Embed Size (px)
Citation preview

OSTEOPOROSIS: OVERVIEW, WORKUP, DIAGNOSIS
Rick Pope MPAS, PAC, DFAAPA
8:00-9:00 AM
July 30, 2011

Faculty Disclosures
Amgen- Advisory committee denosumab
URL Pharma-Advisory committee and speaker’s
bureau colchicine
UCB Pharma-Speaker’s Bureau certolizumab
Takeda-Speaker’s bureau febuxostat

Question #1Bone Density Comparison
Which anatomical site is most likely to give the best information in a patient with degenerative joint disease (“DJD”) when you are comparing her baseline BMD to a subsequent BMD in 2 years?
1. Hip
2. Spine
3. Either location can be used

Case #3Non-responder?
A 57-year-old woman with asthma has been on prednisone 7.5 mg per day for the past 6 months. Her T-score at the spine is –1.4 and at the hip is –1.1. She
is started on alendronate 70 mg once weekly. A repeat DXA 12 months later shows a 3% loss at the
spine and 2% loss at the total hip.Is this patient a “non-responder” to
alendronate?
1. Unclear
2. Yes
3. No

Learning Objectives:
1. Use NOF criteria for initiating treatment of postmenopausal osteoporosis
2. Review the FRAX calculator for use in decisions for treatment of osteoporosis
3. How to monitor effects of therapy based on pt. outcomes and response to treatment using BMD testing
4. Discuss the pros and cons of Vitamin D and Calcium, exercise
5. Review the FDA Approved medications for prevention and treatment

Osteoporosis Definition
Osteoporosis, or porous bone, is a disease characterized by low
bone mass and structural deterioration of bone tissue, leading to
bone fragility and an increased susceptibility to fractures,
especially of the hip, spine and wrist, although any bone can be
affected¹
In simpler terms, osteoporosis is a condition in which the bones
become weak and can break from a minor fall or, in serious
cases, from a simple action such as a sneeze or bumping into
furniture.¹ 1. Fast facts NOF.org simple definition

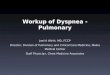
Normal Osteoporosis
Courtesy of David W. Dempster, PhD 2000
MICROARCHITECTURAL CHANGES IN OSTEOPOROSIS
BROKEN CROSSLINKS

STRESS RISER

OsteoporosisPrevalence
h Osteoporosis is a major public health threat for an
estimated 44 million Americans, or 55 percent of the
people 50 years of age and older.
h In the U.S. today, 10 million individuals are estimated
to already have the disease and almost 34 million more
are estimated to have low bone density, placing them
at increased risk for osteoporosis and broken bones.
h While osteoporosis is often thought of as an older
person's disease, it can strike at any age.
National Osteoporosis Foundation Copyright © 2011 All Rights Reserved 1150 17th Street, NW Suite 850 Washington, DC 20036

Background
h It affects all ethnicity/racial groups/both sexes
h 30% white woman over 50 y.o.
h 16% Mexican-American women
h 10% African-American women

Fractures attributable toOsteoporosis US
US OP fractures2005
OtherHipVertebraWristPelvis
Pelvis 7%
Other 33%hands/fingershumerus/claviclepatellatibia/fibula
Hip 14%
Wrist 19%
2 million fractures in 2005
73% nonvertebral sites
29% occurred in men
14% occurred in nonwhites
Vertebra 27%
Adapted from Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden ofosteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22:465-475. 2010 AACE osteoguiidelines

Cost of osteoporosis fractures 2005
Adapted from Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States,
2005-2025. J Bone Miner Res. 2007;22:465-475. 2010 AACE osteoguiidelines

FracturesNational Osteoporosis Foundation
h Approximately one in two women and up to one
in four men over age 50 will have an
osteoporosis-related fracture in their remaining
lifetime.
h Fractures due to osteoporosis are most likely in
the hip, spine and wrist, but any bone can be
affected.

One In Five Women Who Suffers A Hip Fracture Is Assessed or Treated For Osteoporosis
Percentage of women who had either a BMD or a prescription for a drug to either prevent or treat osteoporosis 6 months after the date of fracture shows a decline by 1.4% from 2006 to 2007
*Medicare
National Committee For Quality Assurance State Of Health Care Quality 2008 Report.
HEDIS Measures of CareOsteoporosis Management in Women
Who Had a Fracture
Year % of Patients*
2007 20.4
2006 21.8
2005 20.1
2004 19.0
2003 18.0
Trends in osteoporosis management in women aged 67+ yrs who previously fractured

Risk Factorsfor Osteoporosis
or Fracture
h Conditions, Diseases and Medications That Cause or
Contribute to osteoporosis: (incomplete list)
Gastric bypass, premature ovarian failure,
athletic amenorrhea, prior fracture as adult
h Risk Factors for Falls
prior fall, muscle weakness, balance, gait,
dehydration, visual deficit

Learning Objectives:
1. Use NOF criteria for initiating treatment of postmenopausal osteoporosis
2. Review the FRAX calculator for use in decisions for treatment of osteoporosis
3. How to monitor effects of therapy based on pt. outcomes and response to treatment using BMD testing
4. Discuss the pros and cons of Vitamin D and Calcium, exercise
5. Review the FDA Approved medications for prevention and treatment

WHO FRAX™Risk factors
h Age or DOB
h Gender height weight (low BMI)
h Prior history of fracture (including morphometric
vertebral fracture)
h Parental history of hip fracture
h Current smoking
h Rheumatoid arthritis
How to find the FRAX TOOL www.shef.ac.uk/FRAX or google FRAX

WHO FRAX™Risk factors
h Oral steroids >5 mg/d of pred for > 3 months (ever)
h Alcohol intake (3 or more drinks/d)
h Secondary osteoporosis
h BMD femoral neck T score either gms/cm² or T-score
(machine make)

New NOF guidelines based upon the FRAX tool for estimating absolute fracture risk in
clinical practice
NOF’s Clinician’s Guide states that:h Postmenopausal women and men over 50 with
a T score of -2.5 or lower at the hip, spine, or prior hip or spine fracture should be treated.
h Based on absolute fracture risk calculation, patients with low bone mass (T-score between -1.0 and -2.5 at the femoral neck, total hip or spine) should be treated when:
0 10-year hip fracture probability ≥ 3%,0 10-year all major osteoporosis-related fracture
probability ≥20%, based on the U.S.-adapted WHO algorithm.

Caution!
h Cannot be used for premenopausal women or
h Cannot be used for men under 50 0 Little known about the relationship between BMD
and fracture risk: not the same in the young
Only applies to patients who have not previously received specific pharmacotherapy!
!

CLINICAL
HistoryRisk factors
Signs and symptoms
PhysicalHeight (stadiometer)
Kyphosis
ImagingBone mineral density (BMD) testing
FRAX™X-rays (LVA, IVA)
Laboratory tests

Clinical Evaluation
h Evaluate Risk Factors
h Evaluate risk of falling
h Measure Height (stadiometer)
h Look for kyphosis
h BMD testing

Clinical EvaluationLaboratory Testing
1. √ Vit D 25 status for osteomalacia
2. Malabsorption for celiac disease
3. SPEP
4. iPTH and ionized Ca+
5. 24 hr urine Ca+

Assess Risk Factors and Measure BMD if Patient Has Risk Factors
T-score between -1.0 and -2.5
10-year Probability of Hip Fracture >3% or
Probability of All Major Fractures
>20%
Hip or Vertebral Fractures
orT-score ≤-2.5 (Spine,
FN or Total Hip)
2008 NOF Guidelines: Treatment Initiation Post-menopausal Women And Men ≥50
http://www.nof.org
Other Fractures after
Age 50 (Excluding
Fingers, Toes and Face)
Secondary Causes with High
Fracture Risk*
*such as glucocorticoid use or total immobilization

Learning Objectives:
1. Use NOF criteria for initiating treatment of postmenopausal osteoporosis
2. Review the FRAX calculator for use in decisions for treatment of osteoporosis
3. How to monitor effects of therapy based on pt. outcomes and response to treatment using BMD testing
4. Discuss the pros and cons of Vitamin D and Calcium, exercise
5. Review the FDA Approved medications for prevention and treatment

Biochemical Markers Of Bone Turnover Released During Remodeling Process
i In general, baseline biochemical markers of bone turnover have not proven useful in selecting treatment options in individual patients
i The change in biochemical markers from baseline has shown only a loose correlation with the response to treatment—and feedback to patients has not increased persistence with therapy

T-score: comparison with average young adult value
h Used to diagnose osteoporosis and in calculating fracture risk
Z-score: comparison with age-matched values
h Used to determine if BMD is lower than expected for age
Interpretation of Bone Density Tests
Region BMD T-score Z-score L1 0.589 -3.1 -1.3 L2 0.658 -3.4 -1.4 L3 0.695 -3.5 -1.4 L4 0.725 -3.6 -1.4 L1-L4 0.673 -3.4 -1.4

Monitoring
Objectivesi Main objective of serial BMD measurements is to identify
patients with significant bone lossi Might improve adherence to treatment—but this has not been
formally studied
Endpointsi If BMD increases or stays the same—and the patient has not
fractured--no change in therapy is indicatedi If BMD has decreased beyond the least significant change
(“LSC”), the patient should be evaluated for noncompliance and for secondary causes of bone loss

Monitoring
Challenges
i Changes in BMD are relatively small compared to the precision error of the measurement
i Changes in BMD account for less than 50% of the effect of anti-resorptive therapy on fracture risk
i Proportion of non-responders not well known
i Non-adherence to therapy usually occurs early

Monitoring Change: Requirements
Measure a site that is likely to change
i Spine BMD changes more than the hip BMD
i Cannot use peripheral sites to monitor the response to therapy
Precise, reproducible tests
i Necessary to be able to detect relatively small--but clinically significant--changes in BMD

Requirements For Precise Serial DXA Scans
h General– Same specific densitometer (not
just the same type of densitometer)
h Spine– Same vertebral bodies– No new artifacts
h Hip– Same positioning– Same size and placement of
regions of interest

Most common reasons why BMDdoes not improve
h Vit D deficiency
h BMD monitoring done on different machines and
not comparable
h Exam technique incorrect (see lesser trochanter)
h Non-compliance

Region BMD T-score (g/cm²)
L1 0.589 -3.06 L2 0.658 -3.36 L3 0.695 -3.53 L4 0.725 -3.55 L1-L4 0.763 -3.40
Monitoring
To be statistically significant, the change must be larger than the LSC for the measurements at each lab (numbers below provide some guidance if lab’s values unknown)
i Spine 0.04 gm/cm2
i Total hip 0.05 gm/cm2
i Femoral neck 0.06 gm/cm2
Assess BMD change-- not percent change or change in
T-score

Timing Of Repeat Measurements Depends On Expected Changes In BMD
Approximate rate of loss in spine
(g/cm2/yr)
Time needed to see a significant
change(LSC = 0.04
gm/cm2)
Early menopause
0.02 2 years
>5 years after menopause 0.010-0.005 4-8 years
Starting glucocorticoids 0.06-0.02 6 months – 2 years

h ISCD Recommendations0 Repeat measurement at 1-2 years in spine
(preferred) or total hiph Medicare Policy1
0 Repeat measurement reimbursed after 23 months0 There are exceptions that allow measurement
earlier than 23 monthsh Long-Term Monitoring
0 No official guidelines: Once BMD is stable or improving, less frequent or no monitoring can be considered
Serial Bone Density Testing
1 Bone Mass Measurement Act. 1998

Monitoring Response To Treatment
Janet
i 70 year old female with osteoporosis on therapy for 2 years
i Serial bone density studies (same machine, proper analysis)
Baseline 2 Years
BMD g/cm2 BMD g/cm2
Lumbar spine 0.680 0.750
Total hip 0.682 0.693 +0.011
Change in g/cm2
+0.070
How do you interpret her response?
Spine LSC = 0.04 gm/cm2 Total hip LSC = 0.05 gm/cm2

Treatment Summary
h We have the tools to identify patients at risk; in FRAX®, bone mineral density (BMD), age and previous fractures in particular are strong, independent predictors of fracture risk
h Treatments significantly decrease fracture risk:
0 “Antiresorptive” therapy produces a modest BMD increase, yet decreases fracture risk—especially in the spine—much faster and to a larger extent than predicted by the relatively small change in BMD. This implies an important improvement in bone “quality”
0 Anabolic therapy with teriparatide increases BMD more than antiresorptive treatment, but it is not yet obvious that fracture protection is greater

Objective of Intervention
The most important clinical objective is the
prevention of fractures—both vertebral and
non-vertebral fractures
Changes in surrogate markers--bone mineral
density (BMD) and biochemical markers of bone
turnover--are “necessary” but are not “sufficient”

Learning Objectives:
1. Use NOF criteria for initiating treatment of postmenopausal osteoporosis
2. Review the FRAX calculator for use in decisions for treatment of osteoporosis
3. How to monitor effects of therapy based on pt. outcomes and response to treatment using BMD testing
4. Discuss the pros and cons of Vitamin D and Calcium, exercise
5. Review the FDA Approved medications for prevention and treatment

Non-Pharmacologic Management:Prevention and Treatment
h Smoking cessation
h Calcium: 1,200 mg/day total intake1,2
0 Most need supplement
h Vitamin D: 800 IU/day to 1,000 IU/day2
0 2,000 IU/day safe3
h Exercise
1 NIH Consensus Development Panel on Optimal Calcium Intake. www.consensus.nih.gov;2 NOF Clinician’s Guide to Prevention and Treatment of Osteoporosis 2008. www.nof.org; 3 FORE. www.fore.org/patients/eating_right.html.

Non-Pharmacological Options
h Taken as a whole, non-pharmacological options seem to be relatively inexpensive, and modestly effective
h Exercise in particular has other health benefits, although the same is likely to be true for diet optimization
h Optimization of the diet, exercise and fall prevention should be viewed as important adjuncts to the treatment of osteoporotic patients

Beneficial Effects of Calcium and Vitamin D
Calcium and vitamin D slow or prevent bone loss; necessary but not sufficient part of every regimen1
Vitamin D • 26% reduction in hip and nonvertebral fractures with dose of 700-800
IU/day (meta-analysis)2
• Improves balance and muscle strength and reduces falls3
• Higher 25-OH vitamin D levels associated with4:• Lower risk of prostate, breast, and colon cancer• Lower risk of some autoimmune diseases• Improved immune function
1 Dawson Hughes B, et al. Osteoporos Int. 2005 Jul;16(7):713-62 Bischoff-Ferrari HA, et al. JAMA. 2005;293(18):2257-643 Bischoff-Ferrari HA, et al. JAMA. 2004;291(16):1999-20064 Holick MF. N Engl J Med. 2007;357(3):266-81

Exercise
What exercises are beneficial?• Weight-bearing• Muscle-strengthening
• What benefit might one expect from exercise?• Small (1% to 2%) effect on adult BMD• Maximum effect seen in growing bone• Reduces the loss of muscle mass• May reduce risk of falls by improving strength and
balance • Regular walking shown to decrease risk of hip fractures1
Centers for Disease Control and Prevention. Injury Center. www.cdc.gov/injury.

Learning Objectives:
1. Use NOF criteria for initiating treatment of postmenopausal osteoporosis
2. Review the FRAX calculator for use in decisions for treatment of osteoporosis
3. How to monitor effects of therapy based on pt. outcomes and response to treatment using BMD testing
4. Discuss the pros and cons of Vitamin D and Calcium, exercise
5. Review the FDA Approved medications for prevention and treatment

FDA-Approved Therapeutic Options in the USA
PreventionStops bone loss
TreatmentReduces vertebral fractures
Estrogen
AlendronateRisedronateIbandronate
Zoledronic acidRaloxifene
Calcitonin
PTH (teriparatide)
Denosumab

Resorption = Formation
Normal Coupling of Bone Remodeling
i Most treatment agents (bisphosphonates, SERMs, calcitonin, estrogen) act primarily on the left side of the equation—to decrease bone resorption
i A decrease in resorption is followed by a decrease in formation—and BMD improvement tends to “plateau” after several years
i Only teriparatide acts on the right side of the equation—to stimulate formation

Antiresorptive Treatment: Summary
i Antiresorptive treatment decreases fracture risk more rapidly and to a larger extent than one would predict from the relatively small changes in BMD
Fracture protection can be observed in the absence of a significant change in BMD
i Fracture protection persists even when the BMD reaches a plateau
BMD stability does not mean “non-response”
i Fracture reduction is most conspicuous in older patients with prevalent vertebral fractures

+ documented in randomized, controlled trial; – effect not documented§ effect documented only in a post hoc analysis of a high-risk sub-group (femoral neck T score < -3) and in a meta-analysis of clinical trials (Harris ST, et al. Curr Med Res Opin 2008;24:237-245)
Antiresorptive Agents: Clinical Trial ResultsTrials of Different Agents Cannot Be Compared Directly
Agent Spine Non-spine Hip
Estrogen + + +
Raloxifene + - -
Calcitonin + - -
Alendronate + + +
Risedronate + + +
Ibandronate + § -
Denosumab + + +
Zoledronic acid + + +
Effect on fracture risk

Estrogen Treatment (ET)• Several approved oral and transdermal preparations• Approved for prevention (not treatment)• Treats symptoms of estrogen deficiency• Skeletal effects:
– Decrease in biochemical markers of 50-60%
– 2-year BMD increase of 4-6% at hip and spine
– Decreased incidence of vertebral and hip fractures (34%) after 5 years in the WHI
– Effects in women with osteoporosis have not been evaluated in randomized controlled trials
• Concern about adverse effects• Long-term use not recommended
Writing Group for the WHI. JAMA 2002;288:321

Calcitonin
h Calcitonin (200 units daily by nasal spray)
h Approved for treatment (not prevention)
h Skeletal effects:
0 Decrease in biochemical markers of 20%
0 Small effect (1-2%) on bone density in spine
0 Reduced incidence of vertebral fractures (36%) in women with pre-existing vertebral fractures
0 No effect on non-vertebral or hip fractures has been observed
h Adverse effects: nasal stuffiness
Chesnut CH, et al. Am J Med 2000;109:267-276

Raloxifene• Raloxifene (60 mg daily)• Approved for both prevention and treatment• Skeletal effects:
– Decrease in biochemical markers of 30%
– 3-year BMD increases of 2-3% at hip and spine
– Decreased incidence of vertebral fractures (30-50%) in women with pre-existing vertebral fractures or low bone density. No effect on non-vertebral or hip fractures has been observed.
• Adverse effects: hot flashes, venous thrombosis, leg cramps
• Extra-skeletal effects: reduction in invasive breast cancer-STAR TRIAL
Ettinger B, et al. JAMA 1999;282:637-645

BisphosphonatesAlendronate, Risedronate, Ibandronate and Zoledronic Acid
A number of different bisphosphonates are now available for the prevention and treatment of osteoporosis—in daily oral, intermittent oral and intermittent parenteral formulations:
h Alendronate 10 mg daily or 70 mg weekly for treatment, 5 mg daily or 35 mg weekly for prevention
h Risedronate 5 mg daily or 35 mg weekly; 75 mg on two consecutive days once each month, 150 mg monthly
h Ibandronate 150 mg monthly by mouth; 3 mg IV over 15-30 seconds every 3 months
h Zoledronic acid 5 mg by infusion over a minimum of 15 minutes every year

h Increased bone density in the spine by 5-8% and at the hip by 3-6% after 3 years
h Reduced incidence of vertebral fractures by 40-70%
h Alendronate, risedronate and zoledronic acid reduced non-vertebral fractures (25-40%), including hip fractures (40-60%), in women with osteoporosis
h Ibandronate: overall, no effect observed on non-vertebral or hip fractures. In a post-hoc analysis, non-vertebral fracture reduction was seen in a high-risk subgroup with a baseline femoral neck T-score less than -3.0
Bisphosphonates: Effects Alendronate, Risedronate, Ibandronate and Zoledronic
Acid

hContraindications/Warnings/Precautions
0 Hypocalcemia
0 Creatinine clearance less than 30 cc/min (< 35 cc/min for zoledronic acid)
0 For oral dosing: Esophageal stricture or impaired esophageal motility (alendronate); inability to stand or sit for at least 30 minutes (alendronate/risedronate) or 60 minutes (ibandronate)
Notes: UGI symptoms are not a contraindicationUse in pregnancy: Class C
Bisphosphonates

h “Class warning” regarding UGI symptoms (no increase in UGI complaints in randomized controlled trials)
h “Class warning” regarding infrequent bone, joint and/or muscle pain
h “Class warning” regarding osteonecrosis of the jaw (“ONJ”)
h Influenza-like symptoms may occur after first monthly oral dose or IV injection
h Recent concern about so-called “atypical fractures” after long-term therapy; the magnitude of the problem is currently unclear
Bisphosphonates: Side Effects

•There has been a theoretical concern that “oversuppression” of bone remodeling could impair the repair of microdamage—and increase the risk of atypical fractures
•There are several small series of cases:
- often fractures of femoral diaphysis- transverse rather than spiral
fracture- often on other drugs, especially
steroids or estrogen- some with stress reaction or stress
fracture and prodromal pain syndrome
•There is no consensus about the frequency with which these atypical fractures might occur
1. Goh S-K, et al. J Bone Joint Surg Br. 2007;89:349-3532. Imai K, et al. J Bone Miner Metab. 2007;25:333-3363. Neviaser AS, et al. J Orthop Trauma. 2008;22:346-3504. Odvina C, et al. J Clin Endo Metab. 2005;90:1294-1301
Atypical Fractures

ASBMR Task Force Report on Atypical Femoral Fractures 2010 Incidence
Hip fracture occurrence in US =1,000 to 2,280/100,000 patient-yrs
Atypical femoral fractures with BPs ranged from :
2 to 78 per 100,000 patient-years with 2yr and 8yr h/o BPs respectively10-29 vertebral fx can be avoided per each atypical fx
For every 100 hip fractures prevented, 1 case of atypical subtrochanteric fracture
Reported number in 2011 is about 300
Prevalence not higher in Cancer Rxed bisphosphonate patients
Some patients report prodromal pain in thigh
Shane E and Burr D, Co-Chairs. ASBMR Task Force on Atypical Femoral Fractures. Presented October 26, 2010. 2010 ASBMR, Toronto, Canada.

Osteoporosis Therapy: rhPTH [1-34] Teriparatide
rhPTH [1-34] (20 units daily subcutaneously)
Indication: treatment of men and postmenopausal women with osteoporosis who are at high risk for fractures
Effects1
h Increased bone density in spine by 9% and hip by 3% vs placebo over 18 months
h Reduced incidence of vertebral fractures (65%) and non-vertebral fragility fractures (53%) in women with pre-existing vertebral fractures
h Studies too small to evaluate effect on hip fractures
1 Neer RM, et al. N Engl J Med. 2001;344:1434-41

Denosumab
Denosumab 60 mg SC q 6 months
Indications: Treatment of postmenopausal women at high risk for osteoporotic fracture
Skeletal effects¹
vertebral fracture reduction 68% at 3 years
Hip fracture reduction 40% at 3 years in women with osteoporosis
non-vertebral fracture reduction 20% at 3 years in women with
osteoporosis
• Adverse reactions:
• No ONJ seen in phase III pivotal study
• No atypical fractures seen out to 5 yrs
• Higher incidence of cellulitis and skin reactions
1. NEJM Cummings SR, San Martin J, McClung MR, et al. 2009;361:756-765

Denosumab
BMD continues to increase out to 5 yrs hip and
lumbar spine
Mechanism of action:
Inhibits Rank Ligand
thereby decreasing the function, formation,
and survival of osteoclasts
Antiresorptive but different MOA than
bisphosphonates

Novel Therapies
h SERMs (“Selective Estrogen Receptor Modulators”) (also known as “Estrogen Agonists Antagonists”): lasofoxifene, bazedoxifene, arzoxifene
h Anti-sclerostin antibody (Osteocyte target phase II)
h Cathepsin K inhibitor – odanacatib
h Cyclic analog of PTH (1-31)
h Calcium receptor antagonist – “calcilytic”

Safe and effective therapies are availableAntiresorptive agents
i Prevent bone loss and preserve architecturei Improve quality of bonei Reduce the risk of vertebral fractures (all agents)i Alendronate, risedronate and zoledronic acid proven to reduce the
risk of nonvertebral and hip fracturesi Denosumab reduces the risk of spine, hip, and nonvertebral
fractures
Anabolic agent: rhPTH [1-34] (teriparatide) i Increases bone density and sizei Improves quality of bonei Reduces the risk of vertebral and nonvertebral fractures; no hip
fracture data
Patient factors determine the most appropriate drug to use
Treatment: Summary

1 AWP (Average Wholesale Price) varies by region and distributor* Medi-Span Drug Data. Price Rx® Prescription drug database (Accessed 30 October 2009) Red Book: Pharmacy’s Fundamental Reference. Thomson Medical Economics: Montvale, NJ. 2007.
Drugs to Treat Osteoporosis
Cost per Effect on Fracture Risk
Agent year1 Vertebral Nonvert
HipRaloxifene $976* -- --
Calcitonin $1,517* -- --
Brand alendronate $1,103 Generic alendronate $108
Risedronate $1,110
Ibandronate (oral) $1,024 -- --Ibandronate (IV) $1,938
Zoledronic acid $1,249 Teriparatide $9,786 --Denosumab $1800
: antifracture efficacy proven in clinical trial --: antifracture efficacy not proven in clinical trial

THANK YOU
Helpful online resources
1. National Osteoporosis Foundation:
http://www.nof.org/professionals/Clinicians_Guide.htm
2. International Society of Clinical Densitometry:
http://www.iscd.org/
3. FRAX calculator: http://www.shef.ac.uk/FRAX/
Stay tuned for case presentations