Embed Size (px)
Citation preview
Osteoporosis Treatment Update:Can we Take a Holiday?
Robin Cornell Creamer, DO, FAAPMedical Director, AdventHealth Family Medicine Winter Park, Fl
Disclosure Statement
It is the policy of the AAFP that all individuals in a position to control content disclose any relationships with commercial interests upon nomination/invitation of participation. Disclosure documents are reviewed for potential conflicts of interest. If conflicts are identified, they are resolved prior to confirmation of participation. Only participants who have no conflict of interest or who agree to an identified resolution process prior to their participation were involved in this CME activity.
All individuals in a position to control content for this session have indicated they have no relevant financial relationships to disclose.
Learning Objectives1. Evaluate elderly patients or patients at risk for low bone
mass/osteoporosis using the FRAX® algorithm and consider the impact of fracture risk scores on patient management.
2. Advise patients on appropriate prophylactic strategies for patients with low bone mass/osteoporosis.
3. Compare and contrast management with RANKL inhibitor vs bisphosphonates; and the pros and cons between various bisphosphonates.
4. Determine the risks and benefits of maintaining bisphosphonate treatment for greater than 5 years.
Osteoporosis Diagnosis and Treatment Guidelines and Educational Resources
AACE/ACE (American Assoc Clinical Endo) May 2020 ACP (American College Physicians) endorsed by AAFP: May 2017 NOF (National Osteoporosis Foundation) Clinicians Guide 2014 FRAX: http://www.shef.ac.uk/FRAX or APP University New Mexico. Telementoring Bone Health TeleECHO Clinic.
http://www.ofnm.org/project-echo Mayo Clinic Shared Decision-Making National Resource Center
https://osteoporosisdecisionaid.mayoclinic.org
Complete references in bibliography
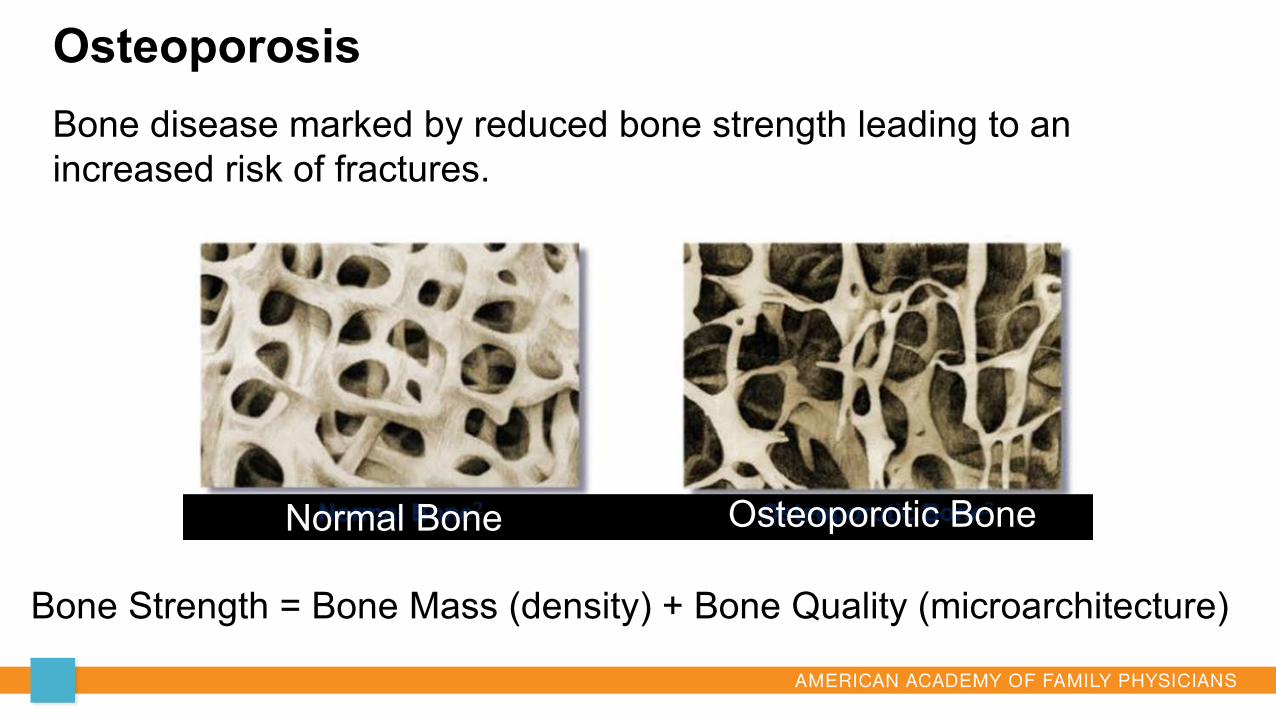
OsteoporosisBone disease marked by reduced bone strength leading to an increased risk of fractures.
Bone Strength = Bone Mass (density) + Bone Quality (microarchitecture)
Normal Bone Osteoporotic Bone
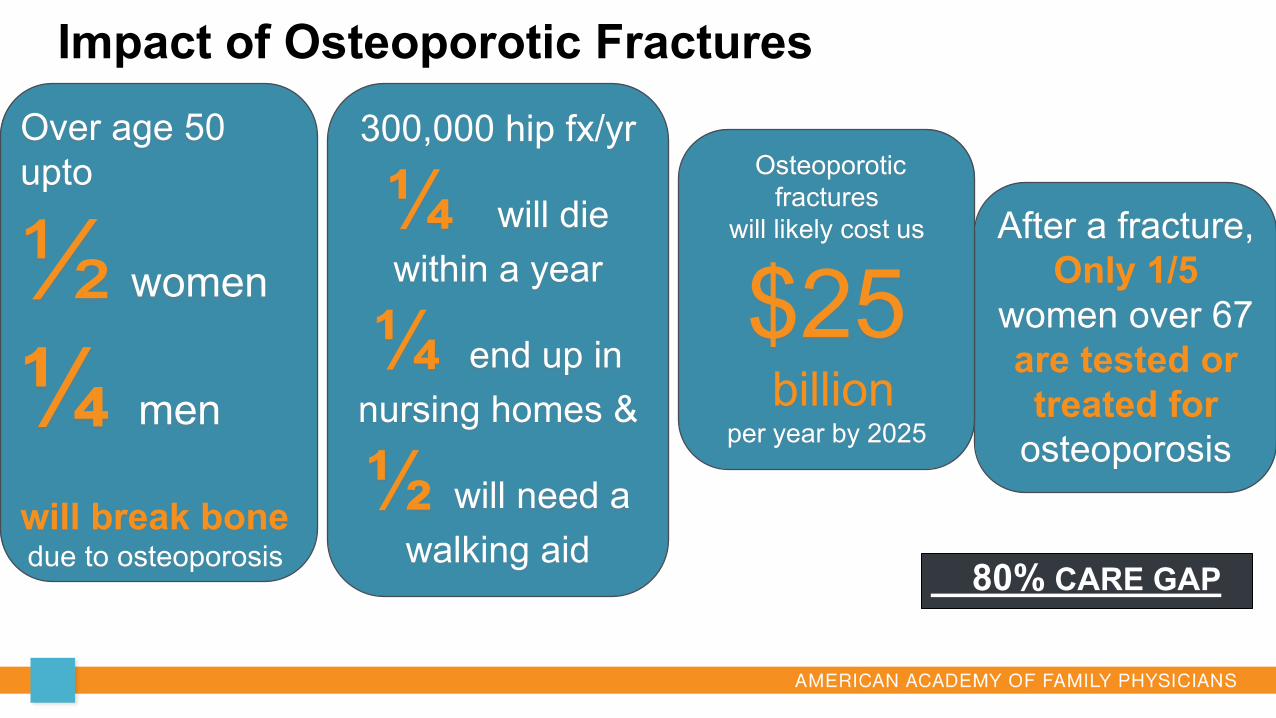
Impact of Osteoporotic Fractures
80% CARE GAP
Over age 50 upto
½ women
¼ men
will break bonedue to osteoporosis
After a fracture, Only 1/5
women over 67are tested or treated for
osteoporosis
Osteoporotic fractures
will likely cost us
$25billion
per year by 2025
300,000 hip fx/yr
¼ will die within a year
¼ end up in nursing homes &
½ will need a walking aid
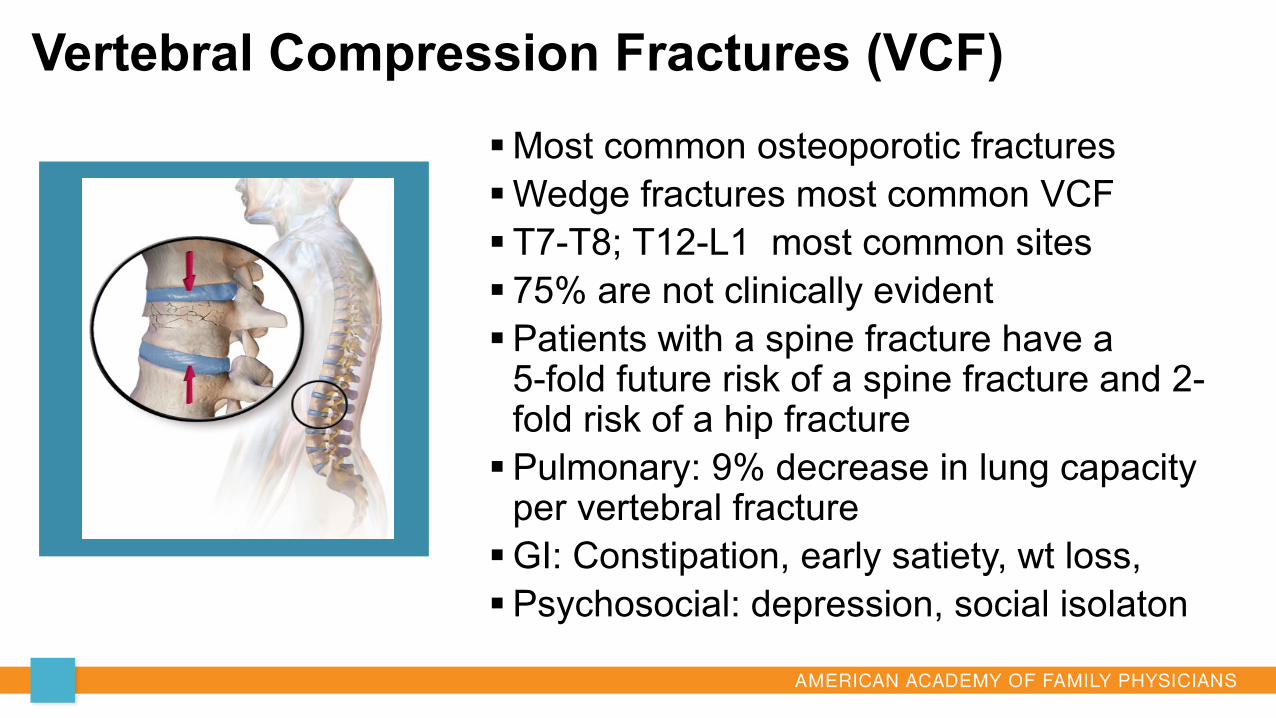
Vertebral Compression Fractures (VCF)Most common osteoporotic fracturesWedge fractures most common VCF T7-T8; T12-L1 most common sites 75% are not clinically evidentPatients with a spine fracture have a
5-fold future risk of a spine fracture and 2-fold risk of a hip fracturePulmonary: 9% decrease in lung capacity
per vertebral fractureGI: Constipation, early satiety, wt loss,Psychosocial: depression, social isolaton
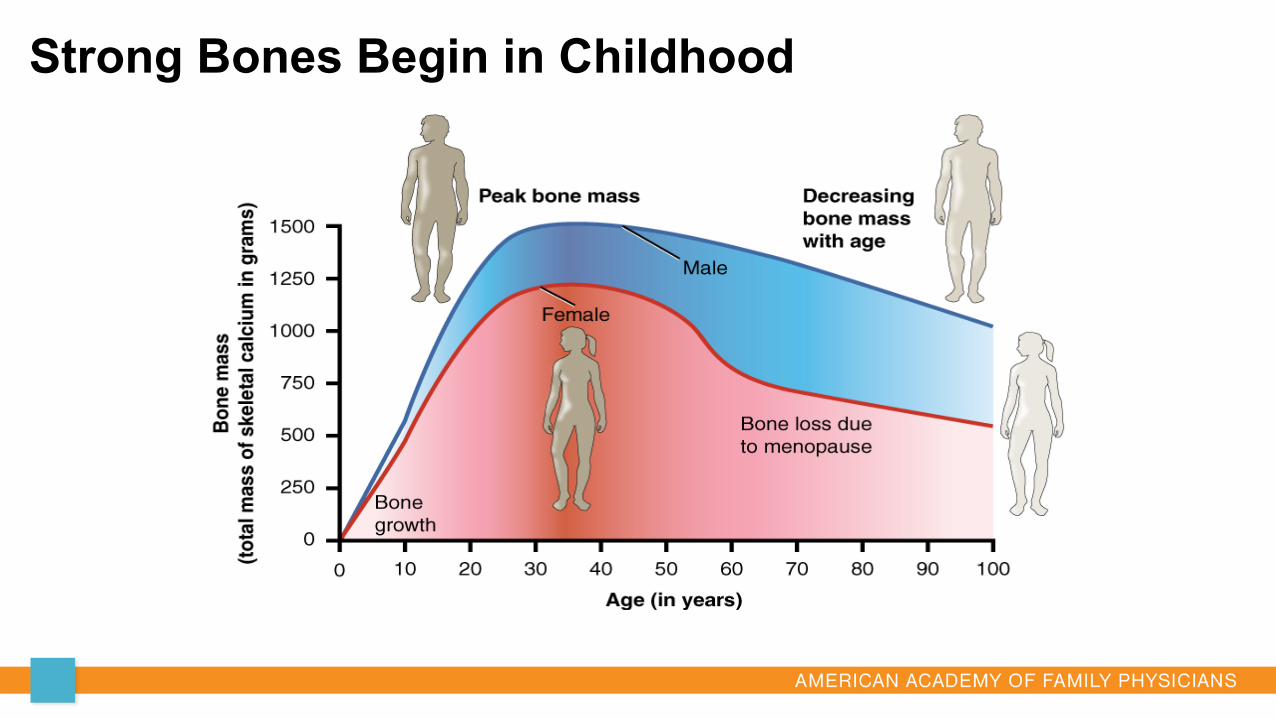
Strong Bones Begin in Childhood
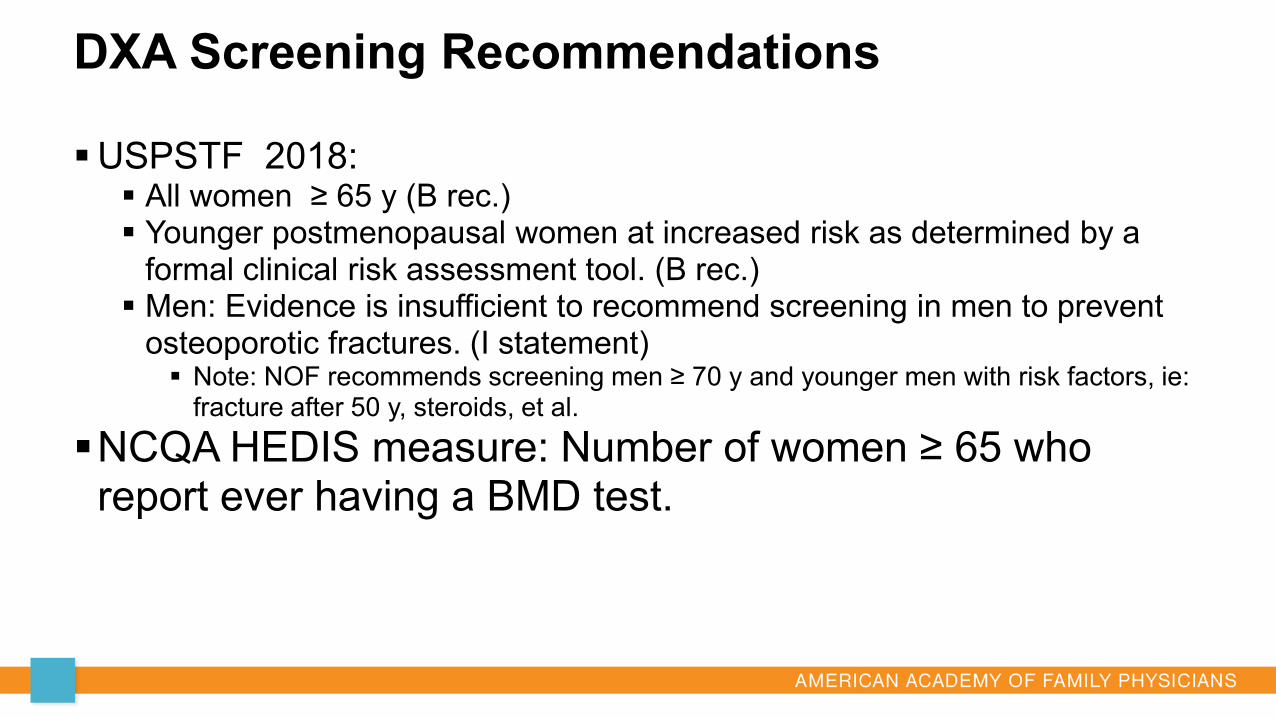
DXA Screening Recommendations
USPSTF 2018: All women ≥ 65 y (B rec.) Younger postmenopausal women at increased risk as determined by a
formal clinical risk assessment tool. (B rec.) Men: Evidence is insufficient to recommend screening in men to prevent
osteoporotic fractures. (I statement) Note: NOF recommends screening men ≥ 70 y and younger men with risk factors, ie:
fracture after 50 y, steroids, et al.
NCQA HEDIS measure: Number of women ≥ 65 who report ever having a BMD test.
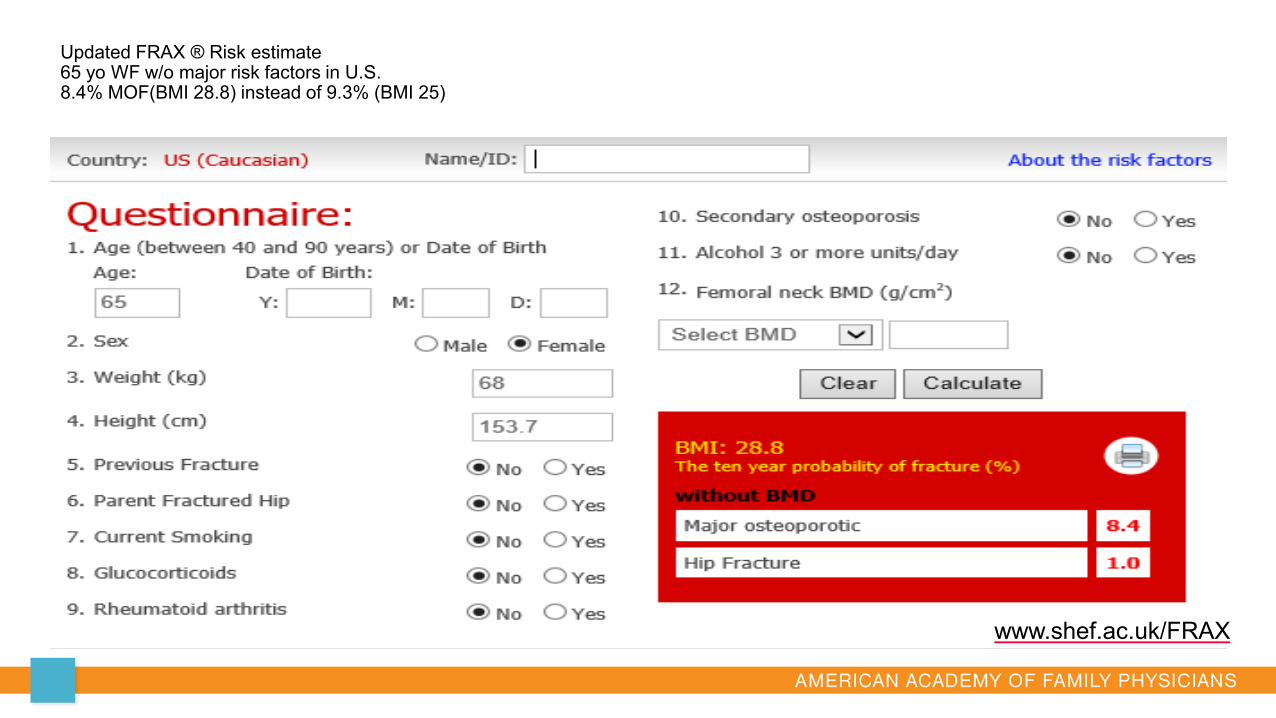
www.shef.ac.uk/FRAX
Updated FRAX ® Risk estimate65 yo WF w/o major risk factors in U.S.8.4% MOF(BMI 28.8) instead of 9.3% (BMI 25)
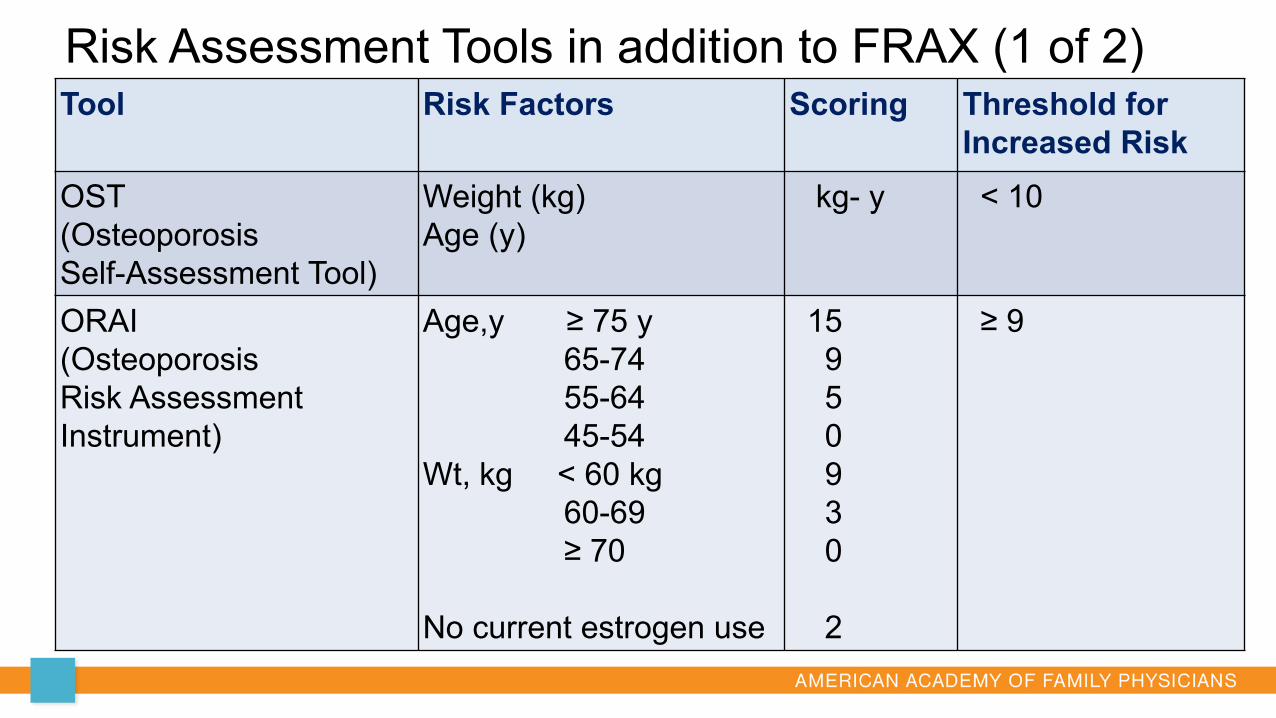
Risk Assessment Tools in addition to FRAX (1 of 2)Tool Risk Factors Scoring Threshold for
Increased RiskOST(OsteoporosisSelf-Assessment Tool)
Weight (kg)Age (y)
kg- y < 10
ORAI(OsteoporosisRisk Assessment Instrument)
Age,y ≥ 75 y 65-7455-6445-54
Wt, kg < 60 kg 60-69≥ 70
No current estrogen use
15950930
2
≥ 9
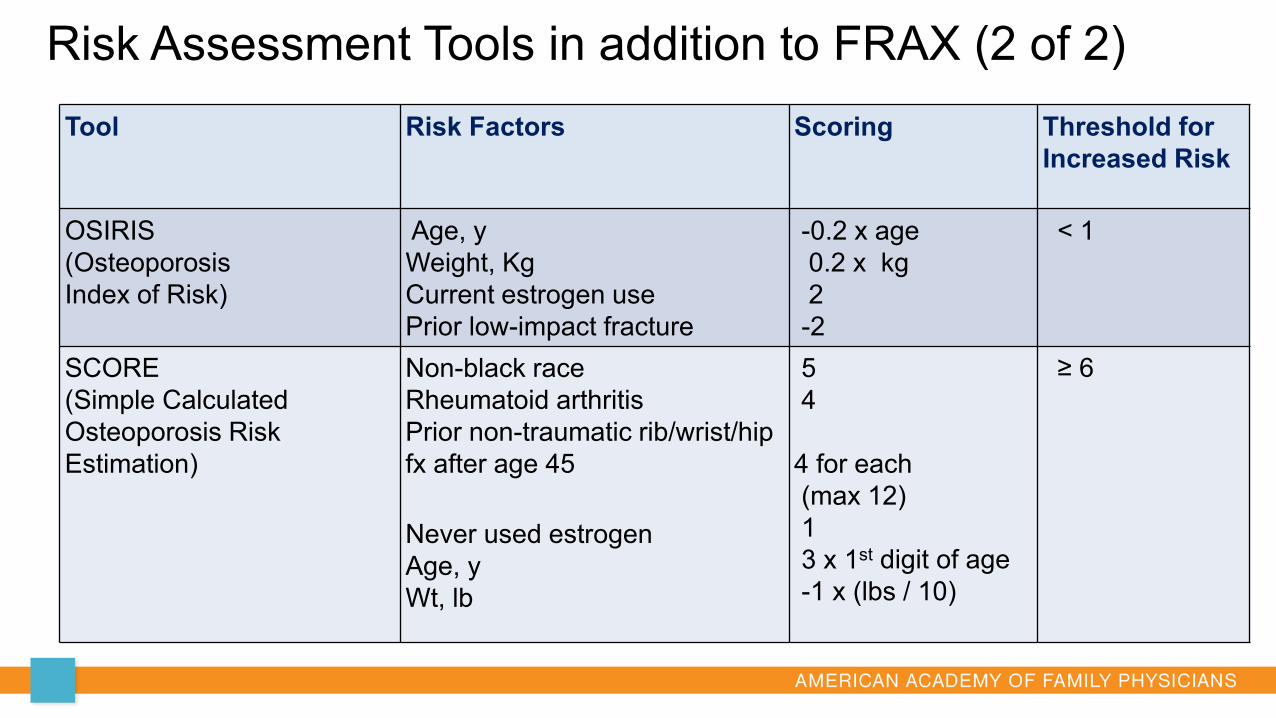
Risk Assessment Tools in addition to FRAX (2 of 2)Tool Risk Factors Scoring Threshold for
Increased Risk
OSIRIS(Osteoporosis Index of Risk)
Age, yWeight, KgCurrent estrogen usePrior low-impact fracture
-0.2 x age0.2 x kg2-2
< 1
SCORE(Simple CalculatedOsteoporosis Risk Estimation)
Non-black raceRheumatoid arthritisPrior non-traumatic rib/wrist/hip fx after age 45
Never used estrogenAge, yWt, lb
54
4 for each (max 12)13 x 1st digit of age-1 x (lbs / 10)
≥ 6
AES Question
In which of the examples below is DXA testing not indicated?
A. 66 yo male with history a non-traumatic fractureB. 75 yo female with normal DXA scan 2 yrs ago, without risk
factors for osteoporosis.C. 80 yo female who has been on oral bisphosphonate for 5
yrs. D. 90 yo female who has not had a baseline DXA scan
Question 1
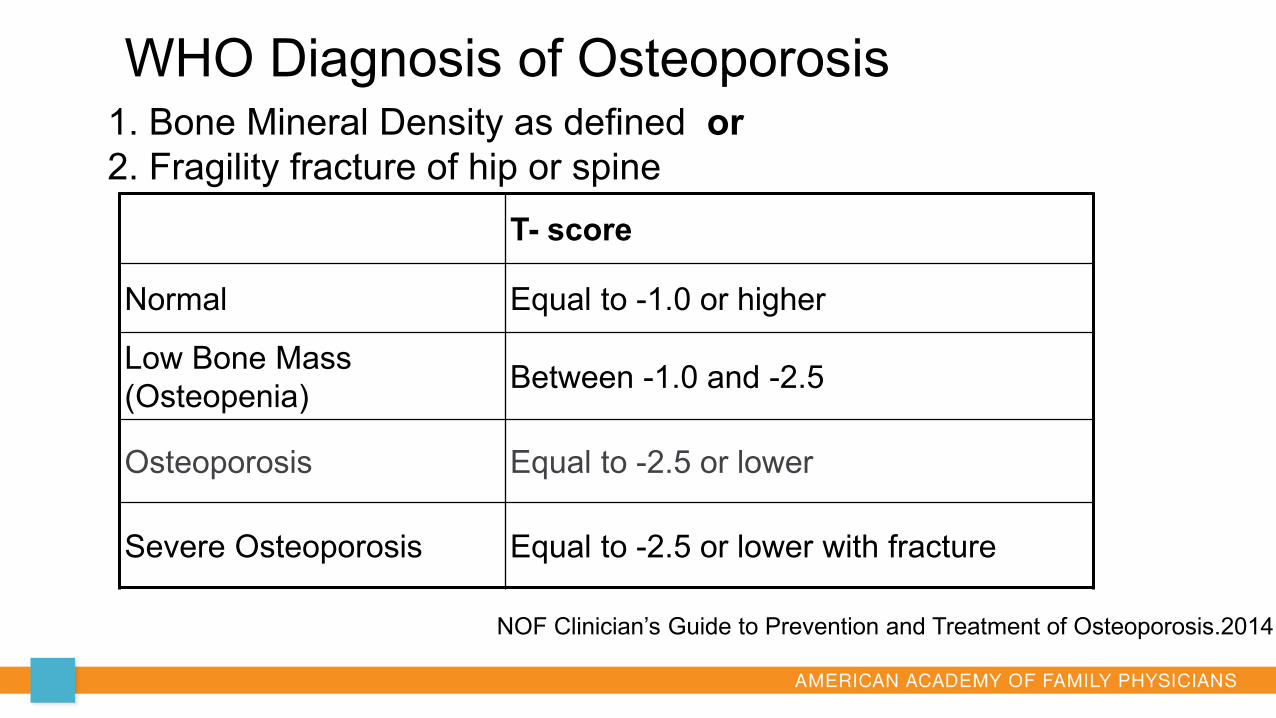
WHO Diagnosis of Osteoporosis
T- score
Normal Equal to -1.0 or higher
Low Bone Mass (Osteopenia) Between -1.0 and -2.5
Osteoporosis Equal to -2.5 or lower
Severe Osteoporosis Equal to -2.5 or lower with fracture
1. Bone Mineral Density as defined or2. Fragility fracture of hip or spine
NOF Clinician’s Guide to Prevention and Treatment of Osteoporosis.2014
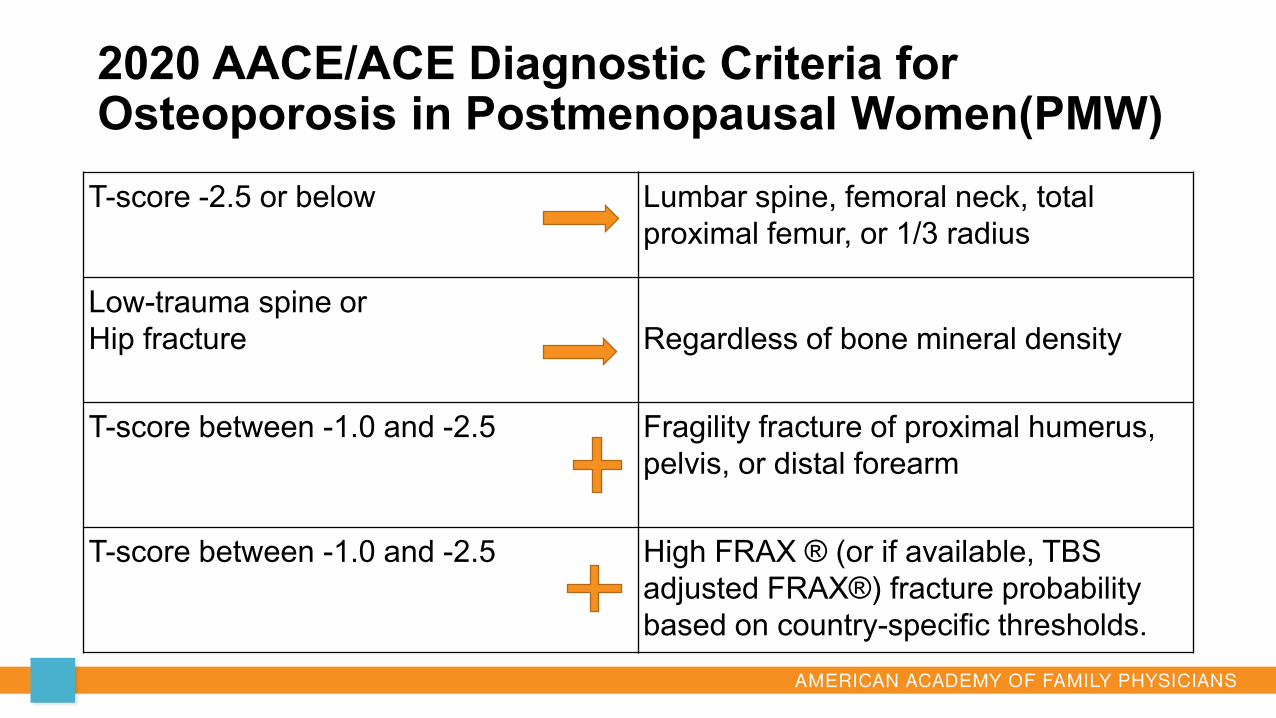
T-score -2.5 or below Lumbar spine, femoral neck, total proximal femur, or 1/3 radius
Low-trauma spine orHip fracture Regardless of bone mineral density
T-score between -1.0 and -2.5 Fragility fracture of proximal humerus, pelvis, or distal forearm
T-score between -1.0 and -2.5 High FRAX ® (or if available, TBS adjusted FRAX®) fracture probability based on country-specific thresholds.
2020 AACE/ACE Diagnostic Criteria for Osteoporosis in Postmenopausal Women(PMW)
FRAX adjusted with Trabecular Bone Score (TBS)FDA approved in 2012, TBS is a Textural index: DXA software
that extracts bone texture information from an AP spine DXA scan imageShown to be related to bone microarchitecture and fracture riskProvides information independent of BMDCannot diagnose osteoporosisCan be used to improve fracture risk assessment
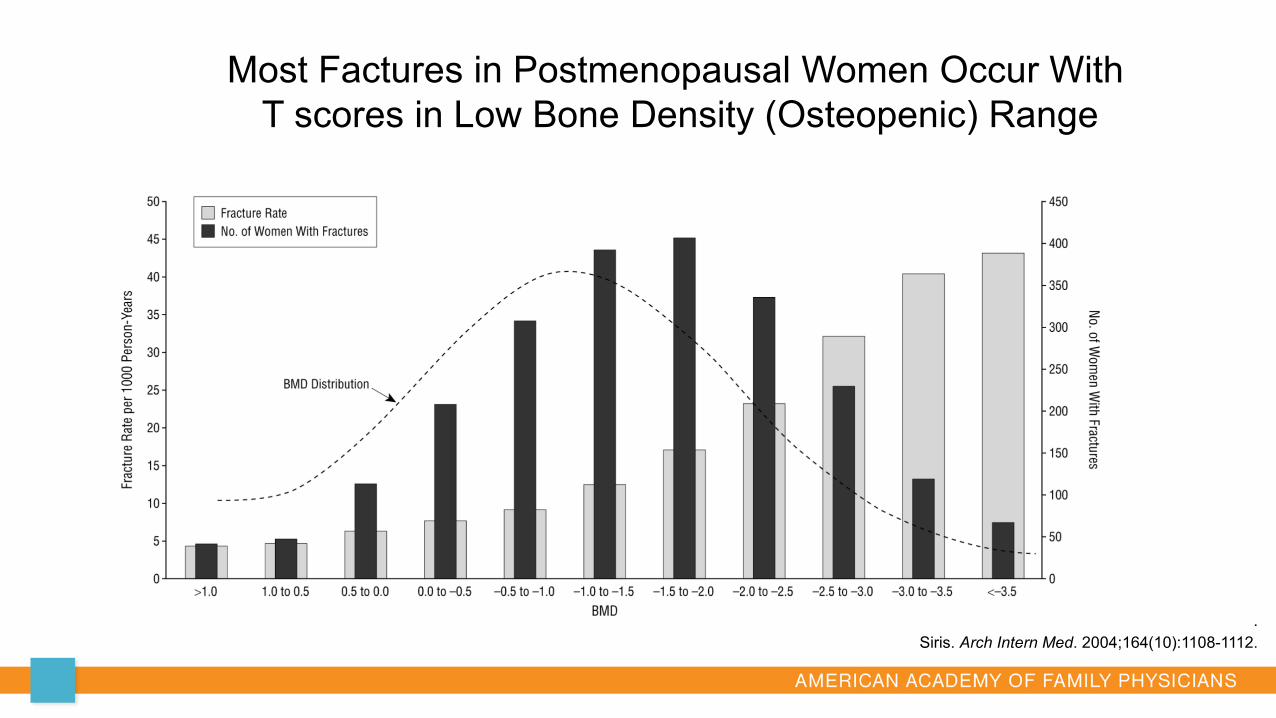
.Siris. Arch Intern Med. 2004;164(10):1108-1112.
Most Factures in Postmenopausal Women Occur WithT scores in Low Bone Density (Osteopenic) Range
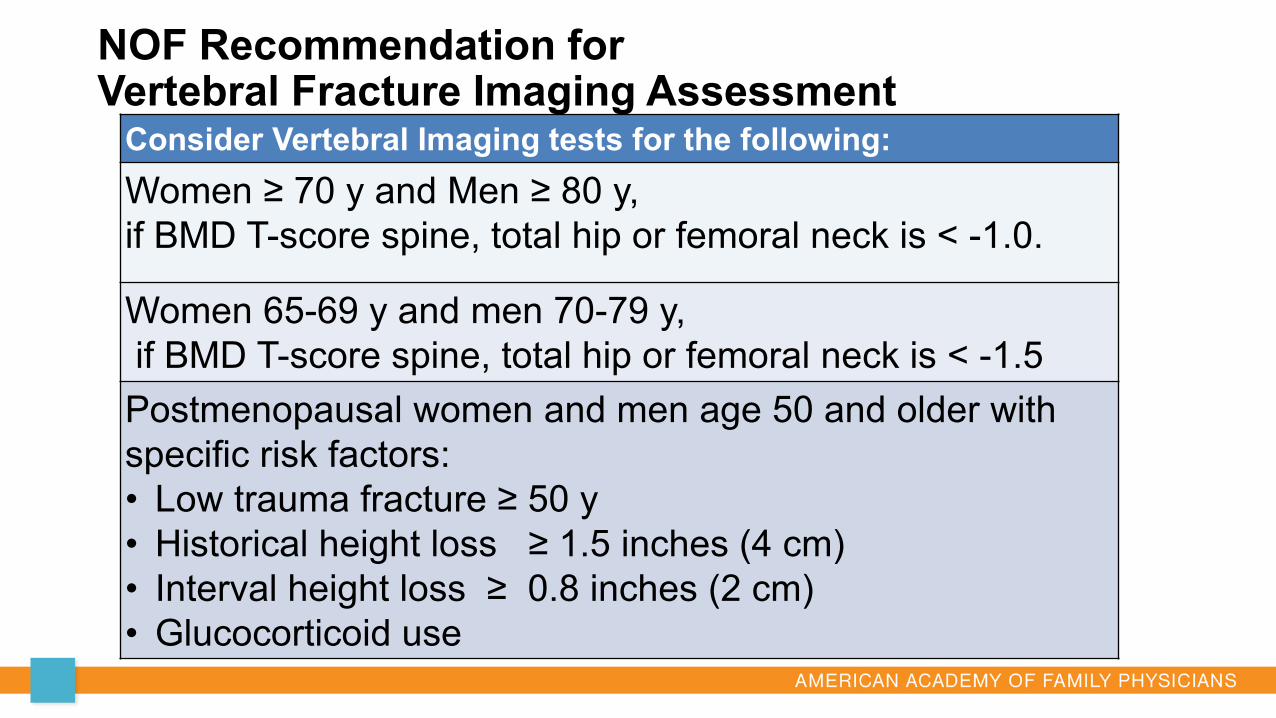
NOF Recommendation for Vertebral Fracture Imaging Assessment
Consider Vertebral Imaging tests for the following:Women ≥ 70 y and Men ≥ 80 y, if BMD T-score spine, total hip or femoral neck is < -1.0.
Women 65-69 y and men 70-79 y,if BMD T-score spine, total hip or femoral neck is < -1.5
Postmenopausal women and men age 50 and older with specific risk factors: • Low trauma fracture ≥ 50 y• Historical height loss ≥ 1.5 inches (4 cm)• Interval height loss ≥ 0.8 inches (2 cm)• Glucocorticoid use
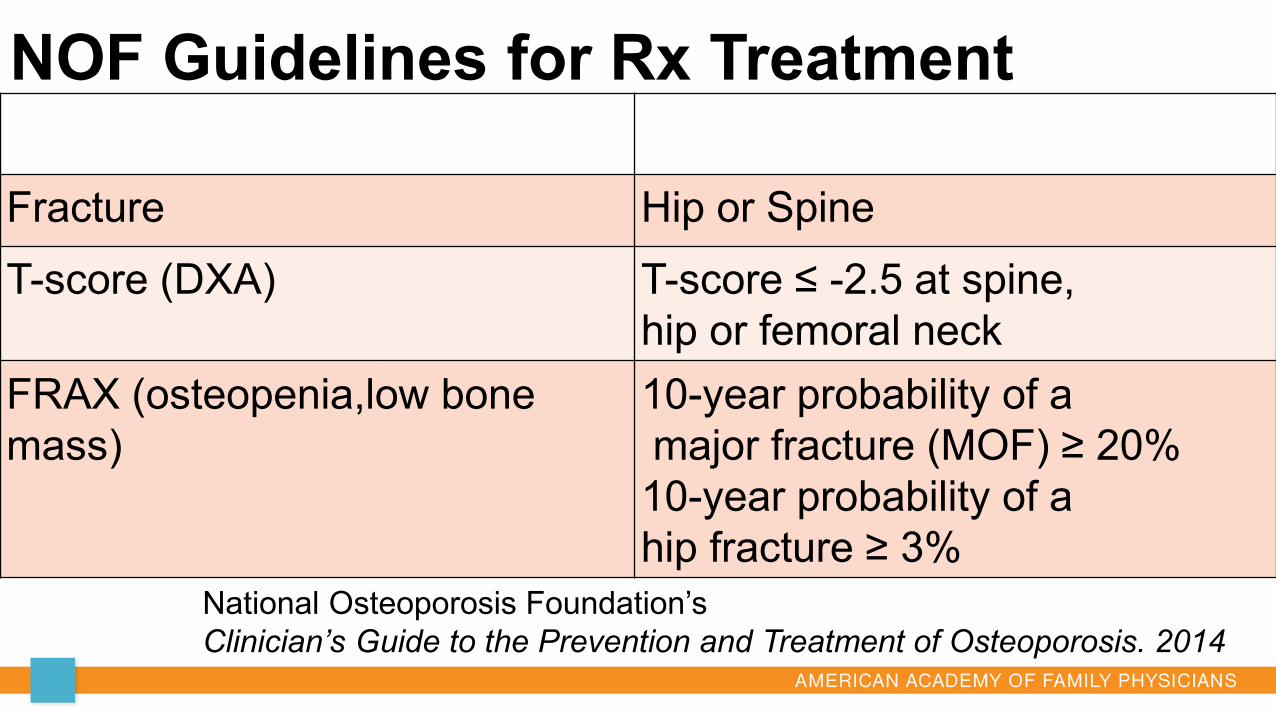
NOF Guidelines for Rx TreatmentFactor Description
Fracture Hip or SpineT-score (DXA) T-score ≤ -2.5 at spine,
hip or femoral neckFRAX (osteopenia,low bone mass)
10-year probability of amajor fracture (MOF) ≥ 20%10-year probability of a hip fracture ≥ 3%
National Osteoporosis Foundation’sClinician’s Guide to the Prevention and Treatment of Osteoporosis. 2014
Most common undiagnosed disorders of bone and mineral metabolismHypercalciuriaMalabsorption of calciumHyperparathyroidismVitamin D DeficiencyHyperthyroidismCushing’s disease
Labs to Consider for Secondary Causes
Chemistry (calcium,renal, phosphorus) Liver function testsCBC TSH, iPTH 25(OH)Vitamin D Testosterone younger men 24-hour urine calcium, Na, creatinine
Selected cases:SPEP/UPEPCeliac disease-(tTG) Iron and ferritinHomocysteine TryptaseProlactinBone turnover markers
Advise Universal Recommendations for Bone Health Regardless of Bone DensityAdvise adequate dietary calcium intake, supplement if diet is
insufficient Advise adequate Vitamin D intake, supplement if diet is
insufficientSmoking cessation. Limit alcohol and caffeine consumptionRecommend exercise program for strength, posture and
balance Fall Prevention
AES Question
Which of the following is true?
A. Advise patients with osteoporosis to consume more calcium than patients with normal bone density.
B. Advise patients with osteoporosis to consume more vitamin D than patients with normal bone density.
C. Advise patients with osteoporosis to avoid spinal forward flexion exercises.
D. Advise patients with osteoporosis to avoid spinal extension exercises
Question 2
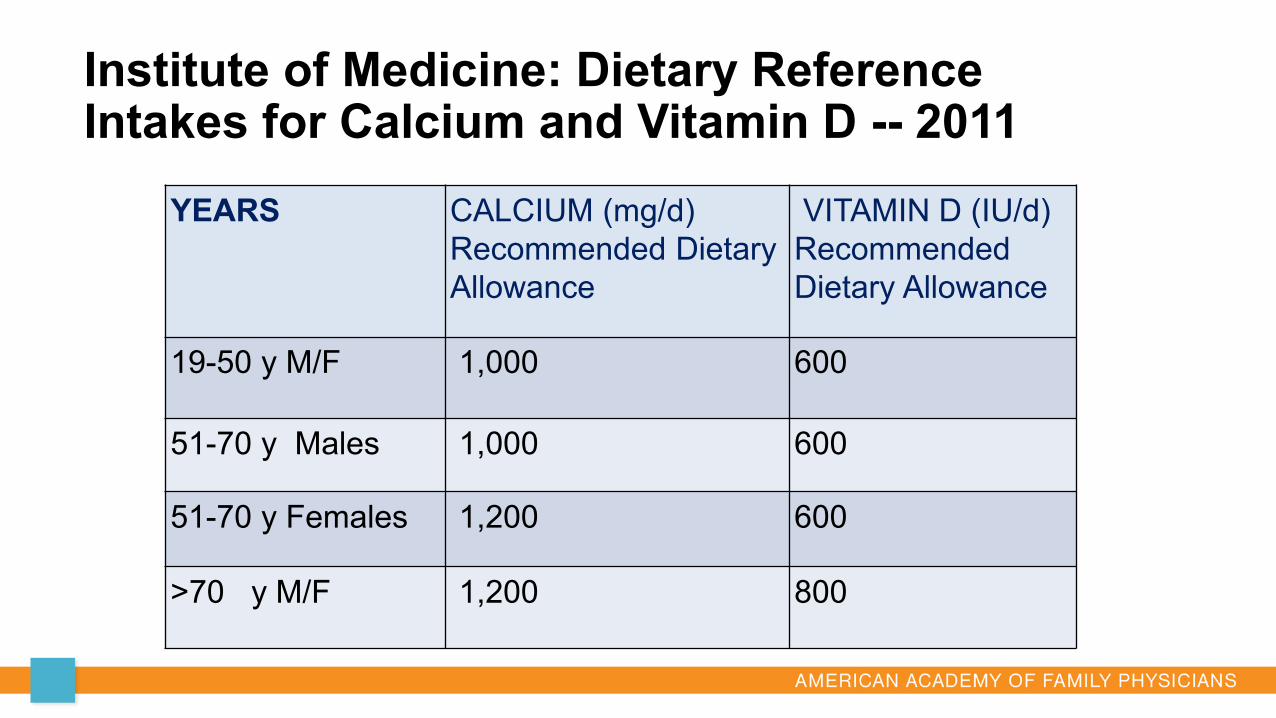
Institute of Medicine: Dietary Reference Intakes for Calcium and Vitamin D -- 2011
YEARS CALCIUM (mg/d)Recommended Dietary Allowance
VITAMIN D (IU/d)Recommended Dietary Allowance
19-50 y M/F 1,000 600
51-70 y Males 1,000 600
51-70 y Females 1,200 600
>70 y M/F 1,200 800
Vitamin D replenishment and Supplementation
If serum 25[OH]D 20 to 29 or < 20, replenish with Vitamin D 5,000 IU daily for 8-12 wks to achieve level ≥ 30
Sturdy study- falls in community dwelling ≥ 70 yrs 200 & 1,000 iu/ day fewer falls than 2,000 or 4,000 iu/ day
groupNo benefit from higher doses
Appel,L; Michols,E, et al. The Effects of Four doses of Vitamin D Supplements on Falls in Older Adutls. Ann Intern Med. 2021;174:145–156.
Too Fit To Fracture RecommendationsFor preventing bone loss and falls, recommend a combination of: Strength training for major muscle groups ≥ 2x/week Balance challenges daily Moderate-to-vigorous aerobic physical activity ≥ 150 min/week, or 20-
30 min per dayTo reduce spine loads, recommend: Exercises for back extensor muscles daily Spine sparing strategies – hip hinge for bending, step-to-turn instead of
twisting, holding loads close to body
Giangregorio LM, et al Osteoporos Int. 2014

https://cdn.nof.org/wp-content/uploads/2016/05/Safe-Yoga-NOF-Flyer-2016.pdf
Physical Therapy for Bone Health
Physical TherapyMedicare accepts Physical Therapy ICD 10 diagnosis code of
Osteopenia (M85.80) or Osteoporosis (M81.0) • 1-3 sessions usually all that is needed for osteopenia to
review posture and exercise routine.Rx: Osteoporosis/ Osteopenia: Physical Therapy to evaluate,
treat and instruct in spine safe posture and exercise to optimize strength and balance. Minimize fall risk.
• VCF- decreases risk of subsequent VCF’s
AAFP Endorsed 2017 - ACP Guideline Update:Treatment of Low Bone Density or Osteoporosis to Prevent Fractures in Men and Women
1. Treat with alendronate, risedronate, zoledronic acid or denosumab to reduce the risk for hip and vertebral fractures in women who have known osteoporosis(grade: strong rec; high-quality evidence)
2. Treat osteoporotic women with pharmacological therapy for 5 years.(Grade:weak rec; low-quality evidence)
3. Treat with bisphosphonates to reduce the risk for vertebral fracture in men who have clinically recognized osteoporosis.(Grade: weak rec:low-quality evidence)
AAFP Endorsed 2017 - ACP recommendations cont.
4. Against bone density monitoring during the 5-yr period pharmacologic treatment period for osteoporosis in women. (Grade:weak rec; low quality evidence).
5. Against using menopausal estrogen therapy or menopausal estrogen plus progestogen therapy or raloxifene for the treatment of osteoporosis in women.(Grade:strong rec; mod-quality evidence).
6. Treat osteopenic women 65 yrs age and older who are at a high risk for fracture based on a discussion of pt preferences, fracture risk profile, and benefits, harms, and costs of medications. (Grade:weak rec.;low-quality evidence)
Pharmacology• Antiresorptive
Bisphosphonates• Alendronate (Fosamax)• Ibandronate (Boniva)• Risedronate (Actonel)• Zoledronic Acid (Reclast)
Denosumab (Prolia)Raloxifene (Evista)EstrogenCalcitonin
Anabolic (Bone Forming)Teriparatide (Forteo)Abaloparatide (Tymlos)Rozosumab (Evenity)
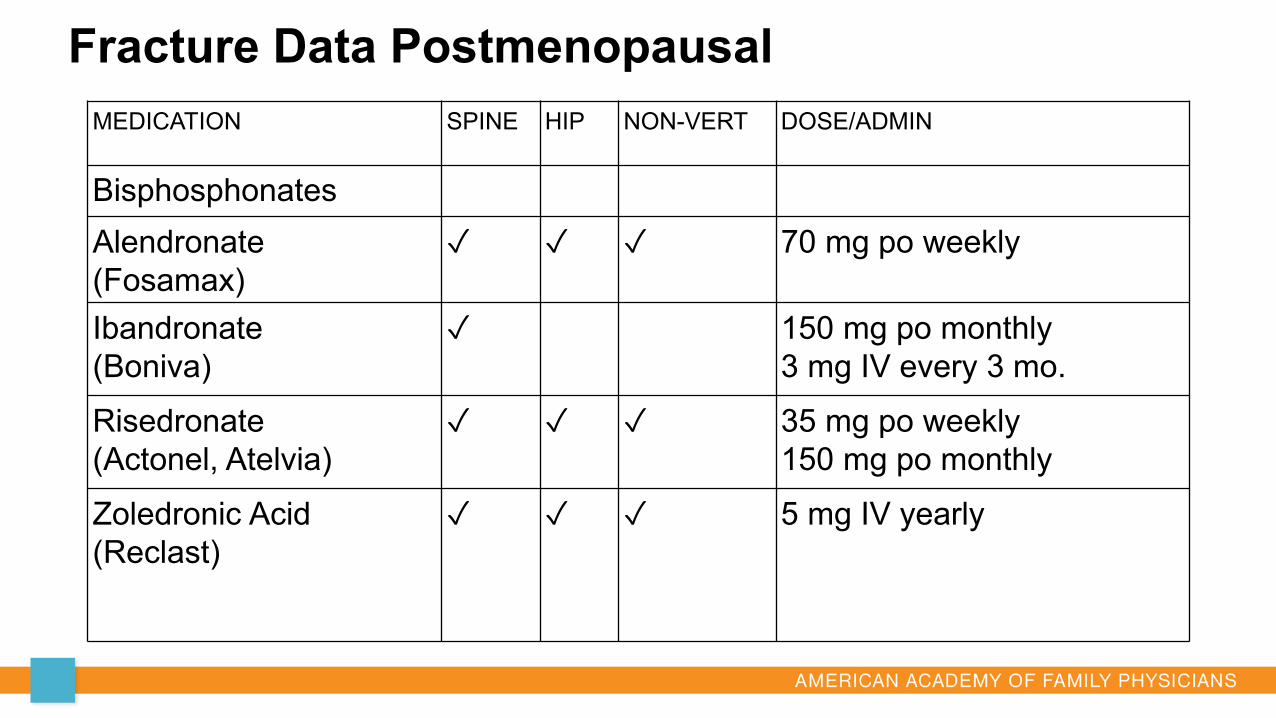
Fracture Data PostmenopausalMEDICATION SPINE HIP NON-VERT DOSE/ADMIN
BisphosphonatesAlendronate(Fosamax)
✓ ✓ ✓ 70 mg po weekly
Ibandronate(Boniva)
✓ 150 mg po monthly3 mg IV every 3 mo.
Risedronate(Actonel, Atelvia)
✓ ✓ ✓ 35 mg po weekly150 mg po monthly
Zoledronic Acid(Reclast)
✓ ✓ ✓ 5 mg IV yearly
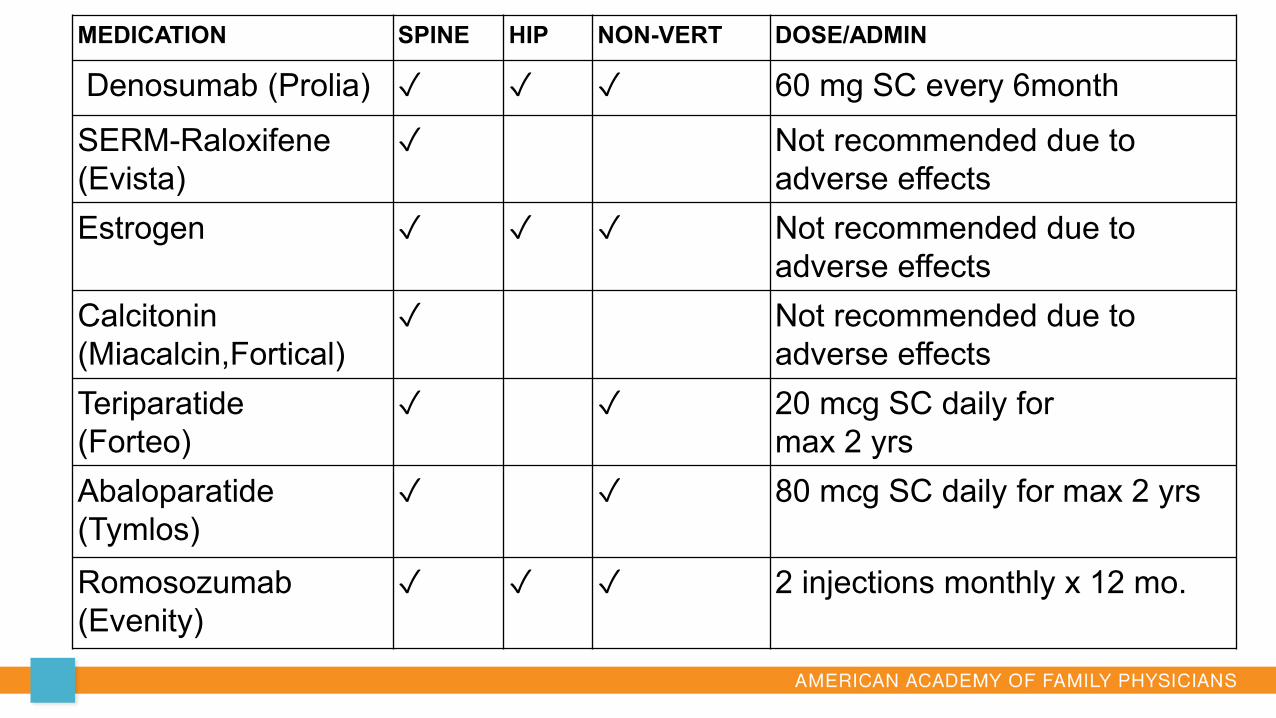
MEDICATION SPINE HIP NON-VERT DOSE/ADMIN
Denosumab (Prolia) ✓ ✓ ✓ 60 mg SC every 6month
SERM-Raloxifene(Evista)
✓ Not recommended due to adverse effects
Estrogen ✓ ✓ ✓ Not recommended due to adverse effects
Calcitonin(Miacalcin,Fortical)
✓ Not recommended due to adverse effects
Teriparatide(Forteo)
✓ ✓ 20 mcg SC daily for max 2 yrs
Abaloparatide(Tymlos)
✓ ✓ 80 mcg SC daily for max 2 yrs
Romosozumab(Evenity)
✓ ✓ ✓ 2 injections monthly x 12 mo.
Bisphosphonates (BP)
• PMW, men, steroid induced osteoporosis• Fx Reduction RR in Postmenopausal women from RCTs:
Spine ~50% alendronate, risedronate, zoledronic acid & ibandronate
Hip ~ 40% with all except ibandronate• Short term (3-5 yrs) benefits far exceed risks• Long term (>5 yrs) benefits smaller, risks higher• Oral alendronate first line due to efficacy, safety data, cost $7/month.• Specific dosing regime due to adverse effects of esophagitis• IV-Zoledronic acid, if unable to follow oral dosing or GI intol• Caution: CrCl <35; Hypocalcemia-monitor Ca, Mg, PO4
AFF: Associated with long-term use >5 yrs. Evaluate for Drug holiday after 5 yrs of treatmentRare <0.1% or absolute risk 5 cases/10,000 pt tx yrsInquire about thigh or groin painEvaluate any pain for stress fracture with bil femur x-rays
ONJ: Rare 1/10,000 to 1/100,000 riskConsider dental exam prior to startingRecommend good oral hygiene
Atypical Femoral Fractures(AFF) & Osteonecrosis of Jaw (ONJ)Rare serious adverse effects: Bisphosphonates
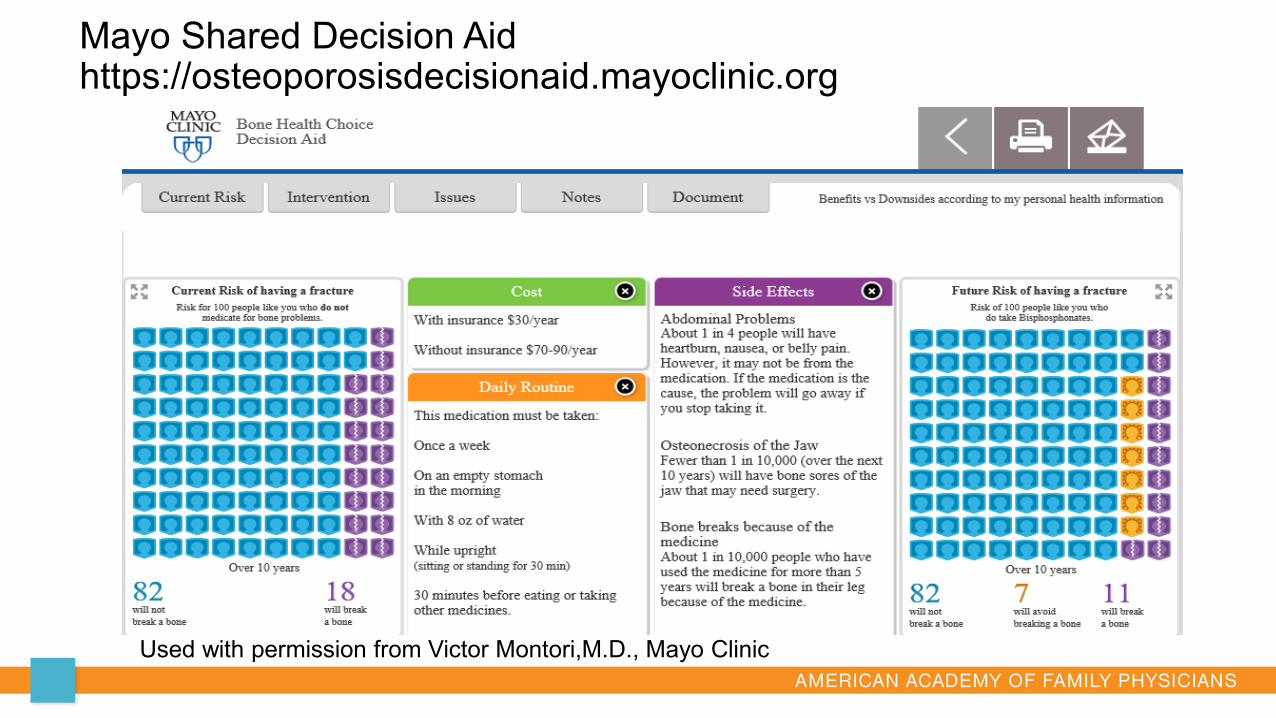
Used with permission from Victor Montori,M.D., Mayo Clinic
Mayo Shared Decision Aid https://osteoporosisdecisionaid.mayoclinic.org
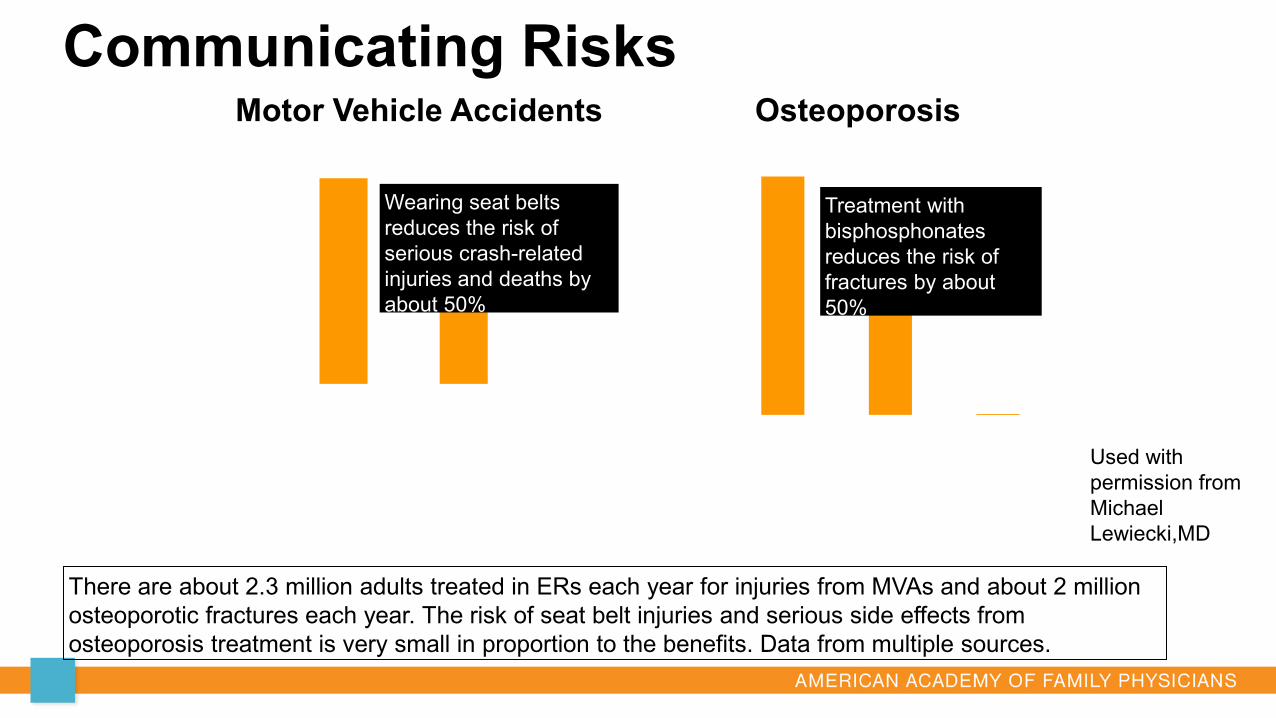
Communicating RisksMotor Vehicle Accidents
0
25
50
75
100
Injuries &Deaths
WearingSeat Belt
Seat BeltInjuries
Osteoporosis
0.
25.
50.
75.
100.
FracturesUntreated
FracturesTreated
ONJ +AFF
Wearing seat belts reduces the risk of serious crash-related injuries and deaths by about 50%
Treatment with bisphosphonates reduces the risk of fractures by about 50%
There are about 2.3 million adults treated in ERs each year for injuries from MVAs and about 2 million osteoporotic fractures each year. The risk of seat belt injuries and serious side effects from osteoporosis treatment is very small in proportion to the benefits. Data from multiple sources.
Used with permission from Michael Lewiecki,MD
AES Question
A. After treatment with an oral bisphosphonate for 5 yrsB. After treatment with IV bisphosphonate (zoledronic acid) for
3 yrsC. After treatment with denosumab for 5 yrsD. After treatment with teriparatide for 2 yrsE. A and B
Question 3
In which scenario is it appropriate to consider a Drug Holiday?
Time for a Bisphosphonate (BPs) Drug Holiday?
Risk of AFF, but not ONJ, increases with BP therapy > 5yrBMD increase for upto 3 yrs, no further gain thereafter. No further reduction in fx risk beyond 3-5 yrsRetained in skeleton with long half life, Residual effect after discontinuationZoledronic acid- longest residual effectRisedronate- shortest
Consider drug holiday, after 5 yr of oral BP or3 yr of IV BP( Zolendronate)
Evaluate with DXA and Vertebral Fracture Assessment (VFA)
Time for a Bisphosphonate Holiday?
Consider a Drug Holiday if fracture risk is no longer high: T-score greater than -2.5Patient has remained fracture freeRepeat DXA after 2 yrs of holiday
Patients remaining high risk, continue oral BP additional 5 yrs(up to 10 yrs) and up to 6 yrs for IV BP(Zoledronate) before drug holiday
AES Question
Which is NOT correct regarding a drug holiday?
A. “Holiday” is a bisphosphonate(BP) specific concept, not appropriate for denosumab or other non-bisphosphonate drugs
B. Consider drug holiday after 5yr oral BPs or 3yrs IV BPs. Patients who remain high fracture risk, consider continuing oral BPs up to 10yr and IV BPs up to 6yr.
C. It not recommended to check a DXA again for patients on BPs Drug Holiday
D. If denosumab is discontinued, patients should be transitioned to a bisphosphonate to lower risk of discontinuation vertebral fractures
Question 4
BPs Drug Holiday ≠ Drug Retirement
During BPs drug holiday, assess need to resume treatment every 2-4y with DXA. Fracture risk starts to increase about 2 yrs after
stopping BPs.Risk of AFF resolves quickly (1 yr) Resume therapy whenA fracture occursPatient meets initial treatment criteria
What if there is progression of bone loss or fracture while on oral Bisphosphonate?
Assess complianceRe-evaluate for causes of secondary osteoporosisSwitch to injectable anti-resorptive(zolendronate or
denosumab) if on oral agent
Roles for Bisphosphonates
Initial treatment for osteoporosisLast treatment for anabolic treatment sequence to
maintain the benefitsTreatment after denosumab withdrawal to lower risk of
discontinuation vertebral compression fractures. Long-term maintenance of BMD, sequence on and off
BPs.
Denosumab –DMab (Prolia) Monoclonal antibody, RANKL inhibitor, approved for PMW and men. Approved for cancer induced bone loss from hormone ablation tx. Administer: SQ inj 60 mg every 6 mo.; Cost $1,000/ inj Freedom Trial: reduces vertebral, non-vertebral, and hip fractures Freedom Ext study 10y low rate of adverse events, fracture risk
further reduced and continued BMD gains with longer term therapy Caution: If risk of hypocalcemia, CrCl < 30, check calcium 10d after
injection. Adverse: Infection skin. Rare complications include AFF and ONJ Delayed dose or discontinuation is associated with Multiple
Vertebral Fractures and rapid loss of BMD. Reasonable initial therapy in those with life expectancy <10 yr Transition to BPs to avoid fractures is complicated.
Transition off Denosumab –DMab (Prolia)Vertebral fractures occurred as early as 2 month delay (8 months
from last inj). Do not stop DMab w/o transition to a BPsAlendronate has been shown to maintain BMD and decrease
vertebral fractures after Dmab.Alendronate can be initiated 6 months after last Dmab dose
minimum of 1-2 yrs, then consider bisphosphonate drug holiday. IV Zoledronic Acid(ZA) likely effective but timing uncertain,
possibly 7 months after last Prolia when bone turnover increases.One expert measures serum CTX monthly beginning seven
months after the last Dmab inj and administers IV ZA once CTX is at the upper limit of the ref range for premenopausal women (eg, >600 pg/mL in an assay with ref range 93 to 630 pg/mL).
Estrogen with or without Progestin; or RaloxifeneRecommend AGAINST for treatment of osteoporosis in women. ACP Grade: strong recommendation against Increased risk of stroke and thromboembolic eventsConsider Raloxifene if independent need for breast cancer
prophylaxis
Estrogen + Bazedoxifene = (Duavee) FDA indication for prevention of osteoporosisNo RCT with primary fracture outcomes
Calcitonin FDA-approved for PMW when alternative treatments are not
suitable. Reduces vertebral fractures 30% in those with prior vertebral
fractures. Not been shown to reduce non-vertebral or hip fractures.Administer: 200 IU intranasal spray. SQ availableAdverse effects: suggested increased risk of malignancies
Risk Stratification-AACE 2020 updateVery High Fracture RiskChoice of initial agent to include anabolic meds in pts with:
Advanced age; frailty; increased fall risk Fractures-
Recent <12 months; multiple or while on therapy; Glucocorticoids T score <-3.0High fracture probability by FRAX
Anabolic Therapy: PTH1 Receptor ligandsTeriparatide(PTH 1-34) and Abaloparatide (PTHrP)
Teriparatide (Forteo) and Abaloparatide (Tymlos) PMW high risk for fracture (h/o of fx or multiple risk factors) or who have
failed/intolerant to other therapies. Reduce vertebral and non-vertebral fractures; not hip Daily SQ injection. Cost estimate: $1,500 to 3,000/ month Limited to 2 years in lifetime Contraindicated: in patients with increased risk of osteosarcoma
Paget’s disease, prior radiation therapy skeleton, bone metastases, hypercalcemia, or a history of skeletal malignancy
Teriparatide- also indicated for men at high fx risk; steroid induced OPAbaloparatide- lower incidence of hypercalcemia, no need to refrigerate
Romosozumab “Evenity”
Monoclonal AB to sclerostin; FDA approved April 2019 Indication: PMW at high risk 2 Injections monthly x 12 months Primarily anabolic Follow by an antiresorptive Serious Reactions: MI, CVA, CV death, hypcalcemia, ONJ, AFF Should not be used if MI, CVA in previous yr
Sequencing of Anabolic and Antiresorptive Therapies Lifelong treatment with sequencing of medications and holidays. Only BPs safely precede holidays. Anabolic agents shown to have greater BMD gains when used
prior to an antiresorptive agent. Consider anabolic agents as initial tx in VERY high risk patientsAnabolic response may be blunted for a period of time after BPs Follow 2 yr anabolic therapy with antiresorptive (BPs or DMab) to
maintain BMD gains.Do not transition to anabolic after Dmab due to increased fx risk.
Interval Care for During Treatment Patients taking medications need to be evaluated annually Calcium, diet, exercise, lifestyle, new meds or chronic diseases Inquire if any thigh or groin pain Exam: height. 2 cm (0.8 in) loss, repeat VFA. Labs: creatinine, calcium, Mg, Vit D
DXA interval BMD testing during treatment- no RCT ACP- recommends against testing during 5 yr treatment.
- Reduced fractures with treatment even if BMD did not increase NOF: recommends every 2 yrs ISCD: If stable or increased, repeat at 5 years. If BMD decrease ≥ 5% Inquire about non-compliance; assess for secondary causes. If poor absorption of oral BP, consider switch to IV bisphosphonate
Healthy Bones for Life: Primary PreventionNCQA HEDIS measure: Number of women ≥ 65 yrs who report ever
having a BMD test. Repeat DXA interval depends on initial BMD. If no risk factors:
- Normal DXA T score >-1.49, repeat 10-15 yrs or more- T score -1.50 to -1.99, repeat in 3-5 years- T score -2.0 or less, repeat in 2 years
Patient education is the foundation of care Provide referral to Physical Therapy, Registered Dietician Consider utilizing CPT code 99490 Chronic Care Management Consider starting an NOF Support Group / Lecture Series
Improving Bone Health after a FractureNCQA HEDIS measure: Number of women ≥ 65-85 yrs who
suffered a fracture and who had either BMD or a prescription for a drug to treat osteoporosis. In adults ≥ 50 y, after a fracture, assess FRAX for DXACare coordination programs after fractureNOF- Fracture Liaison Bone Health TeleECHOAmerican Orthopedic Assoc.: Own the Bone International Osteo Foundation: Capture the Fracture
USPSTF Recommendations 2018Fall prevention in community-dwelling ≥ 65 y
Exercise intervention to prevent falls (B recommendation)Multifactorial interventions to prevent falls (C recommendation) medications, medical conditions, environmental hazards ie: CDC STEADI Program
Vitamin D supplementation not recommended (D recommendation)
These apply to community-dwelling adults NOT known to have osteoporosis or Vitamin D insufficiency or deficiency.
Practice RecommendationsActively counsel patients on the prevention of osteoporosisUse a Formal Risk Assessment Tool to identify patients for
screening and treatment of osteoporosisOsteoporosis treatment should be individualized with long-term
strategies discussed with the patient.Consider oral bisphosphonates as first line for appropriate patientsEvaluate for bisphosphonate drug holidays with DXA and VFACounsel patients on denosumab discontinuation risk & strategies. Encourage patients to exercise to decrease their fracture and fall
risk.

Questions?
Advent Health Family Medicine Residency and Geriatric Medicine
Fellowship
Robin Creamer, DO, CAQGM, [email protected]
133 Benmore Dr, Suite 200Winter Park, FL 32792Office: 407-646-7757Fax: 407-646-7775
References Adler RA, El-Hajj Fuleihan G, et al. Managing Osteoporosis in Patients on Long-Term
Bisphosphonate Treatment:Report of a Task Force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2016 Jan;31(1):16-35. Appel,L; Michols,E, et al. The Effects of Four doses of Vitamin D Supplements on Falls in
Older Adutls. Ann Intern Med. 2021;174:145–156 Black DM, Schwartz AV, Ensrud KE et al (2006) Effects of continuing or stopping alendronate
after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA 296(24):2927–2938 Camacho,P, et al. AACE/ACE Clinical Practice Guidelines for the Diagnosis and Treatment of
Postmenopausal Osteoporosis-2020 update. https://doi.org/10.4158/GL-2020-0524SUPPL Cosman F, de Beur SJ,et al. Clinician’s Guide to Prevention and Treatment of Osteoporosis.
Osteoporosis International. 2014;25:2359-81. PMID 25182228 Ethel S. Siris; et al. Bone Mineral Density Thresholds for Pharmacological Intervention to
Prevent Fractures. Arch Intern Med. 2004;164(10):1108-1112.
References Giangregorio,LM,et al. "Too Fit To Fracture: exercise recommendations for individuals with
osteoporosis or osteoporotic vertebral fracture." Osteoporosis International 25.3 (2014): 821-835. Kanis JA, on behalf of the World Health Organization Scientific Group. Assessment of
osteoporosis at the primary health care level. WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield 2007. Mayo Clinic Shared Decision Making National Resource Center.
http://shareddecisions.mayoclinic.org/decision-aid-information McClung MR, et al (2017) Observations following discontinuation of long-term denosumab
therapy. Osteoporo Int 28:1723-1732 National Committee for Quality Assurance. HEDIS & Performance Measurement.
www.ncqa.org/HEDISQualityMeasurement.aspx National Institute of Health. National Osteoporosis Foundation(NOF) www.nof.org Office of the Surgeon General (US) (2004) Bone health and osteoporosis: a report of the
Surgeon General. Office of the Surgeon General (US), Rockville (MD). Available from: http://www.ncbi.nlm.nih.gov/books/NBK45513
References Qaseem A, et al; Treatment of low bone density or osteoporosis to prevent fractures in
men and women : a clinical practice guideline update from the American College of Physicians. Ann Intern Med. 2017 Jun 6;166(11):818-839. PMID: 28492856 Shepstone L, et al; SCOOP Study Team. Screening in the community to reduce fractures
in older women (SCOOP). Lancet. 2018:391(10122):741-747. doi:10.1016/50140-6736(17)32640-5. U.S. Preventive Services Task Force. Interventions to Prevent Falls in Community-
Dwelling Older Adults. JAMA. 2018;319(16):1696-1704. doi:10.1001/jama.2018.3097 U.S. Preventive Services Task Force. Vit D, calcium or combined supplementation for
Primary Prevention of Fractures in Community-dwelling Adults. JAMA. 2018;319(15):1592-1599. doi:10.1001/jama.2018.3185 U.S. Preventive Services Task Force. Screening for Osteoporosis: U.S. Preventive
Services Task Force recommendation statement. JAMA. 2018;319(24):2521-2531.doi:10.1001/jama2018.7498
Answers
1. B2. C3. E4. C