Embed Size (px)
Citation preview

PEDIATRIC ANNALS 42:1 | JANUARY 2013 Healio.com/Pediatrics | 31
FEATURE
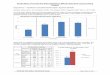
According to current statistics from the US Centers for Dis-ease Control and Prevention,
39.9% of adolescents surveyed have used organic cannabinoids at least once and 23.1% have used it regularly within the last month.1 These statistics show a 3.1% increase from the survey results in 2009. Similar data show that 11.4% of US 12th graders have used “Spice” or “K2” (brand names of synthetic can-nabinoids) in the past year, making synthetic cannabinoids the second most commonly used illicit drug among high school seniors.2
In the Monitoring the Future Sur-vey 2011, data tabulated on drug use in 8th, 10th, and 12th graders, found that
organic cannabinoid use among teens rose (ie, 0.6 %) in 2011, showing an in-crease for the fourth straight year. This is in contrast to the decline that had oc-curred in the preceding decade. It also found that daily organic marijuana use is now at a 30-year peak level among high school seniors.3
Recent trends indicate a decrease in perception of harm from cannabinoids in addition to a decrease in disapproval of use by older peers may be leading to the upswing of cannabinoid use over the past few years.3 Other risk factors, including pre-existing conditions or comorbidities such as mood and anxi-
Organic and Synthetic Cannabinoid Use in AdolescentsSanaa Bhatty, MD; and Wendell Wu, MD
Sanaa Bhatty, MD, is a PGY- II Resident Physi-
cian, Department of Psychiatry and Behavioral
Sciences, The George Washington University
Medical Center. Wendell Wu, MD, is Medical Stu-
dent Clerkship Director, Department of Psychia-
try and Behavioral Sciences, The Children’s Na-
tional Medical Center.Address correspondence to: Sanaa Bhatty, MD,
Department of Psychiatry and Behavioral Scienc-es, The George Washington University Medical Center, 2120 L Street, NW, Suite 600, Washington, DC 20037; fax: 202-741-2891; email: [email protected].
Disclosure: The authors have no relevant fi-nancial relationships to disclose.
doi: 10.3928/00904481-20121221-16 © S
hutte
rsto
ck

32 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:1 | JANUARY 2013
FEATURE
ety disorders, may also play a role.4
With the increased potency of can-nabinoids in both organic marijuana and newer classes of synthetic cannabi-noid compounds, the issue of cannabi-noid abuse likely will become a greater challenge. The purpose of this article is to help the primary care pediatrician understand the nuances, changes, and current complexities of cannabinoid abuse, and how to treat its abuse and possible dependence.
DEFINITIONS/LEGAL STATUSOrganic cannabinoids (ie, marijuana)
are dried flower remnants of Canna-bis sativa. Although Cannabis species can contain more than 60 cannabinoids (which are aryl-substituted meroter-penes), the most potent and psychoac-tive cannabinoid is delta-9-tetrahydro-cannabinol, known as THC. Marijuana can be smoked in a “joint” or self-made cigarette, in pipes, or in “bongs” (ie, by inhaling smoke from an air- and water-tight vessel). It can be eaten or baked into foods via extracting THC into butter or oil, as it is quite fat-soluble.
Advances in cultivation (such as hy-droponic farming and plant-breeding) have also increased the potency of mari-juana. In the 1960s and 1970s, the aver-age marijuana joint contained about 10 mg of THC. Now, a joint may contain as much as 150 mg of THC. Thus, marijua-na in current circulation puts users at risk of exposure to greater quantities of THC, greater intoxication, and potentially lon-ger-term risks than in prior generations.5
Synthetic cannabinoids are nonor-ganic cannabinoids that are synthe-sized and sprayed onto dried herbs or concentrated into powder forms. These are then advertised and sold as incense products. Common brand names in-clude “Spice,” “K2,” “Genie,” and “Aroma,” and they are sold in “head shops” (ie, stores that sell parapher-nalia for tobacco and cannabis users), convenience stores, or over the Inter-
net. They are labeled as “not for human consumption,” but are used in ways similar to marijuana or through insuf-flation for psychoactive effects similar to THC. Although they do not contain THC, they include other cannabinoids and other unknown substances.
Synthetic cannabinoids have been banned throughout the developed world, including the US. The first syn-thetic cannabinoid was made in 1995
by a Clemson University professor. Following the publication of a paper detailing the experiment, including the description of the method and in-gredients required, the cannabinoids first appeared in the European “party scene” before becoming more com-monly known and used.6 Unfortunately, as cannabinoids are often altered to avoid federal regulations and bans, new cannabinoids are frequently being cre-ated. Currently, there are more than 100 compounds with cannabinoid-like ac-tivities waiting for identification.7
Organic cannabinoids are Schedule I substances in the US and are illegal if found in possession.8 Eighteen states and the District of Columbia have also legalized medical cannabis or essential-ly decriminalized it.9 In 2011, the Drug Enforcement Administration (DEA) temporarily banned five synthetic can-nabinoids: JWH-018; JWH-073; JWH-200; CP-47,497; and CP-47,497-C8. This ban, effective for at least 2 years, makes this class of drugs Schedule I. However, as mentioned earlier, new cannabinoids can be made by altering the original molecules, and thus can ef-fectively bypass the ban.
USE, ABUSE, AND DEPENDENCEOrganic cannabinoid intoxication is
described as euphoria, anxiety, the sen-sation of slowed time, impaired motor coordination, and/or social withdrawal that develops during or shortly after use. Physiologic symptoms such as con-junctival injection, increased appetite, dry mouth, and tachycardia, can occur within 2 hours of use.10 According to the Diagnostic and Statistical Manual-IV-Text Revision (DSM-IV-TR), mari-juana abuse is defined as a maladaptive pattern of use leading to clinically sig-nificant impairment or distress during a 12-month period, manifested either by recurrent use that interferes with ma-jor role obligations at work, school, or home; occurs in situations in which it is physically hazardous; results in legal problems related to use; or persistently occurs despite continued social or in-terpersonal problems caused or exacer-bated by the effects of the use.10
In addition, the above criteria re-quire that the symptoms mentioned must have never met criteria for mari-juana dependence.
Organic marijuana has increased in potency and is more likely to build tolerance in its users, possibly result-ing in increased withdrawal symptoms. Thus, marijuana dependence is likely to be a bigger issue now than it has been in the past. According to the DSM-IV-TR, marijuana dependence is defined as a maladaptive pattern of use result-ing in clinically significant impairment or distress in a 12-month period with three symptoms that signify tolerance, including the use of markedly increased amounts of marijuana to achieve the de-sired effect or intoxication; markedly diminished effect with continued use of the same amount of marijuana; and mar-ijuana being used in larger amounts or over a longer period than was intended.
Symptoms also include a persistent desire and unsuccessful efforts to cut down or control use, and spending a
Marijuana dependence is likely to be a bigger issue now than it has
been in the past.

PEDIATRIC ANNALS 42:1 | JANUARY 2013 Healio.com/Pediatrics | 33
FEATURE
great deal of time in obtaining mari-juana, using it, or recovering from its effects. The last two symptoms are the neglect of important social, occu-pational, or recreational activities due to use; and the persistent use despite knowledge of having a recurrent or on-going physical or psychological prob-lem that is probably caused or exacer-bated by use.10
The DSM-IV-TR criteria for mari-juana dependence only includes physi-ologic tolerance and does not specify a withdrawal period.11 However, cur-rent data suggests a withdrawal period does exist. A US epidemiologic survey found that among frequent marijuana users who did not use other substances, 44% reported two or more withdrawal symptoms and 34% reported three or more symptoms when discontinuation of use.12 The most prevalent withdrawal symptoms included fatigue, hypersom-nia, psychomotor retardation, anxiety, depression, and yawning.12
Although withdrawal can be dis-tressing, it is not life-threatening. The withdrawal syndrome begins the day or so after cessation, peaks between days 2 and 6, and resolves within 1 to 2 weeks. Other symptoms such as sleep disturbances and irritability might con-tinue to persist for weeks.13 This may be due to THC being highly lipophilic and redistributing quickly into body fat. The high lipid storage of THC increas-es its elimination half-life and may immediately diminish the severity of withdrawal symptoms, while possibly extending their duration.11
There is a lack of DSM-IV-TR crite-ria for synthetic marijuana intoxication, abuse, or dependence. Synthetic mari-juana intoxication has been reported to lead to symptoms of conjunctival injection, tachycardia, anxiety, aggres-sive behavior, paranoia, hallucinations, inability to speak, dystonia, and short-term memory deficits.14 There also are case reports that demonstrate a with-
drawal syndrome and thus a level of tol-erance from synthetic marijuana use.7
The recently approved and yet to be published Diagnostic and Statistical Manual 5 (DSM-5) will make signifi-cant overhauls to the category of sub-stance use disorders. Per the American Psychiatric Association, the DSM-5 will combine the DSM-IV-TR catego-ries of substance abuse and substance dependence. The belief is that by com-bining criteria, the diagnoses will be strengthened and more accurate. For example, previous substance abuse cri-teria required only one symptom while the DSM-5’s mild substance use dis-order will require two to three symp-toms.15 In addition, it is postulated that the DSM-5 will acknowledge cannabis withdrawal.16 Currently, it is unknown if synthetic marijuana will be discussed in the DSM-5.
RISKS OF USEIndividual risks of cannabinoid use
fall into both physical and psychologi-cal domains. As organic marijuana has been available and used for much lon-ger than synthetic cannabinoids, con-siderably more is known about the ef-fects of its use.
In the physical domain, certain dis-ease processes have been looked at in greater detail. In terms of pulmonary medical risks, there was found to be no association between long-term mari-juana smoking and airflow obstruction measures.17 However, it has been noted that long-term marijuana smoking was associated with increased respiratory symptoms, including cough, phlegm, and wheezing.17 In terms of cancer risk, a 2005 review of epidemiologic studies concluded that there were not sufficient studies available to adequately evaluate the effect of marijuana use on cancer.18
Multiple studies have demonstrated that cannabinoids affect the immune system, and there is evidence that or-ganic marijuana use appears to sup-
press aspects of immunological func-tion. However, it is unclear whether this suppression results in any in-creased rates of disease.19 Lastly, mari-juana smoking is implicated in having an increased risk of periodontal disease in chronic users.2
In the psychological domain, a re-cently published study found that a pattern of persistent organic marijuana use was associated with a neuropsycho-logical decline that occurred broadly across all domains of functioning, even after controlling for years of education. Impairment was concentrated among adolescent-onset organic marijuana us-ers, with more persistent use associated with greater decline. Further, cessation of use did not fully restore neuropsy-chological functioning among adoles-cent-onset organic marijuana users.21 This negated previously held notions, which stated that there was no evidence of significant long-term effects of per-sistent organic marijuana use on neuro-cognitive processes.22
Additionally, a systematic review of longitudinal studies did not find a sig-nificantly increased risk of depression for cannabis users.23 There is one risk however, which was validated by that re-view. Marijuana use was found to show an increased risk of psychosis. This was for any type of psychotic outcome in an individual who had ever used marijuana, and the findings were consistent with a dose-response effect. There was greater risk in those who used marijuana most frequently.23 Also, according to a more recent meta-analysis, it was found that psychosis or schizophrenia-related ill-ness occurred 2.7 years earlier in those who abused marijuana. This signifies a possible causal role of marijuana in inducing psychosis or schizophrenia-related illness.24
However, there is additional evidence that indicates that a genetic predisposi-tion may influence the risk of developing psychosis in those who used marijuana

34 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:1 | JANUARY 2013
FEATURE
as adolescents. This would help explain why the majority of those who use mari-juana do not develop psychosis.25
Less is known about the long-term effects of synthetic marijuana use, giv-en its recent introduction to the public. There have been multiple reports of psychotic symptoms occurring in in-dividuals who used synthetic cannabi-noids that have occurred after the acute effects of intoxication.7 There have also been reports of two deaths in the US, one due to suicide and one due to an ischemic cardiac event.7
INTERVENTION AND TREATMENTThe first step is to screen individu-
als who have admitted to any organic or synthetic marijuana use and determine whether they meet criteria for abuse or dependence. Another option for use that is suspected, but not admitted to, is drug testing. This also is useful for monitor-ing progress for patients in treatment. Urine drug testing is the most common type of testing, as it is readily available and inexpensive. Of note, a positive urine test only establishes past use. As cannabinoid metabolites are highly li-pophilic, they can persist for extended periods of time, and urine tests for can-nabinoids can remain positive after dis-continuation of cannabis for up to 7 to 10 days in a casual user, 2 to 4 weeks in a heavy user, and months in a chronic heavy user.11
Currently, there is no widespread commercially available drug testing for synthetic cannabinoids. As mentioned earlier, synthetic cannabinoids are of-ten altered to avoid legal bans, and thus, it is difficult to test for all cannabinoids currently available. There are some so-phisticated tests for known and banned synthetic cannabinoids, such as JWH-018 and JWH-073; however, these tests are not easily available nor necessarily conclusive of use.26
Treatment for acute ingestion of organic marijuana may require plac-
ing the user in a quiet, low-stimulation environment with gentle interactions until acute effects subside. For some individuals, further symptomatic treat-ment is required with closer observa-tion and low-dose benzodiazepines or antipsychotics for sedating effects to
reduce paranoia or psychotic symptoms from acute use.27 Treatment for acute ingestion of synthetic cannabinoids is similar and may require longer-acting benzodiazepines.28 In general, acute in-gestion of either does not require medi-cal treatment; however, users may seek treatment for dysphoria, severe para-noia, or psychotic symptoms.27, 28
The standard treatment for organic marijuana abuse and/or dependence is psychotherapy. This is based on con-trolled studies proving the benefits of psychotherapy and the lack of estab-lishment of effective pharmacologi-cal treatments.27 Of note, one recent double-blind, randomized, placebo-controlled study showed some benefit of N-acetyl cysteine in producing ces-sation in adolescents with marijuana dependence (in conjunction with psy-
chotherapy); however, further studies will need to be conducted to determine its role in treatment.29
Psychotherapies that have been found to have a positive effect in organ-ic marijuana cessation include cogni-tive-behavioral therapy, family therapy, voucher-based incentives (ie, a behav-ioral therapy that uses rewards such as monetary vouchers as incentives for therapeutically desired behaviors), and motivational enhancement therapy.27 In addition, self-help groups such as Mar-ijuana Anonymous are available; how-ever, no studies have been conducted to determine their effectiveness in can-nabinoid use disorders. There are no long-term studies on the treatment for synthetic marijuana abuse at this time.
The approach to synthetic marijuana could be similar to organic marijuana because the substance effects are also similar. However, due to the variable po-tencies of synthetic marijuana, as well as its fully not yet known properties, future studies may indicate other treatments necessary to combat its effects.
In the adolescent population, pre-vention is key. A meta-analysis of four studies involving middle school students compared a school-based so-cial skills program that advocated for substance use prevention against the usual curriculum. Results showed that the program significantly reduced the use of marijuana at follow-up assess-ments.30 Thus, educating adolescents on the presence and effects of illicit substances, including organic and syn-thetic cannabinoids, may help reduce their use.
In addition, protective factors, in-cluding adequate self-control, paren-tal support and supervision, academic competence and achievement, anti-drug use policies and education, strong com-munity and neighborhood attachments, and access to health services, may also help deter from substance abuse in this vulnerable population.
Urine tests for cannabinoids can remain positive for up to 10 days
in a casual user.

PEDIATRIC ANNALS 42:1 | JANUARY 2013 Healio.com/Pediatrics | 35
FEATURE
CONCLUSIONOrganic and synthetic cannabinoid
use in the adolescent population has become increasingly prominent in the popular media. The recent rise of syn-thetic use and its lack of regulation make it a new issue and, oftentimes, one that is difficult to detect. In addi-tion, as the concentration of the active cannabinoid ingredient THC increases in organic use, the effects of marijuana abuse and/or dependence are worsened.
Evidence has shown that marijuana’s negative effects are greater on the psy-chological domain than on the physical domain. In treatment, prevention is key in the population, and this article may aid those able to educate the adolescent population of these illicit substances and their effects.
REFERENCES 1. Youth Risk Behavior Surveillance-United
States, 2011. Available at: www.cdc.gov/mmwr/pdf/ss/ss6104.pdf. Accessed Dec. 3, 2012.
2. Synthetic Drugs (a.k.a. K2, Spice, Bath Salts, etc.) Office of National Drug Control Policy. Available at: www.whitehouse.gov/ondcp/ondcp-fact-sheets/synthetic-drugs-k2-spice-bath-salts. Accessed on Dec. 3, 2012.
3. Johnston LD, O’Malley PM, Bachman JG, et al. Monitoring the future national results on adolescent drug use: Overview of key findings, 2011. Ann Arbor: Institute for So-cial Research, The University of Michigan. Available at www.monitoringthefuture.org. Accessed Dec. 3, 2012.
4. Bailey JA, Dupont RL, Teitelbaum, SA, et al. Cannabis Use Disorders: Epidemiology, Co-morbidity, and Pathogenesis. In Basow, DS (ed). UpToDate. Waltham, MA: UpToDate; 2012.
5. Ashton C. Pharmacology and effects of cannabis: a brief review. Br J Psychiatry. 2001;178:101-106.
6. Macher R, Burke T, Owen S. Synthetic Mari-juana. FBI Law Enforcement Bulletin: May
2012. Available at: www.fbi.gov/stats-ser-vices/publications/law-enforcement-bulle-tin/may-2012/synthetic-marijuana. Accessed Dec. 3, 2012.
7. Fattore L, Fratta W. Beyond THC: the new generation of cannabinoid designer drugs. Front Behav Neurosci. 2011;5:60.
8. Controlled Substance Schedules. US Depart-ment of Justice, Drug Enforcement Admin-istration. Last reviewed: September 2012. Available at: www.deadiversion.usdoj.gov/schedules/index.html. Accessed Dec. 3, 2012.
9. 18 Legal Medical Marijuana States and DC: Laws, Fees, and Possession Limits. Avail-able at: medicalmarijuana.procon.org/view.resource.php?resourceID=000881. Accessed December 3, 2012.
10. American Psychiatric Association. The Di-agnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV TR). Washington, DC: American Psychiatric Association Press; 2000.
11. DuPont JL, Bailey JA, Teitelbaum SA, et al. Cannabis use disorders: clinical features and diagnosis. In Basow, DS (ed). UpToDate. Waltham, MA: UpToDate; 2012.
12. Hasin DS, Keyes KM, Alderson D, et al. Cannabis withdrawal in the United States: results from NESARC. J Clin Psychiatry. 2008;69:9.
13. Budney AJ, Hughes JR, Moore BA, Vandrey R. Review of the validity and significance of cannabis withdrawal syndrome. Am J Psy-chiatry. 2004;(11)161.
14. Cohen J, Morrison S, Greenberg J, Saidine-jad M. Clinical presentation of intoxication due to synthetic cannabinoids. Pediatrics. 2012;129(4):e1064-e1067.
15. American Psychiatric Association. American Psychiatric Association Board of Trustees Approves DSM-5. Diagnostic manual passes major milestone before May 2013 publica-tion. [press release] Dec. 1, 2012. Available at www.psych.org. Accessed Dec. 5, 2012.
16. Curley B. DSM-V Draft includes major changes to addictive disease classifications. February 12, 2010. Available at: www.drugfree.org/join-together/addiction/dsm-v-draft-includes-major. Accessed Dec. 5, 2012.
17. Tetrault JM, Crothers K, Moore BA, et al. Effects of marijuana smoking on pulmo-nary function and respiratory complica-tions: a systematic review. Arch Intern Med. 2007;167(3):221-228.
18. Hashibe M, Straif K, Tashkin DP, et al. Epi-
demiologic review of marijuana use and can-cer risk. Alcohol. 2005;35(3):65-275.
19. Adams IB, Martin BR. Cannabis: pharma-cology and toxicology in animals and hu-mans. Addiction. 1996;91(11):1585.
20. Thomson W, Poulton R, Broadbent JM, et al. Cannabis smoking and periodon-tal disease among young adults. JAMA. 2008;299(5):525-531.
21. Meier MH, Caspi A, Ambler A, et al. Persis-tent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012; 109(40):2657-2664.
22. Grant I, Gonzalez R, Carey CL, et al. Non-acute (residual) neurocognitive effects of cannabis use: a meta-analytic study. J Int Neuropsychol. 2003;9:679-89.
23. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or af-fective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328.
24. Large M, Sharma S, Compton MT, et al. Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Arch Gen Psy-chiatry. 2011;68(6):555.
25. Caspi A, Moffitt TE, Cannon M, et al. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evi-dence of a gene x environment interaction. Biol Psychiatry. 2005;57(10):1117-1127.
26. Castellanos D, Thornton, G. Synthetic can-nabinoid use: recognition and management. J Psychiatr Pract. 2012;18(2):86-93.
27. Teitelbaum SA, DuPont RL, Bailey JA, et al. Cannabis use disorders: treatment, prog-nosis, and long-term medical effects. In: Basow, DS (ed). UpToDate. Waltham, MA: UpToDate; 2012.
28. Hoecker CC, Ewald MB, Wiley JF. Designer drugs of abuse in children and adolescents. In: Basow, DS (ed). UpToDate. Waltham, MA: UpToDate; 2012.
29. Gray KM, Carpenter MJ, Baker NL, et al. A double-blind randomized controlled trial of N-acetylcysteine in cannabis-dependent adolescents. Am J Psychiatry. 2012;169:805-812.
30. Faggiano F, Vigna-Taglianti F, Versino E, et al. School-based prevention for illicit drugs’ use. Cochrane Database of Systematic Re-views. 2005. Available at: onlinelibrary.wi-ley.com/doi/10.1002/14651858.CD003020.pub2/full. Accessed Dec. 3, 2012.