-
Acta Derm Venereol 2011 ; 91: 704-707
CLINICAL REPORT
Oral Lesion in Leprosy: Borderline Tuberculoid Diagnosis Basedon
Detection of Mycobacterium leprae DNA by qPCRTalita DA SILVA
MARTINEZ', Andr A. NAHASS Mrcia M.N.R FIGUEIRA\ Adeilson V. COSTA',
Maria A. GONALVES', LuizR. GOULART'^ and Isabela M.B. GOULART'
^'National Reference Center in Sanitary Dermatology and Leprosy,
Hospital das Clinicas, 'Graduate Program of Health Sciences, School
of Medicine, Fe-deral University of Uberlndia, 'University Center
of Triangulo-UNITRI, Brazil, and'Department of Medical Microbiology
and Immunology, Universityof California. Davis, USA
Oral lesions are rarely reported in paucibacillary formsof
leprosy. We report here a case with an erythematoushyposensitive
lesion in the palate and no skin lesions.In addition to routine
tests, biopsies of the lesion in thepalate and of clinically normal
surrounding areas wereperformed and subjected to real-time PCR for
detectionof Mycobacterium leprae DNA. The biopsy of the oral
le-sion was positive for bacilli DNA, followed by positiveserum
anti-PGL-1 and Mitsuda test, but with negativehistopathology. The
patient was diagnosed with a bor-derline tuberculoid form. After
multidrug therapy thelesion had significantly regressed and the
bacilli DNAdetection in the former lesion was negative. The
bacilliDNA detection in an oral lesion by real-time PCR notonly
improved leprosy diagnosis, but also helped in theclassification of
clinical form, and in the establishment ofthe appropriate
therapeutic regime. Key words: leprosy;Mycobacterium leprae;
diagnosis; PCR; mouth mucosa.
(Accepted April 4, 2011.)Acta Derm Venereol 2011; 91:
704-707.
Talita da Silva Martinez, National Reference Center inSanitary
Dermatology and Leprosy, Av. Aspirante Mega,77, Bairro Jaragu,
38413-018 Uberlndia/MG, Brazil.E-mail: ttalittasm(^yahoo.com.br
Leprosy, an infectious disease caused by Mycobacteriumleprae, is
a relevant public health issue in Brazil, whichhas the second
highest prevalence worldwide, with37,610 new cases detected in 2009
(1).
An operational classification distinguishes multibacil-lary (MB)
from paucibacillary (PB) forms of leprosy,according to the
bacterial index (BI) and the number oflesions (2); for clinical
form classification, Mitsuda'stest and PGL-1 antibody testing are
reported in additionto the BI (3).
As a result of effective antimicrobial therapy, advan-ced
lesions of the face, nasopharynx and oropharynx arenow rarely seen,
but the presenting signs and symptomsof leprosy still arise
occasionally in the nasal and oralmucosa (4). A case of oral lesion
associated with leprosyhas been described elsewhere in a borderline
tuberculoid
Ada Derm Venereol 91
(BT)-MB patient with papulo-nodular lesions in thecentre of the
hard palate, by histopathological findings(5). However, oral mucosa
lesions are not normallyfound in PB patients (5, 6), and when they
are present,manifestations have been described exclusively in
thetuberculoid and borderline forms in the reactional state,with
few scientific studies and poorly characterizeddescriptions
(7).
Oral lesions of leprosy occur more frequently in areasof the
mouth with a lower surface temperature (8). Themain oral cavify
sites of leprosy include the gingivalin the anterior portion of the
maxilla, the hard and softpalate, the uvula and the tongue (9).
An earlier study detected M leprae DNA by PCRin oral mucosa
samples of patients with MB forms ofleprosy (10), but literature is
scarce regarding detectionof bacilli DNA in PB leprosy forms.
MATERIAL AND METHODSMitsuda's intradermal tests for evaluation
of the cellular im-mune response to M. leprae, and the serum
enzyme-linkedimmunoassay (ELISA) that evaluates the response of
IgMantibodies against the PGL-1 bacillus antigen were
performed,together with M leprae DNA detection in nasal swab,
buccalswab, dermal swabs, peripheral blood, biopsies of the
inferiornasal turbinate and of the sensory nerve, a research
protocoladopted at CREDESH under the UFU Ethics Committee appro-val
number 499/2008.
Real-time PCR (qPCR) was performed for M. leprae DNAdetection in
all samples. The set of primers and probe
(sense5'-TGACATGAATACGCAAGGGGCAGGA-3';
antisense5'-TCATCTCCTGCACCCCGA-3'; probe TaqMan
5'-CACA-TAGGGTCCAGTCGTGCCGC-3') were designed to amplifyand detect
a 69-bp fragment of the ML0024 M leprae gene,a highly specific
region. The genomic region was confirmedby dideoxy sequencing,
which aligned only with the M. lepraegenome in a Basic Local
Alignment Search Tool (BLAST)search (www.ncbi.nlm.nih.gov/BLAST).
The sensitivity ofthe biomarker was close to 60%, detecting all BB,
BL and LLclinical forms. Other Mycobacteria spp. and negative
controlswere used, and confirmed 100% specificity. Interestingly,
ba-cilli DNA were detected by the ML0024 primers in 25% of
thepatients' samples with negative bacilloscopy.
Six-hundred nanograms of DNA (4 ni) from clinical sampleswere
used in a 25-nl PCR reaction, which consisted of 2x Taq-Man
Universal PCR Master Mix (Applied Biosystems), 200 nMeach primer,
and 100 nM probe. The PCR reactions were carriedout at 50C for 2
min, 95C for 10 min, followed by 40 cycles
o 2011 The Authors, doi-. 10.2340/00015555-1175Journal
Compilation O 2011 Acta Dermato-Venereologica. ISSN 0001-5555
-
of 95C for 15 s and 60C for 1 min. All tissues were
weighedbefore DNA extraction to allow the absolute quantification
permilligram of hiopsied tissues. The absolute quantification of
eachDNA sample was calculated based on a standard curve
construc-ted for the gene. All samples were run in triplicate.
ELISA followed the procedures described elsewhere (11).Briefly,
microtitre plates (Maxisorp, NUNC, Rochester, NY,USA) were coated
with 50 nl native PGL-I diluted in absoluteethyl alcohol at a
concentration of 10 ng/ml. Serum sampleswere added in duplicate
using a dilution of 1:100 (native PGL-I) in phosphate buffered
saline/bovine serum albumin (PBS/BSA) 1%, and incuhated for 1 h at
37C, followed by washing.The anti-human IgM-peroxidase conjugate
(Sigma ChemicalCo., St Louis, MO, USA) was added to the plates at a
dilutionof 1:10,000 (PGL-I ELISA) in PBS/BSA 1%. The
suhstrateo-phenylenediamine dihydrochloride (OPD,
Sigma-Aldrich,Inc., St Louis, MO, USA) enzyme suhstrate was added
to theplates and incuhated at room temperature for 10 min in the
dark.The reaction was stopped hy the addition of 25 |jl H S^O^
4N.The optical density (OD) was obtained in a microplate
reader(Thermo Plate, TP-Reader, Rayto Life and Analytical
SciencesC. Ltd, Germany) at 492 nm. Two positive and three
negativecontrols were included in each plate. The cut-off level for
posi-tivity was a standard deviation above the mean OD obtained
forthe three negative controls. The antihody titres were
expressedas the ELISA index (El) according to the following
formula:^ ' " O s^ampie^ OD^^ ,^ ^ in whch the cut-off point was
determinedhy the mean OD of the negative controls plus 3 standard
devia-tions. Values of El > 1.1 were considered positive.
CASE REPORT
A 46-year-old Brazilian woman attended the NationalReference
Center in Leprosy and Sanitary Dermatology(CREDESH), of the
Hospital das Clnicas, at the Fede-ral University of Uberlndia, in
January 2009, referredby her neurologist physician, presenting
hypoesthesiaat the bottom of the right foot, high-stepping gait
andan electroneuromyography demonstrating an axonalmononeuropathy
with moderate to severe intensity ofthe right peroneal nerve,
leading to suspicious leprosy.Although the referred patient had no
known contactwith other patients, it is worth noting that this is
an
Leprosy diagnosis by qPCR in oral lesion 705
endemic region for leprosy, and that the possible sourceof
transmission could not be determined. Clinical eva-luation did not
reveal any skin lesions in any part ofthe patient's body, but did
present an important hypo-esthesia and pain at the bottom of the
right foot, andparesis due to difficulty dorsiflexing the right
foot, inthe region innervated by the right fibular.
For diagnosis, BI of dermal swabs was performed,collected at
seven skin sites of the patient (two earlobes, two elbows, two
knees and a suspected area atthe bottom of the right foot) as well
as a biopsy of theintermediate cutaneous branch of the right
superficialfibular nerve during surgical decompression of the
rightcommon fibular, due to impairment of this nerve, withswelling
and tenderness, associated with sensory lossand muscle paresis.
Other laboratory tests, such as liver and kidney func-tion,
blood sugar, thyroid hormones, antinuclear anti-bodies (ANA),
rheumatoid factor (RF) and urinalysis,were requested to rule out
other causes of neuropathies,including autoimmune diseases and
metabolic disorders.These tests were all negative.
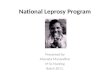
During the intraoral examination, a hypoesthesicerythematous
lesion was observed, without elevatedborders, in the region of the
right hard palate, involvingthe medial line, of approximately 2.0
cm diameter (Fig.lA). Biopsies were collected from the lesion and
fromthe clinically normal adjacent region (control), sparingthe
central region of the lesion in order to avoid the areaof the
greater palatine nerve.
The ELISA anti-PGL-1 serum test was positive, withan El of 2.37.
The Mitsuda test was strongly positive,with a 10 mm-diameter
nodule. BI and qPCR were nega-tive in all the dermal swabs samples,
nerve and inferiornasal turbinate biopsies, buccal swab, nasal
swab, andperipheral blood. The histopathological examinationof
nerve biopsy for the cutaneous branch through theright superficial
peroneal nerve showed no inflammatoryprocess of the neural tissue
fragment and presented
Fig 1. Lesion before and after multidrug therapy. (A)
Erythematous lesion of the hard palate involving the midline. (B)
Regression of the hard palatelesion.
Ada Derm Venereol 91
-
706 T. da Silva Martinez et al.
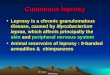
negative acid-fast bacilli by Ziehl-Neelsen staining.The buccal
lesion biopsy of the hard palate displayednegative bacilloscopy,
without apparent pathologicalchanges (Fig. 2); however, the qPCR
presented anamplification curve of the bacillus DNA and
detected1,126 copies of the M leprae DNA per mg of biopsiedtissue.
The clinically healthy mucosa of the hard palatehad negative
results, both in the histopathological andthe qPCR tests.
The possibility of contamination of the sample fromthe buccal
mucosa lesion was excluded with the undis-puted demonstration that
qPCR for the detection of Mleprae DNA was negative in the
clinically healthy areaadjacent to the lesion, in the buccal swab,
the nasalswab, the blood, and the biopsy of the nasal turbinate,a
fact that precludes any possibilify of contaminationby saliva,
nasal secretion and/or blood at the site as aresult of the invasive
biopsy procedure. Furthermore,the biopsy was split into three
samples, which weresubmitted to normal extraction protocols with
the othersampling replications prior to PCR reactions.
Considering the positive ELISA for serum PGL-1, thestrong
positive Mitsuda test, and the positive PCR resultin the oral
lesion, the patient was classified as borderlinetuberculoid, a PB
leprosy form, and received multidrugtherapy (MDT) for 6 months,
with a daily dose of 100mg dapsone, and a monthly dose of 600 mg
rifampicin.Successful treatment was evidenced by the regressionof
the hard palate lesion after the treatment (Fig. IB),by reversed
results of qPCR with total absence of Mleprae DNA (negative), and
by the reduction in El from2.37 to 1.16 (normal liii and eosin
(H&Ex400) showed palatal fragment, showing the deep portion of
the epithelial tissue lining and lamina propria of the mucosa. The
lamina propria consists ofconnective tissue, not modelled,
evidencing collagen bundles of various thicknesses and areas of
neurovascular structures with common aspects of normality.At depth,
there is fatty tissue in the sub-mucosa without apparent
pathological changes. (B) and (C) Magnified view of the
vascular-neural structures observedin the lamina propria and
submucosal tissue (H&E x 400).
Acta Derm lenereot 91
-
Leprosy diagnosis by qPCR in oral lesion IQl
at the site as a result of the invasive biopsy
procedure.Furthermore, the use of qPCR, with two primers andone
intemal probe, avoids excessive manipulation ofthe sample, and
supports a highly sensitive and specificdetection system.
Even though the histopathological examination inthis clinical
case did not suggest or provide evidencefor the disease, the
diagnosis of borderline tuberculoidleprosy was determined by
detection of the bacilli DNAin the oral lesion, which was supported
by other indirectevidence, such as: positive ELISA (meaning
subclinicalinfection, once only 22% of patients with PB present
po-sitive ELISA), positive Mitsuda (commonly detected
inpaucibacillary patients that present a cellular response),and
resolution of disease symptoms and oral lesion afierMDT, with
absence of DNA post-treatment.
Our results demonstrated the great relevance of theqPCR
detection system in oral samples of PB patients,which may be used
not only for leprosy diagnosis, butalso for clinical
classification, especially for the limitedsensitivity and
specificity of the conventional diagnostictools (18).
ACKNOWLEDGEMENTSThe authors thank all the staff of the National
Reference Centerin Sanitary Dermatology and Leprosy for fundamental
support,FAPEMIG/CNPq/CAPES/FINEP and Ministry of Health
forfinancial support, and the Integrated Laboratory of Biologyand
Oral Pathology (LIBIPO) of the Federal University ofUberlndia for
the histopathological analysis.
REFERENCES
1. WHO (World Health Organization). Global Leprosy Situa-tion,
2010. Weekly Epid Rec 2010; 85: 337-348.
2. WHO (World Health Organization). Expert committeeon leprosy
sixth report. World Health Org Tech Rep Ser1988; 768.
3. Teixeira AC, Cmvinel DL, Roma FR, Luppino LF, ResendeLH,
Sousa T, et al. Evaluation of the agreement betweenclinical and
laboratorial exams in the diagnosis of leprosy.Rev Soc Bras Med
Trop 2008; 41: 48-55.
4. Scollard DM, Skinsnes OK, 1999. Oropharyngeal leprosy inart,
history, and medicine. Oral Surg Oral Med Oral PatholOral Radiol
Endod 1999; 87: 463^70.
5. Ghosh S, Gadda Rohit-Bhailal, Vengal M, Pai KM, Ba-lachandran
C, Rao R, et al. Oro-facial aspects of leprosy:report of two cases
with literature review. Med Oral PatolOral Cir Bucal 2010; 15:
459^62.
6. De Abreu MA, Alchome MM, Michalany NS, Weckx LL,Pimentel DR,
Hirata CH. The oral mucosa in paucibacillaryleprosy: a clinical and
histopathological study. Oral Surg OralMed Oral Pathol Oral Radiol
Endod 2007; 103: 48-52.
7. Opromolla DVA, Opromolla MA, Somei U. [Dimorphouslesions in
oral cavity]. Hans Int 2003; 28: 151-155 (inPortuguese).
8. Rendall JR, McDougall AC, Willis LA. Intra-oral tempe-ratures
in man with special reference to involvement ofthe central incisors
and premaxillary alveolar process inlepromatous leprosy. Int J Lepr
Other Mycobact Dis 1976;44: 462-468.
9. Bucci F Jr, Mesa M, Schwartz RA, McNeil G, LambertWC. Oral
lesions in lepromatous leprosy. J Oral Med 1987-42: 4-6.
10. Santos GG, Marcucci G, Guimaraes Junior J, MargaridoLC,
Lopes LHC. [Molecular detection of Mycobacteriumleprae by
polymerase chain reaction in oral mucosal biopsyspecimens]. An Bras
Dermatol 2007; 82: 245-249 (inPortuguese).
11. Lobato J, Silva DA, Mineo TW, Amaral JD, Segundo
GR,Costa-Cruz JM, et al. Detection of immunoglobulin G anti-bodies
to Neospora caninum in humans: high seropositivityrates in patients
who are infected by human immunodefi-ciency virus or have
neurological disorders. Clin VaccineImmunol 2006; 13: 84-89.
12. Goulart 1MB, Goulart LR. Leprosy: diagnostic and
controlchallenges for a worldwide disease. Arch Dermatol Res2008;
300: 269-290.
13. Patrocinio LG, Goulart 1MB, Goulart LR, Patrocinio
JA,Ferreira FR, Fleury RN. Detection of Mycobacterium lepraein
nasal mucosa biopsies by the polymerase chain reaction.FEMS Immunol
Med Mic 2005; 44: 311-316.
14. Naves MM, Patrocinio LG, Patrocinio JA, Mota FMN,Souza AD,
Fleury RN, et al. Contribution of nasal biopsyto leprosy diagnosis.
Am J Rhinol Allergy 2009- 23-177-180.
15. Scheepers A, Lemmer J, Lownie JF. Oral manifestations
ofleprosy. Lep Rev 1993; 64: 37^3 .
16. Brand PW. Temperature variation and leprosy deformityInt J
Lep 1959; 27: 1-7.
17. Girdhar BK, Desikan KV. A clinical study of the mouth
inuntreated lepromatous patients. Lepr Rev 1979; 50: 25-35.
18. Goulart 1MB, Cardoso AM, Santos MS, Gonalves MA,Pereira JE,
Goulart LR. Detection of Mycobacterium le-prae DNA in skin lesions
of leprosy patients by PCR maybe affected by amplicon size. Arch
Dermatol Res 2007'299:267-271.
Acta Derm Venereol 91
-
Copyright of Acta Dermato-Venereologica is the property of
Society for Publication of Acta Dermato-Venereologica and its
content may not be copied or emailed to multiple sites or posted to
a listserv without thecopyright holder's express written
permission. However, users may print, download, or email articles
forindividual use.