Embed Size (px)
Citation preview

, . 182: 92–98 (1997)
OSTEOCLASTS ARE CAPABLE OF PARTICLEPHAGOCYTOSIS AND BONE RESORPTION
. 1, . . . 2, . . . 2, . . . . 1 . . 2,3*1University of Oxford, Nuffield Department of Orthopaedic Surgery, Oxford, U.K.
2Nuffield Department of Pathology and Bacteriology, John Radcliffe Hospital, Oxford OX3 9DU, U.K.3University of Oxford, The Department of Pathology, Nuffield Orthopaedic Centre, Oxford OX3 7LD, U.K.
SUMMARY
Osteoclasts are multinucleated cells specialized for the function of lacunar bone resorption. Although they are known to be capableof phagocytosis of inert particles, it is not known whether this abolishes their ability to respond to hormones or to form resorptionlacunae. Human and rat osteoclasts were isolated from giant cell tumours of bone and rat long bones, respectively, and cultured oncoverslips and cortical bone slices, both in the presence and in the absence of particles of latex (1 ìm diameter) and polymethylmeth-acrylate (PMMA) (<50 ìm). By light microscopy, it was evident that osteoclasts which had phagocytosed both latex and PMMAparticles remained responsive to calcitonin. Osteoclast phagocytosis of particles was also evident on scanning electron microscopy, whereit could also be seen that these cells were associated with the formation of resorption lacunae. These findings underline the fact that theosteoclast is a true member of the mononuclear phagocyte system and that phagocytosis does not abrogate either its hormonal responseto calcitonin or its highly specialized function of bone resorption. That osteoclasts which have phagocytosed biomaterial particles suchas PMMA are still able to carry out lacunar bone resorption is of interest in clinical conditions such as aseptic loosening, where a heavyforeign body particle load is often associated with extensive bone resorption. ? 1997 by John Wiley & Sons, Ltd.
J. Pathol. 182: 92–98, 1997.No. of Figures: 4. No. of Tables: 0. No. of References: 36.
KEY WORDS—osteoclast; macrophage; bone resorption; foreign body; phagocytosis
INTRODUCTION
The osteoclast is a multinucleated cell which uniquelycarries out the highly specialized function of lacunarbone resorption.1,2 Osteoclasts form by fusion of circu-lating mononuclear precursor cells of haematopoieticorigin. They are known to have marrow precursorsin common with monocytes and macrophages;3–5 onthe basis that they share a number of functional, cyto-chemical, and morphological features with macro-phages, osteoclasts are considered to form part of themononuclear phagocyte system (MPS).6,7A characteristic feature of cells of the MPS is their
ability to carry out phagocytosis avidly and efficiently.Chambers8 showed that osteoclasts were capable ofphagocytosing glutaraldehyde-fixed red blood cellsand latex particles in a manner comparable to thatof macrophages. In the same study, he pointed outthat osteoclasts did not phagocytose opsonized orcomplement-coated red cells; this is one of a numberof morphological, cytochemical, and functional differ-ences which distinguish mature macrophages fromosteoclasts.1,2One pathological context in which osteoclast phago-
cytosis may be important is in periprosthetic tissuessurrounding joint arthroplasty components where thereis a heavy biomaterial implant wear particle load andan associated heavy foreign body macrophage and
macrophage polykaryon response.9,10 Biomaterial wearparticles are thought to play an important role in thepathogenesis of aseptic loosening11–14 and osteolysisassociated with osteoclastic activity can be seen at theinterface between the bone and cemented loose arthro-plasy components.9–11,15,16 Although many studies onthe pathobiology of aseptic loosening have examined theeffect of biomaterial wear particles on macrophage func-tion (for review see ref 12, 14, and 17), the effect of theseparticles on osteoclast function has not been examined.In fact, it is not generally acknowledged that osteoclastsare capable of biomaterial wear particle phagocytosis.Willert et al.18,19 concluded from morphological studiesof the bone–implant interface that osteoclasts did notcontain polymethylmethacrylate (PMMA) particles, andthe current consensus opinion appears to be that inaseptic loosening of hip arthroplasties, the multi-nucleated cells that both contain biomaterial wear par-ticles and line a bone surface undergoing resorption arenot osteoclasts.15Given that osteoclasts represent the MPS cell of bone
and are known to be capable of particle phagocytosisin vitro, it would be most surprising if they did not carryout phagocytosis of the numerous biomaterial wearparticles which are found in the pseudomembrane sur-rounding a loose prosthesis. It is not known, however,whether osteoclasts are capable of phagocytosing bio-material wear particles such as PMMA, and whetherosteoclasts that have phagocytosed particles remainfunctionally competent. The aims of this study havetherefore been two-fold: firstly to establish that osteo-clasts are capable of phagocytosing biomaterial wear
*Correspondence to: N. A. Athanasou.
Contract grant sponsor: British Orthopaedic Association WishboneTrust.
CCC 0022–3417/97/050092–07 $17.50 Received 31 July 1996? 1997 by John Wiley & Sons, Ltd. Revised 24 October 1996
Accepted 30 October 1996

particles; and secondly, to determine whether osteoclastswhich have phagocytosed particles retain their specificability to respond directly to calcitonin20 and to carryout lacunar bone resorption.21,22
MATERIALS AND METHODS
Latex particles (1 ìm diameter) were obtained fromSigma (U.K.). PMMA particles were made from CMWacrylic cement (Dupuy, U.K.) and prepared and poly-merized according to the manufacturer’s instructions.Particles were prepared from polymerized bone cementby crushing PMMA using a steel mortar and pestle andthen a Tema Micromill (Siebtechnik, Germany). Theresultant particles were passed through a set of meshsieves to produce PMMA particles less than 50 ìm indiameter. The particles were then weighed, suspended inculture medium, sterilized in absolute alcohol, sonicatedfor 10 min, and then added to culture wells at a concen-tration of 20 ìg/ml. Control cultures consisted of thoseto which no particles had been added. In all cases, thebone slices and glass coverslips were incubated at 37)Cin 5 per cent CO2.
Isolation of osteoclasts
Rat osteoclasts were isolated from the femurs andtibiae of 3-day-old neonatal rats.20 These bones werecuretted in 2 ml of á minimal essential medium (MEM)(Gibco, U.K.) in a 35 mm tissue culture dish. Thecuretted fragments were vigorously agitated using ablunt-ended glass pipette. Large fragments were allowedto settle and approximately 150 ìl of the suspensionwas then added to 7 mm wells containing 6 mm diam-eter glass coverslips, or human cortical bone slices(4#3 mm) prepared as previously described.21Osteoclasts were also isolated from two human giant
cell tumours of bone, which contained abundant osteo-clasts.23 Specimens of fresh giant cell tumour werewashed in MEM and then finely curetted into 2 ml ofMEM; 150 ìl of the suspension was similarly settled onglass coverslips and bone slices as described above.
Osteoclast cultures on bone slices and glass coverslips inthe presence and absence of particles
The osteoclast suspension derived from rat long bonesor human giant cell tumours of bone was settled oncoverslips and bone slices for 30 min. Bone slices orcoverslips were then removed from the 7 mm wells,washed vigorously in MEM to remove non-adherentcells, and placed in 16 mm wells containing 1 ml ofMEM supplemented with 10 per cent fetal calf serum(MEM/FCS). A suspension of 1 ìm latex particles inMEM/FCS was added to the wells to which bone slicesand coverslips had been transferred (final concentration20 ìg/ml). Similarly, PMMA particles suspended inMEM/FCS were added to culture wells to produce afinal concentration of 20 ìg/ml. Particles were not addedto control osteoclast cultures.
Calcitonin response of isolated osteoclasts containingparticles
Osteoclast cultures on 6 mm glass coverslips wereincubated for 24 h, after which time salmon calcitonin(Rorer, U.K.) (1 ìg/ml) was added to each well. Bothcontrol cultures and cultures to which latex and PMMAparticles had been added were continuously observedby phase contrast microscopy in order to determinewhether there was a morphological response to calci-tonin.20 Cultures were then fixed in buffered formalinand Giemsa-stained.
Detection of bone resorption by isolated human and ratosteoclasts containing particles
Human and rat osteoclast cultures on bone slices wereincubated for periods of 24 h and 3 days before theywere fixed in 4 per cent glutaraldehyde for 30 m. Thespecimens were dehydrated through a graded ethanolseries, critical point-dried from CO2, and then sputter-coated with gold and examined in a Philips SEM 505scanning electron microscope to look for evidence oflacunar resorption of the smooth bone surface byparticle-containing osteoclasts.
RESULTS
Light microscopy of osteoclast cultures: response tocalcitoninOsteoclasts derived from neonatal rat long bones and
human giant cell tumours of bone were readily identifiedon phase contrast microscopy by their multinuclearityand large size. These cells possessed abundant cytoplasmwith broad pseudopodia and were highly motile. Byphase contrast microscopy it was evident that 1 ìm latexparticles were rapidly phagocytosed by osteoclasts andwere present within the cytoplasm of most osteoclasts1 h after administration. In 24 h and 3 day cultures, latexparticles were readily identified within the cytoplasm ofall osteoclasts by phase contrast microscopy and afterGiemsa staining (Fig. 1a). In 24 h and 3 day cultures towhich PMMA particles had been added, phagocytosedPMMA particles were evident as clear vacuoles in thecytoplasm of all multinucleated cells in Giemsa-stainedpreparations. These vacuoles represent phagocytosedPMMA particles dissolved out in processing. In anumber of the vacuoles, weakly birefringent bariumparticles were also noted.Following administration of salmon calcitonin (1 ìg/
ml) to 24 h rat osteoclast cultures on glass coverslips,osteoclasts, including those containing PMMA or latexparticles, showed evidence of a calcitonin response, withcessation or marked inhibition of cell motility and rapidretraction of the cytoplasmic processes (Fig. 1b). Noobvious difference was seen in the response time ofosteoclasts to the administration of calcitonin betweencontrol and particle-fed cultures, evidence of a calcitoninresponse being seen within 5–15 min and cessation ofcytoplasmic motility lasting from 2 to 4 h in both controland particle-containing osteoclast cultures.
93OSTEOCLASTS ARE CAPABLE OF PARTICLE PHAGOCYTOSIS AND BONE RESORPTION
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)

Bone resorption by osteoclasts containing PMMA andlatex particles
By SEM, rat and human osteoclasts were readilyidentified in 24 h and 3 day cultures on bone slices bytheir large size and broad cytoplasmic extent. In controlcultures, it was evident that osteoclasts contained manyfine microvilli on their upper surface and at the cellperiphery, lobulated and folded pseudopods or finefilopodia, which made contact with the bone surface.In 24 h and 3 day cultures to which 1 ìm latex
particles had been added, it was clearly evident that ratand human osteoclasts had phagocytosed these particles(Fig 2 and 3). Small undulations were present on the cellsurface of rat and human osteoclasts and cytoplasmic
processes extending from the cell body of human osteo-clasts appeared blunted or rounded. These undulationsand swellings on the cell surface measured approxi-mately 1 ìm in maximum dimension. Large cells con-taining phagocytosed particulate material were foundoverlying or in the immediate vicinity of typical lacunarresorption pits, which were well-defined round or ovalareas containing a base of mineralized collagen fibres.As osteoclasts in culture on glass coverslips were notedto have rapidly (within 1 h) taken up latex particles, andas it is known that lacunar resorption by osteoclastsdoes not occur until they have been cultured on amineralized substrate for several hours,21,22 these resorp-tion pits would appear to have been formed by osteo-clasts which had already phagocytosed latex particles;
Fig. 1—Cells isolated from rat long bones cultured for 24 h in the presence of 1 ìm latex particlesshowing (a) an active multinucleated osteoclast (arrowed) containing numerous 1 ìm latex particles(arrow-head); and (b) an osteoclast containing latex particles after calcitonin administration; there ismarked blunting and retraction of cytoplasmic processes. (Giemsa, #400)
94 W. WANG ET AL.
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)
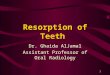
this is supported by our findings of a number of latexparticle-containing osteoclasts which overlie lacunarresorption areas which are still in the process of beingexcavated (Fig. 2). Small cells of macrophage-like mor-phology were also noted to show similar blunting ofpseudopodia and undulations of the cell surface. Thesecells, however, were not associated with resorption pitformation.Lacunar resorption pit formation was also seen in
24 h and 3 day rat and human osteoclast cultures towhich PMMA particles had been added (Fig. 4). In this
case, a discernible change in the shape or morphologicalappearance of the osteoclast was not obvious, althoughPMMA material was often noted attached to the cellsurface of the osteoclast or on the bone surface in thevicinity of osteoclasts.An obvious difference in the amount of bone resorp-
tion was not seen in 24 h and 3 day cultures of control,latex or PMMA-containing rat or human osteoclastcultures. Up to 12 resorption pits were found on boneslices on which rat osteoclasts had been isolated, and upto 15 resorption pits on bone slices containing human
Fig. 2—SEM photomicrograph of rat osteoclast cultured for 24 h on bone slice in the presence of1 ìm latex particles showing (a) a latex particle-containing osteoclast forming a resorption pit on thebone surface (fieldwidth=90 ìm) and (b) a high-power view of the same osteoclast showing smallundulations on the osteoclast cell surface (some arrowed); these represent internalized latex particles.The osteoclast lies above a resorption pit containing exposed collagen fibres. (fieldwidth=22 ìm)
95OSTEOCLASTS ARE CAPABLE OF PARTICLE PHAGOCYTOSIS AND BONE RESORPTION
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)

osteoclasts derives from giant cell tumour of bone, bothin the presence and in the absence of PMMA or latexparticles.
DISCUSSION
The MPS is known to consist of a diverse range ofcells, a number of which exhibit unique features special-ized for particular tissues. These cells have a common
origin in the bone marrow and share certain functionaland cytochemical characteristics;7 one of the mostimportant of these functional characteristics is the abil-ity to carry out phagocytosis avidly and efficiently. Onthis basis, and in view of a number of other morphologi-cal and cytochemical characteristics that osteoclasts areknown to share with monocytes and macrophages, itwas proposed that the osteoclast represents a highlyspecialized MPS cell of bones.6–8 The present studysupports this hypothesis by showing that osteoclasts
Fig. 3—SEM photomicrograph of human osteoclast cultured for 24 h on a bone slice in the presenceof 1 ìm latex particles showing (a) an osteoclast (arrowed) overlying a compound resorption pit. Thecell surface of the osteoclast is irregular and the cell processes (arrow-head) extending from the bodyof the osteoclast are markedly blunted. (fieldwidth=245 ìm) and (b) a high-power view of bluntedcell processes and undulations on the cell surface of the osteoclast. (fieldwidth=42 ìm)
96 W. WANG ET AL.
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)

are efficient phagocytic as well as bone-resorbing cells,capable of phagocytosing not only latex, but alsoPMMA biomaterial wear particles; this activity does notabrogate the ability of these cells to respond to calci-tonin or to carry out the highly specialized function oflacunar bone resorption.Osteoclasts and foreign-body macrophages and
macrophage polykaryons have been shown to possessa number of enzyme and cell surface receptors incommon.1,6,24 Osteoclasts, however, are primarily distin-guished from macrophages and macrophage poly-karyons by their expression of calcitonin receptors,their inhibitory response to calcitonin, and their unique
ability to form resorption lacunae on bone slices.2,25 Wefound that osteoclasts which have phagocytosed particu-late material remained capable of responding to calci-tonin, a hormone which acts directly and specificallyupon osteoclasts, and that phagocytosis of particulatematerial did not abolish their ability to form resorptionlacunae in bone.In both man and experimental animals, it has been
shown that mononuclear osteoclast precursors, isolatedfrom either bone marrow or the circulation, possess thephenotypic characteristics of mononuclear phagocytes;in the process of osteoclast differentiation, monocytesand macrophages are capable of undergoing significant
Fig. 4—Low- and (b) high-power SEM photomicrographs of human osteoclasts cultured for 24 h ona bone slice in the presence of PMMA particles showing an osteoclast and adjacent resorption pit.PMMA particles are present on the cell surface. (a) Fieldwidth=160 ìm; (b) fieldwidth=75 ìm)
97OSTEOCLASTS ARE CAPABLE OF PARTICLE PHAGOCYTOSIS AND BONE RESORPTION
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)

phenotypic modification, losing macrophage andacquiring osteoclast characteristics.26–28 One functionalproperty which osteoclasts do not appear to lose isphagocytosis, which is characteristic of all MPS cells. Inthis regard, it should be noted that mouse mononuclearphagocytes which have phagocytosed latex, PMMA,and other orthopaedic implant biomaterial particleshave been shown to be capable of differentiation intoosteoclastic-bone resorbing cells under specific cellularand hormonal conditions of culture.27,29,30 Both macro-phages and osteoclasts are also capable of recognizingand phagocytosing bone mineral.1,31 Chambers32,33 pro-vided evidence that macrophage giant cell formationmay occur following simultaneous attachment of twomononuclear phagocytes to the same ingestible material,the fusion of endosome margins of these mononuclearphagocytes leading to the formation of a giant cell.Fusion of avian monocytes and osteoclasts has pre-viously been noted34 and it remains a possibility thatsimultaneous particle and/or bone phagocytosis bymacrophage and osteoclasts may result in the fusion ofthese cells.In aseptic loosening of cemented implant components,
a heavy macrophage and macrophage polykaryonresponse is commonly seen in relation to wear particlesderived from PMMA cement and other polymeric andmetal implant-derived biomaterials.9–11 The pseudo-membrane containing this cellular foreign-bodyresponse lies at the bone–implant interface, where multi-nucleated cells can be found lining the bone surfaceundergoing osteolysis. Although it has been claimed thatthe multinucleated cells which both contain biomaterialwear particles and line the resorbing surface of bone arenot osteoclasts,15,18,19 our results do not support thisobservation, as they clearly show that osteoclasts whichhave phagocytosed PMMA wear particles remain capa-ble of lacunar bone resorption. This would accord withthe morphological observation that extensive or rapidosteolysis (‘aggressive granulomatosis’) of cementedimplants is associated with a heavy wear particleload and extensive periprosthetic bone resorption.35,36Although we did not find that phagocytosis of PMMAparticles appeared to compromise the ability of osteo-clasts to respond to calcitonin or to carry out lacunarresorption, further studies need to be carried out toestablish that this is the case for all biomaterial particles.
ACKNOWLEDGEMENTS
We thank Mrs Margaret Pearce for typing themanuscript. This study was supported by the BritishOrthopaedic Association Wishbone Trust.
REFERENCES1. Gothlin G, Ericsson JLE. The osteoclast: review of origin, structure–
function relationship. Clin Orthop 1976; 120: 201–231.2. Chambers TJ. The pathobiology of the osteoclast. J Clin Pathol 1985; 38:
241–252.3. Schneider GB, Relfson M. A bone marrow fraction enriched for
granulocyte–macrophage progenitors gives rise to osteoclasts in vitro. Bone1988; 9: 303–310.
4. Kurihara N, Chenu C, Miller M, Civin C, Roodman GD. Identification ofcommitted mononuclear precursors for osteoclast-like cells formed in longterm human marrow cultures. Endocrinology 1990; 126: 2733–2741.
5. Burger EH, van der Meer JWM, van de Gevel JS, Gribnau JC, ThesinghCW, van Furth R. In vitro formation of osteoclast from long-term culturesof bone marrow mononuclear phagocytes. J Exp Med 1982; 156: 1604–1614.
6. Chambers TJ. The cellular basis of bone resorption. Clin Orthop 1980; 151:284–294.
7. van Furth R. Cells of the mononuclear phagocyte system. Nomenclature interms of sites and conditions. In: van Furth R, ed. Mononuclear Phago-cytes: Functional Aspects. The Hague: Martinus Nijhoff, 1980; 1–30.
8. Chambers TJ. Phagocytosis and trypsin-resistant glass adhesion by osteo-clasts in culture. J Pathol 1979; 127: 55–60.
9. Revell PA. Tissue reactions to joint prostheses and the products of wear andcorrosion. In: Berry C, ed. Current Topics in Pathology. Berlin: Spinger-Verlag, 1982; 73–101.
10. Forest M, Carlioz A, Vacher Lavenu MC, et al. Histologic patterns of boneand articular tissues after orthopaedic reconstructive surgery (artificial jointimplants). Pathol Res Pract 1991; 187: 963–977.
11. Lennox DW, Schofield BW, McDonald DF, Riles LH. A histologiccomparison of aseptic loosening of cemented, press-fit and biologicingrowth prostheses. Clin Orthop 1987; 225: 171–191.
12. Harris WH. Osteolysis and particle disease in hip replacements (a review).Acta Orthop Scand 1994; 65: 113–123.
13. Total Hip Replacement. NIH Consensus Statement 12–14 Sept 1994; 12(5):1–31.
14. Maloney WJ, Lane Smith R. Periprosthetic osteolysis in total hip arthro-plasty: the role of particulate wear debris. J Bone Joint Surg 1995; 77A:1448–1461.
15. Freeman MAR, Bradley GW, Revell PA. Observations upon the interfacebetween bone and polymethylmethacrylate cement. J Bone Joint Surg 1982;64B: 489–493.
16. Pazzaglia UE. Pathology of the bone–cement interface in loosening of totalhip replacements. Arch Orthop Trauma Surg 1990; 109: 83–88.
17. Amstutz HC, Campbell P, Kossovsky N, Clarke IC. Mechanism andclinical significance of wear debris-induced osteolysis. Clin Orthop 1992;276: 7–18.
18. Willert HG, Bertram H, Buchhorn H. Osteolysis in alloarthroplasty of thehip: the role of ultra high molecular weight polyethylene wear particles. ClinOrthop 1990; 258: 95–107.
19. Willert HG, Bertram H, Buchhorn GH. Osteolysis in alloarthroplasty of thehip: the role of bone cement fragmentation. Clin Orthop 1990; 258: 108–121.
20. Chambers TJ, Magnus CJ. Calcitonin alters the behaviour of isolatedosteoclasts. J Pathol 1982; 136: 27–39.
21. Chambers TJ, Revell PA, Fuller K, Athanasou NA. Resorption of bone byisolated rabbit osteoclasts. J Cell Sci 1984; 66: 383–399.
22. Ali NN, Boyde A, Jones SJ. Motility and resorption: osteoclastic activityin vitro. Anat Embryol 1984; 170: 51–56.
23. Chambers TJ, Fuller K, McSheehy PMJ. The effects of calcium regulatinghormones on bone resorption by isolated human osteoclastoma cells.J Pathol 1985; 145: 297–305.
24. Athanasou NA, Quinn J. Immunophenotypic differences between osteo-clasts and macrophage polykaryons: immunohistological distinction andimplications for osteoclast ontogeny and function. J Clin Pathol 1990; 43:997–1004.
25. Nicholson GC, Moseley JM, Sexton PM, Mendelsohn FAO, Martin TJ.Abundant calcitonin receptors in isolated rat osteoclasts. J Clin Invest 1986;78: 355–360.
26. Udagawa N, Takahashi N, Akatsu T, et al. Origin of osteoclasts: maturemonocytes and macrophages are capable of differentiating into osteoclastsunder a suitable microenvironment prepared by bone marrow-derivedstromal cells. Proc Natl Acad Sci USA 1990; 87: 7260–7264.
27. Quinn J, Sabokbar A, Athanasou NA. Cells of the mononuclear phagocyteseries differentiate into osteoclastic lacunar bone-resorbing cells. J Pathol1996; 179: 106–111.
28. Fujikawa Y, Quinn JMW, Sabokbar A, McGee JO’D, Athanasou NA. Thehuman osteoclast precursor circulates in the monocyte fraction. Endocrinol-ogy 1996; 137: 4058–61.
29. Quinn JM, Joyner C, Triffitt JT, Athanasou NA. Polymethylmethacrylate-induced inflammatory macrophages resorb bone. J Bone Joint Surg 1992;74B: 652–658.
30. Pandey R, Quinn J, Joyner C, Murray DW, Triffitt JT, Athanasou NA.Arthroplasty implant biomaterial-associated macrophages differentiate intolacunar bone-resorbing cells. Ann Rheum Dis 1996; 55: 388–395.
31. Chambers TJ. Phagocytic recognition of bone by macrophages. J Pathol1981; 135: 1–7.
32. Chambers TJ. Fusion of macrophages following simultaneous attemptedphagocytosis of glutaraldehyde-fixed red cells. J Pathol 1976; 122: 71–80.
33. Chambers TJ. Multinucleate giant cells. J Pathol 1978; 122: 125–148.34. Zambonin-Zallone A, Teti A, Primavera MV. Monocytes from circulating
blood fuse in vitro with purified osteoclasts in primary culture. J Cell Sci1984; 66: 335–342.
35. Harris WH, Schiller AL, Scholler J-M, Freiberg RA, Scott R. Extensivelocalised bone resorption in the femur following total hip replacement.J Bone Joint Surg 1976; 58A: 612–617.
36. Santavirta S, Konttinen TY, Bergroth V, Eskola A, Tallroth V, LindholmTS. Aggressive granulomatous lesions associated with hip arthroplasty:immunopathological studies. J Bone Joint Surg 1990; 72A: 252–258.
98 W. WANG ET AL.
? 1997 by John Wiley & Sons, Ltd. J. Pathol. 182: 92–98 (1997)

![Review V-ATPases and osteoclasts: ambiguous future of V ...thno.org/v08p5379.pdfosteoclasts, which is a key factor for bone resorption [2]. The V-ATPases-related regulation of extracellular](https://img.pdfslide.net/doc/110x75/5ee15f47ad6a402d666c473b/review-v-atpases-and-osteoclasts-ambiguous-future-of-v-thnoorg-osteoclasts.jpg)