Embed Size (px)
Citation preview
Organizational change:
challenges to infection
prevention and stewardship Dr Mike Cooper
Consultant Microbiologist and Director of Infection Prevention and Control, Royal Wolverhampton NHS
Trust, UK
Organizational Change
• Change is:
– inevitable
– necessary
• Change management
– (?)essential
Organizational Change
• Challenges for infection prevention and
antimicrobial stewardship:
– how to successfully implement change to
produce improvement?
– how to not become the victim of change?
Organizational Change
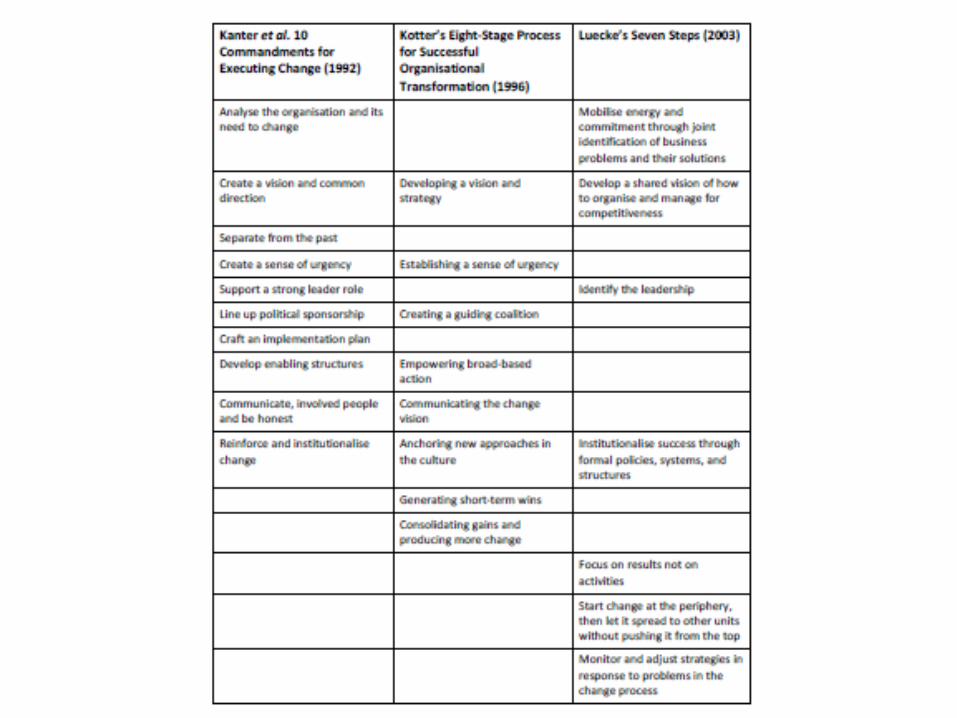
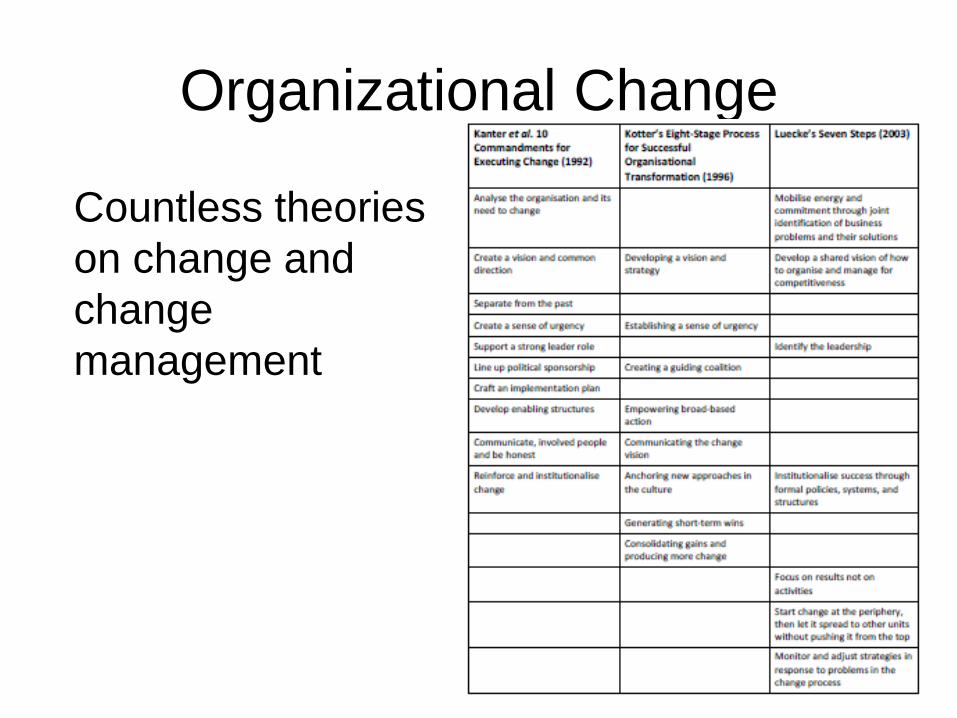
Countless theories on change and change
management:
• Examples:
– Kanter’s 10 Commandments for Executing
Change (1992)
– Kotter’s Eight-Stage Process for Successful
Organisational Transformation (1996)
– Luecke’s Seven Steps (2003)

Organizational Change
• Situation in healthcare similar to manufacturing industries in the 1980s: – competitive pressures required improvements in
product quality
– firms initially focused on technology
– quality improvement didn’t follow
– required changes to organizational structures and processes
• Transition from: “managing by imposing control” to “managing by eliciting commitment”

Organizational Framework
Nadler DA, Tushman ML. Organizational frame bending: principles for managing reorientation.
Acad Manage Exec 1989;3(3):194–204

Organizational Change
• Organizational change occurs as a planned response to a defined set of pressures or forces
• Basic choices that an organization confronts in managing this change:
– how is the change defined?
– who participates in the change process and how?
– how is change implemented?
– how is change institutionalized?
How is the change defined?
• Is change required in a few or many components? – “incremental change”
• minor / single factor change
• implemented without altering any organizational components
– “transformational change”
• System-wide improvements require coordinated changes in multiple components: – clinical procedures, attitudes and behaviours of care
providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, organizational culture
• Different responses to the same pressures may be equally effective
Who participates in the change
process and how? • Successful change requires different organizational
groups to play distinct roles in the change management process: – senior leadership (medical and administrative)
• active, visible role in initiating change, and providing a vision of what needs to be achieved
• energize the change process
– CEO - establish a guiding coalition for change: • includes senior administrators, clinicians, and opinion leaders
from across the organization
– CEO and guiding coalition must create dissatisfaction with the status quo
• impart a sense of “urgency” about the proposed change
– other people involved directly in the care delivery process must participate actively in implementing change locally
Who participates in the change
process and how? • Can be challenging:
– “business as usual”
– senior physicians unaware of issue as remote from routine processes
– clinicians may only view serious harm as a significant issue
– clinicians may not completely understand or generally accept the need for change
– medical staff may view some changes, such as increasing interactions with nurses, as inappropriate or unnecessary
• CEO and the guiding coalition must shatter these assumptions – e.g. information on near misses presented regularly to the
medical staff
• CEO and members of the guiding coalition must visibly participate in the change process – helps to “model” desired changes in behaviours
How is change implemented?
• Two basic features are associated with successful change: – dedicated support structures
• implementation group
• pilot test site
• communication channels
• innovative training programmes
• encourage visits to successful organisations
– multiple tactics required • active participation of members of the guiding coalition in the
supporting structures
• frequent review by hospital administrators and senior medical staff
• facilitating reporting systems
• facilitating working across grades / specialties / disciplines
How is change institutionalized?
• Even if implemented successfully, there is a risk of reversion to earlier behaviours – unable to afford the resources allocated to initiating the change
– organization facing new pressures diverting senior leaders’ attention
– turnover among key employees
• The aim of institutionalization is for the change becomes a robust feature of the organizational context (i.e. part of culture) – needs a formal, long-term plan that integrates multiple
interrelated strategies • commitment of the CEO and senior staff to protect the initiative from
competing priorities
• structural changes that reinforce the change
• roles redesigned to match the new organizational realities
• adapt to emerging and unexpected demands
• leaders must continuously monitor the ongoing change process
Organizational Change
Countless theories
on change and
change
management
Organizational Change
Countless theories
on change and
change
management
Don’t be a victim of organizational
change
• How to predict outcome of changes?
– structured / planned
• buildings / facilities, populations, services
(investigations, treatments / therapies, etc),
administration / management, etc
– subtle / unplanned
• population, cultural, external factors, etc

Don’t be a victim of organizational
change
• Ensure involved in all projects that might
have an impact
• Can never be aware of all changes in
advance
• Impossible to predict and compensate for
all potential consequences of change,
even with advanced knowledge of the
change
Don’t be a victim of organizational
change
• Therefore must constantly monitor for
effects of change
• Surveillance:
– collect data
– analyse data
– understand data
– trust data
– act on findings
Don’t be a victim of organizational
change
• Surveillance for infection prevention:
– alert organism
– alert condition
– audits of practices
– environmental audits
– etc.
• Surveillance for stewardship:
– antimicrobial prescribing
– resistance patterns of pathogens
– etc.
0
1
2
3
4
5
6
7
8
9Ja
n-1
0
Mar-
10
May-1
0
Jul-
10
Sep-1
0
Nov-1
0
Ja
n-1
1
Mar-
11
May-1
1
Jul-
11
Sep-1
1
Nov-1
1
Ja
n-1
2
Mar-
12
May-1
2
Jul-
12
Sep-1
2
Nov-1
2
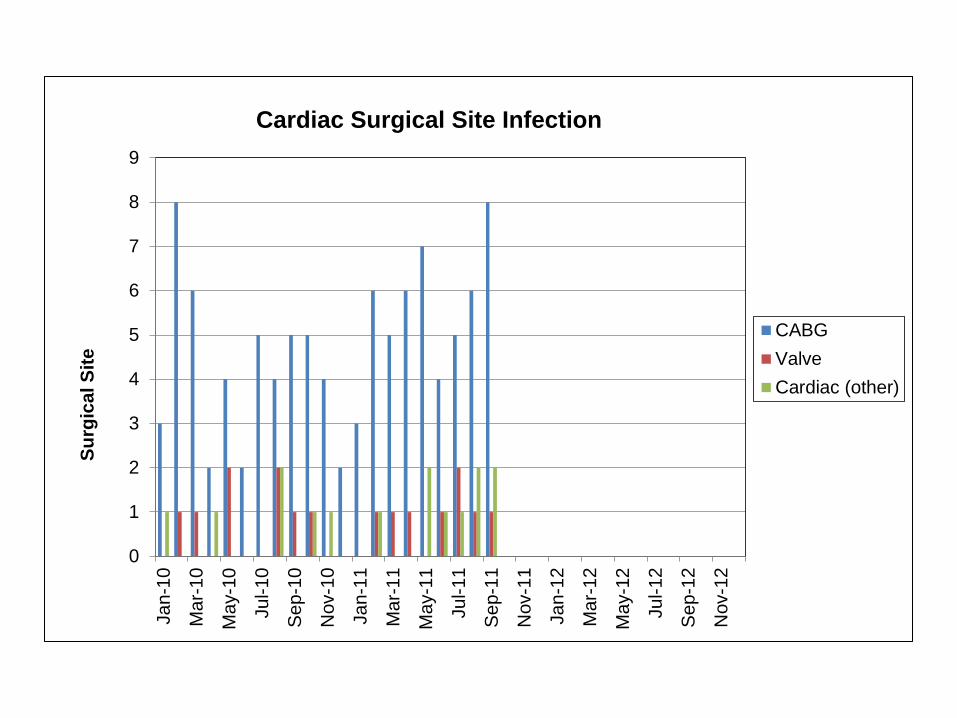
CABG
Valve
Cardiac (other)
Su
rgic
al S
ite
Cardiac Surgical Site Infection
0
2
4
6
8
10
12Ja
n-1
0
Mar-
10
May-1
0
Jul-
10
Sep-1
0
Nov-1
0
Ja
n-1
1
Mar-
11
May-1
1
Jul-
11
Sep-1
1
Nov-1
1
Ja
n-1
2
Mar-
12
May-1
2
Jul-
12
Sep-1
2
Nov-1
2
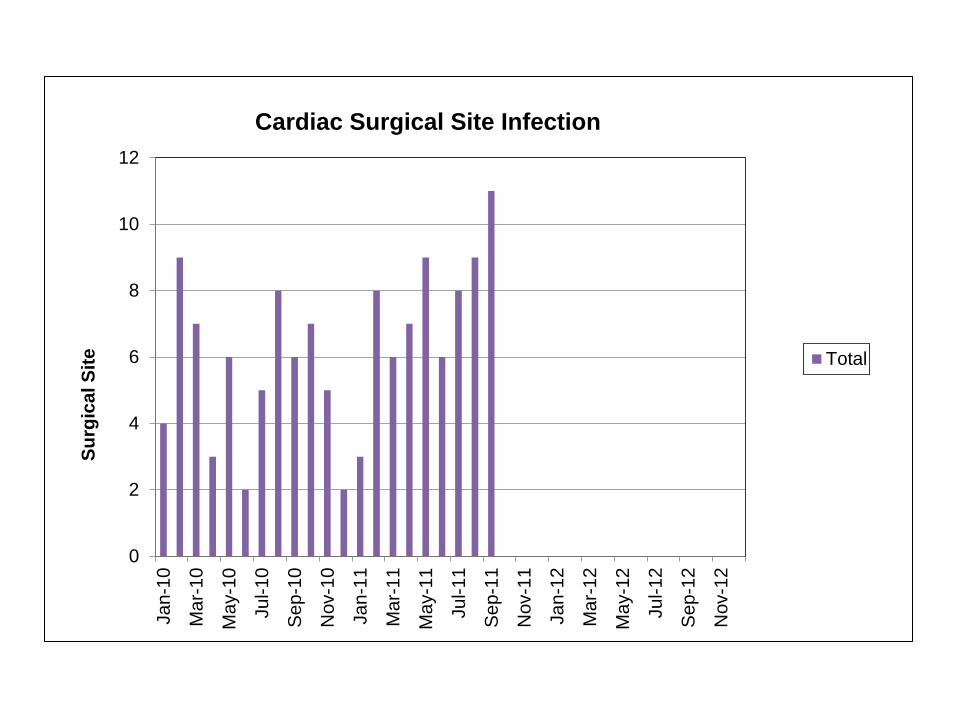
Total
Su
rgic
al S
ite
Cardiac Surgical Site Infection
0
2
4
6
8
10
12
14
Jan-M
ar
10
Apr-
Jun 1
0
Jul-
Sep 1
0
Oct-
Dec 1
0
Jan-M
ar
11
Apr-
Jun 1
1
Jul-
Sep 1
1
Oct-
Dec 1
1
Jan-M
ar
12
Apr-
Jun 1
2
Jul-
Sep 1
2
Oct-
Dec 1
2
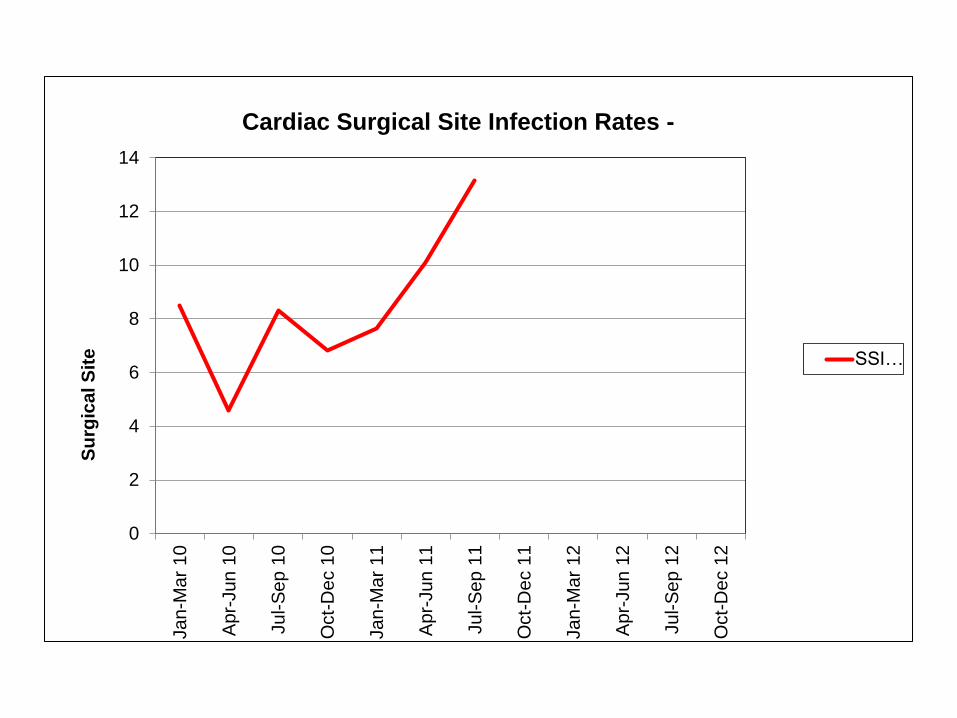
SSI…
Su
rgic
al S
ite
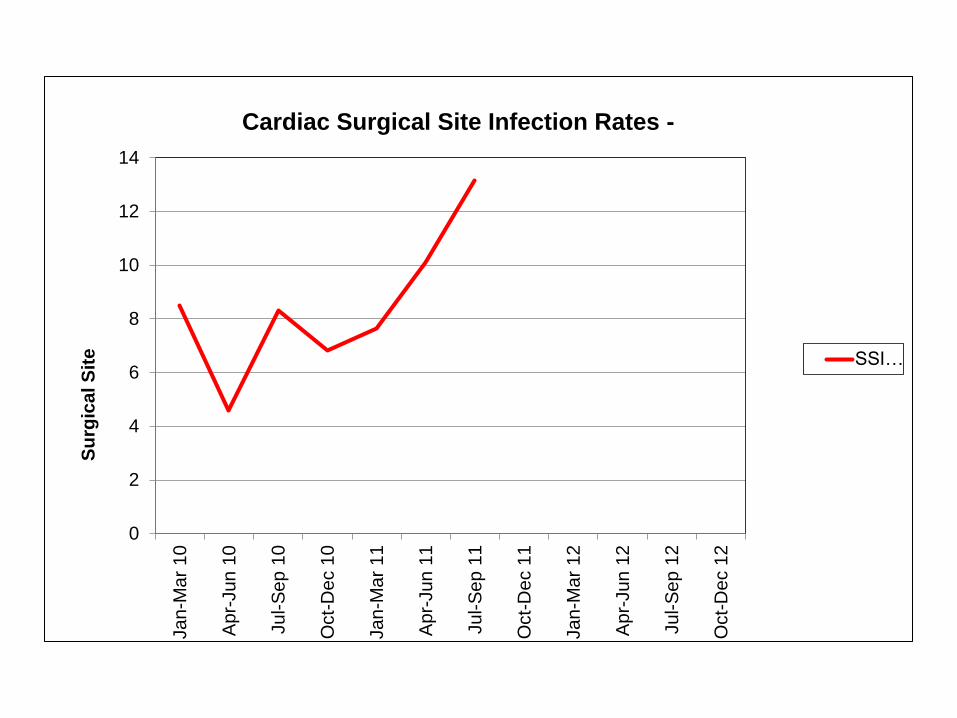
Cardiac Surgical Site Infection Rates -
Is there a problem?
• Not just increase in infection rate:
– increase in early onset (pre-discharge) SSIs
– increase in sternal wound infections
– increase in deep and organ/space SSIs
What had changed?
• No change in:
– theatres
– surgeons
– skin prep
– etc.
What had changed?
• Cardiac anaesthetists unhappy giving local recommended antimicrobial prophylaxis:
flucloxacillin 1 g qds for 4 doses
+
gentamicin 5 mg/kg (LBW) – single dose
• Started giving 3 mg/kg gentamicin – thought it was contributing to post-op AKI
– decision to implement change made amongst themselves
– not discussed with microbiologists (or surgeons)
0
2
4
6
8
10
12
14
Jan-M
ar
10
Apr-
Jun 1
0
Jul-
Sep 1
0
Oct-
Dec 1
0
Jan-M
ar
11
Apr-
Jun 1
1
Jul-
Sep 1
1
Oct-
Dec 1
1
Jan-M
ar
12
Apr-
Jun 1
2
Jul-
Sep 1
2
Oct-
Dec 1
2
SSI…
Su
rgic
al S
ite
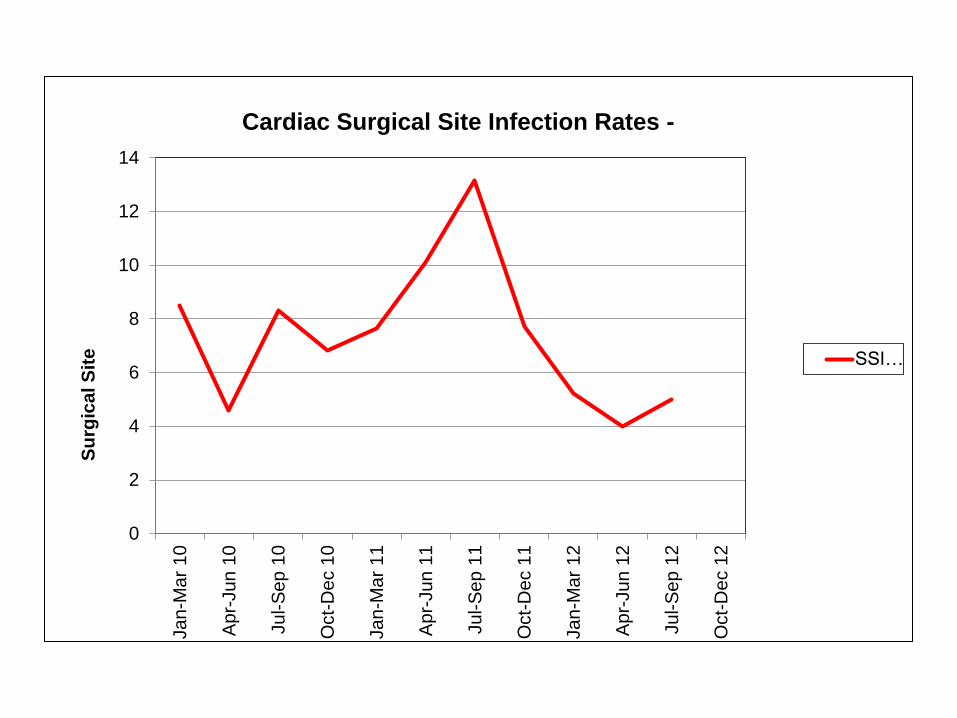
Cardiac Surgical Site Infection Rates -
0
2
4
6
8
10
12
14
Jan-M
ar
10
Apr-
Jun 1
0
Jul-
Sep 1
0
Oct-
Dec 1
0
Jan-M
ar
11
Apr-
Jun 1
1
Jul-
Sep 1
1
Oct-
Dec 1
1
Jan-M
ar
12
Apr-
Jun 1
2
Jul-
Sep 1
2
Oct-
Dec 1
2
SSI…
Su
rgic
al S
ite
Cardiac Surgical Site Infection Rates -
Summary
• Embrace change
• Use change
• Be in a position to detect change
• Communicate!