Embed Size (px)
Citation preview

Oral Hypoglycemic Agents and You
John Kashani DO
St. Josephs Medical Center
New Jersey Poison Center

Objectives
• Outline Insulin physiology, glucose regulation and hypoglycemia
• Discuss type 2 diabetes and medications used in it’s treatment
• Outline the management and disposition of patients exposed to these agents

Physiologic effects of insulin
• Effects will vary depending on the tissue involved– Facilitates the entry of glucose into
muscle, adipocytes and various other tissues
– Stimulates the production of glycogen in the liver

Physiologic effects of insulin
– Activates hexokinase
– Inhibits glucose-6-phosphatase
– Activates phosphofructokinase and glycogen synthase
– Promotes the synthesis of fatty acids
– Inhibits the breakdown of fat in adipose tissue

Physiologic effects of insulin
• Inhibits intracellular lipase
• Stimulates the uptake of amino acids
• Increases the permeability of cells to potassium, magnesium and phosphate ions

Glucagon
• Maintains blood glucose levels between meals and fasting periods
– Initiates glycogenolysis
– Increase the transport of amino acids in the liver – gluconeogenesis
– Activates adipose cell lipase – makes fatty acids available for energy

Cathecholamines
• Norepinephrine and epinephrine
– Maintain blood glucose levels during periods of stress
– Increase lipase activity – increases the mobilization of fatty acids
–inhibits insulin release
–Promotes glycogenolysis

Growth Hormone
• Increases protein synthesis
• Mobilizes fatty acids
• Antagonizes the effects of insulin
• Decreases the cellular uptake of glucose
• Initial plasma glucose-lowering effect

Glucocorticoids
• Critical to survival during periods of fasting and starvation
• Stimulate gluconeogensis
• Decrease tissue use of glucose
• Initial plasma glucose-lowering effect similar to growth hormone

Glucose Regulation
• Glucose maintained between 70-140 mg/dL by several mechanisms
• Above this range, pancreatic beta cells secrete insulin
• Below this range, the major acute defense is glucagon release


Type 2 Diabetes
• Heterogeneous condition describing hyperglycemia and relative insulin deficiency– High, normal or low insulin levels
• No HLA markers or antibodies• Usually middle aged and overweight• Symptoms tend to be more gradual than
type 1

Oral Hypoglycemic Agents
• An increasing number of medications available for the treatment of type 2 diabetes mellitus
• Vary in mechanism of action, adverse effects and toxicity
• There is little experience with toxicity and overdose with some of the newer agents

Common Scenarios
• Accidental ingestion in a child
• Took too much by accident
• Intentional overdose
– Diabetic vs. non-diabetic

Type 2 Agents
• Hypoglycemic agents
– Sulfonylureas
– Benzoic acid derivatives
• Antihyperglycemic agents
– Biguanides -glucosidase inhibitors
– Thiazolidinedione derivatives

Sulfonylureas• Stimulate the beta cells of the pancreas to
produce insulin• Bind to the sulfonylurea receptor on the pancreatic
beta cell• Ineffective in type I diabetics who lack the capacity
to produce insulin• Lower the blood glucose in type 2 diabetic patients• Lower the blood glucose in non-diabetic patients

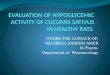
Sulfonylurea Mechanism
Pancreatic cell
Sulfonylurea receptor
sulfonylurea
KATP
Ca
I I
I
I
insulin
K+

Sulfonylureas
• Decrease hepatic insulin clearance
• Increase serum insulin concentrations
• Reduce hepatic glucose production
• Increase peripheral insulin sensitivity

Sulfonylureas
• Highly protein bound
• Metabolized in the liver
• Renal excretion
• Large Vd (10-15 L/kg)

1st Generation Sulfonylureas
• Acetohexamide
• Chlorpropamide
• Tolazamide
• Tolbutamide

1st Generation
• Reduce hepatic clearance of insulin
• Produce active hepatic metabolites
• Long half life and duration of action
• Dependent on urinary excretion to maintain euglycemia

Chlorpropamide• Half-life may be >24 hours with up to
60 hours duration of action• Can cause hyponatremia (SIADH)• Disulfuram reaction• Cholestatic jaundice• Agranulocytosis, thrombocytopenia,
anemia• Elimination enhanced by urinary
alkalinization

2nd Generation Sulfonylureas
• Glimeperide
• Glipizide
• Glyburide
• 100x more potent than first generation
• Improved safety profile

2nd Generation
• Half lives approach 24 hours
• Associated with substantial fecal excretion of the parent drug
• More lipid soluble than first generation

Sulfonylureas
Agent Onset (h) Peak (h) Duration (h)
Acetohexamide 2 4 12-24
Chlorpropamide 1 5 24-72
Glimepride 2.5 24
Glipizide 0.5 1 < 24
Glyburide 0.5 4 24
Tolazamide 1 5 18
Tolbutamide 1 6 6-12

Sulfonylureas
• Chlorpropamide, Glyburide, and Glipizide are the most likely to cause prolonged hypoglycemia
• Duration of action prolonged in presence of renal and hepatic disease

Pediatric Ingestion
• 5 year retrospective review (Clin Tox 34(3)1996)
– 93 cases, 25 patients (27%) developed hypoglycemia
– 79% onset within 4 hours
– Remainder up to 16 hours

Biguanides
• Active component of Galega officinalis, the French lilac
• Lower the blood glucose in diabetic patients
• Does not lower blood glucose in normal patients
• Improves insulin sensitivity

Galega officinalis

Everything Spectatularis

Biguanides
• Phenformin
– Withdrawn from the US market in 1976
– 1/4000 patients develop lactic acidosis
• Metformin (Glucophage)
– Introduced in the US in 1995

Metformin
• Inhibits gluconeogenesis and reduces hepatic glucose output– Reduces fasting plasma glucose– Increases glycogen formation
• Causes increase in glucose uptake and utilization in peripheral tissues
• Reduction of serum insulin concentrations• Inhibits lipolysis

Metformin
• Orally absorbed within six hours
• Peak serum levels 2-3 hours
• Minimally bound to plasma proteins
• Not metabolized by the liver
• Half life 4 - 8.7 hours
• Excreted by the kidney

Metformin
• Lactic acidosis
– 1/40000-80000 patients
– Majority have renal insufficiency
– Has been found in association with levels above 5 ug/ml
– Generally assumed to be type B

Mechanism of Lactic Acidosis
• Inhibit gluconeogenesis - accumulation of pyruvate
• Fat catabolism - oxidation of fatty acids - depletes NAD+ - increases NADH
• Increased ratio inhibits pyruvate dehydrogenase and the entry of pyruvate into the Kreb’s cycle

Mechanism of Lactic Acidosis
• Fatty acid oxidation increases acetyl CoA/CoA ratio - further decreases entry of pyruvate into the Kreb’s cycle
• With pyruvate dehydrogenase inhibited and gluconeogenesis blocked, the accumulated pyruvate is metabolized to lactate

-glucosidase Inhibitors
• Acarbose
• Miglitol
• Do not cause hypoglycemia but may potentiate the action of the sulfonylureas

Acarbose
• Results in competitive inhibition of the -glucosidase on the brush border of the small bowel– Reduces intestinal starch and disaccharide
absorption• Delayed carbohydrate absorption and
redistribution throughout the intestines yields a decreased, constant insulin production due to lowered postprandial glucose concentrations

Acarbose
• Only 1-2% is absorbed by the gut
• Does not cause hypoglycemia
• Toxicity:
– Abdominal discomfort
– Mild GI effects
– Flatulence, abdominal bloating
• Hepatic toxicity has been reported

Thiazolidinediones
• Troglitazone (Rezulin)
– Withdrawn from the market in the US in 2000 due to cases of fatal liver toxicity
• Rosiglitazone (Avandia)
• Pioglitazone (Actos)

Thiazolidinediones
• Increase insulin sensitivity• Decrease hepatic glucose output• Mechanism:
– Bind to nuclear peroxisome proliferator-activated receptors involved in transcription of insulin-responsive genes and in regulation of adipocyte differentiation and lipid metabolism

Thiazolidinediones
• Rapidly absorbed• Highly (>99%) protein bound• Metabolized by CYP3A4
– Loss of contraceptive effect reported with ethinyl estradiol/norethindrone
• Half-life 16 - 34 hours• 2 reports of hepatotoxicity with
rosiglitazone

Benzoic Acid Derivatives
• Repaglinide• Limited experience with this agent
• Binds to the KATP channel on the beta cell at a different receptor from the sulfonylureas– Extrapancreatic effect leading to
increased insulin sensitivity postulated

Repaglinide
• Rapidly absorbed
• Metabolized by the 3A4
• Short half-life (1 hr)
• Excreted primarily in the bile
• Highly protein bound (>98%)
• Hypoglycemia is expected in overdose, no cases reported to date

Repaglinide
• Severe hypoglycemia from clarithromycin-repaglinide drug interaction
– Khamaisi M, Leitersdorf E
– Pharmacotherapy. 2008 May;28(5):682-4

Repaglinide
• Serious hypoglycemia associated with misuse of repaglinide
– Flood TM
– Endocr Pract. 1999 May-Jun;5(3):137-8

Repaglinide
• Hypoglycemia probably due to accidental intake of repaglinide
• Lee IT, Sheu WH, Lin SY
• Chang Gung Med J. 2002 Nov;25(11):783-6

Management
• Patient asymptomatic with normal glucose, but agent known to produce hypoglycemia – Activated charcoal– Prophylactic glucose not recommended– Observe 8 hours, if hypoglycemia
develops admit

Management
• Patient already hypoglycemic: IV dextrose
– Adult initially 1g/kg of D50W
– Children .5 to 1 g/kg D25W
– Neonates .5 to 1 g/kg D10W

IV Glucose
• D10 maintenance infusion • Rate of infusion adjusted to keep the
patient euglycemic• Central venous line when D20 is required• As the patient begins to eat and glucose
rises, taper the infusion• Switch to D5W

Octreotide
• Semisynthetic long-acting analog of somatostatin
• IV half life of 72 minutes
• Inhibits the secretion of insulin, glucagon, growth hormone, gastrin and other hormones

Octreotide
• 50 - 100 g subcutaneously every 8 -12 hours
• Has been shown to reduce the glucose infusion requirements to maintain euglycemia following sulfonylurea overdose
• Most frequent side effect is mild steatorrhea

Diazoxide
• A vasodilator • Effective for refractory hypoglycemia• Directly inhibits insulin secretion by opening
KATP channels• Increases hepatic glucose production• Decreases cellular glucose utilization• Slow IV infusion (300 mg IV over 30
minutes every 4 hours)

Glucagon
• Recruits hepatic glycogen stores and induces gluconeogenesis
• Partially dependent on the adequacy of glycogen stores
• Reserve for temporizing treatment in patients in whom IV access cannot be rapidly established

Dialysis
• Not effective for most oral hypoglycemic agents because of their high protein binding
• May be needed for severe lactic acidosis from biguanides– Corrects metabolic acidosis– Removes lactate, ketones, and
metformin

Other Management Points
• Treat lactic acidosis early and intensively– Sodium bicarbonate for pH < 7.1
• Urinary alkalinization effective only for chlorpropamide– A pH of 7-8 can reduce the half-life
from 49 to 13 hours– Check Potassium frequently

Who Needs Admission?
• Hypoglycemia in the setting of an oral Sulfonylurea
• Pediatric exposures (potential) to a sulfonylurea
• Hypoglycemic Repaglinide exposures

Salient Points
• Don’t F%$# with hypoglycemia• Chlorpropamide excretion may be
increased by urinary alkanilization• 1st generation oral Suffonylurease are
sulfonamide based• GI upset is expected with -glucosidase
Inhibitors• Hepatic toxicity may occur with
Thiazolidinediones