Embed Size (px)
DESCRIPTION
Osteoarthritis ( Oa )
Citation preview
OSTEOARTHRITIS ( OA )• A degenerative joint disease• Most common & most frequent of the disabling joint
disorder• Classified as primary (idiopathic) (of diseases) arising from an unknown
cause or secondary – resulting from previous joint injury or inflammatory dx
• Begins in the 3rd decade of life• Peaks between the 5th & 6th
• Direct correlation with age & the degenerative process
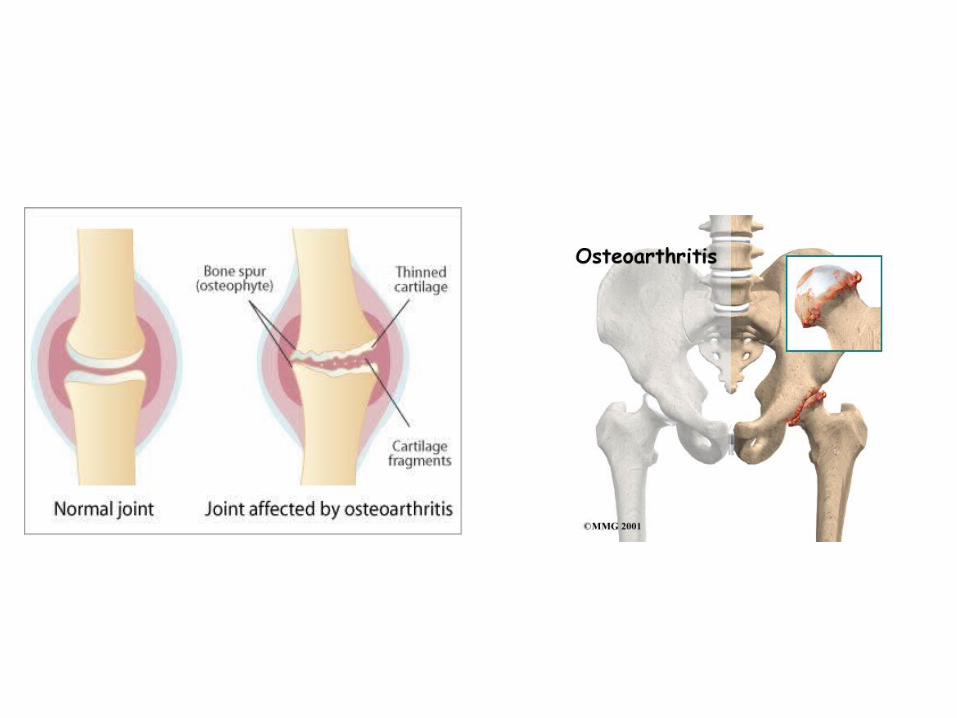
PATHOPHYSIOLOGY OF OA• OA mostly affects cartilage• Cartilage is a tissue that covers the bone in a joint• Healthy cartilage allows bones to glide over each other. It also
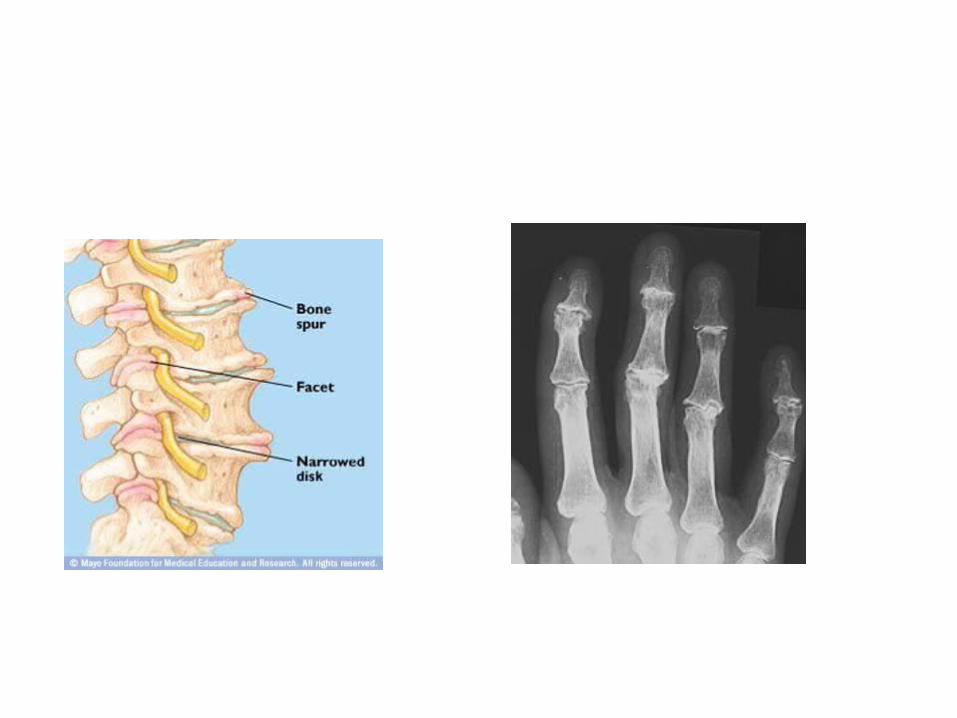
helps absorb shock of movement • In OA, top layer of cartilage breaks down & wears away• This allows bones under the cartilage to rub together• The rubbing causes pain, swelling & loss of motion of the joint• Over time the joint loses its normal shape• Also bone spurs may grow on the edges of the joint• Bits of bone or cartilage can break off & float inside the joint
space, which causes more pain & damage
RISK FACTORS OF OA
• OBESITY – every lb gained add 3 lb of pressure on knees, 6x on hips
• ↑ age• Joint injury• Stress on joints fr certain jobs & sports• Genetics• Muscle weakness – e.g. muscle surrounding the knee• Acromegaly or ↑GH – may have adverse effects on bone &
joints & can lead to OA• People with RA have higher chance of developing OA
SIGNS & SYMPTOMS OF OA• Stiffness in a joint after getting out of bed or sitting
for a long time• Last for less than 30 minutes and ↓ with movement• Joint stiffness after periods of prolonged use• Swelling & tenderness on 1 or more joints• A crunching feeling or the sound of bone rubbing on
bone• Deterioration of coordination, posture & walking• Joint pain is usually less in the morning & worse in
the evening after a day’s activity
ASSESSMENT & DIAGNOSIS
• Difficult to diagnose• Physical assessment – tender enlarged
joints - inflammation
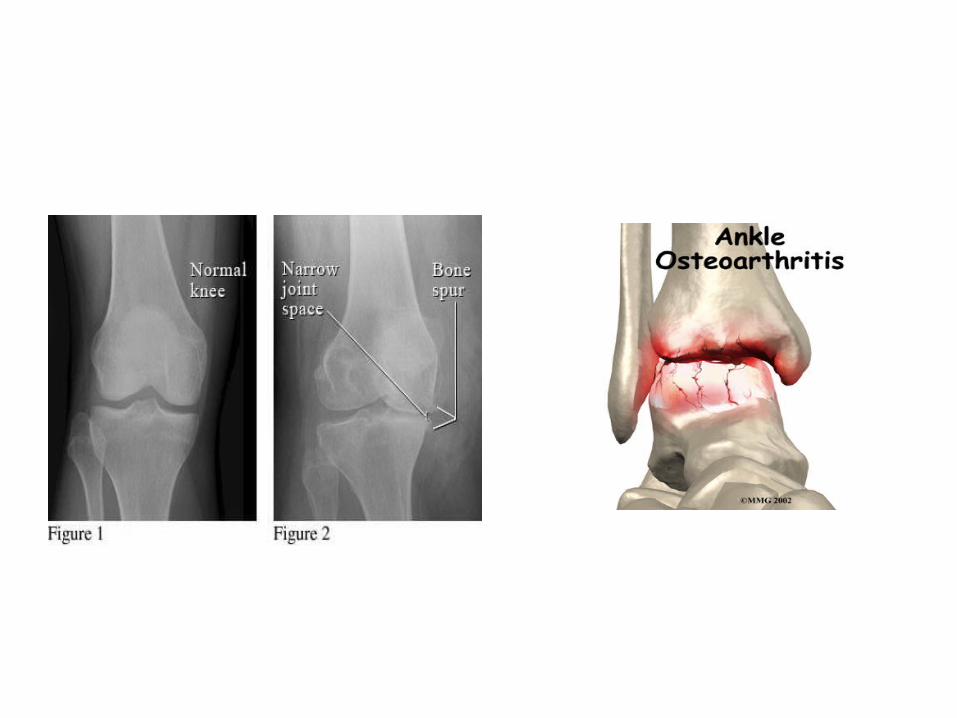
• X- ray – progressive loss of cartilage can be detected
GOALS OF MEDICAL MANAGEMENT
OA treatment has 4 main goals:• Improve joint function• Keep a healthy body wt• Control pain• Achieve a healthy life style
CONSERVATIVE TREATMENT OF OA
• Education• Use of heat• Weight reduction• Joint rest & avoidance of joint overuse• Orthotic devices• Exercises – moderate & regular ex. Strengthen muscle &
bones• Massage• Occupational & physical therapy – strengthen muscle &
improve flexibility
PHARMACOLOGIC TREATMENT OF OA• Paracetamol• Oral NSAIDs – same as in RA• Topical NSAIDs , capsaicin and methylsalicylate cream• Weak opioids & narcotic analgesics for severe pain• Intra-articular injection of corticosteroids• Intra-articular injection of hyaluronic acid• Glucosamine and/or chondroitin sulphate
SURGICAL TREATMENT OF OA• Arthroscopy• Osteotomy• Total joint replacement
TREATMENT OF OAGLUCOSAMINE SULPHATE ( Viartril-S )• Popular treatment for OA - oral• Several studies demonstrated that glucosamine was comparable to NSAIDs for
knee OA• Other studies measuring changes in joint space narrowing suggested an effect
against articular cartilage loss• Real MOA is largely unknown• Thought to stimulate chondrocytes to make proteoglycans• Thought to inhibit cartilage catabolic enzymatic activity• Also improves the lubricant properties of synovial fluid• Safe• Not recommended in pt with seafood allergy – glucasamine is manufactured fr
chitin found in shrimp, crabs & lobster shell or produce synthetically• Sometimes combined with chondroitin sulphate – more effective• Chondroitin sulphate is part of a protein that give cartilage elasticity
Glucosamine - continue
Side Effects :• Upset stomach• Drowsiness• Insomnia• Headache• Skin reaction• Sun sensitivity• Loss of appetite• Nausea & vomiting• Flatulence• Constipation & diarrhoea• ↑ risk of bleeding
Glucosamine - continue
Drug Interaction• May ↑ risk & S/E of diuretics e.g. Lasix• May ↑ risk of bleeding when taken with aspirin, anti-
coagulant, anti – platelet , NSAIDs• Chondroitin also may have anti- coagulant effect
HYALURONIC ACID ( Hyalgan )• In OA, the hyaluronic acid is decreased and compromised in synovial fluid• HA acts as a shock absorber & lubricant in joints• HA is highly viscous, allowing the cartilage surfaces of the bones to glide upon
each other smoothly• Exogenous supplementation of intra-articular HA is thought to support changes in
synovial fluid• Injection of HA into joint or viscosupplementation is an effective treatment for OA• Indicated for OA not responsive to non-pharmacologic measures & to simple
analgesia• Requires sterile technique, remove joint effusion if present prior to injection• 3 – 5 weekly injections recommended • Can be expensive• Pain relief usually by 8 – 12 wks can last up to 6 – 10 months• Treatment can be repeated every 6 months prn
INJECTION HYALURONIC ACID – CONT.Joints Usually Injected• Shoulder• Elbow• Hip• Knee• Hand• Wrist• Foot
Possible S/E• Swelling• Pain
Contraindication• Joint infection / skin infection at injection site• Eggs / poultry allergy
CORTICOSTEROID INJECTIONS• Allow to deliver a high dose of medication to the problem area (direct to
joint)• Suppress inflammation -↓ erythema, ↓ swelling, ↓ heat, ↓ tenderness• Help preserve joint structure & function• Avoid the need for oral steroids which have greater S/E• Not expensive• Significant improvement after 1 week of inj– effect lasting for 3 – 4 wks to
6 months• Allow 4 – 6 weeks between injections• In severe OA – joints can be injected up to 3 – 4 times per year• Avoid injecting several large joints at the same time• E.g. Triamcinolone, methyprednisolone