Embed Size (px)
Citation preview

OtosclerosisOtosclerosis ((OtospongiosisOtospongiosis):):ThomograficThomografic and audiometric and audiometric analisisanalisis..
Diego R. Hermann MD, Diego R. Hermann MD, JoãoJoão F. F. NogueiraNogueira JrJr MD, MD, RonaldoRonaldo R. R. AmAmééricorico MD, MD, IuloIulo S. S. BaraunaBarauna FFoo. MD, Fernando O. . MD, Fernando O. BalieiroBalieiro MD, Aldo C. MD, Aldo C. StammStamm MD PhD.MD PhD.
Sao Paulo ENT CenterProfessor Edmundo Vasconcelos Hospital.
Sao Paulo – Brazil.
INTRODUCTIONINTRODUCTIONINTRODUCTION
AbstractAbstractAbstract
METHODSMETHODSMETHODS
RESULTSRESULTSRESULTS
CONCLUSIONCONCLUSIONCONCLUSION
REFERENCESREFERENCESREFERENCES
Otosclerosis is an osseous dyscrasia limited to the human temporal bone (1). It is diagnosed clinically on the basis of otoscopy, audiometry, and tuning fork tests . CT can be used when the diagnosis is in doubt, in some patients with bilateral disease and in those cases with mixed deafness (2). In the majority of cases, the lesion may appear quiescent and limited to the anterior oval window, without stapes involvement. However, the process can spread across the stapedial annular ligament and fix the stapes, producing a conductive loss. Alternatively, it can surround the cochlea and parts of the labyrinth causing a sensorineural loss (1). Otosclerosis can be classified as fenestral and cochlear. Fenestral otosclerosis occures in the region of the fissula antefenestram, anterior to the oval window niche (3). CT can visualize the extend of the pathology involving the oval window, footplate and the round window. When otosclerotic foci affect the cochlear capsule, there is a variable disruption of the density and outline of the capsule (2).
1.Linthicum FH. Histopatology of Otosclerosis. Otolaryngol Clin North Am. 1993; 26: 335-352.
2. Valvassori GE. Imaging of Otosclerosis. Otolaryngol Clin North Am. 1993; 26 (3): 359-71.
3. Barr MS, Lewin JS. Computed tomografic evaluation of otosclerosis. Am J Otolaryngol. 1993; 14 (4): 282-284.
Temporal bone CT scan, with 1 mm slices, has a high sensitivity in detecting otosclerotic foci in those patients with clinical and audiometric findings of fenestral or cochlear otosclerosis. The focus location (on CT) may predict worse sensorineural hearing loss but had little relationship with other audiometric findings in these patients.
Diego Rodrigo Hermann.R Borges Lagoa, 1450, 3º. Andar.CEP: 04038-905, Sao Paulo, BrazilE-mail: [email protected]
STUDY GROUP20 patients with clinical
and audiometric findings of otosclerosis.
All had mixed deafness. (fig 1).
10 ♀ e 10 ♂.
CONTROL GROUP20 patients presenting
unilateral or bilateral tinnitus.
No clinical evidence of conductive hearing loss
OBJECTIVEOBJECTIVEOBJECTIVEThe purpose of this study was to correlate computed tomographic (CT) scans and audiometric findings in those patients with clinical features of otospongiosis.
All of patients were submitted to audiometric analysis and temporal bone CT. The axial and the 20-degree coronal oblique projections were studied and 1 mm tick slices were obtained. Areas of the ear studied were (Figures 2 -5): FAF (fissula ante fenestra), RW (round window), AC(anterior cochlea), PC (posterior cochlea), A (cochlear apex), SC (semicircular canals). The CT features above were correlated to adudiometric findings in both groups. Spearmann correlation coefficients were used to determine association between categorical data and independent t-test analysis was performed on hearing thresholds between groups.
Exclusion criteria:History of the acoustic traumaEndolynphatic hydropsYounger than 18 years oldSigns of otitis media on the otoscopic examinationChronic noise exposurePaget’s disease, Osteogenisis imperfecta or Syphilis
Fig. 1: mixed deafness.
Objectives: to correlate computed tomographic (CT) scans and audiometric findings in those patients with clinical features ofotospongiosis. Methods: A prospective study of 20 patients patients with clinical fenestral and cochlear otospongiosis. A control group comprised of 20 patients with tinnitus was selected. All patients were submitted to audiometric analysis and CT features of temporal bone. Conclusion: Temporal bone CT scan has high sensibility to detect otosclerotic foci in those patients with otosclerosis. The presence of pericochlear foci was associated with worse sensorineural hearing loss in our patients.
9 cases FAF2 cases RW4 cases FAF + RW1 case -
4 cases: cochlear foci
MIXED DEAFNESS
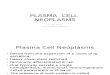
20 patients with otosclerosis, all of them with mixed deafness, and 20 patients with tinnitus completed the study. In 19 patients from study group (Figure 2), there was at least one otospongiosis/otosclerosis focus (95% sensitivity). Nine cases, from the study group, showed only foci in the FAF, two cases in the RW, four cases showed involvement of both FAF and RW. CT scan foci were confirmed at surgery if possible. In the studygroup, four patients presented some foci in the cochlea, in addition to foci in the FAF and RW. In the study group, only one temporal bone CT scan (5%) did not show a radiological feature of disease. In the control group, there were some otoscleroticlike foci in four patients.
0
5
10
15
20
focos
casoscontrole
Figure 2: shows the difference between both groups (study and control) about the presence of otosclerotic foci.
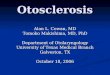
Figure 3: Coronal oblique CT section shows the otosclerosisfoci in the oval window (red arrow) and the cochlea (yellow arrow).
Figure 4: Coronal oblique CT section shows the diffuse involvement of the cochlea (red arrow).
Figure 5: Axial CT section shows the otosclerosis foci in the FAF (red arrow) and the cochlea (yellow arrow).
Figure 6: Three-dimensional MRI shows the diffuse involvement of the cochlea and semicircular canals.
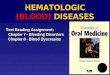
The presence of peri-cochlear (AC,PC,A,SC) or FAF/RW foci did not correlate with the overall PTA loss (Spearman’s Coeff. 0.37 p=0.11 and 0.12 p=0.61). There was a statistically worse SNHL in those patients with peri-cochlear foci (mean∆ 5.3dB p=0.02 Figure 7). The mean air-bone gap (mean∆ 4.1dB p=0.31) and total PTA (mean∆ 9.4dB p=0.10) did not statistically differ in this group. Only one patient did not have FAF/RW involvement and thus a meaningful assessment of data in this group could not be made.
(Study Group)
Fig 7: Influence of peri-cochlear foci
95%Any FAF or RW foci
20%Any pericochlear foci
Range 5 - 3515.8 (SD±6.3)Mean Air-Bone gap
Range 30 - 4536.8 (SD±5.2)Mean cochlear loss (SNHL)
Range 35 - 7052.5 (SD±10.1)Mean PTA
Study group characteristics
Right Ear