Embed Size (px)
Citation preview

Australian Dental Journal, June, 1978 259
Volume 23, No. 3
Orthodontic Seminar: A Realistic Approach Construction, adjustment and repair of appliances::.
John F. Reading, B.D.S., F.D.S.R.C.S., D.0rth.R.C.S.
Senior Tutor (Part tinre), Orthodontic Department, The University of Sydney
ABSTRACT-Details of the design and construction of removable and simple fixed appliances are presented. Equipment, instruments, and supplies are listed. Welding, soldering, banding and bonding are illustrated. Finally, step-by-step descriptions are given of first aid measures for the repair of fixed appliances applicable to the general practice situation.
(Received f o r publication February, 1978)
Construction, adjustment and repair of appliances
Basic equipment Every dental practice can find room for an
orthodontic section, be it ever so humble. It will not only enable orthodontic treatment to be per- formed, but its equipment will enlarge the scope of other daily tasks. Essential to this object are a spot welder, soldering kit, micro-motor, vacuum plaster mixer and vibrator, model trimmer, pliers, and a camera. Supplies would include preformed bands and attachments, bonding materials, wires, springs, plastic modules, elastics, preformed arch wires, preventive materials and general dental supplies, such as cement, plaster, and acrylic.
Removable appliance construction Clasps
Removable appliances require adequate reten- tion. The Adams clasp (Fig. la), and its modifica- tions, in my opinion is still the most versatile clasp for orthodontic purposes. The principles of its design and construction are well described in Adam’s bookl, and should be followed. Failure to observe these principles can lead to failure of the clasp in use. Also helpful are the circumferential clasp, often making use of the gingival undercut on upper first deciduous molars, the helical clasp fitting gingivally to tubes on molar bands (Fig. l b ) , and the ball clasp (Fig. Ic, d ) which differs from the Adams single tooth application in that it fits
Presented at the Australian Dental Association Jubilee Congress. Melbourne, February, 1978.
1 Adams, C. P.-The design and construction of removable orthodontic appliances. Bristol, John Wright and Sons Ltd.. 4th ed., 1970.

260 Australian Dental Journal, June, 1978
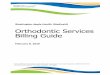
Fig. 1 . 4 a s p s and springs. a, Adams clasps, premolar and molars. b, Clasps over molar tubes palatal helical s rings and guide wire. c, Clasps to fit over molar tubes and boxed-in spring to procine central incisors and free-standing labial springs to retrocline lateral incisors. A bite platform is formed in the palatal acrylic. d, Ball clasps on
deciduous molars: Adams clasps on permanent molars.
into the undercuts of two adjacent teeth. Labial bows
Labial bows can be adapted for various stages of eruption of the mixed dentition but all need an adjusting mechanism to allow for tightening or loosening the labial wire (Fig. 2a). Spoon bite plates used in conjunction with extra-oral traction appliances work well with a simple rigid non- adjustable bow around the four incisors (Fig. 2b). Springs
Active springs must have sufficient strength to resist distortion. A combined spring and guide wire unit has advantages over the “boxed-in” spring (Fig. lb). Screws
Expansion screws for lateral and antero- posterior movement are essential and are easier to place and adjust than Coffin’s W arch. Plier design
While many components of removable appliance construction can now be purchased in a preformed condition, all can be fabricated without difficulty by any experienced dentist or dental technician. The Adams universal plier is specially designed for Adams clasp construction and its dimensions should be as illustrated in the text book. In con- ceiving the plier design, Adams specified longer
and broader handles to fit the palm of most hands. The spring forming pliers have the same handle design. Add to this a three-beaked (Aderer) plier, a broad flat beak plier and a pair of wire cutters and the kit is complete. Plastic base
Most orthodontic removable appliances are today cold cured and processed in the hydroflask and cleaned up and polished conventionally on the lathe.
The vacuum thermoplastic Biostar machine can eliminate many of the above steps, but its cost makes group or laboratory ownership more realistic than for a solo operator. Adjustments
Two or three pliers are sufficient to adjust and activate most removable appliances. The round beak of a spring bending plier can be placed in the helix, provided an open-construction has been used, to effect controlled activation of the spring (Fig. 3a).
Adams clasps are tightened by bending the arrowheads gingivally from the bend on the occlusal surface (Fig. 3b). An incorrectly made clasp often cannot be activated and the appliance may need reconstruction.
The arrowheads should be correctly positioned

Australian Dental Journal, June, 1978 26 1
Fig. 2.- Labial bow and adjustments. a, Labial bow with loop to allow attachment of 3 in latex band. b, Spoon bite plate with fixed, non-adjustable labial bow to be used in conjunction with extra oral traction.
in single undercuts, the length of the arrowheads should be minimal, the bridge joining the arrow- heads should stand clear of the buccal surfaces, the arrowheads should be parallel as they pass inter- proximally. The dentist should be able to bend such an ideal clasp so he can return inadequate ones to the laboratory technician for reconstruc- tion. Preformed clasps are available but do not entirely reproduce the classic modified arrowhead clasp of Adams. Modification of Springs
Careful design of open construction springs and guide wires permits modification as tooth move- ment proceeds. A labial bow can have helices for latex traction, the palatal acrylic being trimmed by two garnet discs on a mandrel. Springs with guide wires can be used to recover space in the dental arches. Guide wires can be converted into active springs (Fig. Ib). “Worked-out” helical springs can be cut off the appliance but a retained helix can act as a h,ook for individual latex traction. Impacted molars can be moved distally with helical springs.
It is possible to solder wire to Adams clasps to provide additional springs or to act as a substitute
Fig. 3.-Pliers and adjustments. a S ring bending pliers inserted into helix of spridg for controlled activation. b, Adam clasps tightened by bending
gingivally with universal pliers.
for a broken spring. In a similar way a labial bow can be soldered to both Adams clasps on the molars.
Free standing labial canine retracting springs (often reinforced in tubing for rigidity) can be adjusted to move canines (and premolars) lingually as well as distally. They can also be modified to accept a latex band to retract the incisors.
Expansion screws should be wound out and back again by operator and patient before the ap- pliance is inserted to loosen up the screw and to give the patient confidence in turning the screw (Fig. 4). An arrow should be incorporated in the plastic to remind the patient of the direction of turning. A thread, chain or piece of floss should be attached to the key to minimize its misplacement or loss.
Time should be spent with the patient learning the routine and practising the insertion and removal of the appliance. Written instructions in the form of a personalized letter reinforce the message. A plastic container duly labelled with the patient’s name and address should be supplied. The patient should then demonstrate his dexterity and know- ledge in his parent’s presence.

262 Australian Dental Journal, June. 1978
Fig. 4.-New appliance insertion. Patient practises activation of expansion screw.
Fixed Appliances Separation
Fixed appliances require separation. Plastic modules make this task easier but the rings must be carefully placed, and accounted for at the next
Fig. 5.-Separation with plastic modules. a, Mosquito- beaked Mathieu pliers; plastic rings threaded on dental
comfortable teeth at the next visit. Hoss. b, Ring is stretched between pliers and floss and inserted between teeth.
(Fig' 5) . * seven-day period provides for
Selection, fitting and adjustment of preformed bands
Band selection from preformed supplies is not difficult but time must be spent in adapting the stock size band to the individual tooth shape. Band removing pliers, contouring pliers and a mechanical band pusher are helpful, as is some judicious grind- ing of the band with a wheel stone in certain cases.
Securing bands in impressions Molar bands should be secured in impressions
with long pins to avoid loosening them by vibrating plaster when casting the impressions.
Lingual arches Lingual arches should always have lugs or tubes
welded to the molar bands on the buccal surfaces to locate the bands in the impression and to facilitate removal.
Lingual arches can be used for space main- tenance, to regain space, e.g. Bazooka or Friel spring (Fig. 6a), and to elevate molars and similar tasks. They act as retainers after active ortho- dontic treatment (Fig. 6b).
Palatal arches Palatal arches can be used as a framework to
supply traction to surgically exposed teeth (Fig. 7% b, c), to expand or contract arches, to advance
Fig. 6.--Lingual arches, a, Frie, spring attached to labial segments in Class 111 ~ a ~ O ~ C ~ U s i O n s and to lingual arch to procline anterior teeth. b, Fixed
retainer soldered to canine bands, commonly used act as a reminder for anti-digit sucking. following fixed appliance therapy.

Australian Dental Journal, June, 1978 263
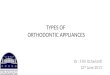
Fig. 7.-Palatal arches. a, Palatal arch and auxiliary spring to bring down canine. Attachment ligature placed through hole drilled in distolingual surface. This tooth moved very quickly and ligature ends irritated the cheek when patient was on holiday. Local dentist rendered first aid by adding cold cure acrylic blob. b, Palatal arch used as a framework for Friel spring used to procline upper anterior teeth. c, Double back auxiliary arch fits into flat oval tube on molar band. Compressed helices provide
traction to surgically exposed canine.
Fig. g.-Rapid maxillary expansion. a, Appliance in position before expansion. b, Appliance twenty-one days later with ligature wire to prevent unwinding, occlusal view.
c, Same as b. Front view showing expansion and advancement of labial segment.
Rapid maxillary expansion theory of adjustment should be understoodz. Labial bands and arch wires
usually necessitates an experienced orthodontic Labial bands (preformed) and arch wires (pre- background (Fig. 8). formed) are available and make tooth alignment Exha-oral traction
?Thurow R. C.-Atlas of orthodontic principles St. Louis,
The use of a rapid maxillary expansion appliance
~ ~ ~ ~ ~ - ~ ~ ~ l traction i s easy to supply but the The 'c. V. Mosby Company, 1970 (pp. 204-220).

264 Australian Dental Journal, June, 1978
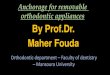
Fig. 9.-First aid to fixed appliances. a, Bracket bonded to canine using acid-etch technique. b, Uprighting spring in Malhieu pliers being placed in lightwire bracket. c, Fine-nosed snipe plier used to tuck ligature under arch wire. d, First aid required. Safety spring dislodged and held only by ligature. This should be carefully removed by cutting ligature wire, and patient returned to orthodontist as soon as possible. e, Coiled spring has opened space for canine which has been exposed and ligated. Gold chain provides attachment for orthodontic traction from safety spring fitted around molar tube.
easier for the dentist and patient (Fig. 9). Provided diagnosis and treatment planning is adequate there is no reason why the general practitioner with ex- perience and interest and time cannot treat many minor malocclusions in this way. Direct boadhg
Polycarboxylate cement will secure standard attachments to teeth which are difficult to band. Acid-etch direct bonding materials, plastic brackets or mesh-backed metal brackets, are now available. While plastic brackets so far seem unsatisfactory for a conventional treatment period of eighteen months, the mesh backed metal brackets offer help to misplaced, partially erupted and anatomically awkward teeth. The day of bonded, rather than banded, teeth may be round the corner but at present the conventional orthodontic stainless steel band appears the safest and most reliable attach- ment for tooth movement.
h a m e l protection Preventive measures such as pretreatment pro-
phylaxis and topical fluoride application are the general practitioner’s prerogative, but last minute reinforcement prior to band placement is beneficial.
First aid for orthodontic appliances in general practice
Many difficulties arise during fixed appliance treatment and, while the specialist orthodontist is generally available to deal with these, the patient may have to turn to his family dentist, who is after all responsible for the total dental care of his patient, for assistance. Loose molar band
In order to cement a loose molar band without taking out the entire arch wire it is necessary to remove the attachment of the second premolar to

Australian Dental Journal, June, 1978
the arch wire to provide flexibility. The end of the arch wire should then be straightened, if necessary, with Howes pliers and the band removed with band removing pliers. Wire brushes should be used to clean the band inside and out after it has been rinsed under the tap, and the hard cement chipped out with a scaler. The band is recontoured, refitted to the tooth to assess retention, and tightened if necessary. With the tooth cleaned, fluoridated, dried and isolated, the band, filled with freshly mixed cement, is inverted over the end of the arch wire and rotated into place and seated with a molar band pusher. After the excess cement has been removed the premolar band is repinned or retied and the end of the arch wire adjusted. Broken arch wire
If an arch wire is broken, say at the canine band, the arch wire should be removed and replaced, if possible, with a preformed arch or custom made wire. A broken arch wire should not be left in place as the arch could be considerably distorted. Of course, the patient should be instructed to dis- continue intermaxillary elastics. Displaced arch wire
I€ an arch wire has come out of the molar tube and cannot be replaced without removing and replacing the arch wire, it can be secured to the molar tube with a double ligature until the patient can visit his orthodontist. Dislodge uprighting spring
These springs can be dislodged accidentally by the patient and are conveniently replaced by securing the open hook in a Mathieu plier, slipping the tail into the bracket, after which the hook is engaged on the arch wire and the plier released (Fig. 9b). Remember, the hook points in direction that the tooth is to move. Repairing a band
A split or loose band should be replaced with a new band. If one is not available, the band can be cleaned and repaired by welding a section of band tape inside the split. Broken face bow
A broken face bow is best discarded and a new one fitted. The old one however would be useful as a template to adapt a preformed face bow to the patient’s requirements. Broken retainer
A broken retainer should be repaired and re- placed. The urgency of this would depend on the newness of the retainer. Lost retainer
If a retainer has been lost, the patient should be
265
returned to his orthodontist. If this is not possible, an impression should be taken and the model sent to the orthodontist to design the retainer. Arch wire adjustmemts
Arch wire adjustments frequently required are: shortening the wire with cut and hold pliers, turning in protruding ends of arch wires with Howes pliers, turning in ligature wires with fine- beaked snipe pliers (Fig. Sc), and also adjusting traction loops that make elastic placement difficult These are all tasks that the family dentist can do to help his patient. Multi-looped arch wires are best left alone as their adjustment in the mouth can lead to distortion forces on the wrong tooth. Lingual arch repair
A lingual arch with ‘U’ loops can be repaired by free-hand soldering. A wax template is made and the U loop is straightened and adapted to the molar band seated on the wax sheet. The band is heated till the solder melts when the broken wire is flicked off. The band and wire are cleaned and the soldered surfaces are freshened with a carborundum stone. Both surfaces are fluxed. Solder is then applied to the lingual arch which is then advanced onto the band, already in the flame, and held momentarily as union takes place. The joined arch is held carefully together and removed from the flame, quenched and polished. It is then adapted, if necessary, to the wax template, tried in the mouth and then cemented. Replacing ligature wire
Red bite wax, given to the patient, can be used as a first aid measure. Ligature wire (0.3 mm soft) is placed with a Mathieu plier and cut with a pin and ligature cutter. The tag is pushed in with a finger and then curled under the arch wire with a pair fine snipe-nosed pliers (Fig. 9c). Surgically exposed teeth
These teeth may have been ligated during surgery and have a gold chain attached for traction. It is important to continue the gentle guidance and the ligature to the chain should be replaced immediately if it breaks (Fig. 9d, e).
Conclusion The general practitioner whose practice includes
children should be prepared to assist in any or all of the above procedures when circumstances pre- vent the patient being returned immediately to the orthodontist.
Park House, 187 Macquarie Street,
Sydney, N.S.W., 2000.