Embed Size (px)
Citation preview
1
Atrial fibrillation (AF) is a frequent complication of long-standing hypertension and represents the most common
cardiac arrhythmia causing significant morbidity and mortal-ity.1–3 During AF, normal atrioventricular (AV) node conduc-tion leads to a rapid and irregular ventricular rate, resulting in an impairment of left ventricular function and exercise capacity.4 Rate control can be achieved by drugs modulating the autonomic nervous system, for example, by β-blockers. Genetic inhibition of inhibitory Gα protein in the AV node reduced heart rate (HR) and prevented AF-associated reduc-tion of cardiac function in a porcine model for persistent AF.5 In addition, AF causes atrial electrical remodeling mainly characterized by a pronounced atrial effective refractory period (AERP) shortening perpetuating AF.6 Alterations in the autonomic nervous system may influence AF-induced atrial electrical remodeling and atrial arrhythmogenesis.7–9 Catheter-based renal denervation (RDN) is a new therapeutic approach to reduce sympathetic activity and blood pressure (BP) and to
improve obstructive sleep apnea severity and glucose metab-olism in resistant hypertension.10–15 However, the effect of RDN on ventricular HR response during AF (rate control) and AF-induced electrical remodeling is unknown.
Herein, we report on the effect of catheter-based RDN, shown previously to reduce renal and whole body sympathetic activity,12-14 on rate control in a patient with permanent AF and resistant hypertension. Subsequently, we investigated the effect of denervation of the afferent and efferent renal sympathetic nerves in a pig model with short-term AF maintained by rapid atrial pacing.
MethodsCatheter-Based RDN in a Patient With AFThe patient gave written informed consent. Catheter-based RDN was performed as described previously.11–15 Renal angiogram was per-formed via femoral access to exclude renal artery stenosis. The treat-ment catheter (Symplicity Catheter System, Ardian/Medtronic USA)
Abstract—Renal denervation (RDN) reduces renal efferent and afferent sympathetic activity thereby lowering blood pressure in resistant hypertension. The effect of modulation of the autonomic nervous system by RDN on atrial electrophysiology and ventricular rate control during atrial fibrillation (AF) is unknown. Here we report a reduction of ventricular heart rate in a patient with permanent AF undergoing RDN. Subsequently, we investigated the effect of RDN on AF-induced shortening of atrial effective refractory period, AF inducibility, and ventricular rate control during AF maintained by rapid atrial pacing in 12 pigs undergoing RDN (n=7) or sham procedure (n=5). During sinus rhythm, RDN reduced heart rate (RR-interval, 708±12 versus 577±19 ms; P=0.0021) and increased atrioventricular node conduction time (PQ-interval, 112±12 versus 88±9 ms; P=0.0001). Atrial tachypacing for 30 minutes increased AF inducibility and decreased AF cycle length. This was not influenced by RDN. RDN reduced ventricular rate during AF episodes by ≈24% (119±9 versus 158±19 bpm; P=0.0001). AF episodes were shorter after RDN compared with sham (12±3 versus 34±4 s; P=0.0091), but atrial effective refractory period was not modified by RDN. RDN reduced heart rate and reduced atrioventricular node conduction time during sinus rhythm and provided rate control during AF. AF-induced atrial electrical remodeling, AF inducibility, and AF cycle length were not modified, but duration of AF episodes was shorter after RDN. Modulation of the autonomic nervous system by RDN might provide rate control and reduce susceptibility to AF. Whether RDN may provide rate control in a larger number of patients with AF deserves further clinical studies. (Hypertension. 2013;61:XXX-XXX.)
Key Words: atrial fibrillation ◼ renal denervation ◼ rate control ◼ electrical remodeling ◼ symplicity
Received September 13, 2012; first decision October 4, 2012; revision accepted October 14, 2012.From the Universitätsklinikum des Saarlandes, Klinik für Innere Medizin III, Homburg/Saar, Germany (D.L., F.M., C.U., M.H., H.-R.N., M.B.);
Cardiovascular Research Institute, Maastricht, the Netherlands (U.S.); Sanofi-Aventis Deutschland GmbH, R&D, Aging/Disability of Cardiovascular and Cerebral Origin, Frankfurt, Germany (K.W.).
*Drs Linz and Mahfoud contributed equally to this work.†Drs Wirth and Bohm share senior authorship.Correspondence to Dominik Linz, Klinik für Innere Medizin III, Universitätsklinikum des Saarlandes, 66421 Homburg/Saar, Germany. E-mail
Renal Sympathetic Denervation Provides Ventricular Rate Control But Does Not Prevent Atrial Electrical Remodeling
During Atrial FibrillationDominik Linz,* Felix Mahfoud,* Ulrich Schotten, Christian Ukena, Mathias Hohl,
Hans-Ruprecht Neuberger, Klaus Wirth,† Michael Böhm†
Original Article
© 2012 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI:10.1161/HYPERTENSIONAHA.111.00182
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from
2 Hypertension January 2013
was introduced into each renal artery using a guiding catheter (internal mammary artery), and ablations were performed in both renal arteries using a standardized treatment protocol and algorithm. Five energy deployments for 120 s with 8 watts each were performed in the right and 4 in the left renal artery. Treatments were delivered from the first distal main renal artery bifurcation to the ostium proximally and were spaced longitudinally and rotationally under fluoroscopic guidance. Morphine and midazolam were administered to manage visceral pain during the energy delivery. Baseline and follow-up procedures at 3, 6, and 12 months consisted of an assessment of BP (Spacelab 90207 device), recording of a resting electrocardiogram (ECG), a 24-hour Holter ECG, and review of medication. To minimize the influence of confounding factors, ECG and BP were obtained at the same daytime 1 to 2 hours after intake of antihypertensive medications. Recording of a 12-lead ECG was performed after 10 minutes of supine rest at standard sensitivity (10 mm = 1 mV) and a paper speed of 50 mm/s. ECGs were analyzed concerning HR and rhythm as described else-where.16 Polymorphic premature ventricular beats were quantified per 24 hours.
Pig Model for AFAll of the animal studies were performed in accordance with the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (publication No. 85-23, revised 1996). In 12 chest-closed male castrated pigs (25–30 kg) of the German Landrace (anesthetized with 20% urethane, 0.8 mL/kg IV load, 0.4 mL/kg per hour of maintenance) and 4% α-chloralose (0.4 mL/kg IV load, 0.1 mL/kg per hour of maintenance), a tracheotomy was performed to place an endotracheal tube.17 Blood pressure was mea-sured by a Millar tip catheter (Millar PC 350; Millar Instruments, Houston, TX) in the femoral artery. Bipolar body surface ECG was recorded using subcutaneous needle electrodes in the classic lead II arrangement. The ECGs were analyzed before and after RDN. In all of the animals, both kidneys were approached through bilateral retro-peritoneal flank incisions. In 7 animals, both kidneys were surgically denervated by cutting all of the visible nerves in the area of the renal hilus and by stripping ≈1 cm of the adventitia from the renal artery. The area was then moistened with a 20% phenol/ethanol solution for 10 to 15 minutes. Left renal flow was measured with a doppler flow probe (transit time flowmeter module system from Transonic Systems Inc) positioned on the blood vessels. After RDN, the animals were allowed to re-equilibrate for 1.5 hours. Significant reduction of a reproducible postapneic BP rise and the absence (<5% change) of a decrease in renal blood flow induced by tracheal occlusion for 2 min-utes were taken as evidence of the completeness of RDN.17 Sham sur-gical procedure with kidney exposition without RDN was performed in the 5 other pigs serving as time controls.
Electrophysiological Examinations in PigsAtrial responses to the pacing procedure were visualized by mono-phasic action potential (MAP) recordings from the endocardium of the right atrium by a MAP pacing catheter (combined MAP and stimulation catheter, 7F catheter, Foehr Medical Instruments GMBH, Seeheim, Germany). The catheter was inserted via a femoral vein. The tip of the catheter was advanced to the lateral right atrium to record a stable and sharp MAP signal. Determination of the diastolic pacing threshold (0.5–1.0 mV) before each tracheal occlusion maneu-ver revealed no significant changes during the experimental period. A train of 10 basic stimuli (S1, pulse duration 1 ms) at twice diastolic pacing threshold was followed by an extra stimulus (S2) starting at ≈30 ms below the expected AERP with a 5-ms increment (UHS 20, universal heart stimulator; Biotronik, Berlin, Germany). The shortest coupling interval able to elicit a propagated atrial response was taken as the AERP. AERP was measured at different stimulation frequen-cies (basic cycle length, 240, 300, and 400 ms) before and after RDN, as described previously.18 The AV node effective refractory periods and the longest cycle length of atrial pacing causing second-degree AV nodal block (antegrade Wenckebach point) were determined. To deliver rapid atrial pacing (basic cycle length, 50 ms) for 30 minutes, a second 7F bipolar catheter was inserted in the right atrial appendage. After each 15 minutes, rapid atrial pacing was temporally stopped for
AERP measurements at a basic cycle length of 240, 300, and 400 ms. During the AERP measurement procedure the shortest premature S2 extrastimulus resulting in a propagated response frequently induced episodes of AF. When atrial MAP signals showed an irregular rapid activation (cycle length, <200 ms; duration, >5 seconds), AF was diagnosed. The mean percentage of AERP measurement triggering AF was used to describe AF inducibility. To determine the mean atrial and mean ventricular cycle length during AF, the AA- and RR-inter-vals, respectively, were measured over a 5-second interval and aver-aged.18 All in all, 5 consecutive AF episodes per animal and per time point have been analyzed and averaged.
StatisticsData are presented as mean±SEM. For comparisons of single repeated measures only, a paired Student t test was used. For multiple repeated-measures comparisons with the same baseline, repeated-measures 2-way ANOVA was used followed by the Dunnet test to compare individual mean difference if ANOVA was significant. A P value <0.05 was considered significant. For all of the statistical calcu-lations software Everstat version 5 based on SAS 8 was used.
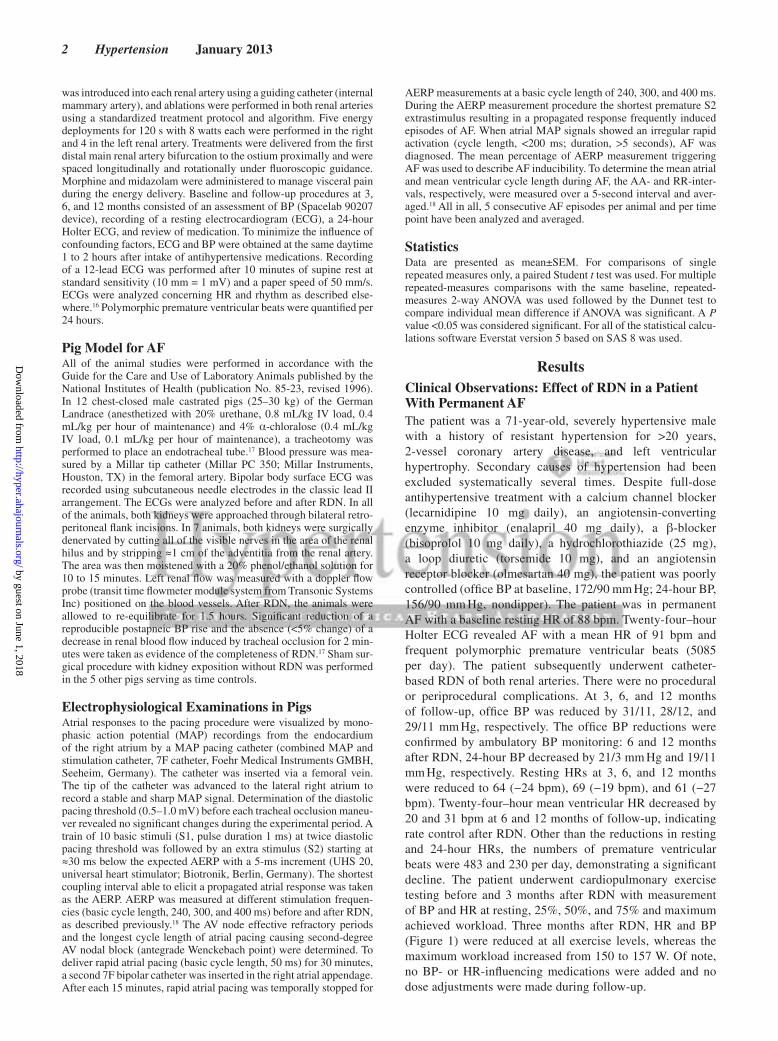
ResultsClinical Observations: Effect of RDN in a Patient With Permanent AFThe patient was a 71-year-old, severely hypertensive male with a history of resistant hypertension for >20 years, 2-vessel coronary artery disease, and left ventricular hypertrophy. Secondary causes of hypertension had been excluded systematically several times. Despite full-dose antihypertensive treatment with a calcium channel blocker (lecarnidipine 10 mg daily), an angiotensin-converting enzyme inhibitor (enalapril 40 mg daily), a β-blocker (bisoprolol 10 mg daily), a hydrochlorothiazide (25 mg), a loop diuretic (torsemide 10 mg), and an angiotensin receptor blocker (olmesartan 40 mg), the patient was poorly controlled (office BP at baseline, 172/90 mm Hg; 24-hour BP, 156/90 mm Hg, nondipper). The patient was in permanent AF with a baseline resting HR of 88 bpm. Twenty-four–hour Holter ECG revealed AF with a mean HR of 91 bpm and frequent polymorphic premature ventricular beats (5085 per day). The patient subsequently underwent catheter-based RDN of both renal arteries. There were no procedural or periprocedural complications. At 3, 6, and 12 months of follow-up, office BP was reduced by 31/11, 28/12, and 29/11 mm Hg, respectively. The office BP reductions were confirmed by ambulatory BP monitoring: 6 and 12 months after RDN, 24-hour BP decreased by 21/3 mm Hg and 19/11 mm Hg, respectively. Resting HRs at 3, 6, and 12 months were reduced to 64 (−24 bpm), 69 (−19 bpm), and 61 (−27 bpm). Twenty-four–hour mean ventricular HR decreased by 20 and 31 bpm at 6 and 12 months of follow-up, indicating rate control after RDN. Other than the reductions in resting and 24-hour HRs, the numbers of premature ventricular beats were 483 and 230 per day, demonstrating a significant decline. The patient underwent cardiopulmonary exercise testing before and 3 months after RDN with measurement of BP and HR at resting, 25%, 50%, and 75% and maximum achieved workload. Three months after RDN, HR and BP (Figure 1) were reduced at all exercise levels, whereas the maximum workload increased from 150 to 157 W. Of note, no BP- or HR-influencing medications were added and no dose adjustments were made during follow-up.
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Linz et al Renal Denervation and Atrial Fibrillation 3
Experimental Observations in Pigs: Electrophysiological Effects of RDN on ECGFigure 2 shows ECG parameters in sham and RDN pigs dur-ing sinus rhythm. RDN reduced HR by ≈17% (sinus cycle length, 708±12 versus 577±19 ms in sham; P=0.0021), and PQ-interval was prolonged by ≈29% (PQ-interval, 112±12 versus 88±9 ms in sham; P=0.0001), whereas P-wave dura-tion was not changed by RDN.
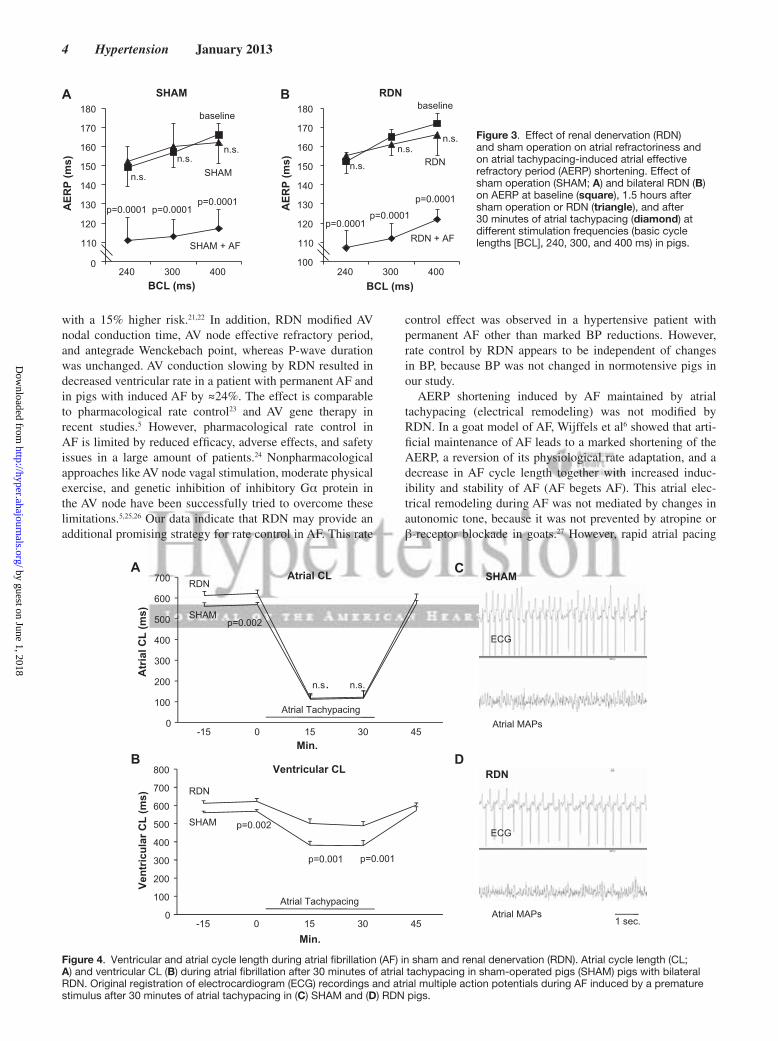
Effect of RDN on Atrial Refractoriness, Electrical Remodeling, and AV Nodal ConductionFigure 3 shows the effects of sham procedure (Figure 3A) and bilateral RDN (Figure 3B) on AERP at baseline and on atrial tachypacing-induced AERP shortening at different stimulation frequencies (basic cycle lengths, 240, 300, and 400 ms). RDN and sham procedure did not significantly influence AERP at baseline, and AERP shortening induced by atrial tachypacing
(electrical remodeling) was not modified by RDN. AV node effective refractory period (240±7 versus 220±9 ms; P<0.01) and antegrade Wenckebach point (222±8 versus 192±5 ms; P<0.01) were prolonged by RDN.
Effect of RDN on Ventricular Rate Response and Atrial Refractoriness During AFFigure 4 shows atrial (Figure 4A) and ventricular (Figure 4B) cycle length during AF induced by a premature stimulus after 15 and 30 minutes of atrial tachypacing in sham and RDN. Ventricular HR during AF was reduced by ≈24% in RDN (119±9 versus 158±19 bpm; P=0.0001), whereas atrial cycle length was not different between the groups. On the right, rep-resentative original registration of the ECG and atrial multiple action potentials during AF induced by a premature stimulus after 30 minutes of atrial tachypacing in sham (Figure 4C) and after RDN (Figure 4D) is shown.
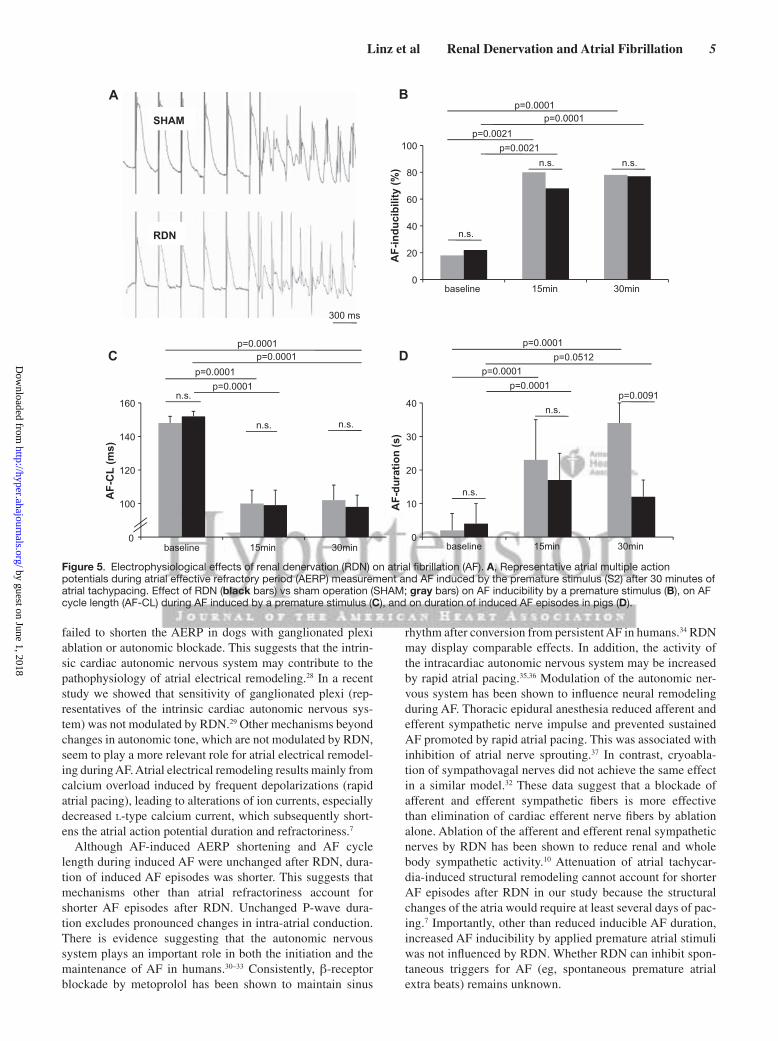
Effect of RDN on AFFigure 5A shows representative atrial multiple action poten-tials during AERP measurement and during AF induced by the premature stimulus (S2) after 30 minutes of atrial tachypac-ing. Increased AF inducibility after atrial tachypacing was not changed by RDN (Figure 5B). AF cycle length (Figure 5C) after 30 minutes of atrial tachypacing was decreased compared with baseline and not further modulated by RDN. However, after 30 minutes of atrial tachypacing, duration of induced AF episodes (Figure 5D) was significantly shortened by RDN (12±3 versus 34±4 s; P=0.0091).
Effect of RDN on BPRDN did not influence normotensive systolic BP significantly when compared with sham (102±4 versus 108±3 mm|Hg in sham; P=0.7992).
DiscussionRDN provided rate control by reducing resting HR, 24-hour HR, and HR during exercise in a patient with permanent AF other than marked reduction of BP and polymorphic prema-ture ventricular beats. This observation motivated a subse-quently conducted experimental pig study. RDN reduced HR as well as AV nodal conduction in pigs during sinus rhythm, prolonged AV node effective refractory period and antegrade Wenckebach point, and provided efficient rate control dur-ing induced AF. Duration of induced AF episodes was short-ened after RDN when compared with sham. However, atrial tachypacing-induced AERP shortening and intra-atrial con-duction (P-wave duration), increased AF inducibility (electri-cal remodeling), and BP was not modified.
The autonomic nervous system affects electrophysiological properties like chronotropy and dromotropy.19 In the present study, RDN reduced HR during sinus rhythm, potentially because of alterations in sympathetic activity by RDN. This is of interest because HR reduction has become a therapeutic target in many cardiovascular diseases.20 The Systolic Heart Failure Treatment With the If Inhibitor Ivabradine Trial has shown a reduction by 18% of cardiovascular death and hospitalization for heart failure in patients with systolic heart failure, in whom a 5-bpm higher HR at baseline corresponded
A B
Figure 1. Cardiopulmonary exercise testing in an atrial fibrillation (AF) patient. Heart rate (A) and blood pressure (B) during cardiopulmonary exercise testing at different levels of achieved workload (x axis, % of maximum workload) before (dotted line, maximum workload 150 W) and 3 months (continuous line, maximum workload 157 W) after renal denervation (RDN).
p=0.0021
p=0.0001n.s.EC
G-in
terv
als
(ms)
SHAM RDN
0
200
400
600
800
SCL PQ P
Figure 2. Electrocardiogram (ECG) analysis. Analysis of ECG in sham-operated pigs (SHAM; gray) vs pigs with bilateral renal denervation (RDN; black). Sinus rhythm cycle length (SCL), P-wave duration (P), and PQ-interval (PQ) are shown.
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from
4 Hypertension January 2013
with a 15% higher risk.21,22 In addition, RDN modified AV nodal conduction time, AV node effective refractory period, and antegrade Wenckebach point, whereas P-wave duration was unchanged. AV conduction slowing by RDN resulted in decreased ventricular rate in a patient with permanent AF and in pigs with induced AF by ≈24%. The effect is comparable to pharmacological rate control23 and AV gene therapy in recent studies.5 However, pharmacological rate control in AF is limited by reduced efficacy, adverse effects, and safety issues in a large amount of patients.24 Nonpharmacological approaches like AV node vagal stimulation, moderate physical exercise, and genetic inhibition of inhibitory Gα protein in the AV node have been successfully tried to overcome these limitations.5,25,26 Our data indicate that RDN may provide an additional promising strategy for rate control in AF. This rate
control effect was observed in a hypertensive patient with permanent AF other than marked BP reductions. However, rate control by RDN appears to be independent of changes in BP, because BP was not changed in normotensive pigs in our study.
AERP shortening induced by AF maintained by atrial tachypacing (electrical remodeling) was not modified by RDN. In a goat model of AF, Wijffels et al6 showed that arti-ficial maintenance of AF leads to a marked shortening of the AERP, a reversion of its physiological rate adaptation, and a decrease in AF cycle length together with increased induc-ibility and stability of AF (AF begets AF). This atrial elec-trical remodeling during AF was not mediated by changes in autonomic tone, because it was not prevented by atropine or β-receptor blockade in goats.27 However, rapid atrial pacing
100
110
120
130
140
150
160
170
180
240 300 400
110
120
130
140
150
160
170
180
240 300 400BCL (ms) BCL (ms)
AER
P (m
s)
AER
P (m
s)
SHAM RDN
p=0.0001 p=0.0001p=0.0001
p=0.0001p=0.0001
p=0.0001
A Bbaseline
SHAM
SHAM + AF
baseline
RDN
RDN + AF
0
n.s.
n.s.n.s.
n.s.
n.s.n.s. Figure 3. Effect of renal denervation (RDN)
and sham operation on atrial refractoriness and on atrial tachypacing-induced atrial effective refractory period (AERP) shortening. Effect of sham operation (SHAM; A) and bilateral RDN (B) on AERP at baseline (square), 1.5 hours after sham operation or RDN (triangle), and after 30 minutes of atrial tachypacing (diamond) at different stimulation frequencies (basic cycle lengths [BCL], 240, 300, and 400 ms) in pigs.
0
100
200
300
400
500
600
700
-15 0 15 30 45
Atrial Tachypacing
Min.
Min.
Atr
ial C
L (m
s)Ve
ntric
ular
CL
(ms)
A
B
Atrial CL
Ventricular CL
C
D
SHAM
RDN
ECG
ECG
Atrial MAPs
Atrial MAPs
1 sec.
Atrial Tachypacing
SHAM
RDN
SHAM
RDN
p=0.001 p=0.001
p=0.002
p=0.002
n.s . n.s.
0
100
200
300
400
500
600
700
800
-15 0 15 30 45
Figure 4. Ventricular and atrial cycle length during atrial fibrillation (AF) in sham and renal denervation (RDN). Atrial cycle length (CL; A) and ventricular CL (B) during atrial fibrillation after 30 minutes of atrial tachypacing in sham-operated pigs (SHAM) pigs with bilateral RDN. Original registration of electrocardiogram (ECG) recordings and atrial multiple action potentials during AF induced by a premature stimulus after 30 minutes of atrial tachypacing in (C) SHAM and (D) RDN pigs.
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Linz et al Renal Denervation and Atrial Fibrillation 5
failed to shorten the AERP in dogs with ganglionated plexi ablation or autonomic blockade. This suggests that the intrin-sic cardiac autonomic nervous system may contribute to the pathophysiology of atrial electrical remodeling.28 In a recent study we showed that sensitivity of ganglionated plexi (rep-resentatives of the intrinsic cardiac autonomic nervous sys-tem) was not modulated by RDN.29 Other mechanisms beyond changes in autonomic tone, which are not modulated by RDN, seem to play a more relevant role for atrial electrical remodel-ing during AF. Atrial electrical remodeling results mainly from calcium overload induced by frequent depolarizations (rapid atrial pacing), leading to alterations of ion currents, especially decreased l-type calcium current, which subsequently short-ens the atrial action potential duration and refractoriness.7
Although AF-induced AERP shortening and AF cycle length during induced AF were unchanged after RDN, dura-tion of induced AF episodes was shorter. This suggests that mechanisms other than atrial refractoriness account for shorter AF episodes after RDN. Unchanged P-wave dura-tion excludes pronounced changes in intra-atrial conduction. There is evidence suggesting that the autonomic nervous system plays an important role in both the initiation and the maintenance of AF in humans.30–33 Consistently, β-receptor blockade by metoprolol has been shown to maintain sinus
rhythm after conversion from persistent AF in humans.34 RDN may display comparable effects. In addition, the activity of the intracardiac autonomic nervous system may be increased by rapid atrial pacing.35,36 Modulation of the autonomic ner-vous system has been shown to influence neural remodeling during AF. Thoracic epidural anesthesia reduced afferent and efferent sympathetic nerve impulse and prevented sustained AF promoted by rapid atrial pacing. This was associated with inhibition of atrial nerve sprouting.37 In contrast, cryoabla-tion of sympathovagal nerves did not achieve the same effect in a similar model.32 These data suggest that a blockade of afferent and efferent sympathetic fibers is more effective than elimination of cardiac efferent nerve fibers by ablation alone. Ablation of the afferent and efferent renal sympathetic nerves by RDN has been shown to reduce renal and whole body sympathetic activity.10 Attenuation of atrial tachycar-dia-induced structural remodeling cannot account for shorter AF episodes after RDN in our study because the structural changes of the atria would require at least several days of pac-ing.7 Importantly, other than reduced inducible AF duration, increased AF inducibility by applied premature atrial stimuli was not influenced by RDN. Whether RDN can inhibit spon-taneous triggers for AF (eg, spontaneous premature atrial extra beats) remains unknown.
0
10
20
30
40
baseline 15min 30min
100
120
140
160
baseline 15min 30min
A
C
SHAM
RDN
AF-
CL
(ms)
AF-
dura
tion
(s)
B
D
AF-
indu
cibi
lity
(%)
300 ms
p=0.0021p=0.0001
p=0.0021
p=0.0001
p=0.0001p=0.0512
p=0.0001
p=0.0001
p=0.0091
p=0.0001p=0.0001
p=0.0001
p=0.0001
0
n.s.
n.s. n.s.
n.s.
n.s. n.s.
n.s.
n.s.
0
20
40
60
80
100
baseline 15min 30min
Figure 5. Electrophysiological effects of renal denervation (RDN) on atrial fibrillation (AF). A, Representative atrial multiple action potentials during atrial effective refractory period (AERP) measurement and AF induced by the premature stimulus (S2) after 30 minutes of atrial tachypacing. Effect of RDN (black bars) vs sham operation (SHAM; gray bars) on AF inducibility by a premature stimulus (B), on AF cycle length (AF-CL) during AF induced by a premature stimulus (C), and on duration of induced AF episodes in pigs (D).
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from

6 Hypertension January 2013
The first supportive data for potential antiarrhythmic effect of acute RDN have been published recently. Ukena et al38 reported reduced ventricular tachyarrhythmias in patients with electrical storm and congestive heart failure after catheter-based RDN. In addition, RDN inhibited pronounced shortening of AERP and increased AF susceptibility in a pig model for obstructive sleep apnea.30 Whether RDN may provide rate control in a larger number of patients with AF deserves further clinical studies.
LimitationsOne might suggest that catheter-based RDN does possibly not completely abrogate renal sympathetic nerves, as indicated by a norepinephrine spillover reduction by ≈50%. Herein, we performed combined surgical and chemical renal nerve ablation, which might be more complete compared with the catheter-based approach. However, in pilot studies, it has been shown that norepinephrine reduction in the kidney was simi-lar to catheter-based RDN and surgical RDN by ≈60% (Paul A. Sobotka, personal communication, unpublished data). In addition, spontaneous occurrence of AF was too rare for a systematic evaluation. In patients with AF, Holter monitor-ing showed that paroxysmal AF is induced by spontaneous premature atrial beats in ≈74.3%.39 Therefore, we applied a premature beat to induce AF, representing a good parameter to characterize atrial vulnerability.6,7,16,17,28 Moreover, only short-term effects of RDN could be investigated through the experimental approach used in the animals of this study. The long-term effects of RDN on AF and its recurrence are still to be explored in animal models for permanent AF.
Conclusions and PerspectivesDuring sinus rhythm, RDN reduces HR and prolongs AV nodal conduction. AV conduction slowing by RDN resulted in efficient rate control during AF. The duration of induced AF episodes was shortened after RDN. However, AF-induced AERP shortening, P-wave duration, and AF inducibility (electrical remodeling) were not altered. RDN displays acute antiarrhythmic effects without changing atrial refractoriness or BP. Modulation of the autonomic nervous system by RDN provides efficient rate control during AF and might be useful to reduce susceptibility to AF in patients with paroxysmal AF. RDN deserves to be tested in AF models for chronic AF with structural, electrical, or neural atrial remodeling and in clini-cal studies. Whether RDN may provide rate control in a larger number of patients with AF deserves further clinical studies.
Sources of FundingDrs Böhm, Mahfoud, and Ukena are supported by the Deutsche Forschungsgemeinschaft (KFO 196). Dr Mahfoud is supported by the Deutsche Hochdruckliga.
DisclosuresNone.
References 1. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA,
Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S; Task Force on Practice Guidelines, American College of Cardiology/American Heart Association; Committee for
Practice Guidelines, European Society of Cardiology; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 guide-lines for the management of patients with atrial fibrillation-executive sum-mary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Eur Heart J. 2006;27:1979–2030.
2. Marini C, De Santis F, Sacco S, Russo T, Olivieri L, Totaro R, Carolei A. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke. 2005;36:1115–1119.
3. Kaarisalo MM, Immonen-Räihä P, Marttila RJ, Salomaa V, Kaarsalo E, Salmi K, Sarti C, Sivenius J, Torppa J, Tuomilehto J. Atrial fibrillation and stroke: mortality and causes of death after the first acute ischemic stroke. Stroke. 1997;28:311–315.
4. Singh SN, Tang XC, Singh BN, Dorian P, Reda DJ, Harris CL, Fletcher RD, Sharma SC, Atwood JE, Jacobson AK, Lewis HD Jr, Lopez B, Raisch DW, Ezekowitz MD; SAFE-T Investigators. Quality of life and exercise performance in patients in sinus rhythm versus persistent atrial fibrilla-tion: a Veterans Affairs Cooperative Studies Program Substudy. J Am Coll Cardiol. 2006;48:721–730.
5. Lugenbiel P, Thomas D, Kelemen K, Trappe K, Bikou O, Schweizer PA, Voss F, Becker R, Katus HA, Bauer A. Genetic suppression of Gαs protein provides rate control in atrial fibrillation. Basic Res Cardiol. 2012;107:265.
6. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation: a study in awake chronically instrumented goats. Circulation. 1995;92:1954–1968.
7. Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiol Rev. 2011;91:265–325.
8. Inoue H, Zipes DP. Changes in atrial and ventricular refractoriness and in atrioventricular nodal conduction produced by combinations of vagal and sympathetic stimulation that result in a constant spontaneous sinus cycle length. Circ Res. 1987;60:942–951.
9. Liang BT, Frame LH, Molinoff PB. Beta 2-adrenergic receptors contrib-ute to catecholamine-stimulated shortening of action potential duration in dog atrial muscle. Proc Natl Acad Sci USA. 1985;82:4521–4525.
10. Sobotka PA, Mahfoud F, Schlaich MP, Hoppe UC, Böhm M, Krum H. Sympatho-renal axis in chronic disease. Clin Res Cardiol. 2011;100:1049–1057.
11. Mahfoud F, Schlaich M, Kindermann I, Ukena C, Cremers B, Brandt MC, Hoppe UC, Vonend O, Rump LC, Sobotka PA, Krum H, Esler M, Böhm M. Effect of renal sympathetic denervation on glucose metabo-lism in patients with resistant hypertension: a pilot study. Circulation. 2011;123:1940–1946.
12. Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, Kapelak B, Walton A, Sievert H, Thambar S, Abraham WT, Esler M. Catheter-based renal sympathetic denervation for resistant hyperten-sion: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373:1275–1281.
13. Schlaich MP, Sobotka PA, Krum H, Lambert E, Esler MD. Renal sym-pathetic-nerve ablation for uncontrolled hypertension. N Engl J Med. 2009;361:932–934.
14. Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Böhm M; Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (the Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376:1903–1909.
15. Witkowski A, Prejbisz A, Florczak E, Kądziela J, ąliwiąski P, Bieleą P, Michałowska I, Kabat M, Warchoł E, Januszewicz M, Narkiewicz K, Somers VK, Sobotka PA, Januszewicz A. Effects of renal sympathetic denervation on blood pressure, sleep apnea course, and glycemic control in patients with resistant hypertension and sleep apnea. Hypertension. 2011;58:559–565.
16. Camm AJ, Kirchhof P, Lip GY, et al. Guidelines for the manage-ment of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369–2429.
17. Linz D, Schotten U, Neuberger HR, Böhm M, Wirth K. Negative tracheal pressure during obstructive respiratory events promotes atrial fibrillation by vagal activation. Heart Rhythm. 2011;8:1436–1443.
18. Linz DK, Afkham F, Itter G, Rütten H, Wirth KJ. Effect of atrial electri-cal remodeling on the efficacy of antiarrhythmic drugs: comparison of amiodarone with I(Kr)- and I(to)/IKur-blockade in vivo. J Cardiovasc Electrophysiol. 2007;18:1313–1320.
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from

Linz et al Renal Denervation and Atrial Fibrillation 7
19. Wallick DW, Martin PJ, Masuda Y, Levy MN. Effects of autonomic activ-ity and changes in heart rate on atrioventricular conduction. Am J Physiol. 1982;243:H523–H527.
20. Palatini P. Role of elevated heart rate in the development of cardiovascular disease in hypertension. Hypertension. 2011;58:745–750.
21. Böhm M, Swedberg K, Komajda M, Borer JS, Ford I, Dubost-Brama A, Lerebours G, Tavazzi L; SHIFT Investigators. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376:886–894.
22. Swedberg K, Komajda M, Böhm M, Borer JS, Ford I, Dubost-Brama A, Lerebours G, Tavazzi L; SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 2010;376:875–885.
23. Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermans AJ, Tijssen JG, Crijns HJ; Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation Study Group. A comparison of rate control and rhythm con-trol in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347:1834–1840.
24. Groenveld HF, Crijns HJ, Van den Berg MP, Van Sonderen E, Alings AM, Tijssen JG, Hillege HL, Tuininga YS, Van Veldhuisen DJ, Ranchor AV, Van Gelder IC; RACE II Investigators. The effect of rate control on quality of life in patients with permanent atrial fibrillation: data from the RACE II (Rate Control Efficacy in Permanent Atrial Fibrillation II) study. J Am Coll Cardiol. 2011;58:1795–1803.
25. Bianchi S, Rossi P, Della Scala A, Kornet L, Pulvirenti R, Monari G, Di Renzi P, Schauerte P, Azzolini P. Atrioventricular (AV) node vagal stimulation by transvenous permanent lead implantation to modulate AV node function: safety and feasibility in humans. Heart Rhythm. 2009;6:1282–1286.
26. Plisiene J, Blumberg A, Haager G, Knackstedt C, Latsch J, Norra C, Arndt M, Tuerk S, Heussen N, Kelm M, Predel HG, Schauerte P. Moderate phys-ical exercise: a simplified approach for ventricular rate control in older patients with atrial fibrillation. Clin Res Cardiol. 2008;97:820–826.
27. Wijffels MC, Kirchhof CJ, Dorland R, Power J, Allessie MA. Electrical remodeling due to atrial fibrillation in chronically instrumented conscious goats: roles of neurohumoral changes, ischemia, atrial stretch, and high rate of electrical activation. Circulation. 1997;96:3710–3720.
28. Lu Z, Scherlag BJ, Lin J, Niu G, Fung KM, Zhao L, Ghias M, Jackman WM, Lazzara R, Jiang H, Po SS. Atrial fibrillation begets atrial fibrilla-tion: autonomic mechanism for atrial electrical remodeling induced by short-term rapid atrial pacing. Circ Arrhythm Electrophysiol. 2008;1: 184–192.
29. Linz D, Mahfoud F, Schotten U, Ukena C, Neuberger HR, Wirth K, Böhm M. Renal sympathetic denervation suppresses postapneic blood pres-sure rises and atrial fibrillation in a model for sleep apnea. Hypertension. 2012;60:172–178.
30. de Vos CB, Nieuwlaat R, Crijns HJ, Camm AJ, LeHeuzey JY, Kirchhof CJ, Capucci A, Breithardt G, Vardas PE, Pisters R, Tieleman RG. Autonomic trigger patterns and anti-arrhythmic treatment of paroxysmal atrial fibril-lation: data from the Euro Heart Survey. Eur Heart J. 2008;29:632–639.
31. Ogawa M, Zhou S, Tan AY, Song J, Gholmieh G, Fishbein MC, Luo H, Siegel RJ, Karagueuzian HS, Chen LS, Lin SF, Chen PS. Left stellate ganglion and vagal nerve activity and cardiac arrhythmias in ambulatory dogs with pacing-induced congestive heart failure. J Am Coll Cardiol. 2007;50:335–343.
32. Tan AY, Zhou S, Ogawa M, Song J, Chu M, Li H, Fishbein MC, Lin SF, Chen LS, Chen PS. Neural mechanisms of paroxysmal atrial fibrillation and paroxysmal atrial tachycardia in ambulatory canines. Circulation. 2008;118:916–925.
33. Patterson E, Lazzara R, Szabo B, Liu H, Tang D, Li YH, Scherlag BJ, Po SS. Sodium-calcium exchange initiated by the Ca2+ transient: an arrhythmia trigger within pulmonary veins. J Am Coll Cardiol. 2006;47:1196–1206.
34. Kühlkamp V, Schirdewan A, Stangl K, Homberg M, Ploch M, Beck OA. Use of metoprolol CR/XL to maintain sinus rhythm after conversion from persistent atrial fibrillation: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol. 2000;36:139–146.
35. Jayachandran JV, Sih HJ, Winkle W, Zipes DP, Hutchins GD, Olgin JE. Atrial fibrillation produced by prolonged rapid atrial pacing is associated with heterogeneous changes in atrial sympathetic innervation. Circulation. 2000;101:1185–1191.
36. Chang CM, Wu TJ, Zhou S, Doshi RN, Lee MH, Ohara T, Fishbein MC, Karagueuzian HS, Chen PS, Chen LS. Nerve sprouting and sympathetic hyperinnervation in a canine model of atrial fibrillation produced by pro-longed right atrial pacing. Circulation. 2001;103:22–25.
37. Yang SS, Han W, Cao Y, Dong G, Zhou G, Li WM, Gan RT, Chang HY, Wang Z. Effects of high thoracic epidural anesthesia on atrial electro-physiological characteristics and sympathetic nerve sprouting in a canine model of atrial fibrillation. Basic Res Cardiol. 2011;106:495–506.
38. Ukena C, Bauer A, Mahfoud F, Schreieck J, Neuberger HR, Eick C, Sobotka PA, Gawaz M, Böhm M. Renal sympathetic denervation for treatment of electrical storm: first-in-man experience. Clin Res Cardiol. 2012;101:63–67.
39. Vincenti A, Brambilla R, Fumagalli MG, Merola R, Pedretti S. Onset mechanism of paroxysmal atrial fibrillation detected by ambulatory Holter monitoring. Europace. 2006;8:204–210.
What Is New?
• RDN provides efficient rate control during AF and reduces duration of AF episodes. However, AF-induced AERP shortening, P-wave duration, and AF inducibility (electrical remodeling) were not altered.
What Is Relevant?
• Modulation of the autonomic system by RDN displays rate control during AF and acute antiarrhythmic effects without changing atrial refractoriness or blood pressure.
SummaryModulation of the autonomic nervous system by RDN is useful to reduce susceptibility to AF in patients with paroxysmal AF and provides efficient rate control during AF, a common comorbidity in hypertension.
Novelty and Significance
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from
Neuberger, Klaus Wirth and Michael BöhmDominik Linz, Felix Mahfoud, Ulrich Schotten, Christian Ukena, Mathias Hohl, Hans-Ruprecht
Atrial Electrical Remodeling During Atrial FibrillationRenal Sympathetic Denervation Provides Ventricular Rate Control But Does Not Prevent
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension published online November 12, 2012;Hypertension.
http://hyper.ahajournals.org/content/early/2012/11/12/HYPERTENSIONAHA.111.00182World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 1, 2018http://hyper.ahajournals.org/
Dow
nloaded from



![FEAGRO 2019 Resultado Categoria · 03.categoria campeonato bezerra menor pontos 1 [006] - dalila gentry schotten 140,00 olenca giller schotten -- rapid bay indiana gentry - et (i.a.)](https://img.pdfslide.net/doc/110x75/5e6a79a6f1c1e814b90a3a8f/feagro-2019-resultado-categoria-03categoria-campeonato-bezerra-menor-pontos-1-006.jpg)