin, this agent was never commercially avail-able in the United States, and rapid resistance has beendescribed when VanB strains undergo teicoplanin ex-posure.21 Transposon 1546 (Tn1546) contains the vanAgene complex which encodes for an eight-peptide se-quence culminating in ligase-mediated modification ofthe cell wall target for vancomycin from a high affinityD-alanine-D-alanine linkage to a low affinity D-ala-nine-D-lactate linkage on the cell wall peptidoglycanterminus.22 The vanB gene cluster has partial DNAhomology with the vanA gene cluster and similarlyencodes for ligase modification of the vancomycin target.The vanA gene has been shown to be transferable invitro to Staphylococcus aureus, and naturally occurringvanA gene–mediated vancomycin resistance, probablydue to horizontal transposon transmission, has beenreported in four methicillin-resistant S. aureus (MRSA)strains in three patients with protracted vancomycinexposure for MRSA infection and a fourth patientwithout prior vancomycin exposure.23–28
Dynamics and Risk Factors for VRE Colonization
and Infection
Colonization with VRE is a necessary prerequisite forVRE superinfection, which will arise only when ana-tomical or other predisposing factors become manifest.Similar to the more susceptible enterococcal strains, thenatural colonizing reservoir for VRE is the intestinaltract, with secondary contiguous reservoirs on the skin,genitourinary tract, and oropharynx.29,30 There are threesequential processes leading to detectable VRE coloni-zation and potential subsequent infection with multiplemodifiers (Fig. 1): (1) Exposure to enterococci contain-ing the vancomycin-resistant genome via contact with ananimate or inanimate source. It should be emphasizedthat the vanA gene does not arise from a spontaneous or
antibiotic-induced mutation. (2) Amplification of theVRE inoculum within the gastrointestinal reservoirusually due to antimicrobial selective pressures. Prioror ongoing antimicrobials may also enhance the risk ofVRE colonization by reducing naturally competing gutflora. (3) Natural- or iatrogenic anatomical or immunedefects that lead to bloodstream or nonbloodstream(tissue) invasion. Perirectal, rectal, or, preferentially,
Figure 1 Sequence of vancomycin-resistant enterococci (VRE)exposure and antimicrobial amplification leading to VRE super-infection and increased VRE transmission.
Table 3 Level and Type of Vancomycin Resistance in Enterococci
Strain
Characteristic
Acquired Resistance Level, Type Intrinsic Resistance.
Low Level Type
VanC1/C2/C3High,
VanA
Variable,
VanB
Moderate,
VanD
Low
VanG VanE
MIC, mg/L
Vancomycin 64–1000 4–1000 64–128 16 8–32 2–32
Teicoplanin 16–512 0.5–1 4–64 0.5 0.5 0.5-1
Conjugation Positive Positive Negative Positive Negative Negative
Mobile element Tn1546 Tn1547 or Tn1549
Expression Inducible Inducible Constitutive Inducible Inducible Constititive
Inducible
Location Plasmid
choromosome
Plasmid
choromosome
Choromosome Choromosome Choromosome Choromosome
Modified target D-Ala-D--Lac D--Ala-D--Lac D--Ala-D--Lac D--Ala-D--Ser D--Ala-D--Ser D--Ala-D--Ser
D-Ala-D-Lac, D-alanine-D-lactate; D-Ala-D-ser, D-alanine-D-serine; MIC, minimum inhibitory concentration.(With permission from Couvalin.20)
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 635

stool cultures have been the traditional sites to detectVRE colonization.31,32 The duration of VRE intestinalcolonization is variable, can last for months to years, andmay be indefinite, in part subject to the inoculum-detection threshold of the surveillance testing methodemployed.33–35 Spontaneous clearance of intestinal col-onization only occurs in the minority of patients inseveral studies analyzing serial cultures in both antimi-crobial- and nonantimicrobial-exposed patients.
Multiple case control and cohort studies haveanalyzed risk factors for either VRE colonization,VRE superinfection, or both.36–39 Two fundamentalrisk factor categories are demographic/illness severityvariables and the type, intensity, and duration of recentantimicrobial exposure. Demographic risks include du-ration of hospital- and ICU length of stay, physicalproximity to VRE-colonized patients in the same unit,and hospitalization in units with a high prevalence ofVRE, ‘‘colonization pressure.’’ Prior administration ofmultiple antibiotics, third-generation cephalosporins,antimicrobials with anaerobic spectrums (metronidazole,clindamycin), and parenteral vancomycin have beenimplicated in case-control analyses of colonization orsuperinfection. Such antimicrobials probably exert aselective effect and amplify otherwise undetectable orsmaller VRE inocula in the intestines and other secon-dary reservoirs. Donskey and colleagues have demon-strated that the density of VRE as measured by serialquantitative stool cultures increased significantly whenpatients received � 1 antianaerobic antimicrobial,whereas this effect was not seen in patients receivingantimicrobials with minimal antianaerobic activity.40
Interestingly, parenteral vancomycin administration re-sulted in no increase in the stool VRE density. More-over, patients with high VRE density coupled with fecalincontinence were also more likely to have positiveenvironmental cultures for VRE. The ‘‘VRE-selective’’effects of antimicrobials and other risk factors becomerelatively diminished when the proportion of patientsalready colonized with VRE is 50% or greater, whichmay explain some studies where newly introduced anti-biotic control measures may only yield modest reduc-tions in VRE colonization and infection rates inhyperendemic settings.41 Patients with comorbidities,including oncologic conditions, especially neutropenia,and prior solid organ transplantation, especially livertransplantation, appear to have the highest rates ofVRE bacteremia and poorest outcomes.
GENERAL ISSUES IN THE TREATMENT OFENTEROCOCCAL INFECTIONThe treatment of serious enterococcal infection is chal-lenging from several aspects. Because enterococci maycolonize skin, wound, and mucosal surfaces and theirisolation is often accompanied by more virulent patho-
gens, a careful clinical assessment of whether the re-ported isolate is a likely cause of the patient’s clinicalsyndrome that merits specific treatment is always war-ranted. Realistically, however, it may be difficult to makethis distinction, particularly in patients who have majorcomorbid conditions or critical illness that is naturallycoupled with colonization or infection due to multidrug-resistant enterococcal strains. Although enterococci areof low virulence, it bears emphasis that they are alsoquite capable of promulgating the systemic inflammatoryresponse syndrome (SIRS), severe sepsis, and septicshock and have been a frequent inciting blood pathogenin recent prospective, randomized sepsis trials.42
Abundant and recent observational studies sup-port the association between appropriate empiricalantimicrobial therapy and survival.43–45 Thus, for thesevere end of the clinical spectrum, strong considerationshould be given to empirical antienterococcal therapy forpatients whose demographic features and clinical pre-sentation place them at high risk for enterococcal in-fection or sepsis. Clearly a major part of this decision alsoincludes estimating the likelihood that the enterococcalstrain could be a multidrug-resistant strain. Such epi-demiological and clinical clues, which might promptempirical enterococcal therapy, are summarized inTable 4.
Does the Enterococcus in the Culture Result
Require Antimicrobial Treatment?
Microbiological culture data that report the presence ofenterococci always require some level of clinical discrim-ination to determine whether they merit treatment.Enterococcal isolates from a respiratory specimen (spu-tum, endotracheal aspirate, bronchoalveolar lavage), andskin, wound, or mucosal surfaces almost always representcolonization. Urine cultures obtained via indwellingbladder (Foley) catheters often represent asymptomaticbacteriuria. Wound and intra-abdominal drains oftenbecome colonized with skin flora, including enterococci.
Table 4 Clinical and Epidemiological Clues That MDREnterococcal Infection Is Present
Significant and recent antimicrobial exposure
Multiple agents
Third-generation cephalosporins
Antianaerobic antimicrobials
Vancomycin
Positive rectal-fecal surveillance culture or vancomycin-resistant
enterococci from a prior clinical site
Intra-abdominal infection (abscess, peritonitis, cholangitis)
Indwelling catheters in place (bladder, intravascular)
High incidence of MDR enterococci in unit, hospital
Prior liver transplant, neutropenia, chemotherapy-related
mucositis
MDR, multidrug-resistant.
636 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007

However, such isolates may be significant when thecharacter of the drainage fluid reveals evidence ofinflammatory response (i.e., pyuria or purulence).Although enterococci may be blood culture contami-nants, particularly when specimens are obtained fromindwelling intravascular catheters, the appropriate clin-ical bias should be that such cultures represent truepathogens in most instances. Finally, simple nonantimi-crobial interventions may obviate the need for antienter-ococcal therapy, such as removal of intravascular orbladder catheters or superficial wound debridement.46,47
Is Bactericidal Therapy Required?
The majority of enterococcal infections are not proven torequire bactericidal treatment and can be managedsuccessfully with a single effective agent.48,49 Eithernative- or prosthetic-valve endocarditis is the prototyp-ical enterococcal infection for which bactericidal anti-microbial therapy is required, usually achieved with thecombination of a cell wall–active agent such as ampicil-lin, penicillin, or vancomycin combined with an amino-glycoside such as gentamicin or streptomycin. Othersites of infection for which bactericidal treatment isprobably merited include enterococcal meningitis andenterococcemia in a neutropenic host.
However, a bactericidal combination is not pos-sible to achieve with enterococci exhibiting high-levelaminoglycoside resistance and almost all strains ofE. faecium strains with high-level vancomycin resistance.Uncommon exceptions are vancomycin-resistant E.faecalis strains, which retain ampicillin and high-levelgentamicin susceptibility. Successful treatment of suchcases has been reported with ampicillin and gentamicin,ampicillinþ ofloxacin, penicillinþ streptomycin, andlinezolidþ gentamicin.50 Limited clinical experienceis available for the treatment of vancomycin-resistantenterococcal endocarditis with the newer agents (seelater discussion).
Nonantimicrobial Treatment of VRE Infection
Many VRE infections may be partially or completelycured with conservative or aggressive nonantimicrobialinterventions. Less serious infections such as bladdercatheter–associated bacteriuria and urinary tract infec-tion may be adequately treated simply with catheterremoval. Postoperative superficial wound infectionsmay also respond to opening the incision and simpledrainage or debridement. Closed-space infection such asintra-abdominal abscesses, cholangitis due to biliaryobstruction, devitalized tissue, or infected foreign bodies(intravascular catheters, synthetic graft or mesh material,prosthetics) are not infrequently the primary source ofVRE bacteremic or nonbacteremic infection. The treat-ment implications for infections with such anatomical
considerations is summarized in Table 5. It also bearsemphasis that the inability to address the nonantimicro-bial considerations of such complex VRE infections hasbeen the principal cofactor leading to the development ofVRE strains that have evolved resistance to the recentlyapproved VRE antimicrobials, quinupristin-dalfopristinand linezolid.
Specific Antimicrobials for the Treatment of
Vancomycin-Resistant Enterococcal Infection
Despite the established high prevalence of multidrug-resistant enterococcal strains with high-level vancomy-cin-resistance there is a remarkable paucity of controlled,comparative trial data on its antimicrobial treatment.Major obstacles have been the slow development ofnovel agents with VRE activity, high levels of comor-bidity that confound outcome interpretation, complexsurgical infection for which antimicrobial therapy aloneis not curative, and the polymicrobial nature of manyVRE infections, particularly those occurring in theabdomen. Both approved and nonapproved treatmentoptions for VRE are summarized in Table 6. At presentthere are only two U.S. Food and Drug Administration(FDA)-approved treatments for VRE (E. faecium) in-fection: quinupristin/dalfopristin (Q/D, Synercid, KingPharmaceuticals, Inc., Bristol, TN) and linezolid (Zyvox,Pfizer, New York, NY) and two other approved agentsthat have in vitro activity against VRE but are notapproved for VRE infection; daptomycin (Cubicin,Cubist Pharmaceuticals, Lexington, MA), which is ap-proved for complicated skin–skin structure infection,
Table 5 Nonantimicrobial Interventions forVancomycin-Resistant Enterococcal Infections
Site of Infection Nonantimicrobial Intervention
Bloodstream Catheter removal
Consider endovascular infection if
no primary source obvious or
patient with risk factors for
endocarditis or other endovascular
material
Closed-space
infection
Consider percutaneous or surgical
drainage, e.g., cholangitis—
percutaneous transhepatic
drainage or endoscopic retrograde
cholangiopancreatography for
stent placement
Urinary tract infection
or bacteriuria
Removal of bladder catheter
Superficial wound
infection
Incision and drainage or debridement
Suspected foreign
body infection
May require removal if refractory
to antimicrobial therapy
or adjacent to devitalized tissue
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 637

and S. aureus bacteremia and tigecycline (Tygacil, WyethPharmaceuticals, Inc., Philadelphia, PA), which is ap-proved for complicated skin–skin structure and intra-abdominal infection.
Prior to the availability of Q/D and linezolidapproval several centers published their experience witha variety of available agents or combinations that dem-onstrated in vitro activity. Clinical success was describedwith high parenteral dosages of ampicillin or ampicillin/sulbactam (18 to 24 g/day), even including endocarditis.Such a strategy appears limited to those uncommon VREstrains with ampicillin MICs of 32 to 64 mg/mL, a targetrange for which plasma ampicillin levels can be achievedwith high dose therapy.50–52 Because no b-lactamaseelaboration occurs with VRE, the mechanism of sulbac-tam activity is not known, although a plausible explan-ation is its intrinsic penicillin-binding protein properties.
Chloramphenicol has bacteriostatic activity againstenterococci and VRE strains; however, its in vivo efficacywas never established. In a retrospective study of 80 casesof VRE bacteremia, 51 patients were treated with chlor-amphenicol from which 22/36 (61%) evaluable patientsdemonstrated a clinical response.53 A microbiologicalresponse was also observed in 33/43 (77%) of the micro-biologically evaluable patients. No survival benefit wasobserved compared with VRE bacteremic patients in thestudy cohort who did not receive chloramphenicol. Sub-sequently at the same center, the prevalence of chloram-phenicol resistance among VRE strains over a 10-yearperiod (1991 to 2000) were observed to increase from 0 to11%, a trend that correlated significantly with priorchloramphenicol or quinolone exposure.54 Isolated re-ports of favorable outcome for VRE infection have also
been reported with the use of tetracycline, doxycycline,and oral novobiocin combined with either ciprofloxacin ordoxycycline; however, such experience has never been rep-roduced in larger clinical series of prospective trials.55–58
Teicoplanin, a glycopeptide not commerciallyavailable in the United States, does have in vitro activityversus VanB phenotypic enterococci. In a Europeanstudy of 63 patients with vancomycin-susceptible enter-ococcal infection, clinical and microbiological responseswere observed in 84% and 87% of cases, respectively.59
This agent remains unstudied for VanB enterococcalinfection, perhaps in part due to the development ofteicoplanin resistance among VanB E. faecalis duringteicoplanin therapy.60,61
Nitrofurantoin has in vitro activity against bothVanA and VanB enterococci.62 Due to its ability toachieve high urinary concentrations nitrofurantoin hasbeen shown to be effective in VRE urinary tractinfection.46,63 Nitrofurantoin cannot be employed forVRE outside the urinary tract and in patients with acreatinine clearance < 30 mL/min because elevatedblood concentrations are associated with hepatic, pul-monary, hematologic, and other toxicities.
QUINUPRISTIN/DALFOPRISTIN
Quinupristin/dalfopristin (Q/D) is a semisyntheticparenteral streptogramin compound, which is derivedfrom its parent natural compound pristinamycin, aproduct of Streptomyces pristinaspiralis, an oral and top-ical antistaphylococcal agent that has been in clinical usein Europe since the 1980s. The major properties of thiscompound are summarized in Table 7. This antimicro-bial is a 30:70 mixture of quinupristin and dalfopristin,
Table 6 Therapeutic Antimicrobial Options for VRE Infection
Antimicrobial(s) Reported Evidence Comments
High-dose ampicillin or
ampicillin-sulbactam
Case reports May be effective with VRE strains
with ampicillin MIC 32–64 mg/mL
Chloramphenicol Case series Resistance reported
Tetracycline, doxycycline Case reports � rifampin or ciprofloxacin
Novobiocin Anecdotal No longer manufactured
Nitrofurantoin Small case series Only for urinary tract infections
Teicoplanin Case reports Not active against VanAResistance in VanB reported
Quinupristin/dalfopristin Large case series but noncomparative Bacteriostatic
Not active against E. faecalis
Resistance reported
Linezolid 1. Dose comparative trial Bacteriostatic
2. Large compassionate use series Resistance reported
Daptomycin 1. Case reportþ series Bactericidal
Resistance reported
Tigecycline In vitro data only Bacteriostatic
Dalbavancin In vitro data only VanA strains resistant
Telavancin In vitro data only
Oritavancin In vitro data only
MIC, minimum inhibitory concentration.
638 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007

which are derivatives of streptogramin types B and A,respectively. It is a unique antimicrobial because it actsthrough sequential ribosomal binding and is internallysynergistic to produce a bactericidal effect. Dalfopristininitially binds to the 50S bacterial ribosome, which in-duces a permanent conformational change that acceler-ates quinupristin ribosomal binding.64 Protein synthesisis impaired via both the interruption of peptide chainelongation and the inhibition of formed peptide extru-sion. SSuch synergism results in bactericidal activityagainst some important gram-positive species, includingStreptococcus pneumoniae, Streptococcus agalacticae, andsome strains of Staphylococcus aureus. However, onlybacteriostatic activity is present for the majority of E.faecium strains by time–killing curve studies. This effect isprimarily mediated by 23S ribosomal modificationencoded for by the ermB gene (erythromycin methylase),which reduces quinupristin affinity for its ribosomalbinding site and thus limits activity to only the dalfopris-tin moiety. Such strains are termed MLSb (macrolide-lincosamide-streptogramin) phenotypes.65 Erythromycinresistance serves as an excellent surrogate marker for thepresence of the MLSb phenotype among enterococci.Q/D is also unique as an antienterococcal agent basedupon its marked disparity in in vitro susceptibility be-tween E. faecium (MIC90¼ 1 to 2 mg/mL) and E. faecalis(MIC90¼ 8 to 16 mg/mL). This disparity is most likelydue to altered ribosomal binding or presence of an activeefflux pump.
Clinical interest in the utility of Q/D for seriousVRE infection began in the mid-1990s with a large-scale, noncomparative, open-label, emergency useprogram for multiresistant gram-positive infection, prin-cipally vancomycin-resistant E. faecium and MRSA in-fection refractory or intolerant to vancomycin.66,67 Thepatient populations in both series had a high prevalenceof acute and chronic comorbidities, including diabetes,oncologic conditions, chronic liver disease, dialysis me-chanical ventilation, and prior organ transplantation.Q/D was administered at 7.5 mg/kg intravenously every8 hours to patients with documented VRE bacteremia ornonbacteremic VRE infection, with the duration oftreatment determined by the primary treating physi-cians. The overall success rate defined as both clinicalsuccess and bacteriologic eradication was 65.8% in theinitial study and 65.6% in the follow-up study. Therehave been several reports of clinical cure combining Q/Dwith doxycycline or high-dose ampicillin in endocarditis;however, no larger-scale experience has been per-formed.68–70
As Q/D usage increased both before and after itsregulatory approval in 1999, several important clinicallimitations became apparent. Peripheral intravenousadministration was associated with a high rate ofphlebitis necessitating central venous administration.Myalgia and arthralgia unassociated with objectiveinflammatory signs were observed in 7 to 10% of patientsin the emergency use program, with much higher rates in
Table 7 Major Features of Quinupristin/Dalfopristin and Linezolid
Feature Quinupristin/ Dalfopristin Linezolid
Antimicrobial class Streptogramn Oxazolidinone
Peak serum concentrations (mg/L) 10-12 15.1
Elimination half-life (h) 0.8 (Q) , 0.6 (D) 5.5
Major metabolic routes Hepatobiliary Peripheral nonoxidative
Major elimination routes Faecal (70-75%) Nonrenal (65%)
Urinary (19%) Urinary (30%)
Protein binding (%) 30 (Q) 70 (D) 31
Mechanism of action Protein synthesis inhibition Protein synthesis inhibition
Site of action 50S ribosome 70S initiation complex
Postantibiotic effect (h) 6–8 1
Bactericidal (vs VRE) No No
Cytochrome P-450 inhibition Yes No
Formulations Parenteral Parenteral þ oral
Dose and administration 5–7.5 mg/kg q 8–12h 600 mg q12 h
Dosage adjustment None None
Approved indications VRE VRE
Complicated SSSI Complicated SSSI
Nosocomial pneumonia Nosocomial pneumonia
Major adverse effects Phlebitis (peripheral) Myelosuppression
Myalgia/arthralgia
Cost ($US per day; 2000 values) $300-350 $115 (parenteral)
$80 (oral)
D, dalfopristin; Q, quinupristin; qXh, every X hours; SSSI, skin and skin structure infection; VRE, vancomycin-resistant enterocooci.(With permission from Linden.42)
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 639

oncologic patients and liver transplant recipients.71,72
Although the precise reason for this toxicity is unknowna neuropathic cause is suspected. Its higher incidence inpopulations with diminished metabolism and excretionsuggest it is due to either native drug or metaboliteaccumulation. Phenotypic resistance to Q/D amongE. faecium (MIC � 4 mg/mL) was observed in six(1.8%) and five (1.3%) of VRE cases, either during orafter treatment, from both published emergency useseries.71,72 Clonal dissemination of Q/D-resistantstrains despite the absence of Q/D or other streptogra-min exposure has been described among pediatric pa-tients.73 Three fundamental resistance mechanisms havebeen discovered: enzymatic modification (acetylation) ofdalfopristin encoded by the vatD or vatE genes, activeefflux by an adenosine triphosphate (ATP)-bindingprotein encoded by the msrC or lsa genes, and alterationof the ribosomal target site encoded for by the ermgenes.70 Because phenotypic resistance requires thepresence of resistance mechanisms to both the quinu-pristin and the dalfopristin components, at least two ormore resistance genes are present. Several surveillancestudies have uncovered large Q/D resistance reservoirsamong E. faecium isolated from both domestic poultryand livestock in the United States, which may relate tothe use of virginiamycin as a growth-promoting foodadditive in domestic poultry.74
LINEZOLID
Linezolid is an oxazolidinone compound, a novel syn-thetic class that inhibits bacterial protein synthesis in aunique fashion via inhibiting the formation of the 70Sinitiation complex (50S and 30S ribosomes, mRNA,initiation factors 2 and 3, and fMet-tRNA).75 The majorproperties of linezolid are summarized in Table 6. Line-zolid exhibits a broad gram-positive spectrum but hasonly bacteriostatic activity against vancomycin-resistantor susceptible enterococci with an MIC90 of 2 mg/mL,which is right at the susceptibility breakpoint. FDAapproval was granted in 2000 for vancomycin-resistantE. faecium infection in addition for other indications,including community-acquired and nosocomial pneu-monia and complicated skin and skin structure infection.Due to the lack of an approved comparator agent,linezolid was evaluated for patients with clinical andmicrobiological evidence of serious VRE infection in ablinded, parenteral, dose-comparative trial comparing66 patients randomized to 200 mg q 12 hours to79 patients treated with 600 mg q 12 hours.76 Amongevaluable patients at end-of-treatment, a modest doseresponse was observed, with 67% and 52% response ratesseen in the high-dose and low-dose groups, respectively.In addition, efficacy and safety were also demonstratedin a large study (n ¼ 796 patients) emergency-useprogram for resistant, or treatment-refractory, or treat-ment-intolerant patients with serious gram-positive
infection.77 Among 549 cases of VRE infection, therewas an 81.4% clinical cure rate at end-of-therapy.Because linezolid is a bacteriostatic agent that displaysno synergistic activity with other agents its efficacy inVRE native- or prosthetic-valve endocarditis remainsquestionable. Both clinical success and failure have beenreported when linezolid has been used as a first-linetherapy or salvage treatment; however, no large-scalerandomized trial experience is yet available.78–80 Inrecent years, linezolid has become the dominant agentfor the treatment of serious VRE infection. Multiplecases report of linezolid-resistance (MIC � 8 mg/mL)occurring in VRE (E. faecium) and vancomycin-suscep-tible E. faecalis strains that were susceptible (MIC 1 to2 mg/mL) at baseline but developed a fourfold or greaterrise in MIC to 8 to 32 mg/mL.81–85 Common to mostcases where linezolid-resistance appeared has been aprotracted length of therapy (> 28 days) associatedwith retained foci of VRE infection such as abscesses,devitalized tissue, or foreign materials. The majority oflinezolid-resistant isolates contain a single base-pairmutation in the genome encoding for domain V of the23S ribosomal binding site (G2476U mutation). Thephenotypic level of resistance as determined by elevationin MIC level has been shown to correlate with the ‘‘genedose’’ or number of copies of 23S rDNA containing theG2466U mutation.86 Notably this mutation was pre-dicted by earlier in vitro spiral plate serial passageexperiments with linezolid.87 Horizontal cross trans-mission of an identical clone of linezolid-resistantE. faecium among linezolid-naive patients within thesame ICU or hospital center have also been de-scribed.88,89 A case- controlled analysis revealed that alonger course of linezolid (38 days vs 11 days) andlinezolid exposure prior to hospitalization were riskfactors for the emergence of linezolid-resistant VRE.90
Thus repeat linezolid susceptibility testing is advisable inpatients who have had prior linezolid exposure or per-sistent isolation of a VRE strain on therapy or in patientstreated in a nosocomial setting with prior linezolidresistance. Although gastrointestinal symptoms are themost common reported toxicity, reversible myelosup-pression (thrombocytopenia, leukopenia, and/or anemia)has been the most important treatment-limiting sideeffect with higher rates observed than the original regis-tration studies. Bone marrow examination has shownchanges similar to those observed with reversible chlor-amphenicol toxicity.91,92 Such toxicity is usually observedonly with sustained linezolid treatment that exceeds2 weeks. Other reported toxicities of note includegastrointestinal upset, rare cases of serotonin syndrome,optic- and peripheral neuropathy, and lactic acidosis.93–96
DAPTOMYCIN
Daptomycin is a novel cyclic lipopeptide compound witha broad gram-positive spectrum and rapid bactericidal
640 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007

activity that is currently approved for complicatedskin–skin structure infection and S. aureus bacteremia,including right-sided endocarditis.97 Its apparentmechanism of action includes attachment to the exteriorof the bacterial cytoplasmic membrane with membranepenetration of a lipophilic tail with disruption of thetransmembrane potential due to ion efflux, an effect thatis both concentration- and calcium ion–dependent andleads to nonlytic bacterial cell death. In vitro studieshave shown nearly uniform activity against vancomycin-resistant E. faecium and E. faecalis strains with an MIC90 of 2–4 mg/mL.98,99 In one recent study examiningonly VRE strains that were either linezolid- or Q/D-resistant, daptomycin demonstrated susceptibility usinga 4 mg/mL provisional breakpoint.100 The MIC break-point is 4 mg/mL for vancomycin-susceptible E. faecalis;however, there is no established breakpoint for vanco-mycin-susceptible or -resistant E. faecium. Regardlessof the testing method (E-test, disk diffusion, or brothdilution) the zone size or MIC result can be signifi-cantly elevated by a two- to eightfold magnitude withinadequate calcium supplementation. To the presenttime, clinical experience with daptomycin for seriousVRE infection remains quite limited. The optimaldosing for enterococcal infection is not yet established;however, daily dosing at 6 mg/kg in the absence of renalinsufficiency has been the most common dosing scheme.A randomized phase 3 trial versus linezolid in VREinfection was aborted due to enrollment difficulties.In a study of nine neutropenic patients with VREbacteremia treated with daptomycin at 4 mg/kg/dayor 6 mg/kg/day, a clinical and/or microbiological re-sponse was observed in only 4/9 (44%).101 In a secondreport a similar response rate of 5/11 (45%) wasobserved in patients with VRE bacteremia and endo-carditis treated with 6 mg/kg/day of daptomycin.102
Unfortunately, daptomycin resistance has been re-ported during treatment for vancomycin-resistantE. faecalis, E. faecium, and E. durans infection with arise in the MIC to � 8 mg/mL.103–106
TIGECYCLINE
Tigecycline is the first approved agent of the glycylcy-cline class, a group closely related to the tetracyclines butsynthetically modified to achieve an enhanced spectrumof activity against MRSA, other multiresistant gram-positive species, and many gram-negative bacilli.107
Tigecycline is currently approved for complicatedskin–skin structure and intra-abdominal infection basedupon phase 3 studies showing comparability to standardcomparator regimens. Vancomycin-resistant enterococciwere not included in these registration trials.However, daptomycin exhibits very low MICs forboth vancomycin-susceptible and vancomycin-resistantversus clinical strains of E. faecium and E. faecalis(MIC90 ¼ 0.012 mg/mL), although National Commit-
tee for Clinical Laboratory Standards (NCCLS) break-points for vancomycin-resistant E. faecium strains are notyet established.108,109 Although clinical experience withtigecycline for VRE infection is not yet availableit appears to be a promising option, particularly forintra-abdominal sites, where it has shown comparableefficacy to meropenem in non-VRE monomicrobial andpolymicrobial infection.
NOVEL GLYCOPEPTIDES (ORITAVANCIN, DALBAVANCIN,
TELAVANCIN)
Several new glycopeptide derivatives have in vitro bac-tericidal activity against VRE. Dalbavancin is a long-acting (half-life 7 to 10 days) derivative of teicoplanin,which has received approval for the treatment of com-plicated skin–skin structure infection; however, similarlyto teicoplanin, this agent lacks in vitro activity againstthe more prevalent VanA enterococcal strains.110
Oritavancin is a semisynthetic glycopeptide that blockspeptidoglycan synthesis and exerts bactericidal activityacross a broad gram-positive spectrum.111 It has superioractivity against vanA and vanB enterococci comparedwith dalbavancin and telavancin, with concentration-dependent bactericidal activity against both E. faeciumand E. faecalis strains (MIC90¼ 1 to 2 mg/mL) and issynergistic with ampicillin against the majority of iso-lates.112 This agent has completed phase 3 trials in cSSSI(complicated skin-skin structure infection); however,concerns pertaining to its long half-life, high proteinbinding, and reports of spontaneous resistance maylimit its development.
Telavancin, a long-acting lipoglycopeptide withmultiple sites of action at the cell membrane and cellwall has shown noninferiority versus standard therapy ingram-positive cSSSI, including MRSA; however, clin-ical data for VRE are not yet available.113,114
REFERENCES
1. Centers for Disease Control and Prevention. NationalNosocomial Infection Surveillance (NNIS) system: report,data summary from January 1992 through June 2003, issuedAugust 2003. Am J Infect Control 2003;31:481–498
2. Wisplinghoff H, Bischoff T, Tallent SM, Seiferd H,Wenzel RP, Edmond MB. Nosocomial bloodstreaminfections in US hospitals: analysis of 24,179 cases from aprospective nationwide surveillance study. Clin Infect Dis2004;39:309–317
3. Moellering RC Jr. The Garrod Lecture. The Enterococcus: aclassic example of the impact of antimicrobial resistance ontherapeutic options. J Antimicrob Chemother 1991;28:1–12
4. Murray BE. The life and times of the Enterococcus. ClinMicrobiol Rev 1990;3:46–65
5. Hodges TL, Zighelboim-Daum S, Eliopoulos GM,Wennersten C, Moellering RC Jr. Antimicrobial suscept-ibility changes in Enterococcus faecalis following variouspenicillin exposure regimens. Antimicrob Agents Chemo-ther 1992;36:121–125
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 641
6. Hamilton-Miller JM, Purves D. Enterococci and antifolateantibiotics. Eur J Clin Microbiol 1986;5:391–394
7. LeClercq R, Couvalin P. Bacterial resistance to macrolide,lincosamide and streptogramin antibiotics by target mod-ification. Antimicrob Agents Chemother 1991;35:1267–1272
8. Lefort A, Mainardi JL, Tod M, Lotholary O. Antienter-ococcal antibiotics. Med Clin North Am 2000;84:1471–1495
9. Rybkine T, Mainardi JL, Sougakoff W, Collatz E,Gutmann L. Penicillin- binding protein 5 sequencealterations in clinical isolates of Enterococcus faecium withdifferent levels of beta-lactam resistance. J Infect Dis 1998;178:159–163
10. Grayson ML, Eliopoulos GM, Wennersten CB, et al.Increasing resistance to b-lactam antibiotics amongstclinical isolates of Enterococcus faecium: a 22-year review atone institution. Antimicrob Agents Chemother 1991;35:2180–2184
11. Horodniceanu T, Bougueleret L, El-Solh N, Bieth G,Delbos F. High level resistance to gentamicin in Streptococcusfaecalis subsp. zymogenes. Antimicrob Agents Chemother1979;16:686–689
12. Mederski-Samoraj BD, Murray BE. High level resistance togentamicin in clinical isolates of enterococci. J Infect Dis1983;147:751–757
13. Spiegel CA, Hucyke M. Endocarditis due to streptomycin-susceptible Enterococcus faecalis with high-level gentamicinresistance. Arch Intern Med 1989;149:1873–1875
14. Eliopoulos GM. Aminoglycoside resistant enterococcalendocarditis. Infect Dis Clin North Am 1993;7:117–133
15. Leclercq R, Dutka-Malen S, Brisson-Noel A, et al.Resistance of enterococci to aminoglycosides and glycopep-tides. Clin Infect Dis 1992;15:495–501
16. Leclercq R, Derlot E, Duval J, Courvalin P. Plasmidmediated resistance to vancomycin and teicoplanin inEnterococcus faecium. N Engl J Med 1988;319:157–161
17. Centers for Disease Control and Prevention. Nosocomialenterococci resistant to vancomycin—United States 1989–1993. MMWR Morb Mortal Wkly Rep. 1993;42:597–599
18. Biedenbach DJ, Moet GJ, Jones RN. Occurrence andantimicrobial resistance pattern comparisons among blood-stream infection isolates from the SENTRY AntimicrobialSurveillance Program (1997–2002). Diagn Microbiol InfectDis 2004;50:59–69
19. Lai KK, Fontecchio SA, Kelly AL, Baker S, Melvin ZS.The changing epidemiology of vancomycin-resistant enter-ococci. Infect Control Hosp Epidemiol 2003;24:264–268
20. Courvalin P. Vancomycin resistance in gram-positive cocci.Clin Infect Dis 2006;42:S25–S34
21. Handwerger S, Skoble J. Identification of chromosomalmobile element conferring high-level vancomycin resistancein Enterococcus faecium. Antimicrob Agents Chemother1995;39:2446–2453
22. Gold HS. Vancomycin resistant enterococci: mechanismsand clinical observations. Clin Infect Dis 2001;33:210–219
23. Noble WC, Virani Z, Cree RG. Co-transfer of vancomycinand other resistance genes from Enterococcus faecalis NCTC12201 to Staphylococcus aureus. FEMS Microbiol Lett 1992;72:195–198
24. Chang S, Sievert DM, Hageman JC, et al. Infection withvancomycin- resistant Staphylococcus aureus containing thevanA resistance gene. N Engl J Med 2003;348:1342–1347
25. Centers for Disease Control and Prevention (CDC).Vancomycin-resistant Staphylococcus aureus—New York.MMWR Morb Mortal Wkly Rep 2005;53:322–323
26. Miller D, Urdaneta V, Weltman A. Vancomycin-resistantStaphylococcusaureus—Pennsylvania 2002. MMWR MorbMortal Wkly Rep 2002;51:902
27. Sievert DM, Boulton ML, Stolzman G, et al. Staphylococcusaureus resistant to vancomycin—United States 2002.MMWR Morb Mortal Wkly Rep 2002;51:565–567
28. Whitener CJ, Park SY, Browne FA, et al. Vancomycin-resistant Staphylococcus aureus in the absence of vancomycinexposure. Clin Infect Dis 2004;38:1049–1055
29. Donskey CJ. The role of the intestinal tract as a reservoirand source for transmission of nosocomial pathogens. ClinInfect Dis 2004;39:219–226
30. Beezhold DW, Slaughter S, Hayden MK, et al. Skincolonization with vancomycin-resistant enterococci amonghospitalized patients with bacteremia. Clin Infect Dis 1997;24:704–706
31. D’Agata EM, Gautam S, Green WK, Tang YW. High rateof false- negative results of the rectal swab culture methodin detection of gastrointestinal colonization with vanco-mycin-resistant enterococci. Clin Infect Dis 2002;34:167–172
32. Weinstein JW, Tallapragada S, Farrel P, Dembry LM.Comparison of rectal and peri-rectal swabs for detection ofcolonization with vancomycin-resistant enterococci. J ClinMicrobiol 1996;34:210–212
33. Montecalvo MA, Lencastre H, Carraher M, et al. Naturalhistory of colonization with vancomycin-resistant Enter-ococcus faecium. Infect Control Hosp Epidemiol 1995;16:680–685
34. Baden LR, Thiemke W, Skolnik A, et al. Prolongedcolonization with vancomycin-resistant Enterococcus faeciumin long-term care patients and the significance of ‘‘clear-ance.’’ Clin Infect Dis 2001;33:1654–1660
35. Roghmann MC, Aquiyumi S, Schwalbe R, Morris JG Jr.Natural history of colonization with vancomycin-resistantEnterococcus faecium. Infect Control Hosp Epidemiol 1997;18:679–680
36. Tornieporth NG, Roberts RB, Hafner JJ, Riley LW. Riskfactors associated with vancomycin-resistant Enterococcusfaecium infection or colonization in 145 matched case andcontrol patients. Clin Infect Dis 1996;23:767–772
37. Bonten MJ, Hayden MK, Nathan C, et al. Epidemiology ofcolonization of patients and environment with vancomycin-resistant enterococci. Lancet 1996;348:1615–1619
38. Morris JG, Shay DK, Hebden JN, et al. Enterococciresistant to multiple antimicrobial agents including vanco-mycin, establishment of endemicity in a university medicalcenter. Ann Intern Med 1995;123:250–259
39. Warren DK, Kollef MH, Seiler SM, Fridkin SK, Fraser VJ.The epidemiology of vancomycin-resistant Enterococcus in amedical intensive care unit. Infect Control Hosp Epidemiol2003;24:257–263
40. Donskey CJ, Chowdhry T, Hecker M, et al. Effect ofantibiotic therapy on the density of vancomycin-resistantenterococci in the stool of colonized patients. N Engl J Med2000;343:1925–1932
41. Bonten MJ, Slaughter S, Ambergen AW, et al. The role of‘‘colonization pressure’’ in the spread of vancomycin-resistant enterococci: an important infection control varia-ble. Arch Intern Med 1998;158:1127–1132
642 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007

42. Linden P. Can enterococcal infections initiate sepsissyndrome? Curr Infect Dis Rep 2003;5:372–378
43. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequateantimicrobial treatment of infections: a risk factor forhospital mortality among critically ill patients. Chest 1999;115:462–472
44. Kumar A, Robert D, Wood KE, et al. Duration ofhypotension before initiation of effective antimicrobialtherapy is the critical determinant of survival in humanseptic shock. Crit Care Med 2006;34:1589–1596
45. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH.The influence of inadequate antimicrobial treatment ofbloodstream infections on patient outcomes in the ICUsetting. Chest 2000;118:146–155
46. Quale J, Landman D, Atwood E, et al. Experience with ahospital-wide outbreak of vancomycin-resistant enterococci.Am J Infect Control 1996;24:372–379
47. Lai KK. Treatment of vancomycin resistant Enterococcusfaecium infections. Arch Intern Med 1996;156:2579–2584
48. Pankey GA, Sabath LD. Clinical relevance of bacteriostaticversus bactericidal mechanisms of action in the treatment ofgram-positive bacterial infections. Clin Infect Dis2004;38:864–870
49. Finberg RW, Moellering RC, Tally FP, et al. Theimportance of bactericidal drugs, future directions ininfectious diseases. Clin Infect Dis 2004;39:1314–1320
50. Tsigrelis C, Singh KV, Coutinho TD, Murray BE, BaddourLM. Vancomycin-resistant Enterococcus faecalis endocarditis:linezolid failure and strain characterization of virulencefactors. J Clin Microbiol 2007;45:631–635
51. Mekonen ET, Noskin GA, Hacek DM, Peterson LR.Successful treatment of persistent bacteremia due to vanco-mycin resistant ampicillin resistant Enterococcus faecium.Microb Drug Resist 1995;1:249–253
52. Dodge RA, Daly JS, Davaro R, Glew RH. High-doseampicillin plus streptomycin for treatment of a patient withsevere infection due to multi-drug resistant enterococci.Clin Infect Dis 1997;25:1269–1270
53. Murray BE. Vancomycin-resistant enterococcal infections.N Engl J Med 2000;342:710–721
54. Lautenbach E, Schuster MG, Biler WB, et al. The role ofchloramphenicol in the treatment of bloodstream infectiondue to vancomycin-resistant Enterococcus. Clin Infect Dis1998;27:1259–1265
55. Gould CV, Fishman NO, Nakamkin NI, Lautenbach E.Chloramphenicol resistance in vancomycin resistant enter-ococcal bacteremia: impact of prior fluoroquinolone use.Infect Control Hosp Epidemiol 2004;25:138–145
56. Howe RA, Robson M, Oakhill A, et al. Successful use oftetracycline as therapy of an immunocompromised patientwith septicemia caused by a vancomycin-resistant Enterococcus.J Antimicrob Chemother 1997;40:144–145
57. Linden PK, Pasculle AW, Manez R, et al. Utilization ofnovobiocin and ciprofloxacin for the treatment of seriousinfection due to vancomycin-resistant Enterococcus faecium.In: Program and Abstracts of the Thirty-Third InterscienceConference on Antimicrobial Agents and Chemotherapy,New Orleans, LA. Abstract 1027. Washington, DC:American Society for Microbiology; 1993:307
58. Montecalvo MA, Horowitz H, Wormser GP, et al. Effectof novobiocin containing antimicrobial regimens on infec-tion and colonization with vancomycin resistant Enterococcusfaecium. Antimicrob Agents Chemother 1995;39:794
59. Taylor SE, Paterson DL, Yu VL. Treatment options forchronic prostatitis due to vancomycin-resistant Enterococcusfaecium. Eur J Clin Microbiol Infect Dis 1998;17:798–800
60. Schmit JL. Efficacy of teicoplanin for enterococcal infec-tions: 63 cases and review. Clin Infect Dis 1992;15:302–306
61. Aslangul E, Baptista M, Fantin B, et al. Selection ofglycopeptide-resistant mutants of VanB type Enterococcusfaecalis BM4281 in vitro and in experimental endocarditis.J Infect Dis 1997;175:598–605
62. Hayden MK, Trenholme GM, Schultz JE, et al. In vivodevelopment of teicoplanin resistance in a VanB Enterococcusfaecalis. J Infect Dis 1993;167:1224–1227
63. Zhanel GG, Hoban DJ, Karlowsky JA. Nitrofurantoin isactive against vancomycin-resistant enterococci. AntimicrobAgents Chemother 2001;45:324–326
64. Linden P, Coley K, Kusne S. Bacteriologic efficacy ofnitrofurantoin for the treatment of urinary tract infectiondue to vancomycin-resistant Enterococcus faecium. Clin InfectDis 1999;29:999
65. Cocito C, DiGiambattista M, Nyssen E, Vannuffel P.Inhibition of protein synthesis by streptogramins and relatedantibiotics. J Antimicrob Chemother 2007;39(Suppl A):7–13
66. Hershberger E, Donabedian S, Konstantinou K, Zervos MJ.Quinupristin-dalfopristin resistance in gram-positive bac-teria: mechanism of resistance and epidemiology. Clin InfectDis 2004;38:92–98
67. Moellering RC, Linden PK, Reinhardt J, et al. The efficacyand safety of quinupristin/dalfopristin for the treatment ofvancomycin-resistant Enterococcus faecium. J AntimicrobChemother 1999;44:251–271
68. Linden PK, Moellering RC, Wood CA, et al. Treatment ofvancomycin-resistant Enterococcus faecium infections withquinupristin/dalfopristin. Clin Infect Dis 2001;33:1816–1823
69. Brown J, Freeman BB. Combining quinupristin/dalfopristinwith other agents for resistant infections. Ann Pharmac-other 2004;38:677–685
70. Bethea JA, Walko CM, Targos PA. Treatment of vancomy-cin-resistant Enterococcus with quinupristin/dalfopristin andhigh dose-ampicillin. Ann Pharmacother 2004;38:989–91
71. Thompson RL, Lavin B, Talbot GH. Endocarditis due tovancomycin-resistant Enterococcus faecium in an immuno-compromised patient: cure by administering combinationtherapy with quinupristin/dalfopristin and high-dose ampi-cillin. South Med J 2003;96:818–820
72. Raad I, Hachem R, Hanna H, et al. Treatment ofvancomycin-resistant enterococcal infections in the immu-nocompromised host: quinupristin-dalfopristin in combina-tion with minocycline. Antimicrob Agents Chemother2001;45:3202–3204
73. Olsen KM, Rebuck JA, Rupp ME. Arthralgias and myalgiasrelated to quinupristin-dalfopristin administration. ClinInfect Dis 2001;32:e83–e86
74. Werner G, Klare I, Spencker FB, Witte W. Intra-hospitaldissemination of quinupristin-dalfopristin- and vancomy-cin-resistant Enterococcus faecium in a paediatric ward of aGerman hospital. J Antimicrob Chemother 2003;52:113–115
75. Donabedian SM, Perri MB, Vager D, et al. Quinupristin-dalfopristin resistance in Enterococcus faecium isolates fromhumans, farm animals, and grocery store meat in the UnitedStates. J Clin Microbiol 2006;44:3361–3365
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 643
76. Moellering RC. Linezolid: the first oxazolidinone anti-microbial. Ann Intern Med 2003;138:135–142
77. Pharmacia and Upjohn. Linezolid for the Treatment ofVancomycin Resistant Enterococcal Infections: A Double-Blind Trial Comparing 600 mg Linezolid Every 12 Hourswith 200 mg Linezolid Every 12 Hours (study report M/1260/0054A). Peapack, NJ: Pharmacia Upjohn; 1999
78. Birmingham MC, Raynes CR, Meagher AK, Flavin SM,Batts DH, Schentag JJ. Linezolid for the treatment ofmultidrug-resistant gram-positive infections: experiencefrom a compassionate use program. Clin Infect Dis 2003;36:159–168
79. Stevens MP, Edmond MB. Endocarditis due to vancomy-cin-resistant enterococci: case report and review of theliterature. Clin Infect Dis 2005;41:1134–1142
80. Archuleta S, Murphy B, Keller MJ. Successful treatment ofvancomycin-resistant Enterococcus faecium endocarditis withlinezolid in a renal transplant recipient with human immuno-deficiency virus infection. Transpl Infect Dis 2004;6:117–119
81. Babcock HM, Ritchie DJ, Christiansen E, Starlin R, LittleR, Stanley S. Successful treatment of vancomycin-resistantEnterococcus endocarditis with oral linezolid. Clin Infect Dis2001;32:1373–1375
82. Zimmer SM, Caliendo AM, Thigpen MC, Somani J.Failure of linezolid treatment for enterococcal endocarditis.Clin Infect Dis 2003;37:e29–e30
83. Tsigrelis C, Singh KV, Coutinho TD, Murray BE, BaddourLM. Vancomycin-resistant Enterococcus faecalis endocarditis:linezolid failure and strain characterization of virulencefactors. J Clin Microbiol 2007;45:631–635
84. Gonzales RD, Schreckenberger PC, Graham MB, et al.Infections due to vancomycin-resistant Enterococcus faeciumresistant to linezolid. Lancet 2001;357:1179
85. Seedat J, Zick G, Klare I, et al. Rapid emergence ofresistance to linezolid during linezolid therapy of anEnterococcus faecium infection. Antimicrob Agents Chemo-ther 2006;50:4217–4219
86. Marra AR, Major Y, Edmond MD. Central venous cathetercolonization by linezolid-resistant, vancomycin-susceptibleEnterococcus faecalis. J Clin Microbiol 2006;44:1915–1916
87. Rahim S, Pillai SK, Gold HS, Venkataraman L, Inglima K,Press RA. Linezolid-resistant, vancomycin-resistant Enter-ococcus faecium infection in patients without prior exposure tolinezolid. Clin Infect Dis 2003;36:E146–148
88. Swaney SM, Shinabarger DL, Schaadt RD, Bock JH,Slightom JL, Zurenko GE. Oxazolidinone resistance isassociated with a mutation in the peptidyl transferase regionof 23S rRNA [abstract C-104]. In: Program and Abstractsof the 38th Interscience Conference on AntimicrobialAgents and Chemotherapy; San Diego. Washington, DC:American Society for Microbiology; 1998:98–99
89. Herrero IA, Issa NC, Patel R. Nosocomial spread oflinezolid-resistant vancomycin-resistant Enterococcus faecium.N Engl J Med 2002;346:867–869
90. Marshall SH, Donskey CJ, Hutton-Thomas R, Salata RA,Rice LB. Gene dosage and linezolid resistance in Enter-ococcus faecium and Enterococcus faecalis. Antimicrob AgentsChemother 2002;46:3334–3336
91. Pai MP, Rodvold KA, Schreckenbefger PC, Gonezales RD,Petrolatti JM, Quinn JP. Risk factors associated with thedevelopment of infection with linezolid- and vancomycin-resistant Enterococcus faecium. Clin Infect Dis 2002;35:1269–1272
92. Green SL, Maddox JC, Huttenbach ED. Linezolid andreversible myelosuppression. JAMA 2001;285:1291
93. Halpern M. Linezolid-induced pancytopenia. Clin InfectDis 2002;35:347–348
94. Wigen CL, Goetz MB. Serotonin syndrome and linezolid.Clin Infect Dis 2002;34:1651–1652
95. Saijo T, Hayashi K, Yamada H, Wakakura M. Linezolid-induced optic neuropathy. Am J Ophthalmol 2005;139:1114–1116
96. Bressler AM, Zimmer SM, Gilmore JL, Somani J. Peripheralneuropathy associated with prolonged use of linezolid. LancetInfect Dis 2004;4:528–531
97. Apodaca AA, Rakita RM. Linezolid-induced lactic acidosis.N Engl J Med 2003;348:86–87
98. Carpenter CF, Chambers HF. Daptomycin: another novelagent for treating infections due to drug-resistant gram-positive pathogens. Clin Infect Dis 2004;38:994–1000
99. Pfaller MA, Sader HS, Jones RN. Evaluation of the in vitroactivity of daptomycin against 19615 clinical isolates ofgram positive cocci collected in North American hospitals(2002–2005). Diagn Microbiol Infect Dis 2007;57:459–465
100. Jorgensen JH, Crawford SA, Kelly CC, Patterson JE.In vitro activity of daptomycin against vancomycin-resistantenterococci of various Van types and comparison ofsusceptibility testing methods. Antimicrob Agents Chemo-ther 2003;47:3760–3763
101. Anastasiou DM, Thorne GM, Luperchio SA, Alder JD.In vitro activity of daptomycin against clinical isolates withreduced susceptibility to linezolid and quinupristin/dalfo-pristin. Int J Antimicrob Agents 2006;28:385–388
102. Poutsiaka DD, Skiffingeron S, Miller KB, Hadley S,Snydman DR. Daptomycin in the treatment of vancomy-cin-resistant Enterococcus faecium bacteremia in neutropenicpatients. J Infect 2007;54:567–571
103. Segreti JA, Crank CW, Finney MS. Daptomycin for thetreatment of gram-positive bacteremia and infective endo-carditis: a retrospective case series of 31 patients. Pharma-cotherapy 2006;26:347–352
104. Long JK, Choueiri TK, Hall GS, Avery RK, Sekeres MA.Daptomycin-resistant Enterococcus faecium in a patient withacute myeloid leukemia. Mayop Clin Proc 2005;80:1215–1216
105. Munoz-Price LS, Lolans K, Quinn JP. Emergence ofresistance to daptomycin during treatment of vancomycin-resistant Enterococcus faecalis infection. Clin Infect Dis 2005;41:565–566
106. Lewis JS II, Owens A, Cadena J, et al. Emergence ofdaptomycin resistance in Enterococcus faecium during dapto-mycin therapy. Antimicrob Agents Chemother 2005;49:1664–1665
107. Green MR, Anasetti C, Sandin RL, Rolfe NE, Greene JN.Development of daptomycin resistance in a bone marrowtransplant patient with vancomycin-resistant Enterococcusdurans. J Oncol Pharm Pract 2006;12:179–181
108. Stein GE, Craig WA. Tigecycline: a critical analysis. ClinInfect Dis 2006;43:518–524
109. Sader HS, Jones RN, Stilwell MG, Dowzicky MJ, FritscheTR. Tigecycline activity tested against 26,474 bloodstreaminfection isolates: a collection from 6 continents. DiagnMicrobiol Infect Dis 2005;52:181–186
110. Streit JM, Sader HS, Fritsche TR, Jones RN. Dalbabancinactivity against selected populations of antimicrobial resistant
644 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 28, NUMBER 6 2007

gram-positive pathogens. Diagn Microbiol Infect Dis2005;53:307–310
111. Barrett JF. Recent developments in glycopeptide antibacte-rials. Curr Opin Investig Drugs 2005;6:781–790
112. Baltch AL, Smith RP, Ritz WJ, Bopp LH. Comparison ofinhibitory and bactericidal activities and postantibioticeffects of LY-333328 and ampicillin used singly and incombination against Enterococcus faecium. Antimicrob AgentsChemother 1998;42:2564–2568
113. Stryjewski ME, Chu VH, O’Riordan WD, et al. Telavancinversus standard therapy for treatment of complicated skinand skin structure infections caused by gram-positivebacteria: FAST 2 Study. Antimicrob Agents Chemother2006;50:862–867
114. Poulakou G, Giamarellou H. Investigational treatments forpostoperative surgical site infections. Expert Opin InvestigDrugs 2007;16:137–155
OPTIMIZING THERAPY FOR VANCOMYCIN-RESISTANT ENTEROCOCCI (VRE)/LINDEN 645