Embed Size (px)
Citation preview


Orthopedic RadiographyThe Hard Facts
Dr. LeeAnn Pack
Diplomate ACVR

Musculoskeletal Radiography
Permit localization and characterization of a lesion
Size, shape, margination, number, position, opacity
Normal radiographic anatomy Diseases are often bilateral in the
appendicular skeleton Radiographic terms – use appropriately

Approach to Interpretation Soft tissues
– Intra-capsular or extra-capsular
Bones– Evaluate periosteal margins for new bone– Evaluate all cortices and subchondral bone– Evaluate the medullary cavity for changes in
opacity
Joints– Evaluate joint capsule attachments– Evaluate joint spaces and peri-articular margins

Bone Loss
Generalized bone loss– Metabolic or Nutritional disease, disuse
Called osteopenia Radiographic findings:
– Decreased bone opacity, cortical thinning, coarse trabeculation, bone deformity or pathological fractures may occur
– Loss of lamina dura – 2ary HPTism

Generalized Bone Loss

Bone Loss
Localized bone loss– Trauma, infection, tumor
Easier to detect than generalized

Bone Loss
Determining Aggressiveness– Zone of transition– The less distinct the
margin the more aggressive the lesion

Bone Loss
If the cortex is destroyed, the process is more aggressive than if the cortex is allowed to remodel
Intact Destroyed

Focal Bone Loss
Geographic Lysis– Large area of lysis– Usually less
aggressive– If destroys the cortex
aggressive

Focal Bone Loss
Geographic lysis– Expansile
appearance– Expansion of the
cortex around an enlarging mass less aggressive
– Note the intact cortex in the picture

Bone Cyst

Focal Bone Loss
Moth Eaten lysis– Multiple smaller
areas of lysis– Areas may become
confluent– More aggressive
than geographic lysis

Focal Bone Loss
Permeative Lysis– Numerous small and
pin point areas of lysis whose margins are indistinct and fade gradually into normal bone

Permeative Lysis

Spiculated Periosteal Reaction

Amorphous Periosteal Reaction

Differentials
Based on aggressiveness of lesion Location/s Mono/ poly-ostotic / joint centered Must assess signalment and history,
location, additional tests… Many diseases have similar
radiographic appearance – may require biopsy

Primary Bone Tumors
Radiographic Signs:– Lesion may be primarily productive, lytic or
both– Lytic or productive lesions usually have an
aggressive appearance– Away from the elbow and toward the knee

Primary Bone Tumors
Radiographic Signs:– Typically mono-ostotic– Typically located in the
metaphysis– Lesions typically do not
cross joints

Primary Bone Tumor

Primary Bone Tumor

OSA – note the ST enlargement

Fungal Osteomyelitis
Radiographic Signs:– Typically lesions are seen in the
metaphysis– Appear similar to primary bone tumor– Often extensive destruction when a joint is
infected (septic arthritis)– Often is poly-ostotic

Fungal Osteomyelitis Etiological Agents: Blastomyces dermatitidis
– Southern states, mid-west and south-west
Coccidioides immitis– Western states
Histoplasma capsulatum– mid-western states
Cryptococcus neoformans & Aspergillosis– Throughout the US

Fungal Osteomyelitis

Fungal

Fungal Septic Arthritis

Differential Diagnosis Single aggressive lesion of long bones
– Primary bone tumor– Fungal osteomyelitis– Metastatic bone tumors
Carcinomas
Use signalment, geographic location, and clinical findings to prioritize the differential list– May require a biopsy with culture

Synovial Cell Sarcoma
Early in the disease there is intra-capsular and/or peri articular swelling
Swelling then turns to a mass effect Later there is bone lysis of multiple
bones of the joint

Synovial Cell Sarcoma

Synovial Cell Sarcoma

Hypertrophic Osteopathy
Palisading periosteal response– Usually solid
Occurs secondary to a mass somewhere– Thoracic– GU tract– Fungal disease– Heartworm disease

HO
Begins on the abaxial digit and progresses proximal and axially

HO

HO
Radiographs of the chest and abdomen should be made
And abdominal US can be preformed if needed

Cruciate Ligament Rupture
Cranial displacement of the infra-patellar fat pad
Caudal displacement of the fascial stripe

Cruciate Ligament Rupture
DJD– Base and apex of the
patella– Proximal aspect of
the trochlear ridge– Medial and lateral
aspects of the distal femur and proximal tibia
– Fabellae

DJD Stifle Peri-articular osteophytes

DJD – Joint Mice
Joint mice are pieces of articular cartilage that have become detached and are in the joint – they mineralize when they have a blood supply – must R/O avulsion fragment

Intra-capsular ST Swelling
Normal IC Swelling

Cruciate Rupture

Patellar Luxation

Patellar Luxation

Patellar Luxation

Developmental MS Diseases
OCD– Shoulder– Elbow– Stifle– tarsus
Fragmented Medial Coronoid Process
Ununited Anconeal Process
Panosteitis Hypertrophic
Osteodystrophy Hip Dysplasia Legg-Calve-Perthes

Osteochondrosis
Dysfunction of endochondral ossification (bone that forms from cartilage)
Disturbance leads to increased thickness of the cartilage
Cartilage is radiolucent compared to bone therefore, radiographically we see a radiolucent subchondral defect

Osteochondrosis
Subchondral defect – flattening Surrounding sclerosis as time
progresses Joint mice Secondary DJD Locations: shoulder, elbow, stifle, tarsus

Shoulder OCD
Subchondral defect on the caudal aspect of the humeral head
May see a joint mouse May just be flattened Secondary DJD May need arthrogram or explore

Shoulder OCD

Shoulder OCD – note flattening


Elbow OCD Subchondral defect present on the
distal medial aspect of the humerus (humeral condyle)
Surrounding sclerosis

Elbow OCD – CC and Obl

Tarsus OCD
Rotts! Medial trochlear ridge of the talus Often seen small mouse Joint effusion DJD See best on oblique view or flexed
lateral


Tarsal OCD MTR

Fragmented Medial Coronoid Process
On the lateral view– Blunted appearance
to the medial coronoid process

FCP
On the CC view– New bone production
on the medial coronoid process
– Look like has been hit with hammer

FCP A = blunted medial coronoid process B = osteophyte on anconeal process C = osteophyte on medial coronoid process

Ununited Anconeal Process
Forms from a separate center of ossification Should fuse in all dogs by 6 months Lucent line – best seen on flexed lateral

Ununited Anconeal Process
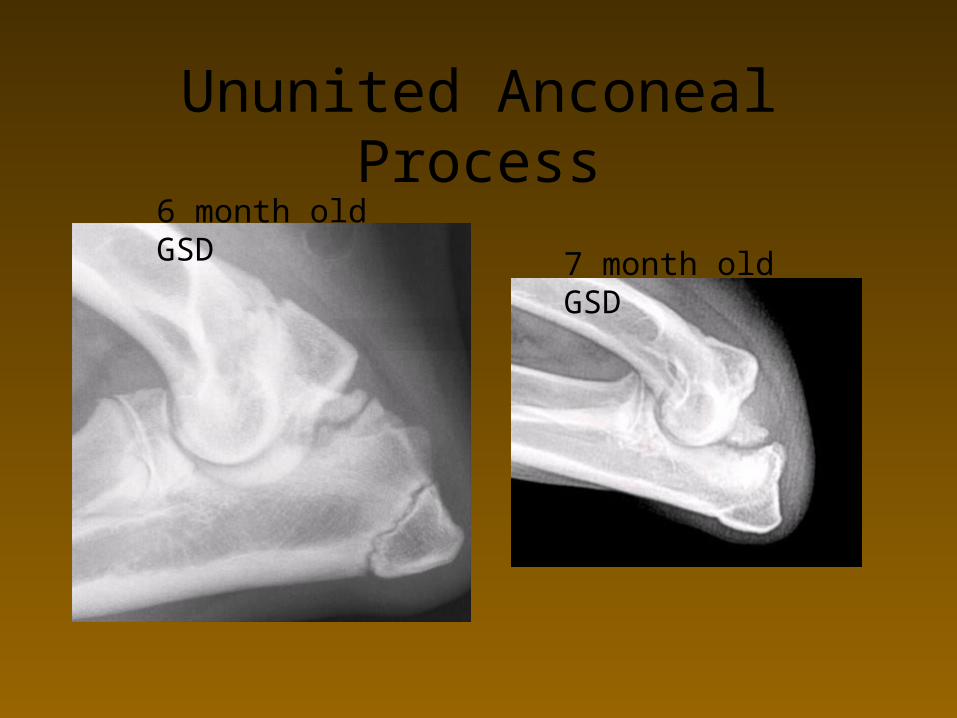
Ununited Anconeal Process6 month old GSD
7 month old GSD

UAP

Elbow Dysplasia
1. Ununited anconeal process
2. Osteochondrosis of medial aspect of distal humeral condyle
3. Fragmented medial coronoid process
4. Premature closure of radius/ulna physis causing incongruency of elbow joint

Elbow DJD
Note the large osteophyte on the anconeal process – this is often times one of the earliest changes seen with DJD in the elbow

Panosteitis
Late– Medullary opacities
become patchy– Opacities appear to
coalesce– Solid periosteal reaction
may be seen on adjacent cortex

Panosteitis Multiple leg involvement is likely Shifting leg lameness

Panosteitis


Hypertrophic Osteodystrophy
Early– A thin band of
radiolucency in the metaphyseal portion of the bone
– Double physis– Cheeseburger sign– Sclerosis seen
adjacent to lucency

HOD

HOD

HOD

Hip Dysplasia
Clinical Features– The laxity of the coxofemoral joint leads to
improper development and degenerative change
– Clinical signs range from mild to severe– Usually bilateral but can be unilateral

Extended VD View
Used for OFA Legs pulled down
and rotated inward Must include the
entire pelvis and stifles

Positioning Effect of Rotation

Normal Anatomy - Coverage
There should be at least 50% coverage of the femoral head by the dorsal acetabular rim

HD with Severe Subluxation

Normal Anatomy
The femoral neck should be more narrow than the femoral head
The femoral neck should have a smooth margin

Hip Dysplasia
The acetabulum is shallow and flattened.

Bilateral Hip Dysplasia

Hip Dysplasia
Periarticular osteophytes will form along the acetabular rim and dorsal edge
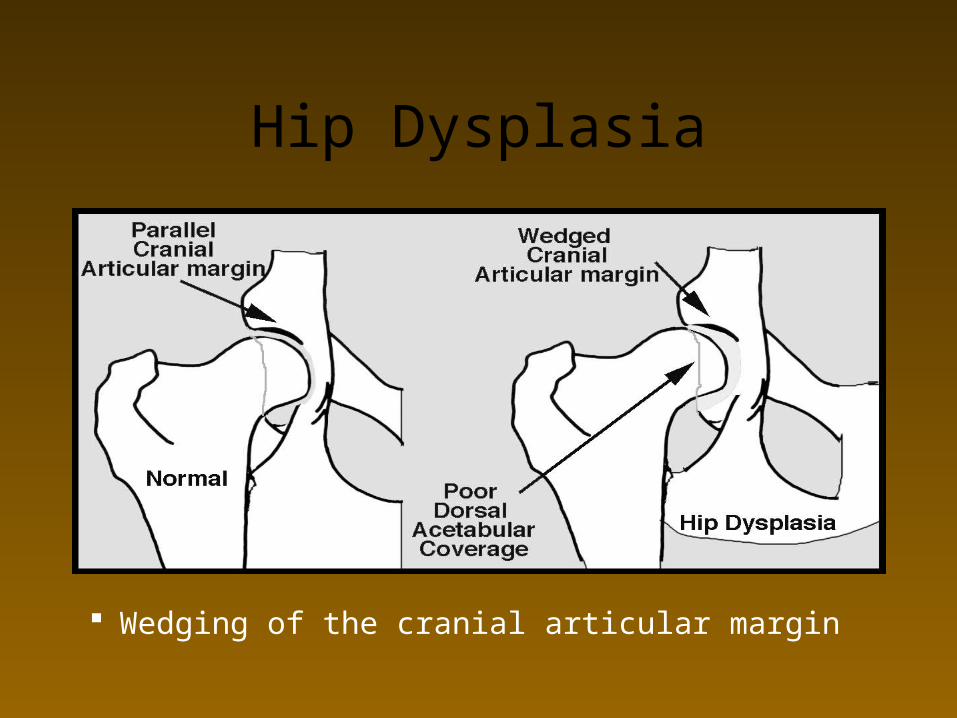
Hip Dysplasia
Wedging of the cranial articular margin

Morgan Line
Enthesiophyte formation on the distal aspect of the femoral neck
Secondary to coxofemoral joint laxity
Early sign of DJD

Does This Dog Have Hip Dysplasia?

Legg-Calve-Perthes
Associated with decreased or lack of blood supply to the femoral capital epiphysis
The normal blood supply comes from:– Synovial membrane– Arteries in the round ligament of the head
of the femur– Nutrient vessels through the metaphysis

Legg-Calve-Perthes
Patchy areas of lysis in the femoral head Invasion of vascular granulation tissue
replacing dead bone

Legg-Calve-Perthes
Deformity of the femoral head Flattening of the femoral head

Legg-Calve Perthes

Shoulder – What Do You See?