Embed Size (px)
DESCRIPTION
Oral Health Needs Assessment proofs 06083
Citation preview

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Introduction
The purpose of needs assessment in health care isto assess unmet health and health care needs in asystematic manner and to gather the informationrequired to bring about change beneficial to thehealth of the population. Health needs assessmentis a systematic approach attempting to ensure thatthe health service uses its resources to improve thehealth of the population in the most efficient way.The concept of need is at the core of health careplanning (Box 4-1). Planning health services is, inturn, rooted in the ethical imperative to use
resources appropriately. Needs assessmentinvolves setting priorities on the basis of healthneeds: that is taking into account the severity ofillness, and/or health care needs, which refers pri-marily to the capacity to benefit (Stevens andRaftery, 1994a; 1994b). A common assumption inthe organisation and provision of health services,including dental health services, which is beingchallenged, is that the need for health care can beobjectively determined by professionals. Now it isknown that health care needs may be defined inother ways, because the definition of any givenstate of ill-health has become open to much wider
Chapter 4
Chapter overviewThe purpose of oral health needs assessment within health service planning is defined. The twomain theoretical approaches for defining health needs assessment, namely the ‘humanitarian’ andthe ‘realistic’, and the different types of need are presented. The shortcomings of normative needand the elements of a more comprehensive measure of oral health needs are highlighted. Conceptsof impairment, functional limitation, disability and handicap are defined. Oral health-related qual-ity of life indicators are discussed and how closely they relate to clinical measures of oral health. Anew system termed the socio-dental approach to assessing dental needs is outlined.
Key wordsNeed for care, need for health, normative need, perceived (felt) need, expressed need (demand),social impact, impairment, functional limitation, disability, handicap, oral health-related quality oflife (OHRQoL) indicators, socio-dental approach
1
Aubrey Sheiham and Georgios Tsakos
Oral Health Needs Assessments
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
interpretation than in the past. Health care needsnow extend beyond a narrow clinical interpreta-tion to issues like:• the impact of ill-health on individuals and on
society• the degree of disability and dysfunction that
ill-health brings• the perceptions and attitudes of patients
themselves towards ill-health • the social origins of many common illnesses.
These factors inf luence the utilisation of healthservices and, ultimately, the effectiveness of treat-ment. In this sense, they represent key concepts
that should be seriously considered in the processof planning health care services.
This chapter will initially focus on the differentapproaches for the definition of need. Then it willmove on to present the shortcomings of the nor-mative need, which is the most commonly usedtype of need, before highlighting the necessaryelements of a measure of health needs assessment.This will be followed by a review of the develop-ment of oral health-related quality of life measures,their applications and important characteristics, aswell as on the studies examining their relationshipwith clinical status outcomes. Finally, a new socio-dental model for assessing dental treatment needswill be presented; firstly, its main components willbe introduced and then their incorporation into acomprehensive system will be highlighted.
Definitions of Need
Old concepts of need were based on a simple butunrealistic approach that unfortunately still dom-inates the service-related approach. That approachputs the main responsibility on the medical/den-tal professional to evaluate whether there is needfor treatment. This is epitomized by a definitionof need by Cooper (1975): ‘a state of health assessedas in need of treatment by a medical practitioner.’There are two distinct theoretical approaches to theassessment of needs for health care:a) the ‘humanitarian’ approach, which
focuses more on the burden of disease;b) the ‘realistic’ approach, which encompass-
es the concept of ‘ability to benefit’ and focus-es on health gain (Acheson, 1978; Stevens andGabbay, 1991; Wright, 1998) (Box 4-2).
The ‘humanitarian’ approach considers need as astate of the client that creates a requirement for careand therefore represents a potential for service(Donabedian, 1973). The key word inDonabedian’s definition is potential. Need does
Aubrey Sheiham and Georgios Tsakos
2
Health care needs assessment provides the opportu-nity for:
■ inf luencing policy;■ assessing the burden of illness and need, that is
describing the size of the problem and patterns ofneed in the local population and the differencesfrom district, regional, or national disease patterns;
■ understanding the needs and priorities of patientsand the local population;
■ highlighting the areas of unmet needs and provid-ing a clear set of objectives to work towards meet-ing these needs;
■ determining goals, objectives and priorities ;■ definition of feasible treatment aims for the serv-
ice;■ quantitative calculation of the total dental treat-
ment needs for the population; ■ deciding rationally how to use resources to
improve their local population's health in the mosteffective and efficient way;
■ interdisciplinary collaboration, or research anddevelopment priorities.
■ providing a method of monitoring and promot-ing equity in the provision and use of health serv-ices and addressing inequalities in health.
(Modified from Wright, 1998)
Box 4-1

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
not always lead to use of services and use of serv-ices does not always result from need, but the exis-tence of disease and normatively defined need doescreate a potential for the use of services (Spencer,1984). The ‘realistic’ approach is based uponMatthew’s (1971) service-related definition thatenriched the humanitarian approach with the con-cept of effectiveness of care and claimed that: ‘aneed for medical care exists when an individual hasan illness or disability for which there is an effec-tive and acceptable treatment or cure.’
The concern with effectiveness and acceptabil-ity is central to any formulation of health careneeds. Matthew’s definition focuses on the ‘needfor care’, which should be distinct from ‘need forhealth’. Health needs represent the distribution ofparticular forms of morbidity, as well as the distri-bution of those environmental, social and eco-nomic variables that inf luence health and illness.Therefore it is important to distinguish betweenthe need for health and the need for health care.Health care is one way of dealing with the need forhealth. The need for health is perceived as relieffrom distress, discomfort, disability, handicap andthe risk of mortality and morbidity (Acheson,1978). With the growing demand for treatmentsbased on evidence-based medicine, Matthew’sdefinition has become widely accepted. Bradshaw(1972) constructed a paradigm of need that incor-porates those concepts and forms a sociologicalbackground that sets up a useful definitional
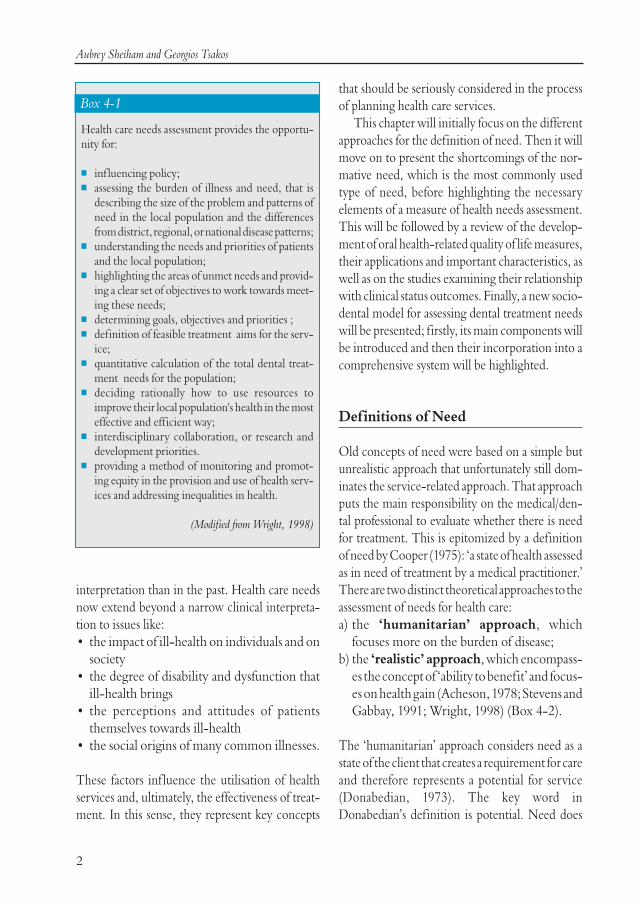
framework. The main types of need are presentedin Box 4-3 and their interrelation is illustrated inFig 4-1.
Shortcomings of Normative Need
The most commonly used type of need assessmentin oral health care planning is normative or pro-fessionally defined need. Most national and localoral health surveys adopt this approach (WHO,1997). Normative need identifies diseases andimpairments without considering the subjectiveperception of the subject. Estimates of dental needsare expressed in terms of numbers of people, num-bers of procedures, hours of work, division oflabour or costs. Despite its usefulness and exten-sive use, normative need is not free from limita-tions.
3
‘Need in health care is commonly defined as thecapacity to benefit. If health needs are to be identi-fied, then there should be an effective interventionavailable to meet these needs and improve health.There will be no benefit from an intervention that isnot effective or for which there are no resources avail-able.’
(Wright, 1998)
Box 4-2
Bradshaw’s taxonomy of Need: Types and definitions
Normative need: Is that which the expert or professional, administrator or social scientist defines as need in any given situation
Perceived (felt) need: This ref lects the individual's own assessment of his or her requirement for health care
Expressed need (demand): This is felt need converted into action by seeking assistance
Box 4-3
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
The shortcomings of the normative method ofassessing need are:1) Lack of objectivity and reliability. Nor-
matively defined need is not as preciselyquantifiable as the term suggests. It may beexpressed in terms of items of dental serviceor resource supply equivalents, such as workvalue units or cost (Spencer, 1980). Resourcesupply equivalents are usually specific to var-ious levels of dental technology, use of aux-iliaries, practice organisation and administra-tion; as such they may hold little validity fromone area to another (Spencer, 1984). Apartfrom the aforementioned variation betweenareas, the critique extends even to assess-ments in the same area. Professional judge-ments in normative need are neither value-free nor objective. Indeed, the lack of objec-tivity of normative treatment decisions hasbeen extensively demonstrated (Eldertonand Nuttall, 1983; Elderton, 1990; Gjermo,1991). The so-called objective assessmentoften depends upon a consensus agreementfrom a number of subjective approaches.
Even within those agreements, there is intra-examiner and inter-examiner variabilityamong different judgements. The significantvariations in dentists’ decisions on diagnosis,prognosis and treatment plan have beenrecently confirmed by systematic reviews(NHS Centre for Reviews and Dissemin-ation, 1999). Therefore, objectivity cannotbe regarded as a property of measures of nor-matively assessed health status and needs.
2) Neglect of psychosocial aspects andquality of life concepts. The global defini-tion of health (WHO, 1948) adopts a muchwider perspective than that of normativeneed and incorporates the concepts of func-tional, psychological and social well-being.Nevertheless, the standard norm of measuresof disease accepted by dentists is not alwaysthe norm in terms of functional or socialrequirements of people examined. Thisproblem occurs particularly in conditionswhich lack easy definition, such as occlusaldisharmonies (Sheiham et al, 1982). Oralhealth problems, but not necessarily the spe-cific pathological conditions, are related to aperson’s ability to carry out usual daily activ-ities and affect the individual's personal com-fort and quality of life. People’s dental satis-faction bears little relation to the clinicalassessment of oral conditions (Giddon et al,1976; Barenthin, 1977; Davis, 1980). Theassessment of health by lay persons differsfrom that of professionals. Furthermore,there are differences in concepts of health anddisease among lay people in different cul-tures. As a result, normative measures fail toassess the level of health-related quality of life(Leao and Sheiham, 1995; Locker andJokovic, 1996).
3) Lack of consideration for health behav-iours and patient compliance. Normativecriteria are insufficient for deciding treat-ment needs because they do not take into
4
Fig 4-1 The relationship between Normative Need,Perceived (Felt) Need, and Expressed Need (Demand).

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
account the attitudes and behaviours ofpatients, which in turn have considerableinf luence on the effectiveness of treatmentsand improvement of oral health. Patients’behaviours, such as diet, f luoride exposureand oral hygiene, are essential for the effec-tiveness of restorations and the progression ofdental caries (Kidd et al, 1992; Blinkhorn andDavies, 1996; Burt, 1998). Oral hygiene is thesingle most important factor for the successof periodontal treatment (Sheiham, 1997). Inorthodontics, lack of cooperation frompatients was the most common cause of fail-ures (Shaw et al, 1991). It seems, therefore,that the effectiveness or achievement oftreatments depends not only on professionalservices, but also on the individuals’ oralhealth behaviours (Maizels et al, 1993);neglecting to measure any of the aforemen-tioned factors indicates a limited and unsuc-cessful approach for the assessment of treat-ment needs.
4) Neglect of consumer rights. The need jus-tif ied by purely professional assessment isquestioned in terms of human or consumerrights. The clinical definition, based on thedisease analogy, rarely coincides with con-sumer definitions. Decisions of priority inhealth care must be discussed publicly andshould not be the sole prerogative of any sin-gle professional group or agency of govern-ment. In addition, recent developments inconsumerism and marketing have highlight-ed the importance of patient attitudes inhealth care decisions.
5) Unrealistic estimates for treatment plan-ning. Finally, normative need is criticized forits paradoxical approach. Although it recom-mends treatment, in the belief that all the sickshould be helped, it fails to consider the con-sequence of limited health care resources. AsAcheson (1978) emphasised: ‘If some of theneedy receive complete care, nothing may be
left for others. We cannot be endlessly gen-erous and continue to be fair.’ This is whyFuchs (1972) described normative need asromantic rather than humanitarian.
Despite the numerous and serious shortcomings,normative need assessment remains useful in manycases. Very few would argue, for example, that areliably diagnosed cavitation does not require fill-ing. But such consensus cannot be reached in thecase of need to replace missing teeth or extract thirdmolars. The inadequacy of normative need is alsoevident in the case of malocclusion, where tradi-tional indicators require supplementation by moresubjective lay assessments of need. Malocclusion isnot a disease and it would be incorrect to consid-er any deviation from an average as an abnormali-ty. The demarcation between acceptable and unac-ceptable occlusions is inf luenced by psychologicaland social factors, and methods of measuring sub-jective or perceived need.
The shortcomings of normative need in oralhealth care were cogently summarised by Locker(1989). He said that ‘from the point of view of con-temporary definitions of health, clinical measureshave serious limitations; they tell us nothing aboutthe functioning of either the oral cavity or the per-son as a whole and nothing about subjectively per-ceived symptoms such as pain and discomfort.’(Box 4-4)
Elements of a Measure of Oral Health Needs
Though dental ill-health affects populations inepidemic proportions and oral diseases are themost prevalent group of chronic disorders, neitherthe definition of dental health, nor current treat-ment need assessments correspond to or ref lect theorigins of dental disease. A measure for dental needshould incorporate not only clinical assessment,but also psychological and social dimensions
Oral Health Needs Assessment
5

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
because the presence of a clinical impairment aloneis neither necessary nor sufficient basis for need.The loss of molars, for example, is a clinical impair-ment. But this does not necessarily mean that thereis a need for dental treatment. A further questionshould be asked: is this impairment disabling?Furthermore, does it lead to handicap? More real-istic assessments of treatment need should includethe functional and the social dimensions of dentaldisease and an assessment of the social motivationalfactors which predispose people towards dental ill-health and inf luence the effectiveness of treatmentand health promotion. Consequently, a compre-hensive measure of dental needs should include thefollowing elements:• a clinical dimension based upon sound
concepts of the life history of the diseases• measures of social dysfunction• the perceived need of the individual• assessment of the propensity of the individ-
ual to take preventive action and the per-ceived barriers to prevention
• a prescription of effective and acceptabletreatments or cures
• assessment of the skills and manpowerrequired.
The clinical dimension refers to normative need,which has already been adequately described. Theother elements have not been traditionally the areaof focus and, consequently, they will be discussedfurther in this chapter. One of the main elementsof a measure of dental needs, namely measures ofsocial dysfunction, can be assessed by indicators oforal health-related quality of life.
Development of Oral Health-RelatedQuality of Life (OHRQoL) Indicators
The new concerns about the impact of the mouthon quality of life and the shortcomings of profes-sionally defined need for health care have led tothe development of broader measurements ofhealth need. The bio psychosocial model of healthproposes that diseases are inf luenced not only bythe underlying pathology, but also by the individ-ual’s perceptions, personality and stress (Engel,1977). Rising expectations have led to a shift awayfrom viewing health in terms of survival, througha phase of defining it in terms of freedom from dis-ease, thence to an emphasis on the individual’s abil-ity to perform daily activities, and now to the cur-rent emphasis on positive themes of happiness,social and emotional well being, and quality of life.
In this expanded theoretical framework, a vari-ety of new subjective indicators that attempt tomeasure the health-related quality of life have beendeveloped and used (Bowling, 1995, 1997; Carr etal, 2003). These indicators are multidisciplinarywith major contributions from psychology, soci-ology, economics, operational research and bio-statistics. They cover a wide non-clinical spec-trum, from condition-specific to general healthassessments, from individual-specific to popula-tion outcome measures, from health profiles tosingle score indices. Consequently, physiologicaloutcome measurements were substituted by healthstatus measurements, allowing insight intopatients’ experience, and ‘health-related quality oflife’ has evolved as an appropriate term to describethis domain of measurement (Guyatt et al, 1989;Testa and Nackley, 1994). This is a multifacetedconcept, attempting to simultaneously assess howlong and how well people live.
The development of oral health-related quali-ty of life indicators demonstrated many similaritieswith the respective trends in the medical field.While a great deal of effort has been devoted to theconstruction of valid and reliable indices of oral
6
Clinical indices are essential for measuring oral dis-ease, but the problem arises when these indices areused as measures of health and treatment need.
Sheiham et al, 1982
Box 4-4
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
disease, behavioural or subjective measures of oralhealth have been used less frequently. There hasgenerally been less development of alternative def-initions of need in dental than in general healthcare. Cohen and Jago (1976) were the first to arguethat clinical indicators of oral health would begreatly improved and be more relevant for policymaking by adding a dimension of social impact,thus defining a new type of oral health indicator(Box 4-5).
Following similar trends in the general healthfield, the term ‘oral health-related quality of lifemeasures’ has been adopted for these subjectivehealth status measures. They are subjective indica-tors that provide information on the impact of oraldisorders and conditions, and the perceived need fordental care. Their use should be complementary tothe clinical measures of oral status and needs(Cushing et al, 1986; Locker and Jokovic, 1996).
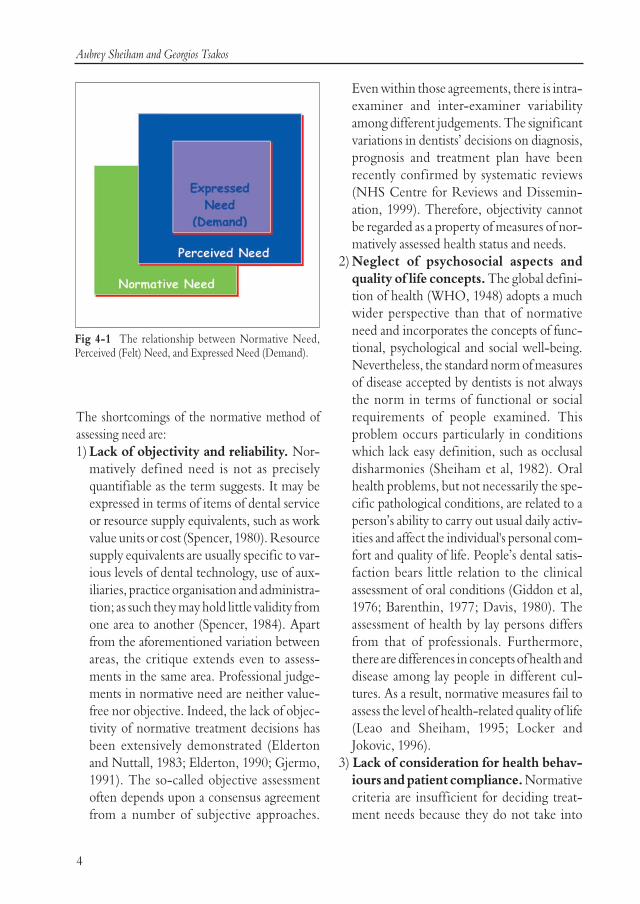
The concepts of impairment, functional limita-tion, disability, and handicap have become pivotalto the development of oral health-related quality oflife indicators. Locker (1988) suggested a coherenttheoretical framework, based on those concepts(Fig 4-2), which is an adaptation of the WHOmodel for the International Classif ication ofImpairments, Disabilities and Handicaps (1980).The main definitions of this conceptual model are:
• Impairment is a loss or abnormality of men-tal, physical, or biochemical function eitherpresent at birth or arising out of disease orinjury, such as edentulousness, loss of peri-odontal attachment or malocclusion. Allpathology is associated with impairment, butnot all impairments lead to functional limi-tations.
• Functional limitation is restriction infunction customarily expected of the body orits component organ or system, such as lim-itation of jaw mobility.
• Disability is any limitation in or lack of abil-ity to carry out socially defined tasks and rolesthat individuals generally are expected to beable to do (Pope and Tarlov, 1991).
7
Socio-dental indicators are:
“measures of the extent to which dental and oral dis-orders disrupt normal social role functioning andbring about major changes in behaviour such as aninability to work or attend school, or undertakeparental or household duties”.
Locker (1989)
Box 4-5
Disease Impairment Function al Limi tation Disabil ity Handicap
Death
Discomfort
Disease Impairment Function al Limi tation Disabil ity Handicap
Death
Discomfort
Fig 4-2 The conceptual model of consequences of oral impacts (modified from Locker, 1988).

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
• Handicap is concerned with the broadersocial effects and is defined as the disadvan-tage experienced by impaired and disabledpeople because they do not or cannot con-form to the expectations of society or thesocial groups to which they belong. It is thedisadvantage or restriction experienced byindividuals in their personal and social lifeconsequent upon disability or impairment. Inthis sense, a handicap results from interac-tions between physical impairment, theadjustment to it and the physical and socialenvironment (WHO, 1980). The disadvan-tage is multidimensional and can involve lossof opportunity, actual material and socialdeprivation and dissatisfaction (Locker, 1988;Pope and Tarlov, 1991).
The relationship between impairment, disability,and handicap is a dynamic continuum that isreversible. Impairment may or may not lead to dis-ability and handicap. For example, a malposed ormissing tooth (impairment) can, but does notinevitably, lead to a restriction in eating or to avoid-ance of hard foods (disability), which in turn canmake people feel embarrassed and avoid eating infront of others (handicap). Some impairments may– but not necessarily – give rise to different formsor severities of disability and some disabilities mayhave handicapping effects. Malocclusion, gingivi-tis or missing teeth are impairments but do notalways disable nor handicap individuals. However,an individual may be impaired and not disabled butnevertheless handicapped, because disability ismeasured by restriction of activities and functionwhereas handicap is socially defined. Although thisapproach presents operational difficulties (it is notpossible, for example, to predict that a given degreeof impairment will produce a similar degree of dis-ability or handicap), it nonetheless focuses atten-tion on the importance of the socio-psychologicalaspects of health needs assessment.
The development and testing of health-relatedquality of life outcome measures have become pri-ority research areas in social epidemiology (Bader,1992; Frazier, 1992), though this trend has pro-ceeded at a slower pace for measures of oral thangeneral health (Coulter et al, 1994). A variety oforal health-related quality of life indicators havebeen developed and used in oral health surveys(Slade, 1997). They have demonstrated some con-tent similarities, but are characterized by consid-erable variation in their precise aims, number ofitems and technical characteristics. They vary withrespect to the presence or absence of subscales, themethod of administration, the response choicesoffered, the incorporation or lack of weights, andthe provision or not of a final score. Most of theoral health-related quality of life indicatorshave been used in cross-sectional oral health sur-veys, while only a handful have been introducedto longitudinal or intervention studies, in order tomeasure change in quality of life (Locker, 1996,1998; Slade et al, 1998).
Measurement of oral health-related quality oflife has been characterized by complex conceptu-al issues. Like health-related quality of life, oralhealth-related quality of life is a multidimensionalconcept that incorporates relatively abstract andnot clearly demarcated domains such as: survival,illness and impairment, social, psychological andphysical function and disability, oral health per-ceptions, opportunity, as well as interactionsbetween the aforementioned domains (Gift andAtchison, 1995). Furthermore, the respectiveindicators are predominantly subjective and con-stantly evolving and inf luenced by the social, cul-tural, political and practical contexts, in which theyare measured (Locker, 1997).
8

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
Applications of Oral Health-RelatedQuality of Life Indicators
Apart from the conceptual background for thedevelopment of oral health-related quality of lifeindicators, the determination of the context oftheir potential applications remains a crucial issue,since it may affect the desirable characteristics ofan indicator. Ware et al (1981) identified five broadcategories of use of the major health status meas-urements:• measuring the efficiency or effectiveness of
health interventions• assessing the quality of life• estimating the health needs of a population• improving clinical decisions• understanding the causes and consequences
of differences in health.
The application of oral health-related quality of lifeindicators for each specific purpose may vary con-siderably. Thus, it is essential when selecting indi-cators to assess needs, to see which matches thepurpose and qualities of currently established indi-cators. Locker (1996) suggested three non-exclu-sive broad categories of applications for these meas-ures, namely political, theoretical and practical(Box 4-6).
The theoretical role relates to the facilitation ofthe investigation of important relationships (e.g.disease and illness) in the fields of medical sociol-ogy, health psychology and health servicesresearch. Practical applications are further cate-gorised into research (e.g. use in clinical trials orhealth policy studies), public health, which refersto populations (e.g. assessing oral health needs),and clinical practice, which concentrates on theindividual rather than the population level (e.g.monitoring the course of a patient’s illness).
Choosing an Oral Health-RelatedQuality of Life Indicator
Apart from identifying the possible applications ofan oral health-related quality of life indicator, con-siderable effort should be dedicated to making aninformed choice of instrument, thus evaluating itskey characteristics. There are five major factorsthat must be considered in choosing an instrumentfor measuring health status (Ware et al, 1981),namely:• practicality• reliability• validity• objectivity/subjectivity, and • whether global measures are preferable to
more specific ones.
Specifically in relation to the needs assessment ina population, at least three major qualificationsshould be considered as crucial for health plan-ning:• the index should be brief and easy to use in a
large population within a reasonable time• scaling according to units should be relevant
to decision-making criteria, and• the index should measure variables specified
by a system model to provide cause and effectrelationship information for policy makers.
9
■ Political Applications (allocation of health careresources)
■ Theoretical Applications
■ Practical Applications- Research- Public Health- Clinical Practice
Box 4-6

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
Existing subjective measures of oral health have notbeen shown to conform well to all of these crite-ria.
Relationship between Oral Health-Related
Quality of Life Indicators and Clinical Oral
Health Measures
Although relationships between clinical and socialvariables were weak, those that were significantcould be used as a stepping stone to start buildinga picture of characteristics, both clinical and social,of people who experience dental problems. Fromthe different clinical measures used in a studyexploring the relationship between the socialimpacts of dental disease and clinical status(Cushing et al, 1986), only the number of func-tioning teeth, that is the sum of sound teeth andfilled teeth (Sheiham et al, 1987), was significant-ly associated with the overall prevalence of oralimpacts. Other clinical measures were significant-ly associated with specific impact dimensions butnot with the overall prevalence. People whoreported having eating problems, for instance, hada higher DMFT and fewer functioning teeth thanthose with no problems. In a later study ofemployed adults (Rosenoer and Sheiham, 1995)that used the same indicator of the social impact ofdental diseases, oral impacts correlated positivelywith DMF-T and negatively with the number ofteeth, but the significant associations were weak.In addition, participants with five or more poste-rior occluding pairs of teeth (POPs) had signifi-cantly lower levels of impacts.
Atchison and Dolan (1990) compared theGeriatric Oral Health Assessment Index (GOHAI)scores with clinical variables in people aged 65 yearsand over. Those with 21 to 32 teeth and no remov-able denture had higher GOHAI score (that is lowerlevels of impacts) and did not perceive a need fordental treatment. Again, those significant correla-tions were relatively weak. The same pattern ofassociations was also observed by Locker (1992) ina study of adults aged 50 years or older. Clinical
variables were weakly, but significantly, correlat-ed with subjective measures except for pain symp-toms. The number of missing teeth and mean peri-odontal attachment loss were significant predic-tors of impact scale scores.
These f indings were reinforced by f indingsfrom a study (Locker and Slade, 1994) that used theOral Health Impact Profile (OHIP) indicator. Thenumber of missing teeth, number of functionalunits and number of posterior functional unitswere significantly correlated with all OHIP sub-scales and total scores, while significant correla-tions were also revealed for the number of decayedand filled teeth, DMF-S and loss of attachmentindices. Despite being the relatively strongest clin-ical predictor, the number of missing teeth couldonly explain 18% of the variation in OHIP scores.An additional 14% was accounted to the effects ofgeneral health status, life stress, dental insurancecoverage, household income and age.
Slade and Spencer (1994) used the OHIP inolder adults in South Australia and showed thatedentulous persons reported significantly moresocial impact in four sub-scales: functional limita-tion, physical disability, social disability and hand-icap. Among dentate persons, tooth loss was asso-ciated with all seven sub-scales of social impact.Anterior tooth loss was associated with moreimpact, whether or not there was replacement ofthe missing teeth by prosthetic units, while poste-rior tooth loss was associated with social impactonly when there were unfilled spaces. Similar find-ings were reported using the Dental Impacts onDaily Living (DIDL) index in a population aged35–44 years (Leao and Sheiham, 1995). The worsethe oral status, the worse the subjective impact.These findings suggest that despite their overallsignif icance, clinical variables, together withsocio-demographic determinants, could explainless than 30% of the variation in the total DIDLscore. Using the Oral Impacts on DailyPerformance (OIDP) indicator in an elderly pop-ulation, Srisilapanan and Sheiham (2001a) showed
10

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
significant associations between oral impacts and avariety of clinical measures. More specif ically,edentulous people experienced higher levels ofimpacts in comparison to the dentate. Within thedentate group, higher impact scores were observedin people with anterior tooth loss, posterior toothloss, mobile teeth and loss of attachment, but therelationship between OIDP and caries (both coro-nal and root) was not significant.
Overall, the associations between clinical statusindicators and measures of oral health-related qual-ity of life were weak. But the associations were bet-ter for specific clinical conditions such as missingteeth, particularly anterior teeth, and occludingpairs of natural teeth (Locker and Slade, 1994; Sladeand Spencer, 1994; Leao and Sheiham, 1995;Srisilapanan and Sheiham, 2001a). Different levelsof oral status have different impacts on people’s dailyliving. In some instances, the weak associationsbetween clinical and subjective oral health indica-tors are to be expected given the nature of the meas-ures employed; they exist because the clinical indi-cators are mediated by functional and experientialvariables, such as chewing capacity and pain, and bysocio-demographic factors (Locker, 1992). A morecomprehensive explanation relates to the concep-tual distinction between health and disease (Hunt etal, 1986; Locker, 1992; Bowling, 1997). Diseasedoes not always negatively affect subjective percep-tions of well-being, and even when it does, its impactis inf luenced by expectations, preferences, materi-al, social and psychological resources and, moreimportantly, socially and culturally derived values(Locker, 1992). Therefore clinical status and multi-ple social and psychological dimensions should beassessed simultaneously when assessing people’sdental needs.
A New Comprehensive System of Assessing Treatment Needs for Oral Health Care: the Socio-dental Approach
A new system for the assessment of dental treat-ment needs should overcome the deficiencies asso-ciated with the sole assessment of normative need,thus considering dental treatment need not onlyfrom professional judgement, but also incorporat-ing the related socio dental impact and behaviour-al factors such as people’s perception and propen-sity. The development of this new system conformsto the modern theoretical multifactorial approachfor the assessment of needs for oral health care andincorporates the following elements:1) clinical estimates of normative need2) general health status3) subjective perceptions, including perceived
treatment needs and oral health impacts inrelation to functional, psychological andsocial dimensions
4) propensity to adopt health promoting behav-iours
5) scientif ic evidence of the effectiveness oftreatments.
This new system, that is termed a socio-dentalapproach to assessing dental needs, aims torationalize the needs assessment process and, con-sequently be more useful for oral health care plan-ning.
The clinical component associated with nor-mative need has been extensively reviewed earlierin this chapter. The only modification at the nor-mative need level is that general health factorsshould be taken into account. Dental care will beplanned for people with normative need who alsoexperience general health problems affecting theprognosis of dental disease or the maintenance ofacceptable oral health after treatment (Srisilapananand Sheiham, 2001b). High priority groups fordental care are those in greatest need due to their
11

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
general health problems and to those where den-tal disease will affect the condition of a chronic dis-ease or their general health status. This integrationof general health factors with normative need mayfacilitate the prioritization of treatment needs, aswell as adopting a more selective approach. Theremainder of this section will concentrate onbrief ly reviewing the rationale for the inclusion ofthe other components of the socio-dentalapproach. Finally, the method of incorporatingthem all into a coherent system will be described.
Subjective Perceptions of Need
The role of subjective perceptions and perceivedneeds for dental care is an essential part in the con-cept of dental need. Perceived needs are frequent-ly inconsistent with normative needs. In additionto the well documented significant gaps betweenprofessional and lay perception of need, morerecent literature strongly emphasises the impor-tance of patients’ feelings and their relative prior-ity to professional assessments (Bowling 1997;Anderson, 1998). Bradshaw’s (1972) taxonomy ofneeds (Box 4-3) illustrates the difference betweenperceived and normative needs, and puts greatemphasis on perceived and expressed need. Suchdifferences imply that people measure differentconcepts of health to professionals. Subjectivemeasures seem to relate to human experiences andthe process of people’s perceptions involves inter-action between various factors in people’s life,namely, biological, psychological and socio-envi-ronmental factors. Subjective perceptions includethe assessment of: • perceived need for dental treatment• oral impacts and oral health-related quality of
life.
There is a strong association between perceivedimpacts, perceived oral health and needs (Atchisonand Dolan, 1990; Matthias et al, 1995; Locker and
Jokovic, 1996; Gift et al, 1998; Tsakos et al, 2001).Furthermore, people that perceive need for den-tal treatment are the most likely to benefit fromthe provision of treatment and may be consideredas a high priority group at a time of scarce resources(Locker and Jokovic, 1996). While the assessmentof dental treatment needs is carried out by askinga direct question, oral impacts are measuredthrough an oral health-related quality of life indi-cator. The Oral Impacts on Daily Performance(OIDP) is an indicator of oral health-related qual-ity of life that specifically allows for the assessmentof treatment needs (Aduyanon and Sheiham,1997). The theoretical framework on which theOIDP index is based is modified from the WHO'sInternational Classif ication of Impairments,Disabilities and Handicaps (1980). The main mod-ification is that different levels of the concepts areestablished (Fig 4-3), namely:• Level 1: oral status and oral impair-
ments, which most clinical indices attemptto measure.
• Level 2: ‘intermediate impacts’, whichrefer to the possible early negative impactscaused by oral health status – pain, discom-fort, functional limitation or dissatisfactionwith appearance. Any of these dimensionsmay lead to impacts on performance ability.
• Level 3: ‘ultimate impacts’, which ref lectsthe translation of the aforementioned dimen-sions into impacts on the ability to performdaily activities. This level covers the conceptsof disability and handicap.
The OIDP index focuses on the third level ofmeasurement, thus assessing impacts on the abili-ty to perform daily activities. It is a way to screenfor the significant impacts, by eliminating verysmall negative perceptions from oral conditionswhich do not lead to an impact on daily perform-ances. In addition, it is more accurate to measurethe behavioural impacts in terms of performancethan the feeling state dimension. More impor-
12

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
13
tantly, though, the screened outcomes should bemore useful in the context of policy planning. TheOIDP covers major oral impacts in relation to dailyactivities and behaviours (e.g. eating, speaking,sleeping, maintaining usual emotional state, meet-ing people) and provides a final score that incor-porates the measurements of both the frequencyand the severity of the effect those impacts had inthe daily life of the person in the last six months.Furthermore, through the additional calculation ofthe Condition-Specific OIDP, it allows for theimpacts to be attributed to specific oral conditions,thus making the index suitable for needs assessmentand treatment planning.
Propensity for Health PromotingBehaviours
Achieving and maintaining good oral health andsuccessful treatment outcomes depends on boththe professional intervention and the individualattitudes and behaviours. Indeed, people’s attitudesand behaviours have a strong inf luence on theeffectiveness of treatment and improvement of oralhealth (Maizels et al, 1993). The socio-dentalapproach in needs assessment focuses on achievingthe optimal benefits from available resources.Consequently, on a population level, differentstrategies may be planned for different groups inorder to gain the maximum benefit within avail-able resources. Accordingly, in addition to assess-ing the perceived need for treatment, factors that
predict whether a person will comply with treat-ment and with oral health instructions must beassessed. Within a certain level of need, people thatare more likely to benefit from treatments shouldbe given a higher priority in comparison to thoseless likely to benefit. Therefore, the system shouldbe f lexible enough to allow dental service plannersto prioritise needs and make rational decisions inresource allocation, and behavioural factors affect-ing health gain from dental therapies should alsobe included in needs estimations (Maizels et al,1993). These behavioural factors are the propensi-ty to carry out preventive behaviours and self careand compliance with treatment instructions.
Most definitions of need have emphasised the needfor treatment. Little attention has been given to theneeds for the promotion of health and the primaryprevention of disease. Since health/sickness andfunction/dysfunction can each be conceived asbeing on a single continuum parallel to one anoth-er, attention should be given to the needs of peo-ple at all points along the continuum and not justto those at the sickness and dysfunction ends.Despite the fact that dental diseases are virtuallyavoidable by preventive measures, little is knownabout the factors which underlie the propensity ofindividuals to undertake preventive care or theirresponse to health education. Thus, while preven-tive methods hold the greatest potential for drasti-cally reducing dental disease, knowledge is lackingof the very factors which are crucial to the successof any preventive programme.
Level 1 Oral impairments
Level 2 Pain Discomfort
Functional limitation Appearance dissatisfaction
Level 3 Physical Psychological Social
Impacts on daily performance
(Disability and Handicap)
Fig 4-3 Theoretical model forthe development of the OralImpact on Daily Performance(OIDP) index.

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
When clinicians assess the need for treatment theyestablish the clinical status, the medical history, theattitudes and past behaviours of the individual witha view to assessing the propensity of that person torespond to treatment. In periodontal treatment, inall instances, whatever the degree of periodontaldestruction, the effective control of reasonablyaccessible plaque by the patient is paramount.Success of both non surgical and surgical treat-ments has been shown to depend primarily uponthe maintenance of a high level of supragingivalplaque control by the patient. Prescribing a partialdenture or surgical periodontal treatment forsomeone with poor hygiene and dietary habitswould be considered bad treatment planning. Yetall the normative need assessments ignore meas-ures of propensity or compliance. In addition, sur-vey manuals, such as Oral Health Surveys: BasicMethods (WHO, 1997), which is widely used fordental public health planning, do not incorporatethe propensity to adopt health promoting behav-iours into the process of planning for treatmentneed.
The behavioural factors included in the newcomprehensive system for the assessment of den-tal treatment needs refer to the propensity to adopthealth promoting behaviours and cover four basicbehaviours with established importance for oralhealth care. They are:• use of f luoride toothpaste• frequency of tooth brushing• sugar intake• pattern of dental attendance.
All four factors inf luence oral health status andtreatment outcomes. The use of f luoride tooth-paste has been strongly associated with the declineof dental caries; in industrialised countries, in par-ticular, it has been considered as the single mostimportant factor (Petersson and Bratthall, 1996;Milgrom and Reisine, 2000). A recent systematicreview of the effectiveness of f luoride concludedthat the high quality trials provide clear evidence
that f luoride toothpastes are efficacious in pre-venting caries (Marinho et al, 2003). The impor-tance of tooth brushing, in terms of improving per-sonal oral hygiene, relates to the promotion of peri-odontal health and to the prevention of dentalcaries. Effective plaque control and maintenanceof sound oral hygiene affect the success of peri-odontal treatment (Sheiham, 1997; McDonaldand Avery, 2000). In addition, the frequency oftooth brushing played an important role in theeffectiveness of f luoride toothpaste (Sutcliffe,1996). Furthermore, Rodrigues and Sheiham(2000) showed that children brushing their teethless than once daily were more likely to have high-er caries increments.
The direct and strong association between sugarconsumption and dental caries has been clearly estab-lished (Arens, 1998; The British NutritionFoundation, 1998; Sheiham, 2001; Moynihan,2002; WHO, 2003). A recent systematic reviewconcluded that limiting sugar intake is an importantfactor for preventing dental caries (Burt and Pai,2001). Finally, the pattern of dental attendance is ameasure of compliance that is closely related to theperception of dental treatment needs (Tickle andWorthington, 1997) and plays an important role,particularly in treatments that require several dentalvisits (McDonald and Avery, 2000). The consider-ation of the aforementioned behavioural aspects inthe system of treatment needs assessment facilitatesthe completion of the system and makes it directlyrelevant for planning dental health services.
The Effectiveness of Treatment
Sackett and Snow (1979) caution that the strategiesapplied to change compliance behaviour must meetat least three preconditions: the diagnosis must becorrect; the therapy must do more good than harm;and the patient is an informed, willing partner inthe execution of all interventions. It follows logi-cally that clinical judgment includes the balancing
14

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
of probabilities for benefit and harm. The need forcare is widespread while cure is rare (Cochrane,1972)5. Accordingly, the point on the distributionat which therapy begins to do more good than harmshould be established. An important criterion ofneed is whether there is an effective treatment forthe condition. Matthew (1971) considers that aneed for treatment exists, only if there is an effec-tive and acceptable treatment. Epidemiological datafor the distribution of diseases in a population canonly be useful for planning services when there iseffective treatment or care available.
The treatment which is professionally judged tobe needed for a specific impairment should be eval-uated for its effectiveness. The need for healthtechnology assessment arises from the concern thathealth technology may neither be used wisely, norproduce the expected health benefit. Many stud-ies using the randomized controlled trial (RCT)have given ample warnings of how dangerous it isto assume that well established medical therapieswhich have not been tested are always effective(Cochrane, 1972). Few dental therapies have beensubjected to rigorous randomized controlled tri-als, and there are limited quantitative assessmentsof effectiveness. Where analyses have been done,using systematic reviews, most commonly per-formed treatments, such as removal of supragingi-val calculus and orthodontics were found to be rel-atively ineffective without unrealistic complianceregimens (Shaw et al, 1991; Antczak Bouckoms etal, 1993; Addy and Koltai, 1994). Furthermore,there was little evidence to support or refute thepractice of encouraging the 6-monthly dentalcheck-ups (Davenport et al, 2003).
Considerations of dental treatment effective-ness should be based on the investigation of avail-able therapy appraisal data, as well as the possibleresources and qualified personnel to perform suchtreatment effectively in each planning setting. Animportant future challenge is to help professionals
be more critical in their appraisal of new technol-ogy, so that a large proportion of the interventionsoffered to the population are those that have beenshown by the performance of good quality researchto be effective. If interventions are of unprovenefficacy or are doing more harm than good, deci-sion-makers must ensure that either they are notintroduced – ‘stop starting them’ – or, if they havealready been introduced, that they are no longerpracticed – ‘start stopping them’ (Muir Gray,1997). Health policy planners should not solelybase their decisions on effectiveness on textbooksor individual studies. Systematic reviews, likethose available from the Oral Health Group of theCochrane Collaboration, have appraised the pub-lished papers and reports and provide valuableinformation on the effectiveness of interventions.Up to now (September 2005), 51 systematicreviews present and evaluate the evidence on avariety of dental care interventions, thus formingthe backbone of an increasing library of evidenceappraisal in oral health. In the era of evidence-based health care, uncritical decisions are unac-ceptable.
Incorporating the Components into a Whole New System
Having described the different components of theneeds assessment system, the field is considerablybroadened and complicated and the crucial issueahead relates to their meaningful incorporationinto a coherent system. The theoretical frameworkof the system could be described as a gradual inte-grating process, whereby normative need assess-ments are incorporated with subjective percep-tions, as well as with information on the effective-ness of treatments (evidence-based dentistry) andpeople’s propensity for health promoting behav-iours. Evidence-based dentistry is a concept
15
5 Chapter 5: Reviewing Existing Data: Appraising the Evidence

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
underlying and covering all levels of the socio-den-tal system of treatment needs assessment. Plannersshould refer to published guidelines when decid-ing on appropriate treatments. Moreover, selec-tion of treatments depends on the local setting,available resources and extent of general needs inthe community.
This process allows for three levels of treatmentneeds measurement, each taking into accountgradually more key factors (Fig 4-4). The three lev-els are:• Normative Need• Impact-related Need• Propensity-related Need
The first level of measurement refers to NormativeTreatment Need. This is followed by the assessmentof Impact-related Need, through the incorporation ofsubjective assessments into the system. People thathave normative needs and oral impacts have‘Impact-related Needs’ and they can be further pri-oritized according to the third level of measure-ment. People with normative need but without oralimpacts are not following the treatment pathway;instead, they are considered as needing dentalhealth education, thus forming a population groupin need of oral health promotion with the aim tomodify their health behaviours. After that, theymay further follow the treatment pathway and fol-low the third level of measurement, that is thePropensity-related Need. At this third level, treatmentis prescribed in the light of probability of success,using the best available evidence on effectiveness of
treatments and the individual’s behaviouralpropensity. Propensity-related Need categorizesthe population into appropriate treatment groups,by considering the behavioural propensity of theperson. In this sense, people may be categorizedinto high, medium and low propensity-relatedneed groups, according to their behaviour in rela-tion to the use of f luoride toothpaste, frequency oftooth brushing, sugar intake and pattern of dentalattendance. Then, different options of effectivetreatment and care may be available for the differ-ent groups. Taken together with the availability ofresources, this concept of propensity would allowhealth authorities to estimate the amount of differ-ent types of care required for a defined population.
Having explained the basic concepts and meas-urement levels of this system of gradual integra-tion, discussion needs to be directed towards areasof potential confusion. Indeed, there are impor-tant issues to be considered when combining clin-ical with subjective measures. There are conditionswhere normative need is of prime importance:• life threatening conditions, such as oral
cancer or precancerous lesions, fractures ofjaw, and severe infections.
• chronic progressive oral conditions, suchas active dentinal caries.
In life-threatening or chronic progressive condi-tions, treatment or further investigation is essentialeven without the impact being assessed. Dentalneed is based on the best available evidence in rela-tion to the natural history of diseases. Con-
16
Dental Need Level Key Factors
Normative Need Clinical impairments
General health status
Impact-Related Need
Clinical impairment
General health status
Perceived oral health impacts and needs
Propensity-Related Need
Clinical impairment
General health status
Perceived oral health impacts and needs
Behavioural propensity for treatment
* Evidence-based treatment is a factor considered throughout the socio-dental system.
Fig 4-4 Levels of dental treat-ment needs and relevant keyfactors.* Evidence-based treatment is a factor considered throughout the socio-dental system
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
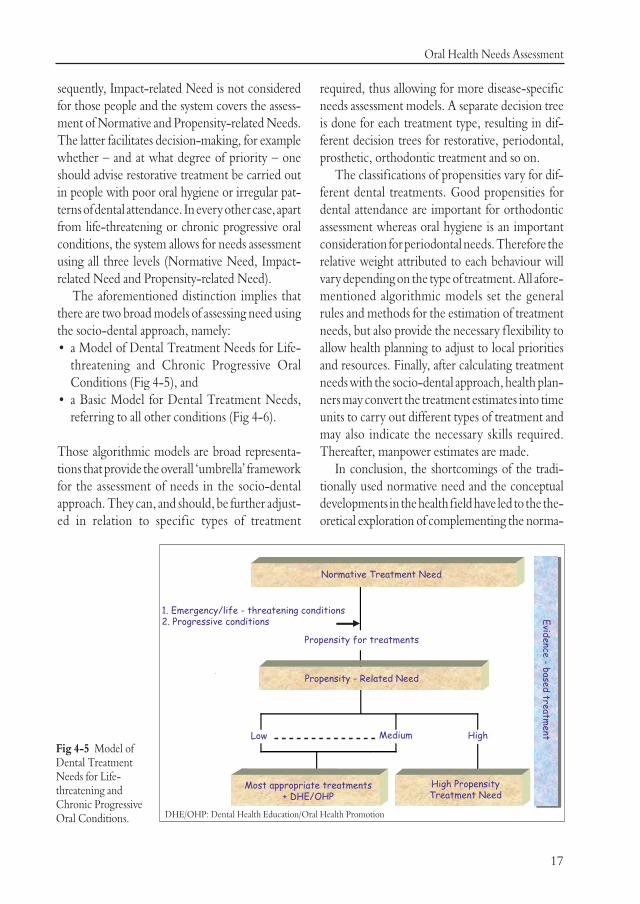
sequently, Impact-related Need is not consideredfor those people and the system covers the assess-ment of Normative and Propensity-related Needs.The latter facilitates decision-making, for examplewhether – and at what degree of priority – oneshould advise restorative treatment be carried outin people with poor oral hygiene or irregular pat-terns of dental attendance. In every other case, apartfrom life-threatening or chronic progressive oralconditions, the system allows for needs assessmentusing all three levels (Normative Need, Impact-related Need and Propensity-related Need).
The aforementioned distinction implies thatthere are two broad models of assessing need usingthe socio-dental approach, namely:• a Model of Dental Treatment Needs for Life-
threatening and Chronic Progressive OralConditions (Fig 4-5), and
• a Basic Model for Dental Treatment Needs,referring to all other conditions (Fig 4-6).
Those algorithmic models are broad representa-tions that provide the overall ‘umbrella’ frameworkfor the assessment of needs in the socio-dentalapproach. They can, and should, be further adjust-ed in relation to specif ic types of treatment
required, thus allowing for more disease-specificneeds assessment models. A separate decision treeis done for each treatment type, resulting in dif-ferent decision trees for restorative, periodontal,prosthetic, orthodontic treatment and so on.
The classifications of propensities vary for dif-ferent dental treatments. Good propensities fordental attendance are important for orthodonticassessment whereas oral hygiene is an importantconsideration for periodontal needs. Therefore therelative weight attributed to each behaviour willvary depending on the type of treatment. All afore-mentioned algorithmic models set the generalrules and methods for the estimation of treatmentneeds, but also provide the necessary f lexibility toallow health planning to adjust to local prioritiesand resources. Finally, after calculating treatmentneeds with the socio-dental approach, health plan-ners may convert the treatment estimates into timeunits to carry out different types of treatment andmay also indicate the necessary skills required.Thereafter, manpower estimates are made.
In conclusion, the shortcomings of the tradi-tionally used normative need and the conceptualdevelopments in the health field have led to the the-oretical exploration of complementing the norma-
17
Fig 4-5 Model ofDental TreatmentNeeds for Life-threatening andChronic ProgressiveOral Conditions. DHE/OHP: Dental Health Education/Oral Health Promotion

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
18
tive approach with socio-psychological and broad-er system factors. As Mechanic (1995) has accuratelystated: ‘the irony is that while so much of the chal-lenge in health care is social – to enhance the capac-ity of individuals to perform desired roles and activ-ities – the thrust of the health enterprise is sub-stantially technologic and reductionist, treatingcomplex socio-medical problems as if they areamenable to simple technical fixes.’ The new socio-dental approach to assessing dental needs attempts toovercome these inadequacies, by incorporating thenormative assessment with measurements of sub-jective perceptions and of the propensity to adopthealth promoting behaviours, while also account-ing for the provision of effective care. Thus, it pro-vides the theoretical framework necessary to reori-ent needs assessment from the narrow normativefocus towards the broader socio-environmentalperspective. And as such, it is a useful tool in plan-ning oral health services. The incorporation of suchsystems in the process of policy planning and eval-uation should be seen as a priority.
Summary of Main Points
• There are two distinct theoretical approach-es to defining health needs: the “humanitar-ian” approach, which focuses more on theburden of disease, and the “realistic”approach, which encompasses the concept of“ability to benefit” and focuses on healthgain.
• The most commonly used type of need assess-ment in oral health care planning is norma-tive or professionally defined need.Nevertheless, it has been severely criticized.
• Measures of perceived need, which ref lectsthe individual’s own assessment, should alsobe used. This implies using oral health-relat-ed quality of life indicators, which are sub-jective indicators that provide information onthe impact of oral disorders and conditions,and the perceived need for oral health care.
• The socio-dental approach is a comprehen-sive system for the assessment of oral health
Fig 4-6 Basic Model for Dental Treatment Needs, referring to all other conditions.
DHE/OHP: Dental Health Education/Oral Health Promotion

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
needs, consisting of the following elements:a) clinical estimates of normative need, b) gen-eral health status, c) subjective perceptions,including perceived treatment needs and oralhealth impacts, d) propensity to adopt healthpromoting behaviours, e) scientific evidenceof the effectiveness of treatments.
Key Question
What do you understand by the term ‘need’?Discuss the implications of these for Dental PublicHealth.
19
References
Acheson RM. The definition and identification of need forhealth care. J Epidemiol Community Health1978;32:10–15.
Addy M, Koltai R. Control of supragingival calculus. J ClinPeriodont 1994;21:342–346.
Adulyanon S, Sheiham A. Oral Impacts on DailyPerformances. In: Slade GD (ed). Measuring Oral Healthand Quality of Life. Chapel Hill, NC: University of NorthCarolina, Dental Ecology 1997;151?160.
Anderson JD. The need for criteria on reporting treatment out-comes. J Prosthet Dent 1998;79(1):49–55.
Antczak-Bouckoms A, Joshipura K, Burdick E, Tulloch JF.Meta-analysis of surgical versus non-surgical methods oftreatment for periodontal disease. J Clin Periodontol1993;20(4):259–268.
Arens U. Oral health, diet and other factors. Amsterdam:Elsevier, 1998.
Atchison KA, Dolan TA. Development of the Geriatric OralHealth Assessment Index. J Dent Educ 1990;54:680–687.
Bader J. Health services research in dental public health. JPublic Health Dent 1992;52:23–26.
Barenthin I. Dental health status and dental satisfaction. Int JEpidemiol 1977;6:73–79.
Blinkhorn AS, Davies RM. Caries prevention. A continuedneed worldwide. Int Dent J 1996;46(3):119–125.
Bowling A. Measuring disease: a review of disease-specificquality of life measurement scales. Buckingham, UK: OpenUniversity Press, 1995.
Bowling A. Measuring health: a review of quality of life meas-urement scales (2nd Edn.). Buckingham, UK: OpenUniversity Press, 1997.
Bradshaw JS. A taxonomy of social need. In: McLachlan G (ed).Problems and progress in medical care, Seventh Series.Oxford: Oxford University Press, 1972;69–82.
Burt BA. Prevention policies in the light of the changing dis-tribution of dental caries. Acta Odontol Scand1998;56(3):179–186.
Burt B, Pai S. Is sugar consumption still a major determinantof dental caries? A systematic review. In: ConsensusDevelopment Conference on diagnosis and management ofdental caries throughout life. Bethesda, MD: NationalInstitute of Health, 2001.
Carr AJ, Higginson IJ, Robinson PG. Quality of life. London:BMJ Books, 2003.
Cochrane AL. Effectiveness and efficiency: random ref lectionson health services. London: Nuffield Provincial HospitalsTrust, 1972.
Cohen K, Jago JD. Toward the formulation of socio-dentalindicators. Int J Health Serv 1976;6:681–687.
Cooper MH. Rationing health care. London: Croom Helm,1975.
Coulter ID, Marcus M, Atchison KA. Measuring oral healthstatus: theoretical and methodological challenges. Soc SciMed 1994;38:1531–1541.
Cushing AM, Sheiham A, Maizels J. Developing socio-dentalindicators: the social impact of dental disease. CommunityDent Health 1986;3:3–17.
Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, Taylor R. The clinical effectiveness andcost-effectiveness of routine dental checks: a systematicreview and economic evaluation. Health Technol Assess2003;7(7):iii–v,1–127.
Davis P. The social context of dentistry. London: CroomHelm, 1980.
Donabedian A. Aspects of medical care administration: speci-fying requirements for health care. Cambridge, MA:Harvard University Press, 1973.
Engel GL. The need for a new medical model: a challenge forbiomedicine. Science 1977;196:129–136.
Elderton RJ. Clinical studies concerning re-restoration ofteeth. Adv Dent Res 1990;4:4–9.
Elderton RJ, Nuttall NM. Variation among dentists in plan-ning treatment. Br Dent J 1983;154(7):201–206.
Frazier JP. Research on oral health education and promotionand social epidemiology. J Public Health Dent1992;52:18–22.
Fuchs VR. The contribution of health services to the Americaneconomy. In: Fuchs VR (ed). Essays on the economics ofhealth and medical care. New York: Columbia UniversityPress, 1972.
Giddon DB, Moser M, Colton T, Bulman J. Quantitative rela-tionships between perceived and objective need for healthcare – dentistry as a model. Public Health Rep1976;91:508–513.
Gift HC, Atchison KA. Oral health, health, and health-relat-ed quality of life. Med Care 1995;33:NS57–NS77.

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Aubrey Sheiham and Georgios Tsakos
Gift HC, Atchison KA, Drury TF. Perceptions of the naturaldentition in the context of multiple variables. J Dent Res1998;77(7):1529–1538.
Gjermo P. Factors inf luencing the assessment of treatmentneeds. J Clin Periodontol 1991;18(6):358–361.
Guyatt GH, Veldhuyzen Van Zanten SJO, Feeny DH, PatrickDL. Measuring quality of life in clinical trials: a taxonomyand review. Can Med Assoc J 1989;140:1441–1448.
Hunt SM, McEwen J, McKenna SP. Measuring Health Status.London: Croom Helm, 1986.
Kidd EA, Toffenetti F, Mjor IA. Secondary caries. Int Dent J1992;42(3):127–138.
Leao A, Sheiham A. Relation between clinical dental statusand subjective impacts on daily living. J Dent Res1995;74:1408–1413.
Locker D. Measuring oral health: a conceptual framework.Community Dent Health 1988;5:3–18.
Locker D. An Introduction to Behavioural Science andDentistry. London: Routledge, 1989.
Locker D. The burden of oral disorders in a population of olderadults. Community Dent Health 1992;9:109–124.
Locker D. Applications of self-reported assessments of oralhealth outcomes. J Dent Educ 1996;60:494–500.
Locker D. Concepts of oral health, disease and the quality oflife. In: Slade GD (ed). Measuring Oral Health and Qualityof Life. Chapel Hill, NC: University of North Carolina,Dental Ecology, 1997;11–23.
Locker D. Issues in measuring change in self-perceived oralhealth status. Community Dent Oral Epidemiol1998;26:41–47.
Locker D, Jokovic A. Using subjective oral health status indi-cators to screen for dental care needs in older adults.Community Dent Oral Epidemiol 1996;24:398–402.
Locker D, Slade G. Association between clinical and subjec-tive indicators of oral health status in an older adult popu-lation. Gerodontology 1994;11:108–114.
Maizels J, Maizels A, Sheiham A. Socio-dental approach to theidentif ication of dental treatment-need groups.Community Dent Oral Epidemiol 1993;21:340–346.
Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoridetoothpastes for preventing dental caries in children and ado-lescents (Cochrane review). In: The Cochrane Library,Issue 3, 2003. Oxford: Update Software.
Matthew GK. Measuring need and evaluating services. In:McLachlan G (ed). Portfolio for health: the role and pro-gramme of the DHSS in health services research. London:Oxford University Press, 1971;27–46.
Matthias RE, Atchison KA, Lubben JE, de Jong F, ScweitzerSO. Factors affecting self-ratings of oral health. J PublicHealth Dent 1995;55:197–204.
McDonald RE, Avery DR. Dentistry for the child and ado-lescent (7th edn.). St. Louise: Mosby Inc, 2000.
Mechanic D. Emerging trends in the application of the socialsciences to health and medicine. Soc Sci Med1995;40:1491–1496.
Milgrom P, Reisine S. Oral health in the United States: thepost-f luoride generation. Annu Rev Public Health2000;21:403–436.
Moynihan PJ. Dietary advice in dental practice. Br Dent J2002;193(10):563–568.
Muir Gray JA. Evidence-based health care. London: ChurchillLivingstone, 1997.
NHS Centre for Reviews and Dissemination. Dental restora-tion: what type of f illing? Effective Health Care1999;5(2):12.
Petersson GH, Bratthall D. The caries decline: a review ofreviews. Eur J Oral Sci 1996;104:436–443.
Pope AM, Tarlov AR. Disability in America. Toward a nation-al agenda for prevention. Washington, DC: NationalAcademy Press, 1991.
Rodrigues CS, Sheiham A. The relationships between dietaryguidelines, sugar intake and caries in primary teeth in lowincome Brazilian 3-year-olds: a longitudinal study. Int JPaediatr Dent 2000;10(1):47–55.
Rosenoer LM, Sheiham A. Dental impacts on daily life andsatisfaction with teeth in relation to dental status in adults.J Oral Rehabil 1995;22:469–480.
Sackett DL, Snow JC. The magnitude of compliance and non-compliance. In: Haynes RB, Taylor DW, Sackett DL (eds).Compliance in health care. Baltimore, MD: John HopkinsUniversity Press, 1979;11–22.
Shaw WC, Richmond S, O'Brien KD, Brook P. Quality con-trol in orthodontics: indices of treatment need and treat-ment standards. Br Dent J 1991;170:107–112.
Sheiham A. Is the chemical prevention of gingivitis necessaryto prevent severe periodontitis? Periodontol 20001997;15:15–24.
Sheiham A. Dietary effects of dental diseases. Public HealthNutrition 2001;4(2B):569–591.
Sheiham A, Maizels JE, Cushing AM. The concept of need indental care. Int Dent J 1982;32:265–270.
Sheiham A, Maizels J, Maizels A. New composite indicators ofdental health. Community Dent Health 1987;4: 407–414.
Slade GD. Measuring Oral Health and Quality of Life. ChapelHill, NC: University of North Carolina, Dental Ecology,1997.
Slade GD, Spencer AJ. Social impact of oral conditions amongolder adults. Aust Dent J 1994;39:358–364.
Slade GD, Strauss RP, Atchison KA, Kressin NR, Locker D,Reisine ST. Conference summary: assessing oral healthoutcomes – measuring health status and quality of life.Community Dent Health 1998;15:3–7.
Spencer AJ. The estimation of need for dental care. J PubHealth Dent 1980;40:311–327.
Spencer AJ. Evaluation of changing normative needs for den-tal care in planning for the delivery of dental care to theAustralian adolescent population. PhD Thesis. Universityof Melbourne, 1984.
Srisilapanan P, Sheiham A. The prevalence of dental impactson daily performances in older people in NorthernThailand. Gerodontology 2001a;18:102–108.
20

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Oral Health Needs Assessment
Srisilapanan P, Sheiham A. Assessing the difference betweensocio-dental and normative approaches to assessing pros-thetic dental treatment needs in dentate older people.Gerodontology 2001b;18:25–34.
Stevens A, Gabbay J. Needs assessment. Health Trends1991;23:20–23.
Stevens A, Raftery J. Health care needs assessment. The epi-demiologically based needs assessment reviews. Volume 1.Oxford: Radcliffe Medical Press, 1994a.
Stevens A, Raftery J. Health care needs assessment. The epi-demiologically based needs assessment reviews. Volume 2.Oxford: Radcliffe Medical Press, 1994b.
Sutcliffe P. Oral cleanliness and dental caries. In: Murray JJ(ed). The prevention of oral diseases. Oxford: OxfordUniversity Press, 1996;68–77.
Testa MA, Nackley JF. Methods for quality-of-life studies.Annu Rev Public Health 1994;15:535–559.
The British Nutrition Foundation. Healthy teeth. In: UpdateSoftware, 1998. http://www.nutrition.org.uk/informa-tion/dietandhealth/healthyteeth.html
The Cochrane Collaboration Oral Health Group.http://www.cochrane-oral.man.ac.uk (last visitedSeptember 2005).
Tickle M, Worthington HV. Factors inf luencing perceivedtreatment need and the dental attendance patterns of olderadults. Br Dent J 1997;182:96–100.
Tsakos G, Marcenes W, Sheiham A. Evaluation of a modifiedversion of the index of Oral Impacts on Daily Performances(OIDP) in elderly populations in two European countries.Gerodontology 2001;18(2):121–130.
Ware JE, Brook RH, Davies AR, Lohr KN. Choosing meas-ures of health status for individuals in general populations.Am J Pub Hlth 1981;71:620–625.
World Health Organization. Preamble to the Constitution ofthe World Health Organization as adopted by theInternational Health Conference, New York, 19–22 June,1946; signed on 22 July 1946 by the representatives of 61States. Official records of the World Health Organization,no. 2, p.100. World Health Organization, 1948.
World Health Organization. International classification ofimpairments, disabilities and handicaps. Geneva: WorldHealth Organization, 1980.
World Health Organization. Oral health surveys: Basic meth-ods (4th Edn.). Geneva: World Health Organization, 1997.
World Health Organization. Diet, nutrition and the preven-tion of chronic diseases. Report of a Joint WHO/FAOExpert Consultation. Geneva: World Health Organization,2003.
Wright J. Health Needs Assessment in Practice. London: BMJBooks, 1998.
21

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication