Embed Size (px)
Citation preview
OSPEDALEPER INTENSITÀ DI CURA:QUALE IMPATTO SULLA QUALITÀDELLA RISPOSTA AL BISOGNO DIRICOVERI IN URGENZA
Gaddo FLEGO – Direttore SanitarioPrimiano IANNONE – Direttore S.C. Pronto SoccorsoASL 4 “Chiavarese”RETE LIGURE HTA
Qualità della risposta dell’ospedaleal bisogno di ricoveri urgenti
da Pronto Soccorso
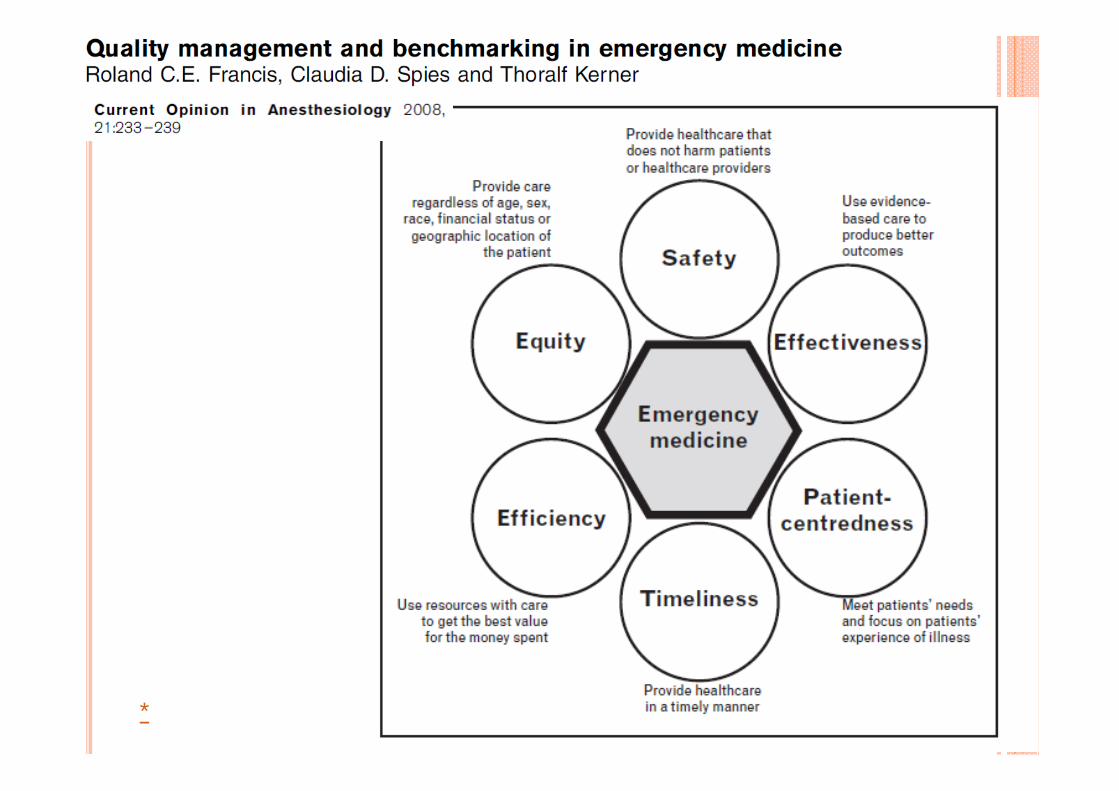
Un concetto necessariamente multidimensionale
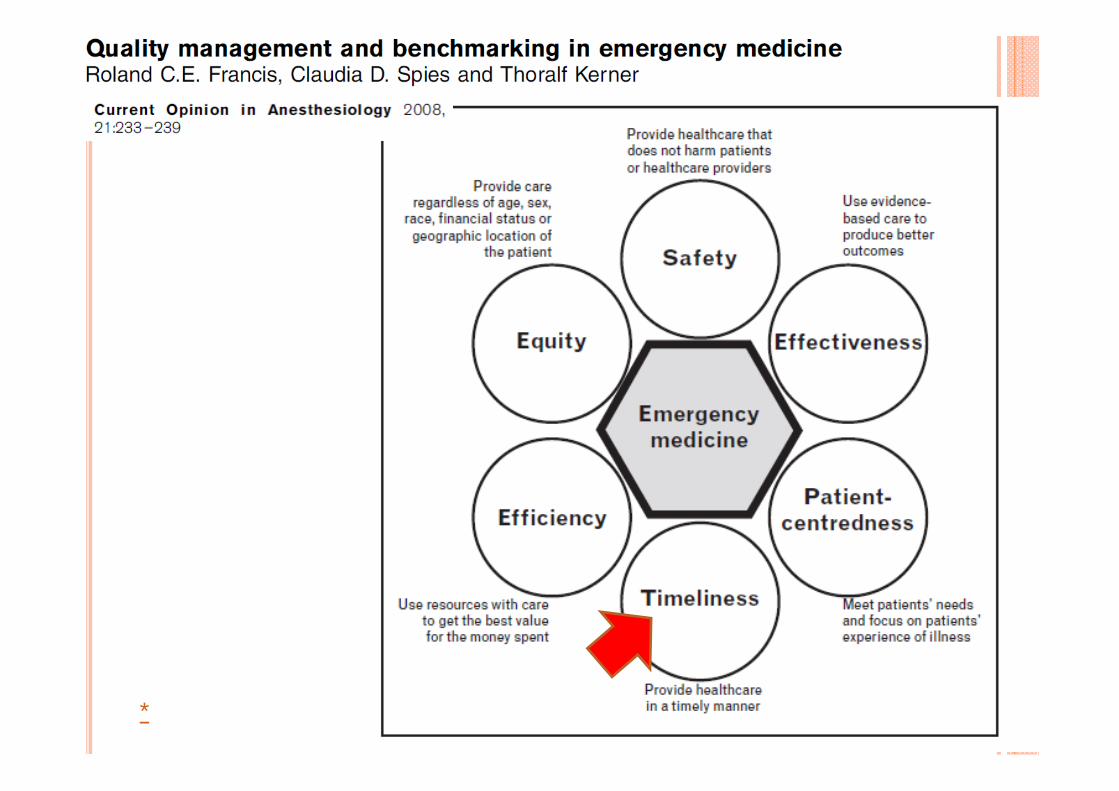
*

RITARDO NEI RICOVERI DA PS(CASO LIMITE: ACCESS BLOCK)
Allungamento durata della degenzaEccesso di mortalità
• overcrowding• Disagi all’utenza e stress per gli
operatori• Aumentato rischio clinico• Ritardi diagnostici e
terapeutici• «Boarding»• Diversione ambulanze
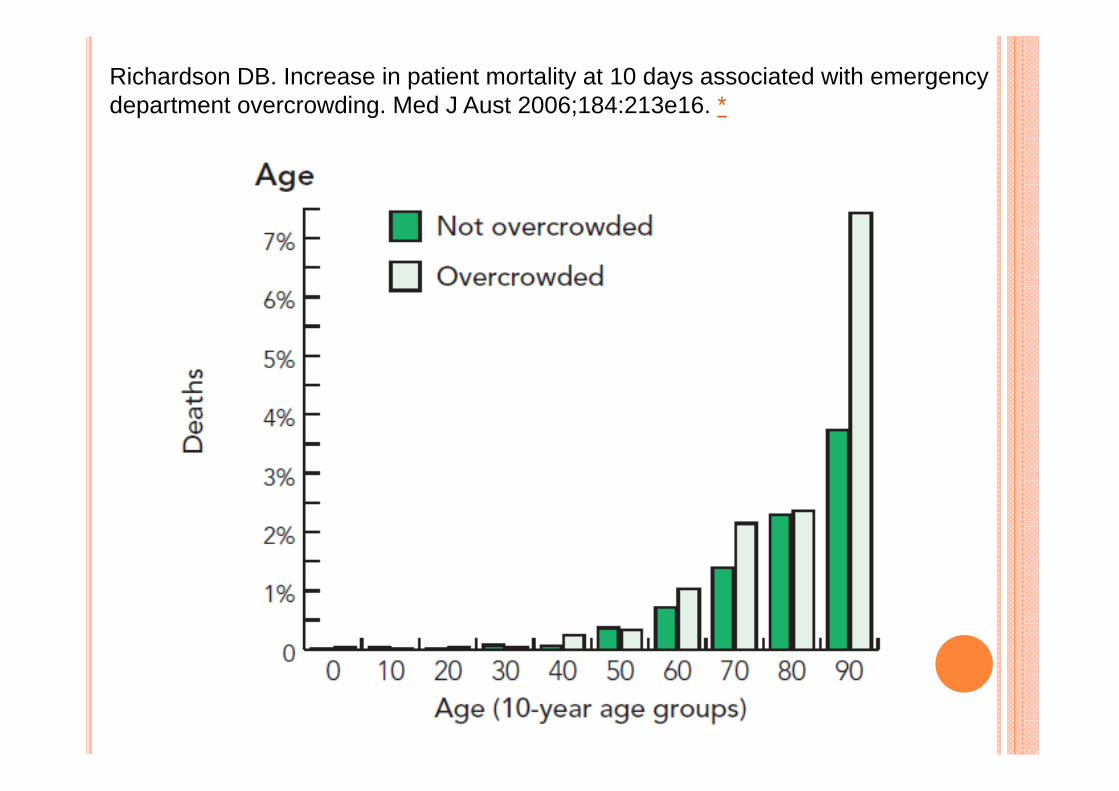
Richardson DB. Increase in patient mortality at 10 days associated with emergencydepartment overcrowding. Med J Aust 2006;184:213e16. *
*
*

Dynamics of bed use in accommodating emergencyadmissions: stochastic simulation modelAdrian Bagust, Michael Place, John W PosnettBMJ 1999;319:155–8
*

boarding
Aumentato rischio clinico
over one half of all “sentinel event” cases of morbidity and mortality secondary to delays in treatment occur in hospital EDs, and ED overcrowding has been cited as a contributing factor in 31% of these cases
Joint Commission on Accreditation of Healthcare Organizations(JCAHO). Sentinel event alert, June 17, 2002
Ospedale stratificato per intensità di cura:più tempestività per i ricoveri da PS ?
“Lean is an iconic term for the philosophybehind the Toyota Production System ofcar manufacturing, also known as the“thinking people system.” It defines asystem designed to provide the tools forpeople to continually improve their workand add value to the product or servicethey are producing. It is based on aphilosophy that abhors waste, that is,any action that does not add value to theproduct—or, in health care, to the patientexperience.”
Dickson, Ann Emerg Med. 2009;54:504-510 *


Esempi di un approccio Lean (più o meno consapevole)con ricadute sulla tempestività dei ricoveri d’urgenza
• See & treat• Percorsi «fast track»• Streamlining di patologie rilevanti per costi rischi o frequenza• Unità di osservazione breve• Percorsi di centralizzazione (Politrauma, STEMI)• Holding units, Medical Assessment & Planning Units (UK) • Bed Management• Hospitalism/Acute Medicine• «cure intermedie» – transitional care

«There was a significant reduction in admissionrates after institution of the new policy, with a relativereduction of 35.9% for total medical admissions,52.7% for chest pain, 49.2% for bronchial asthma,34.7% for heart failure, 59.1% for pneumonia and43.3% for pyelonephritis compared with the periodbefore the policy was instituted»
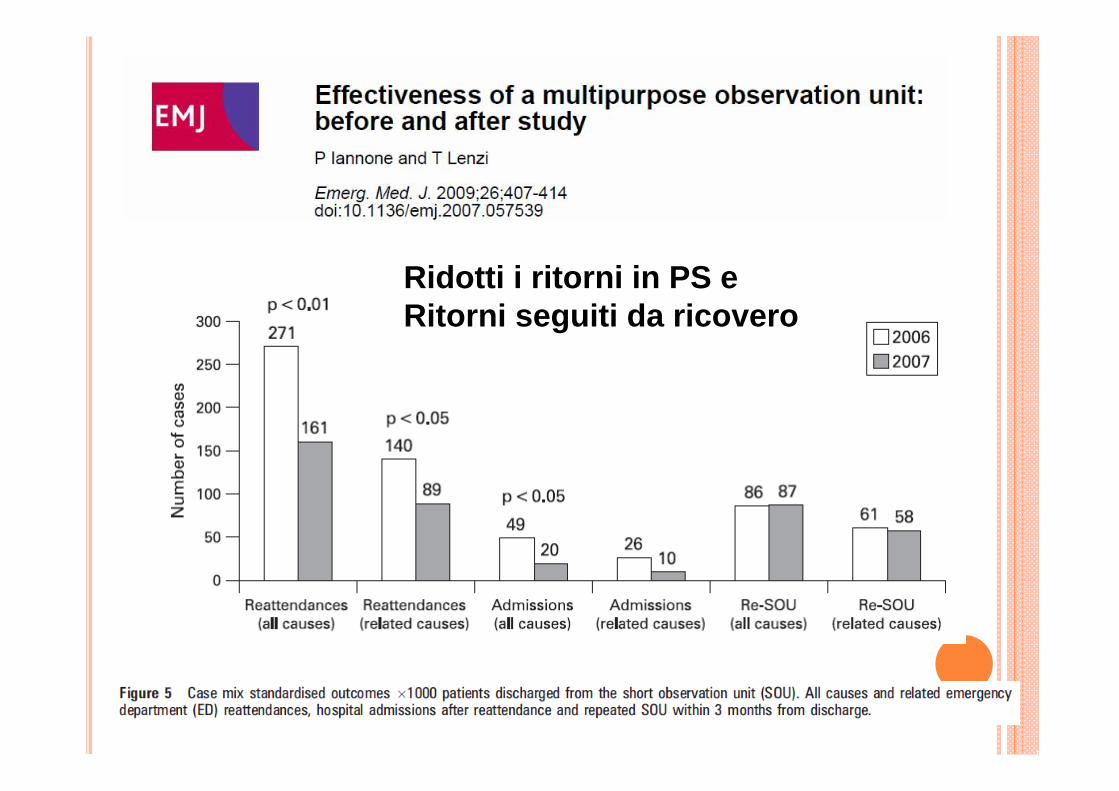
Ridotti i ritorni in PS eRitorni seguiti da ricovero
«Hospitals can establish coordinated bed managementprograms to optimize the occupancy of inpatient beds. A“bed czar” or “bed team” could receive early notice ofimpending discharges, facilitate rapid turnaround of vacantbeds, make interunit transfers, communicate hospital censusinformation, assign waiting patients to inpatient beds, andinitiate ambulance diversion. Bed management programscould direct increased attention, additional resources, andexplicit procedures toward the goal of making the mostefficient use of hospital beds.
Ann Emerg Med. 2009;53:612-617


Il metodo Lean (e l’ospedale stratificato) esempi di Interventi sanitari complessi, cioè:
«In the field of service delivery, interventions become complex anddifficult to define if, as is often the case, (1) they are deliveredacross the primary-secondary care interface; (2) they are deliveredin new settings; or (3) there is an added behavioural dimension andstaff perform new behaviours or current behaviours in a newcontext» …
…» Complex health interventions Are Non-Linear and Produce ‘‘Irregular’’ Outcomes”
Sasha Shepperd PLoS Medicine, August 2009 Can We Systematically Review Studies That EvaluateComplex Interventions?

Variabili di interesse sull’efficacia dell’ospedale stratificato
• Contesto di partenza (caratteristiche locali e bisogni dell’organizzazione)• Modalità di implementazione del cambiamento
• Top down manageriale (ospedale stratificato «chiavi in mano») vs• Enpowerment degli operatori e partecipazione attiva alla
individuazione e soluzione dei problemi (costruzione step-by-step)• Campo di intervento / scope dell’iniziativa Lean
• Processi assistenziali• Abilità –ruoli professionali• Ambiente lavorativo, modifiche strutturali, organizzative• Relazioni professionali• Reingegnerizzazione di reti assistenziali• Centralità del paziente• Interfaccia con cure primarie-intermedie
• Modalità di misurazione degli esiti• Soddisfazione degli utenti/qualità della vita• Soddisfazione degli operatori• Consumo/spreco di risorse• Eventi clinici / avversi• ….

Da De Giacomi et al. Posti letto in Italia: andamento nei trent’anni di Sistema Sanitario Nazionale - AGENAS

Da De Giacomi et al. Posti letto in Italia: andamento nei trent’anni di Sistema Sanitario Nazionale - AGENAS
INFLUENZA OUTBREAKS AND HOSPITAL BEDOCCUPANCY IN ROME: CURRENT MANAGEMENT DOESNOT ACCOMODATE FOR SEASONAL VARIATIONS INDEMAND
C.A. PERUCCI, MD; D. FUSCO, MD, ET AL.
SERV MANAGE RES 2006; 19:36-43
Daily occupancy by influenza-related cases represents 2.8% of total hospital occupancy and 7% of general medicine occupancy during the influenza season. When comparing the influenza season with the rest of the year, general medicine occupancy by influenza-related cases increases by 51% versus the 25-32% increase in other specialty wards. Little change in daily occupancy by influenza-unrelated cases was observed in all specialties when comparing the influenza season with the rest of the year.
CONCLUSIONS:Hospital specialty wards react poorly and single handedly to a minor and predictable burden. Any winter bed crisis in the Lazio region is probably the result of defective management of available beds more than excess in demand.
DODICI ANNI FA…UN LUNEDÌ.
- Professore, ci sono pazienti suoi in tutti i reparti!- Dove?- Ovunque! Ce ne sono almeno 6!- E quando sono arrivati?- Non so… ieri, stanotte…- Ma chi li ha ricoverati?- Il Pronto Soccorso!- Ah, ma quelli sono i pazienti del Pronto! I miei,
sono tutti nei miei letti!
Active Bed Management by Hospitalists and Emergency Department Throughput
Eric Howell, MD; Edward Bessman, MD; Steven Kravet, MD, MBA; Ken Kolodner, ScD; Robert Marshall, MBA; and Scott Wright, MD
Ann Int Med 2008; 149: 804‐810
In Search of a New Rhythm on Today’s Wards
FEBRUARY 8, 2012
Besides studying patient safety and watching all five seasons of The Wire, my other major goal for my London sabbatical was to understand the way the Brits organize hospital care. Mirroring the U.S. hospitalist movement, a new field—called “acute medicine”— emerged about 15 years ago and became the country’s fastest growing specialty.But there is a key difference: acute physicians are hospitalists working inside a smaller box, the acute medical unit. While the young field has enjoyed some striking successes, I recently spoke at its national conference and challenged acute physicians to be a bit more ambitious—to put a little more of the “disruptive” in their disruptive innovation.
Acute Physicians: Hospitalists Bounded by Time and Space
There are some important differences between Acute Medicine in the UK and Hospital Medicine in the US. Acute physicians largely limit their work to the AMU, meaning they have the benefit of a geographic unit (all their patients are in one place) but a far narrower reach than hospitalists: the 50% of patients who require hospital stays longer than 48 to 72 hours must be handed off to one of the subspecialty wards, a handoff that hospitalist systems avoid.

One of the most important decisions we made in the early years of hospital medicine was to embrace the “two patients” mantra, namely, “I have two sick patients: the person in the bed and the system I work in. My job is to fix both.”
I also encouraged the acute physicians to carefully challenge the boundaries of their 48-72 hour AMU cage. Right now, they’re limited in their ability to do so by both workforce constraints (there aren’t enough trained acute physicians to expand their mission very much) and predictable political friction points with their subspecialty colleagues. And it may well be that, for some patients, transfer to a subspecialty service might be the best path. But for others, eliminating the need for a handoff and taking charge of the discharge transition seem like positive steps for patients, the NHS, and the acute medicine field.
What sounds like a perfectly sensible idea (who can argue against having patients cared for by the relevant specialist?) rapidly spirals into a chaotic, inefficient, and sometimes even dangerous mess. And so it was in the UK in the late 1990s.
*






























