Embed Size (px)
Citation preview

IVBImmunization Costing & Financing:
A Tool and User Guide for comprehensive
Multi-Year Planning (cMYP)
WHO/IVB/06.15ORIGINAL: ENGLISH
Immunization, Vaccines and Biologicals

IVBImmunization Costing & Financing:
A Tool and User Guide for comprehensive
Multi-Year Planning (cMYP)
Immunization, Vaccines and Biologicals
WHO/IVB/06.15ORIGINAL: ENGLISH

i i
The Department of Immunization, Vaccines and Biologicalsthanks the donors whose unspecified financial support
has made the production of this document possible.
This document was produced by theExpanded Programme on Immunization
of the Department of Immunization, Vaccines and Biologicals
Ordering code: WHO/IVB/06.15Printed: December 2006
This publication is available on the Internet at:www.who.int/vaccines-documents/
Copies may be requested from:World Health Organization
Department of Immunization, Vaccines and BiologicalsCH-1211 Geneva 27, Switzerland
• Fax: + 41 22 791 4227 • Email: [email protected] •
© World Health Organization 2006
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press,World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 3264;fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translateWHO publications – whether for sale or for noncommercial distribution – should be addressed to WHOPress, at the above address (fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning the legalstatus of any country, territory, city or area or of its authorities, or concerning the delimitation of itsfrontiers or boundaries. Dotted lines on maps represent approximate border lines for which there maynot yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended by the World Health Organization in preference to others of a similar naturethat are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguishedby initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the informationcontained in this publication. However, the published material is being distributed without warranty ofany kind, either expressed or implied. The responsibility for the interpretation and use of the material lieswith the reader. In no event shall the World Health Organization be liable for damages arising from itsuse.
The named authors alone are responsible for the views expressed in this publication.
Printed by the WHO Document Production Services, Geneva, Switzerland

i i i
Contents
Tables and figures ............................................................................................................ v
Abbreviations and acronyms ........................................................................................ vii
Acknowledgement ........................................................................................................... ix
Introduction ..................................................................................................................... xi
1. Strategic planning for immunization with costing ....................................... 1A new approach to planning for immunization ................................................. 1Why cost a cMYP? ................................................................................................ 2What are the costing linkages in the cMYP guidelines? ................................... 2What are the cMYP linkages with broader health sectorcosting exercises? .................................................................................................. 4What is the difference between costing a cMYP and the FSP? ....................... 5
2. Overview of the cMYP costing and financing tool ....................................... 6Can the tool be used in a decentralized setting? ............................................... 8Can the Tool be damaged? ................................................................................... 8What is the Tool not designed to do? .................................................................. 9Where to send feedback and seek technical support? ....................................... 9
3. Some principles and suggestions on procedure ............................................ 11
4. Important concepts, methodologies and terms............................................ 144.1 What to cost in a cMYP? ............................................................................. 144.2 What is the difference between a cost and a resource requirement? .... 164.3 What are the basic costing methodologies used? ..................................... 184.4 What are some methodological differences and limitations? .................. 21
5. Using the cMYP costing and financing tool ................................................. 235.1 Overview of the “1. Data Entry” worksheet ........................................... 235.2 Review of each data table contained in the “1. Data Entry”
worksheet ...................................................................................................... 285.3 Costing results and tables ............................................................................ 725.4 Overview of the financing and financing projections worksheets......... 775.5 Steps to complete the “4. Financing” worksheet ..................................... 78
6. Analysis of results .............................................................................................. 826.1 Analysis of past costing and financing (baseline) ..................................... 836.2 Analysis of future resource requirements, financing and gaps............... 856.3 Analysis of immunization strategies .......................................................... 906.4 Sustainability analysis .................................................................................. 91

i v
7. Scenario-building ................................................................................................ 937.1 Types of Scenario.......................................................................................... 947.2 Using the Tool for scenario-building ......................................................... 94
8. Annual monitoring using the costing and financing tool .......................... 96
9. Other uses of the costing and financing tool information ........................ 99
Annex I: Summary table of data needs and sources ........................................ 100
Annex II: Glossary of important cMYP costing terms ..................................... 107

v
Table 1: System components to cost in a cMYP ................................................ 15Table 2: Summary table of methods used in the Tool ...................................... 21Table 3: Sections and data tables of the “1. Data Entry” worksheet
of the Tool .................................................................................................. 24Table 4: Costing table design ................................................................................ 72Table 5: Examples of costing and financing scenarios to develop ................. 94Table 6: Comparative analysis of different scenario results .......................... 95
Figure 1: Costing linkages in cMYP guidelines ..................................................... 3Figure 2: Reconciling various objectives when planning for
immunization .............................................................................................. 4Figure 3: Screen shots of cMYP costing and financing tool ............................... 7Figure 4: Design of the Tool ...................................................................................... 8Figure 5: Broad elements to cost in a cMYP........................................................ 14Figure 6: Typical cost profile of an immunization programme ....................... 18Figure 7: Illustration of the detailed costing table ............................................. 73Figure 8: Illustration of the FSP style costing table ........................................... 74Figure 9: Example of baseline costing and financing graphs ............................ 83Figure 10: Example of the future resource requirements,
financing and gap graphs ....................................................................... 86Figure 11: Example of the gap analysis section of the Tool ................................ 87
Tables and figures

v i

vii
Abbreviations andacronyms
AE adverse events
AD auto-disable syringe
APR annual progress report
BCG Bacille Calmette-Guérin (vaccine)
CBAW childbearing age women
CEA cost-effectiveness analysis
cMYP comprehensive Multi-Year Plan for Immunization
cMYP Tool cMYP Costing and Financing Tool
DFID Department for International Development (UK)
DT diphtheria-tetanus (vaccine)
DTP diphtheria-tetanus-pertussis (vaccine)
EPI Expanded Programme on Immunization
FIC fully immunized children
FSP financial sustainability plan
GAVI Global Alliance for Vaccines and Immunization
GDP gross domestic product
GHE government health expenditure
GIVS Global Immunization Vision and Strategy
HepB Hepatitis B (vaccine)
Hib Haemophilus influenza type B (vaccine)
HIPC highly indebted poor country
ICC inter-agency coordinating committee
IEC information, education and communication
IMF International Monetary Fund
IMR infant mortality rate
JE Japanese encephalitis
JICA Japan International Cooperation Agency
JRF WHO-UNICEF Joint Reporting Form

viii
LCU local currency units
MDG Millennium Development Goals
MDRI multilateral debt relief initiative
MMR mumps, measles, rubella (vaccine)
MNT maternal and neonatal tetanus
MoF Ministry of Finance
MoH Ministry of Health
MTEF medium term expenditure framework
MYP Multi-Year Plan for Immunization
NGO nongovernmental organization
NHA national health accounts
NIP National Immunization Programme
OPV oral poliovirus vaccine
PRSP poverty reduction strategy papers
PW pregnant women
SI surviving infants
SIA supplemental immunization activities (campaigns)
SWAp sector wide approach
TB tuberculosis
THE total health expenditure
TT tetanus toxoid
U1P under one population
ULY useful life years
UNICEF United Nations Children’s Fund
USAID United States Agency for International Development

i x
Acknowledgements
The immunization Costing and Financing Tool and User Guide were developed bythe World Health Organization (WHO) Immunization Vaccines & BiologicalsDepartment (IVB), and is the result of team work between partners to theGlobal Alliance for Vaccines and Immunization (GAVI) which is committed to thefinancial sustainability of immunization programmes in the poorest countries.These include the Bill & Melinda Gates Foundation, the Centre for GlobalDevelopment, the Children’s Vaccine Programme at PATH, the United NationsChildren’s Fund (UNICEF), the United States Agency for International Development(USAID), the World Bank, and the World Health Organization.
WHO is grateful to members of the GAVI Financing Task Force who have supportedthis effort.

x

x i
Introduction
Responding to global immunization challenges, including the need to protect morepeople and introduce new vaccines, and in consultation with their other partners,the World Health Organization (WHO) and the United Nations Children’s Fund(UNICEF), developed the Global Immunization Vision and Strategy (GIVS) for theperiod 2006–2015. GIVS is a framework that offers policy-makers and stakeholdersa unified vision of immunization and a set of strategies from which countries canselect those most suited to their specific needs. In conjunction with GIVS, and as away of implementing GIVS at national level, countries are encouraged to developtheir own comprehensive Multi-Year Plans (cMYP) for immunization.
In 2005, in conjunction with their GAVI partners, WHO and UNICEF developedthe Guidelines for Developing a Comprehensive Multi-Year Plan (cMYP) forimmunization1 as a means of providing support for countries to improve theirimmunization planning. This new approach was guided by the need to simplify andharmonize the proliferation of varied immunization planning activities at nationallevel, which in turn had lead to duplication of effort, high transaction costs for nationalpartners and those with variable degrees of national ownership, and a lack of alignmentwith national systems. Through the GIVS initiative and framework, the cMYP processis expected to streamline immunization planning process at national level into a singlecomprehensive and costed plan. It is within this context that these new guidelinesbuild on existing multi-year planning experience, while adding the critical elementsof costing and financing by drawing heavily upon the methods developed for theimmunization financial sustainability plans (FSPs). In the same way it is hoped thatthe costing and financing exercise will build on FSP costing tools and methodologies.
In developing these guidelines it was broadly recognized that strategic planning forimmunization would require credible information on how much was being spent,what it was being spent on, from which source, and how much future funding wouldbe needed to reach programme objectives. Analysing the costing and financing of acomprehensive Multi-Year Plan (cMYP) is therefore a key step in the planning processof a national immunization programme (NIP).
1 See www.who.int/immunization_financing/tools) or WHO Department of Immunization Vaccinesand Biologicals (IVB) Documents Centre, reference (WHO/IVB/05.20).

xii
To help undertake the costing and financing elements of a cMYP, a MicrosoftExcel-based tool was developed — the cMYP Costing and Financing Tool — tomake it easy to estimate past costs and financing for immunization, to aid in makingfuture projections of resource requirements and financing, and for analysing thecorresponding financing gaps in reaching immunization programme objectives.The Tool is accompanied by this comprehensive User Guide which provides anoverview of important concepts, methodologies and definitions. It also providesstep-by-step instruction on how to use the cMYP Costing and Financing Tool,guidance on sources of information, and results analysis, as well as interpretation offindings.
The User Guide is structured as follows:
• introduction on strategic planning for immunization and costing;
• overview of the costing and financing tool;
• suggestions on procedures;
• basic concepts, methodologies and terms;
• how to use the costing and financing tool;
• how to analyse the results and interpret findings;
• how to develop alternative scenarios for costing and financing;
• how to use the tool for annual monitoring;
• other uses of the information from the costing and financing tool;
• annexes of reference summary table of data needs, sources, and terminology.
While the Tool and User Guide are principally targeted towards national immunizationprogramme managers in the context of developing a comprehensive multi-year plan,they can also be used by researchers, consultants, international donors, and otherhealth planners in developing countries. No prior experience or formal training inhealth economics is necessary for using the cMYP Costing and Financing Tool andunderstanding its User Guide.
The intention is that these materials will be continually improved and updated.We therefore recommend that the User regularly visit the website to obtain thelatest versions: at www.who.int/immunization_financing/tools.

1WHO/IVB/06.15
A new approach to planning for immunization
Responding to global immunization challenges, including the need to protect morepeople and introduce new vaccines, WHO and UNICEF, in consultation with otherpartners, have developed the Global Immunization Vision and Strategy (GIVS) forthe period 2006—2015. GIVS is a framework that offers policy-makers andstakeholders a unified vision of immunization and a set of strategies from whichcountries can select those most suited to their specific needs.
In conjunction with GIVS, countries are encouraged to develop a cMYP forimmunization. Yet to date, the planning experience at country level for immunizationhas revealed many shortcomings: plans are based upon a review of past achievementsand problems; they are not sufficiently forward-looking; there are separate plans foreach initiative or target disease; plans may be developed to fit particular fundingproposals rather than reflecting country priorities; plans are not well costed to identifyclear funding needs and resources gaps; and many plans have very little linkageswith the broader health sector or macroeconomic context.
This experience has taught us that planning needs to reflect country priorities,to be aligned with country planning cycles, and to simplify and harmonize procedures.To address these issues, the WHO and UNICEF cMYP process for immunizationbegan in 2005 with the formulation of new guidelines and tools. Through the GIVSinitiative and framework, efforts have begun to streamline the immunization planningprocess at country level into a single comprehensive and costed plan.
In summary, the WHO-UNICEF Guidelines for Developing a ComprehensiveMulti-Year Plan for Immunization provides a new approach to planning that:
• ensures that the strategies in the plan are sufficiently comprehensive;
• integrates and consolidates activities with other health interventions and withinthe immunization programme to solve shared problems;
• plans by immunization system components rather than by disease or initiative;
• evaluates the costs and financing of the cMYP to ensure the improved financialmanagement sustainability of the programme;
• links annual work plans to the multi-year plan;
• links to the broader health sector planning and budgeting processes.
1. Strategic planning forimmunization with costing

cMYP Costing & Financing Tool – User Guide2
Why cost a cMYP?
It is broadly recognized that strategic planning for immunization requires credibleinformation about cost to achieve the programme objectives, estimate availablefunding, allocate funds within the programme, and avoid funding shortfalls.For this reason, analysing the costing and financing of a cMYP is a key step in theplanning process. Indeed, the costing of a cMYP is thought to:
1) Strengthen national budgeting and planning for immunization and help answerthe fundamental questions of how much it will cost to reach programmeobjectives, who will pay for these needs, and how to prioritize activities basedon available funding?
2) Help in decision-making about programme improvements. An example wouldbe understanding the cost implication of introducing new vaccines. A baselinecosting of the programme would enable the development of scenarios forimprovements, and understanding the incremental costs of such improvements.
3) Generate information that will help advocacy and mobilize the resources neededfor vaccines and immunization. A solid understanding of the funding gaps canfacilitate discussion with ministries and donors on how to mobilize the resourcesrequired for the programme.
What are the costing linkages in the cMYP guidelines?
The WHO-UNICEF Guidelines for Developing a Comprehensive Multi-Year Planfor Immunization2 provides a series of steps to developing a comprehensive plan.Step 6 of these guidelines relates to analysing the costs, financing, and financial gapsin a cMYP. Note that the basis of the costing should be the programmatic objectivesand milestones defined during Steps 1 to 3.
1 See www.who.int/immunization_financing/tools) or WHO Department of Immunization Vaccinesand Biologicals (IVB) Documents Centre, reference (WHO/IVB/05.20).

3WHO/IVB/06.15
Figure 1: Costing linkages in cMYP guidelines
Step 2 - Developing and prioritizing national objectives and milestones
Step 3 - Planning strategies for each system component
Step 6 - Analyzing the costs, financing, and financial gaps in the cMYP
Programmatic Objectives Costing Objectives
Step 11 - Establishing the timelines, responsible units and financial resources
Step 1 - Conducting a situational analysis
1. Health sector analysis2. Estimating costing and financing of the cMYP3. Scenario building using the costing tool4. Interpreting costs, financing and gap results5. Developing financial sustainability strategies6. Financial sustainability indicators and targets
In broad terms, Step 6 has six components to it. The first is to undertake a diagnosisof the macroeconomic and health sector environment in which the immunizationprogramme operates. This diagnosis recommends exploring three areas: (1) trendsin government financing of health services; (2) the planning and budgeting processesfor the health sector; (3) current or potential reforms which may have an impact onthe immunization programme. Such a diagnosis will strengthen any projections offuture financing for immunization, and assessment of the reliability of future funding.
The second and third components of Step 6 are to estimate the baseline costing andfinancing of the immunization programme, making future projections of resourcerequirements based on the programmatic objectives defined under Steps 1 to 3 of thecMYP, and to develop alternative scenarios for resource requirements and financing.
The fourth component of Step 6 is to analyse the results and interpret the findings,particularly with regard to the financing gaps for immunization. Lastly, identifyingstrategies and indicators that will help you move towards financial sustainability arethe final components of Step 6.

cMYP Costing & Financing Tool – User Guide4
What are the cMYP linkages with broader health sector costing exercises?
Neither strategic planning for immunization, nor its costing, has ever been an easyprocess. The immunization programme is one of many components of a country’shealth system. It is supported by a broad range of national and international partnersand actors that can have differing objectives and needs, and might view planning forimmunization within a different lens and context (see the diagram below).
Figure 2: Reconciling various objectives when planning for immunization
MoH Policy
GAVI
MoF Priorities
World
EPI objectives
New vaccine introduction,
increasing coverage…
Polio, measles, campaigns,outbreaks,
surveillance…
Poverty Reduction (MDG, PRSP,
MTEF…)
Health Sector Planning,
integration, SWAp…
Bank
For example, the Ministry of Finance (MoF) might view immunization in the contextof the Millennium Development Goals (MDG), or how it can contribute to povertyreduction. Thus any strategic planning for immunization should fit into these broaderobjectives as laid out in the MDG’s, and any budgeting for immunization wouldneed to appear in the relevant national budgeting processes such as a medium termexpenditure framework (MTEF).
The Ministry of Health (MoH), on the other hand, would view immunization in thecontext of the broader health sector objectives and planning processes. The nationalimmunization programme may have its own specific planning and budgetingobjectives, and these can be different from those of the international agencies andinitiatives supporting the programme.

5WHO/IVB/06.15
Although the different planning processes and objectives are not necessarily incompetition, reconciling all these in the context of a strategic plan for immunizationis not an easy task, and it is therefore important that objectives and priorities arealigned. Similarly, the costing information generated through the cMYP developmentshould link to the relevant consolidated costing and budgeting plan for the healthsector. If applicable, it can be useful to link various ongoing exercises such as:poverty reduction strategy papers (PRSP); health sector and public expenditurereviews; budgeting, allocation, and expenditure (MTEF, NHA); and externalsupport and resource mobilization processes (such as donor round tables, SWAp,etc.). This has the effect of increasing the visibility of immunization during healthsector planning processes and can increase the chances of mobilizing the resourcesneeded for the programme.
Because the relevant planning cycles and costing/budgeting exercises for the healthsector differ between countries, and budgeting formats can also vary from one countryto the next, it is not possible to develop a costing template that will fit every existingsituation. To reconcile this difficulty, the cMYP Costing and Financing Toolincludes a costing table that provides the most disaggregated level of costing possible.This facilitates how specific budget lines in the cMYP costing table can be linkedand matched to budget lines in another. [More on the costing table is available inPart 5.3]. Also, the period covered by resource estimation should be set forfive years, as with a longer timeframe, more assumptions need to be made for futureprojections, and estimates become unreliable. Minimum five-year projections thereforeseem useful, especially when linked to annual operational plans and allocations.
What is the difference between costing a cMYP and the FSP?
The new guidelines build on existing multi-year planning experience, while addingthe critical elements of costing and financing, by drawing heavily upon the methodsdeveloped for the immunization FSP. In the same way, the costing and financingexercise builds on FSP costing tools and methodologies. Thus, for countries eligiblefor support from GAVI and the GAVI Fund, it is likely that an FSP has been developedusing the Guidelines for Preparing a National Immunization Programme FinancialSustainability Plan, and related tools developed by the GAVI Financing Task Force.
If this is the case, the costing exercise of the cMYP will be greatly facilitated.The cMYP Costing and Financing Tool and User Guide is a variation of theFSP Costing, Financing and Gap Analysis Tool (available on www.who.int/immunization_financing/tools), and it applies the same principles, concepts andmethodologies.
It is also possible that most of the costing data used in the FSP costing tool is applicableto the cMYP costing tool and can be updated to reflect the appropriate changes. Forassistance with transferring the data from the FSP to cMYP costing tool, contactyour regional counterpart, or send an email to [email protected].

cMYP Costing & Financing Tool – User Guide6
The cMYP Costing and Financing Tool (referred to as the Tool throughout theremainder of this User Guide) is a Microsoft Excel-based template that containseight worksheets:
0) Print & Read Me
1) Data Entry
2) Calculations
3) Costing
4) Financing
5) Gap & Indicators
6) Graphs
7) Sustainability
Of the eight worksheets, only two require data input
The “1. Data Entry” worksheet is where you need to enter all the data for thecosting and resource requirements projections. The worksheet contains a series ofdata entry tables for the calculation of vaccines, injection supplies, personnel,vehicles and transport, cold chain and maintenance, supplemental immunizationactivities, other recurrent and capital costs, and other costs not specified elsewhere.Given the importance of this worksheet, Parts 5.1 and 5.2 of the User Guide arededicated to explaining how to complete the worksheet and how to find the requireddata.
The data on past and future financing is entered in the “3. Financing” worksheets.Some suggestions on procedures to collect financing information is provided inParts 5.4 and 5.5 of the User Guide and in Annex I.
2. Overview of the cMYPcosting and financing tool

7WHO/IVB/06.15
Figure 3: Screen shots of cMYP costing and financing tool
1. Data entry worksheet 3. Costing worksheet
5. Gap and indicators worksheet 6. Graphs
The remaining worksheets are automatically generated based on the informationentered in the “1. Data Entry” and “4. Financing” worksheets.
The “2. Calculations” worksheet consolidates the formulas that convert theinformation and data provided in the “1. Data Entry” worksheet into thecosting and estimates for resource requirements. The broad underlyingmethodology used in the “2. Calculations” worksheet is described in Part 4of the User Guide.
The “3. Costing” worksheet is linked to the “2. Calculations” worksheet andpresents the results by means of various costing tables. These costing tablesare described in Part 5.3 of the User Guide.
The “5. Gap & Indicators” worksheet is linked to the “4. Financing” worksheetand generates a summary table of costs, future resource requirements,financing and gaps needed for complete financial diagnosis of the cMYP.This worksheet automatically calculates a range of indicators that should beused in the analyses. It contains several tables presenting year-to-year variationof secure and probable financing, and makes overall estimates for the financinggaps and how they will evolve over time. These indicators are explained inParts 6.1 and 6.2 and in the Annex to the User Guide.
The “6. Graph” worksheet is linked to numerous other worksheets inthe Tool and contains a number of automatically generated charts and graphsneeded for analyses. This worksheet contains charts that plot thefuture resource-requirement profiles and the future financing and gap profiles.These help clarify the level of resource requirements needed by the NIP,and also what financing will be available in the future. More information isavailable in Parts 6.1 and 6.3 of this User Guide.

cMYP Costing & Financing Tool – User Guide8
The “7. Sustainability” worksheet is linked to numerous other worksheets inthe Tool and contains a number of automatically generated macroeconomicand financial sustainability indicators that can be used for the analyses.More information is available in Part 6.4 of the User Guide.
Note that all the worksheets in the Tool are printer friendly.
Figure 4: Design of the Tool
Data Collection
1. Data Entry Worksheet
Data on Financing
4. FinancingWorksheet
Data on Inputs & Activities
Calculation Worksheet
Costing & Activities
Financing Tables
Gap, Indicators, Graphs and Sustainability Worksheets*
* Automatically generated worksheets
Can the tool be used in a decentralized setting?
It is important to note that the Tool allows for a generalized approach but can becustomized to fit a particular country situation or context. For instance, it is notrestricted to any particular country administrative level. In a decentralized setting,different parts of the Tool may need to be used at different levels of the system(sub-nationally). This may be of particular relevance in large country settings andwhere data collection needs to be undertaken at lower levels in the system.
Can the Tool be damaged?
Owing to its intricate linkages and formulas, the Tool is very sensitive toany formatting changes (adding/deleting cells, rows or columns) or editing(cut, copy and standard pasting of information from different sources). In order toprotect it from any damage caused by formatting or editing changes, protectivemeasures have been put in place and the worksheets are also password-protected.More detailed information about Tool protection and passwords is provided inPart 5.1 of this User Guide.

9WHO/IVB/06.15
What is the Tool not designed to do?
The main purpose of the Tool is to provide assistance for the costing and financingelements of a cMYP, and to make projections of future resource requirements andfinancing to achieve the programme objectives. However, the Tool currently hasthree areas of limitation.
1) The first is that it was not designed for cost-effectiveness analysis (CEA) whichcan assist in evaluation and comparison for alternative uses of scarce resources.Although defining programme objectives and strategies during the developmentof a cMYP should be based on cost-effectiveness considerations (particularlyin relation to new vaccine introduction), the Tool, in its current design,is ill equipped to strengthen such a priority- setting exercise. Likewise,the Tool is not designed to determine allocative efficiency, when a criticalconsideration in any planning and budgeting exercise must be the efficient useof funds.
2) The second limitation is that, in its current format, the Tool does notautomatically factor in any scale effect. Ideally, costs would vary as the scaleof immunization interventions changed. For instance, in economies of scale,costs would decrease as the scale (such as coverage) increased, as fixed inputs(such as buildings) were used more efficiently. There could however also bedis-economies of scale, whereby costs increase proportionally if the last peopleto be reached and immunized live in areas that are difficult to access.There can even be economies of scope, when combining interventions resultsin cost savings. While techniques and methodologies are rapidly becomingavailable for a global level costing exercise where scale-up effects can beincluded, these have not yet been assimilated in this Tool. In the meantime,any scale effect needs to be done manually.
3) Finally, the Tool is immunization specific, and is therefore not adapted to includethe costing of other health interventions. Moreover, it has limited linkage withother existing tools available for costing health intervention programmes andpackages of services.
Work is ongoing to improve the Tool and to overcome these limitations.
Where to send feedback and seek technical support?
We welcome questions and comments on the Tool and User Guide. We have triedto identify any inconsistencies in the system, but if you discover any errors,encounter any problems, or have any suggestions on how to improve these materials,we encourage you to bring these to our attention. Please direct your comments to:
The World Health OrganizationDepartment of Immunization, Vaccines & BiologicalsExpanded Programme on Immunization20 Avenue AppiaCH -1211 Geneva [email protected].

cMYP Costing & Financing Tool – User Guide10
For questions, comments and technical assistance related to the development of acMYP, contact your Regional Office. For general information on submitting thecMYP as part of a GAVI funding application, visit the GAVI website atwww.vaccinealliance.org.
More general information on immunization financing is available at www.who.int/immunization_financing.

11WHO/IVB/06.15
Before starting the cMYP costing and financing exercise, several principles shouldbe noted. The first is the importance of creation of leadership and ownership of thecMYP development process within the immunization department of your MoH.It is equally important to inspire commitment and buy-in to the process, priorities,and strategies for immunization, from the stakeholders represented on theinter-agency coordinating committee (ICC). Because any costing and financingresource requirement projection exercise will invariably be based on manyassumptions, limited data and future uncertainties mean that these assumptions needto be fixed upon in close cooperation and agreement with all stakeholders so that thefinal estimations for the cMYP will be credible, acceptable, and useful.
Unfortunately, there is no blueprint for the process, and therefore considerable timecan be taken up tailoring the cMYP costing and financing exercise to each individualcountry. The exercise cannot be done in isolation and will need the collaboration ofcolleagues in the MoH and the MoF, as well as all development partners supportingimmunization, for data collection, analysis feedback, and review.
The second principle is the importance of putting together a good team to work onthe cMYP costing and financing exercise. It will need to be composed of the rightpeople, with the right skills, and it will need the right amount of time to complete theexercise. A focused and manageable group is needed of no more than three people.It will also be important to decide on who will lead and who will coordinate theteam.
Below are some suggestions on steps and procedures for the team.
1) The cMYP development team should read the WHO-UNICEF Guidelines forDeveloping a Comprehensive Multi-Year Plan for Immunization2 payingparticular attention to Step 6 - Analyzing the costs, financing, and financialgaps in the cMYP. Discuss the steps so that the group fully understands thetask in hand, how the costing steps of the cMYP development will inform theoverall financial sustainability planning for the NIP, and also what needs to bedone to achieve these objectives.
3. Some principles andsuggestions on procedure
2 Available on www.who.int/immunization_financing/tools) or from WHO Department ofImmunization Vaccines and Biologicals (IVB) Documents Centre, reference (WHO/IVB/05.20).

cMYP Costing & Financing Tool – User Guide12
2) Read the User Guide to understand the methodologies, key concepts andterms needed, and to obtain step-by-step instructions on how to usethe Tool and where to obtain the necessary data. The latest versions ofthe Tool and User Guide are available for download at www.who.int/immunization_financing/tools. Because these materials will be constantlyimproved and updated, it is important to visit the website regularly to obtainthe latest version.
3) Review the objectives, strategies, and macroeconomic/health-sector contextdeveloped for your cMYP, and determine what will constitute your baselinescenario for the costing. For example, the baseline scenario needs to includethe same coverage objectives, immunization schedule and expansion,and the same timing of specific campaigns as those defined in the cMYP.Also, activities that are specified in the cMYP should be budgeted for in theTool (e.g. expanding the cold chain, strengthening outreach services, etc.).
4) Review the “1. Data Input” worksheet of the Tool to determine what data isneeded and how best to collect it. Collecting and synthesizing data can bedifficult since information- sharing among external development agenciesinvolved in health, and the different ministries and their internal departments,may be weak. It may be more useful to print the entire worksheet to use as adata-collection instrument. This way the different data tables can be distributedto those people that will be collecting the data or who will be providing theinformation. Refer to Annex I of this User Guide for suggestions as to whereto find data for the costing, or techniques for estimating data needs.
5) Once all the data on inputs and activities has been collected, these should beentered in the appropriate tables of the “1. Data Entry” worksheet.Review this worksheet carefully for any errors in data entry, or any omissionsor oversights of data needs for the tables. Remember that the Tool is password-protected so data should not be pasted into the “1. Data Entry” worksheetfrom another Excel worksheet. This could damage formulas, provide wrongresults, or render the Tool useless.
6) Review the results of the costing in the “3. Costing” worksheet.Close inspection of the tables may yield strange results. This could be due toerrors in the data, or data entry into the Tool, or omissions of required datainputs. These should be reviewed. It can also happen that costing results donot appear in the costing table. If this is the case, it could be due to importantinformation not having been entered into the “1. Data Entry” worksheet.
7) Double-check the work as often as you think necessary. Remember to savethe work frequently — this updates the file and helps to ensure that you do notlose significant amounts of data once it is entered in the Tool.
8) After completion of the data and entry in the “1. Data Entry” worksheet,a first analysis should be made of the results obtained. Parts 6.1 to 6.4 of thisUser Guide offer suggestions on how to analyse the findings. Ensure review ofthe “5. Gaps & Indicators” and “6. Graphs” worksheets of the Tool.It is important to make a first analysis so that the team can present the resultsand validate them with a broader group, such as the ICC.

13WHO/IVB/06.15
9) Once the costing of the cMYP is finalized, and estimates have been made forfuture resource requirements, the team will need to collect information onpast and future financing. This information should be entered in the“4. Financing” worksheets. For future financing, it is important toclassify the funding according to its level of risk - secure versus probable.Suggestions on how to collect financing data are developed in Parts 5.4 and5.5 of the User Guide.
10) Once the financing data is entered in the Tool , the work should bedouble-checked for any mistakes or results that merit double-checking.To identify errors, it can be helpful to review the “5. Gap & Indicators” and“6. Graphs” worksheets. Once the team is happy with the results and thesehave been double-checked for errors, the Tool can be saved as the baselinescenario.
11) A second analysis of the results should be made by comparing theestimated resource requirements and available funding — the difference beingthe funding gaps needed to meet desired programme objectives. Again, it canbe helpful to review the “5. Gap & Indicators” and “6. Graphs” worksheetsin the analysis.
12) Using the baseline scenario, the team may be interested in exploring alternativesto evaluate what impact a change in cMYP objective may have on projectedresource requirements, financing and gaps. Various scenarios can be developed,and guidance on this is provided in Parts 7.1 and 7.2 of this User Guide.

cMYP Costing & Financing Tool – User Guide14
This section of the User Guide provides important background information aboutbasic costing concepts, methodologies and terms. Before starting the cMYP costingand financing exercise, it is essential to become familiar with these.
4.1 What to cost in a cMYP?
The costing exercise needs to account for all the inputs and activities designed tocarry out the strategies needed to reach the programme objectives, as defined in thecMYP.
Figure 5: Broad elements to cost in a cMYP
4. Important concepts,methodologies and terms
cMYPObjectives
Strategies
Inputs(e.g. vaccines)
Activities(e.g. training)
The table below illustrates the types of inputs and activities that are usual in animmunization programme. These are linked to the five system-components definedin the WHO-UNICEF Guidelines for Developing a Comprehensive Multi-Year Planfor Immunization.

15WHO/IVB/06.15
Table 1: System components to cost in a cMYP
System Components Inputs Activities
1. Service delivery Human resources/salaries, outreach Training, workshops, etc.per diems, fuel for transport, operationalcost of campaigns, etc.
2. Advocacy and communication Information, education and Social mobilization, IEC, developingcommunication (IEC) materials, advocacy and communication plansuch as posters, etc.
3. Surveillance Surveillance and laboratory equipment Surveillance activities (sentinel sites,outbreak investigation, etc.)
4. Vaccine supply, quality and Vaccines, auto-disable (AD) syringes, Monitoring, vaccine stocklogistics safety boxes, other injection supplies, management activities
cold-chain equipment, vehicles, spareparts, incinerators, etc.
5. Programme management Computers, office supplies, etc. Meetings, planning, research, datamanagement, expanded programmeon immunization (EPI) reviews,cold-chain assessment, etc.
The Tool is designed around this framework and requires the necessary data entry tocalculate the costs and resource requirements for inputs and activities relevant toeach immunization programme. This is described in more detail in Parts 5.1 to 5.5 ofthis User Guide.
At minimum, it is important to estimate the costs, financing and future resourcerequirements of each cMYP for all immunization-specific inputs and activities.All inputs and activities that are shared with the immunization programme, such aspersonnel, transportation and buildings, are optional.
What is the difference between an immunization-specific input and a shared input?
Immunization-specific costs include the value of inputs and activities that are used specifically for immunization.In other words, their utilization is 100% for the NIP. Typically, immunization-specific recurrent inputs include:vaccines; injections supplies; full time immunization personnel (including outreach and supplemental immunizationactivities); transport costs incurred by the NIP (e.g. fuel and maintenance cost of the vehicles owned by the NIP);training activities; social mobilization; surveillance activities, etc. On the other hand, immunization-specific capitalinputs can include vehicles and cold-chain equipment to be used specifically for the NIP, together with other inputsused specifically by the programme (e.g. waste disposal, etc.). A complete listing and definition of the immunization-specific inputs are found in Annex II at the end of this User Guide.
Shared costs include the value of inputs that are not specific to immunization and which are used by differentprogrammes or activities in the health sector — i.e. their utilization for immunization is less than 100%. For instance,a nurse working in a district health centre is likely to be providing immunization services as well as other curativeand preventive services. Only a portion of that nurse’s salary and time can be attributable to immunization.Likewise, a vehicle in a district health centre (such as a four-wheel drive), may be used by staff working forprogrammes other than immunization, such as malaria or tuberculosis (TB) programmes. Therefore, only aportion of the fuel and maintenance cost of these vehicles will be paid for by the NIP. This makes it difficult toseparate out the portion of these inputs that can be attributed to immunization. These are classified as shared costs.The use of buildings such as health centres are other typical shared inputs.

cMYP Costing & Financing Tool – User Guide16
Given the relative difficulty in collecting information on shared costs in a programmeand the fact that these costs are not tied to funding that is specifically set aside forimmunization (the most relevant for the cMYP costing and financing exercise),the estimation of shared costs is optional.
However, we strongly recommend that these shared costs are taken intoaccount, since in most countries shared inputs are likely to be quite significant.The added investment in time will result in a more accurate costing exercise.By excluding the shared inputs, the analysis will: (a) underestimate the truegovernment contribution to immunization since many of the shared inputs tend tobe funded from national resources (especially for personnel costs); (b) underestimatethe total cost/resource requirements of the programme if other inputs (such as vehicles)are frequently shared with other programmes.
The Tool has been set up to allow for the calculation of shared inputs, if so desired.The process whereby the shared portion of a shared cost is separated out, is knownas cost allocation, and the main method used is to allocate shared inputs to aprogramme based on the percentage time spent on immunization.
Finally, estimations of costs, financing and future resource requirements should bemade for a particular set of years or time period.
• One past year. The rationale for looking at a past year is to have a baselinereference year from which comparisons can be made between how much theprogramme currently costs, and what will be the future resources required.
• Between 3 and 5 future years. This is considered the standard period formaking future projections of costs and resource requirements in a comprehensivemulti-year plan (cMYP), especially if this is linked to annual operational plans.
• Optional forecast (beyond 5 years). In some instances, it may be useful toforecast the costs and resource requirements for the programme beyond the3–5 year planning cycle of the cMYP. This is explained in greater depth inParts 7.1 and 7.2 of the User Guide. Note that in the case of a longer timeframe,more assumptions have to be made regarding the possible unreliability of futuretrends and estimates.
4.2 What is the difference between a cost and a resource requirement?
So far, the terms cost and resource requirement have been used interchangeably,but it is important to clarify the difference between them. Generally speaking,a costing exercise is associated with a retrospective analysis (past year),whereas resource requirements are associated with a prospective analysis of futureprojections (3–5 future years).
In the Tool, the distinction between the term “cost” and the term “resourcerequirement” relates to how capital equipment is treated. Capital costs reflect inputsthat are not consumed or replaced in one year or less (e.g. a vehicle or cold-chainequipment). In most cases, the treatment of recurrent inputs is the same whetherreferring to cost or resource requirements, although some differences in thecalculation for vaccines will be mentioned in Part 4.5.

17WHO/IVB/06.15
What is the difference between a capital and a recurrent cost?
A capital cost corresponds to an input that has a useful life of more than one year. In other words, these are inputsthat are not consumed or replaced every year. The capital cost categories used in the Tool include the following:vehicles; cold-chain equipment; and other immunization-specific equipment (e.g. waste disposal). The suggestedmethod for the treatment of capital cost is a simple straight line depreciation, i.e. the value of the new equipment isdivided by its number of useful life years (ULY).
A recurrent cost corresponds to an input that will be consumed or replaced in one year or less. The recurrentcost categories used in the cMYP include the following: vaccines; injection supplies; personnel; transport; maintenanceand overheads; training; social mobilization/IEC; surveillance and monitoring. Refer to Annex II at the end of thisUser Guide for a complete definition of these cost categories.
When the term cost or cost projection is used it implies that the value ofcapital equipment is depreciated (or amortized) over its lifetime — known as usefullife years (ULY). In other words, the value of the capital equipment is spread outover the number of years it will be used and brought to an annual equivalent.Once the capital equipment is older than its number of ULY, the equipment isconsidered to be fully depreciated (or amortized). This means that it no longer has afinancial value.
To simplify the calculation, the methodology used in the Tool recommendsusing standard ULY for equipment (five years for vehicles, cold chain and other suchitems, and 25 years for buildings). Even if the equipment is older than five years andis still being used by the programme, the Tool considers this item to be completelydepreciated with zero financial value. It is possible to choose alternative values ofULY.
The first advantage of depreciating (or amortizing) capital equipment when makingcost estimates and cost projections, is that their value can be added to the recurrentcosts for an accurate estimation of the total annual cost – recurrent inputs are thosethat will be consumed or replaced in one year or less (e.g. vaccines, salaries, etc.).A second advantage is that important cost indicators can be computed with indicatorsthat are comparable over time (e.g. annual variations in the cost per capita, cost perfully immunized child or the cost as a percentage of gross domestic product (GDP)).
However, as the object of the exercise is to calculate the financial resources that willneed to be mobilized each year to reach the cMYP objectives, and also who will fundthese needs over time, the costing approach described above has certain limitations.For example, suppose that next year, there is a need to purchase 10 new refrigeratorsfor the cold chain. Even if these refrigerators will last several years, it will still benecessary to mobilize all the funds in the next year to buy the 10 refrigerators.Taking the costing approach, you will underestimate the true financial resourcesthat are needed in that particular year. This is the rationale for the resourcerequirements approach.

cMYP Costing & Financing Tool – User Guide18
When the term resource requirements is used (sometimes referred to as resourceneeds), it implies that the full purchase cost of new units of capital equipment will beaccounted for. Since this assumes that the existing equipment has already been paidfor, the resource requirements approach is most relevant when looking at exactamounts of financing that need to be mobilized each year. This approach allows forcomparisons between resource requirements and needed financing, and also howthe two need to be matched in order to reduce any financial gaps.
4.3 What are the basic costing methodologies used?
Broadly speaking, the Tool employs three methods for costing and making projectionsof future resource requirements.
The first method is known as the ingredients approach where the value of an inputis based on quantities, unit prices and percentage use for immunization — these arethe ingredients. As vaccines, injection supplies, personnel, transport, vehicles,and cold-chain equipment account for the bulk of the cost/resource requirement ofan immunization programme (at least 80% of the total), considerable emphasis isgiven to assessing these inputs accurately. If not, small inaccuracies in the estimationscould translate into large over- or under-estimations of the total cost/resourcerequirement.
Figure 6: Typical cost profile of an immunization programme
29%
10%
16%7%
19%
5%
14%
Vaccines
Injection Supplies
Personnel
Transport
Other recurrent costs
Vehicles
Cold Chain

19WHO/IVB/06.15
The basic methodology for calculating these inputs is based on the formulas listedbelow.
1) Past costing
• Recurrent (RCx, Yi) = existing quantities (RCx, Yi) x US$ price (RCx, Yi) x percentageuse for immunization (RCx, Yi)
• Capital (CCx, Yi) = [existing quantities (CCx, Yi) x US$ price (CCx, Yi)]/ULY(CCx, Yi)x percentage use for immunization (CCx, Yi)
• Total cost = sum of all recurrent costs + sum of all capital costs
2) Future resource requirements
• Recurrent (RCx, Yi) = future quantities needed (RCx, Yi) x US$ (price (RCx, Yi) xΩ) x percentage use for immunization (RCx, Yi)
• Capital (CCx, Yi) = future quantities needed (CCx, Yi) x (US$ price (CCx, Yi) x Ω)x percentage use for immunization (CCx, Yi)
• Total resource requirements = sum of all recurrent resource requirements+ sum of all capital resource requirements
3) Cost Projections — to compare between past cost and future resourcerequirements
• Recurrent (RCx, Yi) = future quantities needed (RCx, Yi) x (US$ price (RCx, Yi) xΩ) x percentage use for immunization (RCx, Yi)
• Capital (CCx, Yi) = [ (existing + future quantities needed (CCx, Yi) ) x(US$ price (CCx, Yi) x Ω)] / ULY (CCx, Yi) x percentage use for immunization
(CCx, Yi)
• Total cost projections = sum of all recurrent cost projections + sum of allcapital cost projections
Where:
RCx = for recurrent cost category x
CCx = for capital cost category x
Yi = for year i
Ω = for inflation

cMYP Costing & Financing Tool – User Guide20
Which inflation and exchange rate should be used?
Inflation refers to the phenomenon of prices rising over time. In this way costs/resource requirements can rise overtime simply because of a rise in prices, rather than a rise in the quantity or quality of inputs purchased. Forexample, increasing fuel prices will increase the cost of transportation.
Because the final costs/resource requirement estimates are reported in US dollars (although the Tool allows pricesto be entered in local currency), a standard inflation rate of 2% is recommended. This rate is based on theaverage consumer price inflation in the US dollar between 1993 and 2003, and represents the best estimate offuture price inflation.
The US dollar exchange rate selected for use in the Tool needs to be based on the published figures utilized ineach country. These should be reported in the Background Information section of the “1. Data Entry” worksheet.The Tool assumes a constant exchange rate over the projection period. Sources of the US dollar exchange rateinclude the Ministry of Finance or central bank, as well as the World Bank and International Monetary Fund (IMF)offices.
The second method used by the Tool estimates costs and future resource requirementsof certain categories of input based on some agreed rules-of-thumb appliedautomatically in the Tool. This applies to injection supplies, cold chain and vehiclemaintenance as follows.
• For injection supplies an approach that accurately reflects the use of resourcesis based on immunization practices for each antigen, linking this to the numberof doses of vaccines. For example, one dose of measles would require oneauto-disable (AD) syringe, one mixing syringe for reconstituting a 10-dosevial, and a portion of a safety box for disposal of the used syringes. Using theunit costs of each of these injection supplies, an approximate cost of suppliesper measles dose administered can be calculated based on the vaccine forecastfor measles. Future resource requirements for injection supplies are based onthe same rule-of–thumb, as well as future projected doses of each vaccine inthe vaccination schedule.
• For cold-chain maintenance the rules-of-thumb to estimate the likelymaintenance needs work by applying a set percentage of the capital cost ofthis equipment. The Tool recommends using 5% but this amount can be changedto suit a particular country setting.
• For vehicle maintenance the rule-of-thumb is to estimate the likely need basedon a set percentage of fuel costs. Fuel for vehicles is likely to be the single mostimportant input for transportation and one for which records are reasonablygood. Basing the set percentage on fuel rather than on the capital cost of theequipment (similar to cold chain), takes into consideration the utilization ofthe vehicles, where higher fuel consumption implies higher utilization andtherefore higher maintenance needs. The Tool recommends using 15% butthis amount can be changed for a particular country setting.
For other categories of inputs and activities such as training, social mobilization,IEC, surveillance, etc., the ingredients, or rules-of-thumb approaches, are not used.Because they do not represent the major cost drivers for immunization programmes,less emphasis is placed on estimating them accurately, and approximations can bemade using past spending (the budgeting approach). This is a method that is likely to

21WHO/IVB/06.15
yield estimates that are as accurate as applying the more complicated ingredientsapproach, and it has the advantage of requiring less data. This is therefore the thirdmethod used by the Tool.
Table 2: Summary table of methods used in the Tool
Method Name Methodology Inputs Activities
Ingredients approach Quantities x price x Vaccines, personnel, Vaccines, personnel,percentage use for transport, vehicles, transport, vehicles,immunization cold-chain equipment cold-chain equipment
Rule-of-thumb Immunization practice, Injection supplies, Injection supplies,fix percentage of the value of cold-chain maintenance, cold-chain maintenance,cold-chain equipment, vehicles maintenance vehicles maintenancefix percentage of fuel costs
Past spending or budgeting Lump-sum spending or Training, social mobilization, Training, social mobilization,approach based on past expenditure IEC, surveillance and others IEC, surveillance and
and budgets others
4.4 What are some methodological differences and limitations?
For some inputs, there will be slight deviations from the basic methodology describedabove. These are worth noting as they concern differences in approach between pastcosting and the estimation of future resource requirements.
For vaccines
The method used to estimate the past cost of vaccines is based on the amount ofvaccines supplied during a given year and the corresponding amount of vaccinesthat were administered. The quantity supplied per type of vaccine (Q supplied) iscalculated according to the following formula:
QZ Used = (QZ Received + QZ Initial Stock) - (QZ Remaining in Stock) where z = DPT, measles, OPV,etc.
An example
Vaccines Stock at Quantities End of year stock Quantities usedbeginning of supplied during
the year the year
Doses Doses Doses Doses
Measles 5,000 100,000 10,000 95,000
DTP 2,000 85,000 12,000 75,000
BCG 10,000 135,000 20,000 125,000
OPV 15,000 250,000 150,000 115,000
The cost of vaccines is calculated by multiplying the quantities supplied (Q supplied) bythe unit price for a given vaccine (P).

cMYP Costing & Financing Tool – User Guide22
For example, the cost of DTP vaccine supplied in 10-dose vials would be:
Cost DTP (10) = Q DTP (10) Supplied x P DTP (10)
An advantage of using this method is that vaccine wastage is implicitly assumed andcan be derived from the same data using the following formula:
Wastage rate Z = (doses supplied Z - doses administered Z) / doses supplied Z x 100
where z = DTP, measles, OPV, etc.
On the other hand, the method used to forecast future vaccine requirements is basedon coverage targets, wastage rate targets, unit prices and the size of the targetpopulation.
QZ needed = (births x target coverage Z) x doses in schedule x wastage
Cost Z = QZ needed x PZ
where the vaccine price (PZ) is kept constant for the whole forecast period.
For capital equipment
Because capital items like vehicles and cold-chain equipment are purchased in oneyear, but will be used in the programme for several years until they need to be replaced(the ULY concept), they are treated differently. In Part 3.5 above, the different methodsfor treating capital costs are explained when describing the difference between theterms cost and resource requirements.
To summarize, the cMYP costing exercise looks at one past year. Therefore theTool is estimating a past cost, and the value of capital equipment is converted to anannual equivalent by using a straight line depreciation. This is equivalent to theannual financial cost of the capital goods and is calculated by dividing the value ofthe goods by the total ULY number in order to get an annual equivalent. For example,a new vehicle purchased in the year 2000 for US$ 20,000 which will lastfive years before needing to be replaced, will have an annual financial cost ofUS$ 4,000 (US$ 20,000/5 ULY).
The rational for this adjustment is that, without depreciating the value of inputs thatlast for more than one year, it would be easy to get a distorted view of the long-termaverage annual cost of the programme. This would be the case if the total cost of theNIP was examined in a particular year when large investments in new vehicles andequipment had been made.
Alternatively, when making future projections, it is important to know what resourcesare needed for each year of the programme, irrespective of whether they are forinputs that will last for a year or more. This is because regardless of whether theinput or activity is a recurrent or a capital cost, these will need to be purchased at agiven point in time, and these resource requirements will need to be matched withcorresponding financing. This understanding is vital to the financial sustainability ofthe programme — knowing what financial resources will need to be mobilized eachyear to reach the cMYP objectives, and who will be funding these needs over time.

23WHO/IVB/06.15
This section of the User Guide provides step-by-step instruction on how to use thecMYP Costing and Financing Tool, guidance on sources of information and how toanalyse results and interpret findings.
At first glance, the Tool can appear overwhelming, as it contains many interrelatedworksheets. Fortunately, it is only necessary to work in two of these3 .
• The “1. Data Entry” worksheet is where all the data necessary for the costingand resource requirements projections has to be entered. It contains a series ofdata tables for the calculations of vaccines, injection supplies, personnel, vehiclesand transport, cold chain and maintenance, supplemental immunizationactivities, other recurrent and capital costs, and other costs not specifiedelsewhere.
Parts 5.1–5.2 will explain the “1. Data Entry” worksheet in greater detail.
• The “4. Financing” worksheet is where information on past and futurefinancing is entered. Some suggestions on procedures to collect financinginformation is provided in Parts 4.3 to 4.5 of this User Guide and in Annex I.
Parts 5.4–5.5 will review the “4. Financing” worksheet in more detail.
5.1 Overview of the “1. Data Entry” worksheet
Data Tables
The “1. Data Entry” worksheet is divided into eight sections that regroup thekey inputs and activities that were described earlier. Each section contains a series ofdata tables required for the costing exercise. The titles of the eight sections and24 data tables are summarized below.
5. Using the cMYPcosting and financing tool
3 If Microsoft Excel 2003 (or later) is used, these worksheet tabs are colour-coded in light purple.

cMYP Costing & Financing Tool – User Guide24
Table 3: Sections and data tables of the“1. Data Entry” worksheet of the Tool
0. Reference information
1. Vaccines & injection supplies
1.1 Demographic and other vaccine forecast information
1.2 Immunization schedule, vaccine prices and other vaccine reference information
1.3 Average price of injection equipment and cost of other injection supplies
1.4 Coverage and wastage objectives
1.5 Past and future DTP3 coverage
1.6 Specific target population for campaigns
2. Personnel costs
2.1 Staff categories, salaries/per diems and time spent on immunization
2.2 Average time spent on immunization and outreach (reference table)
2.3 Existing numbers of staff and future human resource needs (only in addition to those currently working for theprogramme)
3. Vehicles & transport costs
3.1 Average prices and utilization of vehicles
3.2 Existing vehicle numbers and future needs (including the future replacement of existing vehicles)
3.3 Other transport needs not covered elsewhere
4. Cold-chain equipment, maintenance & overheads
4.1 Average prices, running and maintenance costs of cold-chain equipment
4.2 Existing and future needs of cold-chain equipment (including the replacement of those currently used for theprogramme)
4.3 Other cold-chain needs not covered elsewhere
5. Operational cost of campaigns
5.1 Operational cost of campaigns
5.2 Average operational cost per child (used for future campaign operational costs)
6. Programme activities, other recurrent costs and surveillance
6.1 Total spending and future budget needs for programme activities and other recurrent costs
6.2 Total spending and future budget needs for surveillance and monitoring
7. Other equipment needs and capital costs
7.1 Average prices of other equipment needs
7.2 Projected number of additional equipment needs (including the replacement of those currently used for theprogramme)
8. Building & buildings’ overheads
8.1 Average prices and overheads costs of buildings
8.2 Existing and future needs of buildings

25WHO/IVB/06.15
Cell colour-coding and worksheet protection
The “1. Data Entry” worksheet has specific colour-coding for cells. The numericaldata entries are white and easily recognizable, but other cells are colour-coded.The “Print & Read Me” worksheet in the Tool provides a legend explaining thecolour-coded cells.
Surrounding the 22 data tables of the “1. Data Entry” worksheet are a number ofyellow text boxes. These provide guidance on the tables and how to fill them out.In addition, there are click-on cell notes that look like this:
(Click on Cell)
Budget SupportPooled Funds
World Bank Loans
Channelled Funds(Click on Cell)
Data Source Tip
Important Note(Click on Cell)
When you click on, or select, these cells, a pop-up note will appear. These should beread carefully.
Tool protection
The Tool is very sensitive to any formatting changes (adding/deleting cells,rows or columns) or editing (cut, copy or pasting of information from differentsources). In order to protect it from any damages that could be caused by formattingor editing changes, certain protective measures have been put in place. For instance,the cells and worksheets in the Tool are locked and password-protected to avoid thedeletion of rows or columns, since this would affect the integrity of the Tool,and could damage it. Likewise, some cells have been protected to prevent informationbeing entered in the wrong cells. If information is entered in the wrong cell, or alocked spreadsheet is deleted or modified, the following messages will appear.
However, you can always insert new worksheets in the Tool in order to make separatecalculations, create other graphs, or analyse the data.

cMYP Costing & Financing Tool – User Guide26
How to unprotect the Tool?
If it becomes necessary to unprotect the Tool and its worksheets, use the followingpassword: MYPCT
If you are unable to enter information into the Tool, it is possible that your computerhas a firewall or an activated virus protection system that prevents you from usingthe Tool on your computer. If this is the case, and to by-pass the anti-virus softwareprotection, you will need to unprotect the Tool using the password provided above,save it under a new file name, and then re-protect the Tool.
Cutting & pasting data
The Tool is very sensitive to the cut, copy and paste function of Excel. Copying andpasting data from other Excel workbooks into the Tool could break critical links,calculations and formulas, and create errors that could damage the Tool.
The copy and paste function therefore carries a high risk of damaging the Tool,which would result in work having to be redone. If there is no option of enteringdata other than by pasting information into the Tool, use the “paste special values”option instead of the “standard paste”. This option is available from the Edit menuof Excel, and the following pop-up will be displayed.

27WHO/IVB/06.15
Currency and inflation
Because prices and costs can be expressed in different currencies and can rise overtime, the Tool has been designed to accommodate different currencies and inflationrates. At the beginning of most data tables, a “Yes/No” pull-down option allowsyou to select the currency of the price data to be entered in the table. For example,it may be easier to enter information on wages and salaries in local currencywhereas the price of an imported vehicle has probably been quoted in US dollars.Note that you cannot mix both — that is, enter prices or values in both local currencyand US dollars in the same table.
Depending on whether data and prices are reported in local currency or US dollars,you will need to select the appropriate currency option, and the Tool will then makethe exchange rate conversion to show the results in US dollars.
The Tool also offers the possibility to enter the relevant price inflation rates.The default and recommended value is 2%. Note that this is a default US dollarinflation rate and not a local currency inflation rate.
The currency and inflation option boxes look like this:
Entering information in local currency? N
Forecasting inflation rates 2 %
Totals or average quantities
The information for Sections 2, 3, 4 and 8 of the “1. Data Entry” worksheet isrequired by each country at administrative level (e.g. central, provincial, district andhealth centre levels). Depending upon data availability, you can either choose towork in averages, or total quantities of personnel, vehicles, or cold-chain units ofequipment by administrative level.
The Tool offers the work option either using total quantities of an input(e.g. the total number of motorcycles), or an average quantity by administrativelevel (e.g. 10 motorcycles per province) which is then multiplied by the correspondingnumber of administrative levels to produce a total amount.
An option box has been included to accommodate for this and it looks like this:
Entering average quantities per administration level? N
Further suggestions on working with total or average quantities will be explained ingreater detail in Part 5.2 below.

cMYP Costing & Financing Tool – User Guide28
5.2 Review of each data table contained in the “1. Data Entry”worksheet
The “1. Data Entry” worksheet is divided into eight sections each containing aseries of data tables that require information for the cMYP costing exercise.Each of these sections is described below, including the 22 data tables,the methodologies used, and some general guidance for data sources.
Section 0 - Reference information
The reference information section is where essential country-specific details need tobe entered. This is a crucial section of the “1. Data Entry” worksheet. Formulas inthe Tool are contingent upon the information provided here. If the information isonly partially complete, the calculations may not yield the correct answers,and essential labelling of tables will not be done. Therefore it is very important thatthis section of the worksheet is completed as accurately and as comprehensively aspossible.
The table below lists the data needs for the general information section of the Tool.
Information needs Remarks
Country Enter the full country name.
Scenario To experiment with various scenarios, label the starting point scenario(e.g. Baseline, HepB introduction, etc.). More about scenario building isdeveloped in Parts 7.1–7.2.
First year of projection Enter the first year of the cost/resource requirement projection. For example,if you are developing a cMYP for the period 2006–2010, the first year ofprojection will be 2006.
Name of country administrative structures Enter information on the names of the country health administration structure,starting with the highest level (e.g. central or national) and ending with thelowest level (e.g. health centre or health community).
Number of country administrative structures Enter information on the number of health administration structures in thecountry (e.g. number of provinces, districts or health centres). These shouldcorrespond to the number of administrative levels mentioned above(e.g. 1 central level; 18 provinces, etc.).
Names of country administrative structures Because the Tool has the option to enter prices and costs in local currency,it is important to provide exchange rate information so that the finalcalculations of costing, financing, resource requirements and gaps will bereported in US dollars. Enter the exchange rate for the years you aredeveloping your cMYP. For instance, if in 2005 you are developing acMYP for the period 2006–2010, then it is likely that the latest exchange rateinformation you have will be for the year 2005.
Names of funding sources for immunization Enter the names of the different funding sources for the NIP (e.g. government,UNICEF, World Bank, etc.). There is an option to enter 16 different fundingsources. Two funding sources are set as default values (national andsubnational government).
Macroeconomic indicators Enter information on GDP in million local currency units (LCU), total healthexpenditure (THE) as a percentage of GDP,, and government healthexpenditure (as a percentage of government health expenditure (GHE)).
Officer responsible for the cMYP Costing Enter the name and contacts of the main officer responsible for the Tool.and Financing Tool

29WHO/IVB/06.15
It is important to mention that the “7. Sustainability” worksheet of the Toolrequires that data on the macroeconomic indicators be entered in this section of the“1. Data Entry” worksheet. It is also better to use national data. However, in theabsence of available information on GDP and health expenditures, internationalsources of data may be used. The following websites provide a good source ofinformation.
National health accounts (NHA) http://www.who.int/nha/country/en/
World Bank data http://devdata.worldbank.org/data-query/
Section 1 - vaccines & injection supplies
Vaccines and injection supplies are potentially the most important inputs tocalculate for the cMYP costing exercise. Firstly, they will reveal the importance ofvaccines as an input to the programme, as well as the implications for adopting anew or underused vaccine into the schedule. Secondly, this is one area for scenariobuilding (e.g. changing coverage targets) and also understanding the impact ofimproving efficiency (e.g. reducing wastage or changing vaccine presentation).
Given the importance of vaccines and injection supplies, this section of the“1. Data Entry” worksheet contains six required data tables.
1. Vaccines & injection supplies
1.1 Demographic and other vaccine forecast information
1.2 Immunization schedule, vaccine prices and other vaccine reference information
1.3 Average price of injection equipment and cost of other injection supplies
1.4 Coverage and wastage objectives
1.5 Past and future DTP3 coverage
1.6 Specific target population for campaigns
The information in these tables is needed to calculate the past costs and future resourcerequirements of vaccines and injection supplies for both routine immunization servicesand campaigns — supplemental immunization activities (SIAs).

cMYP Costing & Financing Tool – User Guide30
The six data tables require the following information:
1.1 Demographic and other vaccine forecast information
In table 1.1 enter the demographic data essential for making future projections ofthe target population. To make the calculations, you will need to provide informationon:
• the year of the last population census in the country;
• total population in the last census year;
• estimate of population growth rate;
• birth rate as a share of total population;
• infant mortality rates (IMRs) as a share of births;
• information on pregnant women (PW) as a factor of births. The default valuewould be set at one, so in other words, for every pregnant women there wouldbe at least one birth;
• information on childbearing age women (CBAW).

31WHO/IVB/06.15
Year
of la
st po
pulat
ion ce
nsus
(or y
ear o
f bes
t esti
mate)
Total
popu
lation
(cen
sus y
ear)
(or be
st es
timate
)
Popu
lation
grow
th (%
)20
0420
0620
0720
0820
0920
10
Birth
s (%
total
popu
lation
)
Infan
t Mor
tality
Rate
(per
1,00
0 live
birth
s)
Preg
nant
wome
n (as
a fac
tor of
birth
s)
Child
bear
ing ag
e wom
en (C
BAW
) (% of
total
popu
lation
)

cMYP Costing & Financing Tool – User Guide32
Note that there are two possible options for arriving at a figure for thetarget population – either using the under one population (U1P) or surviving infants(U1P minus the under one mortality).
The current convention is to make projections of vaccine requirements basedon births. To do this you will need information on birth rates (as a percentage ofthe total population) only. If you decide to make projections based on survivinginfants, you will need to enter the U1P as a percentage of the total population,and enter information on the IMR as a percentage of births.
Entering the above information in table 1.1 will allow the Tool to make forecasts forthe target population that will be used to calculate future needs for most vaccines.
Finally, a special case arises for projecting the needs of Tetanus Toxoid vaccine (TT)where the target population can either be pregnant women (PW) or childbearingage women (CBAW) aged between 15 and 46. In order to make the vaccineforecasts for TT vaccine, you will need to enter data on PW, or preferably CBAW.The Tool allows for calculation of TT vaccine requirements for either targetpopulations, depending on the country situation. Although there is some potentialfor double-counting, the TT coverage of PW is traditionally low, and is not consideredto represent a significant cost factor.
1.2 Immunization schedules, vaccine prices and other vaccine referenceinformation
In table 1.2 you need to verify and enter information on the vaccine schedule.There is a standard list of vaccines already available and spaces for entering othervaccines not in the standard list. If you use a vaccine which is not listed such asdiphtheria tetanus (DT), mumps, measles, rubella (MMR), or happen to procure thesame vaccine in different vial sizes (e.g. routine oral poliovirus vaccine (OPV) inboth 10- and 20-dose vials), these can be entered separately in the relevant cellscoloured yellow.
Note that table 1.2 is separated into two parts, separating routine immunizationactivities from those for SIAs (campaigns). For routine immunization, vaccines areseparated into those that can be considered as basic vaccines from those that are newand underused by the national immunization programme. For campaigns, there is astandard list and also space to enter other types of campaigns that will requirevaccines.
For each vaccine listed you will need to enter the number of doses in the schedule,the vial size, whether a buffer stock needs to be accounted for (only applicable fornew vaccine introduction), whether the vaccine needs to be reconstituted with mixingsyringes, and finally its unit price per dose (including freight and other charges).
Finally, for the past costing of vaccines, table 1.2 requests information be input onthe quantity of vaccines used and the number of doses administered.

33WHO/IVB/06.15
2004
2004
2004
2005
Type
s of v
accin
eDo
ses p
erVi
al siz
eBu
ffer s
tock
Mixin
gVi
tam
in A
Dose
sDo
ses
Aver
age
Price
per
Price
per
sche
dule
syrin
ges
supp
lied
supp
lied
Adm
inW
astag
edo
sedo
se
Rout
ine
Imm
uniza
tion
No.
No.
Y / N
Y / N
Y / N
No. d
oses
No. d
oses
(%)
US$
US$
Trad
ition
al va
ccin
esBC
GDT
PTe
tanus
(TT)
Meas
lesOP
VMe
asles
2nd D
ose
Othe
r vac
cine (
spec
ify)
Othe
r vac
cine (
spec
ify)
Othe
r vac
cine (
spec
ify)
Unde
ruse
d and
new
vacc
ines
Yello
w fev
erDT
P-He
p B-H
ibDT
P-He
p BDT
P-Hi
bHe
p B
Hib
MM
RJE Ot
her v
accin
e (sp
ecify
)Ot
her v
accin
e (sp
ecify
)Ca
mpa
igns
No.
No.
Y / N
Y / N
Y / N
No. d
oses
No. d
oses
(%)
US$
US$
Polio
Meas
lesYe
llow
fever
MNT
camp
aigns
(CBA
W)
Othe
r cam
paign
sOt
her c
ampa
igns
Othe
r cam
paign
sOt
her c
ampa
igns

cMYP Costing & Financing Tool – User Guide34
In order to derive the quantities supplied for each type of vaccine (Q supplied),the following formula should be applied:
Q supplied = (Q received + Q initial stock) - (Q remaining in stock)
The number of doses administered can be calculated based on coverage andthe number of surviving infants, or U1P, depending on what you have chosen intable 1.1.
Note that vaccine wastage rates are calculated based on this information and can beused as a point of reference for future wastage targets. The formula used for wastageis as follows:
Wastage rate = (doses supplied - doses administered) / doses supplied x 100
Please review Part 4.5 of this User Guide for more information on the method forpast costing of vaccines.
Finally, it is important for the costing exercise to have unit prices for vaccines.Standard UNICEF reference prices have been built into table 1.2. These can bechanged if there are country-specific prices you prefer to use for the relevant yearsof the cMYP costing and financing exercise. Make sure that the prices used are perdose and include all freight and other charges.
Vaccine prices and campaign naming
Vaccine prices
Because the future price evolution of vaccines is uncertain, the methodology used in the Tool recommendsmaking projections based on constant prices. In other words, to forecast the future needs of vaccines based on the last available year of vaccine price available, and to use the same prices for the entire projection period(up to five years). The Tool, however, also offers the possibility to enter alternative vaccine prices for future years.For information on vaccine prices, please consult the UNICEF Supplies Division website at http://www.unicef.org/supply.
Campaign naming
In each country the types of campaigns that will be undertaken will vary greatly, and therefore the namingof the campaigns will need to be adjusted accordingly. For instance, suppose that in a particular year there arevarious rounds of polio campaign targeting different population groups. In this instance it could be easier to treatthem as separate campaigns altogether and name them differently in table 1.2 (e.g. 2004 polio campaign round 1,or 2004 polio campaign round 2). Similarly, some routine immunization activities may have special outreachsessions targeting the hard-to-reach. These can be labelled as a type of campaign in table 1.2. Finally, anycontingency for outbreaks of vaccine preventable diseases should be listed as a campaign, and labelled accordingly.

35WHO/IVB/06.15
1.3 Average prices of injection equipment and cost of other injection supplies
In table 1.3 enter the average unit price of injections equipment for AD syringes,reconstitution syringes, and safety boxes. Note that UNICEF reference prices havealready been included in the table. These prices are incremented by a standard 15%freight charge. In some countries other taxes may be levied on injection equipmentand these should be added (e.g. value added tax or customs duty). These unit pricescan be changed if there are country-specific prices you prefer to use.

cMYP Costing & Financing Tool – User Guide36
Injec
tion e
quip
men
tUn
it pric
eFr
eight
(%)
Taxe
sTo
tal u
nit
(impo
rt, V
AT(
cost
Rout
ine i
mm
uniza
tion a
nd ca
mpa
igns
US$
(%)
(%)
US$
AD sy
ringe
AD sy
ringe
for B
CG
Reco
nstitu
tion s
yring
e (BC
G/Hi
b)
Reco
nstitu
tion s
yring
e (Me
asles
/Yello
w fev
er)
Safet
y box
es (5
litre
s)
Vitam
in A (
per g
el ca
ps)
Was
tage o
n inje
ction
equip
ment
No. s
yring
es pe
r safe
ty bo
x
Othe
r sup
plies
2005
Rout
ine
imm
uniza
tion
US$
(Ente
r total
expa
nditu
res)
Cotto
n
Vacc
inatio
n card
s
Othe
r (spe
cify)
Othe
r (spe
cify)
Othe
r (spe
cify)

37WHO/IVB/06.15
Below table 1.3 there is the choice to enter an average wastage rate on injectionsupplies and syringe capacities of safety boxes. The default value on the wastage ofinjection equipment is set at 10% and 100 syringe capacity for a 5 litre safety box.
Finally, there is an additional table that allows you to enter any other informationregarding average lump-sum spending on other injection supplies (cotton for example).
1.4 Coverage and wastage objectives
In table 1.4 enter projected coverage and wastage targets for each vaccine in theschedule that was specified in table 1.2. Note that coverage targets for routineimmunization and for supplemental immunization activities should be enteredseparately.

cMYP Costing & Financing Tool – User Guide38
Cove
rage
objec
tives
Was
tage o
bjecti
ves
Type
of va
ccin
e20
0520
0620
0720
0820
0920
0520
0620
0720
08Ro
utin
e im
mun
izatio
n%
%%
%%
%%
%%
Trad
itiona
l vac
cines
BCG
DTP(
1)TT
- Pre
gnan
t wom
enTT
- Chil
d bea
ring a
ge w
omen
Meas
lesOP
V (1
)Me
asles
2nd d
ose
Othe
r vac
cine (
spec
ify)
Othe
r vac
cine (
spec
ify)
Othe
r vac
cine (
spec
ify)
Unde
ruse
d and
new
vacc
ines
Yello
w fev
erDT
P-He
p B-H
ib (1
)DT
P-He
p B (1
)DT
B-Hi
b (1)
Hep B
(1)
Hib (
1)M
MR
JE Othe
r vac
cine (
spec
ify)
Othe
r vac
cine (
spec
ify)
Camp
aigns
%%
%%
%%
%%
%Po
lioMe
asles
Yello
w fev
erMN
T ca
mpaig
ns (C
BAW
)Ot
her c
ampa
igns
Othe
r cam
paign
sOt
her c
ampa
igns
Othe
r cam
paign
s

39WHO/IVB/06.15
It is important to note the WHO-UNICEF recommendations for the forecasting ofvaccines that have more than a one dose schedule, and that these should be basedon the first dose coverage target of these vaccines. For instance, any forecastingof DTP vaccine should be based on DTP1 and not DTP3 coverage objectives.Note that DTP1 coverage = DTP3 coverage + DTP3 drop-out rate. The latterinformation should be available from the WHO-UNICEF Joint Reporting Form(JRF).
Coverage targets when phasing in a new vaccine
In cases where you would like to phase in the introduction of a new vaccine in your country, you will need to makethe adjustment in table 1.4 using the coverage targets entered. For instance, if you wish to introduce DTP-HepBvaccine gradually, this means that some population groups will be covered by DTP, while others will be coveredby the new vaccine. Eventually the whole country will have the new combination vaccine, but in the interim youwill need to adjust your coverage targets to ensure that the overall target is not exceeded, otherwise you will over(or under) project vaccine needs. Table 1.4 below shows an example of a country with an overall DTP coverageobjective of 80% for 2006–2010 and which is gradually phasing out DTP vaccine in favour of DTP-HepBvaccine.
Example:
1.4 Coverage and wastage objectives
Coverage objectives
Type of vaccine 2006 2007 2008 2009 2010
Routine immunization % % % % %
Traditional vaccines
BCG
DTP(1)
Measles
OPV (1)
Underused and new vaccines
Yellow fever
DTP-Hep B-Hib (1)
DTP-Hep B (1)
1.5 Past and future DTP3 coverage
Future DTP3 coverage objectives
2006 2007 2008 2009 2010
% % % % %
DTP3 coverage

cMYP Costing & Financing Tool – User Guide40
1.5 Past and future DTP3 coverage
In table 1.5 enter past and future DTP3 coverage rates. This information is notused for vaccine forecasting, but is needed to calculate various indicators in the“5. Gap Indicators” worksheet of the Tool.
1.6 Specific target populations for the campaigns
Since the target populations for campaigns can be different from the targetpopulations for routine immunization, and these can vary depending on the type andtiming of campaigns being conducted, this information needs to be entered separatelyin table 1.6.
Section 2 - personnel costs
As personnel is frequently the single largest input to a NIP, considerable emphasisshould be given to the accuracy in assessing its input, in particular to the assessmentof salaries and staff time actually spent on immunization activities. Small errors inestimation can translate into a large overestimation or underestimation of the costingexercise.
Estimating personnel costs is complicated by the fact that some personnel time is:
• specific to the delivery of immunization services. This relates to staff timedirectly associated with the immunization service, spending 100% of theirtime working for the NIP (for example, all central-level staff working for theimmunization department of the MoH);
• shared with other health services. This relates to staff time that is only partlyassigned to immunization activities (for example a nurse at the health facilitylevel spending 10% of her time providing vaccinations and the rest of her timeworking on other preventive/curative services).
Personnel will be the main input where a large proportion of the costs are likely tobe shared with other programmes. It is therefore important to get an accurate measureof the proportion of their time that staff actually work on immunization, as apartfrom the basic importance of personnel as a main cost driver to immunizationprogrammes, this proportion is often used to estimate other shared costs. For example,if it is difficult to measure the proportion of vehicles or buildings’ costs that areallocated to immunization, you can simply use staff time devoted to the programmeas a way of allocating the value of shared vehicles and buildings’ costs, and this willgive a good approximation.
Collecting data on the percentage time spent on immunization is time-consuming,but this information will more accurately reflect the amount of government input tothe programme, and so reporting shared personnel costs is invaluable. Specifictechniques for this are provided below, and the Tool facilitates these calculations.
Given the importance of personnel, this section of the “1. Data Entry” worksheetcontains three required data tables.

41WHO/IVB/06.15
2. Personnel costs
2.1 Staff categories, salaries/per diems and time spent on immunization
2.2 Average time spent on immunization and outreach (reference table)
2.3 Existing numbers of staff and future human resource needs (only in addition to those currently working for theprogramme)
The information in these tables is needed to calculate the past costs and future personnelresource requirements.
The three data tables require the following information:
2.1 Staff categories, salaries/per diems and time spent on immunization
In table 2.1 first enter information on the types or categories of staff working onthe immunization programme, and whether they are full-time or part-time staff(e.g. EPI manager at national level, or outreach vaccinator at district level). You willneed to enter the staff categories for each administrative level in the country(as reported in the reference information section).
Note that the personnel in categories already listed in the table are there as examplesonly, and should be replaced by the ones relevant to your country context.
Then enter information on average gross monthly salaries per category of staff listedin table 2.1, and any other benefits such as special non-transport allowances orsubsidies.

cMYP Costing & Financing Tool – User Guide42
Rout
ine
imm
uniza
tion
Outre
ach a
ctivi
ties
Supe
rvisi
on
Type
of st
aff
Gros
sOt
her
% T
ime
Aver
age N
o.Av
erag
e No.
mon
thly
mon
thly
work
ing
onda
ys pe
rpe
r diem
sda
ys pe
rpe
r diem
swa
gebe
nefit
sim
mun
izatio
nm
onth
mon
thCe
ntral
US$
US$
(%)
No. d
ays
US$/
day
No. d
ays
US$/
day
Nip m
anag
erEP
I offic
erAd
minis
tratio
nMe
dical
docto
rMe
dical
office
rMe
dical
assis
tant
Healt
h offic
erLa
borta
ry pe
rsonn
elLo
gistic
ianMo
nitor
ing/S
urve
illanc
e/Eva
luatio
n offic
erNu
rseSe
cretar
yDr
ivers
Secu
rity gu
ard
Othe
r (spe
cify)
Prov
incial
US$
US$
(%)
No. d
ays
US$/
day
No. d
ays
US$/
day
Healt
h offic
erMe
dical
office
rTe
chnic
ians
Cold
chain
tech
nician
Logis
tician
sMo
nitor
in/Su
rveilla
nce/E
valua
tion o
fficer
Secre
taries
Drive
rsOt
her (s
pecif
y

43WHO/IVB/06.15
Then, for each category of staff, indicate whether they work full-time (100%) orpart-time (less than 100%) for the national immunization programme. The percentagetime spent on immunization can be difficult to estimate. In general expert opinion,or responses from a small sample survey, will provide sufficient information toestimate an average percentage time spent on immunization per category of staff.
Because outreach activities in many countries are an essential component of routineimmunization services, table 2.1 requires information on the number of days spentworking in an outreach capacity each month for the relevant category of staff,and the corresponding daily per diem rates. Although there are provisions in thetable for staff per diem rates at most administrative levels of the system, it is expectedthat data will be concentrated at the lower levels, since these staff are most likely tobe involved in outreach immunization activities.
Finally, in the last columns of table 2.1, enter the same information for supervisoryactivities, i.e. the average number of days per month conducting supervisory visitsfor the relevant staff categories, and the corresponding daily per diem rates.

cMYP Costing & Financing Tool – User Guide44
Data collection tips
Because of the importance of getting good information for the calculation of personnel, some recommended stepsfor collecting the data are provided below.
If calculating immunization personnel using total number of staff working for the programme, follow the stepsbelow.
1) Identify all staff working for immunization (full-time or part-time) at each administrative level (e.g. national,provincial, district, and service delivery levels), including all staff involved in outreach activities and supervision.Only include national staff and do not include the costs of international staff/consultants working on immunizationfor donor agencies.
2) Group all staff according to their category or grade level at the MoH (e.g. EPI manager, medical doctor,medical assistant, nurse, vaccinator, etc.).
3) Identify and attribute the gross monthly salary for each category of staff based on the salary scales availablefrom the MoH. Note that when travel allowances are paid to staff, these should be included in the transportationcost category and not listed under personnel.
4) Identify all other allowances and benefits and estimate the average monthly value of these for each categoryof staff listed.
5) Identify the average time spent on immunization for each category of staff.• For routine activities the average percentage time spent on immunization should be used.• For outreach the average number of workdays per month is the most reliable indicator of time spent on
this activity.
For calculating immunization personnel using an average number of staff at each administrative level.
(Unless this information is readily available at the central or national level, it might be easier to work with averagenumbers of staff by administrative level. If you decide to work with averages, see below for the steps recommendedfor data collection).
1) Collect information on the total number of fixed health facilities in the country by category and by differentadministrative levels (e.g. provincial hospitals, district health centres, dispensaries, or other fixed sites).These health facilities must provide immunization services.
2) For each type of health facility, select one that is representative (i.e. a representative provincial hospital ora representative district health centre). The term representative implies representative in size (total numberof health workers) and utilization (in terms of children being immunized).
3) Interview these representative health facilities by administrative level, either by fax, telephone or direct visit,and request information on:• total number and category of staff involved in immunization;• average percentage of staff time spent each month on routine immunization services;• average monthly staff salary, plus other allowances and benefits;• number of days a month spent on outreach and outreach per diems;• number of days a month spent on supervision and the per diem rates.

45WHO/IVB/06.15
2.2 Average time spent on immunization and outreach (reference table)
Table 2.2 is a reference table and does not require any information to be entered.The table is automatically generated based on the information provided in tables2.1–2.3. It will calculate the overall average percentage time spent on immunizationfor all staff at each administrative level. It will also calculate the average percentagetime spent on outreach for all staff involved in outreach activities.
Note that table 2.2 will not be activated unless table 2.1 includes information on thepercentage time spent on immunization, and table 2.3 contains information aboutquantities. The purpose of this table is to facilitate the calculation of other sharedcosts. For example, if it is not possible to measure the proportion of shared vehicleor buildings’ inputs for immunization, staff time devoted to the programme can beused as a way of allocating the value of shared vehicles and buildings’ inputs.This will give a good approximation and will also save time.
2.3 Existing numbers of staff and future human resource needs (only in additionto those currently working for the programme)
In table 2.3 enter the number of staff currently working for immunization,by staff type and for the different administrative levels, and also your projections offuture staff needs. Estimates of future staff should be based on the needs to reachprogramme objectives as defined in the cMYP. Do not enter the future evolution oftotal staff but only the additional numbers of staff needs above and beyond thosealready engaged in immunization (e.g. in order to improve coverage at the districtlevel your programme may need an additional 100 vaccinators). Also, only enter thenumber of staff in the year they are expected to begin working.
Note that for future projections of staff needs, it is only necessary to enter thequantities for the year in which the staff will start working. The Tool will automaticallyinclude these for the remainder of the period (because it is a recurrent cost) and willcalculate the total cumulative number of staff for the projection period. If any staffare expected to be laid off, these should be deducted by entering each individual as anegative number in the year the person ceases to work.
Table 2.3 has an option to work with total numbers of staff, or average numbersby administrative level. To work with average numbers of staff by administrativelevel, select “Y” on the options box for table 2.3, and only include the average numberof staff per administrative level obtained in your survey. Otherwise, select “N”.For the calculations to work, you need to ensure that the total number of administrativelevels in the country are reported in the background information section of the“1. Data Entry” worksheet.
In some instances, collecting information on the number of staff can be made easierby surveying the personnel in a sample of health facilities in each administrativelevel, and extrapolating for the rest of the country by multiplying by the totalnumber of corresponding administrative levels. For example, if each district has onehealth facility with an average of one vaccinator and one medical officer workingfor immunization, then it is possible to estimate the total staff by multiplying thisaverage number of staff per district by the total number of districts in the country(see the data collection tips box above).

cMYP Costing & Financing Tool – User Guide46
Section 3 - vehicles & transport costs
Vehicles and transportation in many countries are the weakest link in anyimmunization programme. For this reason it is important to know how much isneeded to operate and maintain a fleet of vehicles to deliver vaccines, supplies andimmunization services. Because some of the data needs for estimating transportation(such as maintenance), are related to the capital cost of vehicles, vehicle costs andtransportation are covered together in the “1. Data Entry” worksheet.
The methodology used for estimating vehicle costs is based upon the numbers ofvehicles used by the NIP (quantities), their unit cost (prices), and their utilization bythe programme (percentage spent on immunization).
The methodology used for calculating transportation focuses on fuel, as fuel is likelyto be the single most important item for transportation and an input for which recordsare reasonably good (i.e. average mileage of vehicles, average fuel consumption perunit of mileage, and the price of fuel). Since data on vehicle maintenance is amongthe most difficult to measure, the Tool will use methods to approximate them byapplying a percentage increment on the known value of fuel. The Tool recommendsapplying 15% but you have the option to change this percentage factor to any othervalue you consider more appropriate.
At the start of this section of the “1. Data Entry” worksheet, you can enter andverify essential parameters for the calculations (such as fuel prices, rules-of-thumbfor maintenance, ULY, etc.).

47WHO/IVB/06.15
Enter
ing in
forma
tion i
n loc
al cu
rrenc
y ?N
(Ente
r N fo
r $ P
rices
)
Enter
the a
nnua
l % in
creas
e in p
rice o
f petr
ol2%
(Rec
omme
nded
value
is 2%
. Note
that
this i
s a U
S$ in
flatio
n rate
. Do n
ot en
ter a
LCU
inflat
ion ra
te)
Fuel
price
per li
tre (2
004)
(in U
S$)
Enter
the a
nnua
l % in
creas
e in p
rice o
f petr
ol2%
(Rec
omme
nded
value
is 2%
. Note
that
this i
s a U
S$ in
flatio
n rate
)
Vehic
le ma
inten
ance
as a
% of
fuel
costs
15%
(Rec
omme
nded
value
is 15
%)
Aver
age u
seful
life y
ear o
f veh
icles
(ULY
)5
(Rec
omme
nded
value
is 5
year
s - N
ot mo
re th
an 10
year
s)

cMYP Costing & Financing Tool – User Guide48
Given the importance of vehicles and transportation, Section 3 of the “1. Data Entry”worksheet contains three required data tables.
3. Vehicles & transport costs
3.1 Average prices and utilization of vehicles
3.2 Existing vehicle numbers and future needs (including the future replacement of existing vehicles)
3.3 Other transport needs not covered elsewhere
The information in these tables is necessary to calculate the past costs and futureresource requirements of vehicles and transportation. The three data tables are asfollows:
3.1 Average prices and utilization of vehicles
In table 3.1 first enter information on the types or categories of vehicles used by theimmunization programme, and whether these vehicles are in use all, or part, of thetime. Enter vehicle categories for each administrative level in the country. Note thatthe vehicle categories listed in table 3.1 are examples only, and you can replace theexisting categories with the relevant ones for your country setting. There is alsoroom to include more categories of vehicles, and this should be done in the yellowcells in the first administrative level of table 3.1. Once the categories of vehicles areentered, they will automatically be updated for lower administrative levels, and inthe other tables (table 3.2).
Then enter the estimated average unit price (including all taxes) for each type ofvehicle, and information on the average number of kilometres travelled each year,and the average fuel consumption per 100 km for each of the vehicles listed.

49WHO/IVB/06.15
123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
Per v
ehicl
e typ
e
Type
of ve
hicle
sAv
erag
e pric
eDi
stanc
eFu
el%
Tim
e us
edne
w (20
05)
(Ave
rage
km’s
cons
umpt
ion
for
per y
ear)
(litre
s per
100k
m)
imuu
niza
tion
Natio
nal
US$
Km’s
l/100
km’s
(%)
4 WD
vehic
les
Truc
ks
Cars
Boats
(moto
r)
Bicy
cle
Motor
cycle
s
Vehic
les fo
r sur
eveil
lance
Regi
onal
US$
Km’s
l/100
km’s
(%)
4 WD
vehic
les
Truc
ks
Cars
Boats
(moto
r)
Bicy
cle
Motor
cycle
s
Vehic
les fo
r sur
eveil
lance

cMYP Costing & Financing Tool – User Guide50
Finally, enter data on the utilization of vehicles for immunization. If the vehicles areexclusively purchased for the NIP, enter 100%.
For other vehicles, the percentage time spent on immunization may be difficult toestimate, but expert opinion or responses from a small sample survey of facilitiesmay provide the necessary data. Alternatively, you could use the information includedin table 2.2 by applying the average percentage time spent on immunization by staffat different levels. Alternatively, if ‘Drivers’ are listed as a staff category in table 2.1,you can use the information to obtain the percentage time that they are spending onimmunization.
3.2 Existing vehicle numbers and future needs (including future replacement ofexisting vehicles)
In table 3.2 enter the total number of existing vehicles and future additional needs,by vehicle type and by administrative level. For existing vehicles, you will need toseparate those units that were purchased during the baseline year, from those thatwere purchased before. For future projections, make sure to include the replacementof those currently used for the immunization programme. The Tool will automaticallycompute the year when vehicles need to be removed from service based on theULY specified. However, it will not automatically account for their replacement.New vehicles therefore need to be reported separately, and in line with your preferredmethods of purchase and timing. Estimates should be based on the needs toreach programme objectives and targets and those outlined in the cMYP and existingcold-chain reviews.
3.3 Other transport needs not covered elsewhere
In case there are other transport needs that are not captured in tables 3.1 and 3.2,these should be entered in table 3.3. For example, there may be separate fuel budgetsfor vaccine delivery or for payment of transport per diems to outreach vaccinators,etc. To account for these, enter lump- sum costs in table 3.3 as well as any projectionsof future budget needs.
It is important to ensure that transportation needs are not repeated in table 3.3.In other words, only include transportation needs that are not already captured inthe transportation costs of tables 3.1 and 3.2.

51WHO/IVB/06.15
Expe
nditu
reFu
ture
budg
et ne
eds
Othe
r tra
nspo
rt co
sts
2004
2006
2007
2008
2009
2010
US$
US$
US$
US$
US$
US$
Vacc
ine de
liver
y
Tran
sport
per d
iems f
or ou
treac
h
Othe
r (spe
cify)
Othe
r (spe
cify)
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide52
Data collection tips
Because of the importance of getting good information for the calculation of vehicles and transport,some recommended steps for collecting the data are provided below.
If calculating vehicles using total number of vehicles used by the programme, take the following steps.
1) Collect information on the total fleet of vehicles used by the immunization programme by vehicle category:numbers of cars; four-wheel drive vehicles; motorcycles; bicycles; boats, etc.
2) Select from each type of vehicle, one that is representative. For instance, the fleet of four-wheel drivevehicles may be composed of several models (e.g. Toyota Land-Cruiser or Mitsubishi). Choose the modelthat is most representative in terms of numbers, age, mileage, and usage.
3) Interview drivers at the central level NIP department of the MoH. For each vehicle type, ask them to provide(to the best of their knowledge), an average fuel consumption for these vehicles, the average distancetravelled per year, the percentage time the vehicle is used for immunization-related activities, and theaverage ULY of the vehicles. Preferably choose drivers that have been working for the NIP for severalyears and so have the most knowledge of this information.
4) Get information on how many vehicles would be needed in the future.
If calculating vehicles by using the average number of vehicles by administrative level.
(Unless this information is readily available at the central or national level, it might be easier to work with averagenumber of vehicles by administrative level. If you decide to work with averages, the recommended steps to collectthe needed data are as follows).
1) Collect information on the total number of fixed health facilities in the country by category and by differentadministrative levels (e.g. provincial hospitals, district health centres, dispensaries, or other fixed sites).These health facilities must provide immunization services.
2) For each type of health facility, select one that is representative (i.e. a representative provincial hospital ora representative district health centre). The term representative implies representative in size (total numberof health workers) and utilization (in terms of children being immunized).
3) Interview these representative health facilities by administrative level, either by fax, telephone, or direct visit,and request information on:• total number of vehicles used in immunization and by category;• average percentage time these vehicles are used by the NIP;• average price of each type of vehicle;• average ULY of vehicles;• average annual distance travelled (in kilometres) and the average fuel consumption (in Litres per
100 Km) for each vehicle type• the number of vehicles that would be needed in the future.

53WHO/IVB/06.15
Section 4 - Cold chain equipment, maintenance and overheads
The cold-chain equipment needed for any national immunization programme is asimportant as the vaccines themselves. Therefore particular importance should bepaid to the estimation of needs for cold chain, particularly in the context of newvaccine introduction.
Because some of the data needs for estimating cold-chain maintenance and overheadsare related to the capital cost of cold-chain equipment, these costs are covered togetherin the “1. Data Entry” worksheet.
The methodology used for estimating the cost of cold-chain equipment is based onunits of equipment (quantities), and their unit cost (prices). In the Tool it is assumedthat the cold-chain equipment is immunization specific. In other words,their utilization is 100% for the immunization programme. Therefore, there is noneed (as with personnel or vehicles) to specify the percentage of time spent onimmunization.
At the start of this section of the “1. Data Entry” worksheet, you can enter andverify essential parameters for the calculations (such as rules-of-thumb formaintenance, ULY, etc.).
Given the importance of the cold chain, section 4 of the “1. Data Entry” worksheetcontains three required data tables.
4. Cold-chain equipment, maintenance & overheads
4.1 Average prices, running and maintenance costs of cold-chain equipment
4.2 Existing and future needs of cold-chain equipment (including the replacement of those currently used for theprogramme)
4.3 Other cold-chain needs not covered elsewhere
The information in these tables is needed to calculate the past costs and futureresource requirements for cold-chain equipment, their maintenance (spare parts),and overhead costs (fuel, electricity, etc.). The three data tables are as follows.
4.1 Average prices, running and maintenance costs of cold-chain equipment
In table 4.1 first enter information on the types (or categories) of cold-chainequipment used by the NIP (e.g. freezers, refrigerators, cold boxes, or vaccinecarriers), as well as the main categories of spare parts (e.g. burners, wicks, etc.) andother cold-chain supplies (e.g. ice packs, etc.). In table 4.1 there are listings for typesof cold-chain equipment. These should be replaced by categories that are relevant toyour NIP. If the equipment used is not already listed in the table, you can replace theexisting categories with the relevant ones. There is also room to include morecategories if you wish.
Secondly, you need to enter average unit prices (including all taxes) for each type ofcold-chain equipment listed, such as the average price of a new refrigerator or coldbox. As mentioned in Part 3.4 of this User Guide, a rule-of-thumb used to estimatethe likely maintenance costs of each type of cold-chain equipment, is by applying aset percentage of the capital cost of the equipment. The Tool recommends using 5%but you have the option to change this percentage factor to any other value youconsider more appropriate for your country setting.

cMYP Costing & Financing Tool – User Guide54
Per u
nit o
f equ
ipm
ent
Type
of c
old
chain
Aver
age p
rice
Aver
age m
onth
lyAv
erag
e yea
rlyNe
w (20
05)
over
head
costs
main
tenan
ce co
stEq
uipm
ent
US$
US$
US$
Cold
room
Cold
boxe
s
Vacc
ine ca
rriers
Refrig
erator
(elec
tric)
Refrig
erator
(gas
)
Main
spar
e par
ts an
d oth
erUS
$US
$US
$
Ice pa
cks
Therm
ocou
ples
Electr
ic he
aters
Burne
rs
Gene
rators
Othe
r (spe
cify)

55WHO/IVB/06.15
4.2 Existing and future needs of cold-chain equipment (including thereplacement of those currently used for the programme)
In table 4.2 enter the total number of existing units of cold-chain equipmentthat are used by the NIP along with your future projection of needs, by type ofcold-chain equipment and by administrative level. For existing cold-chain equipment,you will need to separate those units that were purchased during the baseline yearfrom those that were purchased before. When making future projections, be sure toinclude the replacement of those currently used for the programme. The Tool willautomatically compute the year when the cold-chain equipment needs to be removedfrom service, based on the ULY specified. However, it will not automatically accountfor their replacement. You need to report these separately and in line with yourpreferred methods of purchase and timing. Estimates should be based on the needsto reach programme objectives and targets and those outlined in the cMYP andexisting cold-chain reviews.
4.3 Other cold-chain needs not covered elsewhere
If this is relevant to your NIP, enter in table 4.3 any of the lump sum costs of othercold chain needs not specified elsewhere. For example, you may need to include abudget for ice for outreach activities, or extra fuel for the cold chain.
It is important to ensure that cold-chain needs are not repeated in table 4.3. In otherwords, only include cold-chain needs that are not already captured in thetransportation costs of tables 4.1 and 4.2.

cMYP Costing & Financing Tool – User Guide56
Expe
nditu
reFu
ture
budg
et ne
eds
Othe
r col
d cha
in ne
eds
2004
2006
2007
2008
2009
2010
US$
US$
US$
US$
US$
US$
Ice fo
r Outr
each
Activ
ities
Fuel
for C
old C
hain
Othe
r (spe
cify)
Othe
r (spe
cify)
Othe
r (spe
cify)

57WHO/IVB/06.15
Data collection tips:
Because of the importance of getting good information for the calculation of cold-chain equipment and its relatedmaintenance and overheads, some recommended steps for collecting the data are provided.
If calculating cold-chain equipment using total list of equipment in the country, take the following steps.
1) Assemble an itemized list of all cold-chain equipment in the country by type of equipment (e.g. freezers,refrigerators, cold boxes, vaccine carriers, etc.), and spare parts. This information should be available fromthe cold-chain logistics person at the central cold room.
2) Using expenditure statements, invoices and receipts on the purchase of cold-chain equipment (or a recentcold-chain review), attribute the correct purchase price to each type of cold-chain equipment. If the purchaseprice for a specific model is not known, use the average price for that category of equipment. For instance,there may be various models of fridges and freezers (e.g. RCW, Electrolux, Sibir, etc.). If the unit price ofeach model is not known, use the average price for the whole category.
3) By means of interviews with the cold-chain logistics and repairs staff, determine the average monthly runningcost, the average yearly maintenance cost of type of cold-chain equipment listed, and the average ULY ofthe equipment.
4) Collect information on the future upgrading of the cold chain.
If calculating cold-chain equipment using the average number of cold-chain units by administrative level.
(Unless this information is readily available at the central or national level, it might be easier to work with averagenumbers of cold-chain units by administrative level. If you decide to work with averages, the recommended stepsto collect the needed data are as follows.)
1) Collect information on the total number of fixed health facilities in the country by category and by differentadministrative levels (e.g. provincial hospitals, district health centres, dispensaries, and other fixed sites).These health facilities must provide immunization services.
2) For each type of health facility, select one that is representative (i.e. a representative provincial hospital ora representative district health centre). The term representative implies representative in size (total numberof health workers) and utilization (in terms of numbers of children being immunized).
3) Interview these representative health facilities by administrative level, either by fax, telephone, or direct visit,and request information on:• total number of cold-chain units used, and by categories of cold chain;• average price of each type of cold-chain unit;• average monthly running cost, the average annual maintenance cost per type of cold-chain equipment,
and the average ULY;• information on future upgrading of the cold chain.

cMYP Costing & Financing Tool – User Guide58
Section 5 - Operational costs of campaigns
Increasingly, campaigns and supplemental immunization activities (SIAs) arebecoming an integral part of country national immunization programmes, and animportant strategy for eradicating and controlling diseases, and for raising coverage.While the needs for vaccines and injection supplies for campaigns are taken intoaccount in Section 1 of the “1. Data Entry” worksheet, you still need to budget forthe operational costs.
The methodology used to calculate the operational costs of campaigns is based uponestimates of an average campaign operational cost per child, and by applying thisunit cost to the future target number of children in the campaign. This simplifies thecosting exercise and allows you to take into account the fact that a campaign may betargeting an entirely different age group than for routine immunization.
Section 5 of the “1. Data Entry” worksheet contains two required data tables.
5. Operational cost of campaigns
5.1 Operational cost of campaigns
5.2 Average operational cost per child (used for future campaign operational costs)
The information in these tables is needed to calculate the past costs and future resourcerequirements for the operational needs of the campaigns. The two data tables arebelow.
Note that it is necessary to specify and name a type of campaign in table 1.2.
5.1 Operational costs of campaigns
In table 5.1 you need to provide information on past operational costs by type ofcampaign (e.g. polio, measles, etc.). The main operational costs are broken downinto per diems awarded to health workers during the campaign (that is, the personnelcosts of the campaign), and other operational costs. Typically these would includetraining, transport, and social mobilization inputs that were provided specifically foreach campaign listed.
The amounts entered in table 5.1 should exclude any spending on vaccines andinjection supplies. Note however that these are shown in the table as reference cells.

59WHO/IVB/06.15
Operational cost/child
Type of campaigns 2004 2004 2004
US$ US$ US$
Polio
Vaccines
Per diems
other operational costs
Measles
Vaccines
Injection supplies
Per diems
Other operational costs
Yellow fever
Vaccines
Injection supplies
Per diems
Other operational costs
Once the lump-sum amounts are entered into table 5.1, the average operationalcost per child will be automatically calculated. This amount is the ratio between thelump-sum operational amount and the number of children vaccinated, as reported intable 1.2. These average operational costs per child can be used in the projections offuture needs for supplemental activities.
It is important to note that this method assumes that any capital equipmentpurchased for supplemental activities will subsequently be used in the routineprogramme. These should therefore be included and adequately labelled as part ofthe Section 3 and 4 data tables.
5.2 Average operational cost per child (used for future campaign operationalcosts)
In table 5.2 you need to report average campaign operational costs per child.These will be used to make the projections of future resource requirements forcampaigns that are planned for in table 1.6.
It is important to ensure that tables 1.2, 1.4 and 1.6 are completed correctly.Remember that it is possible to use the average operational costs per child that arecalculated in table 6.1 as a reference number. However, if these are not calculated(e.g. there were no past yellow fever campaigns but you plan to conduct some in thefuture), they will need to be estimated, or approximated, using the average operationalcost per child from other similar types of campaigns. For example, the averageoperational cost per child for a measles campaign is likely to be very similar to thatof a yellow fever campaign. Most in-depth costing studies for campaigns find thatthe average operational costs per campaign hover between US$ 0.5 and US$ 0.7 perchild. If you do not have any existing data, we recommend you use these amounts.

cMYP Costing & Financing Tool – User Guide60
Section 6 - Programme activities, other recurrent costs and surveillance
Programme activities, other recurrent costs and surveillance are critical componentsof an immunization programme but are often under-funded. For the most part,these inputs will not be the major cost drivers of the programme and for this reasonless emphasis is placed on estimating these costs accurately. However it is critical tobudget for them accordingly.
Typically, programme activities and other recurrent cost categories will cover areasuch as social mobilization, advocacy and communication activities, training,programme management, and monitoring and disease surveillance.
Section 6 of the “1. Data Entry” worksheet contains two required data tables.
6. Programme activities, other recurrent costs and surveillance
6.1 Total spending and future budget needs for programme activities and other recurrent costs
6.2 Total spending and future budget needs for surveillance and monitoring
The information in these tables is needed to calculate the past costs and futureresource requirements for programme activities, other recurrent costs and surveillance.The two data tables are below.
6.1 Total spending and future budget needs for programme activities and otherrecurrent costs
In table 6.1 you need to enter past expenditure and future budget needs for activitiesand other recurrent cost categories listed. Future budgets can be approximated bythe total lump-sum expenditure on these categories, and the future resourcerequirements will be projected by inflating these amounts forward. In many countries,these elements of the programme are often financed by external donors,usually through annual lump-sums for these inputs. Tracking the financing providedwill be a good proxy of their cost and this information should be used.

61WHO/IVB/06.15
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
1234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345
Expe
nditu
reFu
ture
budg
et ne
eds
Prog
ram
me A
ctivi
ties a
nd O
ther
Rec
urre
nt C
osts
2005
2007
2008
2009
2010
2011
US$
US$
US$
US$
US$
US$
Socia
l Mob
ilizat
ion,
Adv
ocac
y, an
d Co
mm
unica
tion A
ctivi
ties
Budg
et for
socia
l mob
ilizati
on
Mass
med
ia
ed m
ateria
ls (b
anne
rs, po
sters,
IEC
mater
ials…
)
Othe
r (spe
cify)
Train
ing
and
Wor
ksho
ps
Train
ing ac
tivitie
s
Othe
r (spe
cify)
Prog
ram
me M
anag
emen
t
Meeti
ngs
Evalu
ation
s: Pr
ogra
mme r
eview
s and
asse
ssme
nts
Offic
e sup
plies
Renta
l of b
uildin
gs
Othe
r (spe
cify)
Othe
r act
ivitie
s
Finan
cial s
ustai
nabil
ity ac
tivitie
s
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide62
6.2 Total spending and future budget needs for surveillance and monitoring
Table 6.2 covers expenditure and future budget needs for surveillance and monitoringfor detection and notification, case and outbreak investigation, data management,and laboratory and supportive activities.
Future budgets can be approximated by the total lump-sum expenditure onsurveillance and monitoring, and the future resource requirements will be projectedby inflating these amounts forward. In many countries, these elements ofthe programme are often financed by external donors, usually through annuallump-sums for these inputs. Tracking the financing provided will be a good proxy oftheir cost and this information should be used.

63WHO/IVB/06.15
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
Expe
nditu
reFu
ture
budg
et ne
eds
Surv
eillan
ce a
nd m
onito
ring
2005
2007
2008
2009
2010
2011
US$
US$
US$
US$
US$
US$
Dete
ctio
n and
Not
ifica
tion
Stan
dards
Identi
ficati
on an
d prep
aratio
n of s
ites
Clini
cian a
dvoc
acy
Notifi
catio
n and
comm
unica
tion
Activ
e sur
veilla
nce
Case
and o
utbr
eak v
erifi
catio
n and
inve
stig
atio
n
Stan
dard
opera
ting p
roced
ures
Disp
atch o
f spe
cimen
s to t
he la
b
Data
Mana
gem
ent
Stan
dard
s of fl
ow, fr
eque
ncy a
nd fo
rmat
of da
ta ex
chan
ge
Supp
lies f
or da
ta ma
nage
ment
Feed
back
bulle
tin
Labo
rato
ry
Spec
imen
kits
and c
arrie
rs
Comm
unica
tions
Data
mana
geme
nt
Supp
ortiv
e Act
ivitie
s
Evalu
ation
and p
lannin
g
Reso
urce m
anag
emen
t

cMYP Costing & Financing Tool – User Guide64
Section 7 - Other equipment needs and capital costs
In the event that you need to include equipment other than vehicles and cold chain,Section 7 of the “1. Data Entry” worksheet is included for reporting otherimmunization-specific capital inputs relevant to each immunization programme.
Section 7 of the “1. Data Entry” worksheet contains two required data tables.
7. Other equipment needs and capital costs
7.1 Average prices of other equipment needs
7.2 Projected number of additional equipment needs (including the replacement of those currently used for theprogramme)
The information in these tables is needed to calculate the past costs and future resourcerequirements for other equipment needs and capital costs. The 2 data tables arebelow.
7.1 Average prices of other equipment needs
In table 7.1 you first need to enter information on the types (or categories) of capitalequipment you will be reporting on (e.g. computers, generators or incinerators).If the NIP uses capital equipment that is not already listed in the table, you canreplace the existing categories with the relevant ones. There is also room to includemore categories.
Enter information on the average prices (including all taxes), and overheads of otherequipment needs and capital costs listed. Typically these will include equipment forwaste management (such as incinerators), surveillance and laboratory equipment,and office equipment (such as computers).

65WHO/IVB/06.15
Per u
nit o
f equ
ipm
ent
Othe
r equ
ipm
ent
Aver
age p
rice
Aver
age m
onth
lyAv
erag
e yea
rlyNe
w (20
04)
runn
ing c
osts
main
tenan
ce co
stUS
$US
$US
$
Was
te m
anag
emen
t
Incine
rators
Othe
r (spe
cify)
Surv
eillan
ce/L
ab E
quip
men
t
Spec
imen
kits
and c
arrie
rs
Lab e
quipm
ent
Othe
r (spe
cify)
Offic
e Equ
ipm
ent
Desk
top co
mpute
rs
Photo
copy
mac
hine
er
Othe
r (spe
cify)
Othe
r
Othe
r (spe
cify)
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide66
7.2 Projected number of additional equipment needs (including thereplacement of those currently used for the programme)
In table 7.2 enter the total number of existing units of other equipment that are usedby the NIP, as well as future projections of needs by type of equipment. When makingthe future projections, be sure to include the replacement of those currently used forthe programme. Your estimates should be based on the need to reach programmeobjectives and targets as outlined in the cMYP.
Remember that because equipment, once purchased, lasts for more than a year,their value needs to be depreciated to an annual equivalent using the ULY numbersof the vehicles. The method retained in the Tool is to use five ULYs for equipment.The ULY number can be changed if you wish to use a more appropriate number foryour country context.

67WHO/IVB/06.15
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
1234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345
1234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345123451234512345
12341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234123412341234
Exist
ing
Old
No.
New
inTo
tal
Addi
tiona
l equ
ipm
ent n
eede
d in t
he fu
ture
Othe
r equ
ipm
ent
< 200
420
0420
0420
0620
0720
0820
0920
10
No.
No.
No.
No.
No.
No.
No.
No.
Was
te m
anag
emen
t
Incine
rators
Othe
r (spe
cify)
Surv
eillan
ce/L
ab E
quip
men
t
Spec
imen
kits
and c
arrie
rs
Lab e
quipm
ent
Othe
r (spe
cify)
Offic
e Equ
ipm
ent
Desk
top co
mpute
rs
Photo
copy
mac
hine
er
Othe
r (spe
cify)
Othe
r
Othe
r (spe
cify)
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide68
Section 8 - Buildings and buildings’ overheads
A final input to be considered for the cMYP costing exercise is the building spaceused to provide fixed-site immunization service deliveries (e.g. outreach post),for the storage of vaccines and supplies (e.g. cold-room building) or other buildingspace used by the NIP (e.g. surveillance laboratory or incinerator building). In viewof the relatively small value of building space in the total annual cost or futureresource requirements of the immunization programme, approximations can be madeand are likely to yield an estimate that is as accurate as applying a more complicatedmethod. Types of buildings to include would be hospitals, provincial hospitals, districthealth centres, dispensaries, and other typical fixed health posts available in the countryand used to deliver immunization services.
The simplest way to estimate the value of buildings is to use estimates of newconstruction costs for suitable buildings. Calculating the capital cost of buildingsalso involves an allocation of space devoted to immunization activities. A divisioncan be roughly estimated using staff time allocation, and the information calculatedin table 2.2 can be used to do this.
The buildings and buildings’ overheads section of the “1. Data Entry” worksheetcontains two data tables. These tables are optional but we strongly recommendedyou use them if the data is available. The tables are needed to calculate past cost andfuture resources requirements for the portion of building space and buildings’overheads (electricity, etc.) used by the NIP.
8. Building & buildings’ overheads
8.1 Average prices and overheads costs of buildings
8.2 Existing and future needs of buildings
The information in these tables is needed to calculate the past costs and future resourcerequirements for other equipment needs and capital costs. The two data tables arebelow.
8.1 Average prices and overhead costs of buildings
In table 8.1 you first need to enter information on the types of buildings that provideimmunization services, by administrative level. Various building categories are listedin the table. You may change or add categories according to your country situationand administrative structure. If there are building categories relevant to you whichare not already listed in the table, you can replace the existing ones.
For each building type, enter the average cost of the construction of the buildings,the average monthly running costs of these building (e.g. electricity, etc.), and thepercentage space used for immunization.

69WHO/IVB/06.15
Per b
uild
ing
type
Build
ing t
ype
Aver
age p
rice
Aver
age m
onth
ly%
Spa
ceNe
w (20
04)
over
head
cost
sus
ed fo
r EPI
Natio
nal
US$
US$
(%)
EPI O
ffices
Centr
al co
ld ro
om
Healt
h Clin
ic
Healt
h Fac
ilities
Disp
ensa
ries
Surve
illanc
e Lab
orato
ry
Othe
r (spe
cify)
Regi
onal
US$
US$
(%)
EPI O
ffices
Cold
room
Healt
h Clin
ic
Healt
h Fac
ilities
Disp
ensa
ries
Surve
illanc
e Lab
orato
ry
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide70
8.2 Existing and future needs of buildings
In table 8.2 enter the total number of existing buildings used by the NIP alongwith your future projection of needs, by type of building and by administrative level.For the existing buildings, separate those units that were built during the baselineyear, from those that were built before. When making future projections, the estimatesshould be based on the needs to reach programme objectives and targets, and asoutlined in the cMYP.

71WHO/IVB/06.15
Exist
ing
Old
No.
New
inTo
tal
Addi
tiona
l bui
ldin
gs n
eede
d in
the f
utur
e
Build
ing t
ype
< 200
520
0520
0520
0720
0820
0920
1020
11
No.
No.
No.
No.
No.
No.
No.
No.
EPI o
ffices
Centr
al co
ld ro
omHe
alth c
linic
Healt
h fac
ilities
Disp
ensa
ries
Surve
illanc
e lab
orato
ryOt
her (s
pecif
y)No
.No
.No
.No
.No
.No
.No
.No
.EP
I Offic
esCo
ld ro
omHe
alth c
linic
Healt
h fac
ilities
Disp
ensa
ries
Surve
illanc
e lab
orato
ryOt
her (s
pecif
y)No
.No
.No
.No
.No
.No
.No
.No
.Ou
treac
h fac
ilities
Build
ing fo
r incin
erator
sHe
alth c
linic
Healt
h fac
ilities
Disp
ensa
ries
Othe
r (spe
cify)
No.
No.
No.
No.
No.
No.
No.
No.
Outre
ach f
aciliti
esBu
ilding
for in
cinera
tors
Healt
h clin
icHe
alth f
acilit
iesDi
spen
sarie
s
Othe
r (spe
cify)

cMYP Costing & Financing Tool – User Guide72
5.3 Costing results and tables
Once all the data for the cMYP costing exercise has been collected and entered inthe appropriate tables of the “1. Data Entry” worksheet of the Tool, you can reviewthe results of the costing exercise in the “3. Costing” worksheet. This worksheetcontains three tables of results which are automatically generated.
The first is a summary table that aggregates the cost and future resource requirementaccording to the five components of a cMYP.
The second table provides the complete detail of the costing by disaggregated budgetlines according to the five components and sub-components of a cMYP.
Table 4: Costing table design
Components Sub components
Vaccine supply and logistics
1. Adequate supply of vaccines and injection equipment
Traditional routine vaccines
Underused and new vaccines
Campaigns
2. Procurement of adequate cold-chain equipment and spare parts
3. Procurement of vehicles
4. Procurement of other equipment
Service delivery
5. Adequate human resources
6. Adequate transportation needs and other recurrent overheads forservice delivery
7. Capacity-building
8. Operational costs of campaigns
Advocacy and communication
Monitoring and disease surveillance
Programme management

73WHO/IVB/06.15
Figure 7: Illustration of the detailed costing table
The detailed costing results, and the quantities, are provided for each year in thistable. For instance, the vaccine cost for a particular year will be provided along withthe number of doses needed.
The third and final table is the standard costing table that breaks down the cost bycategory (recurrent and capital), and by strategy (total NIP, routine and campaign).

cMYP Costing & Financing Tool – User Guide74
Figu
re 8
: Illu
stra
tion
of
the
FSP
styl
e co
stin
g ta
ble
Expe
nditu
reFu
ture
budg
et ne
eds
Cost
categ
ory
2004
2006
2007
2008
2009
2010
Tota
l20
06 - 2
010
Rout
ine R
ecur
rent
Cos
tUS
$US
$US
$US
$US
$US
$US
$Va
ccine
s (ro
utine
vacc
ines o
nly)
--
--
--
-Tra
dition
al Va
ccine
s-
--
--
--
New
and u
nder
used
vacc
ines
--
--
--
-Inj
ectio
n sup
plies
--
--
--
-Pe
rsonn
el-
--
--
--
Salar
ies of
full-t
ime N
IP he
alth w
orke
rs (im
muniz
ation
spec
ific)
--
--
--
-Pe
r diem
s for
outre
ach v
accin
ators/
mobil
e tea
ms-
--
--
--
Per d
iems f
or su
pervi
sion a
nd m
onito
ring
--
--
--
-Tra
nspo
rtatio
n-
--
--
--
Fixed
site
and v
accin
e deli
very
--
--
--
-Ou
treac
h acti
vities
--
--
--
-Ma
inten
ance
and o
verhe
ads
--
--
--
-Co
ld ch
ain m
ainten
ance
and o
verh
eads
--
--
--
-Ma
inten
ance
of ot
her c
apita
l equ
ipmen
t-
--
--
--
Build
ings o
verh
eads
(elec
tricity
, wate
r…)
--
--
--
-Sh
ort-te
rm tra
ining
--
--
--
-IE
C/so
cial m
obiliz
ation
--
--
--
-Di
seas
e Sur
veilla
nce
--
--
--
-Pr
ogram
me M
anag
emen
t-
--
--
--
Othe
r routi
ne re
curre
nt co
sts-
--
--
--
Subt
otal
Recu
rrent
Cos
ts-
--
--
--
Rout
ine C
apita
l Cos
t-
--
--
--
Vehic
les-
--
--
--
Cold
chain
equip
ment
--
--
--
-Ot
her c
apita
l equ
ipmen
t-
--
--
--
Subt
otal
Capi
tal C
osts
--
--
--
-

75WHO/IVB/06.15
Figu
re 8
: Illu
stra
tion
of
the
FSP
styl
e co
stin
g ta
ble
(con
t’d.
..)
Expe
nditu
reFu
ture
budg
et ne
eds
Cost
categ
ory
2004
2006
2007
2008
2009
2010
Tota
l20
06 - 2
010
Cam
paign
sUS
$US
$US
$US
$US
$US
$US
$Po
lio-
--
--
--
Vacc
ines
--
--
--
-Ot
her o
perat
ional
costs
--
--
--
-Me
asles
--
--
--
-Va
ccine
s and
supp
lies
--
--
--
-Ot
her o
perat
ional
costs
--
--
--
-Ye
llow
Feve
r-
--
--
--
Vacc
ines a
nd su
pplie
s-
--
--
--
Othe
r ope
ration
al co
sts-
--
--
--
MNT c
ampa
igns
--
--
--
-Va
ccine
s and
supp
lies
--
--
--
-Ot
her o
perat
ional
costs
--
--
--
-Ot
her c
ampa
igns (
Year
1 - R
ound
1)-
--
--
--
Vacc
ines a
nd su
pplie
s-
--
--
--
Othe
r ope
ration
al co
sts-
--
--
--
Othe
r cam
paign
s (Ye
ar 1
- Rou
nd 2)
--
--
--
-Va
ccine
s and
supp
lies
--
--
--
-Ot
her o
perat
ional
costs
--
--
--
-Ou
tbrea
ks-
--
--
--
Vacc
ines a
nd su
pplie
s-
--
--
--
Othe
r ope
ration
al co
sts-
--
--
--
Othe
r cam
paign
s-
--
--
--
Vacc
ines a
nd su
pplie
s-
--
--
--
Othe
r ope
ration
al co
sts-
--
--
--
Subt
otal
Cam
paig
n Cos
ts-
--
--
--

cMYP Costing & Financing Tool – User Guide76
Figu
re 8
: Illu
stra
tion
of
the
FSP
styl
e co
stin
g ta
ble
(con
t’d.
..)
Expe
nditu
reFu
ture
budg
et ne
eds
Cost
categ
ory
2004
2006
2007
2008
2009
2010
Tota
l20
06 - 2
010
Othe
r Cos
tsUS
$US
$US
$US
$US
$US
$US
$Sh
ared
Per
sonn
el Co
sts-
--
--
--
Share
d Tran
sport
ation
Cos
ts-
--
--
--
Cons
tructi
on of
New
Buil
dings
--
--
--
-Su
btot
al Op
tiona
l-
--
--
--
GRAN
D TO
TAL
--
--
--
-Ro
utin
e (Fi
xed D
elive
ry)
--
--
--
-Ro
utin
e (Ou
treac
h Act
ivitie
s)-
--
--
--
Cam
paign
s-
--
--
--

77WHO/IVB/06.15
Before moving on to financing, review the results of the costing in the “3. Costing”worksheet. Closer examination of the tables may yield strange results. This couldeither be due to errors in the data, or data entry into the tool, or omissions of requireddata inputs. These should be reviewed. It can happen that costing results do notappear in the costing table, and if this is the case, it means that an important piece ofinformation has not been entered in the “1. Data Entry” worksheet.
5.4 Overview of the financing and financing projections worksheets
Once the costing exercise is completed, the next step is to collect information onfinancing. This will help you analyse and understand who has been funding yourimmunization in the past, and how much financing needs to be mobilized in thefuture in order to meet cMYP objectives and targets.
The “4. Financing” worksheet has been developed for entering information neededon past and future financing, and is a crucial step in the analysis of the funding gaps.
Past Financing
Information on past financing allows for analysis of the NIP financing structure,understanding of who comprise the main donors to the programme, and alsothe level of government contribution in relation to the complete funding forimmunization. Information on past financing for the NIP will need to be enteredin the first table of the “4. Financing” worksheet.
Future Financing
Financing projection allows for the quantification and classification of potentialfuture funding. Combined with information on future resource requirements,the Tool will help you evaluate the funding gaps, i.e. the difference betweenresource requirements and available funding. This is a critical element offinancial sustainability planning. Information on future financing also needs tobe entered in the other five tables of the “4. Financing” worksheet.
Accuracy and reliability of future projections
We recognize that it is difficult to predict future financing accurately. The accuracy of projections will tend to declineas years are added to the predictions. Likewise, it is difficult to make accurate predictions about future financingtrends, particularly as governments and external partners are often unable to make long-term commitments forfunding. It will be necessary to make the most reliable projections possible through: (1) diagnosis of themacroeconomic and health sector environment in which the immunization programme operates; (2) discussionswith focal points at the MoH Finance Department, the MoF, and ICC partners. Since the financing projections madecan only be best estimates, it is important to remember that a funding gap of some size is always to be expectedwhen projecting many years into the future. It is useful to think of the final results as indicative of the futurerequirements and financing challenges faced by the NIP.
Given the uncertainty surrounding the future, especially when it relates to financing,two types of funding need to be considered — secured funding and probable funding.The exercise of classifying future financing into these two categories is known as therisk assessment.

cMYP Costing & Financing Tool – User Guide78
Secure funding refers to projected future financing available in the short term, that is considered assured.This implies that the funding has been committed and is guaranteed to be made available (for instance, there is acommitment in writing). For the most part, secure funds are pledged over two to three years or less - except in thecase of GAVI Fund awards, budget support, monies that are pooled (e.g. in a sector wide approach (SWAp),or debt relief funding for immunization (such as highly indebted poor country (HIPC) or multilateral debt reliefinitiatives (MDRI).
Probable funding refers to all other funding that is not assured but is likely to be made available in the short andmedium term. The term “probable” indicates that the projected future funding is likely to be based on historicaltrends or other information, including discussions with ministries and donors. For instance, if certain internationaldonors, such as UNICEF, have been supporting the NIP for many years but can only commit funds one year ata time, any funding beyond this year might be classified as probable, with past trends and amounts used as a guideto the future. Another example of probable funding could be future funds awarded from debt relief programmes,or new donors that could support the programme.
When completing the “4. Financing” worksheet, discuss the risks associated witheach source of financing with the ICC members, and come to a consensus on thosefunds which should be classified as secure, and conversely, which funds should beconsidered as probable.
5.5 Steps to complete the “4. Financing” worksheet
There are four steps necessary to complete the “4.Financing” worksheet.
Step 1 – Enter names of funding sources
The first step is to specify the names of the different sources of funding for yourNIP. These need to be entered in the reference information section of the “1. DataEntry” worksheet, where you can enter up to 16 different sources of funding (e.g.WHO, UNICEF, GAVI, or World Bank), of which two are default names(government and sub-national government). Each funding name entered willcorrespond to a funding column in the “4.Financing” worksheet.
What is meant by a financing source?
A source of financing refers to the agents providing the funds for immunization. Given the difficulties in tracking theexact source of financing, countries are asked to report only the source of financing closest to the end use.Therefore, transfers of bilateral donor agency resources to multilateral agencies (such as WHO or UNICEF), orto a health fund or the national treasuries (through pooled funds or budget support) are not attributed to the donorcountries. This is of particular (and growing) significance in countries receiving bilateral aid through sector-wideapproach (SWAp) programmes and national budget support.
In the Tool, only the last source of funding before use by the programme is reported. For example, if the UnitedStates Agency for International Development (USAID) channels their funds for immunization through UNICEF, thefunding is considered as UNICEF funds. In other words, UNICEF is the end source.

79WHO/IVB/06.15
Step 2 – Collect information on past and future financing
The second step involves collecting information on past and future financing.First, review key planning documents (e.g. national health sector plan, past MYP forimmunization, financial sustainability plan, expenditure reports submitted to donors,etc.) for any information on past or future financing for the NIP.
Secondly, review any available information on historical trends in governmentfinancing for immunization, and growth rates in immunization budgets and healthspending, as well as any past trends in international donor support for immunization.
Thirdly, to ensure the most reliable projections for future financing, this can be donethrough: (a) diagnosis of the macroeconomic and health sector environment in whichthe immunization programme operates; (b) discussions with focal points at the MoHFinance Department, the MoF, and ICC partners.
Proceed as follows to obtain the other financing information needed.
1) Meet with each source of funding (existing and potential) as identified inStep 1 above.
2) Provide them with the results of the costing/future resource requirementsanalysis of your NIP. You may consider presenting the “3. Costing” worksheetsfor their examination.
3) Print copies of the “4. Financing” worksheet for use in your discussions witheach funding source. Alternatively you might leave prints of these tables andask them to fill them out for you.
4) Use the ICC mechanism to facilitate this process.
5) When making future financing projections, you are encouraged to explore otherfunding possibilities.
Step 3 – Enter the information collected into the “4. Financing” worksheet
Once you have gathered all the financing data, it needs to be entered in the“4. Financing” worksheet. Past financing should be reported in the first financingtable. Future financing data should be entered in the last five tables.
Step 4 – Risk assessment
Because future financing is uncertain, it is necessary to classify the funding(identified in Step 2 and reported in the financing tables in Step 3) into those fundsthat can be considered as secure and those which should be considered as probable.The process of classifying future financing into these two categories is known as therisk assessment.
You may use information on the financing structure of your NIP, and past trends infinancing from each source to help with this assessment. Alternatively, ask donors toclassify their own risk assessment of the financing for you. This can be done inStep 2.

cMYP Costing & Financing Tool – User Guide80
For past financing there is no risk assessment to be made. By definition, all pastfunding was secured. However, the risk assessment for future financing is done byusing the “Type Risk” column next to each source-of-financing column. Simply enter“1” for secure funding and “2” for probable funding using the definitions outlinedabove. The table below provides you with an example.
Notice that if you enter a “1” in the “Type Risk” column, the financing willautomatically appear in the column of total secure funding. If “2” is entered in the“Type Risk” column, the financing will automatically appear in the column of totalprobable funding. The column “UNFUNDED” is the difference between totalresource requirements and total secure and probable funding. This refers to theamounts that are not covered by any funding.
In order to avoid any miscalculations based on the risk assessment, the column“Type Risk” will only accept entries for “1” and “2”. If you enter any other value,the following pop-up message will appear.

81WHO/IVB/06.15
Blue
cells
are
formu
la ce
lls
Total
reso
urce n
eeds
colum
n is a
utoma
ticall
yim
porte
dIf r
isk ty
pe =
1 the
finan
cing w
ill au
tomati
cally
bere
porte
d in t
he co
lumn “
Secu
re”. I
f risk
type
= 2 t
hefin
ancin
g will b
e rep
orted
in th
e colu
mn “P
roba
ble”
Type
risk
colum
n
Year
2007
Futu
re ne
eds a
nd fin
ancin
gCo
st ca
tegor
yTo
tal R
esou
rce
Tota
l sec
ured
Tota
l pro
babl
eUn
fund
edGo
vern
men
tRi
skre
quire
men
tsfin
ancin
gfin
ancin
gtyp
eRo
utin
e rec
urre
nt co
stUS
$US
$US
$US
$US
$Va
ccine
s (ro
utine
vacc
ines o
nly)
--
--
Tradit
ional
Vacc
ines
--
--
New
and u
nder
used
vacc
ines
--
--
Injec
tion s
uppli
es-
--
-Pe
rsonn
el-
--
-Sa
laries
of fu
ll-tim
e NIP
healt
h wor
kers
(immu
nizati
on sp
ecific
)-
--
-Pe
r diem
s for
outre
ach v
accin
ators/
mobil
e tea
ms-
--
-Pe
r diem
s for
supe
rvisio
n and
mon
itorin
g-
--
-Tra
nspo
rtatio
n-
--
-Fix
ed si
te an
d vac
cine d
elive
ry-
--
-Ou
treac
h acti
vities
--
--
Maint
enan
ce an
d ove
rhead
s-
--
-Co
ld ch
ain m
ainten
ance
and o
verh
eads
--
--
Maint
enan
ce of
othe
r cap
ital e
quipm
ent
--
--
Build
ings o
verh
eads
(elec
tricity
, wate
r…)
--
--
Short
-term
traini
ng-
--
-IE
C/so
cial m
obiliz
ation
--
--
Dise
ase S
urve
illanc
e-
--
-Pr
ogram
me M
anag
emen
t-
--
-Ot
her ro
utine
recu
rrent
costs
--
--
Subt
otal
Recu
rrent
Cos
ts-
--
--

cMYP Costing & Financing Tool – User Guide82
6. Analysis of results
Once all the required information is entered in the Tool, a number of basic analysesshould be undertaken to understand what the data has uncovered about the situationwith regard to costing, financing and funding gaps. Analysing the results is also away of determining whether information entered in the “1. Data Entry” and“4. Financing” worksheets is comprehensive and accurate, and reflects the objectivesand strategies of the cMYP.
Any analysis of the results of the cMYP Tool is likely to draw upon the informationpresented in the “5. Gap & Indicators”, “6. Graphs” and “7. Sustainability”worksheets.
• The “5. Gap & Indicators” worksheet contains several tables presentingyear-to-year variations in resource requirements, secure and probable financing,and financing gaps. In addition, this worksheet contains specific tables andgraphs that analyse the composition of funding gaps.
• The “6. Graphs” worksheet contains key charts on baseline costing andfinancing results, and other graphs on future resource requirements, financingand gaps. These will help you understand the level of resource requirementsneeded, and what financing will be available in the future.
• The “7. Sustainability” worksheet contains a table and chart that contextualizethe immunization programme within the broader macroeconomic and healthsystems. This sheet is important when considering the overall financialsustainability of the programme.
In the event that you wish to calculate other indicators, or prepare other charts thatare not presented in the “5. Gap & Indicators” and “6. Graphs” worksheets,you can easily insert new worksheets into the Tool to carry out separate analyses.
Remember that when developing your cMYP document, it is important to prepare awritten analysis of the data and findings, including the use of indicators and graphs.Some suggestions are provided below.
Important notes on analysis
Prior to analysing the results from the Tool remember that the choice of the information used can change the resultsand conclusions obtained. For instance, the costing results will be different depending on whether you choose toinclude only immunization specific costs, or also shared costs. Likewise, because of the risk assessment done onfuture financing, any analysis of future trends in financing and gaps will be different depending on whether youchoose to present only secured funding, probable funding, or both. Make sure that the analysis specifies whichinformation is being included.

83WHO/IVB/06.15
6.1 Analysis of past costing and financing (baseline)
A baseline analysis of past costing and financing for the programme will give you asense of how much it currently costs, what are the major cost drivers, and who ispaying for what. To help you analyse the baseline costing and financing of yourprogramme, consider commenting on the following.
• The baseline cost profile. This shows the breakdown of immunization by costcategory and as a relative share of the total. This will help identification ofwhat have been the major NIP cost drivers, and any changes through theyears. The pie graph presented below shows an example of a cost profile foran immunization programme. In many instances, it is likely that vaccines andpersonnel will account for at least 50% of the overall costs of a programme.
• The baseline financing profile. This shows the structure and breakdown ofimmunization financing by source and relative share of the total. This will helpidentification of the major sources of funding for the programme. When lookingat the financing profile it is useful to compare the share of government versusexternal funding for immunization. This will give you an impression of howself-sufficient, financially sustainable, or donor-dependant your immunizationprogramme will be.
Figure 9: Example of baseline costing and financing graphs
• Baseline indicators. These are calculated in the “5. Gap & Indicators”worksheet, and refer to items such as the cost per capita and the cost perDTP3 child. Refer to Annex II at the end of this User Guide for a completedefinition of these indicators and how to interpret them.
Baseline Cost Profile (Routine Only)
8%
28%
7%
22%
3%
18%
4%
10%
TransportationOther routine recurrent costsVehiclesCold chain equipment
Baseline Financing Profile (Routine Only)
9%
28%
7%14%
42%
GovernmentDonor 1Donor 2Donor 3GAVI
Traditional VaccinesNew and underused vaccinesInjection suppliesPersonnel

cMYP Costing & Financing Tool – User Guide84
In a written analysis of the baseline costing and financing of the programme,consider commenting on some summary figures, such as:
• total NIP programme costs;
• vaccine costs as a share of total costs;
• share of financing by government, versus other external sources of funds.
Sample analysis(EXAMPLE ONLY)
Example of the first indicators table from the “5. Gap & Indicators” worksheet :
2004
(US$)
Total Immunization Expenditures 14 353 935
Campaigns 7 256 603
Routine Immunization only 7 097 331
per capita 0.4
per DTP child 16.3
% Vaccines and supplies 38.0%
% National funding 6.9%
% Total Health Expenditures 7.5%
% Gov. Health Expenditures 13.7%
% GDP 0.2%
Total Shared Costs Specific Costs 2 685 752
% Shared health systems cost 16%
TOTAL 17 039 687
In the baseline year (2004), total spending on immunization amounted to US$ 14.3 million - half of whichwas to cover the costs of supplementary immunization campaigns. In other words, 1 in every 2 dollars forimmunization was spent on routine services. In per capita terms, the cost of immunization was about US$ 0.4.Likewise, the immunization cost per DPT3 immunized child (approximation of the cost per fully immunized child),was US$ 16. Analysing the breakdown by cost category we find that half the costs are to cover for vaccines,injection supplies and staff costs. Looking at financing, we note that less than 10% of the immunization programmeis funded using government resources. UNICEF and the GAVI Fund are the two largest donors to the programmeand account for half the financing. This indicates that the programme is highly donor-dependant for a priority healthintervention like immunization. However this is not entirely surprising as funding for the health sector has remainedlow at around US$ 5–6 per capita. To fully support the national immunization programme in the future,would require allocating about 10% of the overall government health budget. It will be important to strengthenefforts to ensure continued increase in government and partner funding for immunization, and to ensure that futurefunds are secured.
Baseline Indicators (2004)

85WHO/IVB/06.15
6.2 Analysis of future resource requirements, financing and gaps
In the same way as with past costing and financing, a number of basic analyses canbe undertaken to understand future resource drivers of each immunizationprogramme, the main sources of secured funding, how resources are mobilizedand spent over the projected period, and how quickly the gap begins to grow.During a five-year projected period, resource requirements can be expected toincrease with population growth, the introduction of new or underutilized vaccines,periodic supplementary immunization activities, and purchases of cold-chainequipment. It is useful to review how these change over time.
To help analysis of future costing and financing of the programme,consider commenting on the following.
• The future cost profile. Analysing future resource requirements by costcategory and trends over the projected period, will help identification of themajor cost drivers of your NIP and any changes over the years. The areagraph presented below is an example of a future cost profile for an immunizationprogramme. This graph is available in the “6. Graphs” worksheet of the Tool.In many instances, it is likely that vaccines and personnel will account for atleast 50% of the overall costs of a programme.
• The future financing profile. Analysing future financing by source and itstrend over time, will highlight who are the future major contributors to theimmunization programme. Remember that with risk assessment, there will betwo estimates of future funding — a worst case scenario using only securefunds, and a best case scenario using secure and probable funds. The areagraph presented above is an example of a future financing profile for animmunization programme. This graph is available in the “6. Graphs” worksheetof the Tool. This analysis will be very helpful in identifying future fundinggaps and where efforts need to be concentrated to mobilize resources.
• The level and composition of the gaps. The “5. Gap & Indicators” worksheetof the Tool will be the most useful in the analysis of any gaps, and the indicatorstable will provide a broad sense of their magnitude. A specific section of theworksheet is dedicated to the composition of the gaps which will help youidentify the major cost categories of the programme that remain unfunded, thesize of the funding gaps, and any changes over the years.

cMYP Costing & Financing Tool – User Guide86
Figure 10: Example of the future resource requirements,financing and gap graphs
Projection of Resource Requirements
$0
$2
$4
$6
$8
$10
$12
$14
2006 2007 2008 2009 2010
Mill
ions
Traditional VaccinesInjection suppliesTransportationVehiclesCampaigns
New and underused vaccinesPersonnelOther routine recurrent costsCold chain equipmentShared Costs
Future Secure Financing and Gaps
$0
$2
$4
$6
$8
$10
$12
$14
2006 2007 2008 2009 2010
Mill
ions
Funding GapGAVIDonor 2
Donor 1Sub-national Gov.Government

87WHO/IVB/06.15
Composition of the Funding Gap*
0% 20% 40% 60% 80% 100%
2006
2007
2008
2009
2010
Vaccines and injection equipmentPersonnelTransportActivities and other recurrent costsLogistics (Vehicles, cold chain and other equipment)Campaigns
Figure 11: Example of the gap analysis section of the Tool
* Immunization specific funding gap. Shared costs are not included.
Composition of the funding gap 2006 2007 2008 2009 2010 Total2006 - 2010
US$ US$ US$ US$ US$ US$Vaccines and injection equipment 324 882 2 351 616 2 873 398 2 959 616 3 208 029 11 717 541
Personnel 39 326 141 769 1 533 306 1 624 674 1 725 180 5 064 255
Transport - 8 631 385 874 365 308 489 016 1 248 829
Activities and other recurrent costs 802 699 790 974 1 983 068 2 033 616 2 093 166 7 703 523
Logistics (Vehicles, cold-chain and other equipment) 755 820 152 419 361 918 3 514 246 723 725 5 508 127
Campaigns - 2 346 745 - 2 268 597 3 671 427 8 286 769
Total Funding Gap* 1 922 727 5 792 153 7 137 564 12 766 057 11 910 543 39 529 045
Note that with the risk assessment on funding, there will be two estimates of thefinancing gap. The Tool allows you to analyse the composition of the gap accordingto secure funding only, or by both secure and probable funding.

cMYP Costing & Financing Tool – User Guide88
What are the different types of funding gaps?
Gap with secure funding. This refers to the difference between projected resource requirements and securefinancing over the corresponding period. [gap with secure funding = resource requirements - secure funding]
Gap with probable funding. This refers to the difference between projected resource requirements and bothsecure and probable financing over the corresponding period. [gap with probable funding = resource requirements- (secure + probable funding)]
• Many indicators are calculated in the “5. Gap & Indicators” worksheet,for example future cost per capita, cost per DTP3 child, and funding gaps as ashare of total resource requirement. Refer to Annex II at the end of thisUser Guide for a complete definition of these indicators and how to interpretthem.
In a written analysis of the future costing and financing of the programme,you may consider commenting on some summary figures, such as:
• total projected resource requirements over the cMYP period;
• total projected funding gap;
• funding gap as a percentage of resource requirements;
• total projected funding gap as a share of projected total spending on the healthsector;
• vaccine expenses as a share of total gap.

89WHO/IVB/06.15
Example of the Gap and Indicators table :
Resource requirements, financing and Gaps 2006 2007 2008 2009 2010 Total2006 - 2010
US$ US$ US$ US$ US$ US$Total Resource Requirements 9 141 567 10 989 081 7 568 146 13 159 783 12 239 297 53 097 873
Total Resource Requirements (Routine only) 8 158 193 7 753 196 7 568 146 10 891 186 8 567 869 42 938 590
per capita 0.4 0.4 0.4 0.5 0.4 0.4per DTP targeted child 15.7 14.5 13.0 17.1 13.1 14.7% Vaccines and supplies 41% 45% 46% 33% 45% 41%
Total Financing (Secured) 6 963 226 4 999 869 603 344 639 982 657 731 13 864 152
Government 869 169 820 400 603 344 639 982 657 731 3 590 626Donor 1 3 149 119 3 342 504 6 491 623Donor 2 831 070 836 965 1 668 035Donor 3Donor 4GAVI 2 113 868 2 113 868
Funding Gap 2 178 341 5 989 211 6 964 802 12 519 801 11 581 566 39 233 721
% of Total Needs 24% 55% 92% 95% 95% 74%
Total Financing (Not Secured - Probable) 1 330 702 2 896 371 6 552 964 8 766 163 5 546 254 25 092 455
Government 117 337 961 802 992 159 947 123 3 018 422Donor 1 1 995 106 2 043 598 2 096 308 6 135 012Donor 2 854 122 844 653 893 694 2 592 469Donor 3 250 000 275 000 302 500 332 750 366 025 1 526 275Donor 4 755 820 152 419 361 918 3 514 246 723 725 5 508 127GAVI 324 882 2 351 616 2 077 516 1 038 758 519 379 6 312 149
Funding Gap 847 640 3 092 840 411 837 3 753 638 6 035 311 14 141 266
% of Total Needs 9 % 28% 5 % 29% 49% 27%
Sample analysis(EXAMPLE ONLY)
In order to reach the cMYP objectives, expenditure on immunization would need to increase. Over the2006–2010 period, a resource envelope of about US$ 54 million would be needed. These resources include allneeds for inputs (vaccines, personnel, cold chain, vehicles, transport, etc.), and activities (training, social mobilization,surveillance, outreach, etc.). The 2006–2010 resource envelope translates to US$ 16 per DTP3-targeted child. Thisunit cost is about the same as the 2004 baseline cost, as the increase in cost is offset by higher coverage.As more children are immunized, the overall unit cost per child will drop as the costs, and particularly the fixed costs,are spread across a larger number of children. The year 2009 marks a year where large investments in equipmentrenewal will be needed. Looking at future financing, it is estimated that US$ 16 million can be considered as securedfunding between 2006 and 2010. Out of the total resource envelope required, a funding gap ofUS$ 38 million emerges. In other words, 71% of resources needed to meet programme objectives do not havesecured funding. If monies are included that will probably be made available but are not secured, the funding gap forthe entire period drops to US$ 13 million, in other words 25% of overall resources are unfunded. In the future mostof the funding gaps will be for vaccines, activities and logistics.

cMYP Costing & Financing Tool – User Guide90
6.3 Analysis of immunization strategies
In addition to the analyses that focus on the composition of cost by cost category(to understand the cost drivers of the programme), it will be useful to look at thecomposition of the costs according to immunization strategies. In other words,trying to understand how the costs are broken down into different delivery strategiesto raise coverage — fix site delivery, outreach and campaigns — and what will bethe dominant strategy.
Such an analysis will also confirm whether the strategy as defined in the cMYPobjectives has been adequately represented. For instance, you can check whetherthe timing of campaigns is aligned with those outlined in your cMYP objectives.Similarly, if one of the cMYP objectives is to strengthen outreach activities,you would expect that a significant portion of the costs would go towards this strategy.Finally, it can also highlight any imbalance in the choice of strategies. For instance,it is widely considered that focusing too strongly on campaigns at the expense ofroutine delivery systems is not sustainable in the long term. It is important to ensurethat campaigns complement routine activities, rather than the reverse.
The cost by strategy graph in the “6. Graphs” worksheet gives an example of howfuture resource requirements needed to meet cMYP objectives, can be divided intodifferent delivery strategies.

91WHO/IVB/06.15
Sample analysis(EXAMPLE ONLY)
Example of the Cost by Strategy graph of the “6. Graphs “ worksheet :
Costs by Strategy (US$ Millions)
$0.0
$2.0
$4.0
$6.0
$8.0
$10.0
$12.0
$14.0
$16.0
2006 2007 2008 2009 2010
Mill
ions
CampaignsRoutine (Fixed Delivery)Routine (Outreach Activities)
Supplemental activities are necessary in order to reach cMYP objectives. For instance, a polio sub-nationalimmunization day is planned for 2006, measles campaigns are scheduled for 2007 and 2010, and a tetanuscampaign for 2009. While in the 2004 baseline year, almost 50% of expenditure went on campaigns, suchactivities and costs will be lower in the 2006–2010 period. The average spending on campaigns over the next fiveyears will average 20% of overall spending on immunization.
6.4 Sustainability analysis
The results of the cost, financing, and gap analysis can be further analysed to give acomprehensive picture of prospects for financial sustainability. For example, the cMYPobjectives and strategies could be considered affordable if the projected funding gapwith government and partner financing was small enough to be realistically filled,taking into account financing constraints in the health sector.
The “7. Sustainability” worksheet contains a table and chart linking future resourcerequirements to the broader macroeconomic and health systems context, such asGDP or health expenditure. The table in this worksheet calculates a number ofindicators which will be extremely useful when evaluating the overall financialsustainability of your programme. For instance, if resource requirements for theimmunization programme account for a very large share of the overall health budget,it will be necessary to consider whether some elements of the programme areaffordable or even realistic.

cMYP Costing & Financing Tool – User Guide92
Example of the table and graph of the “7. Sustainability “ worksheet :
Immunization in relation to 2006 2007 2008 2009 2010macroeconomic indicators
US$ US$ US$ US$ US$ReferencePer Capita GDP ($) 265 270 276 281 287Total Health Expenditures per capita ($) 5.5 5.6 5.7 5.8 6.0Population 18 405 140 18 920 484 19 450 257 19 994 865 20 554 721
GDP ($) 4 879 914 985 5 116 883 657 5 365 359 528 5 625 901 386 5 899 095 158Total Health Expenditures ($) 101 375 511 106 298 305 111 460 151 116 872 656 122 547 992Government Health Expenditures ($) 55 756 531 58 464 068 61 303 083 64 279 961 67 401 396
Resource Requirements for ImmunizationRoutine and Campaigns ($) 9 314 444 11 223 077 7 868 289 13 466 288 12 618 615Routine Only ($) 8 331 070 7 987 192 7 868 289 11 197 692 8 947 187per DTP3 child ($) 17.0 15.9 14.3 18.7 14.5% Total Health ExpendituresResource Requirements for ImmunizationRoutine and Campaigns 9.20% 10.60% 7.10% 11.50% 10.30%Routine Only 8.20% 7.50% 7.10% 9.60% 7.30%Funding GapWith Secure Funds Only 1.90% 5.40% 6.10% 10.60% 9.40%With Secure and Probable Funds 0.60% 2.70% 0.20% 3.10% 4.90%% Government Health ExpendituresResource Requirements for ImmunizationRoutine and Campaigns 16.70% 19.20% 12.80% 20.90% 18.70%Routine Only 14.90% 13.70% 12.80% 17.40% 13.30%Funding GapWith Secure Funds Only 3.40% 9.90% 11.20% 19.30% 17.10%With Secure and Probable Funds 1.10% 5.00% 0.40% 5.70% 8.90%% GDPResource Requirements for ImmunizationRoutine and Campaigns 0.19% 0.22% 0.15% 0.24% 0.21%Routine Only 0.17% 0.16% 0.15% 0.20% 0.15%Per CapitaResource Requirements for ImmunizationRoutine and Campaigns 0.51 0.59 0.40 0.67 0.61Routine Only 0.45 0.42 0.40 0.56 0.44
The annual resource requirement needed to reach the cMYP objectives over the 2006–2010 period will representbetween 9% and 11% of the overall health budget. Considering only government health budgets, the needs for theprogramme will represent between 13% and 21%. The important yearly fluctuations result from timing of campaignsand renewal of important equipment (such as cold chain). Reaching the objectives of the cMYP will place significantpressure on the health budgets, particularly in a context where spending on health is low — less than US$ 10 percapita.
Sample analysis(EXAMPLE ONLY)

93WHO/IVB/06.15
Strategic planning for immunization will require considering alternative programmaticimprovements, or strategies, for reducing funding gaps, by exploring differentoptions for mobilizing funding by using existing financial resources for immunizationmore efficiently. Since estimating future resource requirements for immunizationis not a science, the results will be very dependent upon the availability of data andthe assumptions made. Resource estimations should be an interactive process,whereby the results improve in time as better data becomes available. Thus scenario-building is a relevant exercise for careful priority setting and the standard way ofdealing with such uncertainty (and dependence on assumptions), whether these arerelated to costs or financing.
Although baseline projections of future resource requirements, financing and gapsshould be your best estimates (realistic and reliable), it may be useful to explore theimpact on total resource requirement, financing and funding gaps for other programmescenarios. In its simplest form, scenario building implies varying key assumptions(such as costs or coverage), and assessing how sensitive the resource requirementestimations are to those changes. Similarly, scenarios can reflect more ambitiousprogramme objectives and targets, or alternatively less ambitious ones followinghistoric financing allocation trends. Resource estimations can also be made for thedifferent levels of future financing and budget constraints which are in place.
7. Scenario-building

cMYP Costing & Financing Tool – User Guide94
7.1 Types of Scenario
Scenarios can be devised in many ways as illustrated in the table below.
Table 5: Examples of costing and financing scenarios to develop
Types of scenario Examples
Costing For measuring the impact on the cost of reducing vaccine wastage, changing coveragetargets, introducing a new vaccine, changing vaccine presentation, strengthening outreachrenewing the cold chain, etc.
Financing For measuring the impact on available financing and the funding gaps of increasinggovernment contributions, alternative ways of using GAVI Fund grants, generation of newresources through alternative health financing mechanisms, or earmarking of HIPC funds forimmunization, etc.
Costing and financing For measuring the combined effect on costs, financing and funding gaps of introducing a newvaccine and increasing government funding.
Administrative level In many countries, provinces or regions vary in terms of geographical terrain, populationdensity, and socio-economic levels. These differences at the sub-national level can affect theability of immunization programmes to function and the amount of resources required for eacharea. Additionally, in countries with decentralized planning processes, decision-making aboutresources available for operational costs is often conducted at the sub-national level.For these reasons, it is often useful to estimate resource requirements at the sub-nationallevel rather than at the national level.
Long-term horizon In most cases, the planning horizon will be five years or less. In the rare cases where theplanning horizon is greater, or you simply wish to explore a long-term horizon in the contextof a financial sustainability analysis of the immunization programme, it is possible to create ascenario that will look beyond five years.
7.2 Using the Tool for scenario-building
To develop alternative scenarios, the easiest way to proceed is to create separateversions of the Tool by saving it under different file names. Make sure you label thescenario in the background information section of the “1. Data Entry” worksheetof the Tool and label the Excel file to make it easy to refer to the different versions.
Scenario-building encourages you to identify and consider the main drivers of thegap, to identify cost saving measures, and to explore ways of improving the efficiencyof resources, as well as options to mobilize additional resources for the programme.
Because of the ease of developing costing and financing scenarios using the Tool,we recommend that you develop a comparative table of results that might look likethe one shown below.

95WHO/IVB/06.15
Table 6: Comparative analysis of different scenario results
Scenario name Description Total resource Total financing Total gapsrequirements (US$) (US$ )
(US$)
Baseline Based on current objectives and $5,000,000 $2,000,000 $3,000,000targets as defined in your cMYP
Scenario 1 example: introduction of a new vaccine $8,000,000 $2,000,000 $6,000,000in 5 years
Scenario 2 example: alternative coverage and $4,000,000 $2,000,000 $2,000,000wastage targets
Scenario 3 example: increase government financing $5,000,000 $3,000,000 $2,000,000
Scenario 4 example: alternative coverage and $4,000,000 $3,000,000 $1,000,000wastage targets and increasegovernment financing
In a written analysis of the scenario, select one or two of the most feasible andaffordable ones. The findings from these scenarios should be analysed in the sameway as the baseline scenario (refer to Section 6 of the User Manual). In any case,it is essential to clearly communicate the results of the different scenarios.The final choice of these on the resource requirement estimates and/or future financing,should be based upon discussions with the various stakeholders and partners.This will increase the acceptability and “buy-in” of the results and lead to formulationof the most realistic scenario-building exercise.

cMYP Costing & Financing Tool – User Guide96
The cMYP costing and financing exercise should not be regarded as a one-off exercise,but needs to be updated in conjunction with the annual planning exercise,or as programme objectives and goals change, or are adjusted. This is an interactiveprocess in which the results improve as time goes by and better data becomes available.
The Tool is designed to make annual updates relatively straightforward, and westrongly encourage that you do this. The largest investment in time is the initialeffort to input the Tool with all the essential data, and subsequent updates ormodifications, as better data becomes available, or as programme objectives andgoals change, will not be time consuming. These will also provide many advantagesin terms of strengthening the annual planning and budgeting exercise forimmunization, reviewing changes to key assumptions, parameters and programmeobjectives to give up-to-date cMYP costing estimates, and also strengthen financialmanagement of the programme and its reporting requirements.
Annual planning and financial resources
The WHO-UNICEF Guidelines for Developing a Comprehensive Multi-Year Plan(cMYP) for Immunization recommend that for every year of the cMYP period,an annual workplan be prepared for the forthcoming year, and that this shouldinclude relevant costing and financing elements. Strong annual and multi-yearplanning, in conjunction with a budgeting process, is absolutely essential to plan for,monitor and manage the immunization programme, and to ensure that enough moneyis available to support planned inputs and activities aimed at reaching objectives andtargets.
Taking into account its estimations of resource requirements and financing needsover the cMYP period, the Tool is a good starting point for amassing the annualcosting and financing data needed for the annual workplan, and for getting a sense ofavailable funding, and funding shortfalls. Much information will be available fromthe “3. Costing” worksheet where, for each year, the tables provide both the detailedcosting results and annual quantities for inputs (e.g. vaccines, cold-chain equipment,etc.). In the same way, budgeted amounts for activities can provide a useful startingpoint for identifying the overall resource envelope planned for each year.
Review of key assumptions on costing
It will be useful to return to the Tool annually to review key assumptions. For instance,if a new population census was undertaken recently which provided new demographicdata, this can easily be entered in the Tool and all the calculations will automaticallybe recalculated based on this new information (for example, vaccine forecasts).
8. Annual monitoringusing the costing and
financing tool

97WHO/IVB/06.15
It is also possible that during the implementation phase of the cMYP, certain activitiesor programmatic objectives might change, such as, for example, the rescheduling ofa vaccination campaign, or the postponement by one year of the introduction of anew vaccine.
Such changes in key assumptions to the cMYP costing are easy to make in the Tooland should be done in the “1. Data Entry” worksheet. Systematically reviewing theassumptions and making any corresponding changes will ensure that your cMYPcosting estimates are always up-to-date.
Financial management and trends in immunization financing
If regularly updated and used, the Tool has the potential to be a powerful financialmanagement tool for an immunization programme. For instance, every year it isworth reviewing the financing projections made in the light of risk assessments done,to verify whether funding that was classified as secure has materialized,or alternatively how much of the probable funding resulted in being used that yearas payment for inputs and activities necessary to reach planned objectives. This willgive an indication of how effective the resource mobilization strategies forimmunization have been, how volatile the programme is to changes in levels offunding being made available, and how programme targets and goals are affected byfunding shortfalls, such as coverage for instance.
Ideally, expenditure on immunization for a given year should match the financingplanned for it. If estimates are correct and management is good, expenditures willmatch planned financing, and should indicate that enough resources were identified,and that cMYP objectives and targets were on track and had enough resources toachieve them. On the other hand, if planned financing is higher than actual expenditurefor a given year, it indicates that not all activities that were planned took place.Lastly, if expenditure is much higher than planned financing, it could mean that theprogramme spent funds on last–minute activities, or that activities cost more thananticipated. Either way, this can reflect a need to improve financial management.
With financing, the most common reason for expenditure being less than planned,is that money that had been anticipated never materialized. This can happen when aMoF releases only a portion of the money that had been promised in the governmentbudget, or a donor partner provides less money to support immunization objectivesthan had been anticipated.
In each of these situations, the immunization programme could be at risk becausemoney that managers had planned to use for programme implementation never becameavailable. Highlighting shortfalls such as these illustrates the dangers of inadequateand unreliable funding.
Monitoring trends in financing using the Tool will require making annual updates tothe “3. Financing” worksheet. This is a simple task of reviewing the funding thatwas planned and comparing it to the funding that was available, at the end of eachyear. It is also a useful exercise to verify how much of the probable funding anticipatedfor that year, ended up paying for inputs and activities. The exercise of doing theseyearly updates to the financing information will help build up trend informationabout the financing of the immunization programme. It will improve future planning

cMYP Costing & Financing Tool – User Guide98
for the programme and better anticipate and identify financing needs and gaps.It was also provide better understanding of volatility in financing and this can bemitigated, strengthen resource mobilization activities, and support advocacy byproviding evidence of how unreliable funding flow is detrimental to the programmeand can jeopardize attainment of the cMYP goals.
Reporting requirements
Regularly updating the Tool and using it as a financial management tool will facilitatethe task of completing any external monitoring reporting requirement forimmunization, particularly those that require costing and financing information, suchas the WHO-UNICEF joint reporting form mechanism (JRF), the GAVI annualprogress report (APR), or other reporting systems back to country-level donors.Likewise, any country that has up-to-date information on immunization costing andfinancing will be at an advantage in developing a strong proposal for funding support.This will be relevant if they are submitting an application for GAVI support.

99WHO/IVB/06.15
While the main purpose of the Tool is to help undertake the costing and financingelements of a cMYP, and to make projections of future resource requirements,financing, and gaps in reaching programme objectives and targets as defined in themulti-year plan, the Tool is not designed for cost-effectiveness analysis (CEA).Although defining programme objectives and strategies during the development of acMYP should be based on cost-effectiveness considerations, the Tool, in its currentdesign, is ill equipped to strengthen this priority-setting exercise. Likewise, the Toolis not designed to determine allocative efficiency, when a critical consideration inany planning and budgeting exercise should be the efficient use of funds.
However, the costing data and information generated by the Tool can support acost-effectiveness analysis. In the case of immunization, CEA methods can helpdetermine whether investment in a new vaccine will achieve greater or lesser publichealth outcomes relative to investment in another type of vaccine presentation orpublic health programme. They can also identify which delivery strategies will givethe best value for money in terms of protecting children against vaccine preventablediseases.
In the same way, the financing information from the Tool (particularly if it is used asa financial management tool, and trend information is available), can help programmemanagers improve future allocative efficiency of funds and aid in analysis ofprogramme cost-saving measures.
There are several published methods and approaches to cost effectiveness,allocative efficiency and cost-savings analysis, and information to be found on thewebsites listed below will provide a good starting point.
Cost Effectiveness http://www.who.int/choice/en/.
Health Economics http://www.who.int/topics/health_economics/en/.
Health Financing http://www.who.int/health_financing/en/.
9. Other uses of thecosting and financing tool
information

cMYP Costing & Financing Tool – User Guide100
The following table summarizes the data required for the “1. Data Input” worksheetof the Tool including guidance on data sources and strategies for obtaining thisinformation. This table provides guidance on the nature and extent of the workinvolved in the data collection process.
However the table is not a substitute for the guidance on the “1. Data Entry”worksheet provided in Part 4 of this User Guide, and this should be read beforestarting work.
Annex I:Summary table of data needs and sources

101WHO/IVB/06.15
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
1.Va
ccine
s & in
jectio
nDe
mogr
aphic
data:
The v
accin
e log
istics
perso
n at th
e cen
tral c
old ro
om sh
ould
have
reco
rds o
f dist
ributi
on, u
sage
and
supp
lies
last p
opula
tion c
ensu
s; tot
al po
pulat
ion; p
opula
tion g
rowth
rate;
stock
s of v
accin
es an
d inje
ction
supp
lies (
includ
ing un
it pric
es).
birth
rate;
unde
r 1 po
pulat
ion; in
fant m
ortal
ity ra
te (IM
R);
preg
nant
wome
n (PW
); chil
dbea
ring a
ge w
omen
(CBA
W).
If the
vacc
ines a
re la
rgely
exter
nally
finan
ced,
inter
natio
nal d
onor
s in t
he co
untry
(e.g.
UNI
CEF,
JICA,
etc.) w
ill als
o hav
e rec
ords
of va
ccine
supp
lies,
includ
ing un
it pric
es.
Vacc
ine in
forma
tion:
vacc
inatio
n sch
edule
; vial
size
of va
ccine
s; pr
ices p
er do
se;
They
are a
lso lik
ely to
have
relev
ant in
forma
tion o
n the
purch
ase o
f injec
tion s
uppli
es.
past
quan
tities
supp
lied a
nd ad
minis
tered
; pas
t cov
erag
e rate
s;fut
ure c
over
age a
nd w
astag
e tar
gets.
Coun
tries u
sing l
ocal
proc
urem
ent s
ystem
s for
vacc
ines a
nd pu
rchas
ing di
rectl
y thr
ough
the m
arke
t,sh
ould
have
reco
rds a
nd in
voice
s on t
he pu
rchas
ing an
d sup
plies
of va
ccine
s (inc
luding
unit p
rices
) at
Injec
tion s
uppli
es:
the M
oH.
need
s for
mixi
ng sy
ringe
s; un
it pric
es fo
r auto
-disa
ble (A
D) sy
ringe
s;re
cons
titutio
n syri
nges
and s
afety
boxe
s; fre
ight a
nd ot
her ta
xes o
nCo
untrie
s tha
t hav
e a lin
e item
for v
accin
es in
their
natio
nal b
udge
t can
obtai
n info
rmati
on fro
minj
ectio
n sup
plies
.go
vern
ment
reco
rds a
t the M
oH or
the M
oF.
Relev
ant in
forma
tion m
ay be
avail
able
from
the m
ulti-y
ear p
lans,
a rec
ent E
PI as
sess
ment
or G
AVI
docu
ments
such
as an
nual
prog
ress
repo
rts (A
PRs).
The a
nnua
l NIP
actio
n plan
shou
ld be
cons
ulted
for a
ny re
levan
t data
.

cMYP Costing & Financing Tool – User Guide102
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s (c
ont’
d...)
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
2. Pe
rsonn
elTo
tal nu
mber
of ex
isting
staff
invo
lved i
n imm
uniza
tion a
nd th
eW
hen c
ollec
ting i
nform
ation
on pe
rsonn
el, it
is ea
sy to
tabu
late t
he to
tal nu
mber
of w
orke
rs by
categ
ory.
categ
ory o
f staf
f.Th
en us
e sala
ry gr
ades
avail
able
at the
MoH
and a
pply
these
to th
e diffe
rent
categ
ories
of pe
rsonn
el.De
tails
of oth
er be
nefits
can b
e coll
ected
from
direc
t inter
views
with
indiv
iduals
and a
vera
ged b
yAv
erage
perce
ntage
of st
aff tim
e spe
nt ea
ch m
onth
on ro
utine
categ
ory of
staff
.im
muniz
ation
servi
ces (
staff t
ime =
100%
for im
muniz
ation
spec
ificpe
rsonn
el; st
aff tim
e < 10
0% fo
r sha
red p
erso
nnel)
.Ex
pend
iture
reco
rds a
nd pa
yrolls
in th
e MoH
or M
oF w
ill su
pply
infor
matio
n on s
alarie
s, all
owan
ces
and s
alary
grids
by ty
pe of
staff
.Av
erag
e mon
thly s
alary
of the
staff
and o
ther a
llowa
nces
and b
enefi
ts.Pe
r diem
s for
outre
ach a
nd su
pervi
sion s
taff a
re of
ten pa
id by
inter
natio
nal d
onor
s, an
d the
rates
shou
ldAv
erag
e num
ber o
f day
s a m
onth
cond
uctin
g outr
each
and
be av
ailab
le dir
ectly
from
the do
nor a
genc
ies pr
esen
t in th
e cou
ntry.
supe
rvisio
n.Th
e ave
rage
perce
ntage
time s
pent
on im
muniz
ation
can b
e esti
mated
by su
rveyin
g a sa
mple
ofAv
erag
e per
diem
rate
for co
nduc
ting o
utrea
ch ac
tivitie
s and
repr
esen
tative
healt
h fac
ilities
at ea
ch ad
minis
trativ
e lev
el.su
pervi
sion.
Total
numb
er of
future
staff
need
s and
the c
atego
ry of
staff.
If you
choo
se to
wor
k with
aver
age p
erso
nnel
by ty
pe an
d by d
iffere
nt ad
minis
trativ
e lev
els or
type
s of
healt
h fac
ility i
n the
coun
try, w
e rec
omme
nded
you u
nder
take a
small
surve
y. Th
e step
s to c
ollec
t the
nece
ssar
y data
are a
s foll
ows.
1.Co
llect
infor
matio
n on t
he to
tal nu
mber
of fix
ed he
alth f
acilit
ies in
the c
ountr
y by c
atego
ry an
d by
differ
ent a
dmini
strati
ve le
vels
(e.g.
prov
incial
hosp
itals,
distr
ict he
alth c
entre
s, dis
pens
aries
, and
other
fixed
sites
). The
se he
alth f
acilit
ies m
ust p
rovid
e imm
uniza
tion s
ervic
es.
2.Fo
r eac
h typ
e of h
ealth
facil
ity, s
elect
one t
hat is
repr
esen
tative
(i.e.
a rep
rese
ntativ
e pro
vincia
lho
spita
l or d
istric
t hea
lth ce
ntre)
. The
term
repr
esen
tative
impli
es re
pres
entat
ive in
size
(total
numb
erof
healt
h wor
kers)
, and
utiliz
ation
(num
bers
of ch
ildre
n imm
unize
d).
3.Int
ervie
w the
se re
pres
entat
ive he
alth f
acilit
ies by
admi
nistra
tive l
evel,
eithe
r by f
ax, te
lepho
ne or
direc
t visi
t and
ask f
or in
forma
tion o
n:the
total
numb
er of
staff
invo
lved i
n imm
uniza
tion a
nd th
e cate
gory
of sta
ff;av
erag
e per
centa
ge of
staff
time s
pent
each
mon
th on
routi
ne im
muniz
ation
servi
ces;
aver
age m
onthl
y sala
ry of
the st
aff an
d othe
r allo
wanc
es an
d ben
efits;
numb
er of
days
a mo
nth co
nduc
ting o
utrea
ch, a
nd th
e outr
each
per d
iems;
numb
er of
days
a mo
nth co
nduc
ting s
uper
vision
and t
he pe
r diem
rates
.

103WHO/IVB/06.15
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s (c
ont’
d...)
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
3.Ve
hicles
and t
ransp
ortVe
hicles
The v
ehicl
e log
istics
perso
n at th
e cen
tral le
vel im
muniz
ation
depa
rtmen
t sho
uld ha
ve an
itemi
zed l
isting
Numb
er of
vehic
les us
ed en
tirely
or pa
rtially
for im
muniz
ation
,of
all ve
hicles
used
for th
e nati
onal
immu
nizati
on pr
ogra
mme.
by ve
hicle
type a
nd by
admi
nistra
tive l
evel
in the
coun
try.
Expe
nditu
re re
cord
s may
give
some
indic
ation
of th
e tota
l cos
t of o
pera
ting a
nd m
aintai
ning v
ehicl
es,
Unit p
rice o
f veh
icles
by ty
pe. T
he pr
ice sh
ould
includ
e fre
ight
but it
is lik
ely th
at int
ervie
wing
drive
rs an
d mec
hanic
s, an
d con
sultin
g log
book
s will b
e nec
essa
ry to
get
char
ges a
nd ot
her re
levan
t taxe
s.a s
uffici
ently
detai
led pi
cture.
Avera
ge pe
rcenta
ge tim
e use
d for
immu
nizati
onFu
rther
infor
matio
n can
be ob
taine
d by l
ookin
g at e
xpen
ditur
e rec
ords
, invo
ices f
or ve
hicle
repa
irs, fu
el(1
00%
= im
muniz
ation
spec
ific; <
100%
= sh
ared
).bil
ls, et
c., w
hich c
an gi
ve an
indic
ation
of th
e tota
l cos
t of o
pera
ting a
nd m
aintai
ning v
ehicl
es.
Aver
age n
umbe
r of u
seful
life y
ears
(ULY
)Su
pply
reco
rds,
invoic
es, a
nd re
ceipt
s for
vehic
les pu
rchas
ed by
inter
natio
nal d
onor
s, ar
e ano
ther
sourc
e of d
ata.
Addit
ional
futur
e num
ber o
f nee
ded v
ehicl
es us
ed en
tirely,
or pa
rtially
for im
muniz
ation
by ve
hicle
type a
nd by
admi
nistra
tive l
evel
in the
The p
erce
ntage
time s
pent
on im
muniz
ation
can b
e diffi
cult t
o esti
mate.
In ge
nera
l, exp
ert o
pinion
orco
untry
.re
spon
ses f
rom
a sma
ll sam
ple su
rvey o
f facil
ities m
ay pr
ovide
the n
eces
sary
data
to es
timate
perce
ntage
time.
Tran
spor
tAv
erag
e num
ber o
f kilo
metre
s tra
velle
d per
year
by ve
hicle
type.
Relev
ant in
forma
tion a
nd un
it pric
es m
ay be
avail
able
from
the m
ulti-y
ear p
lan an
d rec
ent E
PIas
sess
ments
. The
annu
al NI
P acti
on pl
an sh
ould
be co
nsult
ed fo
r relev
ant d
ata.
Aver
age f
uel c
onsu
mptio
n in l
itres p
er 10
0 km
by ve
hicle
type.
If you
choo
se to
wor
k on a
vera
ge ve
hicle
numb
er by
type
and b
y diffe
rent
admi
nistra
tive l
evel
or ty
pe of
Aver
age f
uel p
rice p
er lit
re.
healt
h fac
ility i
n the
coun
try, w
e rec
omme
nd th
at yo
u und
ertak
e a sm
all su
rvey.
The s
teps t
o coll
ect th
ene
eded
data
are a
s foll
ows.
1.Co
llect
infor
matio
n on t
he to
tal fle
et of
vehic
les fo
r immu
nizati
on by
vehic
le typ
e, su
ch as
numb
er of
cars,
four
-whe
el dr
ive ve
hicles
, moto
rcycle
s, bic
ycles
, boa
ts, et
c.2.
Selec
t from
each
type
of ve
hicle,
one t
hat is
repr
esen
tative
. For
insta
nce t
he fle
et of
four-w
heel
drive
vehic
les m
ay be
comp
osed
of se
vera
l mod
els (s
uch a
s Toy
ota La
nd-C
ruise
r or M
itsub
ishi).
Choo
se th
e mod
el tha
t is m
ost re
pres
entat
ive in
term
s of n
umbe
rs, ag
e, mi
leage
, and
usag
e.3.
Inter
view
drive
rs for
each
vehic
le typ
e and
ask t
hem
to pr
ovide
(to th
e bes
t of th
eir kn
owled
ge), a
nav
erag
e fue
l con
sump
tion,
the av
erag
e dist
ance
trave
lled p
er ye
ar, an
d the
perce
ntage
time t
heve
hicle
is us
ed fo
r immu
nizati
on re
lated
activ
ities.
Prefe
rably
choo
se dr
ivers
that h
ave b
een
worki
ng fo
r the n
ation
al im
muniz
ation
prog
ramm
e for
seve
ral y
ears
and h
ave t
he be
st kn
owled
ge of
this in
forma
tion.
4.Ob
tain i
nform
ation
on ho
w ma
ny ve
hicles
will b
e nee
ded i
n the
futur
e.

cMYP Costing & Financing Tool – User Guide104
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s (c
ont’
d...)
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
4.Co
ld-ch
ain eq
uipme
nt an
dCo
ld ch
ainTh
e cold
-chain
logis
tics a
nd re
pairs
perso
n at th
e cen
tral c
old ro
om of
the M
oH sh
ould
have
an ite
mize
dma
inten
ance
/overh
eads
Numb
er of
exist
ing un
its of
cold
chain
used
entire
ly for
immu
nizati
on,
listin
g of a
ll cold
-chain
equip
ment
used
by th
e NIP.
by ty
pe of
cold
chain
and b
y adm
inistr
ative
leve
l in th
e cou
ntry.
Supp
ly re
cord
s, inv
oices
and r
eceip
ts for
cold-
chain
equip
ment
purch
ased
by in
terna
tiona
l don
ors a
reUn
it pric
e of c
old-ch
ain eq
uipme
nt by
type
. The
price
shou
ld inc
lude
anoth
er so
urce o
f infor
matio
n.fre
ight c
harg
es an
d othe
r relev
ant ta
xes.
Rece
nt co
ld-ch
ain re
views
are a
good
sour
ce of
infor
matio
n on t
he ite
mize
d list
ing of
exist
ing co
ld-ch
ainAv
erag
e num
ber o
f ULY
.eq
uipme
nt an
d futu
re re
place
ment
need
s. Su
ch re
views
are l
ikely
to inc
lude u
nit pr
ices.
The a
nnua
l plan
of ac
tion f
or th
e NIP
shou
ld be
cons
ulted
for re
levan
t data
.Ad
dition
al fut
ure n
umbe
r of c
old-ch
ain un
its ne
eded
by ty
pe an
d by
admi
nistra
tive l
evel
in the
coun
try.
If you
choo
se to
wor
k on a
vera
ge co
ld-ch
ain eq
uipme
nt by
type
and b
y diffe
rent
admi
nistra
tive l
evels
ortyp
es of
healt
h fac
ility i
n the
coun
try, w
e rec
omme
nd th
at yo
u und
ertak
e a sm
all su
rvey.
The s
teps t
oMa
inten
ance
/over
head
sco
llect
the ne
eded
data
are a
s foll
ows.
Aver
age m
onthl
y run
ning c
osts
of the
cold
chain
by ty
pe of
equip
ment.
1.Ga
ther th
e item
ized l
ist of
all c
old-ch
ain eq
uipme
nt in
the co
untry
by ty
pe of
equip
ment
(free
zers,
Aver
age y
early
main
tenan
ce ch
arge
s for
the c
old ch
ain by
type
ofre
friger
ators,
cold
boxe
s, va
ccine
carri
ers,
etc.).
equip
ment.
2.Us
ing ex
pend
iture
state
ments
, invo
ices a
nd re
ceipt
s on t
he pu
rchas
e of c
old-ch
ain eq
uipme
nt (o
r are
cent
cold-
chain
revie
w), a
ttribu
te the
corre
ct pu
rchas
e pric
e to e
ach t
ype o
f cold
-chain
equip
ment.
Whe
n the
purch
ase p
rice f
or a
spec
ific m
odel
is no
t kno
wn, u
se th
e ave
rage
price
for th
at ca
tegor
yof
equip
ment.
For in
stanc
e the
re m
ay be
vario
us m
odels
of fri
dges
and f
reez
ers (
e.g. R
CW,
Elec
trolux
, Sibi
r, etc.
). If th
e unit
price
of ea
ch m
odel
is no
t kno
wn, li
st the
aver
age p
rice f
or th
ewh
ole ca
tegor
y.3.
By m
eans
of in
tervie
ws w
ith th
e cold
-chain
logis
tics a
nd re
pairs
staff
, dete
rmine
the a
vera
gemo
nthly
runn
ing co
st an
d ave
rage
year
ly ma
inten
ance
cost
of the
type
s of c
old-ch
ain eq
uipme
ntlis
ted.

105WHO/IVB/06.15
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s (c
ont’
d...)
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
5.Ca
mpaig
nsPa
st sp
endin
g on o
pera
tiona
l cos
ts fro
m SI
A, by
type
of ca
mpaig
ns.
In ma
ny co
untrie
s, ca
mpaig
ns an
d othe
r sup
pleme
ntal im
muniz
ation
activ
ities a
re of
ten fu
nded
byex
terna
l don
ors.
Usua
lly go
od ex
pend
iture
reco
rds a
re ke
pt an
d the
se sh
ould
be av
ailab
le dir
ect fr
om th
eAv
erag
e ope
ratio
nal c
ost p
er ch
ild by
type
of ca
mpaig
n.do
nor a
genc
ies pr
esen
t in th
e cou
ntry.
Pre-
camp
aign r
epor
ts an
d micr
o-pla
ns ar
e like
ly to
be a
good
sour
ce of
infor
matio
n. Th
e ann
ual N
IPac
tion p
lan sh
ould
be co
nsult
ed fo
r relev
ant d
ata.
Post-
camp
aign r
eport
s ofte
n rep
ort th
e ope
ration
al co
sts of
the c
ampa
ign, in
cludin
g the
avera
geop
erati
onal
costs
per c
hild a
nd ex
pend
iture
.
6.Ac
tivitie
s and
othe
rPa
st sp
endin
g on s
hort-
term
traini
ng, IE
C/so
cial m
obiliz
ation
, othe
rIn
many
coun
tries o
ther re
curre
nt co
sts su
ch as
traini
ng an
d soc
ial m
obiliz
ation
are o
ften f
unde
d by
recurr
ent c
osts
supe
rvisio
n cos
ts (e
xclud
ing pe
r diem
s), m
onito
ring a
nd di
seas
eex
terna
l don
ors.
Usua
lly go
od ex
pend
iture
reco
rds a
re ke
pt an
d the
se sh
ould
be av
ailab
le dir
ect fr
om th
esu
rveilla
nce a
nd ot
her o
utrea
ch co
sts (e
xclud
ing pe
r diem
s, tra
nspo
rtdo
nor a
genc
ies pr
esen
t in th
e cou
ntry.
and i
ce), a
nd an
y othe
r rec
urre
nt co
sts th
at ar
e rele
vant
to the
NIP.
Key i
nform
ants
at the
MoH
and i
mmun
izatio
n dep
artm
ent c
an be
a so
urce
of da
ta. C
onsu
lt the
irex
pend
iture
statem
ents
and r
eport
s as a
poten
tial s
ource
.
Relev
ant in
forma
tion m
ay be
avail
able
from
past
multi-
year
plan
s and
EPI
asse
ssme
nts. T
he N
IPan
nual
actio
n plan
shou
ld be
cons
ulted
for re
levan
t data
.
7.Ot
her c
apita
l cos
tsNu
mber
of ex
isting
equip
ment
used
spec
ificall
y for
the N
IPIn
many
coun
tries o
ther re
curre
nt co
sts su
ch as
traini
ng an
d soc
ial m
obiliz
ation
are o
ften f
unde
d by
(othe
r than
vehic
les an
d cold
chain
), by t
ype o
f equ
ipmen
t.ex
terna
l don
ors.
Usua
lly go
od ex
pend
iture
reco
rds a
re ke
pt an
d the
se sh
ould
be av
ailab
le dir
ect fr
om th
edo
nor a
genc
ies pr
esen
t in th
e cou
ntry.
Estim
ated p
rice o
f the e
quipm
ent b
y typ
e.Ke
y info
rman
ts at
the M
oH an
d imm
uniza
tion d
epar
tmen
t can
be a
sour
ce of
data.
Con
sult t
heir
Aver
age n
umbe
r of U
LY.
expe
nditu
re sta
temen
ts an
d rep
orts a
s a po
tentia
l sou
rce.
Futur
e num
ber o
f unit
s of e
quipm
ent n
eede
d by t
ype.
Relev
ant in
forma
tion m
ay be
avail
able
from
past
multi-
year
plan
s and
EPI
asse
ssme
nts. T
he N
IPan
nual
actio
n plan
shou
ld be
cons
ulted
for re
levan
t data
.

cMYP Costing & Financing Tool – User Guide106
Sum
mar
y Ta
ble
of d
ata
need
s an
d so
urce
s (c
ont’
d...)
Data
inpu
t sec
tion
Data
need
sDa
ta so
urce
tips
8.Bu
ilding
and b
uildin
gs’
Build
ings
The p
lannin
g or b
uildin
g dep
artm
ents
of the
MoH
will b
e able
to pr
ovide
the t
otal n
umbe
r of h
ealth
facil
ities
overh
eads
Numb
er of
exist
ing bu
ilding
s whe
re im
muniz
ation
servi
ces a
reby
type
and b
y adm
inistr
ative
leve
l in th
e cou
ntry (
hosp
itals,
prov
incial
hosp
itals,
distr
ict he
alth c
entre
s,(O
ption
al)pr
ovide
d in t
he co
untry
, by t
ype o
f buil
ding.
disp
ensa
ries,
and o
ther fi
xed s
ites).
Estim
ated v
alue o
f buil
dings
by ty
pe.
As m
ainten
ance
and o
verh
eads
costs
are u
suall
y fina
nced
by th
e MoH
, it is
not u
ncom
mon f
or ea
chhe
alth f
acilit
y to r
eceiv
e mon
thly,
quar
terly
or an
nual
funds
from
the na
tiona
l or s
ub-n
ation
al lev
el to
cove
rAv
erag
e per
centa
ge sp
ace u
sed f
or im
muniz
ation
all op
erati
ng co
sts fo
r the h
ealth
facil
ities (
such
as, s
alarie
s, ma
inten
ance
and o
verh
eads
).(1
00%
= im
muniz
ation
spec
ific; <
100%
= sh
ared
).
Avg.
numb
er of
ULY
.Ac
coun
ts for
each
type
of fa
cility
(rec
orde
d in t
heir e
xpen
ditur
e rep
orts)
may
be av
ailab
le at
the M
oH or
MoF.
This
is on
e cate
gory
wher
e rec
orde
d exp
endit
ure d
ata is
quite
adeq
uate.
Rec
urre
nt co
sts fo
rBu
ilding
s ove
rhea
dsbu
ilding
s will
norm
ally b
e list
ed un
der s
uch h
eadin
gs as
“Utili
ties”,
“Main
tenan
ce”, “
Clea
ning”
, or
Aver
age m
onthl
y run
ning c
ost p
er bu
ilding
type
.“S
ecur
ity”.
The s
imple
st wa
y to e
stima
te the
value
of bu
ilding
s is t
o use
estim
ates o
f new
cons
tructi
on co
sts fo
rsu
itable
build
ings.
The a
vera
ge pe
rcenta
ge sp
ace u
sed f
or im
muniz
ation
can b
e app
roxim
ated u
sing s
taff ti
me al
locati
on.
For e
xamp
le, if
50%
of th
e staf
f in a
repr
esen
tative
healt
h fac
ility s
pend
20%
of th
eir tim
e on
immu
nizati
on, th
en 10
% of
the v
alue o
f the b
uildin
g migh
t reas
onab
ly be
attrib
uted t
o imm
uniza
tion.
The i
nform
ation
calcu
lated
for p
erson
nel c
an be
used
to m
ake t
he ap
portio
nmen
t.
If you
choo
se to
wor
k on a
vera
ge co
ld-ch
ain eq
uipme
nt by
type
and b
y diffe
rent
admi
nistra
tive l
evels
ortyp
es of
healt
h fac
ility i
n the
coun
try, w
e rec
omme
nd th
at yo
u und
ertak
e a sm
all su
rvey.
The s
teps t
oco
llect
the ne
cess
ary d
ata ar
e as f
ollow
s.
1.Co
llect
infor
matio
n on t
he to
tal nu
mber
of fix
ed he
alth f
acilit
ies in
the c
ountr
y by c
atego
ry (p
rovin
cial
hosp
itals,
distr
ict he
alth c
entre
s, dis
pens
aries
, and
othe
r fixe
d site
s). Id
entify
the t
otal n
umbe
r of
healt
h fac
ilities
that
prov
ide im
muniz
ation
servi
ces b
y typ
e.2.
For e
ach t
ype o
f hea
lth fa
cility
, sele
ct on
e tha
t is re
pres
entat
ive (i.
e. a r
epre
senta
tive p
rovin
cial
hosp
ital o
r a re
pres
entat
ive di
strict
healt
h cen
tre). T
he te
rm re
pres
entat
ive im
plies
repr
esen
tative
insiz
e (tot
al nu
mber
of he
alth w
orke
rs) an
d utili
zatio
n (in
terms
of nu
mber
s of c
hildr
en im
muniz
ed).
3.Int
ervie
w the
se re
pres
entat
ive he
alth f
acilit
ies, e
ither
by fa
x, tel
epho
ne or
dire
ct vis
it and
ask f
orinf
orma
tion o
n the
aver
age v
alue o
f the b
uildin
g, an
d the
aver
age m
onthl
y ope
ratio
nal c
osts
forru
nning
the b
uildin
g (ex
cludin
g sala
ries).

107WHO/IVB/06.15
The list of required cost categories retained for the data tables are defined below.
Cost and resource requirements
Recurrent costs. These include the costs associated with inputs that will beconsumed or replaced in one year or less. The recurrent cost-categories used in theTool include the following: vaccines (traditional and new and underused vaccines);injection supplies; personnel; transport; maintenance and overheads; training;social mobilization/IEC; surveillance and monitoring.
• Vaccines. These include the cost of all the vaccines used in the nationalimmunization programme and following each country’s vaccination schedule— traditional vaccines such as, Bacille Calmette-Guérin vaccine (BCG),diphtheria-tetanus-pertussis (DTP), polio vaccine (OPV), measles vaccine andtetanus toxoid vaccine (TT), as well as new and underused vaccines such as,Hepatitis B (HepB), Haemophilus Influenza type B (Hib), and yellow fevervaccine. The cost of the vaccines includes the international market price aswell as transport and handling costs.
• Injection supplies. These include items such as needles, syringes, auto-disablesyringes (AD), safety boxes and other injection supplies. The cost of theinjection supplies includes the international market value of injection equipmentas well as transport and handling charges.
• Personnel. Includes the salaries and benefits of full-time (programme-specific)personnel involved with the organization and delivery of immunizationactivities, and should be recorded at the central, provincial and district levels.Personnel costs include per diems and other incentives for service deliveryand outreach activities. Note that countries are encouraged to estimate theshared cost of personnel, even though this is not required in the MYP.
• Transport. Includes the costs related to the operations and maintenance ofvehicles for the delivery of vaccines, supplies and immunization services(fuel for example). Countries are encouraged to estimate the shared cost oftransport even though this is not required in the MYP.
• Maintenance and overheads. Includes the maintenance costs of cold-chainequipment and buildings’ overheads and costs (such as electricity).
• Training. Includes short-term in-service training for immunizationactivities (for any type of health staff involved), that occur on a regular basis(e.g. training for new vaccine introduction, injection safety, logistics,vaccine management, etc.).
Annex II:Glossary of important cMYP costing terms

cMYP Costing & Financing Tool – User Guide108
• Social mobilization/IEC. Includes spending on social mobilization activitiesand IEC materials relating to the benefits of immunization.
• Disease surveillance and monitoring. Includes spending on diseasesurveillance, supervision and monitoring activities.
• Other recurrent costs. Includes any other recurrent NIP cost category whichis not specified elsewhere.
Capital costs. These are the costs of resources that have a value over US$ 100 andare not consumed or replaced every year. Given that capital equipment will last formore than one year, its value is depreciated (or amortized) over its lifetime — theULY. The capital-cost categories used in the Tool include: vehicles; cold-chainequipment; and other immunization-specific equipment such as incinerators,laboratory equipment, etc. The suggested method for the treatment of capital cost isa simple straight line depreciation — the value of the new equipment is divided by itsULY.
• Vehicles. Includes the annual value of the existing fleet of vehicles usedspecifically by the NIP. These typically consist of cars, four-wheel drive vehicles,trucks, motorcycles, bicycles, and/or boats.
• Cold-chain equipment. Includes the annual capital cost of existing and newcold-chain equipment specifically for use by the NIP. These typically consistof freezers, refrigerators, cold boxes and vaccine carriers.
• Other capital costs. Includes the annual value of any other capital-cost categorynot specified elsewhere. Countries are encouraged to estimate the shared costof buildings, even though this is not required in the cMYP costing exercise.
Specific costs. Also termed “programme-specific costs”, these include the cost ofall inputs used specifically for immunization and not shared with any other healthservice. Their utilization will be 100% for the national immunization programme.Specific costs are intended to be those that the immunization programme has tomobilize for itself alone. They are also considered to be those that are the mostcomparable across countries, with the least chance of distortion due to differences inestimation methods.
Shared costs. Include the cost of inputs that are shared among multiple health services.Traditionally, shared costs include those for service delivery personnel, since theyoften perform multiple duties beyond immunization, making it difficult to separateout the share to be attributed to immunization. The process whereby the sharedportion of certain costs is separated out is known as cost allocation. Other sharedcosts will be those associated with transportation and buildings.
Cost projections. This corresponds to the total future costs of both recurrent andcapital inputs to the NIP and is based on its the programme objectives.However, the future value of capital equipment is depreciated (or amortized) overits lifetime — the ULY. In other words, the value of the capital equipment is spreadout over the number of years it will be used and brought to an annual equivalent.An advantage of working with future cost projections is that important cost indicatorscan be computed and these are comparable over time (e.g. annual variations in theNIP cost per capita, or cost per fully immunized child). The cost projection approach

109WHO/IVB/06.15
has certain limitations, which are that it does not allow for an accurate comparisonbetween future financial resource requirements of the programme and requiredfunding. This is the rational for the resource requirements approach.
Projection of future resource requirements. This corresponds to the total futureresource requirements (also termed “future resource needs”), of both recurrent andcapital inputs to the NIP and is based on the its programme objectives. For capitalequipment this means that the value of the capital inputs are not depreciated as is thecase in the cost projections approach. Since existing capital equipment has alreadybeen paid for, the resource requirements approach is most relevant when looking atexact amounts of future financing that need to be mobilized each year. The advantageof this approach is that it allows for comparisons between future resourcerequirements and future financing, and how the two need to be matched in order toreduce the financial gaps.
Strategies
NIP. This refers to the National Immunization Programme in its entirety. The NIPstrategy includes all costs, resource requirements and financing for both routineimmunization services and campaigns (also known as supplemental immunizationactivities). [NIP = routine + campaigns]. Note that the total NIP costs, resourcerequirements and/or financing aggregates can be based on either programme specificcosts or both specific and shared costs.
Routine. This refers to routine immunization. The routine strategy will include allcosts, resource requirements and financing for routine immunization services only,and excludes campaigns (also known as supplemental immunization activities).[routine = NIP - campaigns]. Note that the total routine costs, resource requirementsand/or financing aggregate can be based on either programme specific costs or bothspecific and shared costs.
Campaigns. This refers to supplemental immunization activities. The campaignstrategy will include all costs, resource requirements and financing for supplementalimmunization activities such as mass measles campaigns or national polioimmunization days. By definition, the campaign strategy will exclude any costs,resource requirements and financing for routine immunization delivery services.[campaigns = NIP - routine]. Note that the total campaign costs, resource requirementsand/or financing aggregates can be based on either programme-specific costs orboth specific and shared costs.
Financing and Gaps
Total secure funding. Secure funding refers to projected future financing which isavailable in the short term and which is considered as assured. This implies that thefunding has been committed, and is guaranteed to be made available (i.e. there is acommitment in writing). Once awarded, GAVI Fund commitments are consideredas secured funding. For the most part, secure funds are pledged over two to threeyears or less — except in the case of GAVI funds where it is five years, monies frompooled funds such as in a sector wide approach (SWAp), or debt relief funding forimmunization, such as the HIPC initiative.

cMYP Costing & Financing Tool – User Guide110
Total probable funding. Probable funding refers to all other funding that is notassured, but is likely to be made available in the short and medium term. The term“probable” indicates that the projected future funding is likely to be based on historicaltrends, or other information, following discussions with the relevant ministries anddonors.
Gap with secure funding. This refers to the difference between projected resourcerequirements and secure financing over the corresponding period. [gap with securefunding = resource requirements - secure funding]
Gap with probable funding. This refers to the difference between projected resourcerequirements and both secure and probable financing over the corresponding period.[gap with probable funding = resource requirements - (secure + probable funding)].
Financing Sources
Financing source. Financing source refers to the agents providing the fundsfor immunization. Given the difficulties in tracking the exact source of financing,countries are asked to report only the source of financing closest to the end user.Therefore, transfers of bilateral donor agency resources to multilateral agencies(such as WHO or UNICEF), or to a health fund or the national treasuries(through pooled funds or budget support), are not attributable to the donor countries.This is of particular (and growing) significance in countries receiving bilateral aidthrough the SWAp programmes and national budget support. In the Tool, only thelast source of funding before use in the programme is reported (i.e. if a bilateraldonor channels its funds for immunization through UNICEF, the funding is consideredas UNICEF funding. In other words, UNICEF is the end source).
• Government. This source of financing refers to domestic public funding forimmunization derived from taxation or other sources of public revenue at thecentral and/or sub-national level, and allocated through a formal budgetaryprocess. It can include the non-concessionary portion of a development loan,national budget support or debt relief proceeds.
• Bilateral agencies. This source of financing refers to external public funds forimmunization from official development assistance. Typically these are fundsderived from taxation in donor countries, and they constitute the grant fundingfrom bilateral international aid agencies (e.g. DFID, USAID, JICA, etc.).
• Foundation. This source of financing refers to external private funds forimmunization from foundations.
• Multilateral agencies. This source of financing refers to external public grantfunding for immunization which is channelled through multilateral internationalaid agencies such as UNICEF, or WHO, and the grant portion of developmentloans from international and regional development banks such as the WorldBank or Asian Development Bank.
• NGO. This source of financing refers to external private funds for immunizationfrom nongovernmental organizations (NGOs).
• Private Sector. This source of financing refers to domestic private funds forimmunization.

111WHO/IVB/06.15
Indicators
Percentage of government funding. This indicator refers to the ratio betweengovernment financed spending on immunization, and total spending on immunization,irrespective of the funding source, and gives the relative share of government fundingfor immunization compared with other sources of financing. The same indicator canbe calculated for specific cost categories, such as percentage government fundingfor vaccines. Note that this indicator is very sensitive to the inclusion or not ofshared costs.
Cost per capita. This indicator links total immunization cost or resource requirementsto total population in the country and provides a sense of affordability of theimmunization programme. It can be compared to the total per capita spending onhealth to give an indication of the relative importance of the immunization programmewithin overall health sector spending. If this indicator is going to be used to makecross-country comparisons, it is recommended that the total routine cost is used as anumerator.
Cost per DTP3 child. This indicator links total immunization cost of immunizationto the total number of children under one year of age who have received their thirddose of DTP vaccine. The number of DTP3 immunized children is calculated bymultiplying the total number of surviving infants by DTP3 coverage. Children underone year of age who receive DTP3 are considered to be fully immunized children(FIC). The cost per DTP3 child is used as an approximation of the value of resourcesrequired to fully immunize a child. If this indicator is going to be used to makecross-country comparisons, it is recommended that the total routine cost is used as anumerator.
Resource requirements, financing or gaps per DTP3 targeted child. The futureresource requirements, financing and gaps per targeted DTP3 child are the ratios ofthe total projected resource requirements, financing or gaps divided by the totalnumber of future children targeted to receive three doses of DTP. The number ofDTP3 targeted children is calculated by multiplying the projected number of survivinginfants by DTP3 coverage targets. This indicator is used to measure future resourcerequirements and gaps in a way that permits easier interpretation than by examiningabsolute values. If this indicator is going to be used to make cross-countrycomparisons, it is recommended that you use the total routine resource requirements,or cost, as a numerator.

cMYP Costing & Financing Tool – User Guide112

IDepartment of Immunization, Vaccines and BiologicalsFamily and Community Health
World Health Organization
CH-1211 Geneva 27
Switzerland
Fax: +41 22 791 4227
Email: [email protected]
or visit our web site at: http://www.who.int/vaccines-documents
The World Health Organization has managed cooperation with its Member States and provided technical support in the field of vaccine-preventable diseases since 1975. In 2003, the office carrying out this function was renamed the WHO Department of Immunization, Vaccines and Biologicals.
The Department’s goal is the achievement of a world in which all people at risk are protected against vaccine-preventable diseases. Work towards this goal can be visualized as occurring along a continuum. The range of activities spans from research, development and evaluation of vaccines to implementation and evaluation of immunization programmes in countries.
WHO facilitates and coordinates research and development on new vaccines and immunization-related technologies for viral, bacterial and parasitic diseases. Existing life-saving vaccines are further improved and new vaccines targeted at public health crises, such as HIV/AIDS and SARS, are discovered and tested (Initiative for Vaccine Research).
The quality and safety of vaccines and other biological medicines is ensured through the development and establishment of global norms and standards (Quality Assurance and Safety of Biologicals).
The evaluation of the impact of vaccine-preventable diseases informs decisions to introduce new vaccines. Optimal strategies and activities for reducing morbidity and mortality through the use of vaccines are implemented (Vaccine Assessment and Monitoring).
Efforts are directed towards reducing financial and technical barriers to the introduction of new and established vaccines and immunization-related technologies (Access to Technologies).
Under the guidance of its Member States, WHO, in conjunction with outside world experts, develops and promotes policies and strategies to maximize the use and delivery of vaccines of public health importance. Countries are supported so that they acquire the technical and managerial skills, competence and infrastructure needed to achieve disease control and/or elimination and eradication objectives (Expanded Programme on Immunization).





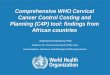




![Immunization Program Strategic Plan 2013 – 2017 · 1 2013-2017 Immunization Program [Immunization Program Strategic Plan 2013 – 2017] Maintaining and Improving Immunization Rates](https://img.pdfslide.net/doc/110x75/5e18e16c0228f448f3787c8f/immunization-program-strategic-plan-2013-a-2017-1-2013-2017-immunization-program.jpg)

















