-
8/16/2019 Oral Injury
1/50
1 www.aap.org/oralhealth/pact
Protecting All Children’s Teeth
Oral Injury
-
8/16/2019 Oral Injury
2/50
2www.aap.org/oralhealth/pact
Introduction
Dental injuries are very common, and up to 30% of children
injure their primaryteeth. These injuries occur most often during
the toddler years when children areactive, but unsteady on their
feet.
These injuries become common again in the midelementary
school years !ages "to #0$ as children join sports teams and become
more independently activeoutdoors !eg, bicycles, playgrounds,
trampolines$.
n adolescence, motorvehicle accidents and assault become
increasinglyimportant in the epidemiology of dental injury.
&verall, tooth injury is more common in males !greater than
a '(# ratio$, and
almost half of all children will incur some type of tooth damage
by the time theyreach adolescence.
)sed with permission from *ontent +isionary
-
8/16/2019 Oral Injury
3/50
3
Learner Objectives
)pon completion of this presentation, participants will be able
to(
Describe the incidence and epidemiology of dental injury in
the)nited tates.
&utline a proper e-amination following an oral injury.
ist and describe the categories of tooth injury, their
basicmanagement, and possible seuelae.
Discuss in detail the proper management of an avulsed tooth.
1rovide appropriate anticipatory guidance for oral injury
prevention. *ompare and contrast the 3 basic types of mouth guards
and
summari2e the 1D recommendations on mouth guard use
inathletics.
)sed with permission from *ontent +isionary
-
8/16/2019 Oral Injury
4/50
4 www.aap.org/oralhealth/pact
Patterns and Risk Factors
The most common injury site is the ma-illary !upper$
centralincisors,
which account for more than 40% of all dental injuries.
&ral injuries typically result from falls !most common$,
bi5e andcar accidents, sportsrelated injuries, and violence.
The mouth is also a common site for nonaccidental trauma,
andchild abuse should always be considered in a child
presentingwith oral trauma.
-
8/16/2019 Oral Injury
5/50
5 www.aap.org/oralhealth/pact
Patterns and Risk Factors
1ediatricians should be aware of the following ris5 factors
fororal trauma(
*hildren with compromised protective re6e-es or
poorcoordination 8yperactivity ubstance abuse !by the
adolescent or within the family$
*hild abuse or neglect 9alocclusion with protruding
front teeth :ailure to use protective face and mouth gear
-
8/16/2019 Oral Injury
6/50
-
8/16/2019 Oral Injury
7/507 www.aap.org/oralhealth/pact
Ea!ination Follo"ing Oral Injury#
continued
#. rrigate to remove blood and debris and to improve
visuali2ation.
'. >-amine soft tissues for edema, tenderness, and
lacerations.
3. >-amine bony structures for pain or malocclusion.
@. ssess patient-amine the tooth ridge for AstepoBsC, which can
indicate a
fracture of the underlying alveolar bone.. >-amine the teeth
for tenderness and mobility.
. ccount for all teeth and determine if injury has occurred to
the
primary or permanent dentition.
-
8/16/2019 Oral Injury
8/508 www.aap.org/oralhealth/pact
$issing Teeth
9issing teeth should be accounted for.
Do not assume that missing teeth were lost at the scene of
theaccident because they may be imbedded in soft tissues,
intruded
into the alveolar bone or sinus cavity, aspirated, or
swallowed.
?adiographs !soft tissue and chest Erays$ should be done to
loo5
for missing teeth.
-
8/16/2019 Oral Injury
9/509 www.aap.org/oralhealth/pact
%ental Trau!a
t is important that clinicians be familiar
with the diBerent types of dental trauma
and be able to appropriately triageinjured patients.
Dental followup is necessary for all
tooth trauma because even seemingly
minor injuries can result in tooth death.
n general, management of primary
tooth injury is dictated by concern for
the safety of the permanent dentition.
)sed with permission from ?ocio ;. Fuinone2, D9D, 9, 918G
ssociate1rofessor Department of 1ediatric Dentistry, chool of
Dentistry
-
8/16/2019 Oral Injury
10/5010 www.aap.org/oralhealth/pact
Ty&es o' Tooth Injury
Tooth injury can be divided into main
categories(
#. *oncussion
'. ublu-ation
3. ateral u-ation
@. ntrusion
4. >-trusion. vulsion
. :racture )sed with permission from 9artha nn Heels, DD, 1hDG
Division 8ead of Du5e 1ediatricDentistry,
Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
11/50
11 www.aap.org/oralhealth/pact
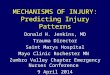
Concussion
*oncussion involves injury to supporting structures ofthe
tooth, without loosening or displacement.
Tooth is tender to percussion.
?ecommended Treatment(
tic5 to a soft diet for ' wee5s.
9onitor for changes in tooth color.
?efer to dentist for nonurgent evaluation.
-
8/16/2019 Oral Injury
12/50
-
8/16/2019 Oral Injury
13/50
13 www.aap.org/oralhealth/pact
Lateral Luation
ateral lu-ation involves injury to the
tooth and its supporting structures,
resulting in tooth displacement. The
injured tooth is at ris5 for pulpal necrosis
and root resorption.
This type of injury reuires prompt referral
to a dentist for repositioning of the injured tooth/teeth.
>ven primary teeth should be e-amined by a dentist, because
the
)nderlying permanent tooth may be injured.
)sed with permission from 9artha nn Heels, DD, 1hDG Division
8ead ofDu5e 1ediatric Dentistry, Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
14/50
14 www.aap.org/oralhealth/pact
Intrusion
Jith intrusion injuries, the tooth is
pushed into the soc5et and thealveolarbone. t may appear
shortened orbarely visible.
ntrusion has a poor prognosis and
high ris5 for complications,including
root resorption, pulp necrosis, and
infection. 9ay reuire a root canal.ntrusion injuries may also
damage underlying permanent dentiespecially if an infection
develops.
)sed with permission from 9artha nn Heels, DD, 1hDG Division8ead
of Du5e 1ediatric Dentistry, Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
15/50
15 www.aap.org/oralhealth/pact
Intrusion# continued
Jith intrusion injuries, teeth may reerupt. f a primary tooth
does
K&T reerupt, it will reuire e-traction to not interfere
with
permanent tooth eruption.
?ecommended Treatment(
Do not attempt to remove intruded tooth. nstead, focus on
pain
control and consider antibiotic prophyla-is.
:or a primary tooth, see5 dental evaluation within # wee5
!orearlier, for signi=cant symptoms$.
:or a permanent tooth, refer to a dentist immediately
for
repositioning and splinting.
-
8/16/2019 Oral Injury
16/50
16 www.aap.org/oralhealth/pact
Etrusion
Jith an e-trusion injury, the tooth
is partially displaced from its soc5et.
This type of injury reuires
repositioning and stabili2ation.
?efer to a dentist promptly to
evaluate the e-tent of injury, as well
as any associated injury !e.g.
fracture$. )sed with permission from ?ama &s5ouian
-
8/16/2019 Oral Injury
17/50
17 www.aap.org/oralhealth/pact
Avulsion
Jith this type of injury, the
tooth
is completely out of the soc5et.
9anagement of avulsion
injuriesdepends on the tooth type.
)sed with permission from ?ama &s5ouian
-
8/16/2019 Oral Injury
18/50
18 www.aap.org/oralhealth/pact
Avulsion o' a Pri!ary Tooth
Do K&T reimplant a primary tooth, as this may
damage the underlying permanent tooth.
nstead, refer to a dentist within '@ hours.
-
8/16/2019 Oral Injury
19/50
19 www.aap.org/oralhealth/pact
Avulsion o' a Per!anent Tooth
This is a dental emergencyL
vulsion should be managed as follows(
#. Gently rinse oB debris with saline or mil5. 8old
tooth by crown only.
'. void touching the root. Do not clean or rub it. t is
important to
preserve the periodontal ligament for tooth survival.
3. ?eimplant an avulsed permanent tooth immediately,
ensuring
correct orientation. The tooth should be reimplanted within
'0
minutes, but the best outcome is with teeth replaced
within 4 minutes.
@. nstruct patient to bite on gau2e or a hand5erchief or to hold
the
tooth in place.
-
8/16/2019 Oral Injury
20/50
20 www.aap.org/oralhealth/pact
Avulsion o' a Per!anent Tooth#
continued
4. end to a dentist or ma-illofacial surgeon immediately for
radiographs, splinting, and antibiotic prophyla-is.
. f the tooth cannot be reimplanted on scene, transport it
!orderedby preference$ in( a tooth storage solution, warm mil5,
saline, or
saliva.
. tooth should not be transported dry or in plain water, as
this
signi=cantly decreases the chance of ligament
survival.
". Kever suggest a child hold the damaged tooth in his or her
mouth because of the ris5 of aspiration or bacterial
contamination.
-
8/16/2019 Oral Injury
21/50
21 www.aap.org/oralhealth/pact
Fracture
There are 4 basic types of tooth fracture(
#. In'raction( incomplete fracture !crac5$ of the enamelwithout
loss of tooth structure.
'. )nco!&licated Cro"n 'racture( an enamel fracture oran
enameldentin fracture that does not involve the pulp.
3. Co!&licated Cro"n 'racture( an enameldentinfracture with
pulp e-posure.
@. Cro"n*root 'racture( an enamel, dentin, and cementumfracture
with or without pulp e-posure.
4. Root Fracture( a dentin and cementum fractureinvolving
the pulp
-
8/16/2019 Oral Injury
22/50
22
)nco!&licated Cro"n Fracture
This type of fracture is a crac5 of the enamel ordentin
that does not involve the pulp. t may havea sharp edge.
?ecommended Treatment(
M nspect injured lips, tongue, and gingiva to ruleout presence
of tooth fragments.
M 1rovide a soft diet, avoiding temperaturee-tremes.
M f a permanent tooth is injured, refer to a dentistfor
evaluation 1 !within #' to '@ hours$.
M ?ecommend longterm followup to evaluate forcomplications,
which are uncommon.
)sed with permission from:a. Rocio B. Quinonez, DMD, MS, MPH;
Associate Professor Department of Pediatric
Dentistry, Schoo of Dentistry
b. 9artha nn Heels, DD, 1hDG Division 8ead of Du5e 1ediatric
Dentistry,Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
23/50
23 www.aap.org/oralhealth/pact
Co!&licated Cro"n Fracture
*omplicated crown fracture is an enameldentin fracture with pulp
e-posure.
ite of a complicated crown fracture hasa reddish tinge or will
bleed.
This type of fracture can cause e-tremepain and may lead
to pulpal necrosis, root
resorption, or infection in e-posed pulp.
?efer to dentist as soon as possible!within #' to '@ hours$ for
evaluation.
)sed with permission from(a. ?ebecca latyton DD, 1hD
!. Rocio B. Quinonez, DMD, MS, MPH; Associate Professor
Department
of Pediatric Dentistry, Schoo of Dentistry
-
8/16/2019 Oral Injury
24/50
24 www.aap.org/oralhealth/pact
Cro"n*Root Fracture
>namel, dentin, and cementum fracture with or without
pulpe-posure.
i5ely complications include root resorption and
pulpnecrosis.
?efer to dentist as soon as possible !within #' to '@ hours$for
evaluation, where diagnosis will be made via radiograph.
Treatment consists of reduction and splinting or
e-traction.
-
8/16/2019 Oral Injury
25/50
25 www.aap.org/oralhealth/pact
Root Fracture
>-cessive mobility of the tooth may indicate a
root fracture. This type of fracture includes
pulp e-posure. 1otential complications for aroot fracture
include resorption and pulp necrosis.
?efer to a dentist 1 !within #''@ hours$ forevaluation, where
diagnosis is made radiographically.
Treatment consists of reduction and splinting for
permanent teeth or e-traction, depending on the e-tent of
the
traumatic lesion.
)sed with permission from 9artha nn Heels,DD, 1hDG Division 8ead
of Du5e 1ediatric
Dentistry, Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
26/50
26 www.aap.org/oralhealth/pact
Co!&lications and Conse+uences o'
Tooth Injury
There are many possible conseuences of an oral injury(
1ain, which can be severe. nfection, including
abscess. n5ylosis. n6ammatory root
resorption. esthetic conseuences. Kegative impact on
selfesteem. mpaired oral or phonetic function. 8igh
cost.
:or these reasons, prevention of tooth injury is paramount.
-
8/16/2019 Oral Injury
27/50
27 www.aap.org/oralhealth/pact
Prevention
1revention is the most eBective intervention.
1rimary care clinicians are in a uniue positionto help families
prevent accidental trauma,including oral trauma, by providing
anticipatory guidance at routine visits.
-
8/16/2019 Oral Injury
28/50
28 www.aap.org/oralhealth/pact
Accident Prevention
uggestions for accident prevention speci=cally related to
oral
trauma(
#. dvise parents about possible injury to developing
permanent teeth from trauma if a primary tooth is
injured.
'. ?eview and anticipate developmental milestones.
3. *ounsel about the ris5s of wal5ers and trampolines.
@. Discuss childproo=ng the home.
4. ?eview safety measures for outdoor activities and sports.
. tress the importance of adeuate supervision at all times,
especially on furniture, stairs, at the playground, and at
athletic
events or practices.
-
8/16/2019 Oral Injury
29/50
29 www.aap.org/oralhealth/pact
(&orts and Protective ,ear
ports participation poses a signi=cant ris5 for trauma
The highest ris5 sports for oral trauma are baseball,
soccer, football,bas5etball, and hoc5ey.
5ateboarding, rollerblading, and bicycling injuries are also
common.
-
8/16/2019 Oral Injury
30/50
30 www.aap.org/oralhealth/pact
(&orts and Protective ,ear#
continued
8elmet and face mas5s should be properly =tted and worn
during all games and practices for the sports in which
theyare
recommended.
tatistically, children are more often injured in practice
than
during a game, so all protective gear should be worn
duringpractice as well.
-
8/16/2019 Oral Injury
31/50
31 www.aap.org/oralhealth/pact
$outh ,uards
9outh guard use is mandatory for football, icehoc5ey, lacrosse,
=eld hoc5ey, and bo-ing.
everal states have passed regulations mandating
mouth guards for soccer, bas5etball, andwrestling.
-
8/16/2019 Oral Injury
32/50
32 www.aap.org/oralhealth/pact
Facts About $outh ,uard )se
#. 9outh guards help to protect the teeth and soft
tissues ofthe mouth from injury.
'. The better the =t, the more protection oBered.
3. 9outh guard use may reduce the ris5 or severity of a
concussion.
-
8/16/2019 Oral Injury
33/50
33 www.aap.org/oralhealth/pact
Ty&es o' $outh ,uards
There are 3 types of mouth guards(
#. toc5.
'. 9outhformed, or Aboilandbite.C
3. *ustom =t.
)sed with permission from 9artha nn Heels, DD, 1hDG Division
8ead ofDu5e 1ediatric Dentistry, Du5e *hildrenIs 8ospital
-
8/16/2019 Oral Injury
34/50
34 www.aap.org/oralhealth/pact
(tock $outh ,uards
These preformed, overthecounter, readyto
wear mouth guards are generally the leastcomfortable and,
therefore, the least li5ely to beworn.
;ecause of poor =t, they also oBer the leastprotection and
reuire constant biting down tostay in place.
-
8/16/2019 Oral Injury
35/50
35 www.aap.org/oralhealth/pact
-oil and -ite $outh ,uards
9ade of thermoplastic material that conforms to theshape of
the teeth after being placed in hot water, these mouthguards
are commercially available and the most common typeused by
athletes.
They vary in =t, comfort, and protection.
)sed with permission from *ontent +isionary
-
8/16/2019 Oral Injury
36/50
36 www.aap.org/oralhealth/pact
Custo! Fit $outh ,uards
This type of mouth guard must be made by a dentist for
theindividual.
t is the most e-pensive, but also oBers the most protection
and
comfort.
*ustom mouth guards are preferred by dentists and usually
preferred
by athletes because of their increased comfort, wearability,
and
retention, as well as ease of spea5ing when worn.
This type of mouth guard is particularly important for
adolescents
with orthodontic appliances.
-
8/16/2019 Oral Injury
37/50
37 www.aap.org/oralhealth/pact
Reco!!endations 'or $outh ,uards
The merican cademy of 1ediatric Dentistry!1D$ recommends
properly =tted mouth
guards for all children participating in organi2edand
unorgani2ed contact and collision sports.
The 1D supports mandated for use of athletic
mouthguards in any sporting activity containinga ris5 of
orofacial injury.
-
8/16/2019 Oral Injury
38/50
38 www.aap.org/oralhealth/pact
.uestion /0
1hich teeth are !ost co!!only a2ected by oralinjury3
. *entral ma-illary incisors
;. *entral mandibular incisors
*. *anines
D. 9olars
>. There is no common pattern to oral injuries
-
8/16/2019 Oral Injury
39/50
39 www.aap.org/oralhealth/pact
Ans"er
1hich teeth are !ost co!!only a2ected by oralinjury3
. *entral ma-illary incisors
;. *entral mandibular incisors
*. *anines
D. 9olars
>. There is no common pattern to oral injuries
-
8/16/2019 Oral Injury
40/50
40 www.aap.org/oralhealth/pact
.uestion /4
1hich o' the 'ollo"ing is not a risk 'actor 'or oraltrau!a3
. 9alocclusion
;. *hild abuse or neglect
*. >arly childhood caries
D. 8yperactivity
>. ubstance abuse within the family
-
8/16/2019 Oral Injury
41/50
41 www.aap.org/oralhealth/pact
Ans"er
1hich o' the 'ollo"ing is not a risk 'actor 'or oraltrau!a3
. 9alocclusion
;. *hild abuse or neglect
*. >arly childhood caries
D. 8yperactivity
>. ubstance abuse within the family
-
8/16/2019 Oral Injury
42/50
42 www.aap.org/oralhealth/pact
.uestion /5
1hich o' the 'ollo"ing is !ost likely 'ollo"ing intrusiono'
a
&ri!ary toothN
. ?oot resorption
;. ?eeruption of the primary tooth
*. 1ulpal necrosis with possible root infection
D. :racture of the underlying permanent tooth>. Damage to the
underlying tooth and failure of permanenttooth to
erupt
-
8/16/2019 Oral Injury
43/50
43 www.aap.org/oralhealth/pact
Ans"er
1hich o' the 'ollo"ing is !ost likely 'ollo"ing intrusiono'
a
&ri!ary toothN
. ?oot resorption
;. ?eeruption of the primary tooth
*. 1ulpal necrosis with possible root infection
D. :racture of the underlying permanent tooth>. Damage to the
underlying tooth and failure of permanenttooth to
erupt
-
8/16/2019 Oral Injury
44/50
44 www.aap.org/oralhealth/pact
.uestion /6
1hich o' the 'ollo"ing is the &ro&er !anage!ent o'
anavulsed &ri!ary tooth3
. The tooth should not be reinserted
;. The tooth should be transported in mil5 and the child rushed
to a
dentist or >? for reinsertion
*. The tooth should be transported in water and the child rushed
toa
dentist or >? for reinsertion
D. t should be reinserted immediately
>. Kone of the above
-
8/16/2019 Oral Injury
45/50
45 www.aap.org/oralhealth/pact
.uestion /6
1hich o' the 'ollo"ing is the &ro&er !anage!ent o' an
avulsed
&ri!ary tooth3
. The tooth should not be reinserted
;. The tooth should be transported in mil5 and the child rushed
to adentist
or >? for reinsertion
*. The tooth should be transported in water and the child rushed
to a
dentistor >? for reinsertion
D. t should be reinserted immediately
>. Kone of the above
-
8/16/2019 Oral Injury
46/50
46 www.aap.org/oralhealth/pact
.uestion /7
1hich o' the 'ollo"ing is a conse+uence o' oralinjury3
. 8igh cost
;. mpaired oral or phonetic function
*. 1ain
D. nfection, including abscess
>. ll of the above
-
8/16/2019 Oral Injury
47/50
47 www.aap.org/oralhealth/pact
Ans"er
1hich o' the 'ollo"ing is a conse+uence o' oralinjury3
. 8igh cost
;. mpaired oral or phonetic function
*. 1ain
D. nfection, including abscess
>. ll of the above
-
8/16/2019 Oral Injury
48/50
48 www.aap.org/oralhealth/pact
Re'erences
#. merican cademy of 1ediatric Dentistry. Decision Tree for an
vulsed Tooth. ?esource ection, pg '3. vailable online
at(http(//www.aapd.org/media/policiesOguidelines/
rsOtrauma6owsheet.pdf.
ccessed 9ay '4, '0#'.'. merican cademy of 1ediatric Dentistry.
1revention of ports?elatednjuries. #PPP. pg. 3". vailable online
at(http(//www.aapd.org/pdf/sports.pdf. ccessed Qanuary #4, '00.
3. merican cademy of 1ediatric Dentistry *ouncil on *linical
Bairs.Ruideline on 9anagement of cute Dental traumaG ?eference
9anualGrevised '00@( #34#@0. vailable online at(
http(//www.aapd.org/media/1oliciesORuidelines/ROTrauma.pdf.
ccessed Qanuary #4, '00.
@. merican cademy of 1ediatric Dentistry *ouncil on *linical
Bairs1olicy on 1revention of portsrelated &rofacial njuries.
revised '00, pg(@"40. vailable online
at(http(//www.aapd.org/media/policiesOguidelines/pOsports.pdf.
ccessed Qanuary #4, '00.
-
8/16/2019 Oral Injury
49/50
49 www.aap.org/oralhealth/pact
Re'erences# continued
4. merican cademy of 1ediatrics( njuries ssociated Jith
nfantJal5ers. *ommittee on njury and 1oison 1revention. Pediatrics.
'00#G#0"!3$( P0P'. vailable online at(
http(//pediatrics.aappublications.org/cgi/content/full/#0"/3/P0.ccessed
Qanuary #4, '00.
. merican cademy of 1ediatrics( Trampolines at 8ome, chool,
and?ecreational *enters. *ommittee on njury and 1oison 1revention
and*ommittee on ports 9edicine and :itness. Pediatrics. #PPPG
#03!4$(#043#04. vailable online at(
http(//pediatrics.aappublications.org/cgi/content/full/#03/4/#043.
ccessed Qanuary #4, '00.
. *ohen , ;urns ?*. 1athways of the 1ulp. >ighth edition.
". *onference on ports njuries in South. ;ethesda, 9D(
Kationalnstitutes of 8ealthG #PP'. K8 1ublication Ko P33@@@.
P. 8ergenroeder *. 1revention of ports njuries. Pediatrics.
#PP"G#0#!$( #04#03.
-
8/16/2019 Oral Injury
50/50
Re'erences# continued
#0. 8su , Rroleau R. Tetanus in the >mergency Department(
*urrent?eview. Journal of Emergency Medicine. '00#G
'0!@$(344.##. Kewsome 1?, Tran D*, *oo5e 9. The role of the
mouthguard in the
prevention of sportsrelated dental injuries( a review. Int J
Paediatr Dent .'00#G ##!$(3P@0@.
#'. 1rotecting Teeth with 9outh guards. 1atient nformation
1amphlet. JADA. '00G +ol. #3( #'. vailable online
at(http(//www.ada.org/prof/resources/pubs/jada/patient/patientOP.pdf.ccessed
Qanuary #4, '00.
#3. The ociety of Teachers of :amily 9edicine Rroup on &ral
8ealth.miles for life( national oral health curriculum for family
medicine.'00. www/smilesforlifeoralhealth.org. ccessed Qune @,
'0#'.#@. ) Department of 8ealth and 8uman ervices. &ral health
inmerica( ?eport of the urgeon Reneral. ?oc5ville 9D( )
Departmentof 8ealth and 8uman ervices, Kational nstitute of Dental
and*raniofacial ?esearch, Kational nstitutes of 8ealthG '000.
vailableonline at( http(//www.nidcr.nih.gov/
Datatatistics/urgeonReneral.