Embed Size (px)
Citation preview

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Other Immigrant Studies:
Cancer and Cancer Registration
Prof. Oliver Razum
Melina Arnold
EUNAM Meeting
Ferrara, 9 Sep 2011 1

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Outline
• Examples of „typical“ projects• MigHealthNet
• MEHO
• MEHO: WP Cancer in Migrants• Migrant health from a lifecourse perspective
• Migration-sensitive Cancer Registration• Survey
• Building migration-sensitive health indicators in
cancer research
• Country Reports2

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
MigHealthNet (1)
• Supported by the EC's Directorate-General Health and
Consumer Protection (DG SANCO) and the Stavros
Niarchos Foundation (completed in April 2009)
Objectives
• to stimulate the exchange of knowledge and the formation
of networks on migrant and minority health through the
development of interactive databases in each of the
participating countries
• to give professionals, policy makers including health
authorities, researchers, educators and representatives of
migrant and minority groups easy access to a virtual
network of expertise3
See also: http://mighealth.net/
Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
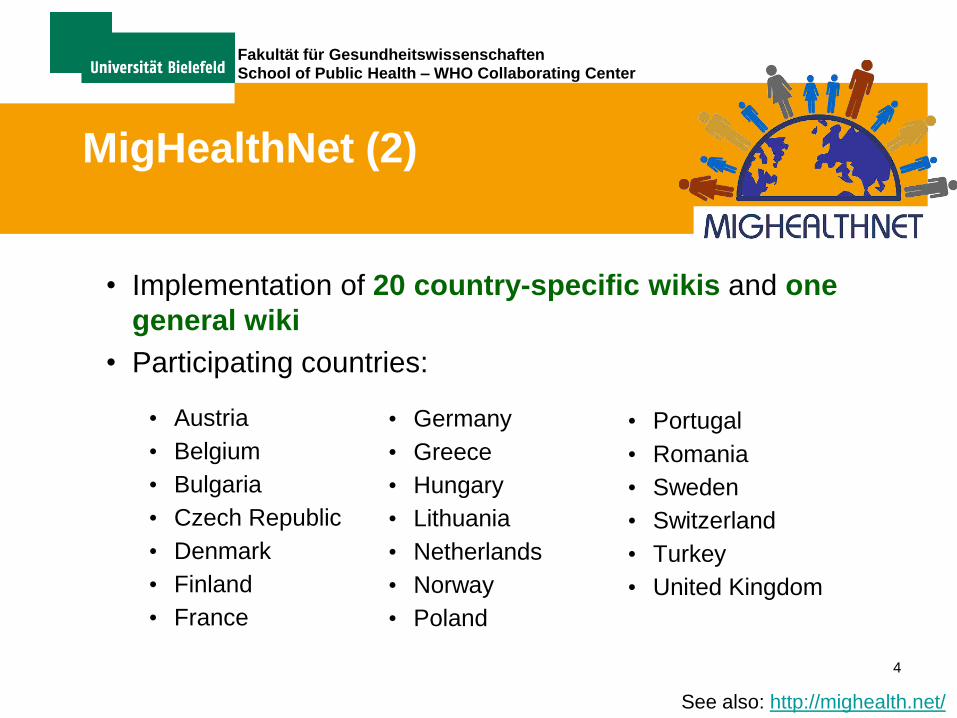
MigHealthNet (2)
• Implementation of 20 country-specific wikis and one
general wiki
• Participating countries:
• Austria
• Belgium
• Bulgaria
• Czech Republic
• Denmark
• Finland
• France
4
• Germany
• Greece
• Hungary
• Lithuania
• Netherlands
• Norway
• Poland
• Portugal
• Romania
• Sweden
• Switzerland
• Turkey
• United Kingdom
See also: http://mighealth.net/

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
MEHO (1)
• Migrant and Ethnic Health Observatory
• Funded under the framework of the Public Health
Programme 2003-2008 of the European Commission
Objectives
• to develop indicators to monitor the health status of
immigrants and ethnic minorities
• to approach the conceptual, methodological, ethical and
practical issue of identifying immigrants and ethnic
minorities in health databases
• to conduct valid comparisons between these groups within
and between European countries and migrant groups 5
See also: http://www.meho.eu.com/

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
MEHO (2)
• Five critical health areas/ workpackages
• Mortality
• Cardiovascular Disease and Diabetes
• Cancer
• Infectious Diseases
• Self-perceived health and health care use
• Partners
• Erasmus MC Rotterdam, The Netherlands
• Amsterdam Medical Center/ University of Amsterdam, The Netherlands
• University of Edinburgh, Scotland
• Bielefeld University, Germany
• University of Copenhagen, Denmark
• University of P.J. Safarik Kosice, Slovakia6
See also: http://www.meho.eu.com/

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Cancer in Migrants (I)
• Cancer risks vary
• geographically
• within and between populations
• Assessing the relevance of
• environmental („nurture“) components
• genetic („nature“) components
Lifecourse perspective
Allowing progress in etiology research
Allowing migrant-specific prevention means
7

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Cancer in Migrants (II)
• Greater likelihood to develop cancers with a relation to infectious diseases
• Oral cavity, nasopharynx, stomach, liver, gallbladder, cervix uteri, lymphoma
• Decreased risk for cancers associated with a ‚Western‘ lifestyle
• Colorectum, pancreas, lung, breast, ovary, kidney, bladder
8
Arnold, M., O. Razum, and J.W. Coebergh, Cancer risk diversity in non-western migrants to Europe: An overview of the
literature. European journal of cancer (Oxford, England: 1990), 2010. 46(14): p. 2647-59.

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Cancer in Migrants (III)
1. Lower all-cancer risk coincide in most studies
irrespective of exact migrant origin
health/epidemiologic transition
2. Susceptibility to certain cancers
life-course perspective can help to identifyimportant exposures during life
3. Cancer risks in migrants converge over time
to be investigated
9
Arnold, M., O. Razum, and J.W. Coebergh, Cancer risk diversity in non-western migrants to Europe: An overview of the
literature. European journal of cancer (Oxford, England: 1990), 2010. 46(14): p. 2647-59.

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Migrant health from a lifecourse perspective
10
Spallek J., Zeeb H., Razum O. What do we have to know from migrants‘ past exposures to understand their health status?
A lifecourse approach. Emerg. Themes Epidemiol. 2011. Aug 15;8(1):6.

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Migration-sensitive
Cancer Registration
11

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Migration-sensitive Cancer Registration
• Questionnaire-based survey among all European
Cancer Registries (n=191)
• Categorization into ‚exemplary‘ and ‚less than
exemplary‘ registries
• Exemplary = Used indicator of ethnicity: country of birth
• Less than exemplary = Used indicators of ethnicity: nationality or race or country of birth of father or country of birth of mother
12

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Survey Results (I)
13
191 cancer
registries
contacted
182 registries got an
online questionnaire
25 emails
returned
9 registries got a paper
questionnaire
21 registries
got a paper
version
39 registries
answered
4 registries
with wrong
email address
2 answered
118
registries
reminded
78 cancer registries answered response: 40.8 %
3 answered 34 answered
191 cancer
registries
contacted
182 registries got an
online questionnaire
25 emails
returned
9 registries got a paper
questionnaire
21 registries
got a paper
version
39 registries
answered
4 registries
with wrong
email address
2 answered
118
registries
reminded
78 cancer registries answered response: 40.8 %
3 answered 34 answered
Reeske, A., J. Spallek, and O. Razum, Migrant and Ethnic Health Observatory (MEHO): Migrant-sensitive cancer registration in Europe – Results of a survey
conducted among European cancer registries., in Network Eurolifestyle, Neumann G and Kirch W, Editors. 2008, Thieme Verlag: Stuttgart. p. 11-18.
Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
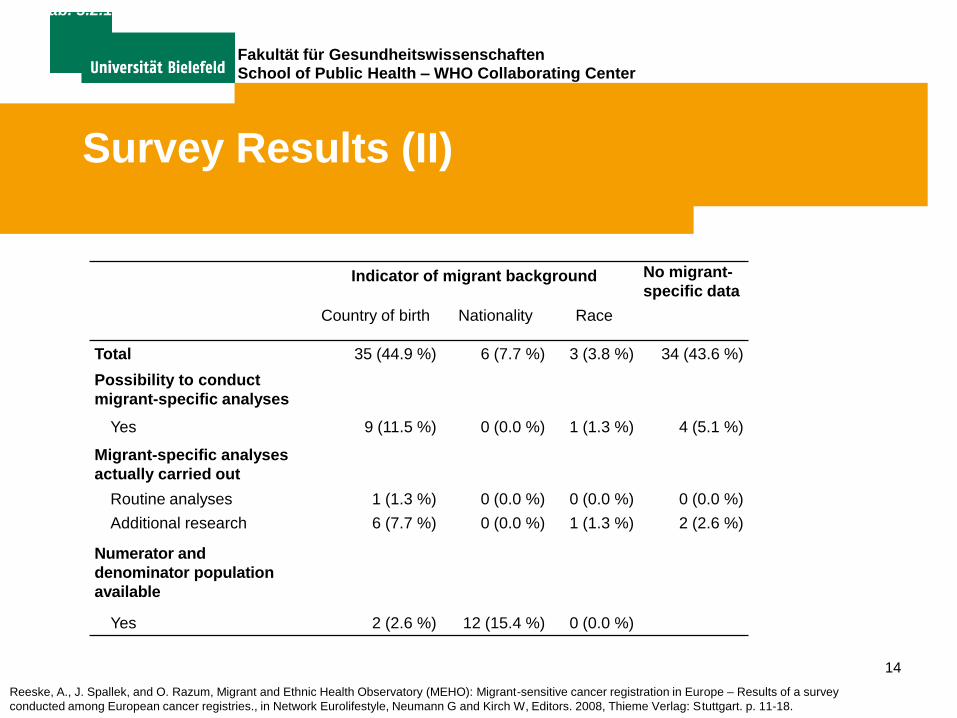
Survey Results (II)
14
Indicator of migrant background No migrant-
specific data
Country of birth Nationality Race
Total 35 (44.9 %) 6 (7.7 %) 3 (3.8 %) 34 (43.6 %)
Possibility to conduct
migrant-specific analyses
Yes 9 (11.5 %) 0 (0.0 %) 1 (1.3 %) 4 (5.1 %)
Migrant-specific analyses
actually carried out
Routine analyses 1 (1.3 %) 0 (0.0 %) 0 (0.0 %) 0 (0.0 %)
Additional research 6 (7.7 %) 0 (0.0 %) 1 (1.3 %) 2 (2.6 %)
Numerator and
denominator population
available
Yes 2 (2.6 %) 12 (15.4 %) 0 (0.0 %)
Tab. 3.2.1: Main results of the survey conducted among European cancer registries in 2007/08 (n = 78)
Reeske, A., J. Spallek, and O. Razum, Migrant and Ethnic Health Observatory (MEHO): Migrant-sensitive cancer registration in Europe – Results of a survey
conducted among European cancer registries., in Network Eurolifestyle, Neumann G and Kirch W, Editors. 2008, Thieme Verlag: Stuttgart. p. 11-18.

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Building migration-sensitive
health indicators in cancer
research
15

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Building migration-sensitive health indicators in cancer research (I)
• For indicators we need
• Cases (numerator of an indicator, e.g. risk)
• Background population (denominator)
• Numerator: Cases are collected in cancer registries
Survey about migrant specific data in European cancer registries
• Denominator: Background population
• Registries might have data or information
• Other data sources, e.g. national statistics
• Data linkage
16

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Building migration-sensitive health indicators in cancer research (II)
• How to merge numerator and denominator:
• Direct methods
• e.g. record linkage
• Indirect methods
• data linkage (ideally using personal identifiers)
• name-based approaches
• Numerator-only approaches
• e.g. PCIR, relative survival, descriptive analyses
17

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Country Reports
18

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Country Reports: An overview
Country Migrants in
(1) General
population (%),
(2) Largest migrant
groups (origin)*
Indicators
available in
(1) Population
data,
(2) Cancer
registry data
Routine
analyses?
Studies on
cancer in
migrants
Main barriers Current/Future
Potentials
Finland:
Finnish Cancer
Registry
(population-
based, national
level)
(1) 4.4% (foreign
country of birth)
(2) Russia, Estonia
(1) Country of
birth,
Citizenship,
Language
(2) None
• No.
• Using linkage
procedures
• Time consuming
permission procedures
• Costs of additional data
extraction
• Small number of cancer
cases among migrants
• Data linkage
through personal
identity code PID
• Inclusion of
country of origin in
CR data
Germany:
Regional
registries (all 16
federal states
covered in 2011,
completeness
fits international
standards in 14
federal states)
(1) ~20% (migration
background)
(2) Eastern Europe
(resettlers),
South and South
Eastern Europe
(Turkey)
(1) None (Country
of birth in
Mikrocensus
data)
(2) None.
• No.
• Using a name-
based approach
to identify
Turkish cancer
cases
• Setting up a
historical cohort
of resettlers
from the FSU
• Data protection not
officially clarified
• German history
(prosecution of ethnic
minorities)
• Organisation of CRs on
federal state level by
federal state law
lacking data comparability
• Lacking of migrant
indicators in population
data
• Indirect methods
(e.g. name-based
approaches)
• Numerator-only
analyses
• Data linkage
procedures
19
Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
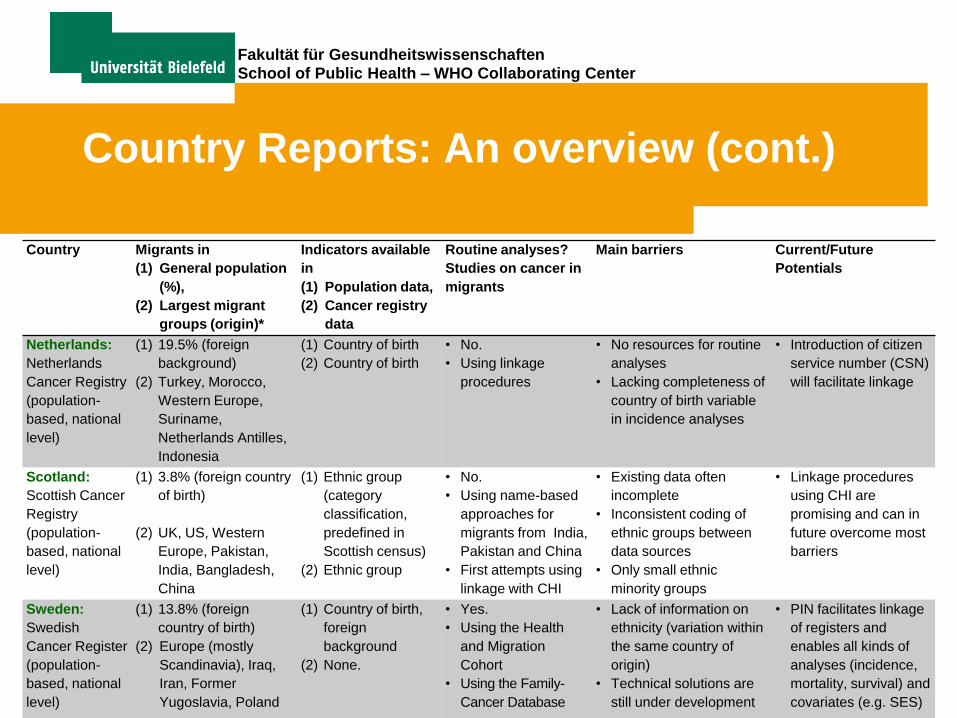
Country Reports: An overview (cont.)
Country Migrants in
(1) General population
(%),
(2) Largest migrant
groups (origin)*
Indicators available
in
(1) Population data,
(2) Cancer registry
data
Routine analyses?
Studies on cancer in
migrants
Main barriers Current/Future
Potentials
Netherlands:
Netherlands
Cancer Registry
(population-
based, national
level)
(1) 19.5% (foreign
background)
(2) Turkey, Morocco,
Western Europe,
Suriname,
Netherlands Antilles,
Indonesia
(1) Country of birth
(2) Country of birth
• No.
• Using linkage
procedures
• No resources for routine
analyses
• Lacking completeness of
country of birth variable
in incidence analyses
• Introduction of citizen
service number (CSN)
will facilitate linkage
Scotland:
Scottish Cancer
Registry
(population-
based, national
level)
(1) 3.8% (foreign country
of birth)
(2) UK, US, Western
Europe, Pakistan,
India, Bangladesh,
China
(1) Ethnic group
(category
classification,
predefined in
Scottish census)
(2) Ethnic group
• No.
• Using name-based
approaches for
migrants from India,
Pakistan and China
• First attempts using
linkage with CHI
• Existing data often
incomplete
• Inconsistent coding of
ethnic groups between
data sources
• Only small ethnic
minority groups
• Linkage procedures
using CHI are
promising and can in
future overcome most
barriers
Sweden:
Swedish
Cancer Register
(population-
based, national
level)
(1) 13.8% (foreign
country of birth)
(2) Europe (mostly
Scandinavia), Iraq,
Iran, Former
Yugoslavia, Poland
(1) Country of birth,
foreign
background
(2) None.
• Yes.
• Using the Health
and Migration
Cohort
• Using the Family-
Cancer Database
• Lack of information on
ethnicity (variation within
the same country of
origin)
• Technical solutions are
still under development
• PIN facilitates linkage
of registers and
enables all kinds of
analyses (incidence,
mortality, survival) and
covariates (e.g. SES)

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Conclusion
• Major barriers identified
- Incompleteness of nationality data in the registries
- Naturalized immigrants
- Background population/denominator must be defined in the same way as numerator
- Heterogeneity of migrant groups and origins
- Heterogeneity of applied definitions and measures of association
- 100% overlap of catchment area of registry and statistical region for background population is needed
21

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Projects
22

Fakultät für Gesundheitswissenschaften School of Public Health – WHO Collaborating Center
Suggested readings
23