Embed Size (px)
Citation preview
ABSTRACT ID: IRIA - 1176
OSLER RENDU WEBER SYNDROME
AIMTo diagnose a rare case of OSLER
RENDU WEBER SYNDROME
Screening methods for first degree relatives of patients for early diagnosis and prevention of complications
METHODOLOGY
Patient was investigated using conventional 4 slice helical ct and 64 slice ct angiography
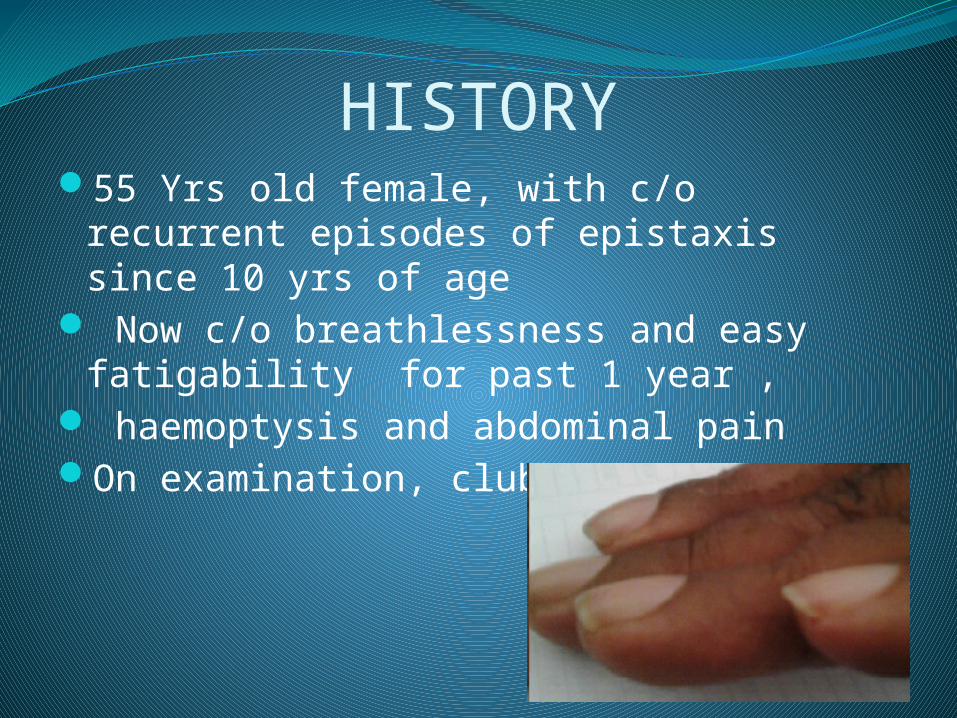
HISTORY55 Yrs old female, with c/o recurrent
episodes of epistaxis since 10 yrs of age Now c/o breathlessness and easy
fatigability for past 1 year , haemoptysis and abdominal painOn examination, clubbing present
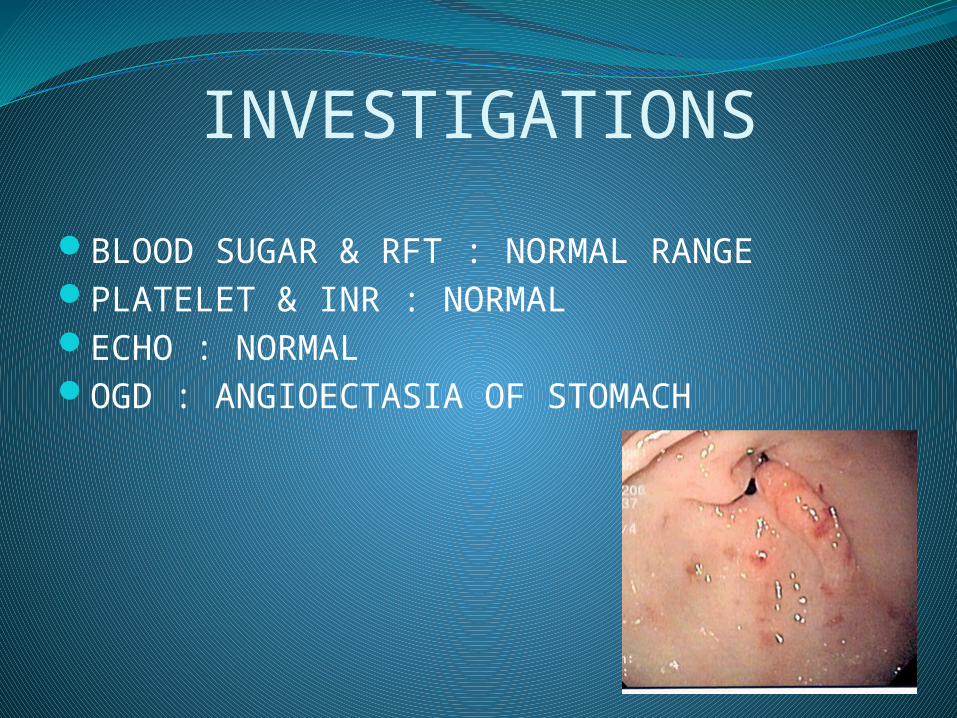
INVESTIGATIONS
BLOOD SUGAR & RFT : NORMAL RANGEPLATELET & INR : NORMALECHO : NORMALOGD : ANGIOECTASIA OF STOMACH
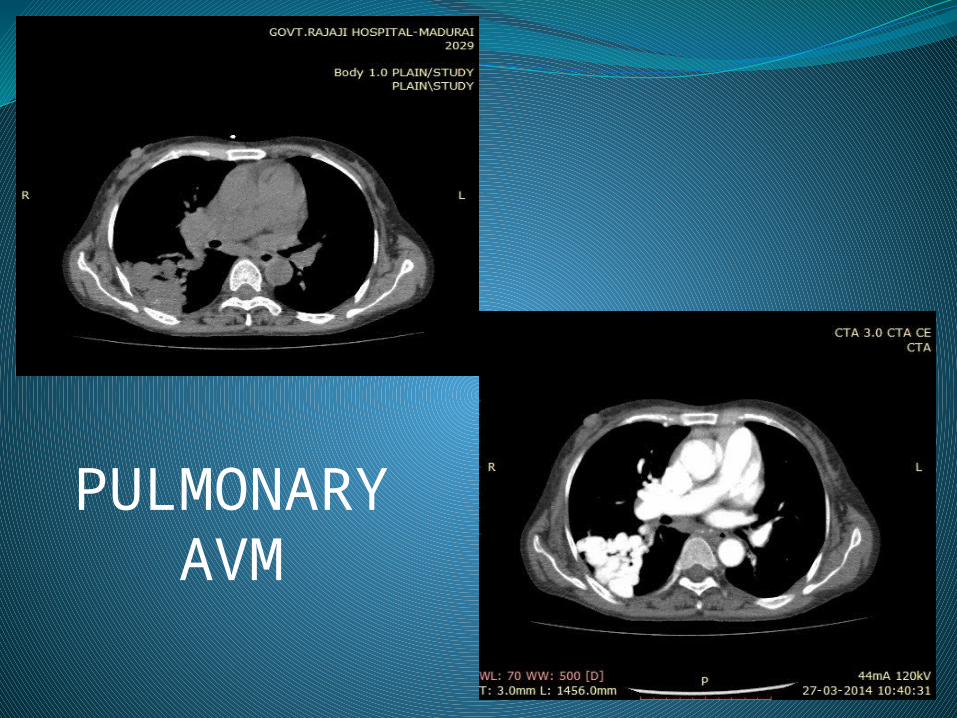
PULMONARY AVM
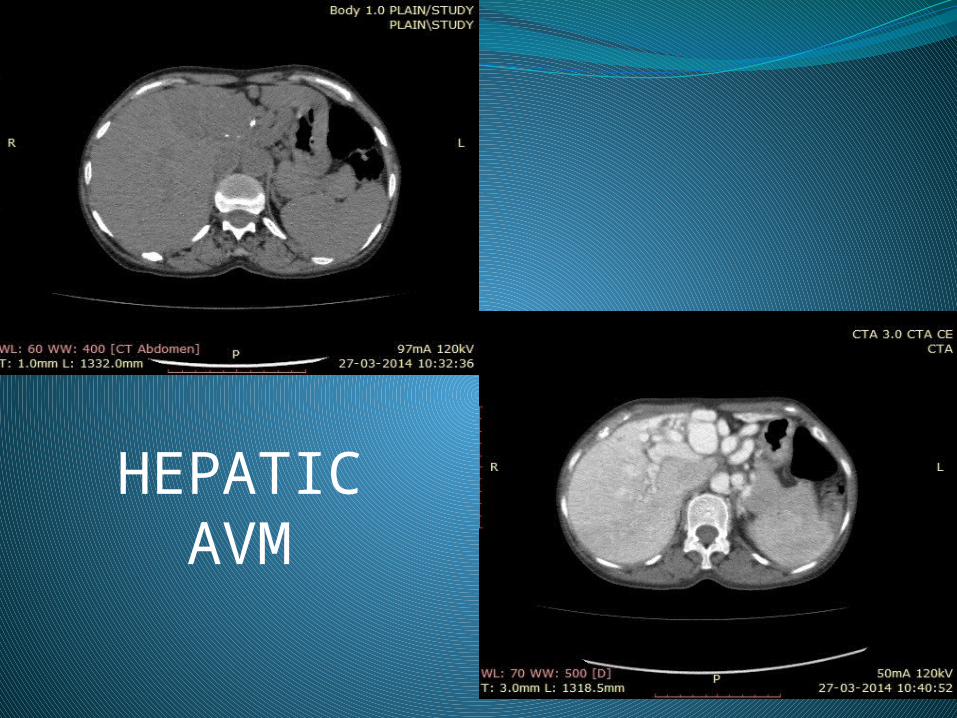
HEPATIC AVM
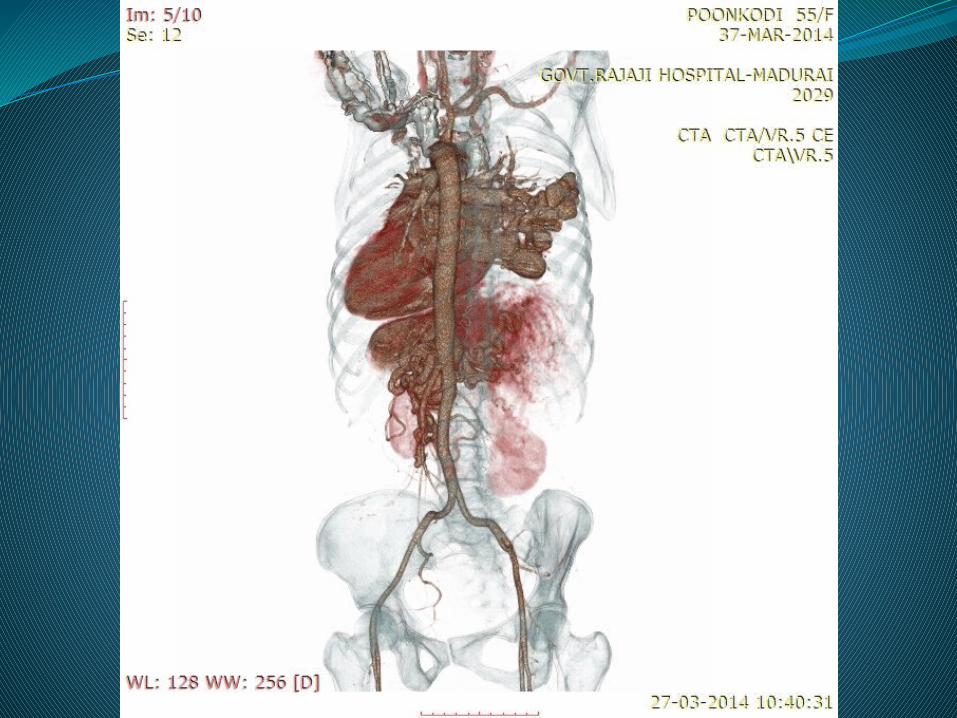
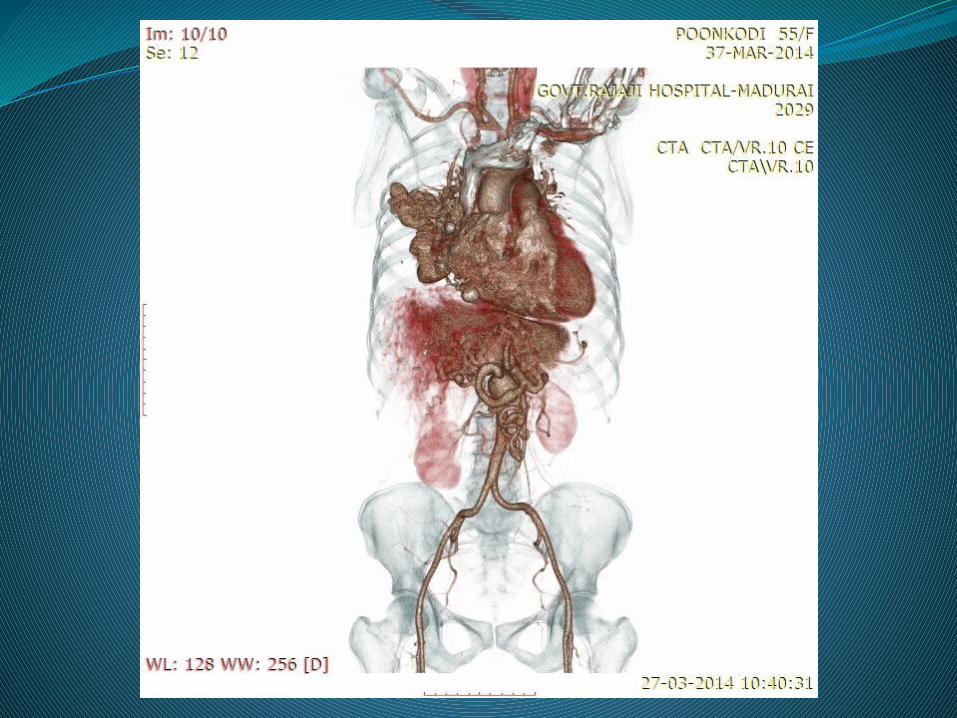
IMAGING FINDINGSCT PULMONARY ANGIOGRAPHY showed AV malformation in right lower lobe
of lung with right pumonary artery as feeding vessel and draining into the left inferior pulmonary veins
• CT ABDOMEN Intrahepatic AVM in left lobe of liver &
dilated hepatic artery
Osler-Weber-Rendu disease (OWRD) is a rare autosomal dominant disorder
It affects blood vessels throughout the body (causing vascular dysplasia) and results in a tendency for bleeding.
The condition is also known as hereditary hemorrhagic telangiectasia
Symptom onset may be delayed until the fourth decade of life (~90% of patients manifest by age 40 years) or later
CURACAO DIAGNOSTIC CRITERIAEPISTAXIS -spontaneous,recurrent
TELANGIECTASES - multiple sites lips,oralcavity,nose,fingers
VASCULAR MALFORMATIONS pulmonary,hepatic,git,cerebral,spinal
FAMILY HISTORY - first degree relative with Hereditory haemorrhagic telangiectasia
Definite diagnosis; 3 criteria present
Possible diagnosis; 2 criteria present
Unlikely ;less than 2 criteria present
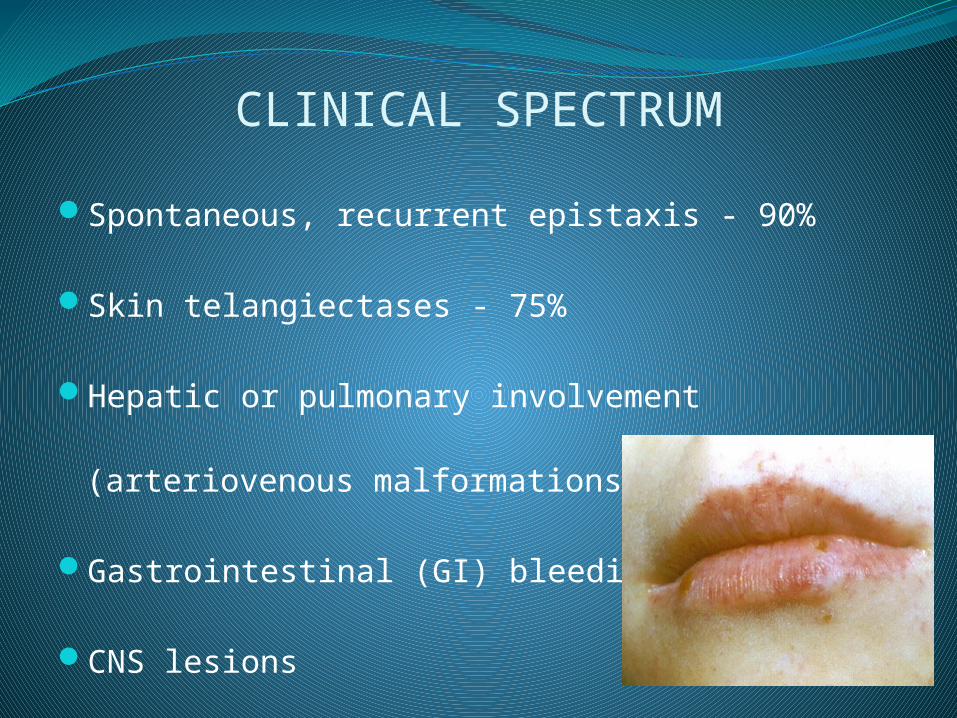
CLINICAL SPECTRUM
Spontaneous, recurrent epistaxis - 90%
Skin telangiectases - 75%
Hepatic or pulmonary involvement (arteriovenous
malformations [AVMs]) - 30%
Gastrointestinal (GI) bleeding - 15%
CNS lesions
DIFFERENTIAL DIAGNOSISAtaxia-Telangiectasia
CREST Syndrome
Dermatologic Manifestations of
Dermatomyositis
Pediatric Syphilis
Rosacea
COMPLICATIONSBrain abscess
Hemorrhagic or ischemic stroke
High-output congestive heart failure
Chronic GI bleeding and anemia
Portal hypertension with esophageal varices
Pulmonary hemorrhage
Liver cirrhosis
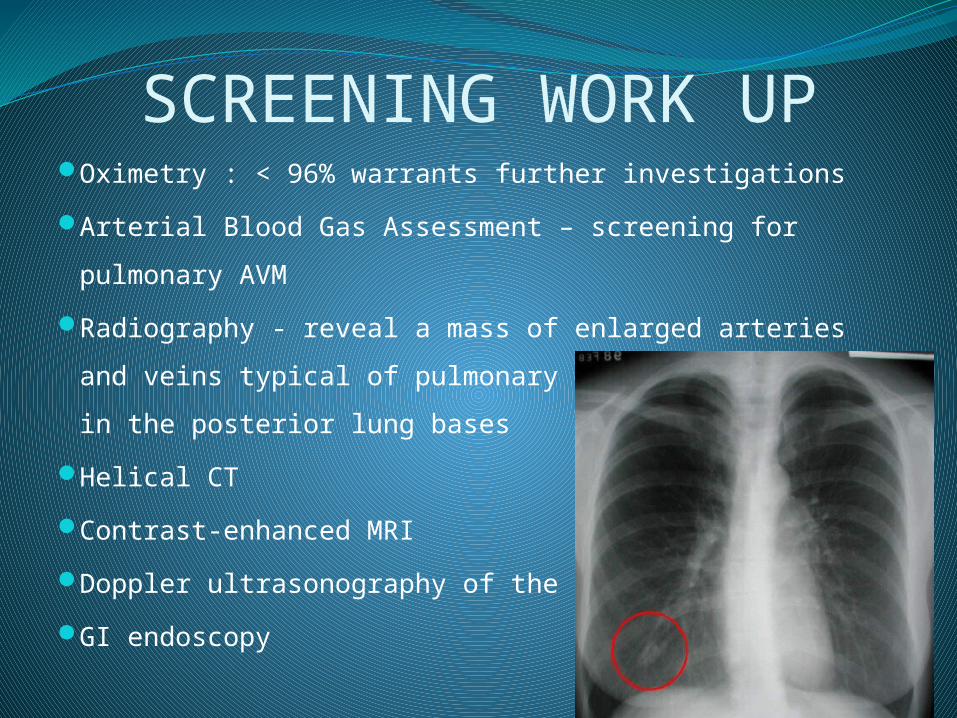
SCREENING WORK UPOximetry : < 96% warrants further investigations
Arterial Blood Gas Assessment – screening for pulmonary
AVM
Radiography - reveal a mass of enlarged arteries and
veins typical of pulmonary AVM. Commonly found in the
posterior lung bases
Helical CT
Contrast-enhanced MRI
Doppler ultrasonography of the liver
GI endoscopy
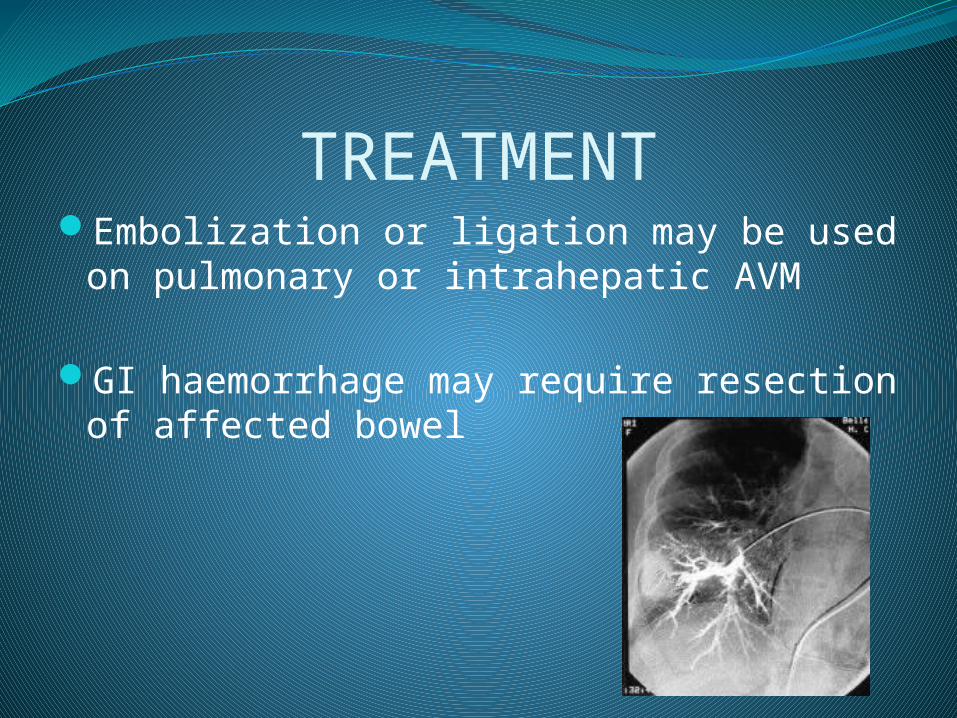
TREATMENTEmbolization or ligation may be used on
pulmonary or intrahepatic AVM
GI haemorrhage may require resection of affected bowel
CONCLUSIONWe are now acquainted with the presentation
and diagnosis of Osler Rendu Weber Syndrome
The presentation is usually in the 4th decade or so.
Hence, Screening of first degree relatives is important as it helps in early detection of disease and helps prevent complications
REFERENCESShovlin CL, Guttmacher AE, Buscarini E, et al.
Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Am J Med Genet. Mar 6 2000;91(1):66-7. [Medline]
Shovlin CL, Letarte M. Hereditary haemorrhagic telangiectasia and pulmonary arteriovenous malformations: issues in clinical management and review of pathogenic mechanisms. Thorax. Aug 1999;54(8):714-29.[Medline].
Nanda S, Bhatt SP. Hereditary hemorrhagic telangiectasia: epistaxis and hemoptysis. CMAJ. Apr 14 2009;180(8):838. [Medline].